

Abstract
[Purpose] The purpose of this study was to examine the agreement between the values obtained by using a hand-held dynamometer with a belt (belt-HHD) and an isokinetic dynamometer (IKD) for the measurement of isometric knee flexion and extension muscle strength. We also studied the factors influencing the measurement. [Participants and Methods] Overall, 26 healthy young adults (16 males, 10 females) participated in the study; the mean age was 21 years. Knee flexion and extension muscle strength were measured by three methods: 1) belt-HHD, 2) conventional IKD with the participant sitting on an attached chair (conv-IKD), and 3) modified IKD with the participant sitting on the same mat table as HHD (mod-IKD). [Results] In the measurement of knee extension, mod-IKD and conv-IKD showed a fixed bias and a proportional bias, conv-IKD and belt-HHD showed a fixed bias, and belt-HHD and mod-IKD showed a fixed bias. In the measurement knee flexion, conv-IKD and mod-IKD showed a proportional bias, belt-HHD and conv-IDK showed a fixed bias, and mod-IKD and belt-HHD showed a fixed bias. In each combination, the measured values were larger in the latter due to errors. However, the types and values of errors differed when analysis was conducted based on gender. [Conclusion] In order to increase the agreement between the values, it is necessary to revise the fixing method of the trunk, and the fixing method of the belt and the sensor pad in belt-HHD.
Keywords: Muscle strength, Hand-held dynamometer, Knee flexion and extension
INTRODUCTION
Measurements of muscle strength using a hand held dynamometer (HHD) are taken by an examiner who is holding the HHD or wearing it on the hand. Therefore, when the moment due to the force applied by the examiner is smaller than the moment of force due to the maximum muscular strength of the person, the value of the measurement is lower than the actual maximum muscle strength of the person1).
Katoh et al.1) examined the reliability of an isometric strength measuring method using a belt to compensate for the fixation of HHD (Belt-HHD) when measuring the strength of the hip joint, knee joint, ankle joint. In the measurement of isometric knee extension muscle strength using the Belt-HHD, the measured foot of the person is fixed with a belt to the pillar of the training bed where the person is sitting. Similarly, when measuring knee flexion muscular strength, the lower leg of the person is fixed by connecting it to the examiner’s leg with a belt. Both knee extension and flexion muscle strength measurements, the length of the belt was adjusted and connected with a metal buckle (Fig. 1).
Fig. 1.
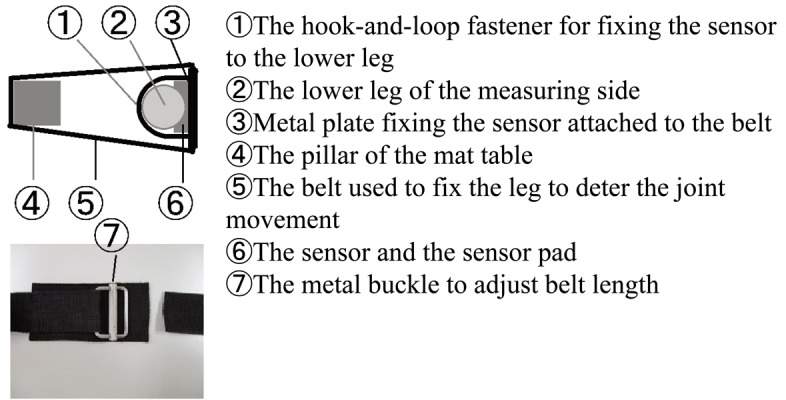
Method for fixing lower limb of measurement side in measurement of knee extension muscle strength using a hand-held dynamometer with a belt.
The validity of muscle strength measurement by HHD is considered on the criterion basis of the measurement value by isokinetic dynamometer (criterion-related validity)2,3,4,5,6,7,8,9,10,11,12). Most of them are examination of knee extension strength measurement. Katoh et al.2) examined the validity of hip joint and knee joint muscle strength measurements using the Belt-HHD and reported that the Pearson’s correlation coefficient between the Belt-HHD measurement and isokinetic dynamometer (IKD) measurement was 0.88 for knee flexion and 0.75 for knee extension. There was a significant difference between measurements obtained by the Belt-HHD and IKD. Therefore, the agreement between the value by isokinetic dynamometer and the value by HHD (and Belt-HHD) is open for examination. In measurement using conventional IKD (Conv-IKD), the back of the seat is inclined low, there is a backrest, and the trunk and pelvis are fixed to the seat with a belt. In Belt-HHD, the seat is horizontal, there is no backrest, and the trunk and pelvis are not fixed. Therefore, Belt-HHD measurements are likely affected by the fact that the pelvis rises during measurement, and the trunk cannot be held vertical. The effect is assumed to be affected when the people have high muscle strength such as young healthy adults and athletes. Therefore, in order to identify the cause of the difference in measurement value between the two, it is necessary to examine the difference due to the difference in slope of the seat surface, trunk, pelvis and thigh fixation, and measurement equipment. Conv-IKD is used to examine the influence of slope of the seat surface, and trunk, pelvis and thigh fixation. In the measurement using IKD, the measurment value when fixing the trunk etc. on the attached chair (Conv-IKD) is compared with the measured value when not fixing the trunk etc. by sitting on the mat table [modified IKD (Mod-IKD)]. In order to examine the influence of the measurement equipment, the measurement values measured by sitting on a mat table are used. Compare the measurement values using Belt-HHD and Mod-IKD.
The purpose of this study was to examine the agreement between Belt-HHD values and Conv-IKD values in isometric knee flexion and extension muscle strength measurements. Therefore, isometric knee flexion and extension strength measurements were measured by three methods: 1) Measurement using Belt-HHD, 2) Measurement using conventional IKD sitting on an attached chair (Conv-IKD), and 3) Measurement using modified IKD sitting on the same mat table as HHD (Mod-IKD). Then, by comparing the values of Belt-HHD and Conv-IKD, and Mod-IKD and Conv-IKD, the influence of seat inclination, trunk, pelvis and thigh fixation was examined. Also, the influence of the measuring equipment was examined by comparing the values of Belt-HHD and Mod-IKD.
PARTICIPANTS AND METHODS
Participants were 26 healthy young adults (16 males, 10 females) with a mean age of 21 years (SD=0.6 years). The average height of participants were 167.3 cm (SD=8.9 cm), and the average weight were 62.0 kg (SD=12.0 kg). The participants were students at Ryotokuji University and volunteered to participate in this research. The research Ethics Committee of Ryotokuji University approved this study (No. 2709), and informed consent was obtained from all participants both orally and in writing.
The isometric knee flexion and extension muscle strength of each participant’s dominant foot (the leg used for kicking a ball) was measured by Belt-HHD, Conv-IKD, and Mod-IKD. Measurements were made by four male physical therapists. All measurements were made under the supervision and management of the main researchers. Measurements were not shared with a participant until all measurements were completed. The two types of muscle activity (knee flexion and extension) were measured in random order. In addition, the order of the three measurement methods (Belt-HHD, IKD, and Mod-IKD) was random. The equipment used for HHD was μTas F-1 (Anima Co., Ltd., Tokyo, Japan), and the system used for IKD was Biodex system 3 PRO (Biodex Medical Systems Inc., New York, NY, USA).
Isometric knee flexion and extension muscle force measurements were made with the knee joint at 90° flexion. For the Belt-HHD measurement, participants sat on the treatment bed, placing both arms on the side of the body and placing the femoral part parallel to the ground by placing a folded bath towel under the popliteal fossa. The height of the bed was set to the height at which the toe on the non-measured side touched the floor. The HHD sensor pad was placed on the distal part of the tibia. The lower end of the HHD sensor pad was adjusted to the height of the upper edge of the medial malleolus. The HHD sensor pad was applied on the anterior surface of the lower leg to measure knee extension and on the posterior surface of the lower leg to measure knee flexion. The sensor pad was affixed to the belt with a hook-and-loop fastener. Then, the HHD sensor was fixed to the participants using a belt. The belt was connected to the pillar of the treatment bed to measure knee joint extension strength and to the lower limb of the examiner to measure knee joint flexion strength. Participants performed knee extension or flexion contraction with maximum effort. However, since the articulation is deterred by the belt, a maximum voluntary isometric muscle strength value is obtained (Fig. 2A, 2B). The unit of measurement was Newton (N). The moment of force (Nm) was calculated by multiplying the measurement value (N) by the distance (m) from the center of the HHD sensor pad to the lateral cleft of the knee joint.
Fig. 2.

Methods of isometric knee flexion and extension muscle strength measurements. A: Knee flexion using by hand-held dynamometer and a belt. B: Knee extension using by hand-held dynamometer and a belt. C: Knee flexion and extension using by conventional isokinetic dynamometer. D: Knee flexion and extension using by modified isokinetic dynamometer.
For Conv-IKD measurements, participants sat on a seat attached to the equipment, both arms were folded in front of the chest, and the trunk and pelvis were fixed to the seat using the attached belt (Fig. 2C).
For Mod-IKD measurements, participants sat on the treatment bed, and both arms were placed on the side of the body (similar to Belt-HHD). Measurements were performed in a sitting position after the femoral part parallel to the ground, the knee joint was flexed 90°, lower limbs were relaxed without exerting strength by muscle contraction, and a bath towel was placed under the popliteal fossa of the side being measured. The height of the treatment bed was set to the height at which both feet of the participant leave the floor. (Fig. 2D). Conv-IKD and Mod-IKD measurements were made in the isometric contraction mode, and the unit of measurement was Nm.
In each measurement, participants performed an isometric contraction exercise with maximum effort for 5 seconds, and the maximum strength during exercise was measured. After one practice, knee extension and flexion muscle strength were each measured twice; a 30-second break was provided after the practice and between each measurement. The larger value of the two measurements was used.
In addition, agreement between values was examined using Bland Altman analysis. R2.8.1 (CRAN, freeware) was used for statistical analysis, and the significance level was set at 1%.
RESULTS
The value of Mod-IKD was lower than that of Conv-IKD in isometric knee extension muscle strength measurements. Knee extensibility measurement showed a fixed bias of 55.8 Nm on average, and also a proportional bias of 32.1% difference on average. Males had an average of 77.4 Nm and females had an average of 21.3 Nm of fixed bias. The value using Belt-HHD was lower than Conv-IKD, and a fixed bias of 33.9 Nm was observed on average. Males on average had a fixed bias of 41.5 Nm, but females did not have a systematic bias. The value using Belt-HHD was higher than Mod-IKD, and a fixed bias of 22.0 Nm was recognized on average. Males had a fixed bias of 35.9 Nm on average. Females had lower Belt-HHD values, with an average deviation of 2.6% difference (Tables 1, 2).
Table 1. Isometric knee flexion and extension muscle values by 3 methods.
| Actions | Gender | n | Methods | Mean (SD) [Nm] |
|---|---|---|---|---|
| Knee extension | F and M | 26 | Belt-HHD | 158.0 (60.9) |
| Mod-IKD | 136.3 (45.5) | |||
| Conv-IKD | 191.9 (70.8) | |||
| M | 16 | Belt-HHD | 193.2 (45.9) | |
| Mod-IKD | 157.8 (44.8) | |||
| Conv-IKD | 234.8 (54.5) | |||
| F | 10 | Belt-HHD | 101.6 (32.4) | |
| Mod-IKD | 101.9 (20.6) | |||
| Conv-IKD | 123.2 (21.3) | |||
| Knee flexion | F and M | 26 | Belt-HHD | 67.9 (23.3) |
| Mod-IKD | 81.4 (22.8) | |||
| Conv-IKD | 81.3 (29.5) | |||
| M | 16 | Belt-HHD | 80.1 (19.8) | |
| Mod-IKD | 94.2 (18.2) | |||
| Conv-IKD | 98.3 (22.3) | |||
| F | 10 | Belt-HHD | 48.4 (13.0) | |
| Mod-IKD | 61.0 (11.6) | |||
| Conv-IKD | 54.0 (15.4) | |||
F: female; M: male; Belt-HHD: Measurement using a HHD and a belt; Conv-IKD: Measurement using the isokinetic dynamometer sitting on an attached chair (Conventional IKD); Mod-IKD: Measurement using isokinetic dynamomete sitting on a mat table (Modified IKD).
Table 2. Results of the Bland-Altman analysis.
| Actions | Gender | n | Systematic bias | Random bias | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Fixed bias [LOA (Nm)] | Proportional bias [%difference] | |||||||||
| Mesurement methods | Mean | Upper | Lower | Mean | Upper | Lower | MDC (Nm) | |||
| Knee extension | ||||||||||
| Conv-IKD–Belt-HHD | M, F | 26 | 33.9 | −15.0 | 82.7 | |||||
| Conv-IKD–Mod-IKD | M, F | 26 | 55.8 | −10.8 | 122.4 | 32.1 | −0.4 | 122.4 | ||
| Belt-HHD–Mod-IKD | M, F | 26 | 22.0 | −36.7 | 80.6 | |||||
| Conv-IKD–Belt-HHD | M | 16 | 41.5 | −2.3 | 85.4 | |||||
| Conv-IKD–Mod-IKD | M | 16 | 77.4 | 20.5 | 134.4 | |||||
| Belt-HHD–Mod-IKD | M | 16 | 35.9 | −19.4 | 91.2 | |||||
| Conv-IKD–Belt-HHD | F | 10 | 59.6 | |||||||
| Conv-IKD–Mod-IKD | F | 10 | 21.3 | 4.1 | 38.4 | |||||
| Belt-HHD–Mod-IKD | F | 10 | −2.6 | −13.7 | 8.4 | |||||
| Knee flexion | ||||||||||
| Conv-IKD–Belt-HHD | M, F | 26 | 13.4 | −10.7 | 37.5 | |||||
| Conv-IKD–Mod-IKD | M, F | 26 | −3.5 | −26.4 | 19.6 | |||||
| Belt-HHD–Mod-IKD | M, F | 26 | −13.5 | −36.2 | 9.2 | |||||
| Conv-IKD–Belt-HHD | M | 16 | 18.3 | −4.1 | 40.6 | |||||
| Conv-IKD–Mod-IKD | M | 16 | 18.6 | |||||||
| Belt-HHD–Mod-IKD | M | 16 | −14.1 | −36.8 | 8.6 | |||||
| Conv-IKD–Belt-HHD | F | 10 | 22.3 | |||||||
| Conv-IKD–Mod-IKD | F | 10 | −7.0 | −13.8 | −0.2 | |||||
| Belt-HHD–Mod-IKD | F | 10 | −12.6 | −19.8 | −5.4 | |||||
F: female; M: male; Belt-HHD: Measurement using a HHD and a belt; Conv-IKD: Measurement using the isokinetic dynamometer sitting on an attached chair (Conventional IKD); Mod-IKD: Measurement using isokinetic dynamomete sitting on a mat table (Modified IKD); LOA: limits of agreement; MDC: minimal detective change.
The value of Mod-IKD was higher than that of Conv-IKD in isometric knee flexion muscle strength measurement, and a proportional error of 3.5% difference was recognized on average. Males did not have systematic bias, but females had a fixed bias of 7.0 Nm on average. The value using Belt-HHD was lower than Conv-IKD, and a fixed bias of 13.4 Nm was recognized on average. Males had an average of 18.3 Nm fixed bias, but females did not have a systematic bias. The value using Belt-HHD was lower than Mod-IKD, and fixed bias of 13.5 Nm was recognized on average. Males had an average of 14.1 Nm and females had an average of 12.6 Nm of fixed bias (Tables 1, 2).
DISCUSSION
In a previous study, a consensus was reached indicating the presence of a significant correlation between measurements of knee flexion strength and extension muscle strength using Belt-HHD and IKD (Conv-IKD)2, 11, 12). However, in those studies, there were statistically significant differences between Belt-HHD and IKD (Conv-IKD) values for knee extension muscle strength. This study is novel in that the effects of seat inclination and trunk, pelvis and femur fixation were examined in terms of agreement with measured values using Conv-IKD and Belt-HHD. This study is also novel in that it uses Mod-IKD as the measurement method.
In the isometric knee extension muscle strength measurement, the value by Mod-IKD was lower than Conv-IKD, and fixed bias and proportional bias were recognized. The cause of the bias was considered to be the effect of fixing the trunk, pelvis, and thigh to a dedicated chair and the inclination of the seat in Conv-IKD. The bias was considered to be greater for subjects with greater muscle strength, or greater for men than women. In addition, the Belt-HHD value was low, the fixed bias was recognized, and similar effects were considered. Males had a fixed bias but females did not have a systematic bias. Therefore, it is necessary to modify the measurement method in order to improve the consistency between the Belt-HHD and Conv-IKD measurements in all participants. However, in previous studies, the validity of HHD or Belt-HHD values based on Conv-IKD has been reported. Therefore, comparison between Belt-HHD values is sufficiently possible.
In the isometric knee extension muscle strength measurement, the comparison results of Mod-IKD and Belt-HHD differed in male and female. The mat bed used and the measurement posture are the same for both measurement methods. Therefore, the cause of the gender difference in the result may be the effect of the device used or the difference in the pad applied to the measurement site. In the future, it is necessary to consider modification of the measurement method.
In the isometric knee flexion muscle strength measurement, the value by Mod-IKD was lower than Conv-IKD, and a proportional bias was recognized. In addition, the value using Belt-HHD was lower than Conv-IKD, and fixed bias was recognized. As these factors, in Conv-IKD, it was thought that the influence which fixed the trunk etc. to a chair and the inclination of the seat influenced. However, the bias for males and females was significantly different for both results. In order to increase the agreement between Belt-HHD and Conv-IKD measurements in all participants, it is necessary to modify the measurement method. In measurement of knee flexion, the buttocks are likely to shift forward and the measured value may be low. In the previous study2), the correlation coefficient of the value using Belt-HHD based on IKD (Conv-IKD) was 0.49. Therefore, in the measurement using Belt-HHD, it was considered at least necessary to prevent the shift of the buttocks.
The value of Belt-HHD was lower than Mod-IKD in isometric knee flexion muscle strength measurement, and fixed bias was observed. However, because the posture and mat bed used were the same, this factor was considered to be different from the inclination of the seat and the fixation of the trunk. In addition, the conditions are the same for the shift of the buttocks. With Belt-HHD, the lower leg of the participant and the lower leg of the examiner were fixed by a belt. It was predicted that fixation of the lower leg, inclination of the lower leg (often inclined forward), and swelling or resilience of the sural region may affect fixation of the HHD sensor. Reconsideration of the fixing method with the belt is necessary for knee flexion. As a result, the value by Belt-HHD may further approximate the value by Mod-IKD. This will increase the agreement between the values of Belt-HHD and CONV-IKD. The present study is novel in that Conv-IKD and agreement between measured values of Belt-HHD are examined including factors of the difference. There is also novelty in that Mod-IKD is adopted as the measurement method.
From these facts, in the isometric knee muscle strength measurement using Belt-HHD for healthy young subjects, there is a problem in the agreement of the measurement values using Belt-HHD and Conv-IKD. In order to determine the value agreement, in knee extension, it is necessary to consider modification of the fixation method of the trunk, pelvis and thigh, modification of the application of the sensor pad, and modification of the sensor pad itself. In knee flexion, it is necessary to consider modification of the measurement method, including the method of fixing the belt.
If the agreement between the isometric knee flexion using Belt-HHD and the measured value of extension muscle strength and the value by Conv-IKD is improved, it is considered that the compatibility of the measured values is enhanced and it becomes a more useful index.
Conflict of interest
There is no conflict of interest in this research.
REFERENCES
- 1.Katoh M, Yamasaki H: Comparison of reliability of isometric leg muscle strength measurements made using a hand-held dynamometer with and without a restraining belt. J Phys Ther Sci, 2009, 21: 37–42. [Google Scholar]
- 2.Katoh M, Hiiragi Y, Uchida M: Validity of isometric muscle strength measurements of the lower limbs using a hand-held dynamometer and belt: a comparison with an isokinetic dynamometer. J Phys Ther Sci, 2011, 23: 553–557. [Google Scholar]
- 3.Bohannon RW: Hand-held compared with isokinetic dynamometry for measurement of static knee extension torque (parallel reliability of dynamometers). Clin Phys Physiol Meas, 1990, 11: 217–222. [DOI] [PubMed] [Google Scholar]
- 4.Gagnon D, Nadeau S, Gravel D, et al. : Reliability and validity of static knee strength measurements obtained with a chair-fixed dynamometer in subjects with hip or knee arthroplasty. Arch Phys Med Rehabil, 2005, 86: 1998–2008. [DOI] [PubMed] [Google Scholar]
- 5.Deones VL, Wiley SC, Worrell T: Assessment of quadriceps muscle performance by a hand-held dynamometer and an isokinetic dynamometer. 1994, 20: 296–301. [DOI] [PubMed] [Google Scholar]
- 6.Martin HJ, Yule V, Syddall HE, et al. : Is hand-held dynamometry useful for the measurement of quadriceps strength in older people? A comparison with the gold standard Bodex dynamometry. Gerontology, 2006, 52: 154–159. [DOI] [PubMed] [Google Scholar]
- 7.Trudelle-Jackson E, Jackson AW, Frankowski CM, et al. : Interdevice reliability and validity assessment of the Nicholas Hand-Held Dynamometer. J Orthop Sports Phys Ther, 1994, 20: 302–306. [DOI] [PubMed] [Google Scholar]
- 8.Sullivan SJ, Chesley A, Hebert G, et al.: The validity and reliability of hand-held dynamometry in assessing isometric external rotator performance. J Orthop Sports Phys Ther. 1998, 213–217. [DOI] [PubMed] [Google Scholar]
- 9.Reed RL, Den Hartog R, Yochum K, et al. : A comparison of hand-held isometric strength measurement with isokinetic muscle strength measurement in the elderly. J Am Geriatr Soc, 1993, 41: 53–56. [DOI] [PubMed] [Google Scholar]
- 10.Piao C, Yoshimoto N, Shitama H, et al. : Validity and reliability of the measurement of the quardriceps femoris muscle strength with a hand-held dynamometer on the affected side in hemiplegic patients. J UOEH, 2004, 26: 1–11. [DOI] [PubMed] [Google Scholar]
- 11.Hansen EM, McCartney CN, Sweeney RS, et al. : Hand-held dynamometer positioning impacts discomfort during quadriceps strength testing: a validity and reliability study. Int J Sports Phys Ther, 2015, 10: 62–68. [PMC free article] [PubMed] [Google Scholar]
- 12.Bohannon RW, Bubela DJ, Wang YC, et al. : Adequacy of belt-stabilized testing of knee extension strength. J Strength Cond Res, 2011, 25: 1963–1967. [DOI] [PMC free article] [PubMed] [Google Scholar]