

Abstract
Cutaneous metastases of genitourinary malignancies are an extremely rare phenomenon. Few cases of skin metastasis from urothelial carcinoma of the bladder have been reported. We report a case of 71-year-old female with primary bladder transitional cell carcinoma who presented with the initial presentation of cutaneous skin lesions that covered the entire lower abdominal wall.
Keywords: Bladder, Cancer, Skin, Metastasis, Cutaneous, Urothelial
Introduction
Cutaneous metastasis of bladder cancer is an unusual phenomenon with a handful of cases reported in literature. Bladder cancer normally metastasizes to regional lymph nodes, liver, lung, and bone. Overall incidence of documented skin metastasis is 2.9% of all cancer patients.1 We present the most extensive case of cutaneous metastasis of bladder urothelial carcinoma in a female who presented with no urinary symptoms.
Case report
A 71-year-old female presented with a 6-month history of left lower extremity edema and 1-month history of right lower extremity, suprapubic, and external genital edema. She denied any history of hematuria, flank pain, vaginal bleeding, constipation, fevers, chills, shortness of breath or unintended weight loss. Physical exam showed suprapubic edema extending to the umbilicus with a large erythematous indurated plaque (Fig. 1) and significant right inguinal lymphadenopathy. Abdominal/pelvic MRI showed 3 cm left lateral bladder-wall mass with concerns of serosal extension and significant retroperitoneal, iliac, and inguinal lymphadenopathy. CT scan (Fig. 2) was consistent with the MRI results with the additional finding of left adrenal mass. Patient underwent transurethral resection of the bladder tumor (TURBT) with incomplete resection and an inguinal LN and skin biopsy was taken from the left abdomen. Biopsy results came back positive for P63, P40, CK7, CK20, and uroplakin consistent with uroepithelial carcinoma of the bladder (Stage 4, T3N3M1) (Fig. 3).
Fig. 1.

Nodular and erythematous skin lesions on the lower abdominal wall.
Fig. 2.
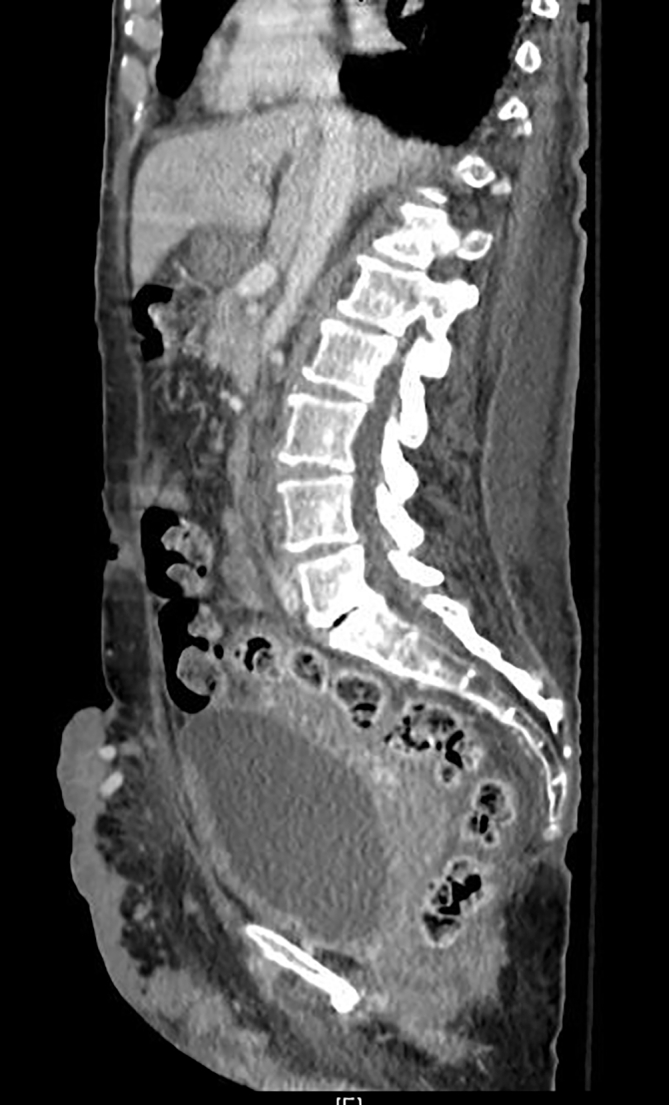
Initial CT findings confirming serosal extension of bladder-wall mass.
Fig. 3.

H&E 4x: Highlights the low-power infiltrating nature of the high-grade urothelial carcinoma into the muscularis layer.
Patient was started on palliative cisplatin 75mg/m2 D1 + gemcitabine 1000mg/m2 D1, 8, 15, q28 days. However, the patient could not continue her D15 gemcitabine due to cytopenia. A repeat CT scan showed interval size decrease in left-sided lymph nodes and adrenal mass. However, a new enhancing intraluminal lesion was found within the left ureter with moderate hydroureteronephrosis. Creatinine was stable at 1.1. Additional findings include interval size increasing soft tissue nodules along the perianal region, medial gluteal clefts, and the anterior lower pelvis with overlying nodular skin thickening. She was switched from chemotherapy to immunotherapy and started on Atezolizumab 1200mg IV q3 weeks. Despite this management, the patient expired within a week of treatment.
Discussion
Bladder cancer is the second most common malignancy of the genitourinary tract. It commonly metastasizes to regional lymph nodes, liver, lung, and bone. Rarely, bladder cancer can involve the skin due to direct tumor invasion, hematogenous or lymphatic spread, or seeding due to iatrogenic implantation.1 About 5.3% of all malignancies involve skin metastasis with 1.34% of those involving genitourinary tumors; bladder cancer accounts for 0.84%.2
The gross appearance of cutaneous lesions varies and non-distinctive. It may mimic other dermatologic disorders such as melanoma and sarcomas. Infiltrated plaques or nodularity have been commonly associated with cutaneous metastases of urological cancers.2 However, immunohistochemical is warranted for differential diagnosis. Coordinated expression of cytokeratins 7 and 20 are found to be positive for 89% of urothelial bladder cancers.3
The current treatment standard for metastatic bladder cancer is combination chemotherapy with gemcitabine and cisplatin. Some physicians employ the MVAC scheme (methotrexate, vinblastine, doxorubicin and cisplatin). Chemotherapy has reported remission rates to up to 70%, however, it is rarely curative.4 Local radiation therapy has been utilized for cutaneous lesions unresponsive to chemotherapy. Others may benefit from surgical intervention with resection of the tumor metastases in the setting of tumor-related symptoms.4 Recently, systemic immunotherapy is increasingly incorporated in the management of advanced bladder cancer refractory to chemotherapy.5 Five drugs have been approved by the FDA in the use of metastatic urothelial cancer, including Atezolizumab.5 Our patient received two cycles of chemotherapy and was switched to Atezolizumab due to the lack of significant response and cytopenia. This is the first case in literature to apply immunotherapy in the setting of cutaneous metastasis of urothelial bladder cancer.
Prognosis of metastatic bladder cancer is poor. Cutaneous metastasis from a primary urothelial carcinoma of the bladder is a sign of advanced disease with median survival less than 12 months.2,4 Poor outcomes can be attributed to the aggressive nature of the disease, limited treatment options, rarity of the disease process. Our patient's disease was beyond the scope of definitive treatment and expired within 9 months of diagnosis.
Conclusion
We presented a rare case of cutaneous metastasis of urothelial carcinoma of the bladder. Metastatic disease should always be in the differential in any patient who presents with cutaneous lesions. Skin biopsy should be performed for histochemical analysis to prevent misdiagnosis. Imaging is necessary to identify the primary tumor, additional metastatic sites, and staging.
Declaration of competing interest
None.
References
- 1.Mueller T.J., Wu H., Greeenberg R.E. Cutaneous metastases from genitourinary malignancies. Urology. 2004;63:1021–1026. doi: 10.1016/j.urology.2004.01.014. [DOI] [PubMed] [Google Scholar]
- 2.Block C.A., Dahmoush L., Konety B.R. Cutaneous metastases from transitional cell carcinoma of the bladder. Urology. 2006;67:846. doi: 10.1016/j.urology.2005.10.045. [DOI] [PubMed] [Google Scholar]
- 3.Wang N.P., Zee S., Zarbo R.J., Bacchi C.E., Gown A.M. Coordinate expression of cytokeratins 7 and 20 defines unique subsets of carcinomas. Appl immunohistochem. 1995;3:99–107. [Google Scholar]
- 4.Lees A.N. Cutaneous metastasis of transitional cell carcinoma of the urinary bladder eight years after the primary: a case report. J Med Case Rep. 2015;9:102. doi: 10.1186/s13256-015-0585-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dietrich B., Srinivas S. Urothelial carcinoma: the evolving landscape of immunotherapy for patients with advanced disease. Res Rep Urol. 2018;10:7–16. doi: 10.2147/RRU.S125635. [DOI] [PMC free article] [PubMed] [Google Scholar]