

Abstract
Background
To evaluate the feasibility and clinical outcomes of vaginoplasties using a neovaginal polylactic acid prosthesis made with 3-dimensional (3D) printing technology as an intraneovaginal mould.
Methods
This was an interventionist, prospective, and multicentre clinical pilot investigation of a sanitary product (PACIENA prosthesis®) aiming to recruit and operate on 8 patients over 6 months with a follow-up period of 6 months. Only six patients with Rokitansky syndrome and one patient with Morris syndrome (7 patients in total) were operated on in two university hospitals: “La Fe”, Valencia (H1) and “Arrixaca”, Murcia (H2). Interventions: Extensive surgical dissection of a defined space between the urethra and bladder in the front and of the rectum in the back as well as insertion of the PACIENA prosthesis® covered with Interceed® were performed. After 12 days, the prosthesis was changed to the silicone-covered version for daily application.
Results
In the 6 patients with Rokitansky syndrome (86%), the primary endpoint (satisfactory vaginal outcome in terms of appearance, function, and sensation without relevant additional morbidity) was achieved, although only 2 patients (28%) were sexually active at the end of 6 months of follow-up. The patient with Morris syndrome withdrew from the study after 1 month. Patients without bacterial colonization showed positive Schiller tests at 1 month, and subsequent biopsies showed adequate keratinization and epidermization. Epithelization and iodopositivity were delayed in the patients who developed inflammatory granulomas.
Conclusions
Good anatomical and functional results can be achieved with the PACIENA prosthesis® for vaginoplasties without skin grafts. However, adequate patient selection and education, good surgical techniques and haemostasis, postoperative support, and prevention of bacterial colonization are important.
Trial registration
This clinical study was approved by the Ethical Clinical Investigation Committee of San Juan University Hospital on September 27, 2016, to be conducted in the participating centres; it was authorized by the Spanish Agency of Medicines and Health Products (AEMPS) on April 24, 2017 (exp. no. 585/16/EC), to be carried out in that hospitals.
Keywords: Vaginal agenesis, Vaginoplasty, Neovaginal prosthesis, Rokitansky syndrome
Background
Historically, the creation of a neovagina using a split-thickness skin graft and an inert prosthesis or synthetic mould to support the newly formed cavity (McIndoe’s technique) has been the most commonly performed vaginoplasty technique [1–4]. However, many other surgical procedures with different access pathways have also been performed (i.e., laparoscopic, laparotomic, vaginal, or combined procedures [5, 6]). On the other hand, multiple types of tissue have been applied to cover the neovaginal cavity [7]. Good results have been achieved by simply covering the prosthesis with Interceed® [8], and other authors [9, 10] have also obtained good results without using skin grafts, with evidence of squamous epithelization of the neovaginal vault. Acién et al. [11–13] suggested that by using a prosthesis made of poly-lactic acid (PLA, a biodegradable polymer derived from lactic acid often used as a scaffold in tissue engineering and regenerative medicine [14, 15] and whose contribution to epithelization has been studied by different authors [16, 17]) and designed and manufactured with 3-dimensional (3D) printing technology as a vaginal mould, skin grafting could be avoided, and vaginoplasty would be simpler, with good anatomical and functional results. We do not know of any other neovaginal prostheses for humans with the design, printing and characteristics of our PLA prosthesis.
Study objective
This study aimed to evaluate the feasibility and clinical outcomes of vaginoplasty using a PLA prosthesis (PACIENA prosthesis®) as an intraneovaginal mould in patients with vaginal agenesis undergoing surgery following McIndoe’s technique without skin grafts.
Methods
This study was an interventionist, prospective, and multicentre clinical investigation of a sanitary product (PACIENA prosthesis®) that aimed at recruiting and operating on 8 patients over 6 months with a follow-up period of an additional 6 months (Canadian Task Force Classification II-2). This pilot study was approved by the Ethical Clinical Investigation Committee of San Juan University Hospital on September 27, 2016, and was authorized by the Spanish Agency for Medicines and Health Products on April 24, 2017 (exp. no. 585/16/EC), for 9 participating hospitals (8 in the Community of Valencia and 1 in Murcia).
The PACIENA prosthesis® has been introduced as a new prototype of neovaginal prosthesis adapted to the vagina of normal women and has been patented (utility model U201630650, international pub. WO/2017/203076) [11–13]. The basic and novel features of this new prototype of prosthesis for neovaginas were described in [12]. This prosthesis is 130 mm long, and the diameter shows a progressive decrease from a maximum value of 38 mm up to 20 mm at the lower end to be located in the introitus; there is a recess in the lower front part, which is provided for urethral protection. The prosthesis is hollow to minimize weight and to ensure drainage through holes at both ends. A removable plate is also provided to be attached at the lower end, with holes to allow for the fixing of fastening tapes or belts. The prosthesis is made of PLA, a biocompatible material often used as a scaffold in tissue engineering and regenerative medicine applications, whose properties related to epithelial regeneration in different applications have been reported in the literature [14–17]; the use of PLA also allows customized design and manufacturing with 3-dimensional (3D) printing technology. A prosthesis that is the same shape but is covered with silicone with a smoother surface was prepared as a maintenance device (see Fig. 1).
Fig. 1.
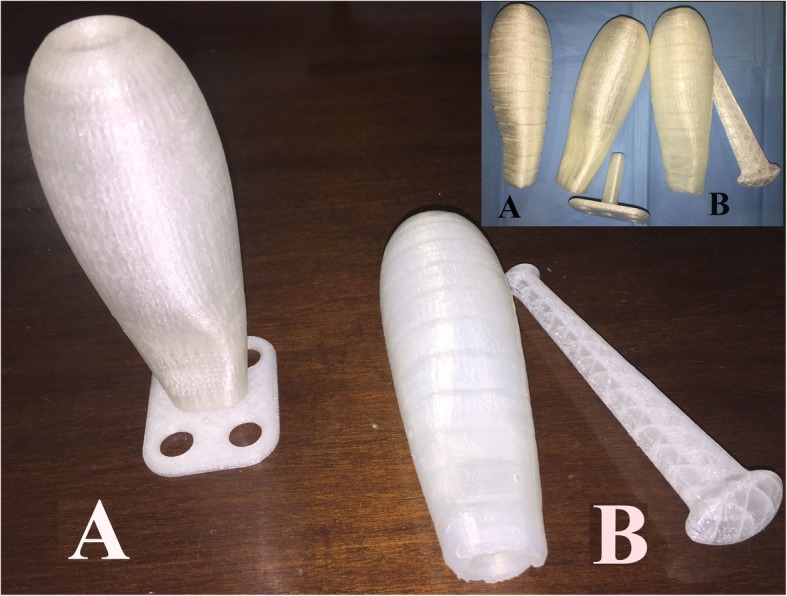
PACIENA prosthesis®. a Surgical prosthesis. b Coated silicone version of the prosthesis (the marks on the prosthesis correspond to 1 cm in length)
Inclusion criteria
1) vaginal agenesis due to MRKH (or Rokitansky) syndrome or CAIS (Morris syndrome) in women who were willing to undergo surgery for neovagina creation (McIndoe’s technique without skin grafts) after rejection or failure of previous self-dilation attempts, 2) adult age or parental authorization for younger patients, and 3) provision of written informed consent.
Exclusion criteria
1) presence of medical illness (metabolopathy, cardiovascular, coagulation, breathing difficulties, intestinal disease) that prohibits surgery or compromises the surgical results, 2) lack of parental authorization in younger patients, and 3) a previous neovaginal surgery attempt.
Research plan and procedures
The patients were evaluated before surgery: karyotype analysis, hormonal profile test, abdominal or transrectal ultrasound and eventually computed tomography or magnetic resonance imaging, complete physical examination, and gynaecological and mammary assessments. The diagnosis of vaginal agenesis due to Rokitansky syndrome or Morris syndrome was confirmed before surgery. The procedure consisted of the use of a prosthesis (stent or mould) that was temporarily introduced into the defined space between the bladder and the rectum of women with vaginal agenesis through the surgical intervention known as McIndoe’s technique in order to create an artificial vaginal cavity or neovagina with a suitable luminal diameter. Antibiotic cream (betametasone and gentamicin) was applied on the introduced prosthesis, and the prosthesis was covered with Interceed® mesh (an oxidized regenerated cellulose-absorbable adhesion barrier). After placing the prosthesis in the appropriate position (recess in front, suburethral), urinary flow (Foley® urethral catheter), vital signs, and blood loss were assessed, and finally, the prosthesis was fixed in place using fastening tapes or a belt. The bladder catheter was removed after 2 days, spontaneous micturition was assessed, and the patient was eventually discharged from the hospital. Then, 10–12 days later, the prosthesis was removed and replaced with the silicone-covered version. The second device was self-placed and worn daily during 6 months of follow-up and until repeated sexual intercourse occurred for a decreasing number of hours (from 20 h/day at the beginning to 6–8 h/night after 4 months).
Outcomes
A) Primary endpoint: to achieve the formation of a satisfactory vagina in terms of appearance, function, and sensation without relevant additional morbidity. B) Secondary endpoints: 1) surgical duration, bleeding, and complications; 2) hospitalization period; 3) neovaginal length, culture, and epithelization (Schiller test and biopsy); and 4) time lapse of and satisfaction with sexual intercourse (Rosen’s Female Sexual Function Index [FSFI] [18]).
Safety and adverse effects
Adverse effects were defined as the presence of A) stenosis due to neovaginal wall retraction, B) neovaginal fundus granulomas, C) recto-vaginal or bladder-urethra-vaginal fistulae, and D) necrosis due to compression of the urethral wall. In this study, patients with a positive vaginal culture for Pseudomonas aeruginosa were also included and analysed, although there were no signs of clinical infection, and additional cultures were performed after the clinical study on used and unused prostheses.
Statistical analysis
Sample size: Due to the low incidence of this pathology, we intended to conduct a pilot study recruiting 8 patients, with an inclusion period from May to November 2017 and a follow-up period of an additional 6 months; however, only 7 patients were recruited within the authorized period. Statistical study: All data were introduced and analysed using SPSS version 25.0 (IBM, Madrid, Spain). As the number of cases was low, the main qualitative and quantitative variables were directly included in the tables, although several data are also expressed as percentages, means ± standard deviations (SDs), and 95% confidence intervals (CIs), if applicable.
Results
Seven patients with vaginal agenesis were ultimately included during the recruitment period between May and November 2017. Of these patients, 6 had been diagnosed with MRKH (or Rokitansky) syndrome, and 1 patient was confirmed to have Morris syndrome. The hormonal profile of the 6 MRKH cases was as follows: FSH, 5.6 ± 2.8 mUI/mL; LH, 11.6 ± 14.4 mUI/mL; oestradiol, 73.4 ± 33.5 pg/mL; TSH, 2.3 ± 1.2 μUI/mL; PRL, 25 ± 13.3 ng/mL; and testosterone, 0.4 ± 0.23 ng/mL.
The age, diagnostic profile, and clinical characteristics of the patients are shown in Table 1. Patients c3 and c4 were operated on at the University Hospital “Virgen de la Arrixaca” (H2) in Murcia, whereas the other 5 patients were operated on at the University and Polyclinic Hospital “La Fe” (H1) in Valencia. All patients were examined, operated on, and evaluated following the protocol (with some variations as decided by the researcher in the intervention hospital); however, patient c6 with Morris syndrome and previous psychological instability refused the use of the silicone-covered maintenance device and refused to participate in the study in the second month. In the 6 patients with Rokitansky syndrome (86%), the primary endpoint was achieved, although only 2 of them (28%) had repeated and satisfactory sexual relations during the period of study. The other 4 did not have a sexual partner at that time. The mean age was 21 ± 3.3 (95% CI 17.9–24.1) years but varied between 19.2 ± 1.4 years (H1) and 25.5 ± 0.7 years (H2).
Table 1.
Patient profiles
| Case | Hospital | Age (range) | Diagnosis | Other anomalies | Karyotype | Urological anomalies | Uterus/ovaries | Weight (kg) | Height (cm) | BMI (kg/m2) |
|---|---|---|---|---|---|---|---|---|---|---|
| C1 | H1 | < 18 | MRKH syndrome | Umbilical hernia | – | No | Absent/both normal | 50 | 157 | 20 |
| C2 | H1 | (18–21) | MRKH syndrome | – | 46XX | No | Absent/both normal | 51 | 165 | 18.2 |
| C3 | H2 | (22–25) | MRKH syndrome | Scoliosis (op), hypoplasia MR | 46XX | No | Rudimentary/both normal | 51 | 160 | 19.9 |
| C4 | H2 | (> 25) | MRKH syndrome | Congenital anomalies, “cat eye syndrome” |
47XX + mar [18], partial trisomy 22q11.2 in mosaic |
Reflux VU (op), normal kidneys | Absent/both normal | 60.1 | 161 | 23.2 |
| C5 | H1 | (18–21) | MRKH syndrome | Renal hypoplasia | 46XX | Right renal hypoplasia, previous left nephrectomy and kidney transplant | Absent/both normal | 63.3 | 154 | 26.8 |
| C6 | H1 | (18–21) | Morris syndrome | Gonadectomy in childhood, Tietze syndrome | 46XY | No | Absent/both absent | 74 | 171 | 25 |
| C7 | H1 | (18–21) | MRKH syndrome | Scoliosis, low back pain | 46XX | No | Absent/both normal | 58.2 | 155 | 24.3 |
H1 University and Polyclinic Hospital “La Fe” in Valencia, H2 University Hospital “Virgen de la Arrixaca” in Murcia; MRKH Mayer-Rokitansky-Kuster-Hauser; BMI body mass index, Op operation, MR magnetic resonance, VU vesico-ureteral
The surgery duration, complications, number of hospitalization days, Schiller test results, neovaginal length, culture results, and eventual sexual intercourse results are presented in Table 2. The duration of the intervention in the 7 patients was 49.3 ± 6.1 (95% CI 43.7–54.9) min (51 ± 5 min in H1 and 45 ± 7 min in H2). The length of hospital admission (7.4 ± 6.6 days, 95% CI 1.3–13.5 days) varied depending on the hospital (9.6 ± 6.7 days in H1 versus only 2 ± 0 days in H2). The mean neovaginal length at 1 and 4 months was 9 ± 1.4 (95% CI 7.6–10.2) cm and 8.7 ± 1.6 (95% CI 7–10.4) cm, respectively, remaining similar at the 6-month follow-up (8.5 ± 0.8 CI 7.6–9.4). Figure 2 shows some images of the sequence of observations in the studied cases. However, it is remarkable that the evolution and results differed between the 2 hospitals where the patients attended, as follows:
Table 2.
Post-surgical follow-up
| Case | Hospital | Date of surgery | Duration (min) | Complications | Length of admission (days) | Change of prosthesis and culture | Evaluationat 1 month | Evaluation at 3–4 months | Evaluation at 6 months | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sc T | Vl (cm) | Cu | Sc T | Vl (cm) | Cu | Ic | Sc T | Vl (cm) | Cu | Ic | |||||||
| C1 | H1 | June- 2017 | 50 | Postoperative discomfort, epidural analgesia | 5 | D12, smaller prosthesis, PA | – | 9 | PA | At 3 months: areas (+), granulomas | 9 | At 3 months: PA | No | (+) | 8 | – | Yes, FSFI = 31,8 |
| C2 | H1 | June-2017 | 50 | Bleeding, pelvic haematoma | 14 | D12, haematoma in resolution, smaller prosthesis | – | 8 | PA | At 3 months: weak iodine areas, granulomas | 11 | PA, granulomas | No | (+/−), Granulomas | 8 | PA | No |
| C3 | H2 | October-2017 | 40 | No | 2 | D12 | (+) | 10 | (−) | (+) | 8 | (−) | No | (+) | 8 | – | No |
| C4 | H2 | October-2017 | 50 | No | 2 | D12 | (+) | 11 | (−) | (+) | 10 | (−) | Yes, repeated and satisfactory | (+) | 10 | – | Yes, FSFI = 32,1 |
| C5 | H1 | Nov-2017 | 60 | Moderate blood loss | 3 | D12, smaller prosthesis (25 mm) | – | 9 | PA | (+) Iodine areas, polyp | 8.5 | PA, biopsy: inflammatory granulation tissue | No | (+) | 8 | – | No |
| C6 | H1 | Nov-2017 | 45 | Postoperative denial | 19 | D12, smaller prosthesis 25 mm | Left the study, no prosthesis | 6,5 | Escherichia coli | – | – | – | – | – | – | – | – |
| C7 | H1 | Nov-2017 | 50 | No | 7 | D12, smaller prosthesis (25 mm) | – | 9 | – | (+) iodine areas, exeresis of granulomas | 9 | PA | No | (+), Granulomas | 9 | – | No |
Sc T Schiller test, Vl neovaginal length, Cu vaginal cultures, Ic intercourse, D day; PA Pseudomonas aeruginosa, FSFI Female Sexual Function Index
Fig. 2.
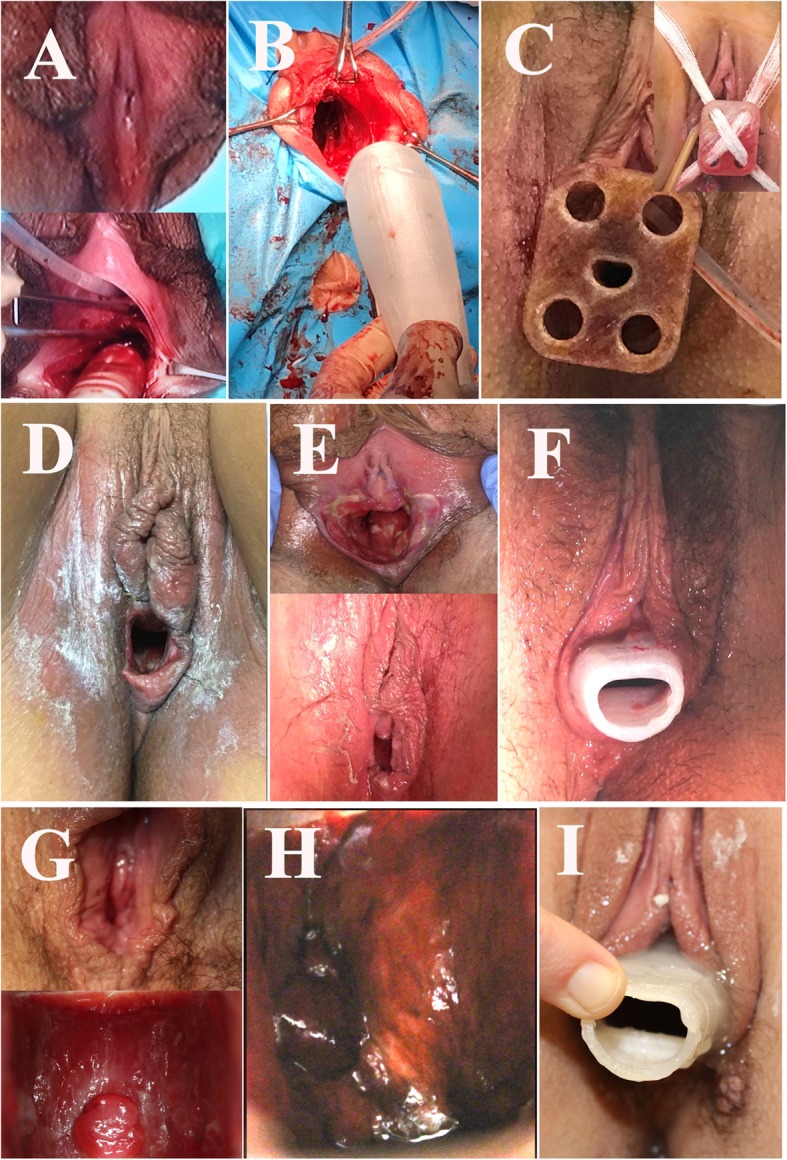
Images of the sequence of observations in the studied cases. a Before and at the start of the operation in c5. b Introduction of the Interceed®-covered prosthesis in c2. c Prosthesis introduced in c3 with the adapted fixation plate and cross bandages for prosthesis support. d. After extracting the surgical prosthesis at 12 days in c7. e State and extraction of the surgical prosthesis at 12 days in c5. f With the silicone prosthesis after the change at 12 days in c1. g State and Schiller’s test at 3.5 months in c3. h Schiller’s test at 3.5 months in c4. i With the silicone prosthesis at 3.5 months in c3
- Patients c1 and c2 were operated on in H1. In patient c1, due to postoperative discomfort, epidural anaesthesia was maintained, and the patient remained hospitalized until the 5th day. In patient c2, slight bleeding occurred during surgery, and postoperatively, the patient developed a pelvic haematoma and remained hospitalized for 14 days. Both patients experienced difficulties with the introduction of the silicone-covered maintenance prosthesis upon the first attempt; thus, they were given a thinner model that was later changed to the standard-sized version. In both patients, the cultures were repeatedly positive for P. aeruginosa. At 2 and 3 months, patched areas were observed in the Schiller test, and fundal granulomas were detected. The requirement of daily prosthesis replacement was not completely fulfilled, but at 6 months, the Schiller test was positive in both patients, and patient c1 maintained repeated and satisfactory sexual intercourse, with FSFI = 31.8 (max 36, normal mean values 27.5 ± 5.6 in [18]).
- Patients c3 and c4 attended and were operated on in H2, and they were discharged from the hospital on the 2nd day. One month after surgery, both neovaginas had a good appearance, the cultures were negative, and the Schiller test was completely positive. Patient c4 began regular sexual intercourse during the 4th month with mild dyspareunia but with a good FSFI at 6 months (32.1/36). Vaginal biopsies showed adequate keratinization and epidermization in both patients (see Fig. 3).
Fig. 3.
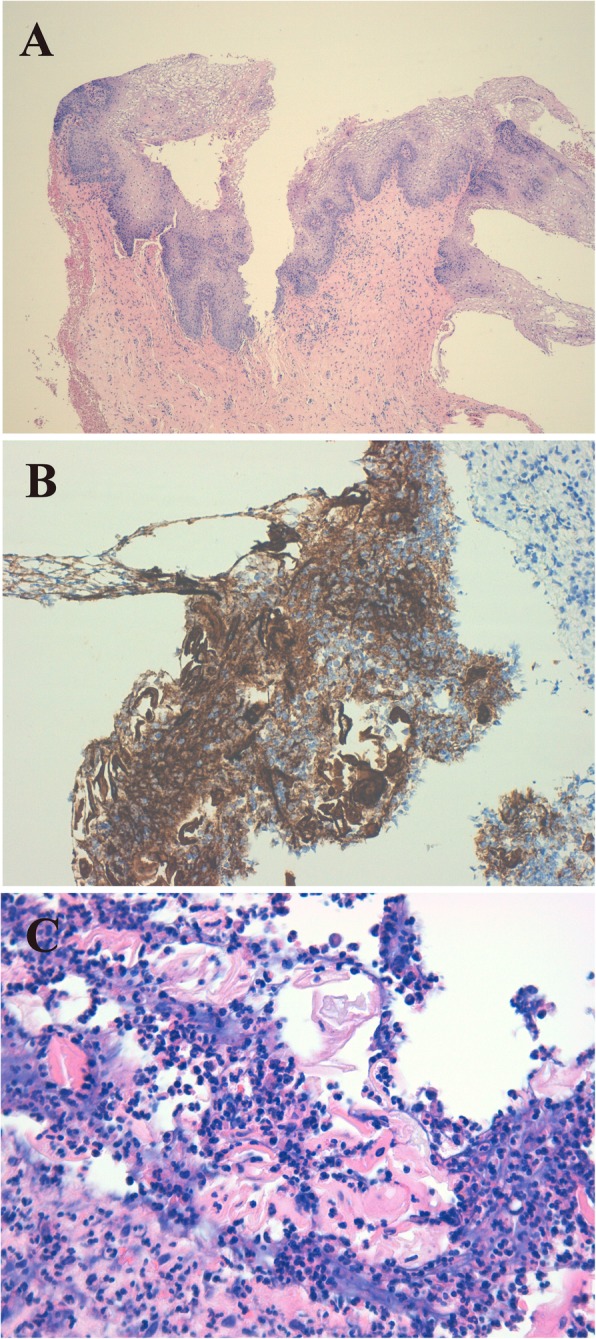
Vaginal biopsy at 6 months. a Well-structured, mature squamous epithelium (haematoxylin-eosin [H-E], × 40) in c4. b Intense staining for cytokeratin AE1-AE3 (CKAE1-AE3) on the surface of the fragment, which helps in recognizing the epithelium at that level and with greater magnification to see the epithelial positivity to cytokeratins (CKAE1-AE3, × 200). c Among abundant inflammatory polymorphic cells, the presence of keratin sheets (dyed more homogeneous pink) can be estimated. With greater magnification, the keratin sheets are more evident (H-E, × 400)
- Patients c5, c6, and c7 were operated on in H1. Patient c5 had moderate blood loss during the intervention but was discharged after 3 days, whereas patient c6 adopted a negative attitude postoperatively and remained hospitalized for 19 days. All patients had difficulties with the introduction of the silicone-covered maintenance prosthesis upon the first attempt; thus, they were given a thinner model that was later changed to the standard-sized version. However, the requirement of daily prosthesis replacement was not completely fulfilled. In patients c5 and c7, the cultures were positive for P. aeruginosa, the Schiller test showed patched areas, and fundal granulomas were present requiring subsequent exeresis. Patient c6 dropped out of the study. None of these patients had sexual intercourse during the 6-month follow-up period.
The results of the aerobic cultures taken from the prostheses, as an additional post-clinical study evaluation, are presented in Table 3. Cultures of both unused PACIENA prosthesis® versions showed growth of standard skin flora bacteria (coagulase-negative Staphylococcus). In the prosthesis culture of patient c4, after use, enteral flora were detected. However, the cultures of both used prostheses from patients c2 and c7 presented abundant P. aeruginosa that continued to be detected after liquid sterilization methods.
Table 3.
Additional post-clinical study microbiological studies
| Studied prosthesis | Results of aerobic culture | Repeated cultivation after Instrunet© 30 min |
|---|---|---|
| Unused surgical prosthesis | Habitual flora of the skin (St.c.n) | – |
| Unused silicone prosthesis | Habitual flora of the skin (St.c.n) | – |
| Silicone prosthesis used in c4 (H2) | Enteric flora, no P. aeruginosa | – |
| Silicone prosthesis used in c2 (H1) | P. aeruginosa | P. aeruginosa |
| Silicone prosthesis used in c7 (H1) | P. aeruginosa | P. aeruginosa |
P. Pseudomonas, St.c.n coagulase-negative Staphylococcus
Discussion
Our study shows that neovaginal formation and epidermization with the performance of vaginoplasty following McIndoe’s technique without the use of skin grafts and with the use of a PLA prosthesis, covered with Interceed®, as an intraneovaginal mould can be achieved with good anatomic and functional results, especially if other adverse effects (such as hospital bacterial colonization) can be alleviated. In this sense, the use of the PACIENA prosthesis® has not been associated with any complications.
The great simplicity of the operation owing to the avoidance of skin grafting and related surgery, the shortened hospital stay and the good anatomical and functional results in patients who adequately maintain the use of the silicone-covered prosthesis suggest that our vaginoplasty method using the PACIENA prosthesis may be recommended for neovaginal creation in patients with vaginal agenesis.
The well-established techniques used for vaginoplasty include grafting with split-thickness skin [1–4], peritoneum [19], bowel, free jejunal autograft, ileum [20], or sigmoid colon [21]. The Vecchietti technique has been used as a less-invasive approach to surgical vaginoplasty or as modified technique of Brucker, Rall, and Wallwiener [5, 6] using vagino-abdominal blunt perforation without vesicorectal tunnelling. Other less-invasive methods have been proposed, including Creatsas vaginoplasty (modified Williams method) [22], the labial and vestibular flap method [23], and the use of a small graft of perineal skin at the introitus to line the distal posterior aspect of the newly created vagina [24, 25]. In gender reassignment surgery, the most commonly used method is penile inversion vaginoplasty with scrotal flaps [26], sometimes combined with autologous buccal micro-mucosa free grafts [27]. However, several techniques have been attempted to cover (and epithelize) the newly formed vagina. Dhall [28] used a human amnion graft, whereas Zhang et al. [7] and Zhu et al. [29] used a biological mesh (tissue-engineered biomaterial graft). Other authors have used Interceed® [8], or the placement of this mesh between the stent and a skin graft (meshed) and thus reducing the size of the graft, while maintaining good results related to neovaginal epithelization [30].
Nevertheless, all these techniques involve dissecting the vesicorectal space and inserting a stent into the neovagina to help the adherence of the graft or to maintain patency. For such purposes, some authors have proposed the use of a silicone mould of different dimensions or even a customized mould [31, 32]. Other authors used stents of different materials (foam rubber, wood, plastic, glass, Teflon, Dexon, vacuum expandable condom, a simple syringe or a polyethylene bag [7, 30, 33–36]), many of which are not anatomically designed. These stents are usually hand-made, using weighty and strong materials, and can produce bedsores on the recto-vaginal septum or necrosis on the urethra and hypospadias. Therefore, the stent or neovaginal mould might be important for achieving good anatomical and functional results.
The shape and dimensions of the PACIENA prosthesis® are adapted to the normal vagina, and it is made of PLA, which is a biocompatible material used in several biomedical applications and whose effect on tissue growth has been reported in different scenarios [14–17, 37–39]. For example, Sharma et al. [17] developed a skin substrate made of PLA scaffold with minced skin grafts; skin cells were shown to migrate along the fibres of the scaffold, new collagen was formed, and epithelial and stromal cells were confirmed by immunohistochemistry and scanning electron microscopy [17].
In our pilot study, we used an Interceed® mesh to cover the PLA prosthesis as a barrier to prevent the adhesion of the newly created neovaginal tissue to the prosthesis and that has to be removed after several days. As a result, it might have been the combination of the geometry of the prosthesis, the anatomical design, the manufacturing of the PLA, and the Interceed® covering that has led to satisfactory results avoiding the need for skin grafts. In addition, the design and shape of the prosthesis (wider in the fundus with a decreasing diameter at the bottom end) allow self-support by the perineal muscles without needing to use other fastening aids or suturing of the labia.
Therefore, if a prosthesis has the adequate dimensions and the basic and novel features of the PACIENA prosthesis®, then good anatomical and functional results and adequate epidermization can be expected, similar to what occurs in normal vaginal embryology from the urogenital sinus [40], which in an adult woman is the vaginal introitus.
Clinical relevance
The following aspects suggest that this technique could be the most suitable method for vaginoplasty in the congenital absence of a vagina and in other situations, including gender reassignment surgery, ablation, or surgery for an acquired pathology (synechiae): a simple technique requiring only the dissection and opening of the vesicorectal space, making the procedure minimally invasive; the absence of complications related to skin grafting or to the use of a hard and heavy prosthesis; and the anatomical design of the PLA prosthesis using 3D technology, with a material composition that favours tissue growth.
Study limitations and unexpected findings
This pilot study was designed and authorized to recruit 8 patients for evaluation over 6 months (with an additional 6 months of follow-up); however, only 7 patients could be included. Only 6 patients (all with Rokitansky syndrome) completed the 6-month use of the prosthesis and the follow-up. All patients treated in H1 were positive for P. aeruginosa, which could have induced inflammation and granulomas as well as worsened the results. Some influence of age, psychological preparation before surgery, or surgical technique might also be present.
Conclusions
Good anatomical and likely good functional results can be achieved with the PACIENA prosthesis® for neovaginal creation (vaginoplasty) following a modification of McIndoe’s technique to avoid skin grafting. However, a good surgical technique and haemostasis, postoperative support, and the prevention of bacterial colonization are also important. Moreover, adequate patient selection with appropriate education, prosthesis self-replacement recommendations, and psychological support before and after surgery also seem fundamental.
Acknowledgements
To all hospitals and researches of the same participants in the project: HOSPITAL CLINICO UNIVERSITARIO DE VALENCIA (Prof. Antonio Cano Sánchez, Dr. Víctor Martín González, Dr. Lorenzo Abad de Velasco); HOSPITAL UNIVERSIATRIO DE SAN JUAN (Prof. Fco. Quereda Seguí, Dra. Maribel Acién Sánchez); HOSPITAL GENERAL UNIVERSITARIO DE ALICANTE (Dr. Juan Carlos Martínez Escoriza, Dr. José Antonio López Fernandez, Dra. Asunción Quijada Cazorla); HOSPITAL UNIVERSITARIO VIRGEN DE LA ARRIXACA DE MURCIA (Dra. Marisa Sánchez Ferrer, Prof. Anibal Nieto, Dr. F. Machado); INSTITUTO DE GINECOLOGÍA “PROF P. ACIÉN ALVAREZ S.L.” (Dra. Maribel Acién Sánchez, Prof. Pedro Acién Alvarez); HOSPITAL UNIVERSITARIO LA FE DE VALENCIA (Dr. Francisco J. Nohales Alfonso); HOSPITALES UNIVERSITARIOS DE TORREVIEJA Y VINALOPÓ DE ELCHE (Dr. Eduardo Cazorla Amorós); HOSPITAL GENERAL UNIVERSITARIO DE CASTELLON (Dr. Antoni Llueca Abella).
To the researches of the Department of Mechanical Engineering and Energy, Miguel Hernández University, Campus of Elche that manufactured and supplied the prostheses: Prof. Miguel Sánchez-Lozano, Prof. Miguel-Angel Oliva-Meyer, Javier Martínez-Garcia and Clara Gómez Jerez.
To Dr. M.A. Torroba-Caron (Anatomía Patológica, HUVA, Murcia) for the histopathological studies and microphotographies of the cases c3 and c4.
To Dr. V. Ortiz de la Tabla (Microbiología, San Juan University Hospital, Alicante) for the microbiological cultures analysed postrial.
To FISABIO (Estíbaliz López) and OTRI-UMH (Begoña García Jaén).
Abbreviations
- 3D
3-dimensional printing technology
- CAIS
Complete androgenic insensibility syndrome (or Morris syndrome)
- FSFI
Female Sexual Function Index
- H1
University and Polyclinic Hospital “La Fe” in Valencia
- H2
University Hospital “Virgen de la Arrixaca” in Murcia
- MRKH
Mayer-Rokitansky-Kuster-Hauser (or Rokitansky) syndrome
- PLA
Poly-Lactic Acid
Authors’ contributions
PA was the Promoter of the “PACIENA” study, designed the study, coordinated the clinical research with the sanitary product, and wrote and reviewed the manuscript. FN recruited patients from the University Hospital and Polyclinic “La Fe” of Valencia, performed the surgery and follow-up of patients, and reviewed the manuscript. MLSF recruited patients from the University Hospital “Virgen de la Arrixaca” in Murcia, performed the surgery and follow-up of patients, and reviewed the manuscript. MSL directed the manufacture and supply of the sanitary product (PACIENA prosthesis®) and reviewed the manuscript. VNL participated in the revision of the cases and in the introduction of data in SPSS, helped with the bibliographic search, and reviewed the manuscript. MA was the Monitor of the clinical study “PACIENA,” participated in the revision of the cases, helped with the bibliographic search, and wrote and reviewed the manuscript. PA had full access to all study data and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Authors’ information
Not applicable.
Funding
“Ayuda a la trasferencia tecnológica 2017, UMH”; and “Ayuda para el desarrollo de proyectos de innovación y transferencia tecnológica, convocatoria 2018, FISABIO”. Role of the funding source: “The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report”.
Availability of data and materials
PA had full access to all study data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Statement of prior presentation or publications and/or abstract/poster presentation: No prior presentation, including the cases reported. Yes on prosthesis, References 11–13.
Ethics approval and consent to participate
Institutional review board approval: This clinical study was approved by the Ethical Clinical Investigation Committee of San Juan University Hospital on September 27, 2016 to be conducted in the participating centers; and it was authorized by the Spanish Agency of Medicines and Health Products (AEMPS) on April 24, 2017 (exp. no. 585/16/EC), to be carried out in the following hospitals: Hospital Clínico de Valencia, Hospital Universitario “La Fe” (Valencia), Hospital General Universitario de Castellón, Hospital Universitario de San Juan (San Juan de Alicante), Hospital General Universitario (Alicante), Instituto de Ginecología “Prof P Acién Álvarez”, Hospital Universitario de Torrevieja (Alicante), Hospital Universitario del Vinalopó (Elche), and Hospital Universitario “Virgen de la Arrixaca” (Murcia).
All participating patients (or their parent) signed the informed consent to participate in the study.
Consent for publication
All participating patients (or their parent) signed the informed consent to participate in the study as well as their data and images (without personal identification) being used for diagnostic and scientific publication purposes.
Competing interests
The authors declare that they have no competing financial interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Pedro Acién, Email: acien@umh.es.
Francisco J. Nohales-Alfonso, Email: fnohalesa@gmail.com
Maria-Luisa Sánchez-Ferrer, Email: marisasanchez@um.es.
Miguel Sánchez-Lozano, Email: msanchez@umh.es.
Victoria Navarro-Lillo, Email: victoria.nl@coma.es.
Maribel Acién, Email: macien@umh.es.
References
- 1.McIndoe A. The treatment of congenital absence and obliterative conditions of the vagina. Br J Plast Surg. 1950;2:254–267. [PubMed] [Google Scholar]
- 2.Garcia J, Jones HW. The split thickness graft technic for vaginal agenesis. Obstet Gynecol. 1977;49:328–332. [PubMed] [Google Scholar]
- 3.Klingele CJ, Gebhart JB, Croak AJ, DiMarco CS, Lesnick TG, Lee RA. McIndoe procedure for vaginal agenesis: long-term outcome and effect on quality of life. Am J Obstet Gynecol. 2003;189:1569–1573. doi: 10.1016/S0002-9378(03)00938-4. [DOI] [PubMed] [Google Scholar]
- 4.Karapinar OS, Özkan M, Okyay AG, Şahin H, Dolapçıoğlu KS. Evaluation of vaginal agenesis treated with the modified McIndoe technique: a retrospective study. J Turk Ger Gynecol Assoc. 2016;17:101–105. doi: 10.5152/jtgga.2016.16013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brucker SY, Gegusch M, Zubke W, Rall K, Gauwerky JF, Wallwiener D. Neovagina creation in vaginal agenesis: development of a new laparoscopic Vecchietti-based procedure and optimized instruments in a prospective comparative interventional study in 101 patients. Fertil Steril. 2008;90:1940–1952. doi: 10.1016/j.fertnstert.2007.08.070. [DOI] [PubMed] [Google Scholar]
- 6.Rall K, Schickner MC, Barresi G, Schönfisch B, Wallwiener M, Wallwiener CW, Wallwiener D, Brucker SY. Laparoscopically assisted neovaginoplasty in vaginal agenesis: a long-term outcome study in 240 patients. J Pediatr Adolesc Gynecol. 2014;27:379–385. doi: 10.1016/j.jpag.2014.02.002. [DOI] [PubMed] [Google Scholar]
- 7.Zhang X, Liu Z, Yang Y, Yao Y, Tao Y. The clinical outcomes of vaginoplasty using tissue-engineered biomaterial mesh in patients with Mayer-Rokitansky-Küster-Hauser syndrome. Int J Surg. 2017;44:9–14. doi: 10.1016/j.ijsu.2017.06.026. [DOI] [PubMed] [Google Scholar]
- 8.Inagaki M, Motoyama S, Laoag-Fernandez JB, Yasuda R, Maruo T. Two cases reports of less invasive surgery using Interceed (oxidized regenerated cellulose) absorbable adhesion barrier for vaginoplasty in Mayer-Rokitansky-Kuster-Hauser syndrome. Int Surg. 2009;94:48–53. [PubMed] [Google Scholar]
- 9.Marzieh G, Soodabeh D, Narges I, Saghar SS, Sara E. Vaginal reconstruction using no grafts with evidence of squamous epithelialization in neovaginal vault: a simple approach. J Obstet Gynaecol Res. 2011;37:195–201. doi: 10.1111/j.1447-0756.2010.01335.x. [DOI] [PubMed] [Google Scholar]
- 10.Pulman KJ, Kives S, Jamieson MA. A case of vaginoplasty without grafting. J Pediatr Adolesc Gynecol. 2012;25:e17–e19. doi: 10.1016/j.jpag.2011.10.003. [DOI] [PubMed] [Google Scholar]
- 11.Acien P. On a New Neovaginal Prosthesis of PLA (Polylactic Acid). Am J Pharm Pharmacoth. 2016;3:16-9.
- 12.Acien P, Acién M, Oliva-Meyer MA, Sánchez-Lozano M, Martínez-Garcia J. McIndoe operation without skin graft: a new neovaginal prosthesis of Polylactic Acid (PLA) Brit J Med Med Res. 2016;18:1–7. doi: 10.9734/BJMMR/2016/29512. [DOI] [Google Scholar]
- 13.Acién P, Sánchez-Lozano M, Oliva MA, Acién MI, Martínez-Garcia J. A new model of prosthesis designed as mold to perform neovagina in patients with vaginal agenesis. Poland: Varsav; 2016. [Google Scholar]
- 14.Hart DR, Fabi SG, White WM, Fitzgerald R, Goldman MP. Current concepts in the use of PLLA: Clinical synergy noted with combined use of microfocused ultrasound and poly-l-lactic acid on the face, neck, and décolletage. Plast Reconstr Surg. 2015;136(5 suppl):180–17s. doi: 10.1097/PRS.0000000000001833. [DOI] [PubMed] [Google Scholar]
- 15.Farah S, Anderson DG, Langer R. Physical and mechanical properties of PLA, and their functions in widespread applications. A comprehensive review. Adv Drug Deliv Rev. 2016;107:367–392. doi: 10.1016/j.addr.2016.06.012. [DOI] [PubMed] [Google Scholar]
- 16.Kim SS, Gwak SJ, Choi CY, Kim BS. Skin regeneration using keratinocytes and dermal fibroblasts cultured on biodegradable microspherical polymer scaffolds. J Biomed Mater Res B Appl Biomater. 2005;75:369–377. doi: 10.1002/jbm.b.30302. [DOI] [PubMed] [Google Scholar]
- 17.Sharma K, Bullock A, Ralston D, MacNeil S. Development of a one-step approach for the reconstruction of full thickness skin defects using minced split thickness skin grafts and biodegradable synthetic scaffolds as a dermal substitute. Burns. 2014;40:957–965. doi: 10.1016/j.burns.2013.09.026. [DOI] [PubMed] [Google Scholar]
- 18.Blümel JE, Binfa L, Cataldo P, Carrasco A, Izaguirre H, Sarrá S. Indice de función sexual femenina: un test para evaluar la sexualidad de la mujer. Rev Chil Obstet Ginecol. 2004;69:118–125. doi: 10.4067/S0717-75262004000200006. [DOI] [Google Scholar]
- 19.Fedele L, Frontino G, Restelli E, Ciappina N, Motta F, Bianchi S. Creation of a neovagina by Davydov's laparoscopic modified technique in patients with Rokitansky syndrome. Am J Obstet Gynecol. 2010;202:33.e1–33.e6. doi: 10.1016/j.ajog.2009.08.035. [DOI] [PubMed] [Google Scholar]
- 20.van der Sluis WB, Pavan N, Liguori G, Bucci S, Bizic MR, Kojovic V, et al. Ileal vaginoplasty as vaginal reconstruction in transgender women and patients with disorders of sex development: an international, multicentre, retrospective study on surgical characteristics and outcomes. BJU Int. 2018;121:952–958. doi: 10.1111/bju.14155. [DOI] [PubMed] [Google Scholar]
- 21.Yang B, Wang N, Zhang S, Wang M. Vaginal reconstruction with sigmoid colon in patients with congenital absence of vagina and menses retention: a report of treatment experience in 22 young women. Int Urogynecol J. 2013;24:155–160. doi: 10.1007/s00192-012-1799-7. [DOI] [PubMed] [Google Scholar]
- 22.Creatsas G, Deligeoroglou E, Christopoulos P. Creation of a neovagina after Creatsas modification of Williams vaginoplasty for the treatment of 200 patients with Mayer-Rokitansky-Kuster-Hauser syndrome. Fertil Steril. 2010;94:1848–1852. doi: 10.1016/j.fertnstert.2009.09.064. [DOI] [PubMed] [Google Scholar]
- 23.Moon HS, Koo J, Lee H, Joo BS. Simple neovaginoplasty using spontaneous regeneration ability of labial and vestibular flap in patients with Müllerian agenesis. Gynecol Minim Invasive Ther. 2017;6:173–177. doi: 10.1016/j.gmit.2017.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Schätz T, Huber J, Wenzl R. Creation of a neovagina according to Wharton-Sheares-George in patients with Mayer-Rokitansky-Küster-Hauser syndrome. Fertil Steril. 2005;83:437–411. doi: 10.1016/j.fertnstert.2004.06.079. [DOI] [PubMed] [Google Scholar]
- 25.Walch K, Kowarik E, Leithner K, Schätz T, Dörfler D, Wenzl R. Functional and anatomic results after creation of a neovagina according to Wharton-Sheares-George in patients with Mayer-Rokitansky-Küster-Hauser syndrome-long-term follow-up. Fertil Steril. 2011;96:492–497. doi: 10.1016/j.fertnstert.2011.06.004. [DOI] [PubMed] [Google Scholar]
- 26.Saylor L, Bernard S, Vinaja X, Loukas M, Schober J. Anatomy of genital reaffirmation surgery (male-to-female): Vaginoplasty using penile skin graft with scrotal flaps. Clin Anat. 2018;31:140–144. doi: 10.1002/ca.23015. [DOI] [PubMed] [Google Scholar]
- 27.Wei SY, Li FY, Li Q, Li SK, Zhou CD, Zhou Y, et al. Autologous Buccal micro-mucosa free graft combined with posterior scrotal flap transfer for vaginoplasty in male-to-female transsexuals: a pilot study. Aesthet Plast Surg. 2018;42:188–196. doi: 10.1007/s00266-017-0977-x. [DOI] [PubMed] [Google Scholar]
- 28.Dhall K. Amnion graft for treatment of congenital absence of the vagina. Br J Obstet Gynaecol. 1984;91:279–282. doi: 10.1111/j.1471-0528.1984.tb04768.x. [DOI] [PubMed] [Google Scholar]
- 29.Zhu L, Zhou H, Sun Z, Lou W, Lang J. Anatomic and sexual outcomes after vaginoplasty using tissue-engineered biomaterial graft in patients with Mayer-Rokitansky-Küster-Hauser syndrome: a new minimally invasive and effective surgery. J Sex Med. 2013;10:1652–1658. doi: 10.1111/jsm.12143. [DOI] [PubMed] [Google Scholar]
- 30.Acién P. Malformaciones del aparato genital femenino (Cap.18; Fig 18.89) in Tratado de Obstetricia y Ginecología: Ginecología. Ediciones Molloy, ISBN:84–609–0564-0, Alicante, 2004:691–739.
- 31.Rathee M, Boora P, Kundu R. Custom fabricated acrylic vaginal stent as an adjunct to surgical creation of neovagina for a young female with isolated vaginal agenesis. J Hum Reprod Sci. 2014;7:272–275. doi: 10.4103/0974-1208.147496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kamalakannan J, Murthy V, Kularashmi BS, Jajoo K. Customized Silicone Vaginal Stent. J Obstet Gynaecol India. 2015;65:281–283. doi: 10.1007/s13224-015-0734-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Coskun A, Coban YK, Vardar MA, Dalay AC. The use of a silicone-coated acrylic vaginal stent in McIndoe vaginoplasty and review of the literature concerning silicone-based vaginal stents: a case report. BMC Surg. 2007;10(7):13. doi: 10.1186/1471-2482-7-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bhathena HM. The vacuum expandable condom mold for reconstruction of vagina. Plast Reconstr Surg. 2006;115:973. doi: 10.1097/01.PRS.0000153824.10866.EA. [DOI] [PubMed] [Google Scholar]
- 35.Ellabban MG. The use of a simple syringe as a stent for McIndoe vaginal reconstruction. Plast Reconstr Surg. 2004;114:622–623. doi: 10.1097/01.PRS.0000128506.66933.65. [DOI] [PubMed] [Google Scholar]
- 36.Ozek C, Gurler T, Alper M, Gundogan H, Bilkay U, Songur E, et al. Modified McIndoe procedure for vaginal agenesis. Ann Plast Surg. 1999;43:393–396. doi: 10.1097/00000637-199910000-00009. [DOI] [PubMed] [Google Scholar]
- 37.Pawar RP, Tekale SU, Shisodia SU, Totre JT, Domb AJ. Biomedical applications of poly (lactic acid) Recent Patents Regen Med. 2014;4:40–51. doi: 10.2174/2210296504666140402235024. [DOI] [Google Scholar]
- 38.Tyler B, Gullotti D, Mangraviti A, Utsuki T, Brem H. Polylactic acid (PLA) controlled delivery carriers for biomedical applications. Adv Drug Deliv Rev. 2016;107:163–175. doi: 10.1016/j.addr.2016.06.018. [DOI] [PubMed] [Google Scholar]
- 39.Saini P, Arora M, Kumar MNVR. Poly (lactic acid) blends in biomedical applications. Adv Drug Deliv Rev. 2016;107:47–59. doi: 10.1016/j.addr.2016.06.014. [DOI] [PubMed] [Google Scholar]
- 40.Acién P, Acién MI. Malformations of the female genital tract and embryological bases. Curr Women’s Health Rev. 2007;3:248–288. doi: 10.2174/1573404810703040248. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
PA had full access to all study data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Statement of prior presentation or publications and/or abstract/poster presentation: No prior presentation, including the cases reported. Yes on prosthesis, References 11–13.