

Abstract
A structured review study of drug interventions on sleep disorders in patients with autism spectrum disorders (ASD) has not been published to date. This systematic review aimed to investigate drug interventions for the treatment of sleep disorders in children with ASD. The Web of Science, PubMed, and Scopus databases were searched until March 2019. Study quality was assessed using the Delphi checklist. Due to the heterogeneity of the findings, a meta-analysis was not possible. Drug interventions for the treatment of sleep disorders in patients with ASD included melatonin, atomoxetine, and risperidone. Atomoxetine had no effect on sleep disorders in patients with ASD. A total of 10 studies were reviewed. Melatonin appears to be useful for the treatment of sleep problems in patients with ASD, but further studies are needed to determine the effects of other drugs.
Keywords: Drug, Sleep disorders, Autism spectrum disorders, Meta-analysis
Introduction
Autism spectrum disorders (ASD) are a heterogeneous group and lifelong neurodevelopmental disorders characterized by significantly unnatural or impaired social interaction and participation, difficulty communicating, and restricted behaviors and interests [1,2]. Risk factors for ASD include genetic factors, environmental factors, maternal obesity, maternal smoking, alcohol intake, and pregnancy complications such as preeclampsia and antenatal hemorrhage [3,4]. Pregnancy supplements such as folic acid and vitamins are associated with a 40% reduction in the risk of ASD [4,5].
Sleep disorders are a common problem for children with ASD and often remain untreated. Many hypotheses regarding the cause of sleep problems among ASD patients include anxiety, related brain pathologies, and an inability to regulate the sleep hormone melatonin. Sleep disturbances among children with ASD are associated with inadequate melatonin secretion [6-9]. This problem is an important feature that affects social communication, daily life, daytime functioning and behavior, and quality of life and increases parental sleep disruption and stress. Increased aggression, hyperactivity, and social problems can result from sleep disorder [10].
Parent-directed behavioral interventions for sleep disorders are the first-line treatment for children with ASD [11]. Medication use for sleep disorders is common among children with ASD [12]. Various studies have reported the useful effects of medications such as melatonin for the treatment of sleep disorders among children with ASD [1,6,7]. To date, a structured review study of randomized controlled trials of drug interventions used to treat sleep disorders in patients with ASD. Therefore, the aim of this systematic review was to investigate drug interventions used to treat sleep disorders in children with ASD.
Methods
1. Data sources
The present systematic review aimed to identify drugs used to treat sleep disorders among children with ASD. The report based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist was provided of items for reporting systematic reviews and meta-analyses [13]. The Web of Science, PubMed, and Scopus databases were searched for studies published until March 2019.
2. Search strategy
The search strategy used the following terms: (sleep disorder or sleep disturbance or sleep problem) and (drug intervention or drug treatment) and (autism or ASD or autism spectrum disorder) and (clinical trial or controlled trial).
3. Inclusion and exclusion criteria
Inclusion criteria were all full texts that explored drug interventions for sleep disorders among children with ASD based on randomized controlled trials. Exclusion criteria were review studies, letters to the editor, observational studies, case reports, and qualitative studies.
4. Data extraction
Two authors (EJ and SA) independently screened the titles, abstracts, and full texts of the retrieved studies in EndNote X8. Disagreements were resolved by discussion. The included data were: first author, publication year, sample size, child age (range or mean), drug type, drug dose, treatment outcomes, and treatment duration.
5. Quality assessment
Study quality was evaluated using the Delphi checklist [14]. The checklist includes the following: (1) Was a standard randomization performed? (2) Was the interventional allocation concealed? (3) Was the patient blinded? (4) Was the care provider blinded? (5) Was the outcome assessed or blinded? (6) Were the 2 groups similar at baseline? (7) Were the eligibility criteria well-defined? (8) Was the variability of the outcome presented? (9) Was an intention-totreat analysis performed? Accordingly, a maximum score of 9 was allocated to each study.
Results
A total of 671 articles were retrieved in the primary search based on the search strategy to March 2019. We excluded 163 duplicate articles, 487 articles after the title and abstract review, and 8 after the full-text review. A total of 13 articles [1,6,7,9,11,15-19] with 609 participants that met the criteria for inclusion was retrieved in the present systematic review. All articles were published in English. Due to heterogeneity of the findings, a meta-analysis was not possible. A flowchart of the retrieved articles and selection process is shown in Fig. 1.
Fig. 1.
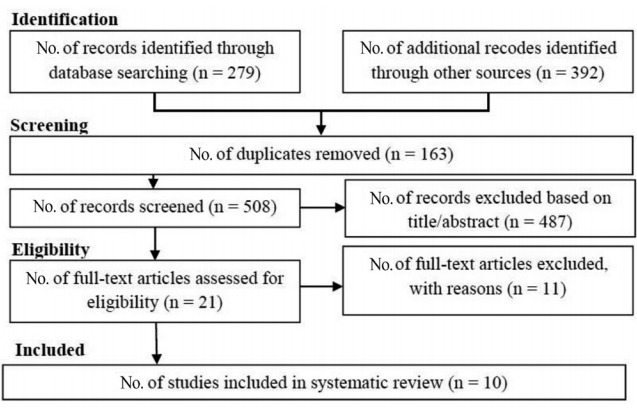
Flow chart of this systematic review.
The present systematic review revealed that atomoxetine had no effect on sleep disorders in patients with ASD (Table 1). It also revealed that melatonin reduced insomnia symptoms, significantly improved sleep latency, improved total sleep time and efficiency, and was a safe long-term treatment option for children with ASD and insomnia. One study reported that risperidone increased the mean sleep time by 29 minutes per day in children with ASD.
Table 1.
Characteristics of the studies included in this systematic review
| Study | Target | Drug name | Dose | Outcome | Treatment duration | Age average | Sample size | Study quality |
|---|---|---|---|---|---|---|---|---|
| Hollway et al. [6] (2018) | ASD | Atomoxetine | The target dose was 1.2 mg/(kg/day), but if necessary this could be increased to 1.8 mg/(kg/day) | There were no significant differences between treatment groups, ATX appears sleep neutral | 10 Weeks | 5.0–14.11 Years | 54 | 6 |
| Cortesi et al. [7] (2012) | ASD | Controlled-release melatonin | 3 mg | Melatonin treatment was mainly effective in reducing insomnia symptoms, while cognitive-behavioral therapy had a light positive impact mainly on sleep latency. | 12 Weeks | 4–10 Years | 134 | 7 |
| Gringras et al. [11] 2017 | ASD | Prolonged-Release Melatonin | dose titration: 2–5 mg/day and up to 10 mg/day | PR-M was efficacious and safe for treatment of insomnia in children and adolescents with ASD | 13 Weeks | 2–17.5 Years | 125 | 7 |
| Maras et al. [1] (2018) | ASD | Prolonged-Release Melatonin | 2, 5, or 10 mg | PR-M, shown to be efficacious versus placebo, is an efficacious and safe option for long-term treatment of children with ASD who suffer from insomnia. | 13 Weeks | 2–17.5 Years | 95 | 7 |
| Wirojanan et al. [15] (2009) | ASD, Fragile X syndrome | Melatonin | 3 mg | The results of this study support the efficacy and toler¬ability of melatonin treatment for sleep problems in children with ASD | 4 Weeks | 2–15.3 Years | 12 | 7 |
| Wright et al. [9] (2011) | ASD | Melatonin | 2 mg to a maximum dose of 10 mg/day | Melatonin significantly improved sleep latency (by an average of 47 min) and total sleep (by an average of 52 min) compared to placebo. The side effect profile was low. | 3 Months | 3–16 Years | 17 | 6 |
| Garstang and Wallis [18] (2006) | ASD | Melatonin | 5 mg | This study provided evidence of effectiveness of melatonin in children with sleep difficulties and ASD. | 4 Weeks | 4 - 16 Years | 11 | 5 |
| Wasdell et al. [16] (2008) | Mixed: neurodevel opmental disabilities, ASD | Controlled-release melatonin | 5 mg | The therapy improved the sleep of 47 children and was effective in reducing family stress. Children with neurodevelopmental disabilities, who had treatment resistant chronic delayed sleep phase syndrome and impaired sleep maintenance, showed improvement in melatonin therapy. | 10 Days | 2–18 Years | 51 | 7 |
| McArthur et al. [17] (1998) | ASD, Rett syndrome | Melatonin | 2.5–7.5 mg | Administration of melatonin appeared to improve total sleep time and sleep efficiency. It is a safe treatment as no adverse side effects were detected. | 4 Weeks | 10.1 Years | 9 | 5 |
| Aman et al. [19] (2005) | Autism | Risperidone | 0.5–3.5 mg | Difficulty falling asleep appeared to decline with Risperidone. Increase in sleep time: mean increase of 29 min of sleep per day, after with risperidone therapy. | 8 Weeks | 5–17 Years | 101 | 7 |
ASD, autism spectrum disorders; ATX, atomoxetine; PR-M, prolonged-release melatonin.
In this systematic review, 3 studies were of low quality and 7 were of high quality according to the Delphi checklist (Table 1).
Discussion
To our knowledge, this is the first systematic review to assess drug interventions for the treatment of sleep disorders in patients with ASD.
The results of this systematic review indicated that melatonin reduced insomnia symptoms, significantly improved sleep latency, improved total sleep time and sleep efficiency, and was a safe longterm treatment option for children with ASD and insomnia.
Hollway et al. [6] assessed the effect of atomoxetine on sleep in youth with ASD. There were no significant differences between the atomoxetine group and the manual parent training program, so atomoxetine appeared ineffective.
Rossignol and Frye [2] conducted a meta-analysis of 5 randomized double-blind studies to evaluate the effect of melatonin in children with ASD in 2011. They presented that melatonin use among children with ASD is associated with improved sleep parameters, better daytime behaviors, and a low incidence of side effects.
Different trials reported that melatonin has good efficacy for sleep disturbances among children with ASD. However, the effects of time long require being thoroughly determined. Despite the widespread use of drugs to treat sleep disorders among children with ASD, the US Food and Drug Administration has not approved any for this indication [20].
A meta-analysis was conducted by Braam et al. [21] in 2009 in which the authors searched the PubMed, MEDLINE, and Embase databases for articles published until 2008. The authors evaluated the effects of melatonin on sleep latency, total sleep time, and number of wakes per night and reported that an abnormal melatonin synthesis led to low nocturnal melatonin levels. Increasing a low melatonin level to a more physiological level may lead to less arousal that intervenes with sleep maintenance.
In 2017, Cuomo et al. [22] conducted another meta-analysis to assess the efficacy of sleep-based interventions for children with ASD. The meta-synthesis included 8 published systematic reviews based on 38 original articles assessing the efficacy of sleep interventions among children with ASD. The included reviews determined 5 major groups of sleep interventions for children with ASD: melatonin therapy, pharmacologic treatments other than melatonin, behavioral interventions, parent education programs, and alternative therapies (iron supplementation, multivitamin use, massage therapy, aromatherapy). The findings of this meta-synthesis propose that no single intervention is effective across all sleep disorders in children with ASD. However, melatonin, behavioral interventions, and parent education programs seem the most effective at improving sleep disorders.
Guénolé et al. [23] performed a systematic review in 2011 on melatonin for sleep disorders in children with ASD by searching the PubMed database for studies published through November 2010. They reported evidence of the useful effects of melatonin on sleep disorders among children with ASD with a low incidence of side effects.
None of the included studies in the present systematic review compared the effects of melatonin to those of other sleep drugs. Therefore, the effectiveness of melatonin compared with other sleep drugs was not determined. However, despite this limitation, the present systematic review reviewed 10 studies and demonstrated that melatonin seems effective for the treatment of sleep problems among children with ASD. Further studies are needed to determine the effects of other drugs for these problems among children with ASD.
Acknowledgments
The protocol of this study was confirmed in Hamadan University of Medical Sciences with code 980210789. The authors thank Hamadan University of Medical Sciences for its financial support of this study.
Key message
Question: What drugs are used to treat sleep disorders in children with ASD?
Finding: Drug interventions for the treatment of sleep disorders in patients with ASD included melatonin, atomoxetine, and risperidone.
Meaning: Melatonin appears to be useful for the treatment of sleep problems in patients with ASD, but further studies are needed to determine the effects of other drugs.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Maras A, Schroder CM, Malow BA, Findling RL, Breddy J, Nir T, et al. Long-term efficacy and safety of pediatric prolonged-release melatonin for insomnia in children with autism spectrum disorder. J Child Adolesc Psychopharmacol. 2018 Oct 11; doi: 10.1089/cap.2018.0020. [Epub]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rossignol DA, Frye RE. Melatonin in autism spectrum disorders: a systematic review and meta-analysis. Dev Med Child Neurol. 2011;53:783–92. doi: 10.1111/j.1469-8749.2011.03980.x. [DOI] [PubMed] [Google Scholar]
- 3.Jenabi E, Karami M, Khazaei S, Bashirian S. The association between preeclampsia and autism spectrum disorders among children: a metaanalysis. Korean J Pediatr. 2019;62:126–30. doi: 10.3345/kjp.2018.07010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lyall K, Schmidt RJ, Hertz-Picciotto I. Maternal lifestyle and environmental risk factors for autism spectrum disorders. Int J Epidemiol. 2014;43:443–64. doi: 10.1093/ije/dyt282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chaste P, Leboyer M. Autism risk factors: genes, environment, and gene-environment interactions. Dialogues Clin Neurosci. 2012;14:281–92. doi: 10.31887/DCNS.2012.14.3/pchaste. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hollway JA, Mendoza-Burcham M, Andridge R, Aman MG, Handen B, Arnold LE, et al. Atomoxetine, parent training, and their effects on sleep in youth with autism spectrum disorder and attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2018;28:130–5. doi: 10.1089/cap.2017.0085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cortesi F, Giannotti F, Sebastiani T, Panunzi S, Valente D. Controlledrelease melatonin, singly and combined with cognitive behavioural therapy, for persistent insomnia in children with autism spectrum disorders: a randomized placebo-controlled trial. J Sleep Res. 2012;21:700–9. doi: 10.1111/j.1365-2869.2012.01021.x. [DOI] [PubMed] [Google Scholar]
- 8.Richdale AL, Schreck KA. Sleep problems in autism spectrum disorders: prevalence, nature, & possible biopsychosocial aetiologies. Sleep Med Rev. 2009;13:403–11. doi: 10.1016/j.smrv.2009.02.003. [DOI] [PubMed] [Google Scholar]
- 9.Wright B, Sims D, Smart S, Alwazeer A, Alderson-Day B, Allgar V, et al. Melatonin versus placebo in children with autism spectrum conditions and severe sleep problems not amenable to behaviour management strategies: a randomised controlled crossover trial. J Autism Dev Disord. 2011;41:175–84. doi: 10.1007/s10803-010-1036-5. [DOI] [PubMed] [Google Scholar]
- 10.Devnani PA, Hegde AU. Autism and sleep disorders. J Pediatr Neurosci. 2015;10:304–7. doi: 10.4103/1817-1745.174438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gringras P, Nir T, Breddy J, Frydman-Marom A, Findling RL. Efficacy and safety of pediatric prolonged-release melatonin for insomnia in children with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. 2017;56:948–57. doi: 10.1016/j.jaac.2017.09.414. e4. [DOI] [PubMed] [Google Scholar]
- 12.Malow BA, Katz T, Reynolds AM, Shui A, Carno M, Connolly HV, et al. Sleep difficulties and medications in children with autism spectrum disorders: a registry study. Pediatrics. 2016;137 Suppl 2:S98–104. doi: 10.1542/peds.2015-2851H. [DOI] [PubMed] [Google Scholar]
- 13.Peters JP, Hooft L, Grolman W, Stegeman I. Reporting quality of systematic reviews and meta-analyses of otorhinolaryngologic articles based on the PRISMA statement. PLoS One. 2015;10:e0136540. doi: 10.1371/journal.pone.0136540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Verhagen AP, de Vet HC, de Bie RA, Kessels AG, Boers M, Bouter LM, et al. The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol. 1998;51:1235–41. doi: 10.1016/s0895-4356(98)00131-0. [DOI] [PubMed] [Google Scholar]
- 15.Wirojanan J, Jacquemont S, Diaz R, Bacalman S, Anders TF, Hagerman RJ, et al. The efficacy of melatonin for sleep problems in children with autism, fragile X syndrome, or autism and fragile X syndrome. J Clin Sleep Med. 2009;5:145–50. [PMC free article] [PubMed] [Google Scholar]
- 16.Wasdell MB, Jan JE, Bomben MM, Freeman RD, Rietveld WJ, Tai J, et al. A randomized, placebo-controlled trial of controlled release melatonin treatment of delayed sleep phase syndrome and impaired sleep maintenance in children with neurodevelopmental disabilities. J Pineal Res. 2008;44:57–64. doi: 10.1111/j.1600-079X.2007.00528.x. [DOI] [PubMed] [Google Scholar]
- 17.McArthur AJ, Budden SS. Sleep dysfunction in Rett syndrome: a trial of exogenous melatonin treatment. Dev Med Child Neurol. 1998;40:186–92. doi: 10.1111/j.1469-8749.1998.tb15445.x. [DOI] [PubMed] [Google Scholar]
- 18.Garstang J, Wallis M. Randomized controlled trial of melatonin for children with autistic spectrum disorders and sleep problems. Child Care Health Dev. 2006;32:585–9. doi: 10.1111/j.1365-2214.2006.00616.x. [DOI] [PubMed] [Google Scholar]
- 19.Aman MG, Arnold LE, McDougle CJ, Vitiello B, Scahill L, Davies M, et al. Acute and long-term safety and tolerability of risperidone in children with autism. J Child Adolesc Psychopharmacol. 2005;15:86984. doi: 10.1089/cap.2005.15.869. [DOI] [PubMed] [Google Scholar]
- 20.Relia S, Ekambaram V. Pharmacological approach to sleep disturbances in autism spectrum disorders with psychiatric comorbidities: a literature review. Med Sci (Basel) 2018 Oct 25;6(4) doi: 10.3390/medsci6040095. pii: E95. doi: 10.3390/medsci6040095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Braam W, Smits MG, Didden R, Korzilius H, Van Geijlswijk IM, Curfs LM. Exogenous melatonin for sleep problems in individuals with intellectual disability: a meta-analysis. Dev Med Child Neurol. 2009;51:340–9. doi: 10.1111/j.1469-8749.2008.03244.x. [DOI] [PubMed] [Google Scholar]
- 22.Cuomo BM, Vaz S, Lee EAL, Thompson C, Rogerson JM, Falkmer T. Effectiveness of sleep-based interventions for children with autism spectrum disorder: a meta-synthesis. Pharmacotherapy. 2017;37:55578. doi: 10.1002/phar.1920. [DOI] [PubMed] [Google Scholar]
- 23.Guénolé F, Godbout R, Nicolas A, Franco P, Claustrat B, Baleyte JM. Melatonin for disordered sleep in individuals with autism spectrum disorders: systematic review and discussion. Sleep Med Rev. 2011;15:379–87. doi: 10.1016/j.smrv.2011.02.001. [DOI] [PubMed] [Google Scholar]