

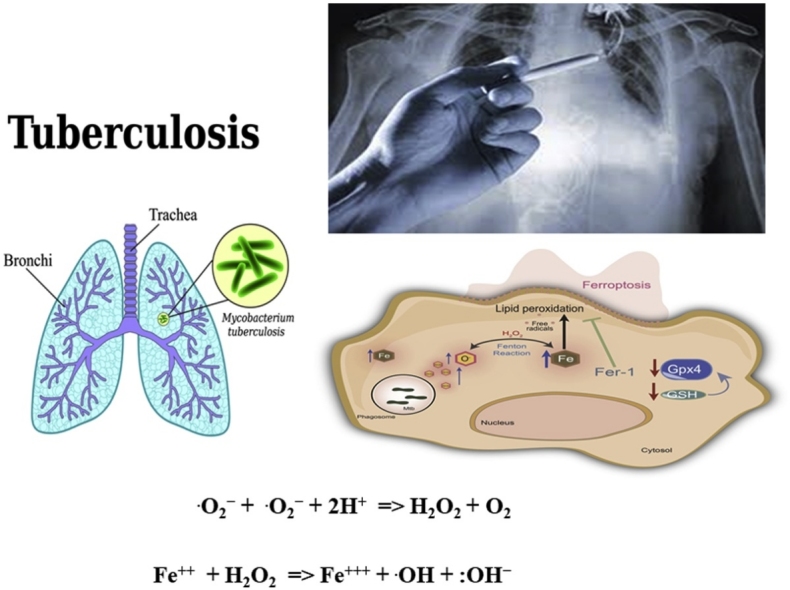
Graphical abstract
Keywords: Pulmonary tuberculosis, Human biological samples, Genders, Atomic absorption spectrophotometer, Smokers
Highlights
-
•
Smoking is linked with tuberculosis recurrence.
-
•
Pakistan has not only high TB number of TB cases (fifth) but also high level of multidrug-resistant TB (fourth) in the world.
-
•
Cu/Zn ratio was also considerably greater in all biological samples of TB patients as compared to the control group.
-
•
The analysis the levels of the elements, {Fe, Cu, Zn and Cu/Zn ratio} may help the studies on the development of TB disease.
Abstract
Tuberculosis is one of the major causes of illnesses and deaths throughout world particularly in Asia. Smoking is linked with tuberculosis recurrence and its mortality and may influence bacteriological conversion, clinical symptoms and treatment outcome. The aim of current study was to estimate association among essential trace elements {zinc (Zn), iron (Fe) and copper (Cu)} in human biological samples particularly blood, serum, scalp hair, saliva, sputum, and nasal fluid of smoking and nonsmoking pulmonary tuberculosis patients (n = 165, age ranged 16–35 years) residents of Hyderabad, Pakistan. The biological samples of age matched healthy controls were chosen as referents of both genders (n = 171) for the comparison purpose. The human biological samples were wet digested in microwave oven by 65 % HNO3 and 30 % H2O2 with (2:1) ratio. The concentrations of elements in acid digested samples were determined by atomic absorption spectrometry. The average zinc and iron concentration was lower, while level of copper was higher in the biological samples of pulmonary Tuberculosis patients as compared to referent subjects (p < .001). It was also concluded as a result of Zn and Fe deficiency combined with high contact of copper due to smoking of tobacco can be synergistic with the risk factors related with pulmonary tuberculosis.
1. Introduction
One hundred thirty seven years ago, Robert Koch identified Tuberculosis (TB). Because poor sanitary conditions in under developed countries complicated with poverty and mal-nutrition and lack of proper diagnosis over 1.5 million people die due TB annually [1]. Annually, almost 9.5 million of TB new events take place globally [1]. It is estimated that about 9.5 million new events of TB may occur globally and according to world TB statistics data, about one-third of the cases are not reported due to improper diagnosis. Nearly 80 % of TB incidence took place in 22 countries out of these some are not yet diagnosed [1]. Six countries had the largest number of occurrence cases in 2014 [1]. During that year one-quarter of world TB cases were reported from India and about one million TB cases were not reported [1]. Internationally, TB ranks as the leading cause of morbidity and mortality [1]. Incidences of TB are increasing globally and in developing countries this disease is regarded as the main reason of adult mortalities. For example 1.7 million people died along with 9.2 million new incidences of TB were reported globally during 2006 [1]. Pulmonary TB caused by Mycobacterium tuberculosis. It is a chronic contagious disease. This disease may be recognized by protracted cough, shortness of breath pain in chest, hemoptysis, along with other symptoms of the disease include anorexia, fever, evening high temperatures followed by night sweats, depression, weight loss and weakness [1]. Pulmonary TB commonly found in poor people affected by malnutrition and their nutritional status with reference to trace elements is still poorly documented [2,3]. The TB is generally provoked by varied damage of Mycobacterium frequently Mycobacterium TB. It usually attacks the lungs, but can also influence other body organs [4] (Garner et al., 2007).
Majority of the infections are asymptomatic (latent TB) and one-tenth of latent TB disease, at the end more than 50 % deaths occurred due to active disease, if not cured [4]. Symptoms of active TB include chronic cough with cracked sputum, fever, weight loss and night sweats. Injury to other parts of the body causes a wide range of symptoms [5]. The relationship between TB and scarcity is well renowned, the maximum rates of TB were found in the poor income community [6]. TB is usually found in poor people living in middle income areas [7]. Scarcity may result in poor nutrition which can alter the immune function. On the Contrary, risk of transmission of TB is more likely to be in congested living conditions, poor exposure to air, and poor hygiene-habits [8]. As compared to women, men are frequently affected. In most of the countries the case declaration is higher in males as compared to females. For example during 2004, 1,400,000 men were reported as against 775,000 women as TB patients [9], which makes global male to female TB ratio 0.47:0.67 globally [10]. The reason for such gender differentiation is unclear. Perhaps due to dissimilarity in the occurrence of disease, time of succession from infection to disease, the dissimilarity in access to services.
Pulmonary TB and smoking are strongly connected to each other. Pakistan has not only high TB number of TB cases (fifth) but also high level of multidrug-resistant TB [MDRTB] (fourth) in the world. Malnutrition is observed mainly in infected TB patients in under-developed nations. TB is positively associate with gender and age, life style particularly use of alcohol, smoking habits and malnutrition specially the body mass index which are considered as major risk factors [11]. The relationship of smoking with TB is a main dilemma which raise the intensity of disease and latent TB is converted into an active TB [12].
It was declared that the public is considerably contaminated with Mycobacterium tuberculosis approximately> 30 % in the globe. The TB is major cause of death; nevertheless, smoking enhances the chances to develop TB; therefore, it enhance casualty by up to 12 % globally [13]. According to worldwide yearly death menace factors, tobacco smokers are major facts. About 90 % of death took place owing to lung cancer due to smoking [14,15]. Many studies have been reported the utmost relationship of TB with smokers with comparison to nonsmokers [[16], [17], [18]]. However, smoking is considered as a major resource of trace and toxic elements particularly, copper (Cu), nickel (Ni) and cadmium (Cd) which are being regarded as the main cause of cigarette smoke-inspired illnesses [19,20]. A study showed that smoking habit has serious withdrawal symptoms such as strong need to smoke, becoming uncomfortable or futile endeavors to quit this habit may emerge in youth [21].
Trace elements including iron (Fe), copper (Cu), and zinc (Zn) have significant role in many biological systems [22,23].These elements play a vital role in the protection and development of human tissues and organs [24]. Furthermore, these elements are considered as possible key aspects in various contagious infections. Various facts stated that a few transition elements facilitate immune system inhibit microorganisms such as Mycobacterium TB [25,26]. The ingestion of toxic elements may lead to pulmonary TB, myocardial infarctions and atherosclerosis related disorders by rising oxidative stress caused by deficiency of an antioxidant element Zinc [27]. Due to the lack of essential nutrients particularly the elements, and homeostatic management or an additional ingestion of various toxic metals may cause chronic illnesses such as hypertension, TB, and cardiovascular disease [28].
As zinc (Zn) is an essential trace metal because it is an important part of biological membranes integrity and is required in many enzymes [29]. Zinc is involved in numerous aspects of cellular metabolism [30]. It is an essential component of some important enzymatic systems. In the human body there may exist over 200 enzymatic systems which are depending on Zn, through which it is realized the elimination of the carbon dioxide carried by red blood cells, the oxidation-reduction processes, the synthesis of the proteins, etc [31]. Cellular immune system uses Zn for bactericidal activity particularly the destruction of Escherichia coli, Tubercle bacilli, etc [32,33]. Protein syntheses processes of many bacteria including M. tuberculosis are regulated by essential metals due to presence of contain metal-responsive DNA-binding sites known as transcriptional repressors [34]. Zn can hold to stabilize biological macromolecules due to its antioxidant-like properties [35]. In biological systems, DNA controls the protein synthesis. Bacterial DNA molecules, particularly in M. tuberculosis have sites for binding of Zinc and Zinc-bound DNA cannot synthesize the needed proteins for proper functioning. This results in death of bacteria. Host cell become immune by utilizing zinc which in turn kill the TB bacteria and Escherichia coli bacteria [35].
Iron being fundamental element for growth of almost all body systems, is found in body in variety of complex binding proteins, such as transferrin, lactoferrin, and ferritin [36]. Furthermore it is also important for both parasite and host cells strength hence pathogens are focused by high similarity up taking processes [37]. Iron is a crucial element for all organisms because it functions as an essential key-factor for metabolic routes and enzyme function. Cells control iron reactivity, availability, and instability to stop free radical damage to proteins, ribonucleic acids, and cell membranes. Iron is necessary and iron insufficiency significantly damage cell proliferation and immune function [38]. Iron is mandatory for the growth of TB in macrophages, and excessive iron consumption is associated with an increase in active TB and its mortality [[39], [40], [41]]. Iron function in pathology, growth and metabolism of TB depends on obtaining iron from the host's resources. As a result, iron deficiency anemia is commonly observed among TB patients [42].
Copper is a vital food ingredient that has a variety of physiological procedures in the human body. Copper is essential for infant growth, host defense mechanisms, bone strengthening, mature red blood cells, white blood cells, iron transport, cholesterol, glucose metabolism, and myocardial infarction [43,44]. Different types of drugs have structures that indicate they are clotting factors and may therefore affect copper metabolism [45]. Copper is involved in the framework of various enzymes that function in redox reactions, such as cytochrome oxidase, lysyl oxidase, superoxide dismutase, ceruloplasmin, and metallothioneins [46]. While copper has various biological advantages, its excess is lethal, and might slow down M. Tuberculosis development [47].
To keep in view of these facts, it is necessary to analyze the essential trace and toxic elemental concentrations in the biological samples of T1DM children, and to monitor their impact on the human metabolism. In many cases, whole blood, serum, plasma, and urine were analyzed [47]. The atomic absorption spectrometry (AAS) is mostly used for the clinical assay due to their specificity, sensitivity, precision, simplicity, and relatively low cost per analysis [48]. Hair analysis has many advantages as compared to serum, blood or other body fluids such as it is easily collected, stable on storage and has a higher concentration of elements, but many individuals and external factors can influence element levels [49,50].
The present study examines Fe, Zn and Cu burden in biological samples, such as blood, serum, saliva, nasal fluid, sputum, scalp hairs of newly diagnosed TB patients (male and female). The other biochemical and clinical parameters were also estimated. These three elements were also determined simultaneously in the samples of healthy volunteers of the same age and gender for comparatives assessment.
2. Material and methods
2.1. Recruitment
Prior permission of ethical review committee of Sindh University was sought so as to initiate the research study.
2.2. Apparatus
A Milestone microwave oven (Rotar MPR-300/12S, pressure 35 bar, with maximum temperature 300 °C) was used. Elemental analysis was performed on a Hitachi (Tokyo) Model 180-50, S.N.5721-2 atomic absorption (AA) spectrophotometer equipped with a flame burner, graphite furnace GA-3, and a deuterium lamp background corrector. Hollow-cathode lamps (Mitorika Company) were used. Operational parameters, including lamp currents and wavelength, were those, recommended by the manufacturer. The spectrophotometer output was connected to a Hitachi recorder (model 056) with a range of 5 mV. The signals measured were the heights of the absorbance peaks for the flame absorption mode, and integrated absorbance values (peak area) were used for the graphite furnace. The instrumental conditions are reported in Table 1a, Table 1b, Table 1c. The Cu, Fe and Zn in scalp hair, blood and serum samples were measured under optimised operating conditions using flame atomic absorption spectrometry (FAAS) mode with an air–acetylene flame, whlist in the saliva, sputum and nasal fluids these samples were determined through electrothermal atomic absorption spectrometry (ETAAS) mode. Signals were measured as absorbance peaks in the flame absorption mode, whereas integrated absorbance values (peak area) were determined in the graphite furnace. The collected samples were heated/ digested by means of domestic microwave oven model Pel (PMO23) which has the heating power of 900 W. Acid washed polytetrafluroethylene (PTFE) vessels/ flasks were utilized for preparation and storage of prepared solutions. Reagents blanks and complex working standard were run in parallel and corrections were made as required.
Table 1a.
Measurement Conditions for Flame Ionization (FAAS).
| Parameters | Lamp current (mA) | Wave length (nm) | Slit width (nm) | Burner height (mm) | Oxidant (Air) L/ min | Fuel (Acetylene) L/min |
|---|---|---|---|---|---|---|
| Zn | 7.5 | 214 | 0.2 | 7.5 | 17 | 2 |
| Fe | 7.5 | 248.5 | 1.3 | 7.5 | 17 | 2 |
| Cu | 7.5 | 324.8 | 1.3 | 7.5 | 17 | 2 |
Table 1b.
Measurement Conditions for Electrothermal Atomization (ETAAS).
| Parameters | Cu | Fe | Zn |
|---|---|---|---|
| Lamp current (mA) | 7.5 | 10.0 | 10 |
| Wavelength (nm) | 324.8 | 248.3 | 213.8 |
| Slit- width (nm) | 1.3 | 0.2 | 1.3 |
| Background correction | D2 | D2 | D2 |
| cuvette | Tube | Tube | Cup |
| Carrier gas (ml/min) | 200 | 200 | 200 |
| Sample volume (μl) | 10 | 10 | 100 |
Table 1c.
Temperature Program.
| Parameters | Cu | Fe | Zn |
|---|---|---|---|
| Dry | 80-120/ 15 | 80-120/ 15 | 80-120/ 15 |
| Ash | 300-600/15 | 300-600/15 | 300-600/15 |
| Atomization | 2500-2600/3 | 2400-2500/3 | 2000-2100/3 |
| Cleaning | 2600–2700/1 | 2500-2600/1 | 2100-2200/1 |
2.3. Reagents and glassware
Ultra pure water was obtained through MiliQ purification system of Millipore Corp (Bedford, USA). Analytical reagent grade chemical were used. H2O2 (30 %), HNO3 (65 %) as well as other necessary chemicals were procured from E. Merck (Germany). Metal contamination of all the chemicals was tested prior to use. certified standard solution (1000 ppm) of Cu, Fe and Zn were got from Fluka Kamica (Buchs, Switzerland). Working standard solutions were organized through serial dilution of stock solution with HNO3 (0.2 mol L−1). All the solutions were kept in polyethylene bottles and stored at 4 °C. To get sensitivity and selectivity of the method, certified reference materials (CRMs) of human hair BCR 397 (Brussels, Belgium), Clinchek®, Control lypholized human serum and blood Recipe (Germany Munich) were collected. For washing and rinsing apparatus and plastic materials, which were already dipped in (2 mol L−1) HNO3 for twenty-four hours, ultrapure and distilled water was used.
2.4. Study design and pretreatment
The data of study population (165 smokers and non smoker pulmonary TB patients of both genders), admitted in Chest Diseases Institute Kotri, Department of Health, Government of Sindh, Pakistan, age ranged as 16–35 years, during 2016–2017, was acquired by collecting and extracting important information. It was a community-based case control study. The study population included adults between the ages of 16–35 years of age residing in lower Sindh, a low-socio economic, pre-urban settlement in Hyderabad. The contributors were tempted to take part and provide the samples. They responded to interview-administered questionnaire covering socio-demographics, lifestyles, dietary habits, and residential and work history. Based on questionnaire, we selected 336 volunteers (aged 16–35, 185 (55 %) male and 151 (45 %) women). Two groups were formed: TB patients and healthy subjects. The referents and TB patients were further divided into two categories, based on their smoking habits. Out of 171 referents (93 male and 78 females), 92 (49 male and 43 females) were nonsmokers and 79 (44 male and 35 females) were smokers. Whilst in 165 TB patients, 84 (45 male and 39 females) were nonsmokers and 81 (47 male and 34 females) were smokers (Table 2). All the TB samples were collected from definitely newly diagnosed pulmonary TB cases attending Institute of Chest Diseases Kotri, Department of Health, Government of Sindh, Pakistan. Pulmonary TB patients had bacteriological tests and clinical examinations. The patients signed an informed written approval. All patients had gone through clinical examinations and bacteriological tests. The informed written approval was signed by the patients. The important biochemical tests are given in Table 3.
Table 2.
Demographic information of smoker and non smoker referents and pulmonary Tuberculosis patients and referents.
| Gender | Smoking habit | Controls (n = 171) | TB Cases (n = 165) |
|---|---|---|---|
| Male | Non Smokers | 49 | 45 |
| Smokers | 44 | 47 | |
| Female | Non Smokers | 43 | 39 |
| Smokers | 35 | 34 |
Table 3.
Anthropometric information of smoker and non smoker referents and pulmonary Tuberculosis patients.
| Important biochemical tests | Non Smokers |
Smokers |
||||||
|---|---|---|---|---|---|---|---|---|
| Male |
Female |
Male |
Female |
|||||
| Referents | T.B patients | Referents | T.B patients | Referents | T.B patients | Referents | T.B patients | |
| CRP (mg/l) | 0.75 ± 0.09 0.72-0.78 | 5.60 ± 0.40 5.47-5.73 | 0.605 ± 0.056 0.586-0.623 | 4.80 ± 0.50 4.61-4.98 | 2.80 ± 0.31 2.70-2.91 | 16.8 ± 0.86 16.5-17.1 | 1.80 ± 0.20 1.71-1.88 | 10.8 ± 1.07 10.4-11.1 |
| BMI (kg/m2) | 20.8 ± 4.36 19.5-22.1 | 17.4 ± 3.76 16.2-18.6 | 20.2 ± 2.17 19.5-20.9 | 16.7 ± 4.33 15.1-18.3 | 19.6 ± 3.16 18.5-20.7 | 16.2 ± 2.68 15.4-17.0 | 18.7 ± 2.39 17.7-19.7 | 15.3 ± 3.20 14.3-16.3 |
| ESR (mm/hour) | 11.0 ± 1.01 10.7-11.3 | 49.0 ± 6.61 46.8-51.2 | 13.0 ± 1.31 12.6-13.4 | 37.0 ± 2.79 35.9-38.0 | 14.0 ± 1.49 13.5-14.5 | 57.0 ± 9.0 54.3-59.7 | 16.6 ± 1.52 15.9-17.2 | 44.0 ± 4.64 42.5-45.5 |
Inclusion criteria for the healthy subjects or non-tuberculosis controls was be: (1) fever, nonexistence of cough, or evidence of pulmonary disease at the time of enrollment; and (2) no earlier diagnosis of TB disease and no known or suspected domestic contact with pulmonary TB in the past 2 years. Healthy individuals were selected using probability sampling. For the section of 171 health subjects, a prior medical checkup of all of the subjects was conducted by a qualified physician.
The selection of TB patients was supported by the following criteria: age 16–35 years; sputum specimen positive for acid-fast bacilli by microscopy and clinical and radiographic abnormalities consistent with pulmonary TB. The enclosure criteria included age > 16 years, renowned case of smear-positive pulmonary TB, < 1 week of anti-TB therapy, conformity to receive anti-TB therapy in Tbilisi, completion of the seventy-two hour summon up instrument at baseline (week 1) and the serial twenty-two hour recalls during two week, and a signed informed approval. Exclusion criteria included the following: Re-treatment TB patients, Patients with extra pulmonary TB or with multi-drug resistant TB, the women who had given birth within the last 6 months of study entry. Those TB patients, who had clinical signs of liver disease, renal failure, HIV positive, cancer, diabetes, hypertension or any other cardiovascular disease; those TB patients, who had used corticosteroids or any supplements containing vitamin A, zinc or iron during previous month prior to treatment. We also excluded those patients who had other chest ailments such as chronic obstructive pulmonary disease (COPD), pneumonia, asthma, and other chest diseases.
2.5. Ethical consideration
Ethical approval for the collection of sample was obtained from the Chest Institute, Kotri, Ministry of Health, Sindh. Declaration of Helsinki code was followed strictly for obtaining the written consent after seeking complete information healthy volunteers and tuberculosis patients or their parents or legal guardian. Confidential identifiers were used to code participant identities. The result and any information regarding patient was kept confidential during and after the completion of the research project by password, protected electronics and locking hard copy files.
2.6. Sample collection
2.6.1. Blood and sera sample collection
Venous blood was drawn aseptically from each case and control by the registered study male nurse. The puncture site was cleaned with trace-element free alcohol to avoid contamination and infection. For trace elemental analysis the blood samples were collected in designed plastic blood collection tubes (BD Vacutainer Trace Element tube with potassium-EDTA, BD, Oxford, UK). Five milliliter of venous blood was drawn after overnight fasting from all proven patients before and after treatment. The blood samples were protected from light with aluminum foil during transport and processing, and were allowed to clot at room temperature for about one hour. For separating sera, samples were centrifuged at 3000 rpm (3000 g) for 15 min at room temperature so as to separate blood cells from serum. Hemolytic sera were discarded. The sera was transferred to polyethylene tubes and kept in freezer at −20 °C till the elemental analysis.
2.6.2. Saliva sample collection
5 ml mixed un-stimulated saliva was collected in polypropylene vials by direct collection. The spit collection method was employed for saliva collection; patients and control were told to accumulate saliva in the oral cavity and then spit it into a pre-labeled vial.
2.6.3. Sputum sample collection
All cases and controls were mandatory to present the study male nurse for the collection of sputum sample, which was collected and transported to National centre of Excellence in Analytical Chemistry (NCEAC), Jamshoro for analysis. Spontaneously expectorated sputum samples were collected from the subjects. Induced sputum was collected from healthy control subjects following inhalation of nebulised 4.5 % hypertonic saline.
2.6.4. Nasal fluid sample collection
Nasal fluid was collected by the use of a small spoon of plastic, about 10 mm x 5 mm x 2 mm and placed as soon as possible in a micro centrifuge tube with a lid of 1.5 ml volume or less, which is kept closed. Minimum volume of sample was 0.25 ml.
2.6.5. Scalp hair sample collection
Around 0.5 g of three hundred thirty six scalp hair samples was collected from each smoker and non-smoker referents and patient with TB disease. All hair samples was collected from the back of the head using stainless steel scissors and stored in metal free containers. The control hair samples were gathered from apparently healthy volunteers (in particular did not have TB or any other lung disease). Their ages were selected to be in the same range of the target group. Among 0.5–2.0 cm segments of hair was collected from the nape of neck (midpoint between the shoulders) as close to the scalp as possible using stainless steel scissors, cleaned after each use with deionized or double distilled water. For each participant separate plastic envelopes were used to put scalp hair samples, which were sealed tightly and given an identification number of the participant and questionnaire.
2.7. Microwave-assisted acid digestion method
All the samples were prepared in duplicate. Six replicate samples of certified reference materials of blood and serum were also prepared. 200 mg of scalp hair and 0.2 ml of each sample of whole blood, serum, saliva, nasal fluid, and sputum was used. The samples were prepared by adding 1 ml freshly prepared mixture of concentrated HNO3– H2O2 (2:1, v/v) to each PTFE flask. The flasks were then heated for 2–3 min to carry out digestion. Next the flasks were allowed to cool at ambient temperature, and volume was made up to 10.0 ml with distilled water. The same procedure was followed for preparation of Blank solution. Finally, Cu, Fe and Zn concentrations in standards samples were analyzed by FAAS. The Cu, Fe and Zn in scalp hair, blood and serum samples of referents and TB patients were measured through FAAS mode, whilst in the saliva, sputum and nasal fluids of referents and TB patients were determined by ETAAS mode.
2.8. Data analysis
The validity and efficiency of the microwave-assisted digestion method was checked with those obtained from the certified reference materials values. The indicative values of Cu, Fe and Zn for microwave-assisted digestion method were calculated as the arithmetic means of six replicates of certified human hair sample (BCR 397), Clinchek®, Control lypholized human serum and blood Recipe. The reproducibility [% relative standard deviation (RSD)] of the results obtained by MDM was calculated as
The relative standard deviation (RSD) values depended on the elements. No significant difference was observed between the metal obtained by microwave-assisted digestion and those obtained from the certified reference materials tabulated values. The percent recovery was calculated by the mean values obtained for each metals in the certified reference materials by microwave-assisted digestion (MDM), divided by tabulated values of each metals in the certified reference materials, and multiplied by 100 (Table 4). The reliability of method was found to be best in accord with certified values of Cu, Fe and Zn, 98.7 and 99.7 % recovery respectively (Table 4). The sample digestion procedure required less than 5 min to process the samples completely. Mean values of both elements varied little (<1-2 %) from the standard values and relative standard deviation (RSD) <2 %.
Table 4.
Determination of Cd and Zn in certified samples (CRM) by microwave digestion method (MWD).
| Elements | Certified values | MWD | T valuea | % Recoveryb |
|---|---|---|---|---|
| CRM of whole serum (mg /1) | ||||
| Iron | 1.30 ± 0.3 | 1.286 ± 0.087 (7.65) | 0.824 | 98.9 |
| Copper | 1.2 ± 0.2 | 1.194 ± 0.074 (6.20) | 0.855 | 99.5 |
| Zinc | 0.97 ± 0.01 | 0.965 ± 0.019 (1.97) | 0.376 | 99.5 |
| CRM of whole blood (mg /1) | ||||
| Iron | 14.2 ± 3.24 | 14.15 ± 0.76 (5.37) | 0.935 | 99.6 |
| Copper e | 13.9 ± 2.7 | 13.85 ± 0.97 (7.00) | 0.910 | 99.6 |
| Zinc | 2.27 ± 0.06 | 2.24 ± 0.05 (2.23) | 0.304 | 98.7 |
| CRM of human hair (μg/ g) | ||||
| Iron | 580.0 ± 10 d | 576.0 ± 21.0 (3.64) | 0.657 | 99.3 |
| Copper | 110 ± 5 f | 109.5 ± 4.33 (3.95) | 0.838 | 99.5 |
| Zinc | 199 ± 5 | 198.5 ± 10.0 (5.04) | 0.872 | 99.7 |
cmg/l.
dInformative value.
eμg/l.
^Paired t-test between Certified Value and MWD DF = 5, T (critical) at 95 % CI = 2.57, p < 0.50 Values in () are %RSD $ % recovery was calculated according to : ([MDM])/([Certified Value]) x 100.
dInformative value.
2.9. Statistical analysis
The resulted data of patients and controls were interpreted different statistical programs such as Excel ((Microsoft Corp., Redmond, WA) and Minitab 13.2 (Minitab Inc., State College, PA). The resulted data of three essential elements in biological samples are mentioned with confidence interval (CI). The CI might be provided some useful information on the clinical importance of results and, like p-values, may also be used to assess 'statistical significance difference. Differences were significant when the P-value was <0.05. Pearson's correlation was used to link the difference in concentration of elements in patients and referents. ANOVA and the Kreskas–Wallis nonparametric test at the 95 % confidence interval were used for the interpretation.
2.10. Analytical figures of merit
Calibration was performed with a series of Cu, Fe and Zn standards. Sensitivity (m) was the slope value obtained by least-square regression analysis of calibration curves based on absorbance signals. The equation (n = 5) for the calibration curves was as follows:
| Y = (4.35 × 10−3) Cu + 4.25 × 10-4, r = 0.999 |
| Y = (1.18 × 10−3) Fe + 1.25 × 10-4, r = 0.999 |
| Y = (8.09 × 10−3) Zn + 7.60 × 10-4, r = 0.999 |
Where Y is the integrated absorbance, r is the regression and the concentration range of Cu, Fe and Zn for calibration curve reached from the detection limits up to 100 μg/L. The limit of detection, equal to 0.005 ng/mg, 0.001 ng/mg, and 0.005 ng/mg for Cu, Fe, and Zn, respectively, was defined as 3 s/m, “s” being the standard deviation corresponding to ten blank injections and ‘m’ the slope of the calibration graph. The quantification limits, defined as 10 s/m were calculated as: 0.0013, 0.003, and 0.014 ng/mg for Cu, Fe, and Zn, respectively.
3. Results
The mean concentrations with standard deviations for both elements (Cadmium and Zinc) in biological (scalp hair, blood, serum, sputum, saliva and nasal fluid) samples are shown in Table 5. The results indicate that the concentrations of essential trace and toxic elements were altered in biological samples (blood, serum, saliva, and nasal fluid)of smoker and nonsmoker TB patients of both genders.
Table 5.
Copper, iron and zinc concentrations in biological samples (blood, serum, saliva, nasal fluid, sputum, scalp hairs) of smokers and nonsmokers referent and pulmonary Tuberculosis patients of both genders.
| Biological specimens | Non Smokers |
Smokers |
||||||
|---|---|---|---|---|---|---|---|---|
| Male |
Female |
Male |
Female |
|||||
| Referents | T.B patients | Referents | T.B patients | Referents | T.B patients | Referents | T.B patients | |
| Zinc | ||||||||
| Scalp hairs (μg/g) | 239 ± 16.4 | 144 ± 16.6 | 207 ± 10.7 | 133 ± 12.5 | 195 ± 19.6 | 136 ± 20.6 | 189 ± 7.54 | 125 ± 11.7 |
| 234-244 | 139-150 | 204 -211 | 128 -137 | 189-202 | 129-142 | 186-192 | 121-128 | |
| Blood (mg/l) | 5.90 ± 0.22 | 4.90 ± 0.21 | 5.77 ± 0.18 | 4.54 ± 0.13 | 5.54 ± 0.20 | 4.60 ± 0.15 | 5.26 ± 0.18 | 4.13 ± 0.15 |
| 5.83-5.97 | 4.82-4.97 | 5.71-5.83 | 4.50-4.59 | 5.47-5.61 | 4.55-4.64 | 5.19-5.33 | 4.08-4.18 | |
| Serum(mg/l) | 1.19 ± 0.19 | 0.98 ± 0.08 | 1.12 ± 0.17 | 0.93 ± 0.09 | 1.11 ± 0.15 | 0.92 ± 0.06 | 1.08 ± 0.15 | 0.84 ± 0.06 |
| 1.13-1.25 | 0.95-1.00 | 1.06-1.17 | 0.90-0.96 | 1.06-1.17 | 0.89-0.94 | 1.01-1.14 | 0.82 -0.87 | |
| Sputum(μg/l) | 362 ± 13.8 | 244 ± 10.7 | 330 ± 35.5 | 242 ± 62.7 | 340 ± 12.4 | 230 ± 7.84 | 301 ± 38.4 | 220 ± 46.1 |
| 358-366 | 241 -248 | 318 -341 | 219-265 | 335-344 | 227-232 | 285-316 | 205-235 | |
| Saliva (μg/l) | 138 ± 12.7 | 100 ± 13.5 | 127 ± 12.9 | 94.6 ± 7.25 | 130 ± 13.8 | 89.9 ± 14.2 | 117 ± 10.8 | 86.0 ± 8.92 |
| 134-142 | 95.7-104 | 123-132 | 91.9-97.3 | 125-134 | 85.7-94.2 | 113-122 | 83.1 -88.8 | |
| Nasal Fluid (μg/l) | 167 ± 20.3 | 146 ± 10.4 | 137 ± 12.8 | 120 ± 12.6 | 160 ± 17.7 | 140 ± 7.20 | 121 ± 13.7 | 105 ± 10.4 |
| 161-173 | 142-149 | 133-142 | 115-124 | 154-166 | 137-142 | 115-126 | 102-108 | |
| Iron | ||||||||
| Scalp hairs (μg/g) | 41.1 ± 3.33 | 33.0 ± 2.87 | 38.5 ± 2.26 | 31.72 ± 1.919 | 36.4 ± 2.38 | 30.3 ± 2.51 | 35.4 ± 1.98 | 29.1 ± 2.23 |
| 40.1-42.1 | 32.1-34.0 | 37.8-39.3 | 31.01-32.42 | 35.5-37.2 | 29.5-31.0 | 34.5-36.2 | 28.4-29.8 | |
| Blood (mg/l) | 483 ± 18.5 | 365 ± 15.96 | 471 ± 15.0 | 348.1 ± 9.98 | 443 ± 16.2 | (331-338) | 432 ± 14.8 | 322 ± 12.0 |
| 478-489 | 360-370 | 466- 476 | 344-352 | 438-449 | 335 ± 11.4 | 426- 438 | 318-328 | |
| Serum (mg/l) | 3.89 ± 0.65 | 2.30 ± 0.205 | 3.50 ± 0.55 | 2.701 ± 0.263 | 3.57 ± 0.50 | (2.06-2.16) | 3.21 ± 0.45 | 2.48 ± 0.20 |
| 3.69-4.09 | 2.23-2.37 | 3.32-3.68 | 2.604-2.80 | 3.40-3.74 | 2.11 ± 0.16 | 3.03-3.40 | 2.41-2.54 | |
| Sputum (μg/l) | 1.39 ± 0.29 | 1.02 ± 0.22 | 1.35 ± 0.14 | 1.00 ± 0.25 | 1.27 ± 0.20 | (0.88-0.98) | 1.23 ± 0.15 | 0.91 ± 0.19 |
| 1.30-1.48 | 0.94-1.09 | 1.30-1.39 | 0.90-1.09 | 1.20-1.34 | 0.93 ± 0.15 | 1.17-1.30 | 0.85-0.97 | |
| Saliva (μg/l) | 0.89 ± 0.08 | 0.60 ± 0.08 | 0.82 ± 0.08 | 0.60 ± 0.04 | 0.81 ± 0.08 | 0.55 ± 0.08 | 0.75 ± 0.06 | 0.55 ± 0.05 |
| 0.86-0.91 | 0.57-0.62 | 0.79-0.84 | 0.58-0.61 | 0.78-0.84 | 0.52-0.57 | 0.72-0.78 | 0.53-0.56 | |
| Nasal Fluid (μg/l) | 1.19 ± 0.14 | 0.87 ± 0.06 | 1.12 ± 0.10 | 0.90 ± 0.09 | 1.09 ± 0.12 | 0.79 ± 0.04 | 1.02 ± 0.11 | 0.82 ± 0.08 |
| 1.14-1.23 | 0.84-0.89 | 1.08-1.15 | 0.86-0.93 | 1.05-1.13 | 0.78-0.81 | 0.98-1.07 | 0.79-0.85 | |
| Copper | ||||||||
| Scalp hairs (μg/g) | 15.3 ± 1.25 | 21.5 ± 1.87 | 16.1 ± 0.95 | 23.4 ± 1.42 | 13.3 ± 0.91 | 19.4 ± 1.46 | 14.5 ± 0.81 | 21.1 ± 1.62 |
| 14.9-15.7 | 20.9-22.2 | 15.8-16.5 | 22.9-24.0 | 13.0-13.7 | 18.9-19.8 | 14.2-14.9 | 20.6- 21.6 | |
| Blood (mg/l) | 1.06 ± 0.04 | 1.53 ± 0.06 | 1.11 ± 0.03 | 1.61 ± 0.09 | 0.95 ± 0.03 | 1.90 ± 0.06 | 0.99 ± 0.03 | 1.44 ± 0.05 |
| 1.05-1.07 | 1.51-1.55 | 1.09-1.12 | 1.57-1.64 | 0.94-0.96 | 1.88-1.92 | 0.98-1.01 | 1.43-1.46 | |
| Serum (mg/l) | 0.81 ± 0.13 | 1.17 ± 0.10 | 0.94 ± 0.14 | 1.37 ± 0.13 | 0.72 ± 0.10 | 1.05 ± 0.07 | (0.80-0.90) | 1.24 ± 0.10 |
| 0.76-0.85 | 1.13-1.20 | 0.90-0.99 | 1.32-1.42 | 0.69-0.76 | 1.03-1.08 | 0.85 ± 0.11 | 1.20-1.27 | |
| Sputum (μg/l) | 619 ± 130 | 898 ± 194 | 699 ± 75.2 | 101 ± 263 | 557 ± 89.8 | 809 ± 134 | (596-663) | 913 ± 191 |
| 580-659 | 835-962 | 675-724 | 918-111 | 527-588 | 768-849 | 629 ± 80.5 | 851-975 | |
| Saliva (μg/l) | 172 ± 15.8 | 249 ± 33.6 | 191 ± 19.4 | 278 ± 20.9 | 154 ± 16.5 | 224 ± 35.4 | (166-179) | 250 ± 26.4 |
| 167-176 | 238-260 | 185-198 | 270-286 | 149-160 | 213-235 | 172 ± 15.8 | 242-259 | |
| Nasal Fluid (μg/l) | 239 ± 29.0 | 348 ± 24.8 | 269 ± 25.0 | 391 ± 41.1 | 215 ± 23.8 | 313 ± 16.1 | (231-254) | 352 ± 35.0 |
| 231-248 | 339-356 | 261-278 | 376-406 | 207-224 | 308-318 | 243 ± 27.4 | 341-363 | |
The Zn contents in scalp hair, blood, serum, sputum, saliva and nasal fluid samples of male nonsmoker and smoker TB patients was found to be lower at 95 % confidence interval {([CI 139–150] μg/g, [4.82–4.97] mg/l, [CI 0.95–1.00] mg/l, [241–248] μg/l, [CI 95.7–104] μg/l, and [142–149] μg/l)} and {([CI 129–142] μg/g, [4.55–4.64] mg/l, [CI 0.89-0.94] mg/l, [227–232] μg/l, [CI 85.7–94.2] μg/l, and [137–142] μg/l)}, respectively, as compared to Zn in scalp hair, blood, serum, sputum, saliva and nasal fluid samples of male smoker and nonsmoker referents {([CI 234–244] μg/g, [5.83–5.97] mg/l, [CI 1.13–1.25] mg/l, [(358–366] μg/l, [CI 134–142] μg/l, and [161–173] μg/l)} and {([CI 189–202] μg/g, [5.47–5.61] mg/l, [CI 1.06–1.17] mg/l, [335–344] μg/l, [CI 125–134] μg/l, and [154–166] μg/l)}, respectively (Table 5).
The Fe concentrations in scalp hair, blood, serum, sputum, saliva and nasal fluid samples of male non smoker and smoker TB patients was found to be lower at 95 % confidence interval {([CI 31.6–34.3] μg/g, [CI 357–372] mg/l, [CI 2.20–2.39] mg/l, [0.92–1.13] μg/l, [CI 0.57-0.63] μg/l, and [CI 0.84- 0.90] μg/l)} and {([CI 29.0–31.5] μg/g, [327–340] mg/l, [CI 2.02–2.19] mg/l, [0.87-0.99] μg/l, [CI 0.51-0.59] μg/l, and [0.77-0.81] μg/l)}, respectively, as compared to Fe in scalp hair, blood, serum, sputum, saliva and nasal fluid samples of male smoker and nonsmoker referents {([CI 39.6–41.8] μg/g, [474–492] mg/l, [CI 3.57–4.21] mg/l, [(1.16–1.55] μg/l, [CI 0.85-0.93] μg/l, and [1.13–1.27] μg/l)} and {([CI 35.17–37.5] μg/g, [436–452] mg/l, [CI 3.32–3.84] mg/l, [1.18–1.36] μg/l, [CI 0.77-0.84] μg/l, and [1.02–1.16] μg/l)}, respectively (Table 5).
The concentrations of Cu in biological samples of biological (scalp hair, blood, serum, sputum, saliva and nasal fluid) samples of nonsmoker and smoker male T.B patients were significantly higher at 95 % C.I. {([CI 20.6–22.3] μg/g, [CI 1.50–1.58] mg/l, [CI 1.10–1.21] mg/l, [CI 796–885] μg/l, [CI 233–265] μg/l and [CI 335–362] μg/l)} and {([CI 18.6–20.3] μg/g, [CI 1.87–1.93] mg/l, [CI 1.01–1.12] mg/l, [CI 749–876] μg/l, [CI 207–240] μg/l and [CI 307–320] μg/l)} compared with those in male healthy nonsmokers and smokers subjects {([CI 14.7–15.8] μg/g, [CI 1.02–1.09] mg/l, [CI 0.77-0.85] mg/l, [CI 558–680] μg/l, [CI 159–185] μg/l and [CI 225–252] μg/l)}and{([CI 12.8–13.5] μg/g, [CI 0.92-0.98] mg/l, [CI 0.67-0.76] mg/l, [CI 513–605] μg/l, [CI 145–163] μg/l and [CI 202–227] μg/l)} (p < 0.01).
An increase in Cu and decrease of Fe and Zn concentrations were observed in the biological samples of pulmonary TB patients of both genders. Moreover, a decrease of Zn/Cu and Fe/ Cu mole ratios in biological samples of smoker and nonsmoker TB patients than healthy subjects was also seen (Table 6).
Table 6.
Zinc/ Copper, Zinc/ iron and Iron/ Copper mole ratio in biological samples (blood, serum, saliva, nasal fluid, sputum, scalp hairs) of smokers and nonsmokers referent and pulmonary Tuberculosis patients of both genders.
| Biological specimens | Non Smokers |
Smokers |
||||||
|---|---|---|---|---|---|---|---|---|
| Male |
Female |
Male |
Female |
|||||
| Referents | T.B patients | Referents | T.B patients | Referents | T.B patients | Referents | T.B patients | |
| Zn/ Cu | ||||||||
| Scalp hairs | 15.18 | 6.508 | 12.5 | 5.52 | 14.246 | 6.812 | 12.665 | 5.76 |
| Blood | 5.41 | 3.112 | 5.051 | 2.74 | 5.666 | 2.352 | 5.163 | 2.79 |
| Serum | 1.43 | 0.814 | 1.16 | 0.659 | 1.498 | 0.851 | 1.235 | 0.66 |
| Sputum | 0.568 | 0.392 | 0.459 | 2.328 | 0.593 | 0.276 | 0.465 | 0.23 |
| Saliva | 0.78 | 0.539 | 0.646 | 0.331 | 0.82 | 0.39 | 0.661 | 0.33 |
| Nasal Fluid | 0.679 | 0.466 | 0.495 | 0.298 | 0.723 | 0.435 | 0.484 | 0.29 |
| Zn/ Fe | ||||||||
| Scalp hairs | 4.9631 | 3.724 | 4.588 | 3.58 | 4.5795 | 3.834 | 4.564 | 3.668 |
| Blood | 0.0104 | 0.011 | 0.01 | 0.011 | 0.0107 | 0.012 | 0.01 | 0.011 |
| Serum | 0.2611 | 0.364 | 0.273 | 0.294 | 0.2656 | 0.372 | 0.287 | 0.289 |
| Sputum | 222.3824 | 303.05 | 209 | 207 | 228.6029 | 211 | 209 | 206 |
| Saliva | 132.4023 | 196.397 | 132 | 135 | 137.0455 | 140 | 133 | 134 |
| Nasal Fluid | 119.8329 | 163.909 | 104 | 114 | 125.343 | 151 | 101 | 109 |
| Fe/ Cu | ||||||||
| Scalp hairs | 3.058 | 1.748 | 2.723 | 1.542 | 3.111 | 1.777 | 2.775 | 1.569 |
| Blood | 0.519 | 0.272 | 0.483 | 0.246 | 0.531 | 0.201 | 0.497 | 0.255 |
| Serum | 0.00547 | 0.00224 | 0.00424 | 0.00224 | 0.00564 | 0.00229 | 0.0043 | 0.00228 |
| Sputum | 0.00256 | 0.00129 | 0.0022 | 0.01127 | 0.00259 | 0.00131 | 0.00223 | 0.00113 |
| Saliva | 0.00589 | 0.00274 | 0.00489 | 0.00246 | 0.00599 | 0.00279 | 0.00496 | 0.0025 |
| Nasal Fluid | 0.00567 | 0.00284 | 0.00474 | 0.00262 | 0.00577 | 0.00287 | 0.00478 | 0.00265 |
4. Discussion
Although many studies have been reported related to trace metals levels in TB patients throughout the world, there is paucity such information in Pakistan. This study is aimed to estimate the essential trace elemental levels, Cu, Fe and Zn, in biological samples of TB patients and controls with smoking and nonsmoking habits in rural areas of Sindh, Pakistan, where malnutrition is common.
Low Zn level reported in TB patients is in concert with reports from Ethiopia, Iran, Italy, Nigeria, Turkey, Indonesia and India respectively [[51], [52], [53], [54], [55]]. The low plasma Zn in TB patients compared with control was probably due to redeployment of Zn from blood circulation to other tissues, reduction in hepatic production of a2-macroglobulin (a Zn carrier protein) or a increase in the manufacture of metallothionein, which is a protein that helps in transportation of Zn to the liver [[56], [57], [58]].
The Zn is involved in antioxidant defense through antioxidant metalloenzyme copper-Zn superoxide dismutase. Particularly, Zn is attached to the oxidative and reductive active sites and avoids the bonds of more damaging metals. Zn also control metallothioneins, which functions in free radical hunt and inflammatory processes [59]. Zinc is necessary for humoral and cellular immunity, and affects the function of adaptive and immune cells [[60], [61], [62]].
The Zn insufficiencies can enhance vulnerability to TB infection and leave individuals susceptible to oxidative stress. Although recent methodological research has suggested that Zn plasma concentrations can be enhanced by supplements during the early stages of treatment, no fixed benefit of supplementation has been demonstrated on outcomes of TB treatment and / or nutritional recovery [63]. Future research is needed to determine the impact of these trace elements on clinical outcomes and also to determine whether the routine management of supplements leads to better TB outcome and / or improved quality of life.
In our study, Zinc was decreased in all TB patients as compared to referents. In case of other lung diseases total elemental zinc levels are exalted in sputum from subjects with CF and non-CF bronchiectasis compared with control subjects. There is a small degree of overlap between cystic fibrosis and control groups, but this can be explained by the discovering that the patients with cystic fibrosis in this small subgroup have a better lung function and thus less severe lung disease (data not shown). Zinc sputum levels were also higher in CF and non-CF bronchiectasis than in chronic obstructive pulmonary disease. Low levels of zinc sputum significantly over the course of worsening cystic fibrosis. Zinc is strongly associated with calprotectin in TV sputum as well as with other inflammatory markers, such as IL-8 and MPO.
Zinc homeostasis may play an important role in modulating the immune response to inflammation, with high concentrations of zinc inducing peripheral blood monocyte apoptosis 26 and promoting cytokine production [64]. Conversely, low concentrations of zinc may suppress monocyte function and decrease neutrophil phagocytosis [65]. Zinc may also interact with the airway epithelium [66,67].
A number of studies depicted the decrease in Fe level in serum of TB patients compared to the healthy subjects [68,69].
This decrease might be explained by increased blood loss from hemoptysis in TB patients or due to the body's defense mechanism to create an iron-scarce environment limiting Mtb growth and expansion. Boelaert et al. 2007 reported that M. tuberculosis multiplication capability inside host macrophages relies on the accessible iron [40], therefore, the iron insufficiency found in TB cases might be because of the mycobacterial iron consumption [70].
Although iron has been reported to play a significant role in myeloperoxidase-dependent generation of hypochlorous acid (a microbicidal factor), there is a need for caution in recommending dietary iron supplementation for TB patients because free iron is used by bacteria for replication. In a perspective study of the relationship between TB and increased dietary iron, increased dietary iron was associated with a 3.5-fold increase in estimated odds of developing active TB and a trend toward higher mortality among TB patients [39]. Thus, giving iron containing supplements to TB patients should be done with caution [71].
Iron is a prerequirement for microbic growth, with greater levels in CF sputum possibly contribute to the propagation of bacteria [72]. The origin of this iron is blurred, with leak from the circulation being suggested, although further work is required to inspect this. Cigarette smoke has also been suggested as a potential source of airways iron [72]. Unlike Zn, and iron, appreciably higher copper levels in serum were noted in PTB patients as compared to referents (Table 5). This finding is comparable with those of previous studies [73,74].
Copper is fundamental for the continued existence of Mycobacterium and is used further in response to infection [51]. It is a significant constituent of immune system in opposition to reactive oxygen species which create in response to TB infection) [52]. Copper is a vital ingredient that enhances immunity against macrophages. It also works to counterbalance oxidative stress. In the current work, Cu was observed greater in PTB relatively in the control group. Our results were supported by other scientists and noted greater Cu levels in the study subjects [52]. The Zn and Cu are the two factors of superoxide dismutase, an enzyme accountable for the synthesis containing hydrogen peroxide. Hydrogen peroxide acts in phagocytosis. Consequently, the insufficiency of Zn and Cu reduces the production of ROS which results in an increase in infection vulnerability and infuriating TB results [51]. Low levels of zinc, which occurs in TB, prevent the entry of copper into the tissues, which leads to a high serum copper level. However, rise in the serum level of certain metals such as Cu or Cd leads to a decrease in iron absorption in the serum in line with our study [75].
Copper is used in several important biochemical processes such as origin of red blood cells and the autoimmune response of the patient, protecting different cellular structures against the action of reactive oxygen species [57,76]. The elevated serum levels of copper may reflect a nonspecific increase in serum concentration of copper-binding protein, ceruloplasmin. In addition, iron and copper are linked by celluloplasmin, which shows the activity of ferroxidase and is suitable for the assessment of free radical activity [25]. It has been reported that maintaining the copper balance, which includes redistribution and packaging, is key to the immune response to TB infection [25].
High serum Cu/Zn ratio has been accounted in patients with TB. Determination of the ratio of copper / zinc is useful in diagnosing many diseases, controlling their transformation, and in reversing the nutritional status of zinc in the human body better than its content in the serum. Elevated copper/Zn ratio was reported in patients with different pathological conditions in others studies [77].
The comparison of essential trace (Cu, Fe and Zn) in referent subjects with reported literature data is presented in Table 7. The concentrations of zinc in scalp hair samples of referent subjects, found in present study, are comparable with Poland, Sudan, Italy, Pakistan and Syria studies [[78], [79], [80], [81], [82]], whilst higher than Ahmad et al., 2011 [83] and Pasha et al., 2010studies [84]. These findings are higher than Suliburska, 2011 study [85]. The concentrations of understudied elements in blood, serum and Sputum samples of referent subjects, found in present study, are comparable with Pakistan, Nigeria, Iran, South Africa and England studies (Khan, 1995; Edem et al., 2015; Lombardo et al., 2012; Pourfallah et al., 2009; Festus et al., 2016; Gray et al., 2010) [51,53,74,[86], [87], [88]].
Table 7.
Comparison of available studies in concentrations of trace elements in biological samples of non exposed healthy participants of different countries.
| Authors et al., Year | Cu | Fe | Zn | --------- | Country |
|---|---|---|---|---|---|
| Scalp hair (μg/g) | |||||
| Wojciak et al 2004 [78] | 10–20 | 10–20 | 160–200 | M&F | Poland |
| Osman 2010 [79] | 12.5 | 217.8 | 200.6 | M | Sudan |
| 11.9 | 313.6 | 228.6 | F | ||
| De Prisco et al., 2010 [80] | 14.23 | 7.7 | 245.59 | M | Italy |
| 14.94 | 6.96 | 188.52 | F | ||
| Suliburska, 2011 [85] | 25.8 ± 19.4 | 22.1 ± 10.5 | 257 ± 87.8 | 19-30 | Poland |
| 17.6 ± 4.15 | 16.8 ± 8.21 | 249 ± 83.9 | 41-50 | Poland | |
| Czerny 2014 [92] | 13.1 ± 3.12 | 14.8 ± 3.06 | 141 ± 32.1 | F | Poland |
| Afridi et al 2011[81] | 12.8 ± 1.0 | 39.8 ± 1.7 | 231 ± 16.7 | M | Pakistan |
| Khuder et al., 2014 [82] | 15.5 | 35.2 | 218 | M | Syria |
| Ahmad et al., 2011 [83] | 18.0 ± 0.55 | 22.8 ± 1.81 | 175 ± 11.5 | F + M | India |
| Pasha et al., 2010 [84] | 21.1 ± 5.73 | 66.3 ± 40.7 | 140.7 ± 79.48 | F + M | Pakistan |
| Blood (mg/l) | |||||
| Khan 1995 [86] | 1.35 | 9.28 | M | Pakistan | |
| 1.38 | 4.35 | F | |||
| Afridi et al., 2011 [81] | 2.2 ± 0.3 1.76-2.57 | 785 ± 817 702- 870 | 8.16 ± 0.83 7.24 - 9.07 | M + F | Pakistan |
| Serum (mg/l) | |||||
| Edem et al., 2015 [51] | 1.05 ± 0.25 | 1.094 ± 0.18 | 0.81 ± 0.22 | Tuberculosis | Nigeria |
| 1.604 ± 0.252 | 1.432 ± 0.59 | 1.483 ± 0.32 | Control | ||
| Lombardo 2011 [87] | 1.666 ± 0.283 | 0.770 ± 0.15 | Control | South Africa | |
| 1.733 ± 0.365 | 0.595 ± 0.11 | Tuberculosis | |||
| Pourfallah et al., 2009 [69] | 1.27 ± 0.134 | 1.43 ± 0.54 | 1.26 ± 0.402 | Control | Iran |
| Festus et al., 2016 [74] | 1.135 ± 0.771 | 1.222 ± 0.204 | Control | Nigeria | |
| 1.348 ± 0.78 | 0.843 ± 0.12 | Subjects M | |||
| 1.35 ± 0.79 | 0.890 ± 0.84 | Subjects F | |||
| Sputum (μg/l) | |||||
| Gray et al 2010 [88] μg/L |
8.6 (3-16.4) | 13.5 (8.6-21.5) | 153.5 (104-256) | Control | England |
| 15.2 (8.6-29.5) | 30.0 (6.9-35.3) | 12.7 (7.2-41.4) | Asthma | ||
| 15.2 (12.2-22) | 21.3 (3.1-35.6) | 25.4 (9.8-50.7) | COPD | ||
| 19.5 (14.5-30.1) | 56.9 (24.3-115.3) | 13.53 (5.42-20.96) | CF | ||
| 15.7 (10.9-33.3) | 54.2 (22.791.6) | 11.13 (4.1-15.07) | Bronchiectasis | ||
| Saliva (μg/l) | |||||
| Liu et al., 2007 [46] | 97.4 ± 33.6 (70-170) | 0.217 ± 0.226 (0.15-0.25) | 31.39 ± 4.49 (23-38) | controls | India |
| Herman et al 2016 [89] | 81.0 ± 29 | 0.688±0.311 | 67.0±58.9 | Male referents | Poland |
| 60 ± 51 | 0.767 ± 0.547 | 46.7±32.1 | Female referents | ||
| Checherita et al., 2016 [90] | 609.3±62.6 | 23.93 ± 8.32 | Controls | Romania | |
| 10.06-47.02 | |||||
| 450.4-740.6 | |||||
The concentrations of zinc in saliva samples of referent subjects, found in present study, are higher than India, Poland, Romania studies [46,89,90](Liu et al., 2007; Herman et al. 2016; Checherita et al., 2016), whilst iron level is comparable with polish study (Herman et al. 2016), whilst higher than Indian study [46] (Liu et al., 2007). The concentration of copper in saliva samples of our referent subjects were found to be lower than Romania study [88] (Checherita et al., 2016), whilst higher than Poland and Indian study [46,87] (Liu et al., 2007; Herman et al. 2016).
In literature, there is no any information about the use of nasal fluid in TB. It is first time probably used for analysis to found any variation in trace essential and toxic metals with respect severity of TB and any changes occur after any treatment. There is a big problem in deciding the accurate constitution of nasal fluid, which explains the reality that there is repeatedly conflict between unlike reports in literature due to unavoidable evaporation of the nasal fluid, the concentration of its components increases over time. Possibly the best assessment of the constitution of nasal fluid is from a sample of nasal fluid directly after a sneeze because this secretion is relatively large and occurs very rapidly, e.g. 0.2 ml in a few seconds (Burke, 2014) [91].
Trace elements including iron (Fe), copper (Cu), and zinc (Zn) have significant role in many biological systems. These elements play a vital role in the protection and development of human tissues and organs. Furthermore, these elements are considered as possible key aspects in various contagious infections [83,92].
Various facts stated that a few transition elements facilitate immune system inhibit microorganisms such as Mycobacterium tuberculosis. The ingestion of toxic elements may lead to pulmonary TB, myocardial infarctions and atherosclerosis related disorders by rising oxidative stress caused by deficiency of an antioxidant element Zinc. Due to the lack of essential nutrients particularly the elements, and homeostatic management or an additional ingestion of various toxic metals may cause chronic illnesses such as hypertension, TB, and cardiovascular disease [93].
Biologically active trace minerals (biotic agents) are essential key factors in a wide range of individual and bacterial enzymes; however, the consistent guideline for their bioavailability is necessary to avoid contamination [[94], [95], [96]]. Some previous studies in chronic bronchitis patients have confirmed higher concentrations of copper in the airway secretions and assumed this mineral may mask the severity of infection. High concentration of copper in the bronchial secretions and assume that copper may manipulate the intensity of infection. The analysis of levels of the elements Fe, Cu, Zn and Cu/Zn may help the studies on the development of TB disease. The enhancement or reduction in the levels of these elements may be linked with typical symptoms of TB [84].
5. Conclusion
Tuberculosis bacillus (TB) is a contagious bacterial disease caused by different types of mycobacterium in humans. When the infection is infected with lung fever, it is called "pulmonary TB". While the infection affects other parts of the body, it is called pulmonary TB. "Patients usually complain of constitutional symptoms (fever, night sweat, weight loss) and local features related to the site of disease. A patient with both pulmonary and extra-pulmonary TB should be classified as a case of pulmonary TB.
The studied elements (Zn, Fe, Cu) were evaluated in scalp hair, whole blood, serum, saliva, sputum and nasal fluid samples of TB patients and referents of age group (16–35) years of both genders along with smoking habit. The concentration of Zn, and Fe, were higher in all the biological samples of non-smokers TB patients as compared to smokers. Compared to the control group, the concentrations of Zn and Fe were significantly lower in TB patients; the decrease in zinc, and Iron in biological samples of patients with TB was possibly persuaded by inflammatory processes contained in these patients. However, the concentration of Cu was considerably greater in all biological samples of TB patients. Cu/Zn ratio was also considerably greater in all biological samples of TB patients as compared to the control group. The analysis of levels of the elements Fe, Cu, Zn and Cu/Zn may help the studies on the development of TB disease. The enhancement or reduction in the levels of these elements may be linked with typical symptoms of TB. Therefore, measurements of trace elements can be used as a tool to assess susceptibility to infection and to signal stage of the inflammatory response.
With evidences obtained from the present study and knowledge acquired, we suggest in future referring this work for evaluation of trace level of other toxic elements that should be followed up and synchronized for general public. Future research is required to determine these trace element levels influence on clinical outcomes and to set up whether routinely providing supplements will result in improved TB treatment outcomes and/or life quality. Smoking habit must be discouraged at every public forum to provide awareness among the public about the association of smoking and higher risk of Pulmonary TB. Awareness programs must be introduced to spread the knowledge about adverse effects of tobacco smoking and their correlations with higher metal intake, through electronic and print media.
Declaration of Competing Interest
The authors declare no conflict of interest.
Acknowledgement
The authors were thankful to National Centre of Excellence in Analytical Chemistry, University of Sindh Jamshoro for financial support for this research work.
Contributor Information
Palwasha Nizamani, Email: palwasha.nizamani@scholar.usindh.edu.pk.
Hassan Imran Afridi, Email: hassan.afridi@usindh.edu.pk.
Tasneem Gul Kazi, Email: tasneem.kazi@usindh.edu.pk.
Farah Naz Talpur, Email: farha.talpur@usindh.edu.pk.
Jameel Ahmed Baig, Email: jameel.baig@usindh.edu.pk.
References
- 1.W. H. Organization . World Health Organization; 2015. Global Tuberculosis Report 2015. [Google Scholar]
- 2.Boloorsaz M.R., Khalilzadeh S., Milanifar A.R., Safavi A., Velayati A.A. Impact of anti-tuberculosis therapy on plasma zinc status in childhood tuberculosis. East. Mediterr. Health J. 2007;13:1078–1084. doi: 10.26719/2007.13.5.1078. [DOI] [PubMed] [Google Scholar]
- 3.Karyadi E., Schultink W., Nelwan R.H., Gross R., Amin Z., Dolmans W.M., van der Meer J.W., Hautvast J.G.J., West C.E. Poor micronutrient status of active pulmonary tuberculosis patients in Indonesia. J. Nutr. 2000;130:2953–2958. doi: 10.1093/jn/130.12.2953. [DOI] [PubMed] [Google Scholar]
- 4.Garner P., Smith H., Munro S., Volmink J. Promoting adherence to tuberculosis treatment. Bul World Health Org. 2007;85:404–406. doi: 10.2471/06.035568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Khan A., Sterling T.R., Reves R., Vernon A., Horsburgh C.R., Consortium T.T. Lack of weight gain and relapse risk in a large tuberculosis treatment trial. Am. J. Respir. Crit. Care. 2006;174:344–348. doi: 10.1164/rccm.200511-1834OC. [DOI] [PubMed] [Google Scholar]
- 6.Khan M.A. Two diseases (TB/HIV) and two medicines (ATT/ART): one patient and one service. South Am J Med. 2015;3:1–11. [Google Scholar]
- 7.Cantwell M.F., Mckenna M.T., Mccray E., Onorato I.M. Tuberculosis and race/ethnicity in the United States: impact of socioeconomic status. Am. J. Respir. Crit. Care. 1998;157:1016–1020. doi: 10.1164/ajrccm.157.4.9704036. [DOI] [PubMed] [Google Scholar]
- 8.Spence D., Hotchkiss J., Williams C., Davies P. Tuberculosis and poverty. BMJ. 1993;307:759–761. doi: 10.1136/bmj.307.6907.759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dye C. Global epidemiology of tuberculosis. Lancet. 2006;367:938–940. doi: 10.1016/S0140-6736(06)68384-0. [DOI] [PubMed] [Google Scholar]
- 10.Diwan V.K., Thorson A. Sex, gender, and tuberculosis. Lancet. 1999;353:1000–1001. doi: 10.1016/S0140-6736(99)01318-5. [DOI] [PubMed] [Google Scholar]
- 11.Kirenga B.J., Ssengooba W., Muwonge C., Nakiyingi L., Kyaligonza S., Kasozi S., Mugabe F., Boeree M., Joloba M., Okwera A. Tuberculosis risk factors among tuberculosis patients in Kampala, Uganda: implications for tuberculosis control. BMC Public Health. 2015;15:13–18. doi: 10.1186/s12889-015-1376-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Udwadia Z., Pinto L. ed. 2011. Why Stop TB Is Incomplete Without Quit SMOKING. [PubMed] [Google Scholar]
- 13.Sharif S., Ranjha N.M., Majeed A., Abbas G., Ajmal M.T., Hassan S., Aftab B., Hussain M., Rehman R.U. Survey of socio-demographic prevalence, risk factors and clinical characterization of tuberculosis in Nishtar Hospital Multan. Pak J Pharma Res. 2016;2:8–14. [Google Scholar]
- 14.Bae J.M., Li Z.M., Shin M.H., Kim D.H., Lee M.S., Ahn Y.O. Pulmonary tuberculosis and lung cancer risk in current smokers: the Seoul Male Cancer cohort Study. J. Korean Med. Sci. 2013;28:896–900. doi: 10.3346/jkms.2013.28.6.896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Memon Z.M., Yilmaz E., Shah A.M., Sahin U., Kazi T.G., Devrajani B.R., Soylak M. Trace elements in blood samples of smoker and nonsmoker active pulmonary tuberculosis patients from Jamshoro, Pakistan. Environ Sci Poll Res. 2017;24:26513–26520. doi: 10.1007/s11356-017-0236-3. [DOI] [PubMed] [Google Scholar]
- 16.Dogar O.F., Shah S.K., Chughtai A.A. E. Qadeer Gender disparity in tuberculosis cases in eastern and western provinces of Pakistan. BMC Infect. Dis. 2012;12:244. doi: 10.1186/1471-2334-12-244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chen H., Du P., Chen J., Hu S., Li S., Liu H. Separation and preconcentration system based on ultrasonic probe-assisted ionic liquid dispersive liquid–liquid microextraction for determination trace amount of chromium (VI) by electrothermal atomic absorption spectrometry. Talanta. 2010;81:176–179. doi: 10.1016/j.talanta.2009.11.054. [DOI] [PubMed] [Google Scholar]
- 18.Pappas R.S. Toxic elements in tobacco and in cigarette smoke: inflammation and sensitization. Metallomics. 2011;3:1181–1198. doi: 10.1039/c1mt00066g. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chiba M., Masironi R. Toxic and trace elements in tobacco and tobacco smoke. Bull. World Health Organ. 1998;70(2):269–275. [PMC free article] [PubMed] [Google Scholar]
- 20.Wang N.X., Cui X.G., Han L., Zhaxi Y., Dawa Z. Change of the trace elements content from cigarettes (tobacco) to its ash and to look at harm of stuck cigarette. Guang Pu Xue Yu Guang Pu Fen Xi. 2007;27:1845–1847. [PubMed] [Google Scholar]
- 21.Serdar M.A., Akin B.S., Razi C., Akin O., Tokgoz S., Kenar L., Aykut O. The correlation between smoking status of family members and concentrations of toxic trace elements in the hair of children. Biol. Trace Elem. Res. 2012;148:11–17. doi: 10.1007/s12011-012-9337-5. [DOI] [PubMed] [Google Scholar]
- 22.Cavallo F., Gerber M., Pujol H., Marubini E., Decarli A., Richardson S., Barbieri A., Costa A. Zinc and copper in breast cancer. A joint study in northern Italy and southern France. Cancer. 1991;67:738–745. doi: 10.1002/1097-0142(19910201)67:3<738::aid-cncr2820670335>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- 23.Schneider J.M., Fujii M.L., Lamp C.L., Lonnerdal B., Zidenberg-Cherr S. The prevalence of low serum zinc and copper levels and dietary habits associated with serum zinc and copper in 12-to 36-month-old children from low-income families at risk for iron deficiency. J. Am. Diet. Assoc. 2007;107:1924–1929. doi: 10.1016/j.jada.2007.08.011. [DOI] [PubMed] [Google Scholar]
- 24.Balogh E., Tolnai E., Nagy B., Jr., Nagy B., Balla G., Balla J., Jeney V. Iron overload inhibits osteogenic commitment and differentiation of mesenchymal stem cells via the induction of ferritin. Biochim. Biophys. Acta. 2016;1862:1640–1649. doi: 10.1016/j.bbadis.2016.06.003. [DOI] [PubMed] [Google Scholar]
- 25.Neyrolles O., Mintz E., Catty P. Zinc and copper toxicity in host defense against pathogens: mycobacterium tuberculosis as a model example of an emerging paradigm. Front. Cell. Infect. Microbiol. 2013;3:89. doi: 10.3389/fcimb.2013.00089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Stokowa-Sołtys K., Barbosa N.A., Kasprowicz A., Wieczorek R., Gaggelli N., Gaggelli E., Valensin G., Wrzesinski J., Ciesiolka J., Kulinski T. Studies of viomycin, an anti-tuberculosis antibiotic: copper (ii) coordination, DNA degradation and the impact on delta ribozyme cleavage activity. Dalton Trans. 2016;45:8645–8658. doi: 10.1039/c6dt00245e. [DOI] [PubMed] [Google Scholar]
- 27.Nawrot T., Thijs L., Den Hond E., Roels H., Staessen J.A. An epidemiological re-appraisal of the association between blood pressure and blood lead: a meta-analysis. J. Hum. Hypertens. 2002;16:123. doi: 10.1038/sj.jhh.1001300. [DOI] [PubMed] [Google Scholar]
- 28.Witte K.K., Nikitin N.P., Parker A.C., von Haehling S., Volk H.D., Anker S.D., Clark A.L., Cleland J.G. The effect of micronutrient supplementation on quality-of-life and left ventricular function in elderly patients with chronic heart failure. Eur. Heart J. 2005;26:2238–2244. doi: 10.1093/eurheartj/ehi442. [DOI] [PubMed] [Google Scholar]
- 29.Kazi T.G., Memon A.R., Afridi H.I., Jamali M.K., Arain M.B., Jalbani N., Sarfraz A. Determination of cadmium in whole blood and scalp hair samples of Pakistani male lung cancer patients by electrothermal atomic absorption spectrometer. Sci. Total Environ. 2008;389:270–276. doi: 10.1016/j.scitotenv.2007.08.055. [DOI] [PubMed] [Google Scholar]
- 30.Classen H., Grober U., Low D., Schmidt J., Stracke H. Zinc deficiency. Symptoms, causes, diagnosis and therapy. Med. Monatsschr. Pharm. 2011;34:87–95. [PubMed] [Google Scholar]
- 31.Biljana E., Boris V., Cena D., Veleska-Stefkovska D. Matrix metalloproteinases (with accent to collagenases) J Cell Anim Biol. 2011;5:113–120. [Google Scholar]
- 32.Botella H., Peyron P., Levillain F., Poincloux R., Poquet Y., Brandli I., Wang C., Tailleux L., Tilleul S., Charrière G.M. Mycobacterial P1-type ATPases mediate resistance to zinc poisoning in human macrophages. Cell Host Microbe. 2011;10:248–259. doi: 10.1016/j.chom.2011.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Stensland I., Kim J., Bowring B., Collins A., Mansfield J., Pluske J. A comparison of diets supplemented with a feed additive containing organic acids, cinnamaldehyde and a permeabilizing complex, or zinc oxide, on post-weaning diarrhoea, selected bacterial populations, blood measures and performance in weaned pigs experimentally infected with enterotoxigenic E. Coli. Animals. 2015;5:1147–1168. doi: 10.3390/ani5040403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Osman D., Piergentili C., Chen J., Chakrabarti B., Foster A.W., Lurie-Luke E., Huggins T.G., Robinson N.J. Generating a metal-responsive transcriptional regulator to test what confers metal-sensing in cells. J Biol Chem M115. 2015 doi: 10.1074/jbc.M115.663427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hennig B., Meerarani P., Toborek M., McClain C.J. Antioxidant-like properties of zinc in activated endothelial cells. Am Coll Nutr. 1999;18:152–158. doi: 10.1080/07315724.1999.10718843. [DOI] [PubMed] [Google Scholar]
- 36.Weinberg E.D. Iron loading and disease surveillance. Emerg Infect Dis. 1999;5:346. doi: 10.3201/eid0503.990305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Litwin C.M., Calderwood S. Role of iron in regulation of virulence genes. Clin. Microbiol. Rev. 1993;6:137–149. doi: 10.1128/cmr.6.2.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Doherty C.P. Host-pathogen interactions: the role of iron. J. Nutr. 2007;137:1341–1344. doi: 10.1093/jn/137.5.1341. [DOI] [PubMed] [Google Scholar]
- 39.Gangaidzo I.T., Moyo V.M., Mvundura E., Aggrey G., Murphree N.L., Khumalo H., Saungweme T., Kasvosve I., Gomo Z.A., Rouault T. Association of pulmonary tuberculosis with increased dietary iron. J. Infect. Dis. 2001;184:936–939. doi: 10.1086/323203. [DOI] [PubMed] [Google Scholar]
- 40.Boelaert J.R., Vandecasteele S.J., Appelberg R., Gordeuk V.R. The effect of the host’s iron status on tuberculosis. J. Infect. Dis. 2007;195:1745–1753. doi: 10.1086/518040. [DOI] [PubMed] [Google Scholar]
- 41.Patel S.J., Lewis B.E., Long J.E., Nambi S., Sassetti C.M., Stemmler T.L., Arguello J.M. Fine tuning of substrate affinity leads to alternative roles of Mycobacterium tuberculosis Fe2+-ATPases. J. Biol. Chem. 2016;116 doi: 10.1074/jbc.M116.718239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.(a) Meneghetti F., Villa S., Gelain A., Barlocco D., Chiarelli L.R., Pasca M.R., Costantino L. Iron acquisition pathways as targets for antitubercular drugs. Curr. Med. Chem. 2016;23:4009–4026. doi: 10.2174/0929867323666160607223747. [DOI] [PubMed] [Google Scholar]; (b) Olivares M., Uauy R. Copper as an essential nutrient. Am. J. Clin. Nutr. 1996;63:791S–796S. doi: 10.1093/ajcn/63.5.791. [DOI] [PubMed] [Google Scholar]
- 43.Bonham M., O’Connor J.M., Hannigan B.M., Strain J. The immune system as a physiological indicator of marginal copper status? Br. J. Nutr. 2002;87:393–403. doi: 10.1079/BJNBJN2002558. [DOI] [PubMed] [Google Scholar]
- 44.Wintergerst E.S., Maggini S., Hornig D.H. Contribution of selected vitamins and trace elements to immune function. Ann. Nutr. Metab. 2007;51:301–323. doi: 10.1159/000107673. [DOI] [PubMed] [Google Scholar]
- 45.Grammer T., Kleber M., Silbernagel G., Pilz S., Scharnagl H., Lerchbaum E., Tomaschitz A., Koenig W., Marz W. Copper, ceruloplasmin, and long-term cardiovascular and total mortality (the Ludwigshafen Risk and Cardiovascular Health Study) Free Radic. Res. 2014;48:706–715. doi: 10.3109/10715762.2014.901510. [DOI] [PubMed] [Google Scholar]
- 46.Liu T., Ramesh A., Ma Z., Ward S.K., Zhang L., George G.N., Talaat A.M., Sacchettini J.C., Giedroc D.P. CsoR is a novel Mycobacterium tuberculosis copper-sensing transcriptional regulator. Nat. Chem. Biol. 2007;3:60. doi: 10.1038/nchembio844. [DOI] [PubMed] [Google Scholar]
- 47.Divrikli U., Horzum N., Soylak M. Trace heavy metal contents of some spices and herbal plants from western Anatolia, Turkey. Int J Food Sci Tech. 2006;41:712–716. [Google Scholar]
- 48.Saraymen R., Soylak M., Narin I. Serum cadmium levels of people living in Kayseri-Belsin region, Turkey. Fresen Environ Bull. 1998;7:403–405. [Google Scholar]
- 49.Soylak M., Saracoglu S., Divrikli U. Copper and zinc concentrations of serum samples of healthy people living in Tokat, Turkey. Trace Elem. Electrolytes. 2001;18:47–50. [Google Scholar]
- 50.Behbahani M., Tapeh N.A., Mahyari M., Pourali A.R., Amin B.G., Shaabani A. Monitoring of trace amounts of heavy metals in different food and water samples by flame atomic absorption spectrophotometer after preconcentration by amine-functionalized graphene nanosheet. Environ. Monit. Assess. 2014;186:7245–7257. doi: 10.1007/s10661-014-3924-1. [DOI] [PubMed] [Google Scholar]
- 51.Edem V., Ige O., Arinola O. Plasma vitamins and essential trace elements in newly diagnosed pulmonary tuberculosis patients and at different durations of anti-tuberculosis chemotherapy. Egypt. J. Chest Dis. Tuberc. 2015;64:675–679. [Google Scholar]
- 52.Bozan N., Dinç M.E., Demir H., Yalınkılıç A., Gönüllü E., Turan M., Demir C., Arslan A., Özkan H., Kundi P. Serum trace elements and heavy metal levels in patients diagnosed with chronic otitis media and their association with surgical treatment outcomes. J. Int. Adv. Otol. 2017;13:345–348. doi: 10.5152/iao.2017.3617. [DOI] [PubMed] [Google Scholar]
- 53.Pourfallah F., Javadian S., Zamani Z., Saghiri R., Sadeghi S., Zarea B., Faiaz S., Mirkhani F., Fatemi N. Evaluation of serum levels of zinc, copper, iron, and zinc/copper ratio in cutaneous leishmaniasis. Iran J Arthropod Borne Dis, 3, 7.Ratledge, C., 2004. Iron, mycobacteria and tuberculosis. Tuberculosis. 2009;84:110–130. 2004. [PMC free article] [PubMed] [Google Scholar]
- 54.Cernat R., Mihaescu T., Vornicu M., Vione D., Olariu R., Arsene C. Serum trace metal and ceruloplasmin variability in individuals treated for pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2011;15:1239–1245. doi: 10.5588/ijtld.10.0445. [DOI] [PubMed] [Google Scholar]
- 55.Rohini K., Srikumar P., Jyoti S., Mahesh K. Alteration in the levels of serum micronutrients in tuberculosis patients. Int. J. Biol. Med. Res. 2013;4:2958–2961. [Google Scholar]
- 56.Ciftci T.U., Ciftci B., Yis O., Guney Y., Bilgihan A., Ogretensoy M. Changes in serum selenium, copper, zinc levels and Cu/Zn ratio in patients with pulmonary tuberculosis during therapy. Biol. Trace Elem. Res. 2003;95:65–71. doi: 10.1385/BTER:95:1:65. [DOI] [PubMed] [Google Scholar]
- 57.Kassu A., Yabutani T., Mahmud Z., Mohammad A., Nguyen N., Huong B., Hailemariam G., Diro E., Ayele B., Wondmikun Y. Alterations in serum levels of trace elements in tuberculosis and HIV infections. Eur. J. Clin. Nutr. 2006;60:580. doi: 10.1038/sj.ejcn.1602352. [DOI] [PubMed] [Google Scholar]
- 58.Koyanagi A., Kuffo D., Gresely L., Shenkin A., Cuevas L. Relationships between serum concentrations of C-reactive protein and micronutrients, in patients with tuberculosis. Ann. Trop. Med. Parasitol. 2004;98:391–399. doi: 10.1179/000349804225003424. [DOI] [PubMed] [Google Scholar]
- 59.Formigari A., Irato P., Santon A. Zinc, antioxidant systems and metallothionein in metal mediated-apoptosis: biochemical and cytochemical aspects. Comp. Biochem. Physiol. C Toxicol. Pharmacol. 2007;146:443–459. doi: 10.1016/j.cbpc.2007.07.010. [DOI] [PubMed] [Google Scholar]
- 60.Steinbrenner H., Al-Quraishy S., Dkhil M.A., Wunderlich F., Sies H. Dietary selenium in adjuvant therapy of viral and bacterial infections. Adv. Nutr. 2015;6:73–82. doi: 10.3945/an.114.007575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Arthur J.R., McKenzie R.C., Beckett G.J. Selenium in the immune system. J. Nutr. 2003;133:1457S–1459S. doi: 10.1093/jn/133.5.1457S. [DOI] [PubMed] [Google Scholar]
- 62.Bonaventura P., Benedetti G., Albarède F., Miossec P. Zinc and its role in immunity and inflammation. Autoimmun. Rev. 2015;14:277–285. doi: 10.1016/j.autrev.2014.11.008. [DOI] [PubMed] [Google Scholar]
- 63.Sinclair D., Abba K., Sudarsanam T.D., Grobler L., Volmink J. Nutritional supplements for people being treated for active tuberculosis. Cochrane Database Syst. Rev. 2011;11 doi: 10.1002/14651858.CD006086.pub3. [DOI] [PubMed] [Google Scholar]
- 64.Driessen C., Hirv K., Rink L., Kirchner H. Induction of cytokines by zinc ions in human peripheral blood mononuclear cells and separated monocytes. Lymphokine Cytokine Res. 1994;13:15–20. [PubMed] [Google Scholar]
- 65.Ibs K.H., Rink L. Zinc-altered immune function. J. Nutr. 2003;133:1452S–1456S. doi: 10.1093/jn/133.5.1452S. [DOI] [PubMed] [Google Scholar]
- 66.Zalewski P.D., Truong-Tran A.Q., Grosser D., Jayaram L., Murgia C., Ruffin R.E. Zinc metabolism in airway epithelium and airway inflammation: basic mechanisms and clinical targets. A review. Pharmacol. Ther. 2005;105:127–149. doi: 10.1016/j.pharmthera.2004.09.004. [DOI] [PubMed] [Google Scholar]
- 67.Zalewski P.D. Zinc metabolism in the airway: basic mechanisms and drug targets. Curr. Opin. Pharmacol. 2006;6:237–243. doi: 10.1016/j.coph.2006.01.005. [DOI] [PubMed] [Google Scholar]
- 68.Van Lettow M., Kumwenda J., Harries A., Whalen C., Taha T., Kumwenda N., Kangombe C., Semba R.D. Malnutrition and the severity of lung disease in adults with pulmonary tuberculosis in Malawi. Int. J. Tuberc. Lung Dis. 2004;8:211–217. [PubMed] [Google Scholar]
- 69.Pourfallah F., Javadian S., Zamani Z., Saghiri R., Sadeghi S., Zarea B., Faiaz S., Mirkhani F., Fatemi N. Evaluation of serum levels of zinc, copper, iron, and zinc/copper ratio in cutaneous leishmaniasis. Iran. J. Arthropod. Dis. 2009;3:7. [PMC free article] [PubMed] [Google Scholar]
- 70.Brahmer J.R., Tykodi S.S., Chow L.Q., Hwu W.J., Topalian S.L., Hwu P., Drake C.G., Camacho L.H., Kauh J., Odunsi K. Safety and activity of anti–PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012;366:2455–2465. doi: 10.1056/NEJMoa1200694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.McDermid J.M., Prentice A.M. Iron and infection: effects of host iron status and the iron-regulatory genes haptoglobin and NRAMP1 (SLC11A1) on host–pathogen interactions in tuberculosis and HIV. Clin. Sci. 2006;110:503–524. doi: 10.1042/CS20050273. [DOI] [PubMed] [Google Scholar]
- 72.Nelson M.E., O’Brien-Ladner A.R., Wesselius L.J. Regional variation in iron and iron-binding proteins within the lungs of smokers. Am. J. Respir. Crit. Care Med. 1996;153:1353–1358. doi: 10.1164/ajrccm.153.4.8616566. [DOI] [PubMed] [Google Scholar]
- 73.De Moraes M.L., de Paula Ramalho D.M., Delogo K.N., Miranda P.F.C., Mesquita E.D.D., Netto A.R., dos Anjos M.J., Kritski A.L., de Oliveira M.M. Association of serum levels of iron, copper, and zinc, and inflammatory markers with bacteriological sputum conversion during tuberculosis treatment. Biol. Trace Elem. Res. 2014;160:176–184. doi: 10.1007/s12011-014-0046-0. [DOI] [PubMed] [Google Scholar]
- 74.Festus O., Omon E., Dada F., Iweka F. Evaluation of some trace elements (copper, selenium, iron, and lead) in patients with active tuberculosis attending central hospital Benin city, Edo State. Eur. J. Pharm. Med. Res. 2016;3(9):37–43. [Google Scholar]
- 75.Wolschendorf F., Ackart D., Shrestha T.B., Hascall-Dove L., Nolan S., Lamichhane G., Wang Y., Bossmann S.H., Basaraba R.J., Niederweis M. Copper resistance is essential for virulence of Mycobacterium tuberculosis. Proc Natl Acad Sci. 2011;108:1621–1626. doi: 10.1073/pnas.1009261108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Valko M., Morris H., Cronin M. Metals, toxicity and oxidative stress. Curr. Med. Chem. 2005;12:1161–1208. doi: 10.2174/0929867053764635. [DOI] [PubMed] [Google Scholar]
- 77.Lin C.C., Huang J.F., Tsai L.Y., Huang Y.L. Selenium, iron, copper, and zinc levels and copper-to-zinc ratios in serum of patients at different stages of viral hepatic diseases. Biol. Trace Elem. Res. 2006;109:15–23. doi: 10.1385/BTER:109:1:015. [DOI] [PubMed] [Google Scholar]
- 78.Wojciak R., Krejpcio Z., Czlapka-Matyasik M., Jeszka J. Comparison of the hair bioelements in vegeterian and non-vegeterian women. Trace Elem. Electrolytes Health Dis. 2004;21:141–144. [Google Scholar]
- 79.Osman O. Sudan Academy of Sciences; 2010. Investigation of Selected Trace Elements in Hair Samples of Eczema Patients. Thesis of Master of Science in Analytical Chemistry. [Google Scholar]
- 80.De Prisco P.P., Volpe M.G., Petitto F., Palladino C., Saturnino C., Capasso A., Di Stasio M., De Prisco R. Level of essential and toxic metals in urban adolescents hair: preliminary study. Biomed. Res. 2010;21:126–130. [Google Scholar]
- 81.Afridi H.I., Kazi T.G., Kazi N., Kandhro G.A., Baig J.A., Shah A.Q., Khan S., Kolachi N.F., Wadhwa S.K., Shah F. Evaluation of zinc, copper and iron in biological samples (scalp hair, blood and urine) of tuberculosis and diarrhea male human immunodeficiency virus patients. Clin. Lab. 2011;57:677–688. [PubMed] [Google Scholar]
- 82.Khuder A., Bakir M.A., Hasan R., Mohammad A., Habil K. Trace elements in scalp hair of leukaemia patients. Nukleonika. 2014;59:111–120. [Google Scholar]
- 83.Ahmad I., Srivastava V., Prasad R., Yusuf M., Saleem M. Deficiency of micronutrient status in pulmonary tuberculosis patients in North India. Biomed. Res. 2011;22:449–459. [Google Scholar]
- 84.Pasha Q., Malik S.A., Shaheen N., Shah M.H. Investigation of trace metals in the blood plasma and scalp hair of gastrointestinal cancer patients in comparison with controls. Clin. Chim. Acta. 2010;411:531–539. doi: 10.1016/j.cca.2010.01.010. [DOI] [PubMed] [Google Scholar]
- 85.Suliburska J. A comparison of levels of select minerals in scalp hair samples with estimated dietary intakes of these minerals in women of reproductive age. Biol. Trace Elem. Res. 2011;144:77–85. doi: 10.1007/s12011-011-9034-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Khan K. Setting health care priorities in Pakistan. J Pak Med Assoc. 1995;45:222–227. [PubMed] [Google Scholar]
- 87.Lombardo C.C. The nutritional status of patients with tuberculosis in comparison with tuberculosis-free contacts in Delft, Western Cape. South Afr. J. Clin. Nutr. 2012;25:180–181. [Google Scholar]
- 88.Gray R.D., Duncan A., Noble D., Imrie M., O’Reilly D.S.J., Innes J.A., Porteous D.J., Greening A.P., Boyd A.C. Sputum trace metals are biomarkers of inflammatory and suppurative lung disease. Chest. 2010;137:635–641. doi: 10.1378/chest.09-1047. [DOI] [PubMed] [Google Scholar]
- 89.Herman M., Golasik M., Piekoszewski W., Walas S., Napierala M., Wyganowska-Swiatkowska M., Kurhanska-Flisykowska A., Wozniak A., Florek E. Essential and toxic metals in oral fluid–a potential role in the diagnosis of periodontal diseases. Biol. Trace Elem. Res. 2016;173:275–282. doi: 10.1007/s12011-016-0660-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Checherita E., Trandafir D., Stamatin O., Carausu E.M. Study of biochemical levels in serum and saliva of zinc and copper in patients with stomatognathic system dysfunctional syndrome following bone injury and prosthetical treatment. Revista de Chimie. 2016;67:1628–1632. [Google Scholar]
- 91.Burke W. The ionic composition of nasal fluid and its function. Health. 2014;6:720. [Google Scholar]
- 92.Pfaender S., Fohr K., Lutz A.K., Putz S., Achberger K., Linta L., Liebau S., Boeckers T.M., Grabrucker A.M. Cellular zinc homeostasis contributes to neuronal differentiation in human induced pluripotent stem cells. Neural Plast. 2016 doi: 10.1155/2016/3760702. 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Czerny B., Krupka K., Ożarowski M., Seremak-Mrozikiewicz A. Screening of trace elements in hair of the female population with different types of cancers in Wielkopolska region of Poland. Transfus. Apher. Sci. 2014;953181:15. doi: 10.1155/2014/953181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Kamal R., Srivastava A.K., Kesavachandran C.N. Meta-analysis approach to study the prevalence of chronic obstructive pulmonary disease among current, former and non-smokers. Toxicol. Rep. 2015;2:1064–1074. doi: 10.1016/j.toxrep.2015.07.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Toure A., Cabral M., Niang A., Diop C., Garat A., Humbert L., Fall M., Diouf A., Broly F., Lhermitte M., Allorge D. Prevention of isoniazid toxicity by NAT2 genotyping in Senegalese tuberculosis patients. Toxicol. Rep. 2016;3:826–831. doi: 10.1016/j.toxrep.2016.10.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Hamza R.Z., El-Shenawy N.S. Anti-inflammatory and antioxidant role of resveratrol on nicotine-induced lung changes in male rats. Toxicol. Rep. 2017;4:399–407. doi: 10.1016/j.toxrep.2017.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]