

Abstract
Background
Children who are securely attached to at least one parent are able to be comforted by that parent when they are distressed and explore the world confidently by using that parent as a 'secure base'. Research suggests that a secure attachment enables children to function better across all aspects of their development. Promoting secure attachment, therefore, is a goal of many early interventions. Attachment is mediated through parental sensitivity to signals of distress from the child. One means of improving parental sensitivity is through video feedback, which involves showing a parent brief moments of their interaction with their child, to strengthen their sensitivity and responsiveness to their child's signals.
Objectives
To assess the effects of video feedback on parental sensitivity and attachment security in children aged under five years who are at risk for poor attachment outcomes.
Search methods
In November 2018 we searched CENTRAL, MEDLINE, Embase, CINAHL, PsycINFO, nine other databases and two trials registers. We also handsearched the reference lists of included studies, relevant systematic reviews, and several relevant websites
Selection criteria
Randomised controlled trials (RCTs) and quasi‐RCTs that assessed the effects of video feedback versus no treatment, inactive alternative intervention, or treatment as usual for parental sensitivity, parental reflective functioning, attachment security and adverse effects in children aged from birth to four years 11 months.
Data collection and analysis
We used standard methodological procedures expected by Cochrane.
Main results
This review includes 22 studies from seven countries in Europe and two countries in North America, with a total of 1889 randomised parent‐child dyads or family units. Interventions targeted parents of children aged under five years, experiencing a wide range of difficulties (such as deafness or prematurity), or facing challenges that put them at risk of attachment issues (for example, parental depression). Nearly all studies reported some form of external funding, from a charitable organisation (n = 7) or public body, or both (n = 18).
We considered most studies as being at low or unclear risk of bias across the majority of domains, with the exception of blinding of participants and personnel, where we assessed all studies as being at high risk of performance bias. For outcomes where self‐report measures were used, such as parental stress and anxiety, we rated all studies at high risk of bias for blinding of outcome assessors.
Parental sensitivity. A meta‐analysis of 20 studies (1757 parent‐child dyads) reported evidence of that video feedback improved parental sensitivity compared with a control or no intervention from postintervention to six months' follow‐up (standardised mean difference (SMD) 0.34, 95% confidence interval (CI) 0.20 to 0.49, moderate‐certainty evidence). The size of the observed impact compares favourably to other, similar interventions.
Parental reflective functioning. No studies reported this outcome.
Attachment security. A meta‐analysis of two studies (166 parent‐child dyads) indicated that video feedback increased the odds of being securely attached, measured using the Strange Situation Procedure, at postintervention (odds ratio 3.04, 95% CI 1.39 to 6.67, very low‐certainty evidence). A second meta‐analysis of two studies (131 parent‐child dyads) that assessed attachment security using a different measure (Attachment Q‐sort) found no effect of video feedback compared with the comparator groups (SMD 0.02, 95% CI −0.33 to 0.38, very low‐certainty evidence).
Adverse events. Eight studies (537 parent‐child dyads) contributed data at postintervention or short‐term follow‐up to a meta‐analysis of parental stress, and two studies (311 parent‐child dyads) contributed short‐term follow‐up data to a meta‐analysis of parental anxiety. There was no difference between intervention and comparator groups for either outcome. For parental stress the SMD between video feedback and control was −0.09 (95% CI −0.26 to 0.09, low‐certainty evidence), while for parental anxiety the SMD was −0.28 (95% CI −0.87 to 0.31, very low‐certainty evidence).
Child behaviour. A meta‐analysis of two studies (119 parent‐child dyads) at long‐term follow‐up found no evidence of the effectiveness of video feedback on child behaviour (SMD 0.04, 95% CI −0.33 to 0.42, very low‐certainty evidence).
A moderator analysis found no evidence of an effect for the three prespecified variables (intervention type, number of feedback sessions and participating carer) when jointly tested. However, parent gender (both parents versus only mothers or only fathers) potentially has a statistically significant negative moderation effect, though only at α (alpha) = 0.1
Authors' conclusions
There is moderate‐certainty evidence that video feedback may improve sensitivity in parents of children who are at risk for poor attachment outcomes due to a range of difficulties. There is currently only little, very low‐certainty evidence regarding the impact of video feedback on attachment security, compared with control: results differed based on the type of measure used, and follow‐up was limited in duration. There is no evidence that video feedback has an impact on parental stress or anxiety (low‐ and very low‐certainty evidence, respectively). Further evidence is needed regarding the longer‐term impact of video feedback on attachment and more distal outcomes such as children's behaviour (very low‐certainty evidence). Further research is needed on the impact of video‐feedback on paternal sensitivity and parental reflective functioning, as no study measured these outcomes. This review is limited by the fact that the majority of included parents were mothers.
Plain language summary
Video feedback for parental sensitivity and child attachment
Background
Children who are securely attached to at least one parent are able to be comforted by that parent when they are distressed and more able to explore the world confidently by using that parent as a 'secure base'. Research suggests that a secure attachment enables children to function better across all aspects of their development. Promoting secure attachment, therefore, is a goal of many programmes that aim to support children and families in the first few years of the child's life. Video feedback involves showing a parent brief moments of videotaped interaction between them and their baby, in order to strengthen their sensitivity to signals from their baby, with the aim of improving attachment.
Review question
To assess the effects of video feedback on parental sensitivity and attachment security in children under five years old who are at risk of poor outcomes, compared to no intervention (no treatment), a mock treatment (such as a phone call) or treatment as usual.
Included studies
This review included 22 studies, made up of 1889 randomised parent‐child pairs or family units. Not all of these could be combined in a meta‐analysis (a statistical method of combining data from several studies to reach a single, more robust conclusion). We combined data from 20 studies (made up of 1757 parent‐child pairs) to examine the effects of video feedback on parental sensitivity. We combined data from fewer studies to look at attachment security, parental stress, parental anxiety and child behaviour.
The included studies were mostly conducted in Canada, the Netherlands, UK and USA. Single studies were conducted in Italy, Germany, Lithuania, Norway and Portugal.
Almost all studies reported some form of external funding, from either a charitable organisation (n = 7) and/or public body (n = 18).
Results
The results show evidence of an improvement in parental sensitivity following the use of video feedback. The results for attachment security were mixed: one meta‐analysis showed that the intervention group were more securely attached, while the second meta‐analysis, which measured the strength of attachment in a different way, showed no evidence of impact. There was no evidence of impact on parental anxiety or stress. No studies measured parental reflective functioning. There was no evidence of impact on child behaviour.
Study certainty
We rated the overall certainty of the evidence (the extent to which we believe that the results are correct or adequate) as moderate for parental sensitivity, and low or very low for the other outcomes. This means that we are reasonably certain that video feedback improves parental sensitivity in the short term, but we are not very certain of its impact on our other findings.
Authors' conclusions
Video feedback may be a helpful method of improving parental sensitivity, but there is currently little or no evidence that it improves child attachment security, parental stress, parental anxiety or child behaviour. More research is needed on the effects of video feedback on other outcomes, including parental reflective functioning, and in fathers.
Summary of findings
Summary of findings for the main comparison. Video feedback versus no intervention or inactive alternative intervention for parental sensitivity and attachment.
| Video feedback versus no intervention or inactive alternative intervention for parental sensitivity and attachment | ||||||
| Patient or population: parent‐child dyads (including foster or adoptive carers), where the child was aged between birth and four years 11 months (inclusive), and where problems had been identified that were impacting or might impact on the parent's sensitivity Setting: community, hospital outpatient and hospital inpatient Intervention: video feedback Comparison: no intervention or inactive alternative intervention | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with no intervention or inactive alternative intervention | Risk with video feedback | |||||
|
Parental sensitivity Follow‐up: postintervention or short‐term follow‐up |
‐ | The mean parental sensitivity score in the intervention group was 0.34 standard deviations higher (0.20 higher to 0.49 higher) | ‐ | 1757 dyads (20 RCTs) |
⊕⊕⊕⊝ Moderatea | Higher scores indicate a better outcome. Effect size of 0.33 standard deviations compares favourably to other similar interventions. |
| Parental reflective functioning | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
|
Attachment security Measured by: Strange Situation Procedure (odds of being securely attached) Follow‐up: postintervention |
Study population | OR 3.04 (1.39 to 6.67) | 166 dyads (2 RCTs) |
⊕⊝⊝⊝ Very lowb,c,d | Higher scores indicate a better outcome. | |
| 341 per 1000 | 612 per 1000 (419 to 776) | |||||
|
Attachment security Measured by: Attachment Q‐sort Follow‐up: postintervention |
The mean attachment security score across control groups ranged from 0.33 to 0.37 (scores can range from + 1.00 to −1.00) | The mean attachment security score in the intervention group was0.02 standard deviations higher (0.33 lower to 0.38 higher) | ‐ | 131 dyads (2 RCTs) | ⊕⊝⊝⊝ Very lowb,c,d | Effect size of 0.02 standard deviations indicates no evidence of effectiveness. |
|
Adverse events: parental stress Follow‐up: postintervention or short term |
‐ | The mean parental stress score in the intervention group was 0.09 standard deviations lower (0.26 lower to 0.09 higher) | ‐ | 537 dyads (8 RCTs) |
⊕⊕⊝⊝ Lowb,c | Higher scores indicate a worse outcome. Effect size of 0.09 standard deviations indicates no evidence of effectiveness. |
|
Adverse events: parental anxiety Follow‐up: short term |
‐ | The mean parental anxiety score in the intervention group was0.28 standard deviations lower (0.87 lower to 0.31 higher) | ‐ | 311 dyads (2 RCTs) |
⊕⊝⊝⊝ Very lowc,d,e | Higher scores indicate a worse outcome. Effect size of 0.28 compares favourably to other similar interventions. |
|
Child behaviour Follow‐up: long term |
‐ | The mean child behaviour score in the intervention group was 0.04 standard deviations higher (0.33 lower to 0.42 higher) | ‐ | 119 dyads (2 RCTs) |
⊕⊝⊝⊝ Very lowb,c,d | Higher scores indicate a worse outcome. Effect size of 0.04 standard deviations indicates no evidence of effectiveness. |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded one level due to inconsistency: moderate heterogeneity, which was not explained by our subgroup analysis. bDowngraded one level for risk of bias: we rated most domains in the 'Risk of bias' assessment at high or uncertain risk of bias. cDowngraded one level due to imprecision: low number of participants, leading to wide confidence interval. dDowngraded one level due to publication bias: few studies in this review reported this outcome. eDowngraded one level due to inconsistency: high heterogeneity.
Background
Description of the condition
Attachment
A child’s relationship with his or her primary carer is the first, and arguably the most important, relationship formed following birth. The primary carer is normally, but not always, the child's birth mother or father. This emotional bond between a child and their primary caregiver is known as a 'selective attachment' relationship. Attachment is a biobehavioural system that has evolved over time. It is intended to bring about protection in the face of both perceived danger as well as the fear that comes with it (Bowlby 1969). When a child is distressed, he or she is programmed to seek and secure proximity to, and contact with, the primary caregiver (Bowlby 1969). Attachment behaviour may be activated by circumstances internal to the child such as illness, hunger or pain; by separation from the primary caregiver such as when a mother leaves the room or discourages proximity; or by external events that cause distress such as frightening events or rejection by others (Bowlby 1969). Depending on the intensity of the threat, the attachment behaviour may be terminated by the appearance of the caregiver or physical contact with them. The younger the child, or the more serious the threat, the more likely that only physical reassurance and containment will provide comfort. The attachment relationship, therefore, is a dynamic one, in which the child plays an active part (see Shin 2008). It has been described by Zeanah and colleagues as a reciprocal relationship of seeker (child) and provider (parent), the purpose of which is to comfort children when they are upset, support the development of emotional regulation, and offer security (Zeanah 1993).
Children whose caregivers provide sensitive and responsive care develop secure attachments to those carers. Children who experience insensitive, unpredictable or intrusive parenting develop attachments that are insecure, putting them at risk of adverse consequences for a range of aspects of their psychosocial development, including being more reliant on teachers; showing less positive affective expression and impaired social problem‐solving skills; showing more frustration and less persistence; more negative responses to others and less overall social competence (Sroufe 2005). In addition to children being classified as either secure or insecure, they may also be classified as disorganised, when there is evidence of a conflict between wanting to approach and wanting to avoid the caregiver when the attachment system is activated (Main 1990a). Disorganised attachment occurs when children are frightened of the caregiver and have been exposed to a range of anomalous, atypical parent‐child interactions (Madigan 2006). Disorganised attachment is associated with predictors of later psychopathology, including externalising behaviours (Fearon 2010), and personality disorders (Steele 2010). Many studies consider only secure and insecure attachment patterns when classifying children, as these were the attachment patterns that were first described (Weinfield 2004). These studies (carried out in the general population) typically find that approximately 60% of children are securely attached, and the remainder (40%) are insecurely attached (Moullin 2014). For insecurely attached children, 25% learn to avoid their parent when they are distressed (avoidant attachment) and 15% learn to resist the parent, often because the parent responds unpredictably or amplifies their distress (resistant attachment; Moullin 2014). In studies where disorganised attachment has been included, around 40% of disadvantaged children are classified as disorganised (Weinfield 2004), and as many as 80% of abused children receive this classification (Cyr 2010).
Although children usually have a particularly strong bond with one primary caregiver, most have more than one attachment relationship, often with fathers, siblings and grandparents as well as with mothers (see, for example, Hallers‐Haalboom 2014). As such, children can be securely attached to one parent but insecurely attached to another. The role of early relationship experiences and the development of child self‐regulatory skills have been linked to the child’s ability to control behavioural and physiological responses such as anger (Gilliom 2002), aggression (Alink 2009), and anxiety (Hannesdottir 2007).
Caregiver sensitivity
One key predictor of child attachment status is the parent's attachment status (Van Ijzendoorn 1995). The impact of the parent's attachment status on the child's attachment appears to be mediated by parental sensitivity to child cues.
Ainsworth and colleagues defined sensitivity as a mother’s ability to attend and respond to her child in ways that accurately match her child's needs (Ainsworth 1978). Sensitive and responsive parents do the following: notice a child’s signals; interpret these signals correctly; and respond to signals in a timely and appropriate manner (Ainsworth 1974). The concept of sensitivity, therefore, refers not to a specific set of maternal behaviours but to something much more dynamic and relational.
Parental sensitivity can be compromised by a variety of factors. These include social influences such as social isolation (Belsky 2002; Kivijärvi 2004), or domestic violence (Levendosky 2006); psychological factors such as maternal depression (NICHD Early Child Care Research Network 1999; Karl 1995; Murray 1997), or personality disorder (Laulik 2013); maternal history of maltreatment (Pereira 2012), substance dependence (Eiden 2014), low self‐esteem (Leerkes 2002; Shin 2008); or cognitive factors such as maternal preconceptions about parenting (Kiang 2004; Leerkes 2010). Child characteristics can also impact negatively on parental sensitivity, including child prematurity (Singer 1999); the presence of excessive negative child behaviour, such as general distress (Leerkes 2002); and the child's proneness to anger (Ciciolla 2013), and irritability (Van den Boom 1991). Some studies have examined father involvement as a mediator of maternal sensitivity (see, for example, Stolk 2008), whilst others have examined the role of the father as caregiver (see, for example, Pelchat 2003). Comparative research on the relative sensitivity of mothers and fathers is scarce and therefore the findings are somewhat inconclusive; some studies report fathers as less sensitive than mothers (see Hallers‐Haalboom 2014; Heerman 1994; Lovas 2005), while others have found no difference (Pelchat 2003).
Although parental sensitivity has been found to be an important predictor of child attachment security, a systematic review of the antecedents to attachment security suggests that it explains around only one third of the variance (De Wolff 1997). Research has also highlighted the importance of mid‐range contingency (Beebe 2010), and maternal reflective functioning (Slade 2005), or mind‐mindedness (Meins 2001). Mid‐range contingency refers to the ability of the parent to regulate flexibly both their own internal emotional states and their interaction with the baby, and is characterised by moments of synchrony or attunement, followed by rupture and then repair. A study by Beebe 2010 found that interaction that occurred outside this mid‐range, resulting from the parent’s preoccupation either with self‐regulation (e.g. depressed parents) or interactive regulation (e.g. anxious parents), was associated with an insecure or disorganised attachment).
Reflective functioning is a term that describes a parent's ability to comprehend their child's behaviour with regards to their internal mental states (Slade 2005). High reflective functioning correlates with positive maternal parenting traits, such as flexibility and responsiveness. Low reflective functioning can be seen in tandem with negative maternal behaviours, such as withdrawal and intrusiveness (Kelly 2005; Slade 2005). Similarly, mind‐mindedness, which refers to the parent's ability both to understand a young child's state of mind and to respond appropriately, has been associated with behavioural sensitivity and interactive synchrony (Meins 2001), and to better predict attachment security of the child at one year of age than maternal sensitivity (Lundy 2003; Meins 2001; Meins 2012).
Other studies have identified the importance of a range of atypical or anomalous parent‐child interactions characterised as ‘Fr‐behaviours’, which are the behaviours of parents who are either frightened or frightening, or both (Jacobvitz 1997; Main 1990b), or who are hostile and helpless (Lyons‐Ruth 2005). Fr‐behaviours have been described as subtle (e.g. periods of being dazed and unresponsive) or more overt (deliberately frightening children; Lyons‐Ruth 2005), and are strongly associated with disorganised attachment (Madigan 2006).
Description of the intervention
Video feedback is a generic term that refers to the use of videotaped interactions of the parent and child to promote parental sensitivity; it has other names, including Video Interaction Guidance (VIG), Interaction Guidance (IG), Video Home Training (VHT) and Video Feedback Intervention to Promote Positive Parenting (VIPP). Developed by Harrie Biemans and colleagues in the 1980s, video feedback is a relationship‐based parenting intervention that aims to enhance maternal sensitivity at the behavioural level (Kennedy 2010). The core aspects of interventions based on video feedback are as follows.
Video‐recording the parent‐child interaction during play or aspects of daily caregiving.
Editing the recording to select micro‐moments of interaction that demonstrate the child's contact initiatives and examples of the parent's attuned response to these signals.
Parent and 'guider' (the person responsible for the therapy) jointly reviewing the recordings, with the guider providing praise to the parent, not for the attunement per se but for engaging in the evaluation of the interactions being viewed.
The intervention model is underpinned by two core concepts: intersubjectivity and mediated learning. Intersubjectivity, or 'shared moments of attunement', is modelled by the therapist (or 'guider') in their relationship and interactions with the parent, as well as being identified in the video recordings of the parent‐child interaction. Mediated learning, or 'scaffolding', refers to the role adults play in helping children learn how to do things that they might not otherwise manage alone. Mediated learning is also modelled by the guider in his or her relationships with the parent, as the guider helps the parent to describe what is happening in the clips being viewed, and what the parent and child in the video might be thinking or feeling, and to identify the consequences for the parent and the child (Kennedy 2011).
Video feedback may be delivered on a one‐to‐one (e.g. VIPP, VIG) or group (e.g. Circle of Security (CS)) basis, and has been used with first‐time mothers (Klein Velderman 2006); hard‐to‐reach families (Kennedy 2010); parents of premature infants (Hoffenkamp 2015); parents with mental health problems, including postpartum depression (Vik 2006); parents of autistic children (Poslawsky 2015), maltreated children (Moss 2011), and adopted children (Juffer 1997); parents of children with atopic dermatitis (Cassibba 2015); ethnic‐minority parents (Yagmur 2014); and parents with an eating disorder (Stein 2006). Although video feedback is usually delivered in the home environment, it has also been used in clinical settings, such as hospital environments with mothers of preterm babies (Hoffenkamp 2015), and residential treatment centres (Kennedy 2010). It is now used in over 15 countries by practitioners who work in a range of helping professions (e.g. social work, education and health; Kennedy 2010).
How the intervention might work
In terms of the underpinning theoretical model, most forms of video feedback are attachment‐based in the sense that they aim to enhance maternal sensitivity, and promote optimal child social and emotional development (Klein Velderman 2006a), with the longer‐term goal of promoting improved child attachment (Juffer 2008). However, the presumed mechanisms by which this is achieved vary across the different models of video feedback. All video‐feedback interventions primarily target the behavioural level using video‐recorded episodes of the parent‐child interaction. The guider provides an opportunity for the caregiver to experience attuned interactions with a sensitively attuned adult (Kennedy 2011), and also to view themselves in interaction with their child and observe positive responses from them. Together, these are hypothesised to bring about a range of meta‐cognitive changes that result from the discrepancy between their own beliefs about their ability to parent and what they can see on the video, in addition to an increase in feelings of empowerment and self‐efficacy, and their ability for self‐reflection (Kennedy 2011).
Some models of video‐feedback intervention include additional components that may provide a more explicit focus on representational issues. For example, Video Feedback Intervention to Promote Positive Parenting with Discussions on the Representational Level (VIPP‐R; Juffer 2008), involves the therapist addressing the mother's representations and attachment using discussions that may, for example, focus explicitly on the mother's own experiences of separation in early childhood and those experienced with her own child (Klein Velderman 2006a).
Other models involve the inclusion of teaching about sensitive discipline techniques, such as Video Feedback Intervention to Promote Positive Parenting ‐ Sensitive Discipline (VIPP‐SD). There is evidence that suggests the effectiveness of video feedback may vary with factors at both the level of the parent and of the child. For example, Klein Velderman 2006 reported that amongst mothers with insecure attachments, those classed as 'insecure dismissing' (who idealise their own parents or minimise the importance of attachment relationships in their own lives) benefited most from video feedback, whilst those classed as 'insecure preoccupied' benefited most when they participated in video feedback together with further discussions about their individual experiences of attachment in childhood.
Why it is important to do this review
Improvement of the health and well‐being of children is part of a global agenda. While the basic needs of children (e.g. food, sanitation, health care) are paramount to survival and development, living with an adult who is responsive to their needs is also important (Jones 2003). UNICEF 2008 highlights that a loving, stable and stimulating relationship with caregivers in the earliest months and years of life are critical for every aspect of a child’s development. Specifically, the empirical literature shows that maternal sensitivity is a key predictor of child attachment security (De Wolff 1997), and that a secure attachment promotes more optimal childhood development (Sroufe 2005), while an insecure or disorganised attachment predicts later behaviour problems (Fearon 2010), and psychopathology (Steele 2010). Research suggests that early, targeted interventions are potentially an effective means of increasing parental sensitivity (Bakermans‐Kranenburg 2003), and although there have been a number of reviews of the impact of video feedback on a range of outcomes including maternal sensitivity (Balldin 2018; Fukkink 2008; Juffer 2018; NICE 2016; Van den Broek 2017), only two conducted meta‐analyses. Fukkink 2008 concluded that video feedback was an effective means of improving parenting behaviour and attitudes, and child development. However, the report did not provide the search dates for the review, which was submitted in June 2008; did not search a wide range of databases; and was very broad in its scope, including all uses of video feedback with no age limits on the children (who ranged in age from birth to seven years, with an average age of 2.4 years (standard deviation (SD) 2.7 years). More importantly, the study authors paid little attention to the quality of included studies (that is, there were no 'Risk of bias' assessments) and included studies without random assignment. Juffer 2018 looked only at studies using one type of video feedback known as 'Video Interaction to promote Positive Parenting' (VIPP) and found that VIPP was effective in improving parental sensitivity.
This systematic review of current best evidence addresses the methodological weakness of Fukkink 2008 and has a broader scope than Juffer 2018. It will be of interest to policy makers and practitioners internationally.
Objectives
To assess the effects of video feedback on parental sensitivity and attachment security in children aged under five years who are at risk for poor attachment outcomes.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) and quasi‐RCTs (in which the allocation to study arms is not truly random; for example, allocation is done through a form of alternation such as days of the week or by date of birth). We included cluster‐ and cross‐over RCTs.
We excluded studies that had an alternative treatment but no control group. Alternative treatment controls are not appropriate when seeking to investigate the effectiveness of an intervention, which was the aim of this review (this is in accordance with advice from Cochrane Developmental, Pyschoscial and Learning Problems).
Types of participants
We included parent‐child dyads (including foster or adoptive carers) or family units, where the child was aged between birth and four years 11 months (inclusive), and where problems had been identified that might impact or were impacting the parent's sensitivity (e.g. poor bonding, depression, eating disorders, maltreatment) or child attachment (e.g. behaviour problems, challenging temperament, preterm birth). The majority of studies looked at parent‐child dyads.
If studies included a proportion of participants aged above four years 11 months, we endeavoured to obtain data on the sample aged up to four years 11 months; where this was not possible, we used outcome data that included children outside our target age group in the meta‐analysis (e.g. Moss 2011; Poslawsky 2015).
We excluded studies in which the intervention was used with a population group where neither parents nor children had any risk factors for attachment problems.
Types of interventions
We included video‐feedback interventions delivered in any setting, in which the parent and child were filmed and then feedback was provided to the parent either on a one‐to‐one basis or in groups, with the aim of improving the sensitivity of their interactions with the child, child attachment, or the reflective functioning of the parent.
We included interventions that, in addition to video feedback, also provided a small number of additional sessions related to the primary aim of the intervention; for example, VIPP‐R or VIPP‐SD.
We included studies in which the intervention was compared with no treatment, an inactive alternative intervention or treatment as usual. Examples of control treatment included a sequence of telephone calls with a parent (Barone 2019; Kalinauskiene 2009; Negrão 2014; Van Zeijl 2006; Yagmur 2014); a limited number of home visits with (1) video recordings between parent and child with no feedback (Benzies 2013; Koniak‐Griffin 1992; Moran 2005); (2) by a play and development service (Green 2010); (3) discussions about parenting (Poslawsky 2015); standard hospital care (Hoffenkamp 2015) or routine care at well baby units (Høivik 2015).
We excluded studies comparing video feedback with other interventions, as well as:
interventions in which video feedback was used as part of a wider set of methods of working with the family and in which we could not differentiate the effect of video feedback, and
programmes that used videotape modelling or videotaped vignettes of parents and their children (e.g. Webster‐Stratton 2015).
Types of outcome measures
We excluded studies that did not measure parental sensitivity or did not do so in an objective way; for example, studies relying on self‐report measures, such as the Parent‐Child Dysfunctional Interaction (PCDI) subscale of the Parenting Stress Index (Abidin 1995).
Primary outcomes
Parental sensitivity, measured by, for example, the Ainsworth Sensitivity Scale (ASS; Ainsworth 1974), the Child‐Adult Relationship Experimental Index (CARE‐Index; Crittenden 2001), the Parental Sensitivity Assessment Scale (PSAS; Hoff 2004), Coding Interactive Behaviour (CIB; Feldman 1998), the Emotional Availability (EA) scales (Biringen 2000a), Global Ratings Scales (GRS) of mother‐infant interaction (Murray 1996), Maternal Behaviour Q‐sort (MBQS; Pederson 1999), or Nursing Child Assessment Teaching Scale (NCATS; Sumner 1994).
Parental reflective functioning, measured by, for example, the Parent Development Interview (PDI; unpublished manuscript by Aber 1985), or the PDI‐Revised (PDI‐R; unpublished manuscript by Slade 2004).
Attachment security, measured by, for example, the Attachment Q‐sort (AQS; Waters 1985; Waters 1987), or the Strange Situation Procedure (SSP; Ainsworth 1978).
Adverse effects. We acknowledge that a worsening of any of our primary outcomes listed above would be considered an adverse effect. However, we also considered the effects of the intervention on parental anxiety and stress, measured by, for example, the Parenting Stress Index (PSI; Abidin 1995), or the Parenting Stress Scale (PSS; Berry 1995).
Secondary outcomes
Child mental health, measured by behavioural assessments of emotional disorders, hyperactivity and conduct disorders.
Child physical and socioemotional development, measured through, for example, the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley‐III; Bayley 2006), or the Strengths and Difficulties Questionnaire (SDQ; Goodman 1997).
Child behaviour, measured by, for example, the Child Behaviour Assessment Instrument (CBAI; Samarakkody 2010).
Costs, measured by direct costs stated by studies.
Timing of outcome assessment
We collected outcome data at time points provided within the included studies and grouped these as postintervention (immediately upon completion of the intervention), short term (up to six months), medium term (up to one year) and long term (over one year).
Search methods for identification of studies
We ran the first database searches in August and September 2016 (Electronic searches) followed by searches of other resources in July 2017 (Searching other resources). In November 2018 we updated the searches, including bibliography screening, and ran further searches of other resources in July 2019. We did not apply any date or language restrictions to the electronic searches and had two papers translated into English (Bovenschen 2012; Kalinauskiene 2009).
Electronic searches
We searched the electronic databases and trials registers listed below.
Cochrane Central Register of Controlled Trials (CENTRAL; 2018, Issue 11), in the Cochrane Library and which includes the Cochrane Developmental, Psychosocial and Learning Problems' Specialised Register (searched 10 November 2018)
MEDLINE Ovid (1946 to November Week 1 2018)
Embase Ovid (1974 to 2018 Week 44)
CINAHL Plus EBSCOhos (Cumulative Index to Nursing and Allied Health Literature; 1937 to 10 November 2018)
PsycINFO Ovid (1806 to 2018 Week 44)
Sociological Abstracts ProQuest (1952 to 10 November 2018)
Social Sciences Citation Index Web of Science (SSCI; 1970 to 10 November 2018)
Social Services Abstracts ProQuest (1979 to 10 November 2018)
Conference Proceedings Citation Index ‐ Social Science & Humanities Web of Science (CPCI‐SS&H; 1990 to 10 November 2018)
LILACS (Latin American and Caribbean Health Science Information database; 1985 to current; lilacs.bvsalud.org/en; searched 10 November 2018).
Cochrane Database of Systematic Reviews (CDSR; 2018; Issue 11), part of the Cochrane Library (searched 10 November 2018)
Database of Abstracts of Reviews of Effects (DARE; 2015; Issue 2. Final issue), part of the Cochrane Library (searched 10 November 2018)
Networked Digital Library of Theses and Dissertations (NDLTD; www.ndltd.org; searched 10 November 2018)
WorldCat (limited to dissertations and theses; www.worldcat.org; searched 10 November 2018)
Clinicaltrials.gov (Clinicaltrials.gov; searched 10 November 2018)
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP; www.who.int/ictrp/en; searched 10 November 2018)
Searching other resources
Two review authors (ES and LOH) screened the bibliographies of included studies (Barlow 2016; Barone 2019; Benzies 2013; Bovenschen 2012; Green 2010; Green 2015; Hodes 2017; Hoffenkamp 2015; Høivik 2015; Kalinauskiene 2009; Klein Velderman 2006; Koniak‐Griffin 1992; Lam‐Cassettari 2015; Moran 2005; Moss 2011; Negrão 2014; Platje 2018; Poslawsky 2015; Seifer 1991; Stein 2006; Van Zeijl 2006; Yagmur 2014) and relevant reviews (Balldin 2018; Fukkink 2008; Juffer 2018; NICE 2015; Van den Broek 2017), to identify any additional relevant publications. They also searched the websites of the following relevant organisations and government departments: United Nations International Children's Emergency Fund (UNICEF) Global Evaluation Database (unicef.org/evaldatabase); National Society for the Prevention of Cruelty to Children (NSPCC) Impact and Evidence Hub (nspcc.org.uk/services‐and‐resources/impact‐evidence‐evaluation‐child‐protection); and the Association for Video Interaction Guidance UK (AVigUK; videointeractionguidance.net) (see Appendix 1). One review author (ES) visited the websites of research groups we knew to be conducting work in this area to screen their listed publications (see Appendix 1). Another review author (LOH) also used Google Scholar to search the internet for unpublished work (see Appendix 1).
Although originally planned (O'Hara 2016), we did not contact experts to enquire about other published work or unpublished work (Table 2).
1. Methods for use in future updates of this review.
| Issue | Method |
| Searching other resources | We will draft a list of included studies to send to experts in the field and ask them to forward to us any published, unpublished or ongoing work that we may have missed. |
| Measures of treatment effect |
Continuous outcome data If necessary, we will compute effect estimates from P values, T statistics, analysis of variance (ANOVA) tables or other statistics, as appropriate. |
| Measures of treatment effect |
Multiple outcomes When a study provides multiple, interchangeable measures of the same construct at the same point in time (e.g. multiple measures of maternal sensitivity), we will calculate the average SMD across these outcomes and the average of their estimated variances. This strategy aims to avoid the need to select a single measure and to avoid inflated precision in meta‐analyses (i.e. preventing studies that report on more outcome measures receiving more weight in the analysis than comparable studies that report on a single outcome measure). |
| Unit of analysis issue |
Cluster‐RCTs In the event that we identify relevant cluster‐RCTs that meet the inclusion criteria of the review, we will deploy appropriate statistical methods based on the guidance provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Where study authors have dealt appropriately with the clustered design in their analyses, we will try to obtain direct estimates of the effect (e.g. an OR with its CI). Where study authors have not dealt appropriately with the cluster design in their analyses, we will extract or calculate effect estimates and their SEs as for a parallel‐group trial, and adjust the SEs to account for the clustering (Donner 1980). To do this, we will need to identify an appropriate ICC, which describes the relative variability in outcome within and between clusters (Donner 1980). Where available, we will look for this information in the reports of relevant trials. If this is unavailable, we will try to obtain the information from the study authors. If this proves unsuccessful, we will use external estimates obtained from similar studies. We will find closest‐matching scenarios (regarding both outcome measures and types of clusters) from existing databases of ICCs. If we are unable to identify any matches, we will perform sensitivity analyses using a high ICC of 0.1, a moderate ICC of 0.01 and a small ICC or 0.001, to cover a broader range of plausible values while still allowing for strong design effects for smaller studies (see Sensitivity analysis). Furthermore, we will combine these estimates and their corrected SEs from the cluster‐RCTs with those from parallel designs using the generic inverse variance method in Review Manager 5 (Review Manager 2014). |
| Dealing with missing data |
Data imputation Where it has not been possible to obtain any unreported data from authors of included studies, and there is reason to believe that it is not missing at random, we will follow the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011, Section16.1), and we will do the following:
|
|
Meta‐regression We will assess the sensitivity of any primary meta‐analyses to missing data using meta‐regression to test for any effect of missingness on the summary estimates (Higgins 2011, Section 16.1.2). | |
| Data synthesis | In the occurrence of severe funnel plot asymmetry, we will present both fixed‐effect and random‐effects analyses under the assumption that asymmetry suggests that neither model is appropriate. If both indicate a presence (or absence) of effect we will be reassured; if they do not agree we will report this. |
| Subgroup analyses | We will investigate heterogeneity using subgroup analyses or meta‐regression, if appropriate. We will group the included studies and analyse them according to the intervention approach, including the following.
|
| Sensitivity analysis | We will assess the robustness of findings to decisions made in obtaining them by conducting sensitivity analyses. We will perform sensitivity analyses by conducting the following reanalysis.
|
| CI: confidence interval; ICC: intra‐class correlation coefficient; OR: odds ratio; RCT: randomised controlled trial; SD: standard deviation; SMD: standardised mean difference; VIG: Video Interaction Guidance; VIPP‐R: Video‐feedback to promote Positive Parenting ‐ Representational level; VIPP‐SD: Video‐feedback to promote Positive Parenting ‐ Sensitive Discipline | |
Data collection and analysis
For this section, we only report those methods used in this review. Other methods that were not relevant to the available data, or that we could not use for other reasons, are summarised in Table 2. One of the review authors (JB) is an author of an included study (Barlow 2016). JB was not involved in data extraction or assessment of risk of bias; the review authors involved in this did not need to seek any further advice on either of these areas with regards to this particular study.
Selection of studies
At least two review authors (from ES, LOH and NH) independently screened titles and abstracts yielded by the searches against the inclusion criteria for the review (Criteria for considering studies for this review). The review authors retrieved the full‐text reports of all studies selected for potential inclusion, or those where there was some uncertainty, and assessed the reports for eligibility. Where review authors could not agree, they further discussed the papers with JB or GM. In one case, Mendelsohn 2005, we wrote to the study authors for the purposes of clarifying whether or not the study met our inclusion criteria (Table 3). We list excluded studies in the Characteristics of excluded studies tables, together with the reason for their exclusion. We report the flow of studies in a PRISMA diagram (Liberati 2009).
2. Summary of contact with study authors.
| Study | Date contact initiated | Reason for contacting study authors | Response received |
| Barone 2019 | 9 July 2019 (Smith 2019a [pers comm]) | The study data for maternal sensitivity were reported in the published paper as part of a composite measure. We requested maternal sensitivity subscore. We also requested study data for overall child behaviour, as the published report only contained externalising behaviour. | The study author provided the maternal sensitivity and child behaviour data for inclusion in the meta‐analysis (Barone 2019 [pers comm]). They excluded children aged 5 years and over from the data sent over, as the original study did include these children. |
| Bovenschen 2012 | 12 January 2018 (Smith 2018b [pers comm]) | The reported data were not labelled sufficiently clearly in the published paper to be used in the meta‐analysis. We requested clarification from the study authors. | The study author provided the necessary, additional study data, so they could be included in meta‐analysis (Bovenschen 2019 [pers comm]). |
| Hodes 2017 | 2 June 2017 (Smith 2017a [pers comm]) | We requested study data relating to parental stress outcomes, reanalysed for children within included age range. | We received no response. As a result, we did not subsequently request the study data on Harmonious Parent‐Child Interaction to be analysed for children within included age range. |
| Hoffenkamp 2015 | 16 January 2017 (O'Hara 2017a [pers comm]) | We requested missing study data relating to parental sensitivity outcomes. | The study author provided the missing data so they could be included in the meta‐analysis (Van Bakel 2017 [pers comm]). |
| Høivik 2015 | 8 February 2018 (Smith 2018c [pers comm]) | The study data for maternal sensitivity were reported in the published paper as part of a composite measure. We requested maternal sensitivity subscore. | The study author provided maternal sensitivity data for inclusion in the meta‐analysis (Hoivik 2018 [pers comm]). |
| Klein Velderman 2006 | 21 February 2018 (Smith 2018g [pers comm]) | The outcomes data for maternal stress were not included in published studies. | The corresponding author provided us with the missing data for the purposes of meta‐analysis (Bakermans‐Kranenburg 2018 [pers comm]). |
| Koniak‐Griffin 1992 | 8 February 2018 (Smith 2018d [pers comm]) | The study data for maternal sensitivity were reported in the published paper as part of a composite measure. We requested maternal sensitivity subscore. | We received no response. |
| Lam‐Cassettari 2015 | 2 June 2017 (Smith 2017b [pers comm]) | The published study data for maternal sensitivity outcomes included children aged 5 years and over. We requested outcomes data with those children excluded. | The study author provided the data with those children aged 5 years and over excluded (Lam‐Cassettari 2018 [pers comm]). |
| Mendelsohn 2008 | 1 February 2018 (Smith 2018i [pers comm] | We requested a copy of the conference abstract. | We received no response. |
| Moran 2005 | 3 June 2017 (O'Hara 2017b [pers comm]) | The maternal sensitivity outcomes were reported as means without standard deviations or standard errors. We requested these data so they could be used in the meta‐analysis. | The corresponding author no longer had access to the data due to retirement, so could not provide the information (Moran 2017 [pers comm]). |
| Moss 2011 | 12 January 2018 Smith 2018h [pers comm] |
The published study data for maternal sensitivity outcomes included children aged 5 years and over, We requested outcomes data with those children excluded. | We received an initial response from the study authors but they did not subsequently provide the data (Dubois‐Comtois 2018 [pers comm]). |
| Negrão 2014 | 12 January 2018 (Smith 2018e [pers comm]) | The maternal stress outcomes data were not reported in the published paper, so we requested this information for the purposes of the meta‐analysis. | The study author provided these data for the purposes of meta‐analysis (Pereira 2018 [pers comm]). |
| Poslawsky 2015 | 12 January 2018 (Smith 2018f [pers comm]) | The reported outcomes included children aged 5 years or older. We requested outcomes data with those children excluded. We also requested means and standard deviations for the relevant 3‐month follow‐up outcome (daily hassles). | The corresponding author was unable to provide the requested data (Poswlawsky 2018 [pers comm]). |
| Seifer 1991 | 22 July 2019 (Smith 2019b [pers comm]) | We requested outcomes data for mental and psychomotor development | We received no response. |
| Stein 2006 | 22 May 2018 (Barlow 2018 [pers comm]) | The outcomes data for 'Verbal responses to infant cues' were reported as medians, so we requested the means and standard deviations. | The study authors provided us with these data for the purposes of meta‐analysis (Stein 2018 [pers comm]). |
Data extraction and management
Two review authors (from NH, LOH, ES) independently extracted data from each included study and recorded the following information on a pre‐piloted data extraction form.
Participant characteristics (age, gender, ethnicity, location)
Intervention characteristics (including delivery, duration, outcomes and measures, and within‐intervention variability)
Comparison characteristics (including whether the study used an active or inactive comparison)
Study characteristics (study design, sample size, length of follow‐up, attrition or dropout, handling of missing data, methods of analysis, dates of study, funding sources, conflicts of interest)
Outcome data (relevant details on all primary and secondary outcome measures used, and summary data, including means, standard deviations (SDs), confidence intervals (CIs) and significance levels for continuous data and proportions for dichotomous data)
Review authors resolved disagreements through discussion. Where clarity was needed over whether an outcome in a study was relevant, the reviewer authors sought advice from JB.
Assessment of risk of bias in included studies
Two review authors (ES for all studies, with either LOH or NH) independently assessed the risk of bias of each included study using the Cochrane 'Risk of bias' tool (Higgins 2017). They assigned judgements of low, high or unclear risk of bias for each of the following domains, using the criteria set out in Appendix 2: sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective reporting and other bias. Where review authors did not agree after discussion, they discussed further with another author (JB or NL). We recorded the judgements in 'Risk of bias' tables.
Measures of treatment effect
We calculated unadjusted treatment effects using Review Manager 5 (RevMan 5) (Review Manager 2014).
Dichotomous outcome data
We calculated the odds ratio (OR) with 95% CI for dichotomous outcomes. For dichotomous outcomes that we included in the 'Summary of findings' tables, we expressed the results as absolute risks and used high and low observed risks among the control groups as reference points.
Continuous outcome data
For continuous outcomes, we calculated the mean difference (MD) if all included studies used the same measurement scale, or the standardised mean difference (SMD) if studies used different measurement scales, and 95% CIs. We calculated SMD using Hedge's g. In one instance, we converted an SMD from Cohen's d to Hedge's g.
Economics issues
We reviewed studies for data on the costs of programmes within the included studies.
Unit of analysis issues
Studies with multiple treatment groups
In the primary analysis, we combined results across all eligible intervention groups and compared them with the combined results across all eligible control groups, and made single pair‐wise comparisons. Where studies compared more than one form of video interaction with a control group or groups, such that combining them prevented investigation of potential sources of heterogeneity, we analysed each video interaction group separately (against a common control group) but divided the sample size for common comparator groups proportionately across each comparison (Higgins 2011; Section 16.5.5). This simple approach allows the use of standard software and prevents inappropriate double counting of individuals. We applied this latter approach to three studies (Benzies 2013; Hoffenkamp 2015; Klein Velderman 2006).
Dealing with missing data
Where necessary, one review author (LOH or ES) contacted the authors of included studies requesting them to supply any unreported data such as missing outcome data (e.g. group means and SDs and details of number of dropouts). Details of which study authors we contacted and why are in the Characteristics of included studies tables and Table 3.
If we were not able to obtain unreported outcome data, we followed the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011, Section 16.1) and did the following:
Analysed the data available, as we assumed the data were missing at random.
Two studies had unreported outcome data on parental sensitivity that the study authors were unable to provide: Koniak‐Griffin 1992 reported a result for a scale with parental sensitivity as a subdomain, but did not report the subdomains; and Moran 2005 reported means but not SDs or standard errors (SE). We did not impute this unreported data, as we assumed the data were missing at random.
Assessment of heterogeneity
We assessed clinical heterogeneity across included studies by examining the distribution of important participant factors (e.g. age) and intervention characteristics (e.g. style, setting, personnel, context of delivery) among studies. The details of this information are included in the Characteristics of included studies tables, and discussed in the Results section.
We assessed methodological heterogeneity across included studies by comparing the distribution of study factors (e.g. allocation concealment, blinding of outcome assessment, losses to follow‐up, treatment type, cointerventions). This information is contained in the Characteristics of included studies tables and 'Risk of bias' tables, and considered in the Discussion.
We described statistical heterogeneity by computing the I2 statistic (Higgins 2002), which describes approximately the proportion of variation in point estimates that is due to heterogeneity rather than sampling error. In addition, we used the Chi2 test (P < 0.10) of homogeneity to detect the strength of evidence that heterogeneity is genuine (Deeks 2017).
Assessment of reporting biases
We drew a funnel plot (estimating differences in treatment effects against their standard error (SE)) when we identified 10 or more studies that provided data on an outcome; in this case, parental sensitivity. We assessed the funnel plot by visual inspection and also by Egger's regression test (Egger 1997). We redrew the funnel plot without an outlying study (Green 2010), to better assess the asymmetry.
We considered the reasons for any asymmetry. Asymmetry might be due to publication bias, but might also reflect a relationship between study size and effect size, such as when larger studies have lower compliance, and compliance is positively related to effect size. It may also be due to clinical variation between the studies (Sterne 2017, Section 10.4), for example the study population, reflecting true heterogeneity.
As a direct test for publication bias, we compared results extracted from published journal reports with results obtained from other sources for the two outcomes for which this was possible, parental sensitivity and parental stress. In these cases we obtained some outcome data directly from study authors that were not reported in the published papers (see Table 3).
Data synthesis
Where interventions were similar in terms of (1) the age of the child(ren), (2) parent gender and (3) intensity, frequency and duration of video feedback, we synthesised results in a meta‐analysis.
We used both fixed‐effect and random‐effects models and compared the results to assess the impact of statistical heterogeneity. Except where the model was contraindicated (e.g. if there was funnel plot asymmetry), we present the results from the random‐effects model. When we report the results of the random‐effects model, we include an estimate of the between‐study variance (Tau2).
We calculated all overall effects using inverse variance methods.
Where some primary studies reported an outcome as a dichotomous measure and others used a continuous measure of the same construct (as in the case of attachment security), we performed two separate analyses rather than converting the OR to a SMD. This was because we could not assume that the underlying measure had a normal or logistic distribution, as the nature of the populations in the two relevant studies means that the distribution of attachment patterns is likely to be skewed (teenage mothers in Moran 2005 and families where children had been subjected to maltreatment in Moss 2011).
Where a trial reported two outcomes within a time period covered by the same meta‐analysis, we combined the data from the time point nearest the end of the intervention. Where possible, we tried to combine outcomes measured at similar time points in the follow‐up period.
'Summary of findings' table
We created a 'Summary of findings' table for the following comparison: video feedback versus no intervention or inactive alternative intervention.
We followed the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2017), and included the following six elements in these tables.
A list of all outcomes
A measure of the typical burden of these outcomes
Absolute and relative magnitude of effect
Numbers of participants and studies that address these outcomes
A rating of the overall certainty of evidence for each outcome
Additional comments
Two review authors (LOH, ES) independently assessed the certainty of the evidence, using the following five GRADE considerations (Schünemann 2017).
Limitations in study design and implementation: for RCTs, for example, these included lack of allocation concealment, lack of blinding and large loss to follow‐up.
Indirectness of evidence: for example, if findings were restricted to indirect comparisons between two interventions. RCTs that met the eligibility criteria but that addressed a restricted version of the main review questions in terms of population, intervention, comparator or outcomes are another example of this and would also have been downgraded.
Unexplained heterogeneity or inconsistency of results: we looked for robust explanations for heterogeneity in studies that yielded widely differing estimates of effect.
Imprecision of results: we downgraded the certainty of evidence for those studies that included few participants and few events and thus had wide CIs.
Publication bias: we downgraded the certainty of evidence level if investigators failed to report studies or outcomes on the basis of results.
We downgraded the ratings (from high to very low), depending on the presence of the five factors.
We used GRADEpro GDT to prepare the 'Summary of findings' table, and specifically, to enable us to produce relative effects and absolute risks associated with the interventions (GRADEpro GDT). We used all primary outcomes and one secondary outcome of interest to populate the ‘Summary of findings’ table (primary outcomes: parental sensitivity at postintervention to six months; reflective functioning; attachment security measured by Strange Situation Procedure at postintervention; attachment security measured by Attachment Q‐sort at postintervention; parental stress measured at postintervention and short‐term follow‐up; and parental anxiety at short‐term follow‐up; secondary outcome: child behaviour measured at long‐term follow‐up). We also used Ryan 2016 to guide our judgements.
Subgroup analysis and investigation of heterogeneity
We investigated heterogeneity by conducting moderator analyses for the outcome of 'parental sensitivity'. To perform this analysis, we used a random‐effects meta‐analysis with a Sidik‐Jonkman estimator, which is robust for small numbers of studies and provides improved CI (Veroniki 2019). We considered the following factors, some of which we decided post hoc.
Prespecified factors
Intervention dose: defined by number of video feedback sessions (zero to five versus six to 10 versus more than 10; grouping this factor in this way was a post hoc decision).
Participating carer: all mothers versus all fathers versus mix of mothers and fathers (we made a post hoc decision to include studies with a mix of parental genders along side those who were all fathers or all mothers).
Type of video feedback (VIPP versus non‐VIPP; grouping types of video feedback in this way was a post hoc decision).
Factors specified post hoc
Age of child (children under one year old versus children aged one year or older; using age of child as a factor was a post hoc decision).
Disability status of children (disability versus no disability; using disability status of the child was a post hoc decision).
In the first step, we assessed the moderators individually and reported their overall contribution to the reduction of heterogeneity (Q‐between). To assess whether moderation effects for study characteristics existed, we conducted a moderator analysis in which we included the three prespecified moderators (type of video feedback, duration of video feedback and participating carer) simultaneously, this accounts for potential correlations between moderators. Given the small number of studies, this analysis should be treated with caution, due to the relatively low power. Predicted values are reported alongside regression results. We did not impute missing data in line with the main analyses.
We conducted the moderator analyses in R version 3.6.1 (R 2018), using the metafor‐package 2.1.0 (Viechtbauer 2010); analysis syntax and data are available from the review authors on request.
Sensitivity analysis
We assessed the robustness of findings to decisions made in obtaining them by conducting the following sensitivity analyses (Deeks 2017).
Reanalysis excluding studies at high or unclear risk of bias
Reanalysis using different statistical approaches (comparing the use of a random‐effects model with a fixed‐effect model).
Results
Description of studies
Results of the search
Our initial electronic searches (August to September 2016 and July 2017) identified 6191 records (see Figure 1). We identified an additional 381 records from other sources. After the removal of duplicates, we screened the titles and abstracts of 4368 records. We obtained and scrutinised 81 full‐text reports for eligibility, 47 of which (37 studies) did not meet the inclusion criteria and were excluded from the review with reasons (see Characteristics of excluded studies), and 34 (19 studies) that did and were included in the review.
1.
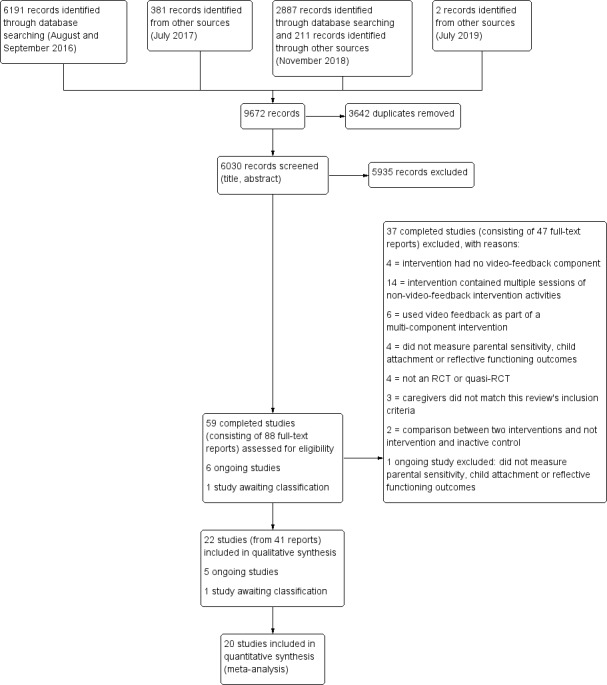
95 Study flow diagram
Our updated electronic searches (November 2018) identified 2887 records. We identified an additional 211 records through other sources in November 2018, and an additional two records in July 2019. After the removal of duplicates, we screened the titles and abstracts of 1662 records. During the title and abstract screening, we identified six ongoing studies, one of which we excluded, leaving five ongoing studies (Euser 2016; Firk 2015; ISRCTN92360616; NCT03052374; Schoemaker 2018), and one study awaiting classification (Mendelsohn 2008). We reviewed seven full‐text reports and added six reports pertaining to three new studies (Barone 2019; Platje 2018; Seifer 1991) and one report of a study identified during our initial search (Hodes 2017), to the review (see Figure 1).
Included studies
This review includes 22 studies (see Characteristics of included studies tables and Table 4), comprising a total of 41 reports and 1889 randomised parent‐child dyads or family units.
3. Type of video‐feedback intervention.
| Study | Aim | Content/delivery |
| Video‐feedback Intervention to promote Positive Parenting (VIPP; Juffer 2008) | ||
| Green 2015 | To test the effect of a parent‐mediated intervention for children at high risk of autism spectrum disorder | Video Interaction for promoting Positive Parenting (iBASIS‐VIPP), a modification for the autism prodome of the VIPP infancy programme. The intervention consisted of 12 sessions (an additional 6 booster sessions compared with VIPP).The intervention uses video feedback "to help parents understand and adapt to their infants' individual communication style to promote optimal social and communicative development" (quote). The study authors describe that "The therapist uses excerpts of parent‐child interactions in a series of developmentally sequenced home‐sessions focusing on interpreting the infant's behaviour and recognising their intentions; enhancing sensitive responding; emotional attunement and patterns of verbal and non‐verbal interaction." (quote) |
| Hodes 2017 | To test if a video‐feedback intervention to promote positive parenting and sensitive discipline reduces child‐related parental stress in parents with mild learning disabilities in comparison with care as usual | A Video‐feedback Intervention for Positive Parenting and Learning Difficulties (VIPP‐LD) where the original protocol of VIPP‐SD (Juffer 2008) was adapted for mild intellectual disabilities. For VIPP‐LD, in each session, the parent is videoed interacting with their child. The coach and parent review the footage together, drawing attention to instances of sensitive responsiveness and sensitive discipline, and the coach helps the parent look at the child from the child's perspective. The adaptation included shortening of each session, shorter video recordings and more real‐life practice. The study authors describe how "Parents also received a personal scrapbook with skills taken from video recordings and quotes from the parents representing the theme of the session." (quote) |
| Kalinauskiene 2009 | To evaluate the effectiveness of a short‐term, interaction‐focused video‐feedback intervention implemented in families with mothers rated low in maternal responsiveness | A Video‐feedback Intervention to promote Positive Parenting (VIPP). The intervention was applied as per protocol with the main goal "to reinforce mothers' sensitive responsiveness to their infants' signals focusing on different aspects of mother‐infant interactions" (quote). Mothers were also "provided with information on attachment‐related issues by giving them brochures about sensitive parenting." (quote) |
| Klein Velderman 2006 | To explore if a combination of attention to parental sensitivity and parental attachment representations might lead to firmer and more enduring changes in both parenting behaviour and children's attachment security | A Video‐feedback Intervention to promote Positive Parenting (VIPP). VIPP programs consisted of four home visits lasting 1.5 hours each, with 3‐4 weeks in between. Each session was focused around a specific theme. VIPP‐R included additional discussions on parental representations. |
| Negrão 2014 | To test the effectiveness of a video‐feedback intervention to promote positive parenting and sensitive discipline in a sample of poor Portuguese mothers and their 1‐4‐year old children | A sensitive discipline video‐feedback intervention to promote positive parenting (VIPP‐SD). The study authors state that "VIPP‐SD is a short term intervention programme that relies on video‐feedback technique to enhance parental sensitivity and positive discipline strategies. The intervention was applied through standardised protocols of six home visits...The VIPP‐SD working method is divided into three steps: (1) Sessions 1 and 2 main goals are building a relationship with the mother, focusing on child behaviour and emphasizing positive interactions in the video feedback; (2) Sessions 3 and 4 actively work on improving parenting behaviours by showing the mother when her parenting strategies work and to what other situations she could apply these strategies; and (3) Sessions 5 and 6 (booster) aim to review feedback and information from the previous sessions in order to strengthen intervention effectiveness." (quote) |
| Platje 2018 | To evaluate a video‐feedback intervention aimed at improving parent‐child interaction for parents of children with a visual or visual and intellectual disability | A Video‐feedback Intervention to promote Positive Parenting adapted to parents of children with a visual or visual and intellectual disability (VIPP‐V). The study authors state that the intervention was based on VIPP, but "this new intervention [is] applicable for use in families with a young child with a visual or visual‐and‐intellectual disability. Particular attention was devoted to increasing (safe) exploration, joint attention, and parent’s abilities to recognize and understand the signals and emotions of their child" (quote). The intervention consists of 7 home visits (5 primary visits plus 2 booster sessions). |
| Poslawsky 2015 | To evaluate the early intervention programme, video‐feedback intervention to promote positive parenting adapted to autism, with primary caregivers and their child with autism spectrum disorder | VIPP adapted to autism (VIPP‐AUTI). The intervention comprised 5 home visits lasting 60‐90 minutes every 2 weeks. Sessions included: (1) "Attachment and Exploration" (quote); (2) "Speaking for the Child" (quote); (3) "Sensitivity Chain" (quote); (4) "Sharing Emotions" (quote); (5) "Booster session" (quote). |
| Van Zeijl 2006 | To test the video‐feedback intervention to promote positive parenting and sensitive discipline in "a large sample of families screened for their children's relatively high scores on externalizing behaviour." (quote) | The study applied VIPP‐SD, aimed at parental sensitivity and sensitive parental discipline. The first four intervention sessions each had their own themes, (1) "exploration versus attachment" (quote); (2) "centered around speaking for the child" (quote); (3) "the intervener stressed the importance of adequate and prompt responses to the child’s signals" (quote); (4) "the importance of sharing—both positive and negative—emotions (sensitivity) and promoting empathy for the child" (quote); (5 & 6) "aimed at consolidating intervention effects by integrating—in video feed‐back and discussion—all tips and feedback given in the previous sessions" (quote). |
| Yagmur 2014 | "To test the effectiveness of the video feedback intervention to promote positive parenting and sensitive discipline adapted to the specific child‐rearing context of Turkish families (VIPP‐TM) in the Netherlands" (quote), including second‐generation Turkish immigrant families with toddlers at risk for the development of externalising problems | "The VIPP‐TM program is a culturally sensitive adaptation of the VIPP‐SD program for Turkish minority families in the Netherlands, but follows the general procedures of the original program...The VIPP‐SD program is described in a detailed protocol and consists of six home visits. The first four visits each have their own themes regarding sensitivity and discipline, and the last two sessions are booster sessions in which the themes from previous sessions are reviewed once more." (quote) |
| Video Interaction Guidance (VIG) | ||
| Barlow 2016 | "To assess the potential of video interaction guidance to increase sensitivity in parents of preterm infants." (quote) | The study authors report that "VIG is a strengths‐based form of video feedback in which parents are invited to jointly observe and reflect on their own successful interactions with their baby...The core aspects of the model involve three home visits comprising (a) video recording the parent‐infant interaction during play or other aspects of care giving, (b) editing of the recording to select micro‐moments of interaction that demonstrate the infant's contact initiatives and the parents attuned response to these signals and (c) joint reviewing of the recordings with the parent." (quote) |
| Hoffenkamp 2015 | To evaluate the effectiveness of hospital‐based video interaction guidance in parents with moderately and very preterm babies | "Video recordings of parent‐infant interactions and the feedback from a VIG professional provide an opportunity for parents to observe, analyse and discuss the infant's behaviour and contact initiatives" (quote). In this study "VIG consisted of three sessions during the first week after birth" (quote), and included "(1) video‐recording parent‐infant interaction; (2) editing the video recordings; (3) reviewing the edited recordings with parents." (quote) |
| Lam‐Cassettari 2015 | To examine "the effect of a family‐focused psychosocial video intervention program on parent‐child communication in the context of childhood hearing loss" (quote) | Parents completed three sessions: "(a) a goal setting session; (b) three filming sessions of parent–child interaction in the family home, and (c) three shared review sessions in which three short video clips (demonstrating attuned responses linked to the family’s goal) were played so families could microanalyze and discuss." (quote) |
| Video feedback of Infant‐Parent Interaction (VIPI) | ||
| Høivik 2015 | To investigate "in a heterogenic community sample of families with interactional problems, whether VIPI would be more effective than standard care (TAU) received in the community" (quote) | VIPI involves at least 6 consultation sessions over a maximum period of 3 months focusing on (1) "Initiative of the infants to contact caregivers and initiate pauses in the dyadic exchange" (quote); (2) "Responses of caregivers" (quote); (3) "Following the child" (quote); (4) "Naming" (quote); (5) "Step‐by‐step guidance" (quote); (6) "Directing attention towards social interaction and exploration" (quote). In this study, "families in the VIPI group received eight video feedback sessions, with the last two sessions tailored to meet the individual family needs regarding any of the six topics in the manual" (quote). |
| Video self‐modelling with feedback | ||
| Benzies 2013 | To explore if fathers of late, preterm children who received video self‐modelling with feedback intervention would have better father‐child interaction skills when the child was 8 months old than fathers who received information only | Self‐modelling "involves the father's active participation that increases his cognitive awareness of specific behaviours such as infant cues and how to stimulate development" (quote). The intervention involved video recording a father‐infant play interaction and providing positive feedback and suggestions to enhance the interaction and language development. |
| Video feedback (non‐specified or other) | ||
| Bovenschen 2012 | To assess "the effectiveness of an attachment‐based short term intervention using video‐feedback" (quote) | Up to 10 sessions of home‐based video feedback |
| Green 2010 | To test a parent‐child communication‐focused intervention in children with core autism | A parent‐mediated communication‐focused intervention: "The intervention consisted of one‐to‐one clinic sessions between therapist and parent with the child present. The aim of the intervention was first to increase parental sensitivity and responsiveness to child communication and reduce mistimed parental responses by working with the parent and using video‐feedback methods to address parent‐child interaction... incremental development of the child's communication was helped by the promotion of a range of strategies such as action routines, familiar repetitive language and pauses...After an initial orientation meeting, families attended biweekly 2 hour clinic sessions for 6 months followed by booster sessions for 6 months (total 18). Between sessions families were also asked to do 30 mins of daily home practice." (quote) |
| Koniak‐Griffin 1992 | To evaluate "the effects of video tape instruction and feedback (video‐therapy) on mothering behaviours" (quote) | The intervention group received two home visits. Participants were "video taped during structured mother‐infant teaching episodes in their homes at 1 and 2 months postpartum" (quote). Participants "reviewed the video tapes with feedback from a professionally trained nurse who emphasised positive aspects of maternal behaviour" (quote) |
| Moran 2005 | To evaluate "the effectiveness of a brief intervention program designed to support adolescent mothers' sensitivity to their infants attachment signals" (quote) | A brief intervention programme (eight home visits) designed to support the mother's sensitivity to her child. The home visits (lasting approximately one hour) were "designed to provide mutually beneficial play interactions and the mother's enjoyment of her infant" (quote). The four goals of the programme included "to affirm parenting strengths already present in the mother...increase the mother's awareness of how her behaviour influenced her child's behaviour...look for ways to augment the mother's awareness of her infant's signals and for ways to establish positive experiences for both the mother and infant" (quote). |
| Moss 2011 | To evaluate the "efficacy of a short‐term attachment‐based intervention for changing risk outcomes for children of maltreating families" (quote) | The intervention consisted of "8 weekly home visits directed at the caregiver–child dyad and focused on improving caregiver sensitivity" (quote). The study authors describe that "All intervention sessions were primarily focused on reinforcing parental sensitive behavior by means of personalized parent–child interaction, video feedback, and discussion of attachment/emotion regulation‐related themes" (quote). |
| Seifer 1991 | To examine the effects of easy‐to‐use interaction coaching techniques on interaction style and developmental status of a population of mothers and their young children with developmental disabilities | "Interaction coaching" (quote; 10‐month programme). "Sessions lasted six minutes and parents were asked to play with their children as they would during a short break at home...After the initial taping session the video record was viewed by the mother and an interaction coach. Suggestions were then provided by the therapist for the mother to employ during interaction with her child...Another 6 minute interaction was then recorded that was reviewed by the intervener and could be used during the next week’s session. The procedure was repeated for a maximum of 6 sessions." (quote) |
| Stein 2006 | To test "whether video‐feedback treatment especially targeting mother‐child interaction would be superior to counselling in improving mother‐child interaction, especially mealtime conflict and infant weight and autonomy" (quote) | "Thirteen 1‐hour treatment sessions were offered in the mothers’ homes beginning when the infants were between 4 and 6 months old and completed by the time the infants were 12 months old. The intervention group received video‐feedback interactional treatment that was a modification of that developed by [Juffer et al]" (quote). Treatment consisted of three stages: "The first concentrated on the infant’s perspective, focusing on his or her signals...The second stage included the mother’s perspective...Third, as treatment progressed, the videotapes were used to help the mother identify and address potential triggers of mealtime conflict" (quote). |
IBASIS‐VIPP: Intervention within the British Autsim Study of Infant Siblings ‐ Video‐feedback Interaction to promote Positive Parenting; Mins: Minutes; TAU: Treatment as usual; VIG: Video Interaction Guidance; VIPI: Video‐feedback of Infant‐Parent Interaction; VIPP: Video‐feedback Interaction to promote Positive Parenting; VIPP‐AUTI: Video‐feedback Interaction to promote Positive Parenting ‐ Autism;VIPP‐LD: Video‐feedback Interaction to promote Positive Parenting ‐ Learning Difficulties; VIPP‐R: Video‐feedback Interaction to promote Positive Parenting ‐ Representational level; VIPP‐SD: Video‐feedback Interaction to promote Positive Parenting ‐ Sensitive Discipline; VIPP‐TM: Video‐feedback Interaction to promote Positive Parenting ‐ Turkish Minorities; VIPP‐V: Video‐feedback Interaction to promote Positive Parenting ‐ Visual or visual and intellectual disability.
Location
Seven studies were conducted in the Netherlands (Hodes 2017; Hoffenkamp 2015; Klein Velderman 2006; Platje 2018; Poslawsky 2015; Van Zeijl 2006; Yagmur 2014), five in the UK (Barlow 2016; Green 2010; Green 2015; Lam‐Cassettari 2015; Stein 2006), three in Canada (Benzies 2013; Moran 2005; Moss 2011), and two in the USA (Koniak‐Griffin 1992; Seifer 1991). One study apiece was conducted in Germany (Bovenschen 2012), Italy (Barone 2019), Lithuania (Kalinauskiene 2009), Norway (Høivik 2015), and Portugal (Negrão 2014).
Design
All but two studies were RCTs (Bovenschen 2012; Seifer 1991). Bovenschen 2012 was originally designed as an RCT but some mothers only agreed to take part if they could participate in the intervention, thereby undermining the randomisation. Seifer 1991 was a quasi‐RCT, with participants allocated based on the day of the week they attended a linked treatment programme.
Two of the 22 included RCTs employed a three‐arm design (Benzies 2013; Klein Velderman 2006). Klein Velderman 2006 allocated parents to either a video‐feedback group, a video‐feedback and discussion group, or a control group. In Benzies 2013, one group was allocated two visits with a video‐feedback intervention, the second group was allocated four visits with a video‐feedback intervention and the final group was allocated to a control condition.
The other studies employed a two‐arm design with parents allocated either to a video‐feedback intervention or control group (see Table 4).
Sample size
The number of dyads randomised in each trial ranged from 14 (Lam‐Cassettari 2015), to 237 (Van Zeijl 2006).
Recruitment
Two studies recruited participants from an inpatient hospital setting (Barlow 2016; Hoffenkamp 2015). The other 20 studies recruited participants from a community setting, including primary care, and hospital outpatient clinics.
Participants
The majority of studies (n = 14) randomised only mother‐child dyads. Seven studies randomised male as well as female caregiver and child dyads (Barlow 2016; Hodes 2017; Hoffenkamp 2015; Høivik 2015; Moss 2011; Platje 2018; Poslawsky 2015). Only one study randomised father‐child dyads (Benzies 2013).
The average age of carers, when reported, ranged from 17.16 years (Koniak‐Griffin 1992), to 42.6 years (Barone 2019).
Twelve studies had a mean age of participant children that was under one year at baseline (Barlow 2016; Benzies 2013; Bovenschen 2012; Green 2015; Hoffenkamp 2015; Høivik 2015; Kalinauskiene 2009; Klein Velderman 2006; Koniak‐Griffin 1992; Moran 2005; Seifer 1991; Stein 2006); the remaining 10 studies had a mean age of participant children that was over one year at baseline (Barone 2019; Green 2010; Hodes 2017; Lam‐Cassettari 2015; Moss 2011; Negrão 2014; Platje 2018; Poslawsky 2015; Van Zeijl 2006; Yagmur 2014). Many studies specified in their inclusion criteria that they were either recruiting babies (children aged under one year) or children (children aged one year or over); however, in some studies, their inclusion criteria included children both under and over one year of age.
Participants were recruited for a range of reasons including: child behaviour problems; parental diagnosis of an eating disorder; adverse family circumstances; parental depression; sensitivity problems; insecure attachment; parental intellectual disability; teenage or single parenthood (or both); migration status; preterm baby; adopted child; deaf children; parents who were being monitored by social services for child maltreatment; parents of children with a visual or visual and intellectual disability; and autistic children or children considered at risk of autism.
It is difficult to summarise the ethnicities of participants as different studies categorised this variable in different ways. Six studies did not report ethnicity (Bovenschen 2012; Hodes 2017; Hoffenkamp 2015; Klein Velderman 2006; Moss 2011; Poslawsky 2015). In 12 studies the majority of participants appeared to be from white European backgrounds (see Characteristics of included studies tables). One study recruited internationally adopted children (Barone 2019), and in one study the majority of participants were from African American or Hispanic backgrounds (Koniak‐Griffin 1992). Two studies used ethnicity as part of their inclusion or exclusion criteria (Negrão 2014; Yagmur 2014).
Type of video‐feedback intervention
Table 4 provides an overview of type of video‐feedback interventions that the included studies evaluated, organised by type. In summary:
10 studies implemented Video‐feedback Intervention to promote Positive Parenting (VIPP) or a variation of VIPP (VIPP with a representational component (VIPP‐R), VIPP and sensitive discipline (VIPP‐SD), VIPP adapted to autism (VIPP‐AUTI), VIPP adapted for Turkish mothers (VIPP‐TM), VIPP‐visual (VIPP‐V), VIPP adapted for fostered or adopted children (VIPP‐FC/A)): (Barone 2019; Green 2015; Hodes 2017; Kalinauskiene 2009; Klein Velderman 2006; Negrão 2014; Platje 2018; Poslawsky 2015; Van Zeijl 2006; Yagmur 2014);
Three studies included Video Interaction Guidance (VIG; Barlow 2016; Hoffenkamp 2015; Lam‐Cassettari 2015);
One study implemented Video‐feedback of Infant‐Parent Interaction (VIPI; Høivik 2015);
One study implemented video self‐modelling with feedback (Benzies 2013); and
Six studies implemented a non‐specified type of video feedback or another type not named above (Bovenschen 2012; Green 2010; Koniak‐Griffin 1992; Moran 2005; Moss 2011; Seifer 1991; Stein 2006).
Treatment intensity
Six studies had between one and five sessions of video feedback (Barlow 2016; Benzies 2013; Kalinauskiene 2009; Klein Velderman 2006; Koniak‐Griffin 1992; Poslawsky 2015); 12 studies had six to 10 sessions of video feedback (Barone 2019; Bovenschen 2012; Hoffenkamp 2015; Høivik 2015; Lam‐Cassettari 2015; Moran 2005; Moss 2011; Negrão 2014; Platje 2018; Seifer 1991; Van Zeijl 2006; Yagmur 2014); and four studies offered more than 10 sessions of video feedback (Green 2010; Green 2015; Hodes 2017; Stein 2006).
Monitoring of treatment fidelity
Two studies reported a quantitative measure of treatment fidelity (Green 2010; Green 2015). Ten studies reported having a process in place to monitor treatment fidelity, although they did not report a quantitative measure of treatment fidelity (Hodes 2017; Hoffenkamp 2015; Høivik 2015; Moran 2005; Moss 2011; Platje 2018; Poslawsky 2015; Stein 2006; Van Zeijl 2006; Yagmur 2014). The 10 remaining studies did not report any monitoring of treatment fidelity.
Comparisons
Eleven studies used either usual care (such as routine visits from community health staff or play support programmes) or no additional intervention for their control group (Barlow 2016; Bovenschen 2012; Green 2010; Green 2015; Hodes 2017; Hoffenkamp 2015; Høivik 2015; Klein Velderman 2006; Lam‐Cassettari 2015; Moss 2011; Platje 2018). The other 11 studies used some sort of inactive alternative treatment, such as telephone calls or videoing the parent‐child dyads, without providing any feedback.
Outcomes and outcome measures
Parental sensitivity
All studies measured parental sensitivity or used a measure that could act as a proxy.
Seven studies (Barone 2019; Høivik 2015; Klein Velderman 2006; Lam‐Cassettari 2015; Negrão 2014; Poslawsky 2015; Yagmur 2014), used the Emotional Availability Scale (Biringen 2000b; Biringen 2008).
Three studies (Bovenschen 2012, Kalinauskiene 2009; Klein Velderman 2006), used the Ainsworth Rating Scale (Ainsworth 1974; Ainsworth 1978), and one (Stein 2006), used an adapted version of this scale.
Two studies (Moran 2005; Moss 2011), used the Maternal Behaviour Q‐sort (Pederson 1999; Pederson 1995).
-
Six other studies used the following scales:
Barlow 2016 used the CARE‐Index (Crittenden 2001);
Benzies 2013 used the Parent Child Interaction Teach Scale (Sumner 1994);
Green 2015 used the Manchester Assessment of Caregiver‐Infant Interaction (Wan 2017);
Hoffenkamp 2015 used an adapted measure based on a coding scale from NICHD Early Child Care Research Network 2005;
Koniak‐Griffin 1992 used the Nursing Child Assessment Teaching Scale (Barnard 1978);
Platje 2018 used an adapted version of the National Institute of Child Health and Human Development Scales (Egeland and Heister 1993); and
Van Zeijl 2006 used measures for parental sensitivity that were taken from Egeland 1990.
Three studies relied on proxy measures (Green 2010; Hodes 2017; Seifer 1991).
Green 2010 used the proportion of parental communications with the child that were synchronous based on observation.
Hodes 2017 assessed harmonious parent‐child interaction (measured using the three‐bag procedure; NIHCD Early Child Care Research Network 2003).
Seifer 1991 used an observer to measure maternal responsive behaviour, but the report does not specify the type of scale used to code observations.
Fourteen studies measured parental sensitivity immediately postintervention (Barone 2019; Bovenschen 2012; Green 2015; Hodes 2017; Hoffenkamp 2015; Høivik 2015; Kalinauskiene 2009; Koniak‐Griffin 1992; Lam‐Cassettari 2015; Moran 2005; Moss 2011Platje 2018; Poslawsky 2015; Seifer 1991), and 17 measured it in the short term (Barlow 2016; Barone 2019; Benzies 2013; Bovenschen 2012; Green 2010; Hodes 2017; Hoffenkamp 2015; Høivik 2015; Klein Velderman 2006; Koniak‐Griffin 1992; Lam‐Cassettari 2015; Negrão 2014; Platje 2018; Poslawsky 2015; Stein 2006; Van Zeijl 2006; Yagmur 2014). None of the studies measured it in the medium term, and just three studies measured it in the long term (Kalinauskiene 2009; Klein Velderman 2006; Moss 2011).
Parental reflective functioning
No study measured this outcome.
Attachment security
Four studies measured child attachment security (Kalinauskiene 2009; Klein Velderman 2006; Moran 2005; Moss 2011), and all but one study, Klein Velderman 2006, measured this outcome postintervention. Klein Velderman 2006 assessed attachment security in both the short and long term.
Three studies, Klein Velderman 2006, Moran 2005 and Moss 2011, used the Strange Situation Procedure (Ainsworth 1978) to measure attachment security, and two studies, Kalinauskiene 2009 and Klein Velderman 2006, used the Attachment Q‐sort (Waters 1985; Waters 1987).
Adverse effects
Parental stress
Eight studies measured parental stress (Barlow 2016; Benzies 2013; Hodes 2017; Kalinauskiene 2009; Klein Velderman 2006; Negrão 2014; Platje 2018; Poslawsky 2015). Four studies measured the outcome postintervention (Hodes 2017; Kalinauskiene 2009; Platje 2018; Poslawsky 2015). Six studies measured this outcome in the short term (Barlow 2016; Benzies 2013; Klein Velderman 2006; Negrão 2014; Platje 2018; Poslawsky 2015). One study measured this outcome at an unspecified follow‐up time point (Hodes 2017).
Two studies, Barlow 2016 and Benzies 2013, used a version of the Parenting Stress Index (full or short form; Abidin 1995; Terry 1991). Three studies, Kalinauskiene 2009, Negrão 2014 and Poslawsky 2015, used the Parenting Daily Hassles or Daily Hassles Questionnaire (Crnic and Greenberg 1990; Kanner 1981). One study, Klein Velderman 2006, used the Support and Stress Questionnaire (Van den Boom 1988). Two studies, Platje 2018 and Hodes 2017, used the Nijmeegse Ouderlijke Stress Index ‐ Dutch version of the Parenting Stress Index (Abidin 1983; De Brock 1992).
Parental anxiety
Only two studies measured parental anxiety. Barlow 2016 measured parental anxiety in the short term using the Hospital Anxiety and Depresssion Scale (Zigmond 1983); and Hoffenkamp 2015 measured parental anxiety in the short and medium term using the State‐Trait Anxiety Inventory (Spielberger 1983).
Child mental health
One study, Green 2010, measured child mental health in the long term, using the Development and Well‐being Assessment (Goodman 2011).
Child physical and socioemotional development
Seifer 1991 measured child psychomotor development at postintervention using the Uzgiris and Hunt Ordinal Scales of Development (Uzgiris 1975); all seven subscales were measured individually.
Five studies measured aspects of children's socioemotional development (Green 2010; Green 2015; Høivik 2015; Poslawsky 2015; Seifer 1991). Høivik 2015 measured this immediately postintervention and in the medium term using the Ages and Stages Questionnaire (Squires 2002). Poslawsky 2015 measured it at both postintervention and in the short term using the Early Social Communication Scales (Mundy 2003). Green 2010 assessed this in the short term using the Vineland Adaptive Behaviour Scales (VABS; Sparrow 2005), and in the long term using the Strengths and Difficulties Questionnaire (Goodman 1997). Green 2015 used the VABS to measure this outcome in the short and long term (Sparrow 2005). Seifer 1991 measured child mental development using the Bayley Scales of Infant Development at postintervention (Bayley 1969).
Child behaviour
Five studies measured child behaviour at different time points, using various versions of the Child Behaviour Checklist (CBCL; Achenbach 1992; Achenbach 2000). Moss 2011 and Barone 2019 measured children's behaviour postintervention; and Van Zeijl 2006 and Barone 2019 did so in the short term. Two studies measured it in the long term (Kalinauskiene 2009; Klein Velderman 2006).
Three studies reported externalising behaviour, which is a domain of child behaviour (Barone 2019; Moss 2011; Van Zeijl 2006), using the CBCL (Achenbach 2000). Two studies reported it at postintervention (Barone 2019; Moss 2011), and two reported it at short‐term follow‐up (Barone 2019; Van Zeijl 2006). No study measured it at long‐term follow‐up.
Costs
None of the studies reported data on costs.
Funding sources
These are listed in the Characteristics of included studies tables. Almost all studies reported some sort of external funding, from a charitable organisation (n = 7) and/or public body (n = 18). No studies reported commercial funding.
Excluded studies
We formally excluded 37 completed studies, consisting of 47 reports, and one ongoing study, details of which can be found in the Characteristics of excluded studies tables.
We excluded completed studies for the following reasons: intervention had no video‐feedback component (4 studies); intervention contained multiple sessions of non‐video‐feedback intervention activities (14 studies); used video feedback as part of a multicomponent intervention (6 studies); study did not measure parental sensitivity, child attachment or reflective functioning outcomes (4 studies); study was not an RCT or quasi RCT (4 studies); caregivers did not match this review's inclusion criteria (3 studies); study was a comparison between two active interventions rather than an intervention and inactive alternative intervention (2 studies).
We excluded one ongoing study because it does not measure parental sensitivity, child attachment or reflective functioning outcomes.
Ongoing studies
We identified five ongoing studies, described in further detail here: Characteristics of ongoing studies. All five studies are RCTs. Three of the studies include parent‐child dyads (Firk 2015; ISRCTN92360616; NCT03052374), one study includes parents and twins (Euser 2016), and one includes foster parents and foster children (Schoemaker 2018). Two studies are being conducted in the Netherlands (Euser 2016; Schoemaker 2018), one study in Germany (Firk 2015), one in Ireland (ISRCTN92360616), and one in Canada (NCT03397719).
Three of the studies include a component of video feedback (Firk 2015; ISRCTN92360616; NCT03052374), and two include an adaptation of VIPP (Positve Parenting and Sensitive Discipline in twin families (VIPP‐twin; Euser 2016); Positive Parenting for Foster Care (VIPP‐FC; Schoemaker 2018)). Three studies used standard care as their control intervention (Firk 2015; ISRCTN92360616; NCT03052374), and two studies used phone calls as their control intervention (Euser 2016; Schoemaker 2018).
Of these studies, two were funded through public sector funding sources (Euser 2016; Firk 2015); two were funded through charitable sources (ISRCTN92360616; Schoemaker 2018), and one did not declare a source of funding (NCT03052374).
Studies awaiting classification
There was one report that we could not obtain in full (Mendelsohn 2008), despite a request to the first author (Smith 2018i [pers comm]). This is listed under Characteristics of studies awaiting classification.
Risk of bias in included studies
We present the 'Risk of bias' tables for each included study beneath the Characteristics of included studies tables. Figure 2 summarises the 'Risk of bias' assessments across all outcomes, and Figure 3 summarises these assessments across all included studies.
2.
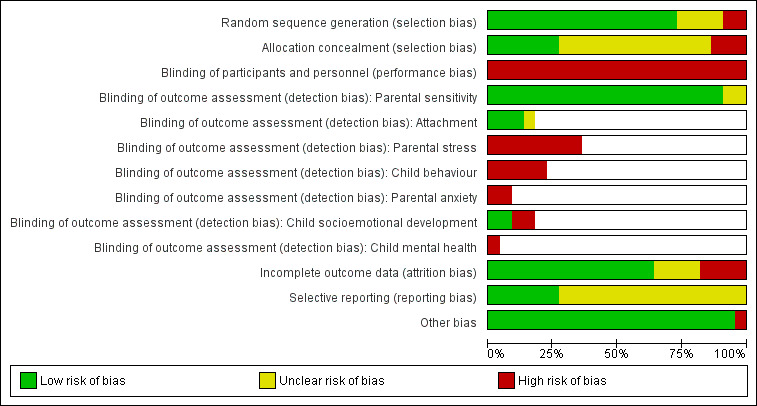
'Risk of bias' graph: review authors' judgements about each 'Risk of bias' item presented as percentages across all included studies
3.
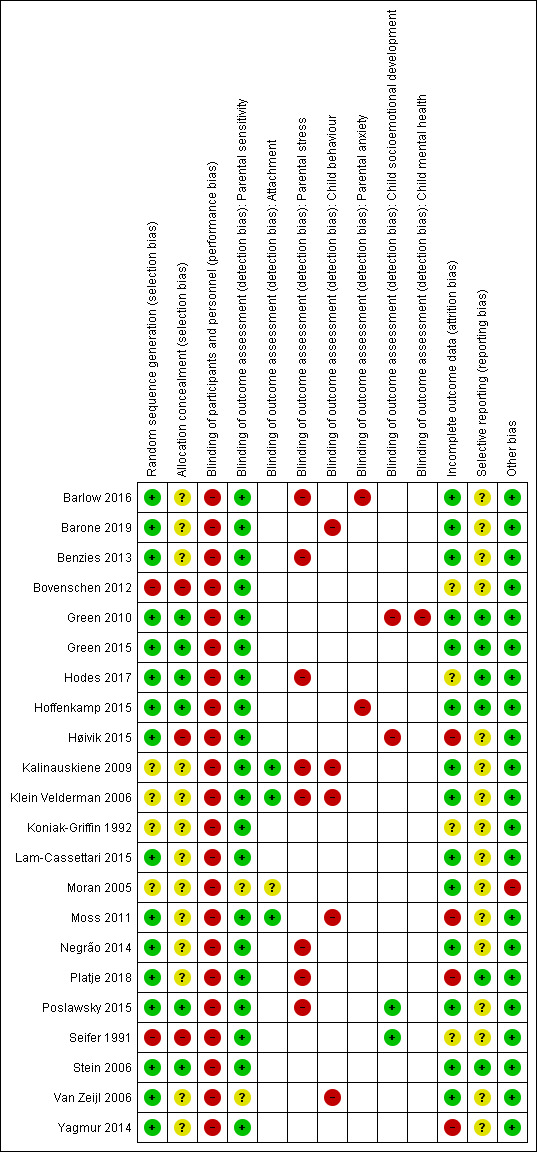
'Risk of bias' summary: review authors' judgements about each 'Risk of bias' item for each included study
Allocation
Random sequence generation
We assessed the risk of selection bias from randomisation to be low in 16 studies (Barlow 2016; Barone 2019; Benzies 2013; Green 2010; Green 2015; Hodes 2017; Hoffenkamp 2015; Høivik 2015; Lam‐Cassettari 2015; Moss 2011; Negrão 2014; Platje 2018; Poslawsky 2015; Stein 2006; Van Zeijl 2006; Yagmur 2014). We assessed two studies as having a high risk of selection bias from poor randomisation (Bovenschen 2012; Seifer 1991); for instance due to randomisation based on the day of the week. Four studies stated that participants were randomised, but did not state how this was carried out (Kalinauskiene 2009; Klein Velderman 2006; Koniak‐Griffin 1992; Moran 2005), so we assessed them as at unclear risk of bias.
Allocation concealment
We assessed the risk of selection bias to be low in six included studies across allocation concealment (Green 2010; Green 2015; Hodes 2017; Hoffenkamp 2015; Poslawsky 2015; Stein 2006). We assessed 13 studies as having an unclear risk of allocation bias, as they did not give sufficient information on how allocation took place (Barlow 2016; Barone 2019; Benzies 2013; Kalinauskiene 2009; Klein Velderman 2006; Koniak‐Griffin 1992; Lam‐Cassettari 2015; Moran 2005; Moss 2011Negrão 2014; Platje 2018; Van Zeijl 2006; Yagmur 2014). We rated three studies at high risk of selection bias: Bovenschen 2012, as the study authors stated that some participants only agreed to take part if they were allocated to a specific arm of the study; Høivik 2015 due to the use of consecutive randomisation; and Seifer 1991 as allocation was based on presentation on a certain day of the week.
Blinding
Given the nature of the intervention, we judged it impossible to truly blind any of the participants, so we rated all studies at high risk of performance bias. Two studies did attempt to address this issue by giving participants limited information about the purpose of the study (Benzies 2013; Moran 2005); however, in our judgement, this was not sufficient to blind participants.
We judged detection bias relating to outcomes that were relevant to this review only. We rated each outcome separately. The results are presented below.
Primary outcomes
Parental sensitivity
All 22 included studies measured this outcome or proxy domain. All except two studies, Moran 2005 and Van Zeijl 2006, were able to adequately blind the outcome assessor(s), so we rated them at low risk of detection bias. As Moran 2005 and Van Zeijl 2006 did not describe the blinding in sufficient detail, we rated them as having an unclear risk of detection bias.
Parental reflective functioning
None of the included studies measured this outcome.
Attachment security
Four studies measured this outcome (Kalinauskiene 2009; Klein Velderman 2006; Moran 2005; Moss 2011). We rated one study, Moran 2005 at unclear risk of detection bias, and the other three studies at low risk of detection bias, as they blinded assessors.
Adverse effects
We examined parental stress and parental anxiety. Eight studies reported parental stress (Barlow 2016; Benzies 2013; Hodes 2017; Kalinauskiene 2009; Klein Velderman 2006; Negrão 2014; Platje 2018; Poslawsky 2015). All of these studies used self‐report scales, so we rated all at high risk of detection bias.
Two studies reported parental anxiety (Barlow 2016; Hoffenkamp 2015). Again, both of these studies used self‐report scales, so we rated them at high risk of detection bias.
Secondary outcomes
Child mental health
A single study measured child mental health (Green 2010). They used the Development and Well‐Being Assessment (DAWBA), which uses a parental assessment of their children. Consequently, we rated it at high risk of detection bias.
Child physical and socioemotional development
Four studies measured children's socioemotional development (Green 2010; Høivik 2015; Poslawsky 2015; Seifer 1991). Green 2010 and Høivik 2015 used scales based on parental assessments of their children, so we rated these studies at high risk of detection bias. Poslawsky 2015 and Seifer 1991 used blinded raters so we rated these studies at low risk of detection bias.
Child behaviour
Five studies measured child behaviour (Barone 2019; Kalinauskiene 2009; Klein Velderman 2006; Moss 2011; Van Zeijl 2006). All of these studies used scales based on parental ratings of their child's behaviour, so we rated all as being at high risk of detection bias.
Incomplete outcome data
Of the 22 included studies, we assessed 14 as being at low risk of attrition bias, due to either appropriate methods of imputation by the study authors, very low or no attrition, or attrition that was balanced across all arms of the study (Barlow 2016; Barone 2019; Benzies 2013; Green 2010; Green 2015; Hoffenkamp 2015; Kalinauskiene 2009; Klein Velderman 2006; Lam‐Cassettari 2015; Moran 2005; Negrão 2014; Poslawsky 2015; Stein 2006; Van Zeijl 2006); four as unclear risk of attrition bias because there was unclear reporting of number of, or reason for, dropouts (Bovenschen 2012; Hodes 2017; Koniak‐Griffin 1992; Seifer 1991); and four as high risk of attrition bias due to unequal attrition across arms that could have been for reasons related to the intervention (Høivik 2015; Moss 2011; Platje 2018; Yagmur 2014).
Selective reporting
The majority of studies did not have protocols, making it difficult to judge whether there was reporting bias. We judged 16 studies as having an unclear risk of reporting bias because they appeared to report all outcomes in their Methods section but did not have a protocol available (Barlow 2016; Barone 2019; Benzies 2013; Bovenschen 2012; Høivik 2015; Kalinauskiene 2009; Klein Velderman 2006; Koniak‐Griffin 1992; Lam‐Cassettari 2015; Moran 2005; Moss 2011; Negrão 2014; Poslawsky 2015; Seifer 1991; Van Zeijl 2006; Yagmur 2014). We rated six studies at low risk of reporting bias because they reported all prespecified outcomes from their published protocols (Green 2010; Green 2015; Hodes 2017; Hoffenkamp 2015; Platje 2018; Stein 2006).
For parental sensitivity, we compared published results with unpublished results, to test for publication bias in the three studies where this was possible (Barone 2019; Hoffenkamp 2015; Klein Velderman 2006). There was no evidence of a difference between the two groups of studies.
For parental stress, we compared published results with unpublished results, to test for publication bias in two studies (Klein Velderman 2006; Negrão 2014). We found no difference; neither group showed evidence of a difference between intervention and control groups.
Other potential sources of bias
We rated Moran 2005 at high risk of other bias as they did not report the maternal sensitivity outcome data completely (data were missing SDs or SEs).
Effects of interventions
See: Table 1
We summarise the results of our meta‐analyses below. We also report the results from single studies that we did not combine in a meta‐analysis because: not enough studies reported that outcome; data were missing and we were unable to obtain them from the study authors; the outcome was measured at a different time point to other studies reporting that outcome, or the study measured the outcome at multiple similar time points, meaning that we selected a single time point for the meta‐analysis. In addition, we present the results of a moderator analysis for the outcome parental sensitivity; we decided post hoc to undertake this analysis (see Differences between protocol and review).
We have organised results for the main comparison under headings corresponding to the primary and secondary outcomes outlined in the Types of outcome measures section.
Numbers given are the total number of participants randomised. Where it has been possible to calculate an effect size, we have reported this with 95% CI. Where the calculated effect size had a P value less than 0.05, we have stated whether or not the result favours the intervention group.
Table 1 summarises the main results of our meta‐analyses.
Video feedback versus no intervention or inactive alternative intervention
Primary outcomes
Parental sensitivity
Using a random‐effects model, we conducted a meta‐analysis of data from 20 studies (1757 parent‐child dyads) that measured the effects of video‐feedback on parental sensitivity from postintervention to six months' follow‐up (Barlow 2016; Barone 2019; Benzies 2013; Bovenschen 2012; Green 2010; Green 2015; Hodes 2017; Hoffenkamp 2015; Høivik 2015; Kalinauskiene 2009; Klein Velderman 2006; Lam‐Cassettari 2015; Moss 2011; Negrão 2014; Platje 2018; Poslawsky 2015; Seifer 1991; Stein 2006; Van Zeijl 2006; Yagmur 2014). We have presented data for mothers and fathers from Hoffenkamp 2015 separately as this is how the data were provided to us by the study authors. We have presented data for Benzies 2013 and Klein Velderman 2006 with two treatment groups, as these were three‐armed studies where both treatment groups in the study met our inclusion criteria. Details of how we managed unit of analysis issues are described in Unit of analysis issues.
The results suggest evidence favouring video feedback compared with the control group (SMD 0.34, 95% CI 0.20 to 0.49, Analysis 1.1). There was evidence of moderate heterogeneity, meaning that the observed variation is likely to be due to statistical heterogeneity (Tau2 = 0.07; Chi2 = 49.21, df = 22 (P = 0.0008); I2 = 55%). The GRADE certainty rating for this meta‐analysis was moderate; we downgraded due to inconsistency (moderate heterogeneity that was not explained by the subgroup analyses).
1.1. Analysis.
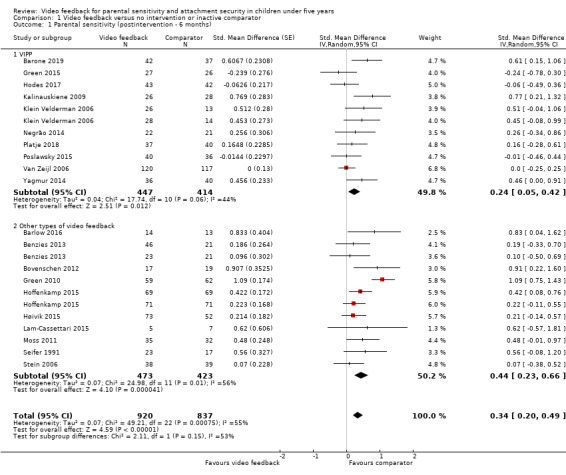
Comparison 1 Video feedback versus no intervention or inactive comparator, Outcome 1 Parental sensitivity (postintervention ‐ 6 months).
We drew a funnel plot (estimating differences in treatment effects against their SE) for the outcome 'parental sensitivity' as this was the only outcome with 10 or more studies that provided data. Figure 4 shows no major asymmetry for this comparison when all studies were included. We ran Egger's regression test for assessing funnel plot asymmetry; there was no evidence for funnel plot asymmetry (P = 0.281). However, when we removed Green 2010, Egger's regression test provided evidence for funnel plot asymmetry (P value = 0.022). The appearance of the funnel plot suggests that the asymmetry might be due to small study effects.
4.
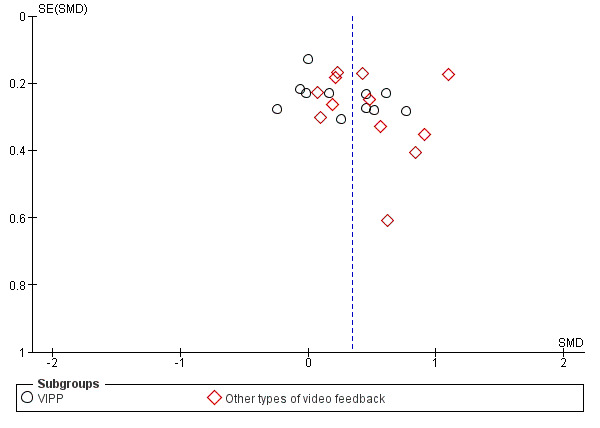
Funnel plot of comparison: 1. Primary outcomes, outcome: 1.1 parental sensitivity (postintervention ‐ 6 months)
Single study results (follow‐up only)
It should be noted that we included postintervention data from all of the following studies in the meta‐analysis for parental sensitivity, except Koniak‐Griffin 1992 and Moran 2005. The following data represent results for later follow‐up time points from these studies, and the single study results are all for later time periods.
Barone 2019 measured maternal sensitivity at six months' follow‐up. The six‐month results were not reported in the study, but the study authors provided us with unpublished means, number of participants (n) and SDs (intervention group: mean = 25.88, SD = 2.8, n = 42; control group: mean = 22.13, SD = 4.13, n = 37). We used these to calculate an SMD of 1.07 (95% CI 0.59 to 1.54), suggesting evidence of a difference between groups.
Bovenschen 2012 reported no evidence of an effect of the intervention at three months' follow‐up. The study authors provided the following unpublished data to us: intervention group: mean = 2.91, SD = 1.89, n = 17; control group: mean = 2.36, SD = 1.36, n = 19). A P value is not reported for this comparison; we used the data reported to calculate an SMD of 0.33 (95% CI −0.33 to 0.99), suggesting no evidence of a difference between groups.
Green 2010 reported the impact on maternal sensitivity 5.75 years after the end of the trial. At 5.75 years there was not strong evidence of a difference between the groups (video‐feedback group: mean = 44.4%, SD = 16.1%, n = 59; comparator group: mean = 43.1%, SD = 15.7%, n = 62; log OR of parent synchrony in video‐feedback group versus comparator group: 0.02 (bootstrap 95% CI −0.30 to 0.36)).
Hodes 2017 reported the impact on maternal sensitivity at three months' follow‐up. At three months' follow‐up there was not strong evidence of a difference between the groups (video‐feedback group: mean = 4.80, SD = 0.63, n = 43; comparator group: mean = 4.84, SD = 0.71, n = 42; repeated measures analysis of variance (ANOVA): F (2, 166) = 0.49, P = 0.61).
Hoffenkamp 2015 reported medium‐term (six months) outcomes for fathers and mothers. At six months' follow‐up there was no evidence of a difference between the two groups (mothers: MD = 0.29, SD = 0.22, P = 0.19; fathers: MD = 0.12, SD = 0.23, P = 0.60). We did not include six‐month follow‐up outcomes in the meta‐analysis as this would have meant two time points from a single trial in the same meta‐analysis.
Koniak‐Griffin 1992 measured maternal sensitivity as part of the NCATS (Nursing Child Assessment Teaching Scale) assessment. We were unable to obtain a breakdown of the data from the study authors, and so could not include them in the meta‐analysis.
Lam‐Cassettari 2015 reported results at three months' follow‐up, but by this time participants in the waiting‐list control group had received the intervention, so the comparison does not fit with the review question.
Moran 2005 measured maternal sensitivity at postintervention and at 12 months' follow‐up and reported that, "none of the t‐tests comparing the Intervention and Comparison group means at each age were significant". The data were not reported and the study author was unable to provide them when requested.
Platje 2018 reported parental sensitivity at three months' follow‐up. The study authors found no strong evidence of a difference between groups with regards to parental sensitivity at three months postintervention (video‐feedback group: mean = 16.39, SD = 1.96, n = 37; comparator group: mean = 16.42, SD = 2.33, n = 40). Repeated measures ANOVA showed no evidence of an interaction between time and condition (Time × Condition interaction F (1, 75) = 0.13, P = 0.715).
Parental reflective functioning
None of our included studies measured or reported data on this outcome.
Attachment security
As described in Measures of treatment effect, we combined data from studies that measured OR separately to those that measured means.
Two studies (Moran 2005; Moss 2011; 166 parent‐child dyads) measured this outcome using the Strange Situation Procedure (Ainsworth 1974), at postintervention. The pooled analysis of these studies using OR under a random‐effects assumption resulted in evidence favouring the intervention (OR 3.04, 95% CI 1.39 to 6.67, Analysis 1.2). We did not assess heterogeneity due to the small number of studies included in this meta‐analysis. We rated the certainty of this evidence as very low using GRADE, due to risk of bias (we rated most domains in the 'Risk of bias' assessment at high or uncertain risk of bias), imprecision (low number of participants, leading to wide CI) and publication bias (few studies in this review reported this outcome).
1.2. Analysis.
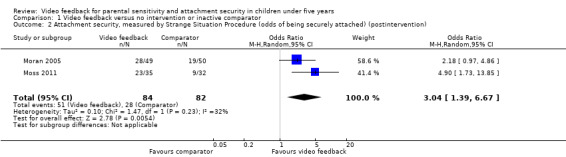
Comparison 1 Video feedback versus no intervention or inactive comparator, Outcome 2 Attachment security, measured by Strange Situation Procedure (odds of being securely attached) (postintervention).
Two other studies (Kalinauskiene 2009; Klein Velderman 2006; 131 parent‐child dyads) measured this outcome using the Attachment Q‐sort, with scores ranging from +1.00 for the perfectly secure child to −1.00 for the most insecure child (Waters 1985; Waters 1987). The time points of the data combined were quite different (one study reported data at postintervention and the other study at 12 months postintervention). The pooled analysis of these studies using SMD under a random‐effects assumption found no evidence of a difference between intervention and control groups (SMD 0.02, 95% CI −0.33 to 0.38, Analysis 1.3). We did not assess heterogeneity due to the small number of studies included in this meta‐analysis. We rated the certainty of this evidence as very low using GRADE: we downgraded one level for risk of bias (we rated most domains in the 'Risk of bias' assessment at high or uncertain risk of bias); one level due to imprecision (low number of participants, leading to wide CI); and one level due to publication bias (few studies in this review report this outcome).
1.3. Analysis.

Comparison 1 Video feedback versus no intervention or inactive comparator, Outcome 3 Attachment security, measured by Attachment Q‐sort (any duration of follow‐up).
Single study results
One study, Klein Velderman 2006, did not report data in a way that we could use in the meta‐analysis. The study found that there was no evidence that attachment security was different between the intervention and control group in the short term (VIPP group compared to control group: d = 0.33, P = 0.11 (one‐tailed), n = 55; VIPP‐R group compared to control group: d = 0.12, P = 0.33 (one‐tailed), n = 53).
Adverse effects
Parental stress
We pooled data from eight studies (537 parent‐child dyads) reporting data at postintervention or short‐term follow‐up (Barlow 2016; Benzies 2013; Hodes 2017; Kalinauskiene 2009; Klein Velderman 2006; Negrão 2014; Platje 2018; Poslawsky 2015). A random‐effects meta‐analysis did not show any strong evidence of a difference between intervention and control groups (SMD −0.09, 95% CI −0.26 to 0.09, Analysis 1.4). Heterogeneity was low (Tau2 = 0.00; Chi2 = 6.36, df = 8 (P = 0.61); I2 = 0%). We rated the certainty of this evidence as low using GRADE. We downgraded one level for risk of bias (we rated most domains in the 'Risk of bias' assessment at high or uncertain risk of bias) and one level due to imprecision (low number of participants, leading to wide CI).
1.4. Analysis.
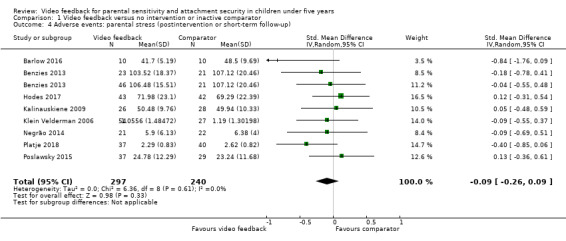
Comparison 1 Video feedback versus no intervention or inactive comparator, Outcome 4 Adverse events: parental stress (postintervention or short‐term follow‐up).
Single study results: three studies reported the impact of video feedback on parental stress in ways that we could not include in the meta‐analysis (Hodes 2017; Platje 2018; Poslawsky 2015).
Hodes 2017 measured the impact of video‐feedback at an unspecified follow‐up time point, reporting no evidence of a difference between intervention and control groups on a repeated measures multivariate ANOVA (MANOVA) (video‐feedback group: mean = 70.4, SD = 24.87, n= 43; comparator group: mean = 72.14, SD = 24.75, n = 42; F (1.57, 130, 6) = 4.39, P = 0.02). We did not include these data in the meta‐analysis as we used data provided by the same study at postintervention.
Platje 2018 reported the impact on parents' stress levels at postintervention and six months' follow‐up. The postintervention data are included in the meta‐analysis. The study found no evidence of a difference between intervention and control groups at six months' follow‐up using a repeated measures ANOVA (video‐feedback group: mean = 2.36, SD = 0.94, n = 37; control group: mean = 2.58, SD = 0.90, n = 40; F (1, 75) = 3.52, P = 0.07, η2 = 0.05).
Poslawsky 2015 measured parental stress at three months, but did not report it and were not able to provide the data when requested.
Parental anxiety
We combined data from two studies (311 parent‐child dyads), measured at short‐term follow‐up, using a random‐effects model (Barlow 2016; Hoffenkamp 2015). Data for mothers and fathers in Hoffenkamp 2015 are included separately, as this is how the data were provided to us. The meta‐analysis found no strong evidence of a difference between the intervention group and the control group (SMD −0.28, 95% −0.87 to 0.31, Analysis 1.5). We did not assess heterogeneity due to the small number of studies included in this meta‐analysis. We rated the evidence as very low certainty using GRADE. We downgraded one level due to imprecision (low number of participants, leading to wide CI), one level due to publication bias (few studies in this review reported this outcome) and one level due to inconsistency (high heterogeneity).
1.5. Analysis.
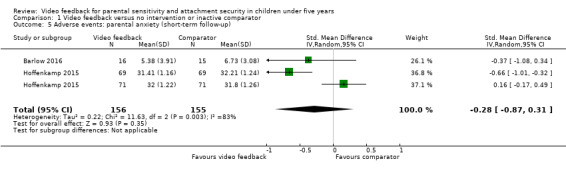
Comparison 1 Video feedback versus no intervention or inactive comparator, Outcome 5 Adverse events: parental anxiety (short‐term follow‐up).
Secondary outcomes
Child mental health
Only one study, Green 2010, measured the rate of child mental illness at long‐term follow‐up, and found no strong evidence of a difference between intervention and control group (log odds of depression in video‐feedback group (n = 50) versus comparator group (n = 44): 0.07 (bootstrap CI −0.85 to 1.03); log odds of conduct/oppositional disorder in video‐feedback group (n = 50) versus comparator group (n = 44): −0.13 (bootstrap CI −1.08 to 0.72); log odds of hyperkinesis in video‐feedback group (n = 50) versus comparator group (n = 44): 0.11 (bootstrap CI −0.70 to 0.93); log odds of anxiety/OCD in video‐feedback group (n = 50) versus comparator group (n = 46): 0.51 (bootstrap CI −0.33 to 1.51).
Child physical and socioemotional development
Four studies measured elements of child socioemotional development in ways that were too clinically different for meta‐analysis to be appropriate (Green 2010; Høivik 2015; Poslawsky 2015; Seifer 1991).
Green 2010 found no strong evidence of a difference between intervention and control groups with regards to prosocial behaviour (log odds of prosocial behavior in video‐feedback group (n = 59) versus control group (n = 62): 0.73 (bootstrap 95% CI −0.08 to 1.64) or peer problems (log odds of peer problems in video‐feedback group (n = 59) versus control group (n = 61): 0.64 (bootstrap 95% CI −0.21 to 1.62)).
Høivik 2015 reported no strong evidence of a difference postintervention between intervention and control groups with regards to their score on the socioemotional element of the Ages and Stages Questionnaire (video‐feedback group: mean = 26.21, SD = 19.61, n = 37; comparator group: mean = 25.74, SD = 17.02, n = 27; P = 0.17). At six months postintervention there was evidence that the intervention group had fewer concerns regarding their child's socioemotional development than the control group (video‐feedback group: mean = 20.44, SD = 13.45, n = 22; comparator group: mean = 25, SD = 16.53, n = 27; P = 0.02).
Poslawsky 2015, after controlling for school attendance, reported evidence that the video‐feedback group (n = 38) had better scores than the comparator group (n = 34) on measures of initiating joint attention (f = 2.35, df = 8, P = 0.03, ƞ2 = i) but not reciprocating joint attention.
Seifer 1991 measured child mental development (measured by Bayley Scales of Infant Development) and child psychomotor development (measured by the Uzgiris and Hunt Ordinal Scales of Development ‐ the study authors report measuring all seven subscales individually) at postintervention. However, they did not report these data did not respond to our request for the data (Smith 2019b [pers comm]).
Child behaviour
We pooled data from two studies (119 parent‐child dyads) looking at child behaviour in the long term (Kalinauskiene 2009; Klein Velderman 2006). A random‐effects meta‐analysis found no strong evidence of a difference between intervention and control groups (SMD 0.04, 95% CI −0.33 to 0.42, Analysis 1.6). We did not assess heterogeneity due to the small number of studies included in this meta‐analysis. The GRADE certainty rating was very low: we downgraded one level for risk of bias (we rated most domains in the 'Risk of bias' assessment at high or uncertain risk of bias); one level due to imprecision (low number of participants, leading to wide CI) and one level due to publication bias (few studies in this review reported this outcome).
1.6. Analysis.
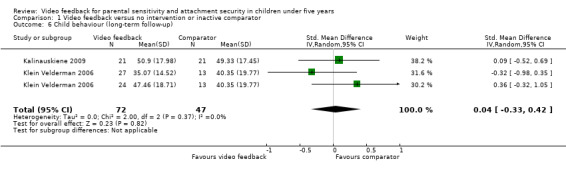
Comparison 1 Video feedback versus no intervention or inactive comparator, Outcome 6 Child behaviour (long‐term follow‐up).
Single study results
Three studies measured aspects of child behaviour that we could not include in a meta‐analysis: one study reported the data at a different time point to other studies reporting this outcome (Barone 2019); and the other studies reported elements of child behaviour at two very different time points (Moss 2011; Van Zeijl 2006).
Barone 2019 measured child behaviour at postintervention and six months' follow‐up. They reported results for externalising behaviour in their published report. The study authors reported that there was no evidence of an effect of the intervention at either time point for any of the outcomes measured, although they did not report a P value. The data reported at postintervention were as follows: video‐feedback group: mean = 16.6, SD = 9.5, n = 44; control group: mean = 14.2, SD = 10.4, n = 39. We used these data to calculate an SMD of 0.24 (95% CI −0.19 to 0.67). The data they reported at six months' follow‐up were as follows: video‐feedback group: mean = 16.1, SD = 10.9, n = 44; control group: mean = 12.7, SD = 10.6, n = 39. We used these data to calculate an SMD of 0.31 (95% CI −0.12 to 0.75). There is no evidence of an effect at either time point.
Moss 2011 reported no strong evidence of a difference between intervention and control groups at postintervention for internalising behaviour (video‐feedback group: mean = 54.43, SD = 7.44, n = 35; comparator group: mean = 55.56, SD =11.45, n = 32) or externalising behaviour (video‐feedback group: mean = 57.85, SD = 9.84, n = 35; comparator group: mean = 57.54, SD = 12.61, n = 32). P values were not reported by the review authors. We used the data reported to calculate an SMD for internalising behaviour of −0.12 (95% CI −0.60 to 0.36), showing no evidence of a difference between groups. For externalising behaviour, we calculated an SMD of 0.03 (95% CI −0.45 to 0.51), again showing no evidence of a difference between groups.
Van Zeijl 2006 reported no strong evidence of a difference between intervention and control groups for externalising behaviour at long‐term follow‐up (video‐feedback group: mean = 21.55, SD = 9.08, n = 83; comparator group: mean = 21.36, SD 8.62, n = 74). P values were not reported. We used the data reported to calculate an SMD of 0.02 (95% CI −0.29 to 0.33), demonstrating no evidence of a difference between groups.
Moderator analysis for parental sensitivity
Moderator analysis
Appendix 3 reports the overall effects by individual moderator. Three studies contained in this moderator analysis have two separate intervention groups (Benzies 2013; Hoffenkamp 2015; Klein Velderman 2006), meaning that for this part of the analysis, k (number of studies) = 23 studies, rather than 20 studies. Adding these as individual studies potentially biases the test statistic, as these intervention groups are not statistically independent. The usual solution to this problem is to conduct a multilevel meta‐analysis; however, the small number of related studies makes this unviable.
Notably, all subgroups except 'more than 10 sessions of video feedback' and studies with ‘only fathers’ and 'both parents' show evidence of an overall treatment effect, measured as SMDs (d). Substantively, the disability subgroup had the largest effect size (d = 0.49**, 95% CI 0.16 to 0.82). This suggests that some moderator effects may exist for some study characteristics when considered individually. For all moderators, heterogeneity is I2 greater than 50%, with evidence of residual heterogeneity (QE).
Figure 5 reports the results from the meta‐regression with all three prespecified moderators for k = 23 studies. There is no evidence that jointly the type of intervention, intervention duration, or gender of the participating carer reduce heterogeneity (Qbetween (F(df1moderators = 7, df2studies = 17) = 1.008, P = 0.4429; R2< 0.01%)), and substantial between‐study heterogeneity still exists (QE (df = 17) = 39.77, P = 0.014; though I2 = 55.6%, see Appendix 4). In addition, none of the three moderators in the meta‐regression are statistically significant (at α (alpha) = 0.05). Parent gender (both parents versus only mothers or only fathers) potentially has a statistically significant negative moderation effect, though only at α = 0.1. This suggests that, when we consider the three prespecified moderators simultaneously rather than as individual subgroups, no moderation effect exists for any specific study characteristics. In other words, we are not able to say that any particular characteristic accounts for the between‐study heterogeneity when controlling for other characteristics. Figure 5 reports the predicted study effect sizes controlling for the moderator variables. As the grey‐shaded polygons indicate, no consistent and strong moderation can be observed.
5.
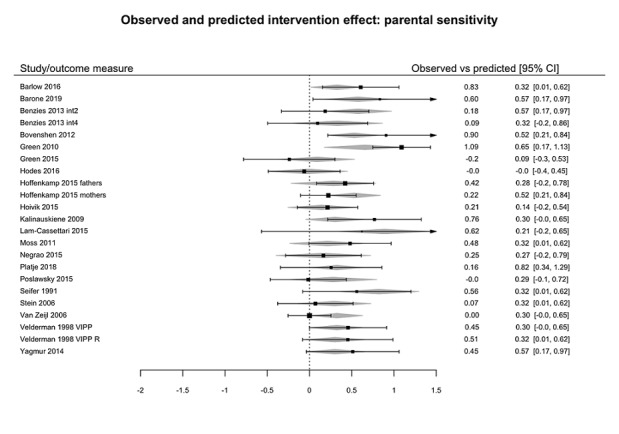
Observed versus predicted intervention effects following moderator analysis
Sensitivity analyses
Reanalysis excluding studies at high or unclear risk of bias
Only two meta‐analyses included data from more than two studies (Analysis 2.1; Analysis 1.4). For these analyses, we explored the effects of excluding studies at a high risk of bias.
Parental sensitivity
For Analysis 2.1, we first considered the effect of excluding four studies classed at high risk of attrition bias (Høivik 2015; Moss 2011; Platje 2018; Yagmur 2014). This had no effect on the results, which continued to show evidence of a difference between groups (16 studies, 1414 dyads; SMD 0.35, 95% CI 0.17 to 0.53). When we removed the two studies at high risk of selection bias (Bovenschen 2012; Seifer 1991), the analysis continued to show evidence of a difference between groups (14 studies, 1338 dyads; SMD 0.32, 95% CI 0.13 to 0.51). When we further removed the two remaining studies at unclear risk of selection bias (Kalinauskiene 2009; Klein Velderman 2006), the analysis still also showed evidence of a difference between groups (12 studies, 1203 dyads; SMD 0.27, 95% CI 0.06 to 0.48).
Adverse effects: parental stress
For Analysis 1.4, we considered the effect of excluding the two studies at high or unclear risk of attrition bias (Hodes 2017; Platje 2018). This had no effect on the analysis, which continued to show no difference between groups (6 studies, 375 dyads; SMD −0.07, 95% CI −0.28 to 0.14). This remained the case when we additionally excluded the two studies (Kalinauskiene 2009; Klein Velderman 2006) at unclear risk of selection bias (4 studies, 240 dyads; SMD −0.09, 95% −0.35 to 0.17).
Reanalysis using different statistical approaches
In the preceding sections, we have presented the results from meta‐analyses conducted using a random‐effects model. We repeated all analyses using a fixed‐effect model. There was no difference in overall outcomes for any of the meta‐analyses other than Analysis 1.5. Under a random‐effects assumption, there was no strong evidence of a difference in parental anxiety between intervention and control groups (311 dyads; SMD −0.28, 95% CI −0.87 to 0.31, Analysis 1.5). Under a fixed‐effect assumption, there was evidence of a reduction in parental anxiety in the short term in the intervention group compared to the comparison group (311 dyads; SMD −0.25, 95% −0.47 to −0.02). The two studies pooled in this meta‐analysis, Barlow 2016 and Hoffenkamp 2015, are clinically very similar: both studies are with parents of preterm children, using three sessions of VIG. This might explain why the fixed‐effect model produces some evidence of an effect; however, given the very high heterogeneity (82%), we chose to present the results of the random‐effects model.
Discussion
Summary of main results
Twenty‐two studies, enrolling 1889 parent‐child dyads or family units, met the inclusion criteria for this review. Parents who participated in the studies were experiencing a variety of problems that might impede their ability to respond sensitively to the cues and needs of their children, and that might therefore also undermine their children's ability to form secure attachments. The evidence suggests that video feedback may help to promote parents' sensitivity (moderate‐certainty evidence). An effect size of 0.34 means that if 10,000 parents were to receive a video‐feedback intervention, around 1100 of them would benefit (Magnusson 2014). Furthermore, although the standard system of rating such effect sizes suggests that this finding is small (Higgins 2017), it is highly favourable when compared with that for other parenting interventions such as home visiting programmes, which show evidence of much smaller overall effect sizes (see for example, Michalopoulos 2019).
There is currently only little, very low‐certainty evidence regarding the impact of video feedback on attachment security, compared with control: results differed based on the type of measure used, and follow‐up was limited in duration. There is no evidence of adverse impacts on parental stress (low‐certainty evidence) or anxiety (very low‐certainty evidence). No study measured parental reflective functioning.
There was also no evidence of a moderator effect for the three prespecified variables (intervention type, number of feedback sessions and participating carer) when jointly tested, although parent gender (both parents versus only mothers or only fathers) potentially has a statistically significant, negative moderation effect.
Overall completeness and applicability of evidence
We set out to evaluate the effectiveness of video feedback for improving parental sensitivity and promoting attachment security in children aged under five years old. In terms of completeness, although some RCTs did not provide data in a form that we could incorporate in a meta‐analysis (e.g. Koniak‐Griffin 1992; Moran 2005), and our attempts to obtain such data from the study authors were not always successful, we are confident that we have identified all of the available published evidence.
In terms of applicability, we identified studies targeting parents and children experiencing a range of difficulties or problems that put them at risk of poor parenting (e.g. parental depression; sensitivity problems; intellectual disability; insecure attachment; first‐time teen or immigrant parent; preterm babies; children with autism). The studies were conducted across a range of countries and with widely diverging ethnic groups, in one of three settings: the home; the community, such as a family centre; and inpatient settings, such as hospitals. We also included a comprehensive range of video‐feedback interventions. Most of the studies included mother‐child dyads or primary caregiver‐child dyads where the primary caregiver was the mother, while few studies had more than 10% of participants who were fathers. There were some meta‐analyses (e.g. for child behaviour or parental anxiety) that contain studies primarily with children under 1 year of age, potentially limiting their generalisability.
However, while the results of these studies should not, as such, be extended to fathers, for whom further research is needed, the findings of the current review regarding parental sensitivity appear to be widely applicable and the findings will be useful to both policymakers and health professionals across a range of contexts.
Quality of the evidence
Using the GRADE approach, we rated the overall certainty of the body of evidence between moderate and very low (see Table 1). We did not downgrade any outcome more than once for any of the five domains.
Limitations in study design and implementation
We downgraded two outcomes for limitations in study design and implementation (attachment security at postintervention and parental stress at postintervention or short‐term follow‐up), and one outcome (child behaviour) for risk of bias.
Indirectness of evidence
We did not downgrade any outcomes for indirectness of evidence.
Unexplained heterogeneity or inconsistency of results
We downgraded two outcomes because of heterogeneity: parental sensitivity at postintervention or short‐term follow‐up due to unexplained moderate heterogeneity and parental anxiety at short‐term follow‐up due to high heterogeneity.
Imprecision of results
We downgraded all outcomes except parental sensitivity at postintervention or short‐term follow‐up for imprecision (wide confidence intervals).
Publication bias
We downgraded all outcomes except parental sensitivity at postintervention or short‐term follow‐up and parental stress at postintervention or short‐term follow‐up for publication bias (most studies in this review did not report these outcomes).
Potential biases in the review process
Our literature searches and screening process conformed strictly to Cochrane criteria, as defined by our Methods. We conducted systematic searches across a large number of highly relevant databases, including trials registers, to identify both completed and ongoing trials. Two review authors independently screened potentially eligible studies for inclusion, extracted data, assessed risk of bias in included studies, and rated the certainty of the evidence. Therefore, any reviewer bias was very limited.
For a small number of studies (Hodes 2017; Moss 2011; Poslawsky 2015), we used outcomes data that included children aged five years and over, as the study authors either did not respond to our request for outcomes data with those children who were outside of our included age range excluded, or were not able to provide it. We judged that the number of children aged five years and over from those studies were likely to be very small, and the benefits of including the outcomes data outweighed any negatives.
In terms of conflict of interest, it should be noted that one of the review authors (JB) was the lead author on one of the included studies (Barlow 2016). However, JB was not involved in study selection, data extraction, assessment of risk of bias or GRADE ratings for this study.
We did not prespecify which time point we would use if there were two time points that could be combined in the same meta‐analysis. We have chosen the time point closest to the end of the intervention for consistency; however, in a number of these studies, there was a diminution of effect over time, so we may have found a different result had we chosen later time points.
We assumed that missing data were missing at random, but this may have been an incorrect assumption. Unexplained attrition was quite high in some studies and this also may have impacted the validity of some results.
Agreements and disagreements with other studies or reviews
There have been a number of reviews of different types of video feedback. At the time the protocol for this review was published (O'Hara 2016), only one quantitative review of the effectiveness of video feedback had been conducted: Fukkink 2008. That review concluded that video feedback was effective in improving a range of outcomes when used with parents of children up to seven years of age. However, it also had a number of limitations, perhaps the most important of all being that it included uncontrolled studies and did not rate the quality of the included studies.
Since the publication of our protocol (O'Hara 2016), we have identified other systematic reviews on this topic. Balldin 2018 undertook a systematic review of RCTs and quasi‐RCTs of video feedback; that review focused on describing the components of video‐feedback programmes and the outcomes from individual studies. However, the authors did not undertake a meta‐analysis of results, and their methods state that they searched only a small number of databases together with Google Scholar. Their list of included studies differs from ours, largely because they included studies that used video feedback alongside other interventions, which we excluded. They concluded that video feedback seems effective in improving parental sensitivity, parent behaviour and child behaviour, which is a broader conclusion than we have reached in this review.
Van den Broek 2017 conducted a systematic review of studies examining issues that should be considered when delivering video feedback for children with visual impairments. They included a wider range of study designs than we have here, and they did not identify any RCTs or quasi‐RCTs. They also searched a smaller number of databases than this review. They concluded by highlighting the themes and issues that are important to consider when adapting video feedback for children with visual impairments.
NICE 2016 recommended that video feedback is one of a small number of interventions for which there is low‐quality evidence of effectiveness in improving maternal attachment for children on the edge of care. This was based on evidence gathered through their own systematic search process for the corresponding NICE guideline (NICE 2015). Our findings were more mixed, although our population of interest was broader.
Finally, the authors of VIPP recently published a book chapter summarising the results of a review of 12 RCTs of VIPP, reporting an effect size of 0.47 (95% CI 0.34 to 0.60) for sensitivity (Juffer 2018). They included two studies that we excluded from this review because they did not have an appropriate control group or were not published, and they reported the data differently. For example, in our review, we report that Poslawsky 2015 shows no evidence of impact on parents at risk for autism, which is consistent with the findings reported in the original paper; Juffer 2018 presents the non‐intrusiveness subdomain of the Emotional Avaliability Scale, which shows evidence of effectiveness, while we use the sensitivity subdomain, which shows no evidence of effectiveness. Qualitatively, however, our findings of the impact of a range of types of video feedback on sensitivity are similar.
Overall, therefore, the results of the current review are consistent with those of other reviews.
Authors' conclusions
Implications for practice.
The findings of this review point to moderate‐certainty evidence that video feedback may be an effective method of improving maternal sensitivity in a range of mother‐infant dyads. Although we aimed to identify evidence for all children aged 4 years 11 months or under, most included studies focused on infants. The results appear to be consistent across study populations with the exception of two studies (Green 2015; Hodes 2017), which targeted parents of children at high risk of autism and parents with intellectual disabilities respectively. There was also limited evidence of its use with fathers. There was, in addition, high consistency across the different settings in which video feedback was delivered (e.g. home; community settings such as family centres; and hospital or residential settings).
In terms of practice, these findings suggest that video feedback can be provided to parents with wide‐ranging challenges and in almost any setting. The findings do not currently support the use of video feedback to improve any other outcomes (e.g. parental reflective functioning, child behaviour or attachment). The moderator analysis did not find any evidence that some types of video feedback (e.g. Video Feedback Intervention to Promote Positive Parenting (VIPP)) are more effective than others, and this may reflect the fact that the core content of such programmes in terms of parental sensitivity is similar (e.g. guided viewing of interaction with feedback). Although this review did not assess the effectiveness of video‐feedback programmes in terms of different programme components, such programmes nevertheless vary in terms of the extent to which they are standardised (for example, VIPP is one of the most standardised programmes). Practitioners need to address which type of video feedback fits best within their own clinical context.
Implications for research.
The findings of this research suggest that, although there is evidence of an impact of video feedback on maternal sensitivity, the evidence of its impact on child attachment security and other outcomes for both parents (e.g. parental reflective functioning) and children (e.g. emotional and behavioural adjustment) is limited. Future research should ensure that such outcomes are assessed using validated measures, in both the short‐ and the longer‐term (i.e. after 12 months). There is also a need for research that examines the effectiveness of video feedback with fathers and with specific groups of parents. There is, for example, currently limited research regarding the effectiveness of video feedback with parents experiencing perinatal mental health problems. Qualitative research is also needed to assess whether parents have a preference in terms of setting or delivery methods.
The review included different types of video feedback, some of which are more standardised (e.g. VIPP) than others. Future reviews might directly compare the different types of video feedback, including the benefits of additional components where these are included.
None of the included studies measured the cost of delivering video feedback, and no studies conducted a cost‐effectiveness analysis or compared the costs of different modes of delivery. There is, as such, also a need to include information on costs in trial reports, to help inform decision‐makers.
Acknowledgements
This review was produced within Cochrane Developmental, Psychosocial and Learning Problems (CDPLP). In particular, we thank Margaret Anderson for her assistance with the search strategy. We would also like to thank Dr Stephan Oelhafen and Leva Radzeviciute for their assistance in translating two of the included studies. We also thank the following reviewers for their comments on an earlier version of this review: Carl J Dunst, PhD, Orelena Hawks Puckett Institute, Asheville, North Carolina, USA; Cristiana Riboni, Italy.
Appendices
Appendix 1. Search strategies
Cochrane Central Register of Controlled Studies, in the Cochrane Library
Search dates: 6 September 2016 (523 records); 10 November 2018 (945 additional records)
#1 [mh "Video recording"] #2 VIG #3 video* #4 VIPP #5 VHT #6 "INTERACTION GUIDANCE" #7 {or #1‐#6} #8 MeSH descriptor: [Parent‐Child Relations] 1 tree(s) exploded #9 [mh Parenting] #10 [mh "paternal behavior"] #11 [mh "maternal behavior"] #12 [mh "object attachment"] #13 [mh "reactive attachment disorder"] #14 Insecure near/3 attachment* #15 secure near/3 attachment* #16 attachment near/3 disorder* #17 parent* near/3 sensitiv* #18 ((mother* or maternal*) near/3 sensitiv*) #19 ((father* or paternal*) near/3 sensitiv*) #20 parent near/3 competenc* #21 ((mother* or maternal) near/3 competenc*) #22 ((father* or paternal) near/3 competenc*) #23 parent near/3 responsiv* #24 parent near/3 positive* #25 ((mother* or maternal) near/3 responsiv*) #26 ((father* or paternal) near/3 responsiv*) #27 disorgani*ed near/3 attachment* #28 (parent* near/3 (interaction or inter next action*)) #29 ((mother* or maternal) near/3 (interaction or inter next action*)) #30 ((father* or paternal) near/3 (interaction or inter next action*)) #31 ((parent* or mother* or maternal* or father* or paternal* or infant* or child*) near/3 (attachment* or bond* or relationship* or dyad* or triad*)) #32 (parent* near/3 (intervention* or skill* or train* or educat* or program*)) #33 [mh Caregivers] #34 (carer* or care next giver* or caregiver*) #35 {or #8‐#34} #36#7 and #35 in Trials
MEDLINE Ovid
Search dates: 1 August 2016 (793 records); 10 November 2018 (304 additional records)
1 exp Video Recording/ 2 VIG.tw. 3 video$.tw. 4 VIPP$.tw. 5 VHT.tw. 6 interaction guidance.tw. 7 or/1‐6 8 exp Parent‐Child Relations/ 9 Parenting/ 10 Paternal Behavior/ 11 maternal behavior/ 12 Object Attachment/ 13 Reactive Attachment Disorder/ 14 (insecure adj3 attachment$).tw. 15 (secure adj3 attachment$).tw. 16 (attachment adj3 disorder$).tw. 17 (parent$ adj3 sensitiv$).tw. 18 ((mother$ or maternal$) adj3 sensitiv$).tw. 19 ((father$ or paternal$) adj3 sensitiv$).tw. 20 (parent$ adj3 competenc$).tw. 21 ((mother$ or maternal$) adj3 competenc$).tw. 22 ((father$ or paternal$) adj3 competenc$).tw. 23 (parent$ adj3 responsiv$).tw. 24 (parent$ adj3 positive).tw. 25 ((mother$ or maternal$) adj3 responsiv$).tw. 26 ((father$ or paternal$) adj3 responsiv$).tw. 27 (disorgani#ed adj3 attachment$).tw. 28 (parent$ adj3 (inter‐action$ or interaction$)).tw. 29 ((mother$ or maternal$) adj3 (interaction or inter‐action$)).tw. 30 ((father$ or paternal$) adj3 (interaction or inter‐action$)).tw. 31 ((parent$ or mother$ or maternal$ or father$ or paternal$ or infant$ or child$) adj3 (attachment$ or bond$ or relationship$ or dyad$ or triad$)).tw. 32 (parent$ adj3 (intervention$ or skill$ or train$ or educat$ or program$)).tw. 33 Caregivers/ 34 (carer$ or caregiver$ or care giver$).tw. 35 or/8‐34 36 randomized controlled trial.pt. 37 controlled clinical trial.pt. 38 randomi#ed.ab. 39 placebo$.ab. 40 drug therapy.fs. 41 randomly.ab. 42 trial.ab. 43 groups.ab. 44 or/36‐43 45 exp animals/ not humans.sh. 46 44 not 45 47 7 and 35 and 46
Embase Ovid
Search dates: 11 August 2016 (809 records); 10 November 2018 (272 additional records)
1 videorecording/ 2 VIG.tw. 3 video$.tw. 4 VHT.tw. 5 VIPP$.tw. 6 interaction guidance.tw. 7 or/1‐6 8 exp child parent relation/ 9 parenting.tw. 10 paternal behavior/ 11 maternal behavior/ 12 object relation/ 13 psychosocial disorder/ 14 (insecure adj3 attachment$).tw. 15 (secure adj3 attachment$).tw. 16 (attachment adj3 disorder$).tw. 17 (parent$ adj3 sensitiv$).tw. 18 ((mother$ or maternal$) adj3 sensitiv$).tw. 19 ((father$ or paternal$) adj3 sensitiv$).tw. 20 (parent$ adj3 competenc$).tw. 21 ((mother$ or maternal$) adj3 competenc$).tw. 22 ((father$ or paternal$) adj3 competenc$).tw. 23 (parent$ adj3 responsiv$).tw. 24 (parent$ adj3 positive).tw. 25 ((mother$ or maternal$) adj3 responsiv$).tw. 26 ((father$ or paternal$) adj3 responsiv$).tw. 27 (disorgani#ed adj3 attachment$).tw. 28 (parent$ adj3 (inter‐action$ or interaction$)).tw. 29 ((mother$ or maternal$) adj3 (interaction or inter‐action$)).tw. 30 ((father$ or paternal$) adj3 (interaction or inter‐action$)).tw. 31 ((parent$ or mother$ or maternal$ or father$ or paternal$ or infant$ or child$) adj3 (attachment$ or bond$ or relationship$ or dyad$ or triad$)).tw. 32 (parent$ adj3 (intervention$ or skill$ or train$ or educat$ or program$)).tw. 33 caregiver/ 34 (carer$ or caregiver$ or care giver$).tw. 35 or/8‐34 36 7 and 35 37 Randomized controlled trial/ 38 controlled clinical trial/ 39 Single blind procedure/ 40 Double blind procedure/ 41 triple blind procedure/ 42 Crossover procedure/ 43 (crossover or cross‐over).tw. 44 ((singl$ or doubl$ or tripl$ or trebl$) adj1 (blind$ or mask$)).tw. 45 Placebo/ 46 placebo.tw. 47 prospective.tw. 48 factorial$.tw. 49 random$.tw. 50 assign$.ab. 51 allocat$.tw. 52 volunteer$.ab. 53 or/37‐52 54 7 and 36 and 53
CINAHL Plus EBSCOhost
Search dates: 11 August 2016 (1072 records); 10 November 2018 (88 additional records)
S55 S7 AND S36 AND S54 S54 S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 OR S50 OR S51 OR S52 OR S53 S53 random* S52 TI ((tripl* N2 mask*) or (tripl* N2 blind*)) or ((trebl* N2 mask*) or (trebl* N2 blind*)) OR AB((tripl* N2 mask*) or (tripl* N2 blind*)) or ((trebl* N2 mask*) or (trebl* N2 blind*)S51 TI((doubl* N2 mask*) or (doubl* N2 blind*)) OR AB((doubl* N2 mask*) or (doubl* N2 blind*)) S50 TI(single N2 mask* or single N2 blind*) OR AB(single N2 mask* or single N2 blind*) S49 (MH "Treatment Outcomes") S48 (MH "Program Evaluation") S47 (evaluat* N2 study or evaluat* N2 research) S46 (prospectiv* study or prospectiv* research) S45 ("follow‐up study" or "follow‐up research") S44 (clinical trial*) or (control* N2 trial*) S43 PT Clinical trial S42 PT randomized controlled trial S41 (MH "Quantitative Studies") S40 (MH "Crossover Design") S39 (MH "Meta Analysis") S38 MH random assignment S37 (MH "Clinical Trials+")1 S36 S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 S35 (carer* or caregiver* or care giver*) S34 (MH "Caregivers") S33 (parent* N3 (intervention* or skill* or train* or educat* or program*)) S32 ((parent* or mother* or maternal* or father* or paternal* or infant* or child*) N3 (attachment* or bond* or relationship* or dyad* or triad*)) S31 ((father* or paternal*) N3 (interaction or inter‐action*)) S30 ((mother* or maternal*) N3 (interaction or inter‐action*)) S29 (parent* N3 (inter‐action* or interaction*)) S28(disorgani#ed N3 attachment*) S27((father* or paternal*) N3 responsiv*) S26((mother* or maternal*) N3 responsiv*) S25(parent N3 positive) S24(parent* N3 responsiv*) S23((father* or paternal*) N3 competenc*) S22((mother* or maternal*) N3 competenc*) S21(parent* N3 competenc*) S20((father* or paternal*) N3 sensitiv*) S19((mother* or maternal*) N3 sensitiv*) S18(parent* N3 sensitiv*) S17(attachment N3 disorder*) S16(secure N3 attachment*) S15(insecure N3 attachment*) S14(MH "Reactive Attachment Disorder") S13object attachment S12(MH "Attachment Behavior+") S11(MH "Maternal Behavior") S10 (MH "Paternal Behavior") S9 (MH "Parenting") S8 (MH "Parent‐Child Relations+") S7 S1 OR S2 OR S3 OR S4 OR S5 OR S6 S6 interaction guidance S5 VHT* S4 VIPP* S3 video* S2 VIG S1(MH "Videorecording")
PsycINFO Ovid
Search dates: 11 August 2016 (1922 records); 10 November 2018 (1236 additional records)
1 Videotapes/ 2 Videotape Recorders/ 3 exp Digital Video/ 4 exp Videotape Instruction/ 5 VIG.tw. 6 video$.tw. 7 VIPP$.tw. 8 VHT.tw. 9 interaction guidance.tw. 10 or/1‐9 11 exp Parent Child Relations/ 12 Parenting/ 13 paternal behaviour.mp. 14 exp Fathers/ or exp Father Child Relations/ 15 mother child relations/ 16 maternal behaviour.mp. 17 object attachment.mp. 18 attachment behavior/ 19 attachment disorders/ 20 (insecure adj3 attachment$).tw. 21 (secure adj3 attachment$).tw. 22 (attachment adj3 disorder$).tw. 23 (parent$ adj3 sensitiv$).tw. 24 ((mother$ or maternal$) adj3 sensitiv$).tw. 25 ((father$ or paternal$) adj3 sensitiv$).tw. 26 (parent$ adj3 competenc$).tw. 27 ((mother$ or maternal$) adj3 competenc$).tw. 28 ((father$ or paternal$) adj3 competenc$).tw. 29 (parent$ adj3 responsiv$).tw. 30 (parent$ adj3 positive).tw. 31 ((mother$ or maternal$) adj3 responsiv$).tw. 32 ((father$ or paternal$) adj3 responsiv$).tw. 33 (disorgani#ed adj3 attachment$).tw. 34 (parent$ adj3 (inter‐action$ or interaction$)).tw. 35 ((mother$ or maternal$) adj3 (interaction or inter‐action$)).tw. 36 ((father$ or paternal$) adj3 (interaction or inter‐action$)).tw. 37 ((parent$ or mother$ or maternal$ or father$ or paternal$ or infant$ or child$) adj3 (attachment$ or bond$ or relationship$ or dyad$ or triad$)).tw. 38 (parent$ adj3 (intervention$ or skill$ or train$ or educat$ or program$)).tw. 39 CAREGIVERS/ 40 (carer$ or caregiver$ or care giver$).tw. 41 or/11‐40 42 random$.tw. 43 ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).tw. 44 (crossover$ or "cross over$").tw. 45 trial$.tw. 46 group$.ab. 47 control.ab. 48 exp program evaluation/ 49 treatment effectiveness evaluation/ 50 treatment outcome clinical trial.md. 51 ((effectiveness or evaluat$) adj3 (stud$ or research$)).tw. 52 (allocat$ or assign$).tw. 53 placebo.ab. 54 or/42‐53 55 10 and 41 and 54
Sociological Abstracts ProQuest
Search dates: 8 September 2016 (17 records); 10 November 2018 (0 additional records)
(“video recording” or VIG or video* or VIPP* or VHT or “interaction guidance”) AND ("parent‐child relations" OR parenting OR "paternal behavior" OR "maternal behavior" OR "object attachment" OR "Reactive Attachment Disorder" OR Insecure NEAR/3 attachment* OR secure NEAR/3 attachment* OR attachment NEAR/3 disorder* OR parent* NEAR/3 sensitiv* OR mother* OR maternal* NEAR/3 "sensitiv* or father* or paternal* near/3 sensitiv* or parent" NEAR/3 competenc* OR mother* OR maternal* NEAR/3 competenc* OR father* OR paternal* NEAR/3 competenc* OR parent* NEAR/3 responsiv* OR parent* NEAR/3 positive OR mother* OR maternal* NEAR/3 responsiv* OR father* OR paternal* NEAR/3 responsiv* OR disorgani*ed NEAR/3 attachment* OR parent* NEAR/3 inter‐action* OR interaction* OR mother* OR maternal* NEAR/3 interaction* OR maternal* inter‐action* OR father* NEAR/3 interaction* OR paternal* NEAR/3 interaction* OR paternal* NEAR/3 inter‐action* OR father* NEAR/3 inter‐action* OR parent* NEAR/3 inter‐action*or parent* NEAR/3 interaction*or mother* NEAR/3 inter‐action* OR mother NEAR/3 interaction* OR maternal* NEAR/3 inter‐action* OR maternal NEAR/3 interaction* OR father* NEAR/3 interaction* OR father NEAR/3 inter‐action* OR paternal* NEAR/3 interaction* OR paternal* NEAR/3 inter‐action* OR parent* NEAR/3 attachment* OR parent* NEAR/3 bond* OR parent* NEAR/3 relationship* OR parent* NEAR/3 dyad* OR parent* NEAR/3 triad*or mother* NEAR/3 attachment* OR mother* NEAR/3 bond* OR mother* NEAR/3 relationship* OR mother* NEAR/3 dyad* OR mother* NEAR/3 triad* OR maternal* NEAR/3 attachment* OR maternal* NEAR/3 bond* OR maternal* NEAR/3 relationship* OR maternal* NEAR/3 dyad* OR maternal* NEAR/3 triad* OR father* NEAR/3 attachment* OR father* NEAR/3 bond* OR father* NEAR/3 relationship* OR father* NEAR/3 dyad* OR father* NEAR/3 triad* OR paternal* NEAR/3 attachment* OR paternal* NEAR/3 bond* OR paternal* NEAR/3 relationship* OR paternal* NEAR/3 dyad* OR paternal* NEAR/3 triad* OR infant* NEAR/3 attachment* OR infant* NEAR/3 bond* OR infant* NEAR/3 relationship* OR infant* NEAR/3 dyad* OR infant* NEAR/3 triad* OR child* NEAR/3 attachment* OR child* NEAR/3 bond* OR child* NEAR/3 relationship* OR child* NEAR/3 dyad* OR child* NEAR/3 triad* OR parent* NEAR/3 intervention* OR parent* NEAR/3 skill* OR parent* NEAR/3 train* OR parent* NEAR/3 educat* OR parent* NEAR/3 program* OR caregivers OR carer* OR caregiver* OR care giver*) AND (randomi*ed NEXT controlled NEXT trial OR "controlled clinical trial" OR random*ied OR placebo* OR "drug therapy" OR randomly OR trial OR groups)
Social Sciences Citation Index Web of Science (SSCI)
Search dates: 15 August 2016 (23 records); 10 November (11 additional records)
(“video recording” or VIG or video* or VIPP* or VHT or “interaction guidance”) AND ("parent‐child relations" or parenting or "paternal behavior" or "maternal behavior" or "object attachment" or "Reactive Attachment Disorder" or insecure near/3 attachment* or secure near/3 attachment* or attachment near/3 disorder* or parent* near/3 sensitiv* or mother* or maternal* near/3 sensitiv* or father* or paternal* near/3 sensitiv* or parent near/3 competenc* or mother* or maternal* near/3 competenc* or father* or paternal* near/3 competenc* or parent* near/3 responsiv* or parent* near/3 positive or mother* or maternal* near/3 responsiv* or father* or paternal* near/3 responsiv* or disorgani*ed near/3 attachment* or parent* near/3 inter‐action* or parent* near/3 interaction* or mother* or maternal* near/3 interaction* or maternal* near/3 inter‐action* or father* near/3 interaction* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or father* near/3 inter‐action* or parent* near/3 inter‐action* or parent* near/3 interaction* or mother* near/3 inter‐action* or mother* near/3 interaction* or maternal* near/3 inter‐action* or maternal near/3 interaction* or father* near/3 interaction* or father* near/3 inter‐action* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or parent* near/3 attachment* or parent* near/3 bond* or parent* near/3 relationship* or parent* near/3 dyad* or parent* near/3 triad* or mother* near/3 attachment* or mother* near/3 bond* or mother* near/3 relationship* or mother* near/3 dyad* or mother* near/3 triad* or maternal* near/3 attachment* or maternal* near/3 bond* or maternal* near/3 relationship* or maternal* near/3 dyad* or maternal* near/3 triad* or father* near/3 attachment* or father* near/3 bond* or father* near/3 relationship* or father* near/3 dyad* or father* near/3 triad* or paternal* near/3 attachment* or paternal* near/3 bond* or paternal* near/3 relationship* or paternal* near/3 dyad* or paternal* near/3 triad* or infant* near/3 attachment* or infant* near/3 bond* or infant* near/3 relationship* or infant* near/3 dyad* or infant* near/3 triad* or child* near/3 attachment* or child* near/3 bond* or child* near/3 relationship* or child* near/3 dyad* or child* near/3 triad* or parent* near/3 intervention* or parent* near/3 skill* or parent* near/3 train* or parent* near/3 educat* or parent* near/3 program* or caregivers or carer* or caregiver* or care giver*) AND (randomi*ed NEXT controlled NEXT trial or "controlled clinical trial" or random*ied or placebo* or "drug therapy" or randomly or trial or groups)
Social Services Abstracts ProQuest
Search dates: 8 September 2016 (48 records); 10 November 2018 (0 additional records)
(“video recording” or VIG or video* or VIPP* or VHT or “interaction guidance”) AND ("parent‐child relations" or parenting or "paternal behavior" or "maternal behavior" or "object attachment" or "Reactive Attachment Disorder" or insecure near/3 attachment* or secure near/3 attachment* or attachment near/3 disorder* or parent* near/3 sensitiv* or mother* or maternal* near/3 sensitiv* or father* or paternal* near/3 sensitiv* or parent near/3 competenc* or mother* or maternal* near/3 competenc* or father* or paternal* near/3 competenc* or parent* near/3 responsiv* or parent* near/3 positive or mother* or maternal* near/3 responsiv* or father* or paternal* near/3 responsiv* or disorgani*ed near/3 attachment* or parent* near/3 inter‐action* or parent* near/3 interaction* or mother* or maternal* near/3 interaction* or maternal* near/3 inter‐action* or father* near/3 interaction* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or father* near/3 inter‐action* or parent* near/3 inter‐action* or parent* near/3 interaction* or mother* near/3 inter‐action* or mother* near/3 interaction* or maternal* near/3 inter‐action* or maternal near/3 interaction* or father* near/3 interaction* or father* near/3 inter‐action* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or parent* near/3 attachment* or parent* near/3 bond* or parent* near/3 relationship* or parent* near/3 dyad* or parent* near/3 triad* or mother* near/3 attachment* or mother* near/3 bond* or mother* near/3 relationship* or mother* near/3 dyad* or mother* near/3 triad* or maternal* near/3 attachment* or maternal* near/3 bond* or maternal* near/3 relationship* or maternal* near/3 dyad* or maternal* near/3 triad* or father* near/3 attachment* or father* near/3 bond* or father* near/3 relationship* or father* near/3 dyad* or father* near/3 triad* or paternal* near/3 attachment* or paternal* near/3 bond* or paternal* near/3 relationship* or paternal* near/3 dyad* or paternal* near/3 triad* or infant* near/3 attachment* or infant* near/3 bond* or infant* near/3 relationship* or infant* near/3 dyad* or infant* near/3 triad* or child* near/3 attachment* or child* near/3 bond* or child* near/3 relationship* or child* near/3 dyad* or child* near/3 triad* or parent* near/3 intervention* or parent* near/3 skill* or parent* near/3 train* or parent* near/3 educat* or parent* near/3 program* or caregivers or carer* or caregiver* or care giver*) AND (randomi*ed NEXT controlled NEXT trial or "controlled clinical trial" or random*ied or placebo* or "drug therapy" or randomly or trial or groups)
Conference Proceedings Citation Index ‐ Social Science & Humanities Web of Science (CPCI‐SS&H)
Search dates: 15 August 2016 (1 record); 10 November 2018 (0 additional records)
(“video recording” or VIG or video* or VIPP* or VHT or “interaction guidance”) AND ("parent‐child relations" or parenting or "paternal behavior" or "maternal behavior" or "object attachment" or "Reactive Attachment Disorder" or insecure near/3 attachment* or secure near/3 attachment* or attachment near/3 disorder* or parent* near/3 sensitiv* or mother* or maternal* near/3 sensitiv* or father* or paternal* near/3 sensitiv* or parent near/3 competenc* or mother* or maternal* near/3 competenc* or father* or paternal* near/3 competenc* or parent* near/3 responsiv* or parent* near/3 positive or mother* or maternal* near/3 responsiv* or father* or paternal* near/3 responsiv* or disorgani*ed near/3 attachment* or parent* near/3 inter‐action* or parent* near/3 interaction* or mother* or maternal* near/3 interaction* or maternal* near/3 inter‐action* or father* near/3 interaction* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or father* near/3 inter‐action* or parent* near/3 inter‐action* or parent* near/3 interaction* or mother* near/3 inter‐action* or mother* near/3 interaction* or maternal* near/3 inter‐action* or maternal near/3 interaction* or father* near/3 interaction* or father* near/3 inter‐action* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or parent* near/3 attachment* or parent* near/3 bond* or parent* near/3 relationship* or parent* near/3 dyad* or parent* near/3 triad* or mother* near/3 attachment* or mother* near/3 bond* or mother* near/3 relationship* or mother* near/3 dyad* or mother* near/3 triad* or maternal* near/3 attachment* or maternal* near/3 bond* or maternal* near/3 relationship* or maternal* near/3 dyad* or maternal* near/3 triad* or father* near/3 attachment* or father* near/3 bond* or father* near/3 relationship* or father* near/3 dyad* or father* near/3 triad* or paternal* near/3 attachment* or paternal* near/3 bond* or paternal* near/3 relationship* or paternal* near/3 dyad* or paternal* near/3 triad* or infant* near/3 attachment* or infant* near/3 bond* or infant* near/3 relationship* or infant* near/3 dyad* or infant* near/3 triad* or child* near/3 attachment* or child* near/3 bond* or child* near/3 relationship* or child* near/3 dyad* or child* near/3 triad* or parent* near/3 intervention* or parent* near/3 skill* or parent* near/3 train* or parent* near/3 educat* or parent* near/3 program* or caregivers or carer* or caregiver* or care giver*) AND (randomi*ed NEXT controlled NEXT trial or "controlled clinical trial" or random*ied or placebo* or "drug therapy" or randomly or trial or groups)
LILACS (Latin American and Caribbean Health Science Information database; www.lilacs.bvsalud.org/en/)
Search dates: 16 August 2016 (0 records); 10 November 2018 (3 additional records)
recording or VIG or video or VIPP or VHT or interaction guidance and parent* or paternal or maternal or father or mother or infant or child and randomized controlled trial or controlled clinical trial or randomzied or placebo or drug therapy or randomly or trial or groups
Cochrane Database of Systematic Reviews (CDSR), part of the Cochrane Library
Search dates: 11 August 2016 (47 records); 10 November 2018 (23 additional records)
("video recording" or VIG or video* or VIPP* or VHT or "interaction guidance") in Title, Abstract, Keywords and ("parent‐child relations" or parenting or "paternal behavior" or "maternal behavior" or "object attachment" or "Reactive Attachment Disorder" or Insecure near/3 attachment* or secure near/3 attachment* or attachment near/3 disorder* or parent* near/3 sensitiv* or mother* or maternal* near/3 "sensitiv* or father* or paternal* near/3 sensitiv* or parent" near/3 "competenc* or mother* or maternal* near/3 competenc* or father* or paternal* near/3 "competenc* or parent* near/3 "responsiv* or parent* near/3 positive or mother* or maternal* near/3 responsiv* or father* or "paternal* near/3 responsiv* or disorgani*ed near/3 attachment* or parent* near/3 inter‐action* or interaction* or mother* or maternal* near/3 interaction* or maternal* inter‐action* or father* near/3 interaction* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or father* near/3 inter‐action* or parent* near/3 inter‐action*or parent* near/3 interaction*or mother* near/3 inter‐action* or mother near/3 interaction* or maternal* near/3 inter‐action* or maternal near/3 interaction* or father* near/3 interaction* or father near/3 inter‐action* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or parent* near/3 attachment* or parent* near/3 bond* or parent* near/3 relationship* or parent* near/3 dyad* or parent* near/3 triad*or mother* near/3 attachment* or mother* near/3 bond* or mother* near/3 relationship* or mother* near/3 dyad* or mother* near/3 triad* or maternal* near/3 attachment* or maternal* near/3 bond* or maternal* near/3 relationship* or maternal* near/3 dyad* or maternal* near/3 triad* or father* near/3 attachment* or father* near/3 bond* or father* near/3 relationship* or father* near/3 dyad* or father* near/3 triad* or paternal* near/3 attachment* or paternal* near/3 bond* or paternal* near/3 relationship* or paternal* near/3 dyad* or paternal* near/3 triad* or infant* near/3 attachment* or infant* near/3 bond* or infant* near/3 relationship* or infant* near/3 dyad* or infant* near/3 triad* or child* near/3 attachment* or child* near/3 bond* or child* near/3 relationship* or child* near/3 dyad* or child* near/3 triad* or parent* near/3 intervention* or parent* near/3 skill* or parent* near/3 train* or parent* near/3 educat* or parent* near/3 program* or caregivers or carer* or caregiver* or care giver*) and (randomi*ed NEXT controlled NEXT trial or "controlled clinical trial" or random*ied or placebo* or "drug therapy" or randomly or trial or groups) in Cochrane Reviews'
Database of Abstracts of Reviews of Effects (DARE), part of the Cochrane Library
Search dates: 8 September 2016 (4 records); 10 November 2018 (0 additional records)
("video recording" or VIG or video* or VIPP* or VHT or "interaction guidance") in Title, Abstract, Keywords and ("parent‐child relations" or parenting or "paternal behavior" or "maternal behavior" or "object attachment" or "Reactive Attachment Disorder" or Insecure near/3 attachment* or secure near/3 attachment* or attachment near/3 disorder* or parent* near/3 sensitiv* or mother* or maternal* near/3 "sensitiv* or father* or paternal* near/3 sensitiv* or parent" near/3 "competenc* or mother* or maternal* near/3 competenc* or father* or paternal* near/3 "competenc* or parent* near/3 "responsiv* or parent* near/3 positive or mother* or maternal* near/3 responsiv* or father* or "paternal* near/3 responsiv* or disorgani*ed near/3 attachment* or parent* near/3 inter‐action* or interaction* or mother* or maternal* near/3 interaction* or maternal* inter‐action* or father* near/3 interaction* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or father* near/3 inter‐action* or parent* near/3 inter‐action*or parent* near/3 interaction*or mother* near/3 inter‐action* or mother near/3 interaction* or maternal* near/3 inter‐action* or maternal near/3 interaction* or father* near/3 interaction* or father near/3 inter‐action* or paternal* near/3 interaction* or paternal* near/3 inter‐action* or parent* near/3 attachment* or parent* near/3 bond* or parent* near/3 relationship* or parent* near/3 dyad* or parent* near/3 triad*or mother* near/3 attachment* or mother* near/3 bond* or mother* near/3 relationship* or mother* near/3 dyad* or mother* near/3 triad* or maternal* near/3 attachment* or maternal* near/3 bond* or maternal* near/3 relationship* or maternal* near/3 dyad* or maternal* near/3 triad* or father* near/3 attachment* or father* near/3 bond* or father* near/3 relationship* or father* near/3 dyad* or father* near/3 triad* or paternal* near/3 attachment* or paternal* near/3 bond* or paternal* near/3 relationship* or paternal* near/3 dyad* or paternal* near/3 triad* or infant* near/3 attachment* or infant* near/3 bond* or infant* near/3 relationship* or infant* near/3 dyad* or infant* near/3 triad* or child* near/3 attachment* or child* near/3 bond* or child* near/3 relationship* or child* near/3 dyad* or child* near/3 triad* or parent* near/3 intervention* or parent* near/3 skill* or parent* near/3 train* or parent* near/3 educat* or parent* near/3 program* or caregivers or carer* or caregiver* or care giver*) and (randomi*ed NEXT controlled NEXT trial or "controlled clinical trial" or random*ied or placebo* or "drug therapy" or randomly or trial or groups)
Networked Digital Library of Theses and Dissertations (NDLTD; www.ndltd.org)
Search dates: August 2016 (344 records); 10 November 2018 (0 additional records)
"video feedback and attachment and random*"
WorldCat (limited to dissertations and theses; www.worldcat.org)
Search dates: August 2016 (1 record); 10 November 2018 (1 additional record)
kw:video feedback kw:sensitivity or attachment kw:random*
Clinicaltrials.gov (www.clinicaltrials.gov)
Search dates: August 2016 (31 records); 10 November 2018 (2 additional records)
parent | video feedback
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP; www.who.int/ictrp/en)
Search dates: August 2016 (5 records); 10 November 2018 (2 additional records)
Video feedback
UNICEF Global Evaluation Database (www.unicef.org)
Search dates: August 2016 (169 records); July 2017 (0 additional records); 10 November 2018 (0 additional records)
video+feedback+parent+random*
NSPCC Impact and Evidence Hub (www.nspcc.org.uk)
Search dates: July 2017 (218 records); 10 November 2018 (199 additional records)
video+feedback
Association for Video Interaction Guidance UK (AVigUK; www.videointeractionguidance.net)
Search dates: July 2017 (162 records); 10 November 2018 (1 additional record)
video feedback parent* random*
Google Scholar
Search dates: July 2017 (2 records); 10 November 2018 (0 additional records)
"Randomised Controlled Trial" AND "parenting" AND ("video feedback" or "VIP" or "VIG" or "VIPP")
VIPP Training and Resource Centre (www.vippleiden.com/en/professionals/publications)
Accessed: July 2017 (0 records) and 9 July 2019 (1 record); all publications listed screened.
Video Interaction Project (www.videointeractionproject.org/publications.html)
Accessed July 2017 (1 record) and 9 July 2019 (0 records); all publications listed screened.
Appendix 2. 'Risk of bias' assessment
| Domain | Criteria for judgement | ||
| Low risk of bias | High risk of bias | Unclear risk of bias | |
| Sequence generation | "Unpredictable: random number table, stratified or block randomisation, computer random number generator" | "Predictable: non‐random (e.g. choice of practitioner, availability), quasi‐random (e.g. ID, day of visit, date of birth)" | "Lack of information or partial information on sequence generation to make a judgement of low or high risk of bias" |
| Allocation concealment | "Unpredictable: sequentially numbered sealed opaque envelopes, central allocation (e.g. phone, internet)" | "Predictable: random sequence known to personnel in advance, envelopes without safeguards" | "Lack of information or partial information on allocation concealment to make a judgement of low or high risk of bias" |
| Blinding of participants or personnel | "Blinding and unlikely that the blinding would have been broken, no blinding or incomplete blinding but outcome unlikely to be influenced" | "No blinding, incomplete blinding and outcome likely to be influenced" | "Insufficient evidence of participant or personnel blinding to make a judgement of low or high risk of bias" |
| Blinding of outcome assessors | "Blinding and unlikely that the blinding would have been broken, no blinding or incomplete blinding but measurement unlikely to be influenced" | "No blinding, incomplete blinding and measurement likely to be influenced" | "Insufficient evidence of blinding of outcome assessors to make a judgement of low or high risk of bias" |
| Incomplete outcome data | "No missing data, reasons for missing data not related to the outcome, missing data balanced across groups and reasons similar, proportion missing or plausible effect size not enough to have a clinically‐relevant effect" | "Reasons related to outcome and imbalance in numbers or reasons, inappropriate use of imputation, ‘as treated’ analysis with substantial departure from allocation, proportion missing or plausible effect size enough to have a clinically‐relevant effect" | "Lack of information on reasons for missing data, insufficient evidence of effect of missing data on outcome, lack of information on imputation methods or insufficient detail on intention‐to‐treat and participant departure from allocation to make a judgement of low or high risk of bias" |
| Selective outcome reporting | "Protocol is available and all prespecified outcomes of interest to the review reported in the prespecified way, protocol is unavailable but all prespecified outcomes of interest are reported" | "Outcomes not reported as prespecified or expected (e.g. missing, added, unexpected measurements), outcomes reported incompletely" | "Insufficient evidence of selective outcome reporting to make a judgement of low or high risk of bias" |
Footnotes
Information in table taken directly from Cates 2016 [pers comm].
ID: identifier.
Appendix 3. Results from individual moderator meta‐analyses, with Knapp/Hartung confidence intervals
| k | N | d | SE | 95% CI | Q | |
| Total | 23 | 1767 | 0.34a | 0.070 | 0.196 to 0.490 | ‐ |
| ‐ | I2 = 54.0% | Qe (22) = 49.2a | ||||
| Age of child | ||||||
| Infant | 15 | 889 | 0.37b | 0.09 | 0.171 to 0.575 | ‐ |
| No infant | 10 | 878 | 0.30c | 0.10 | 0.084 to 0.532 | ‐ |
| ‐ | I2 = 55.4% | Qbetween: F (2, 21) = 11.5a | ||||
| Qe (21) = 49.0a | ||||||
| Type of intervention | ||||||
| VIPP | 10 | 801 | 0.27c | 0.10 | 0.055 to 0.497 | ‐ |
| No VIPP | 15 | 966 | 0.39a | 0.09 | 0.199 to 0.597 | ‐ |
| ‐ | I2 = 53.8% | Qbetween: F (2, 21) = 12.0a | ||||
| Qe (2!) = 46.0b | ||||||
| Presence of disability in participating child | ||||||
| Disability | 5 | 357 | 0.49b | 0.15 | 0.160 to 0.819 | ‐ |
| No disability | 20 | 1410 | 0.30b | 0.07 | 0.142 to 0.470 | ‐ |
| ‐ | I2 = 52.2% | Qbetween: F (2, 21) = 12.3a | ||||
| Qe (21) = 43.7b | ||||||
| Number of video feedback sessions | ||||||
| 0‐5 | 8 | 330 | 0.37c | 0.14 | 0.075 to 0.667 | ‐ |
| 6‐10 | 13 | 1070 | 0.35b | 0.10 | 0.148 to 0.567 | ‐ |
| > 10 | 4 | 367 | 0.27 | 0.16 | −0.07 to 0.622 | ‐ |
| ‐ | I2 = 57.9% | Qbetween: F (3, 20) = 7.39b | ||||
| Qe (19) = 48.6a | ||||||
| Participating carer in study | ||||||
| All mothers | 18 | 1134 | 0.42a | 0.08 | 0.242 to 0.599 | ‐ |
| All fathers | 2 | 203 | 0.29 | 0.22 | −0.17 to 0.771 | ‐ |
| Both | 5 | 430 | 0.15 | 0.14 | −0.14 to 0.444 | ‐ |
| ‐ | I2 = 53.2% | Qbetween: F (3, 20) = 9.04b | ||||
| Qe (19) = 45.1a | ||||||
| CI: confidence intervals; d: average effect sizes per moderator subgroup; k: number of studies; N: number of participants; Q: test statistics for heterogeneity; Qbetween: test for moderators; Qe: test for residual heterogeneity; SE: standard error; VIPP: Video‐feedback to promote Positive Parenting | ||||||
Footnotes
aP < 0.001 bP < 0.01 cP < 0.5
Appendix 4. Mixed‐effects meta‐regression for joint moderation, with Knapp/Hartung confidence intervals
| Moderators | b | SE | Z score | P value | 95% CI | |
| Intercept | 0.376 | 0.151 | 2.491 | 0.023 | 0.058 | 0.695 |
| Intervention type | ||||||
| VIPP | ref. | |||||
| No VIPP | 0.228 | 0.159 | 1.432 | 0.17 | −0.108 | 0.564 |
| Duration | ||||||
| Sessions: 0‐5 | ref. | |||||
| Sessions: 6‐10 | −0.029 | 0.17 | −0.169 | 0.868 | −0.387 | 0.33 |
| Sessions: > 10 | −0.205 | 0.226 | −0.907 | 0.377 | −0.683 | 0.272 |
| Participating carer | ||||||
| All mothers | ref. | |||||
| All fathers | −0.29 | 0.268 | −1.082 | 0.294 | −0.856 | 0.275 |
| Both fathers and mothers | −0.305 | 0.169 | −1.801 | 0.089 | −0.662 | 0.052 |
| Tau2 (SE) | 0.073 | (0.045) | ‐ | ‐ | ‐ | ‐ |
| I2 | 55.56% | ‐ | ‐ | ‐ | ‐ | ‐ |
| R2 | < 0.001 | ‐ | ‐ | ‐ | ‐ | ‐ |
| Qbetween F(5,17) | 1.0080 | P ≥ 0.4429 | ||||
| N studies | 23 | ‐ | ‐ | ‐ | ‐ | ‐ |
| b: beta; CI: confidence intervals; N: number; ref.: reference category for the categorical moderator variables; SE: standard error; Qbetween: test for moderators; VIPP: Video‐feedback to promote Positive Parenting | ||||||
Footnotes
Data and analyses
Comparison 1. Video feedback versus no intervention or inactive comparator.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Parental sensitivity (postintervention ‐ 6 months) | 20 | 1757 | Std. Mean Difference (Random, 95% CI) | 0.34 [0.20, 0.49] |
| 1.1 VIPP | 10 | 861 | Std. Mean Difference (Random, 95% CI) | 0.24 [0.05, 0.42] |
| 1.2 Other types of video feedback | 10 | 896 | Std. Mean Difference (Random, 95% CI) | 0.44 [0.23, 0.66] |
| 2 Attachment security, measured by Strange Situation Procedure (odds of being securely attached) (postintervention) | 2 | 166 | Odds Ratio (M‐H, Random, 95% CI) | 3.04 [1.39, 6.67] |
| 3 Attachment security, measured by Attachment Q‐sort (any duration of follow‐up) | 2 | 131 | Std. Mean Difference (IV, Random, 95% CI) | 0.02 [‐0.33, 0.38] |
| 4 Adverse events: parental stress (postintervention or short‐term follow‐up) | 8 | 537 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.26, 0.09] |
| 5 Adverse events: parental anxiety (short‐term follow‐up) | 2 | 311 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.28 [‐0.87, 0.31] |
| 6 Child behaviour (long‐term follow‐up) | 2 | 119 | Std. Mean Difference (IV, Random, 95% CI) | 0.04 [‐0.33, 0.42] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Barlow 2016.
| Methods |
Design: parallel‐group RCT Unit of allocation: parent‐child dyad. Data were collected on both parents where the family included parents who were a couple; however, only data on primary carers were presented. Dates of recruitment to trial: 1 January 2012‐31 December 2012 |
|
| Participants |
Number randomised: 31 Number randomised to each group: intervention = 16, control = 15 Participants: primary carers and preterm babies; children of both sexes included. Over 90% of primary carers were mothers. Mean age: primary carers = 32 years (SD = 6.1 years); preterm babies: "Just over one‐third of the sample was less than 10 weeks premature, the remainder being 11 weeks or more (range 5–16)" (quote) Ethnicity: 67% of mothers participating were of white British ethnicity, the rest of mixed ethnic origin Inclusion criteria: babies on neonatal intensive care unit that was participating in the RCT; babies born at 32 weeks' gestation or earlier Exclusion criteria: none Country: UK Setting: community, recruited from neonatal intensive care unit |
|
| Interventions |
Duration of intervention: not reported Number of sessions and frequency: 3 home visits; duration not specified Intervention: VIG, which follows a model of videoing normal interactions between mother and child, selecting short sections and jointly reviewing with feedback, taking a strengths‐based approach, plus usual care Control: usual care |
|
| Outcomes |
Timing of outcome assessment: up to 6 weeks after final session Outcome(s) of interest:
Outcome(s) included in meta‐analysis: parental sensitivity, parental stress and maternal anxiety |
|
| Notes |
Source(s) of funding: The Grace Fund Conflict(s) of interest: one of the authors is a supervisor for the Association for Video Interaction Guidance, UK. Another author is an author of this review. Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Telephone randomisation to the intervention or control group was implemented using a computer‐generated number table". |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "the primary outcome [sensitivity from CARE index] was coded by independent researchers who were blind to the study group" |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of the effect of the intervention. |
| Blinding of outcome assessment (detection bias) Parental anxiety | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of the effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: there was low attrition, with reasons given, and it was equal in size across both arms. An ITT analysis was conducted. Therefore, the impact of attrition on the final study results is likely to be limited. |
| Selective reporting (reporting bias) | Unclear risk |
Comment: protocol available, but retrospectively registered Quote: "Thirty‐one dyads were randomised to the study, of whom 16 were allocated to the intervention group and 15 to the control group. Although data were collected from both parents, only data for primary carers has been analysed (mothers n = 29, fathers n = 2) because secondary carers were not always present during the VIG sessions (fathers n = 15; mothers n = 1)." Comment: we did not request these additional data. |
| Other bias | Low risk | Comment: none |
Barone 2019.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyads Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 83 Number randomised to each group: intervention = 44, control = 39 Participants: mothers and their adoptive children aged 14‐75 months Mean age: mothers = 42.6 years (SD = 3.9 years); children = 43.3 months (SD = 15.9 months) at initial assessment Ethnicity: mothers were all white; children were from a range of different countries (29% Asian, 42% European, 12% American, 17% African) Inclusion criteria: mothers and internationally adopted children Exclusion criteria: none Country: Italy Setting: community, recruited from adoption services |
|
| Interventions |
Duration of intervention: not reported Number of sessions and frequency: 7 home visits Intervention: based on VIPP, with some tailoring for the specific needs of adopted children Control: 6 phone calls with general discussion about child development |
|
| Outcomes |
Timing of outcome assessment: post‐test and 6 months postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity at postintervention |
|
| Notes |
Source(s) of funding: none stated Conflict(s) of interest: none stated Comment(s): maternal sensitivity outcome data and child behaviour data were not reported in the published report. We obtained these data directly from the study author, with children aged ≥ 5 years excluded (Barone 2019 [pers comm]). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed as block randomization with 1:1 allocation using a computerized random number generator". |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "The coders were unaware of the experimental condition and of the timing of assessment, and time points were coded independently". |
| Blinding of outcome assessment (detection bias) Child behaviour | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk |
Quote: "Because these missing values were randomly distributed across participants, we performed an intention‐to‐treat analyses, using the last observation carried forward (LOCF) method, whereby the last available measurement for each individual at the time point prior to withdrawal from the study was retained in the analysis". Comment: the use of the ITT analysis means that the impact of attrition on the final study results is likely to be limited. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol was available, so it was not possible to assess this area. |
| Other bias | Low risk | Comment: none |
Benzies 2013.
| Methods |
Design: parallel‐group RCT Unit of allocation: father‐child dyads Dates of recruitment to trial: December 2008‐June 2011 |
|
| Participants |
Number randomised: 113 Number randomised to each group: 3 groups: intervention with 2 visits (Int‐2) = 46; intervention with 4 visits (Int‐4) = 23; control = 44 Participants: fathers; children of both sexes included Mean age: fathers: Int‐2 = 33.7 years (SD = 6.44 years), Int‐4 = 34.28 years (SD = 4.24 years), control = 34.47 years (SD = 6.01 years); children: Int‐2 = 250 days (SD = 6.27 days), Int‐4 = 248 days (SD = 4.24 days), control = 249 days (SD = 6.61 days) Ethnicity: 75.7% of fathers were European Canadian, 5.4% South Asian, 3.6% North American First Nation. Other groups were not specified. Inclusion criteria: “1. First time biological father of a healthy, singleton, late preterm infant; b) age 18 years or older; c) speaking English to infant at least 50% of interactions; d) cohabiting with infant’s mother; and e) living within 100km of the universities.” (quote) Exclusion criteria: none Country: Canada Setting: community |
|
| Interventions |
Duration of intervention: 2‐3 months (depending on which intervention group) Number of sessions and frequency: home visits lasted 1 h; first home visit carried out when the child was 4 months old. Int‐2 received visits when the child was 4 months and 6 months of age; Int‐4 received 2 additional visits when the child was 5 and 7 months of age Intervention: fathers were video recorded at home, without the mother present, in a structured play interaction when the child was 4 months old. Father and home visitor immediately reviewed the video (with feedback). Int‐2 visits: play and feedback was repeated when child was 6 months old. Int‐4 visits: an additional 2 visits were carried out when the child was 5 and 7 months old. Handouts were given at each session. Control: only 1 home visit at 4 months. Fathers were video recorded, without the mother, in a structured play interaction with the child. Video was not viewed. Home visitor discussed information. Most fathers received a phone call when children were 6 months old |
|
| Outcomes |
Timing of outcome assessment: when children were 8 months old Outcome(s) of interest:
Outcome(s) included in meta‐analysis: parental sensitivity and parental stress |
|
| Notes |
Source(s) of funding: Alberta Centre for Child, Family and Community Research; Preterm Birth and Healthy Outcomes Team (PreHOT); Alberta Innovates Health Solutions Interdisciplinary Team Grant (#200700595) Conflict(s) of interest: none Comment(s): both Int‐2 and Int‐4 interventions met the inclusion criteria for this review, so we used data from both groups in the meta‐analysis. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "fathers were assigned to a group following a randomized allocation sequence generated by a biostatistician" |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: the outcome was measured by "outcome assessors (video coders) who were also blind to group assessment" (quote) |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: only 2 families (1.8%) withdrew after the initial, 4‐month home visit in the control group. Reasons were given and were unlikely to be related to the intervention. There is no reference to an ITT analysis, but the study authors state that they replaced missing values according to each measure's procedure. Therefore, the impact of missing data on the final study results is likely to be limited. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Bovenschen 2012.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 39 Number randomised to each group: not reported; 3 mothers dropped out, but unclear which group they were originally randomised to. Results presented for 36 participants: intervention = 17, control = 19 Participants: mothers Mean age: mothers = 22 years (SD = 6.6 years); children = started intervention from birth Ethnicity: not reported Inclusion criteria: "1 of these: 1) teen mother until the age of 20; 2) mother with migration background; 3) mother with mental illness or 4) mother with high ‘psychosocial’ burden (e.g. financial burden, restricted living space, being a single parent)" (quote) Exclusion criteria: none Country: Germany Setting: community |
|
| Interventions |
Duration of intervention: 3 months Number of sessions and frequency: 7 sessions over 3‐month period Intervention: form of developmental counselling using video feedback to film interactions that form the basis of the counselling sessions; interactions from previous sessions form the basis of the next session Control: care as usual |
|
| Outcomes |
Timing of outcome assessment: postintervention and 3 months postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity at postintervention |
|
| Notes |
Source(s) of funding: the evaluation was funded by the Federal Ministry for Family Affairs, Senior Citizens, Women and Youth (BMFSFJ) and the National Centre for Early Support (“Nationale Zentrum Frühe Hilfen”). Conflict(s) of interest: none Comment(s)
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Comment: study authors state that some women only participated if they could get a certain treatment. They do not report how many women were affected in this way. |
| Allocation concealment (selection bias) | High risk | Comment: see above |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: study authors state that raters were unaware of other data assessed through this project |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: dropout was low (3/39 mothers dropped out). However, it is not possible to work out from which arm they dropped out, as initial numbers randomised to each arm were not stated. Reasons for dropout were not given. Therefore, it is not possible to assess the impact of missing data on the final study results. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Green 2010.
| Methods |
Design: parallel‐group, RCT Unit of allocation: mother‐child dyads Dates of recruitment to trial: 13 February 2006‐12 October 2009 |
|
| Participants |
Number randomised: 152 Number randomised to each group: intervention = 77, control = 75 Participants: mothers Mean age: mothers: intervention = 33 years, control = 34 years, at baseline; children: 45 months at baseline in both groups Ethnicity: intervention = 60% both parents white, 34% both parents non‐white, 6% mixed ethnicity parents; control = 55% both parents white, 33% both parents non‐white, 12% mixed ethnicity parents Inclusion criteria: "Families with a child aged 2 years to 4 years and 11 months, and meeting criteria for core autism according to the international standard diagnostic tests (social and communication domains of the ADOS‐G,and two of three domains of the Autism Diagnostic Interview Revised [ADI‐R] algorithm) were included in the study" (quote) Exclusion criteria: "children with a twin with autism; a non‐verbal age equivalent to 12 months or younger on the Mullen Early Learning Scales; epilepsy requiring medication; severe hearing or visual impairment in a parent or the child; or a parent with a severe psychiatric disorder requiring treatment. At home, participating parents spoke English with their child" (quote) Country: UK Setting: outpatient clinic |
|
| Interventions |
Duration of intervention: 12 months Number of sessions and frequency: 45‐min sessions; fortnightly for 6 months then monthly for 6 months Intervention: parent‐mediated, communication‐focused treatment in children with autism (PACT). Manualised intervention, consisting of video feedback to promote parent‐child interaction, then promotion of communication strategies to encourage language development. Home practice encouraged Control: care as usual ‐ Portage (a weekly or fortnightly home‐based play and development service) |
|
| Outcomes |
Timing of outcome assessment: 1 month after the trial and 5.75 years after the end of the trial Outcome(s) of interest:
Outcome(s) included in meta‐analysis: parental synchrony at 1‐month follow‐up |
|
| Notes |
Source(s) of funding: Medical Research Council (MR/K005863/1), with additional funding from the UK Department of Health, the NIHR Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London Conflict(s) of interest: none Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "PACT manager allocated a sequential identification number and provided a statistician at the independent Christie Clinical Trials Unit in Manchester with the child's number, treatment centre, age and autism severity. This statistician ran an allocation schedule that was computer‐generated by use of probabilistic minimisation of imbalance in the marginal distribution of treatment centre, age (≤42 months or >42 months), and autism severity (ADOS‐G algorithm score 12–17 or 18–24)." |
| Allocation concealment (selection bias) | Low risk | Comment: as above ‐ allocation was performed by a statistician at a separate centre through a sequential process. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: the study authors state that the raters were blind to group status. |
| Blinding of outcome assessment (detection bias) Child socioemotional development | High risk | Comment: the outcome was measured using a self‐report scale. As the participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Blinding of outcome assessment (detection bias) Child mental health | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: relatively low attrition that seems relatively balanced between groups. Missing data were imputed as follows: "Multiple imputation, with the iterative‐chained‐equation method (ice procedure25), was used to complete the small amount of missing data." (quote). Therefore, the impact of missing data on the final study results is likely to be limited. |
| Selective reporting (reporting bias) | Low risk | Comment: protocol available (ISRCTN 58133827); all prespecified outcomes reported |
| Other bias | Low risk | Comment: none |
Green 2015.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyads Dates of recruitment to trial: 01 May 2011‐01 April 2013 |
|
| Participants |
Number randomised: 54 Number randomised to each group: intervention = 28, control = 26 Participants: mothers Mean age: parents: not reported; children: intervention = 267.14 days (SD = 20.93 days), control = 276.58 days (SD = 24.25 days), at baseline Ethnicity: intervention = 64% white, 36% other; control = 85% white, 15% other Inclusion criteria: "siblings of autistic probands sampled within the context of the prospective longitudinal observational British Autism Study of Infant Siblings (BASIS), age 7–10 months at baseline" (quote) Exclusion criteria: "any substantial medical disorder in the infant, being a twin, prematurity of less than 34 weeks, or a birthweight of less than 5 lbs (2.27 kg)" (quote) Country: UK Setting: home |
|
| Interventions |
Duration of intervention: 5 months Number of sessions and frequency: 12 sessions, each lasting 2 h Intervention: adapted VIPP (iBASIS‐VIPP). Manualised intervention. Therapist videos parent‐child interactions during everyday interactions then gives feedback Control: no treatment |
|
| Outcomes |
Timing of outcome assessment: postintervention, and at age 27 months and 39 months Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity measured postintervention |
|
| Notes |
Source(s) of funding: BASIS funding consortium led by Autistica (No: 7267), The Waterloo Foundation and Autism Speaks, USA, Medical Research Council (G0701484 and MR/K021389/1), the NIHR Biomedical Research Centre for Mental Health at the South London and Maudsley NHS Foundation Trust and King’s College London, UK Conflict(s) of interest: none Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "using a permuted block approach within the two strata with random block sizes of four or six generated by the Clinical Trials Unit statistician. The statistician informed the trial office and clinical teams of allocation by telephone and email." |
| Allocation concealment (selection bias) | Low risk | Comment: as above |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants or personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "Assessors and supervising research staff were independent from therapists, housed in different buildings, and were unaware of treatment allocation and the method of randomisation". |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: attrition is relatively balanced across the two arms of the study, with reasons stated for dropouts. Missing data imputed "estimated by maximum likelihood using the sem procedure so as to include data from all 54 participants, including those with incomplete records" (quote). Analysis undertaken on an ITT basis. Therefore, the impact of missing data on the final study results is likely to be limited. |
| Selective reporting (reporting bias) | Low risk | Comment: protocol available (ISRCTN 87373263); all prespecified outcomes reported |
| Other bias | Low risk | Comment: none |
Hodes 2017.
| Methods |
Design: parallel‐group, RCT Unit of allocation: parent‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 85 Number randomised to each group: intervention = 43, control = 42 Participants: mothers and fathers (97.5% mothers) Mean age: parents: 30.3 years (SD = 6.7 years) at baseline; children: intervention = 3.32 years (SD = 1.33 years), control 2.92 years (SD = 1.5 years), at baseline Ethnicity: 24% were immigrants (25% from Suriname, 25% from Curacao, 50% from 8 other countries). It was not stated where other parents came from. Inclusion criteria: parents living in rented housing or residential family home, with a mild intellectual disability, who are being supported by 1 of the 10 organisations involved in recruitment; parents who were primary caregiver (at least 4 days a week) of their child aged 1‐7 years and scored ≥ 62nd percentile on parenting stress score Exclusion criteria: parents whose child had an autistic spectrum disorder; those who had received a video‐based intervention in the last 6 months Country: CBCL Setting: home |
|
| Interventions |
Duration of intervention: 3 months Number of sessions and frequency: 15 sessions Intervention: VIPP‐LD. Adaptation of VIPP‐SD to meet needs of parents with a learning disability. 7 sessions with video recording, 7 sessions where videos were watched with feedback given and a closing session. Parents given a book with pictures from videos to act as an aide memoire Control: care as usual |
|
| Outcomes |
Timing of outcome assessment: post‐test and 3 months' follow‐up Outcome(s) of interest:
Outcome(s) included in meta‐analysis: harmonious parent‐child interaction and parenting stress at postintervention |
|
| Notes |
Source(s) of funding: grant 57000006 of ZonMw (The Netherlands Organisation for Health Research and Development) Conflict(s) of interest: none Comment(s): we requested data with children > 4 years 11 months excluded, but the study authors did not reply to our request (Smith 2017a [pers comm]). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "sequential block randomization was used to assign parents to the experimental group or the control group. Randomization was executed by an independent third party using a computer programme every time there were five or six parents available with a subclinical level of parenting stress". |
| Allocation concealment (selection bias) | Low risk | Comment: the allocators were not blinded, but they were independent of the trial process. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants or personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: the study authors state that coders were blind to the treatment group, timing of evaluation and any other information about the participants. |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: relatively low attrition, but not specified which arm dropouts came from. Missing data imputed using previous values. Analysis undertaken on an ITT basis. No reasons given for dropouts, so not possible to assess if this was related to the intervention. |
| Selective reporting (reporting bias) | Low risk | Comment: trial protocol registered (NL31934.029.10 with CCMO ‐ Dutch language version). All prespecified outcomes appear to be reported. |
| Other bias | Low risk | Comment: none |
Hoffenkamp 2015.
| Methods |
Design: parallel‐group, RCT Unit of allocation: family unit (mother or father, or both, plus child) Dates of recruitment to trial: study does not report precise recruitment dates. Dates of study: September 2009‐September 2012 |
|
| Participants |
Number randomised: 150 (150 children with 150 mothers and 144 fathers, 6 mothers were living without a partner) Number randomised to each group: intervention = 75, control = 75 Participants: families (mother, father and child) Mean age: mothers: intervention = 31.1 years (SD = 4.9 years), control = 30.8 years (SD = 5.4 years), at baseline; fathers: intervention = 34.1 years (SD = 5.4 years), control = 33.6 years (SD = 5.5 years), at baseline; children: not reported (range = 0‐7 days at recruitment) Ethnicity: not reported Inclusion criteria: hospital pre‐term delivery at 1 of 7 hospital wards; children born at < 37 weeks Exclusion criteria: Dutch language poorly understood; previous experience of video‐feedback intervention Country: CBCL Setting: inpatient ward |
|
| Interventions |
Duration of intervention: 6 days Number of sessions and frequency: 6 sessions (3 videoing, 3 feedback) Intervention: carried out according to VIG protocol whilst families were on the ward in the postpartum period. Each session had a 15‐min video followed by feedback. Consisted of 3 sessions during the 1st week after birth; videotaped at 1st, 3rd and 6th day postpartum and feedback on the day after the recordings were made. Both parents were present. Control: standard hospital care |
|
| Outcomes |
Timing of outcome assessment: 1 month and 6 months postpartum Outcome(s) of interest:
Outcome(s) included in meta‐analysis: parental sensitivity and anxiety in parents measured at 1 month postpartum |
|
| Notes |
Source(s) of funding: Achmea Foundation Victim and Society (Stichting Achmea Slachtoffer en Samenleving) Conflict(s) of interest: none stated Comment(s):
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: study authors state that random assignment was undertaken using "computerized random numbers" (quote) |
| Allocation concealment (selection bias) | Low risk | Quote: "pre‐specified allocation sequence was concealed from the nurses involved in participant enrollment…a VIG nurse opened one of the sequentially number, sealed envelopes to reveal the treatment assignment" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants or personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: independent coders, who were blind to each participant's group affiliation, assessed the videotapes. |
| Blinding of outcome assessment (detection bias) Parental anxiety | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: the proportion of families lost to follow‐up was similar across both arms, and reasons for dropout were largely similar across the two arms. Analysis was undertaken on an ITT basis, so attrition is unlikely to have impacted the final study results. |
| Selective reporting (reporting bias) | Low risk | Comment: trial registered at the Nederlands Trial Register (NTR3423). All primary outcomes reported; secondary outcomes not reported |
| Other bias | Low risk | Comment: none |
Høivik 2015.
| Methods |
Design: parallel‐group, RCT Unit of allocation: parent‐child dyad Dates of recruitment to trial: March 2008‐September 2012 |
|
| Participants |
Number randomised: 158 Number randomised to each group: intervention = 88, control = 70 Participants: either mother or father. In 23 families both parents took part in the intervention but only one of the parents was included in the study. In most families mothers (98.7%) chose to participate due to practical reasons. Mean age: mothers = 29.7 years (SD = 5.6 years), fathers = 32.8 years (SD = 7.0 years) at baseline; children = 7.3 months (SD = 5.1 months) at baseline Ethnicity: mothers: 82.6% Norwegian, 6.5% other European, 3.3% African, 5.4% Asian, 2.2% South American; fathers: 89.8% Norwegian, 6.8% other European; 2.3% African; 1.1% North American Inclusion criteria: "parent–child interaction problems and children aged 0 to 24 months at the time of inclusion" (quote) Exclusion criteria: "Parents with ongoing psychosis, developmental disorders or substance abuse and parents with insufficient proficiency to fill out the questionnaires" (quote) Country: Norway Setting: community |
|
| Interventions |
Duration of intervention: 4‐5 months Number of sessions and frequency: 8 sessions Intervention: "Video feedback of infant‐parent interaction (VIPI) group received eight video feedback sessions, with the last two sessions being tailored to meet individual family needs regarding any of the six topics in the VIPI manual. If both parents were included in the intervention, separate videotapes were obtained and individual feedback was given to each parent. VIPI parents were also free to visit other health professionals for routine care." (quote) Control: treatment as usual; parents received routine care at the well‐baby units, but they were also free to seek help from others. No form of video feedback given |
|
| Outcomes |
Timing of outcome assessment: immediately post‐treatment and 6 months post‐treatment Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity. We did not include socioemotional development in the meta‐analysis as the ASQ:SE measured different domains of this outcome to the other study reporting this outcome. |
|
| Notes |
Source(s) of funding: Norwegian Extra Foundation for Health and Rehabilitation with extra funds through The Norwegian Council of Mental Health (reference number 2010/2/0303) and the Liaison Committee between the Central Norway Regional Health Authority and Norges Teknisk‐Naturvitenskaplige Universitet Conflict(s) of interest: no competing interests Comment(s): study authors provided the data for the maternal sensitivity outcomes as they were not included in the published results (Hoivik 2018 [pers comm]) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "the families were consecutively randomised to either a treatment group (VIPI) or a control group (TAU [treatment as usual]) in a 1‐2‐1‐2 allocation ratio" |
| Allocation concealment (selection bias) | High risk | Comment: consecutive randomisation in this way would mean that the allocator would know to which group the parent‐child dyad was being allocated. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants or personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "all raters were blind to the randomization" |
| Blinding of outcome assessment (detection bias) Child socioemotional development | High risk | Comment: the outcome was measured using self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: at the final stage of analysis, attrition was higher in the control arm. It is possible that treatment allocation affected the dropout rate. Missing values were excluded rather than imputed. The reasons given for dropout are not clear. Therefore, it is possible that attrition may have led to an overestimate of the effect of the intervention. |
| Selective reporting (reporting bias) | Unclear risk | Comment: study protocol registered (ISRCTN 99793905), but appears to have been registered after the study was published |
| Other bias | Low risk | Comment: none |
Kalinauskiene 2009.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 54 Number randomised to each group: intervention = 26, control = 28 Participants: mothers Mean age: mothers = 26.4 years (SD = 2.94 years); children: intervention = 6.12 months (SD = 0.07 months), control = 6.11 months (SD = 0.06 months), at pre‐test Ethnicity: 77.8% Lithuanian; the ethnicity of remaining mothers was not stated Inclusion criteria: "Mothers scoring low in assessment of maternal sensitivity in ratings by 2 coders; from intact families, who were primary caregivers to their infants, did not work until their children reached 12 months of age, and had at least high school education, were included in the intervention study. Mothers and infants were free of serious health problems." (quote). Firstborn children only Exclusion criteria: none stated Country: Lithuania Setting: home |
|
| Interventions |
Duration of intervention: 4 months Number of sessions and frequency: 5 monthly sessions lasting 90 min Intervention: 4 sessions with mothers only and 1 booster session for mother and father together. During these sessions mother‐child interactions were videotaped. VIPP applied according to manualised protocol Control: contacted by phone for 5 months and asked for information on their child's development. No advice about sensitive parenting or attachment was given |
|
| Outcomes |
Timing of outcome assessment: immediately postintervention and 12 months postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity, child‐mother attachment security and maternal stress at postintervention, and child behaviour at 12 months postintervention. While two separate scales were reported for Parental Daily Hassles Scale, we only used the Frequency of Hassles Scale in the meta‐analysis. |
|
| Notes |
Source(s) of funding: Nederlandse Organisatie voor Wetenschappelijk Onderzoek Spinoza prize and Nederlandse Organisatie voor Wetenschappelijk Onderzoek Vidi grant; additional financial support received from Wereldkinderen Conflict(s) of interest: none stated Comment(s): an English translation was made of the paper written in Lithuanian for the purposes of this review. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: mothers were randomly assigned to the intervention and control groups, but the study authors do not state how this was done. |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants or personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: the study authors state that observers were blinded. |
| Blinding of outcome assessment (detection bias) Attachment | Low risk | Comment: the study authors state that observers were blinded. |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Blinding of outcome assessment (detection bias) Child behaviour | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no missing data |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Klein Velderman 2006.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 84 Number randomised to each group: not reported. Results analysed for 81 dyads. 3 groups: VIPP = 28; VIPP‐R = 26; control = 27 Participants: mothers; children of both sexes included Mean age: mothers = 27.8 years (SD = 3.63 years); children = not reported (aged 4 months at recruitment and 7‐10 months when the intervention took place) Ethnicity: not reported Inclusion criteria: mothers with firstborn, with > 8 but < 14 years of formal education, with insecure classification according to Adult Attachment Interview Exclusion criteria: none Country: CBCL Setting: community |
|
| Interventions |
Duration of intervention: approximately 4 months Number of sessions and frequency: 4 home visits, each lasting 90 min, 3‐4 weeks apart Intervention: VIPP consisted of 4 home visits. Each session started out with making a videotape of mother‐child interactions that would be used during the next intervention session. Then, feedback was given on the videotape from the previous session. Sessions follow a set theme according to a standardised VIPP protocol. VIPP‐R was similar to VIPP, but contained an additional focus on improving maternal representations. Control: not clearly stated but seems to be no video feedback |
|
| Outcomes |
Timing of outcome assessment: 2 outcome time points: 1‐3 months postintervention and (30 months postintervention) Outcome(s) of interest: 1‐3 months postintervention
30 months postintervention
Outcome(s) included in meta‐analysis: maternal sensitivity at 1‐3 months, child‐mother attachment at 30 months (as earlier data not presented numerically), and child behaviour at 30 months |
|
| Notes |
Source(s) of funding: Pioneer Award from the Netherlands Organization for Scientific Research NWO (grant PGS 59‐256) and the NWO/Spinoza Prize Conflict(s) of interests: none reported Comment(s): study did not include the outcome data for maternal stress in the published papers. The corresponding author provided us with the missing data for the purposes of meta‐analysis (Bakermans‐Kranenburg 2018 [pers comm]). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: study authors state that "Mothers were randomly assigned to one of three groups" (quote), but they provide no information on how this was done |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "Two coders, blind to other data concerning the dyads, independently assigned scores to the mothers". |
| Blinding of outcome assessment (detection bias) Attachment | Low risk | Quote: "two coders who were unaware of other information of the dyads sorted the cards" |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect. |
| Blinding of outcome assessment (detection bias) Child behaviour | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk |
Comment: reasons given by study authors for missing data; attrition is roughly even between groups. Missing values were substituted using a reasonable method of imputation. Therefore, the impact of missing values on the final study results is likely to be low. Quote: "In case of missing values for a respondent who did complete a questionnaire, these were substituted by the mean or mode". |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Koniak‐Griffin 1992.
| Methods |
Design: parallel‐group, RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 31 Number randomised to each group: intervention = 15, control = 16 Participants: mothers Mean age: mothers = 17.16 years (SD = 1.51 years) at baseline; children = not reported (range = 4‐6 weeks at baseline) Ethnicity: intervention = 40% black, 20% Hispanic, 40% white; control = 43.8% black, 56.2% Hispanic Inclusion criteria: mothers aged ≤ 20 years; primiparous; completion of normal pregnancy and delivery of healthy, full‐term child; able to speak and read English Exclusion criteria: none Country: USA Setting: residential maternity home |
|
| Interventions |
Duration of intervention: single visit Number of sessions and frequency: 1 session Intervention: 2 structured teaching tasks at 4‐6 weeks were carried out by adolescent mothers with their 4‐6‐week‐old children using the NCATS. The episodes were videotaped and feedback provided Control: mothers received 2 home visits at comparable time intervals. NCATS protocols were similarly applied, and the episodes video recorded, but no instruction or feedback was provided |
|
| Outcomes |
Timing of outcome assessment: post‐test and 1 month postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: we did not include maternal sensitivity in the meta‐analysis. The study did not report a breakdown of the NCATS score for maternal sensitivity. We requested this information from the study authors (Smith 2018d [pers comm]), but unfortunately did not receive a response. |
|
| Notes |
Source(s) of funding: UCLA (University of California, Los Angeles) School of Nursing Conflict(s) of interest: none stated Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote: "subjects were randomly assigned" Comment: does not specify how participants were randomly assigned to experimental and control conditions |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: the videotapes of maternal‐child interactions were reviewed and scored by a NCATS‐certified instructor who was blind to participants' experimental conditions. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: although the study did not report the maternal sensitivity subdomain of the NCATS scale, they did report the full‐scale outcome. They did not state final numbers for outcomes, so it is not possible to assess whether any dropouts occurred. There is no mention of missing data or ITT analysis. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Lam‐Cassettari 2015.
| Methods |
Design: RCT with waiting‐list control Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 14 Number randomised to each group: intervention = 7; control = 7 Participants: mothers Mean age: mothers = not reported; children: intervention = 3 years 4 months (SD = 2.6 years), control = 1 year 4 months (SD 1.10 years), at recruitment Ethnicity: all participants of British origin except for one family of Latvian origin Inclusion criteria: hearing mothers; congenitally deaf and prelingual children Exclusion criteria: children who were not at prelinguistic stage of development and who could produce > 50 signed/spoken words Country: UK Setting: home |
|
| Interventions |
Duration of intervention: about 6 months Number of sessions and frequency: monthly sessions lasting 30‐45 min Intervention: "It involved (a) a goal setting session, (b) three film sessions of parent‐child interaction in the family home and (c) three shared review sessions in which three short video clips (demonstrating attuned responses linked to the family's goal) were played so families could microanalyze and discuss the behaviours that facilitated successful communication with their child. Video Interaction Guidance (VIG) contact principles were used to analyze the interactive behaviours." (quote) Control: waiting list |
|
| Outcomes |
Timing of outcome assessment: for intervention group, 2 weeks after the intervention and 3 months after the intervention; for control group, after waiting for the control group and then postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity, measured at two weeks for the intervention group and at preintervention after waiting for the control group |
|
| Notes |
Source(s) of funding: NIHR, UK Conflict(s) of interest: none Comment(s): we requested data excluding children aged 5 years and over from the corresponding author of the study, who provided these data for maternal sensitivity (Lam‐Cassettari 2018 [pers comm]). We used these data in the meta‐analysis in preference to the published data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Families were randomly stratified to the intervention group (IG) or waiting‐list before intervention group (WG) using a minimization software program (Altman & Bland, 2005) based on child age, sex, level of hearing loss, and additional needs." |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants or personnel to this type of study. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk |
Comment: assessments of primary outcomes in this study were blinded Quote: "all videos were coded by a single coder who was blind to the assessment session for each video…Inter‐rater reliability was obtained by a second coder also blind to the assessment session." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no missing data |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Moran 2005.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 100 Number randomised to each group: intervention = 50, control = 50 Participants: mothers Mean age: mothers = 18.42 years (SD = 1.01 years); children = not reported (aged 5 months at recruitment) Ethnicity: 81% white, 5% Native American, 5% Middle Eastern, 4% Latin American, 1% Caribbean, 1% Asian (ethnicity of remaining 3% was not reported) Inclusion criteria: mothers aged < 20 years and with uneventful delivery; children born full term with no medical complications Exclusion criteria: none stated Country: Canada Setting: hospital |
|
| Interventions |
Duration of intervention: around 5 months Number of sessions and frequency: 8 home visits from 7 months of age until 12 months of age. First 3 visits were carried out within 1 week of each other and subsequent 5 visits were spaced about 3‐4 weeks apart. Each visit lasted 1 h. Intervention: mother and child were videotaped for about 5 min while playing with age‐appropriate toys and the videotape was played back for the mother to observe and discuss Control: received 1 visit when children were 9 months old. They were interviewed about their current relationships and a videotape was made of child‐mother play, feeding and other activities of the mother's choice. |
|
| Outcomes |
Timing of outcome assessment: 12 and 24 months of age Outcome(s) of interest:
Outcome(s) included in meta‐analysis: infant attachment security at 12 months of age |
|
| Notes |
Source(s) of funding: research grant from the Social Sciences and Humanities Research Council and Health Canada Conflict(s) of interest: none stated Comment(s): maternal sensitivity outcomes were reported as means without standard deviations. The corresponding author was unable to provide the required information to be able to include them in a meta‐analysis (Moran 2017 [pers comm]). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote: "mothers were randomly assigned to an intervention or comparison group" Comment: does not state how mothers were randomly assigned |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Unclear risk | Comment: it is not clear whether the assessors were blinded or not. |
| Blinding of outcome assessment (detection bias) Attachment | Unclear risk | Comment: it is not clear whether the assessors were blinded or not. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: reasons for dropout are not stated, and there is no mention of how missing data were handled. However, there was very low attrition (only 1 dyad across both arms), and therefore the impact on the final study results was likely to be low. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | High risk | Comment: maternal sensitivity outcomes were not reported fully (missing SD/SE) |
Moss 2011.
| Methods |
Design: parallel‐group, RCT Unit of allocation: parent‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 79 Number randomised to each group: intervention = 40, control = 39 Participants: parents (i.e. either mother or father; 94% mothers) Mean age: parents = 27.82 years (SD = 7.61 years) at baseline; children = 3.35 years (SD = 1.38 years) at baseline Ethnicity: not reported Inclusion criteria: primary caregiver of child aged 12‐71 months and living with child; French speaking; being monitored for child maltreatment Exclusion criteria: none Country: Canada Setting: home |
|
| Interventions |
Duration of intervention: 8 weeks Number of sessions and frequency: 8 weekly home visits lasting 90 min Intervention: in addition to standard agency services, all intervention sessions were primarily focused on reinforcing parental sensitive behaviour. This was carried out by means of personalised parent‐child interaction, video feedback, and discussion of attachment or emotion regulation‐related themes. Control: standard agency services (monthly home‐monitoring visits) |
|
| Outcomes |
Timing of outcome assessment: immediately postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: parental sensitivity and child attachment. We did not include child behaviour in the meta‐analysis as it was reported at a different time point to other studies reporting this outcome. |
|
| Notes |
Source(s) of funding: grant from the Public Safety Canada's National Crime Prevention Centre (NCPC) in collaboration with the Quebec Minister of Public Security Conflict(s) of interest: none stated Comment(s): we contacted the study authors to request data excluding children aged ≥ 5 years, but these were not provided (Smith 2018h [pers comm], so we used published outcomes that included children outside of our target age group in the meta‐analysis. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "families were randomly assigned to the intervention or control group using a simple 1:1 block allocation sequence". |
| Allocation concealment (selection bias) | Unclear risk | Comment: if allocators were aware of the size of the block, then bias could have been introduced. Study did not state if allocators were blinded. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: blinding is not possible in these types of studies. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Cooment: research assistants conducting the assessments were blinded to assignment of dyads. |
| Blinding of outcome assessment (detection bias) Attachment | Low risk | Comment: research assistants conducting the assessments were blinded to assignment of dyads. |
| Blinding of outcome assessment (detection bias) Child behaviour | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: attrition is balanced between both arms. However, 4/5 who dropped out in the intervention group dropped out because the child was placed into foster care; this did not happen to any families in the control arm, suggesting that the groups potentially were unbalanced in level of risk, despite randomisation. There is no mention of an ITT analysis. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Negrão 2014.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 55 Number randomised to each group: intervention = 29, control = 26 Participants: mothers Mean age: mothers = 29.98 years (SD = 6.19 years) at baseline; children = 29.07 months (SD = 10.49 months) at baseline Ethnicity: 100% Portuguese Inclusion criteria: families with children aged 1‐4 years; on families' Risks and Strengths profile, the presence of at least 1 out of the 23 risk items related to quality of family relations or quality of parenting; living with biological mother as primary caregiver; Portuguese Exclusion criteria: children with severe medical conditions; families from ethnic minorities Country: Portugal Setting: community |
|
| Interventions |
Duration of intervention: about 4 months Number of sessions and frequency: 6 visits. First 4 visits at 2‐week intervals and the last 2 sessions at 1 month apart Intervention: VIPP‐SD. Manualised programme with series of topics to be covered. Each session included videotaping interactions and reviewing video from the previous session. Fathers were invited to participate in last 2 sessions. Booklet with summary information given at end Control: parallel in timing, received 6 telephone calls. Each telephone call revolved around a standard topic regarding child development. |
|
| Outcomes |
Timing of outcome assessment: 1 month postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity and parenting stress at 1‐month follow‐up |
|
| Notes |
Source(s) of funding: Fundação Ciência e Tecnologia (grant numbers: SFRH/BD/45273/2008 and SFRH/BD/48411/2008) Conflict(s) of interest: none stated Comment(s): we obtained the data on parental stress outcomes, which were used in the meta‐analysis, directly from the study authors for the purposes of this review only (Pereira 2018 [pers comm]). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "researchers randomly assigned families...based on a computer‐generated list, stratified by child’s age group, gender, and temperament (considering Portuguese clinical cutoff scores of difficult temperament for the Infant Characteristics Questionnaire)". |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "A team of raters, unaware of experimental condition and other data concerning the participants, independently coded the mother and child scales." |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: The outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: missing data were not imputed, and families who did not have complete data were excluded from the final analysis. However, attrition was reasonably balanced between groups, with similar reasons for dropout across groups, so attrition is likely to have had a low impact on the study results. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Platje 2018.
| Methods |
Design: parallel‐group RCT Unit of allocation: parent‐child dyad Dates of recruitment to trial: not reported. Dates of trial: 01 September 2009‐01 May 2016 |
|
| Participants |
Number randomised: 86 Number randomised to each group: intervention = 44, control = 42 Participants: mothers and fathers (85% of parents in the intervention group were mothers, 89% of parents in the control group were mothers) Mean age: parents: intervention = 34.5 years (SD = 5.5 years), control = 35.65 years (SD = 4.88 years), at baseline; children: intervention = 3.36 years (SD = 1.2 years), control = 3.22 years (SD = 1.02 years), at baseline Ethnicity: intervention = 91% Dutch, control = 86% Dutch; the ethnicity of the other parents was not reported Inclusion criteria: "parents of children aged 1‐5 years with visual or visual and intellectual disability" (quote) Exclusion criteria: none Country: CBCL Setting: community |
|
| Interventions |
Duration of intervention: 9 months Number of sessions and frequency: 7 sessions, each lasting 90 min. The first 5 sessions occurred every 2‐3 weeks and the last 2 sessions took place every 2 months. Intervention: VIPP‐V. Based on original VIPP programme, with "an added component each session addressing specific skills which (parents of) children with visual or visual‐and‐intellectual disabilities often experience difficulties with" (quote) Control: care as usual, with varying frequency of support offered |
|
| Outcomes |
Timing of outcome assessment: all at post‐test and at 6 months postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: parental sensitivity and parent stress, assessed at postintervention |
|
| Notes |
Source(s) of funding: ZonMW‐Inzicht (grant number 60‐00635‐98‐126) Conflict(s) of interest: none stated Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed as stratified (on age and organization) block randomization with a 1:1 allocation using a computerized random number generator." |
| Allocation concealment (selection bias) | Unclear risk | Comment: if allocators were aware of the size of the block, then bias could have been introduced. No information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind parents or personnel from allocation in this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "Videotapes were randomly assigned to a pool of three trained coders, who were blind to condition and assessment". |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: ITT analysis undertaken. However, there was greater attrition in the intervention arm, potentially because of factors relating to the outcomes, suggesting that participants in the two arms were not comparable at baseline despite randomisation. |
| Selective reporting (reporting bias) | Low risk | Comment: trial protocol registered at Nederlands Trial Register (NTR4306). Reported on all outcomes in published protocol |
| Other bias | Low risk | Comment: none |
Poslawsky 2015.
| Methods |
Design: parallel‐group, RCT Unit of allocation: parent‐child dyad Dates of recruitment to trial: June 2008‐April 2012 |
|
| Participants |
Number randomised: 78 Number randomised to each group: intervention = 40, control = 38 Participants: primary caregivers (90% mothers, 10% other) of children with autism spectrum disorder (ASD) Mean age: primary caregivers = 36.6 years (SD = 5.04 years) at baseline; children = 43 months (SD = 9.96 months) at baseline Ethnicity: not reported Inclusion criteria: children aged 0‐5 years, diagnosed with ASD at the university hospital, and their primary caregiver; child and primary caregiver lived at same address; a permanent residence; both parents consented Exclusion criteria: primary caregiver who did not speak Dutch; primary caregivers who did not care for the child; children with interfering comorbid medical problems Country: CBCL Setting: home |
|
| Interventions |
Duration of intervention: around 2 months Number of sessions and frequency: 5 fortnightly visits lasting 60‐90 min Intervention: VIPP‐AUTI. During the home visits, video feedback was provided using film fragments of parent‐child interactions videotaped in the previous session. Control: 5 home visits of 1.5 h, 1‐4 weeks apart, with discussions about parenting, plus usual care |
|
| Outcomes |
Timing of outcome assessment: immediately postintervention and 3 months postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity and parenting stress, assessed at immediately postintervention. We did not include social development in the meta‐analysis as the scale used measured different domains of that outcome to the other study reporting this outcome. |
|
| Notes |
Source(s) of funding: Netherlands Organization for Scientific Research Conflict(s) of interest: none stated Comment(s): we excluded outcome data with children aged > 4 years 11 months at baseline. We requested data for parental stress at 3 months' follow‐up, but the corresponding author was not able to provide the data (Poswlawsky 2018 [pers comm]), so we used reported outcomes that included children outside of our target age group in the meta‐analysis. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomization by computer generated tables" |
| Allocation concealment (selection bias) | Low risk | Comment: randomization by computer‐generated tables by a staff manager, who was not involved in the research project. Randomly assigned to 2 groups indicated by number. Staff manager did not know which number belonged to which group |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "The play sessions were coded by five trained observers...who were unaware of the intervention type parents received." |
| Blinding of outcome assessment (detection bias) Parental stress | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Blinding of outcome assessment (detection bias) Child socioemotional development | Low risk | Quote: "The play sessions were coded by five trained observers who were unaware of the intervention type parents received." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no mention of ITT analysis. However, there was low attrition; reasons for loss to follow‐up were clearly stated and unlikely to be relevant to outcomes. Therefore, the impact of attrition on the final study results is likely to be low. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Seifer 1991.
| Methods |
Design: quasi‐RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not reported |
|
| Participants |
Number randomised: not reported Number randomised to each group: not reported. Number in each group: intervention = 23, control = 17 Participants: mothers Mean age: mothers: intervention = 28 years (SD = 4.6 years), control = 30 years (SD = 5.5 years) at baseline; children: 8.5 months (SD = 5.6 months) at baseline, after correction for prematurity Ethnicity: intervention = 30% from BME backgrounds, control = 58% from BME backgrounds. Across both groups, 24 mothers were white, 13 were black and 3 were Hispanic Inclusion criteria: participants from a "comprehensive early intervention program for children with developmental disability" (quote) Exclusion criteria: none stated Country: USA Setting: clinic |
|
| Interventions |
Duration of intervention: 8 months Number of sessions and frequency: up to 6 sessions, weekly Intervention: interaction coaching. Videotaping of mother‐child interactions, followed by reviewing, with suggestions from therapists about how to improve the interaction Control: no treatment. Mothers watched videotapes of their interactions with their child, but did not receive any feedback. Both groups also received the early intervention programme. |
|
| Outcomes |
Timing of outcome assessment: postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal responsive behaviour at postintervention |
|
| Notes |
Source(s) of funding: US Department of Education's Special Education Programs, Handicapped Children's Early Education Programs and National Institute of Handicapped Research Conflict(s) of interest: none stated Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Comment: quasi‐randomised trial. Sequence generation was based on the day of attendance at the early intervention programme from which participants were recruited. |
| Allocation concealment (selection bias) | High risk | Comment: allocation was based on day of attendance at the early intervention programme from which participants were recruited. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Comment: videotape coders were blinded to the study hypothesis. |
| Blinding of outcome assessment (detection bias) Child socioemotional development | Low risk | Comment: videotape coders were blinded to the study hypothesis. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: not reported. The study authors report that the participants in each arm were those who had completed all assessments, but it is not clear whether there were others who had partially completed assessments who were excluded. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no trial protocol available |
| Other bias | Low risk | Comment: none |
Stein 2006.
| Methods |
Design: parallel‐group, RCT Unit of allocation: mother‐child dyads Dates of recruitment to trial: 08 December 2004‐01 January 2006 |
|
| Participants |
Number randomised: 80 Number randomised to each group: intervention = 40, control = 40 Participants: mothers Mean age: mothers = not reported (median age: intervention = 31 years, control = 29 years, at baseline); children = not reported (range = 4‐6 months) Ethnicity: 70% white, 30% other Inclusion criteria: "women ages 18–45 years with children between 4 and 6 months old. The women met the DSM‐IV diagnostic criteria for an eating disorder, either bulimia nervosa or a similar form of eating disorder of clinical severity, i.e., a bulimic subtype of eating disorder not otherwise specified (4). The inclusion criteria were 1) overevaluation of body shape or weight to a degree reaching clinical severity, 2) recurrent episodes of loss of control over eating (i.e., subjective or objective bulimic episodes), and 3) secondary social impairment." (quote) Exclusion criteria: "Mothers with severe comorbid psychiatric disorders" (quote) Country: UK Setting: home |
|
| Interventions |
Duration of intervention: 6‐8 months Number of sessions and frequency: 13 sessions, each lasting 1 h Intervention: video feedback focused around mother‐child conflict at mealtimes Control: supportive counselling "Both groups also received guided cognitive behavior self‐help for eating disorders" (quote) |
|
| Outcomes |
Timing of outcome measurement: 1 month postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity. There were multiple domains of maternal sensitivity reported. After discussion, we felt that "verbal responses to infant cues" was the most appropriate to combine in the meta‐analysis. |
|
| Notes |
Source(s) of funding: Wellcome Trust (grant number 050892) and funding from the North Central London Research Consortium for the recruitment process in primary care Conflict(s) of interest: none reported Comment(s): we obtained the maternal sensitivity outcomes directly from the study authors as they were reported as medians in the original published paper, which were not suitable for the meta‐analysis. We obtained the means and standard deviations for use in the meta‐analysis (Stein 2018 [pers comm]). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "mothers were randomly assigned to the two interventions by using block randomization with fixed blocks of size 6, computer generated by an independent statistician and stratified according to eating disorder diagnosis (bulimia nervosa or bulimic type of eating disorder not otherwise specified)" |
| Allocation concealment (selection bias) | Low risk | Quote: "Allocation concealment was facilitated by using sequentially numbered opaque sealed envelopes for consecutive and eligible study participants." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of study. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "All videotapes were rated by independent raters blind to group assignment." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: there is no mention of an ITT analysis or a strategy to impute missing data. However, there was very low attrition and reasons for dropout do not seem to be related to factors linked to outcomes. Therefore, the impact of attrition on the final study results is likely to be low. |
| Selective reporting (reporting bias) | Low risk | Comment: study protocol registered (ISRCTN 95026274) and all protocol outcomes reported. |
| Other bias | Low risk | Comment: none |
Van Zeijl 2006.
| Methods |
Design: parallel‐group, RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: May 2001‐December 2002 |
|
| Participants |
Number randomised: 237 Number randomised to each group: intervention = 120, control = 117 Participants: mothers Mean age: mothers = 33.15 years (SD 4.22 years), children = 26.99 months (SD = 9.98 months) at pre‐test Ethnicity: 100% Dutch Inclusion criteria: participants of Dutch cultural background; children living with 2 parents (biological mother as the primary caregiver and biological or stepfather as the second caregiver); children with scores > 75th percentile on the CBCL for ages 1.5‐5; externalising problem scale scores ≥ 13 for those aged 1 year ≥ 19 for those aged 2 years, and ≥ 20 for those aged 3 years Exclusion criteria: mothers with serious medical conditions; twins and children with serious medical conditions Country: the Netherlands Setting: home |
|
| Interventions |
Duration of intervention: 8 months Number of sessions and frequency: 6 sessions. First 4 intervention sessions took place every month and the last 2 sessions took place every other month; each session lasted 1.5 h Intervention: adhered to VIPP‐SD protocol; intervener provided personal feedback on parenting, using videotaped mother‐child interaction in each session Control: mothers in the control group were given 6 telephone calls with a general discussion about their child. Minimal advice and information given |
|
| Outcomes |
Timing of outcome assessment: 4 months postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity. We did not include child behaviour problems in the meta‐analysis as they were measured at a different time point to other studies reporting this outcome. |
|
| Notes |
Source(s) of funding: ZorgOnderzoek Nederland (Netherlands Organization for Health Research and Development; grant number 2200.0097) Conflict(s) of interest: none stated Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a computer generated list randomly assigned families stratified by age" |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Unclear risk | Comment: no information given |
| Blinding of outcome assessment (detection bias) Child behaviour | High risk | Comment: the outcome was measured using a self‐report scale. As participants were not blinded to the intervention, this may have biased their responses, leading to an overestimate of effect of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk |
Quote: "Missing values seem to be randomly distributed across items and participants and therefore they were substituted with the mean score on the variable for children with the same sex, age, parental education level, and experimental condition, as a conservative imputation method to uniformly include the total set of 237 in the analyses." Comment: therefore, the impact of missing data on the final study results is likely to be low |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
Yagmur 2014.
| Methods |
Design: parallel‐group RCT Unit of allocation: mother‐child dyad Dates of recruitment to trial: not stated |
|
| Participants |
Number randomised: 86 Number randomised to each group: intervention = 44, control = 42 Participants: mothers Mean age: mothers = 29.96 years (SD = 3.45 years) at baseline; children = 30.83 months (SD = 6.44 months) at baseline Ethnicity: 100% Turkish Inclusion criteria: child aged 18 months‐3 years; 2nd generation Turkish mothers born in the Netherlands (who have at least 1 parent born in Turkey); CBCL 1.5‐5; externalising problem scale > 75th percentile Exclusion criteria: severe mental or physical health problems of mother or child Country: CBCL Setting: home |
|
| Interventions |
Duration of intervention: 3 months Number of sessions and frequency: 6 visits every two weeks, lasting 2.5‐3 h Intervention: used VIPP‐SD adapted to Turkish minority families (VIPP‐TM) protocol. Intervention sessions took place every 2 weeks. All participants received 6 home visits and completed all steps. Duration of each home visit was 2.5‐3 h. Control: parallel to the intervention sessions, the mothers in the control group received 6 telephone calls, lasting 15‐30 min. |
|
| Outcomes |
Timing of outcome assessment: 6 months postintervention Outcome(s) of interest:
Outcome(s) included in meta‐analysis: maternal sensitivity, assessed at 6 months postintervention |
|
| Notes |
Source(s) of funding: ZorgOnderzoek Nederland (Netherlands Organization for Health Research and Development; grant number 15700.1011); NORFACE (New Opportunities for Research Funding Co‐operation Agency in Europe) research programme on Migration in Europe ‐ Social, Economic, Cultural and Policy Dynamics; Netherlands Organization for Scientific Research Conflict(s) of interest: none stated Comment(s): none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "[dyads] randomly allocated to the intervention or control group (dummy intervention), stratified for age group, gender, and the presence of siblings…after the pretest, a computer‐generated list randomly assigned families" |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information was reported on whether allocation after randomisation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it is not possible to blind participants and personnel to this type of intervention. |
| Blinding of outcome assessment (detection bias) Parental sensitivity | Low risk | Quote: "The three coders were unaware of the experimental condition". |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: dropout is unbalanced across the 2 arms, and some of the reasons for dropout seem related to the intervention (e.g. objection to video recording). There is no mention of an ITT analysis. Therefore, it is possible that attrition might result in an overestimate of the impact of the intervention on the final study results. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none |
ADOS‐G: Autism Diagnostic Observation Schedule ‐ Generic;BASIS: British Autism Study of Infant Siblings; BME: black and minority ethnic; CARE‐Index: Child‐Adult Relationship Experimental Index; CBCL: Child Behaviour Checklist; CCMO: Centrale Commissie Mensgebonden Onderzoek; DSM‐IV:Diagnostic and Statistical Manual of Mental Disorders ‐ Fourth Edition;iBASIS‐VIPP: Intervention in the British Autism Study of Infant Siblings ‐ Video Interaction for promoting Positive Parenting); ITT: intention‐to‐treat NCATS: Nursing Child Assessment Teaching Scale; NIHR: National Institute for Health Research; PACT: Preshool Autism Communication Trial; RCT: randomised controlled trial; SD: standard deviation; SE standard error; VIG: Video Interaction Guidance; VIPI: Video‐feedback of Infant‐Parent Interaction; VIPP: Video‐feedback Intervention to promote Positive Parenting;VIPP‐AUTI: Video‐feedback Intervention to promote Positive Parenting adapted to Autism; VIPP‐LD: Video‐feedback Intervention to promote Positive Parenting ‐ Learning Disabilities; VIPP‐R: Video‐feedback Intervention to promote Positive Parenting ‐ Representational level; VIPP‐SD: Video‐feedback Intervention to promote Positive Parenting ‐ Sensitive Discipline; VIPP‐V: Video‐feedback Interaction to promote Positive Parenting ‐ Visual or visual‐intellectual disability.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Akai 2008 | Intervention has no video‐feedback component |
| Aldred 2001 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Aldred 2004 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Bernard 2012 | Video interaction sessions were part of a multi‐component intervention |
| Bilszta 2012 | Does not measure parental sensitivity, child attachment or reflective functioning outcomes |
| Borghini 2014 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Brisch 2003 | Video interaction sessions were part of a multi‐component intervention |
| Bunder 2011 | Not an RCT or quasi‐RCT |
| Cassiba 2015 | Not an RCT or quasi‐RCT |
| Cates 2012 | Does not measure parental sensitivity, child attachment or reflective functioning outcomes |
| Dozier 2006 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Durett 1984 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Feeley 2012 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Glanemann 2013 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Groeneveld 2011 | Caregivers do not match this review's inclusion criteria (Criteria for considering studies for this review) |
| Groeneveld 2016 | Caregivers do not match this review's inclusion criteria (Criteria for considering studies for this review) |
| Guttentag 2014 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Huber 2016 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Juffer 1997 | Comparison between two intervention programmes rather than intervention and inactive alternative intervention |
| Juffer 2005 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Kim 2005 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Krupka 1995 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Lambermon 1989 | Intervention has no video‐feedback component |
| Landry 2006 | Intervention has no video‐feedback component |
| Lindheim 2009 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Magill‐Evans 2007 | Caregivers do not match this review's inclusion criteria (Criteria for considering studies for this review) |
| Mendelsohn 2005 | Does not measure parental sensitivity, child attachment or reflective functioning outcomes |
| NCT03397719 | Does not measure parental sensitivity, child attachment or reflective functioning outcomes |
| Sheese 2007 | Intervention has no video‐feedback component |
| Smith 2013 | Intervention contained multiple sessions of non‐video‐feedback intervention activities |
| Solomon 2014 | Video interaction sessions were part of a multi‐component intervention |
| Spieker 2012 | Video interaction sessions were part of a multi‐component intervention |
| Sprang 2009 | Video interaction sessions were part of a multi‐component intervention |
| Svanberg 2010 | Not an RCT or quasi‐RCT |
| Van Balkom 2010 | Comparison between 2 intervention programmes, rather than intervention and inactive alternative intervention |
| Van Doesum 2008 | Video interaction sessions were part of a multi‐component intervention |
| Weiner 1994 | Not an RCT or quasi‐RCT |
RCT: randomised controlled trial
Characteristics of studies awaiting assessment [ordered by study ID]
Mendelsohn 2008.
| Methods | RCT |
| Participants | Families |
| Interventions | Video interaction |
| Outcomes | Not known |
| Notes | We believe this to be a report of Mendelsohn 2005, but the web link retrieved during searches is no longer active. We contacted the study author but did not receive a reply (Smith 2018a [pers comm]). |
RCT: randomised controlled trial.
Characteristics of ongoing studies [ordered by study ID]
Euser 2016.
| Trial name or title | Efficacy of the video‐feedback intervention to promote Positive Parenting and Sensitive Discipline in Twin families (VIPP‐Twins) |
| Methods | Parallel‐group RCT |
| Participants |
Inclusion criteria: parents of twins of the same gender who are fluent in Dutch. Parents and grandparents of the twins must be born in Europe. Exclusion criteria: "Children with a congenital disability, psychological disorder, chronic illness, hereditary disease, or a visual or hearing impairment were excluded if the disorder will likely disable the child from performing the behavioral tasks or participating in the intervention. Also, children with a previously diagnosed intellectual disability (IQ < 70) were excluded from participation." (quote) Country: CBCL Setting: the community |
| Interventions |
Intervention: VIPP‐Twins; adapted form of VIPP, consisting of five 2‐weekly sessions with a female facilitator Control: 6 phone calls to parents where they are asked to talk about their children's development |
| Outcomes |
Timing of outcome assessment: 1 month and 2 years postintervention Outcome(s) of interest:
|
| Starting date | 20 July 2015 |
| Contact information | Email: s.euser@fsw.leidenuniv.nl |
| Notes |
Trial registry number:NTR5312 Source(s) of funding: Gravitation program of the Dutch Ministry of Education, Culture, and Science and The Netherlands Organization for Scientific Research (NWO grant number 024.001.003). Additional funding was provided by The Netherlands Organization for Scientific Research (MJBK: VICI Grant no. 453‐09‐003; MHvIJ: NWO Spinoza prize). Conflict(s) of interest: none stated |
Firk 2015.
| Trial name or title | A mother‐child intervention program in adolescent mothers and their children to improve maternal sensitivity, child responsiveness and child development (the TeeMo study): study protocol for a randomized controlled trial |
| Methods | Parallel‐group RCT |
| Participants |
Inclusion criteria: "Maternal criteria: 21 years old or younger at the beginning of pregnancy; Mother and child live together; Sufficient verbal and intellectual abilities to participate in a verbal training program; Caucasian; Written informed consent of the mother and, if <18 years old, of the caregiver of the mother. Child criteria: Between 3 and 6 months old; Written informed consent of the caregiver" (quote) Exclusion criteria: "Maternal criteria: Current substance abuse; Current suicidal ideation; Psychotic disorders; Separation from the child (>3 months)". Child criteria: Preterm birth (<36 weeks gestation); Serious medical problems; Genetic syndromes" (quote) Country: Germany Setting: community |
| Interventions |
Intervention: "STEEP‐b was designed to be relatively brief, completed in 12 to 18 sessions, and started when the children are between 3 and 6 months of age...Adolescent mothers are visited at home every 2 to 3 weeks by the same adviser for 9 months. Furthermore, an optional group meeting is offered every second month that mothers can attend. The exact number of sessions will depend on clinical appropriateness in the 9‐month window." (quote) Control: treatment as usual |
| Outcomes |
Timing of outcome assessment: postintervention and 6 months postintervention Outcome(s) of interest:
|
| Starting date | October 2012 |
| Contact information | Email: rschwarte@ukaachen.de |
| Notes |
Trial registry number:DRKS00004409 Source(s) of funding: German Ministry for Research and Education (BMBF) Conflict(s) of interest: none stated |
ISRCTN92360616.
| Trial name or title | Preterm infant parent programme for attachment (PIPPA study) |
| Methods | Parallel‐group RCT |
| Participants |
Inclusion criteria: "Babies who are born at or less than 32 weeks in the National Maternity Hospital, Dublin and their parents, who are from the area which the hospital serves can take part." (quote) Exclusion criteria: "1. Known major congenital anomaly incompatible with life; 2. Parents' level of English will make completion of the semi‐structured interview difficult; 3. Family does not live within the catchment area of National Maternity Hospital (NMH)." (quote) Country: Ireland Setting: hospital |
| Interventions |
Intervention: PIPPA programme, offered as 3 sessions during an inpatient admission. The first 2 sessions explore the experience of preterm birth, then the baby's cues. The third session involves reviewing a 5‐min video made during the previous session. Control: routine care |
| Outcomes |
Timing of outcome assessment: 6 months postintervention, with the exception of 3 outcomes; social‐emotional development, follow‐up period not specified, and infant biomarkers and MRI, measured at 2 years postintervention Outcome(s) of interest:
|
| Starting date | Enrolment began May 2012 |
| Contact information | Email: atwohig@nmh.ie |
| Notes |
Trial registry number:ISRCTN92360616 Source(s) of funding: National Children's Research Centre, Ireland Conflict(s) of interest: none |
NCT03052374.
| Trial name or title | Video‐feedback interaction guidance for improving interactions between depressed mothers and their infants ("VID‐KIDS") |
| Methods | Parallel‐group RCT |
| Participants |
Inclusion criteria: new mothers > 16 years of age with an Edinburgh Postnatal Depression score of > 12 Exclusion criteria: none Country: Canada Setting: home |
| Interventions |
Intervention: video feedback tailored to mothers in this group; offered as 3 sessions in the home. Each session involves recording the mother‐child interaction and reviewing the recording multiple times. Control: standard care |
| Outcomes |
Timing of outcome assessment: measured at study completion Outcome(s) of interest:
|
| Starting date | 01 May 2017 |
| Contact information | Email: andrea.deane@ahs.ca |
| Notes |
Trial registry number:NCT03052374 Source(s) of funding: none stated Conflict(s) of interest: none |
Schoemaker 2018.
| Trial name or title | The effectiveness of Video‐feedback Intervention to promote Positive Parenting for Foster Care (VIPP‐FC) |
| Methods | Parallel‐group RCT |
| Participants |
Inclusion criteria: "foster families with a foster child of 1 to 6 years of age" (quote) Exclusion criteria: "part time or short‐term crisis placements...Children with severe physical disabilities, diagnosed intellectual disability (IQ < 70) and/or diagnosed autism spectrum disorder...Twins who were placed in the same foster family" (quote) Country: CBCL Setting: home |
| Interventions |
Intervention: "The intervention consists of six home visits: The first four sessions are biweekly and there is an interval of approximately 3 weeks between sessions four and five and sessions five and six. During each home visit, the participating foster parent (primary caregiver) and child are filmed during daily situations for 10 to 30 min, such as playing, mealtime or reading a book together." (quote) Control: 6 dummy phone calls |
| Outcomes |
Timing of outcome assessment: post‐test and 3 months postintervention Outcome(s) of interest:
|
| Starting date | 01 August 2013 |
| Contact information | Email: alinklra@fsw.leidenuniv.nl |
| Notes |
Trial registry number:NTR3899 Source(s) of funding: Stichting Kinderpostzegels Nederland; The Netherlands Organization for Scientific Research (Vidi grant: 016.145.360 Meerwaarde grant: 475–11‐002) Conflict(s) of interest: none |
CBCL: Child Behaviour Checklist; IQ: Intelligence quotient; MRI: magnetic resonance imaging; NWO: Netherlands Organisation for Scientific Research; PIPPA: Preterm Infant Parent Programme for Attachment; RCT: randomised controlled trial; STEEP‐b: Steps Towards Effective and Enjoyable Parenting ‐ b; VIPP: Video‐feedback Intervention to promote Positive Parenting.
Differences between protocol and review
Title. We changed the title of the review from 'Video feedback for improving parental sensitivity and attachment' (O'Hara 2016) to 'Video feedback for parental sensitivity and attachment security in children under five years' following feedback, as we felt that the original title somewhat pre‐empted the results of the review.
Additional authors. The following authors have been added to the review since the publication of the protocol (O'Hara 2016): Emily Smith, Yinghui Wei and Thees Spreckelsen.
Objectives. We added in the qualifier "at risk for poor attachment outcomes" to the description of our population group of interest for clarity.
Types of participants. We clarified our intention to look only at interventions used with high‐risk parent‐child dyads, as this was not clearly stated in the protocol (O'Hara 2016).
-
We amended the types of interventions included from those "with the aim of improving the sensitivity of their [the parents'] interactions with the child or the mental representations of the parent" to those "with the aim of improving the sensitivity of their [the parents'] interactions with the child, child attachment, or the reflective functioning of the parent", because these were our primary outcomes.
In addition to including studies where the comparison group was treatment as usual or no treatment, we also included studies where the comparison group received an attention placebo, because these are standard control conditions.
We excluded studies that did not measure parental sensitivity, child attachment or parental reflective functioning, or did not do so in an objective way, because these were our primary outcomes.
Secondary outcomes. Although we stated in the Measures of treatment effect section of our protocol that we would collect information on costs, we did not list it as an outcome. We have added costs to the list of secondary outcomes.
Searching other resources. We did not contact experts in the field to ask about any published, unpublished or ongoing work that we might have missed, due to limitations of time.
Data collection and analysis. We removed methods that we were unable to use from the main text and reported them in Table 2.
Data extraction and management. We extracted data on the dates of the studies, in addition to the other information prespecified in our protocol (O'Hara 2016), at the request of our Editor.
Data synthesis. In our original protocol we specified that we would collect outcomes data grouped "as postintervention (immediately upon completion of the intervention), short term (up to six months), medium term (up to one year) and long term (over one year)". In our meta‐analysis, we grouped postintervention and short‐term follow up for the outcomes ‘parental sensitivity’ and ‘parental stress’. This was for two reasons: firstly, we found that the 'postintervention' time point was not always clearly specified by studies, and in some cases may possibly overlap with time points described as 'short term' in other studies; secondly, we wanted to maximise our use of available data. We felt that combining postintervention and short‐term follow‐up time points was clinically justifiable.
Assessment of reporting biases. We made a post hoc decision to undertake Egger's regression test (Egger 1997), to assist our assessment of funnel plot asymmetry, in addition to purely visual inspection. We made this decision to strengthen our assessment of the asymmetry.
-
The protocol, O'Hara 2016, stated we would use the following comparisons in our 'Summary of findings' table: 'Video feedback versus no intervention' and 'Video feedback versus alternative intervention'. We amended this for clarity, to make it clear that the comparison would be video feedback versus no intervention or inactive intervention only, as our protocol also stated that we would exclude studies that had an active alternative treatment.
The protocol, O'Hara 2016, stated that we would include a rating of the quality of evidence in our 'Summary of findings' table. However, the version of GRADE that we used rated certainty, not quality.
Subgroup analysis and investigation of heterogeneity. We made a post hoc decision to undertake a moderator analysis of the impact of five moderating factors on parental sensitivity in response to a comment from our Editor. We have included the methods and results from this analysis in the review. Three of the factors were based on prespecified factors (intensity of video feedback, defined by the number of sessions; type of video feedback, based on whether it was Video Feedback Intervention to Promote Positive Parenting (VIPP) or not; participating carers, based on whether carers were mothers, fathers or both mothers and fathers). Groupings of these three factors were decided post hoc. Two factors were based on post hoc decisions (child disability; age of child).
Contributions of authors
Leeanne O'Hara (LOH), Nadeeja Herath (NH), Jane Barlow (JB), Nuala Livingstone (NL) and Geraldine Macdonald (GM) contributed to developing the protocol and methods for this review. LOH conducted the searches. LOH, Emily Smith (ES) and NH contributed to screening searches and data extraction. LOH and ES carried out 'Risk of bias' assessments and GRADE ratings. JB, NL and GM provided guidance and support in resolving disagreements between reviewer authors' opinions during these processes; JB did not arbitrate in cases of dispute of studies in which she was involved. ES conducted the meta‐analysis with statistical support from Yinghui Wei. Thees Speckelsen (TS) conducted the moderator analysis. JB, NL and GM contributed to decisions about which analyses to undertake. LOH, ES, JB, NL, TS and GM contributed to writing up the results of the review. LOH is the guarantor for the review.
Sources of support
Internal sources
-
Queen's University Belfast, UK.
Salary costs for LOH
-
St Helens and Knowsley Teaching Hospitals NHS Trust, UK.
ES is employed by this Trust.
-
Walsall Healthcare NHS Trust, UK.
ES was employed by this Trust for part of the time period she has been involved in this review.
-
University of Warwick, UK.
ES held an NIHR (National Institute for Health Research) Academic Clinical Fellowship that was hosted by the University of Warwick. She completed her work on the review whilst on placement at the University as part of this Fellowship (the views expressed in this review are those of the authors and do not represent those of NIHR, the Department of Health or the NHS).
-
University of Oxford, UK.
Salary costs for TS as a departmental lecturer.
External sources
-
Health and Social Care Research and Development Division, Public Health Agency, UK.
Cochrane Fellowship Award to LOH
-
NIHR Academic Clinical Fellowship, UK.
Salary and study expenses to attend Cochrane Review Author Training for ES (the views expressed in this review are those of the authors and do not represent those of NIHR, the Department of Health or the NHS).
Declarations of interest
Leeanne O'Hara received a Cochrane Fellowship Award from the Health and Social Care Research and Development Division of the Public Health Agency, Belfast, to cover salary expenses, travel, training and research expenses.
Jane Barlow (JB) is the lead author of one of the included studies (Barlow 2016), which was funded by the Grace Fund to evaluate VIG with mothers of preterm infants; she is also in the process of resubmitting an application to NIHR to evaluate the effectiveness of VIG with women experiencing perinatal mental health problems. JB did not extract data from this study, nor did she assess the study for eligibility, assess its potential risk of bias or grade the certainty of its evidence. JB is a coapplicant on a recently funded National Institute for Health Research (NIHR), Health Technology Assessment (HTA) feasibility study of the use of Video‐feedback Intervention to promote Positive Parenting (VIPP) with young children with reactive attachment disorder living in foster care. JB began a training programme to learn how to deliver Video Interaction Guidance but discontinued this and therefore did not receive any accreditation. JB is an Editor with Cochrane Developmental, Psychosocial and Learning Problems (CDPLP).
Nuala Livingstone is an Editor with CDPLP and the Cochrane Editorial and Methods Department.
Geraldine Macdonald is the Co‐ordinating Editor of CDPLP.
Emily Smith (ES) held an NIHR‐funded Academic Clinical Fellowship at the University of Warwick and undertook work for this review whilst on placement. This funding covered her salary, training and travel expenses for the purpose of this review. ES was previously employed by Walsall Healthcare NHS Trust, who granted her study leave to undertake training to carry out this review, and is currently employed by St Helens and Knowsley Teaching Hospitals NHS Trust.
Nadeeja Herath ‐ none known.
Yinghui Wei is a Statistical Editor with CDPLP.
Thees F Spreckelsen (TS) is an Associate Editor (quantitative methods) for the journal Child and Adolescent Mental Health for which he receives an honorarium. TS has worked previously as a quantitative analyst on two industry‐funded (DSM (Dutch State Mines ‐ 'De Nederlandse Staatsmijnen')) randomised controlled trials on omega‐3 DHA (docosahexaenoic acid) supplementation as an intervention for child learning and behaviour (DOLAB study (DHA Oxford Learning and Behaviour) I and II). TS has undertaken paid analyses of clinical records of children and adolescents living with HIV in Nigeria for the International Catholic Relief Services and received an honorarium for teaching introductions to R at the Department of Education's Advanced Quantitative Methods Summer School at the University of Oxford. TS declares that these activities do not relate directly to the content of this review.
Disclaimer: The views expressed in this article are those of the authors, and not of NIHR, the NHS or the Department of Health.
New
References
References to studies included in this review
Barlow 2016 {published data only}
- Barlow J, Sembi S, Underdown A. Pilot RCT of the use of video interactive guidance with preterm babies. Journal of Reproductive and Infant Psychology 2016;34(5):511‐24. [DOI: 10.1080/02646838.2016.1217404] [DOI] [Google Scholar]
Barone 2019 {published and unpublished data}
- Barone L. Re: Cochrane systematic review: data request [personal communication]. Email to: E Smith 10 July 2019.
- Barone L, Barone V, Dellagiulia A, Lionetti F. Testing an attachment‐based parenting intervention‐VIPP‐FC/A in adoptive families with post‐institutionalized children: do maternal sensitivity and genetic markers count?. Frontiers in Psychology 2018;9:156. [DOI: 10.3389/fpsyg.2018.00156; 29515483; PMC5826058 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barone L, Ozturk Y, Lionetti F. The key role of positive parenting and children’s temperament in post‐institutionalized children’s socio‐emotional adjustment after adoption placement. A RCT study. Social Development 2019;28(1):136‐51. [DOI: 10.1111/sode.12329] [DOI] [Google Scholar]
Benzies 2013 {published data only}
- Benzies KM, Magill‐Evans J, Kurilova J, Nettel‐Aguirre A, Blahitka L, Lacaze‐Masmonteil T. Effects of video‐modeling on the interaction skills of first‐time fathers of late preterm infants. Infants and Young Children 2013;26(4):333‐48. [DOI: 10.1097/IYC.0b013e3182a4ed5e] [DOI] [Google Scholar]
Bovenschen 2012 {published and unpublished data}
- Bovenschen I. Systematic review ‐ study data [personal communication]. Email to: E Smith 26 March 2019.
- Bovenschen I, Gabler S, Spangler G, Pillhofer M, Künster A. Video‐based intervention for mother‐infant‐dyads at risk: effects on maternal sensitivity [Videogestützte beratung zur beziehungsförderung bei jungen müttern und ihren säuglingen]. Psychologie in Erziehung und Unterricht 2012;59(4):275‐89. [DOI: 10.2378/peu2012.art21d] [DOI] [Google Scholar]
Green 2010 {published data only}
- Green J, Charman T, McConachie H, Aldred C, Slonims V, Howlin P, et al. Parent‐mediated communication‐focused treatment in children with autism (PACT): a randomised controlled trial. Lancet 2010;375(9732):2152‐60. [DOI: 10.1016/S0140-6736(10)60587-9; PMC2890859 ; PUBMED: 20494434] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pickles A, Couteur A, Leadbitter K, Salomone E, Cole‐Fletcher R, Tobin H, et al. Parent‐mediated social communication therapy for young children with autism (PACT): long‐term follow‐up of a randomised controlled trial. Lancet 2016;388(10059):2501‐9. [DOI: 10.1016/S0140-6736(16)31229-6] [DOI] [PMC free article] [PubMed] [Google Scholar]
Green 2015 {published data only}
- Green J, Charman T, Pickles A, Wan MW, Elsabbagh M, Slonims V, et al. Parent‐mediated intervention versus no intervention for infants at high risk of autism: a parallel, single‐blind, randomised trial. Lancet Psychiatry 2015;2(2):133‐40. [DOI: 10.1016/S2215-0366(14)00091-1; PMC4722333 ; PUBMED: 26359749] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green J, Pickles A, Pasco G, Bedford R, Wan M, Elsabbagh M, et al. Randomised trial of a parent‐mediated intervention for infants at high risk for autism: longitudinal outcomes to age 3 years. Journal of Child Psychology and Psychiatry 2017;58(12):1330‐40. [DOI: 10.1111/jcpp.12728; PMC5724485 ; PUBMED: 28393350] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hodes 2017 {published data only (unpublished sought but not used)}
- Hodes MW, Kef S, Meppelder HM, Schuengel C. The effect of VIPP‐LD intervention with parents with intellectual disabilities on their children's behaviour. Journal of Intellectual Disability Research 2012;56(7‐8):743. [DOI: 10.1111/j.1365-2788.2012.01583_9.x; onlinelibrary.wiley.com/doi/pdf/10.1111/j.1365‐2788.2012.01583_9.x] [DOI] [Google Scholar]
- Hodes MW, Meppelder M, Moor M, Kef S, Schuengel C. Alleviating parenting stress in parents with intellectual disabilities: a randomized controlled trial of a Video‐feedback Intervention to promote Positive Parenting. Journal of Applied Research in Intellectual Disabilities 2017;30(3):423‐32. [DOI: 10.1111/jar.12302; PUBMED: 27878951] [DOI] [PubMed] [Google Scholar]
- Hodes MW, Meppelder M, Moor M, Kef S, Schuengel C. Effects of video feedback intervention on harmonious parent‐child interaction and sensitive discipline of parents with intellectual disabilities: a randomized controlled trial. Child: Care, Health and Development 2018;44(2):304‐11. [DOI: 10.1111/cch.12506; PUBMED: 28868634] [DOI] [PubMed] [Google Scholar]
Hoffenkamp 2015 {published and unpublished data}
- Hoffenkamp HN, Tooten A, Hall RA, Braeken J, Eliëns MP, Vingerhoets AJ, et al. Effectiveness of hospital‐based video interaction guidance on parental interactive behavior, bonding, and stress after preterm birth: a randomized controlled trial. Journal of Consulting and Clinical Psychology 2015;83(2):416‐29. [DOI: 10.1037/a0038401; PUBMED: 25486375] [DOI] [PubMed] [Google Scholar]
- Bakel H. Re: quick query [personal communication]. Email to: J Barlow 12 June 2017.
Høivik 2015 {published and unpublished data}
- Hoivik M. Cochrane review [personal communication]. Email to: E Smith 15 April 2018.
- Høivik MS, Lydersen S, Drugli MB, Onsøien R, Hansen MB, Nielsen TS. Video feedback compared to treatment as usual in families with parent‐child interactions problems: a randomized controlled trial. Child and Adolescent Psychiatry and Mental Health 2015;9:3. [DOI: 10.1186/s13034-015-0036-9; PMC4332722 ; PUBMED: 25699090] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kalinauskiene 2009 {published data only}
- Kalinauskiene L. The possibilities of intervention of mother‐infant attachment relationship [Motinos ir kūdiko prieraišumo santykių korekcijos galimbyės] [PhD thesis]. Vilnius (LT): Vilnius University, 2010. [Google Scholar]
- Kalinauskiene L, Cekuoliene D, Ijzendoorn MH, Bakermans‐Kranenburg MJ, Juffer F, Kusakovskaja I. Supporting insensitive mothers: the Vilnius randomized control trial of video‐feedback intervention to promote maternal sensitivity and infant attachment security. Child: Care, Health and Development 2009;35(5):613‐23. [DOI: 10.1111/j.1365-2214.2009.00962.x; PUBMED: 19323672] [DOI] [PubMed] [Google Scholar]
- Kalinauskiene L, Kusakovskaja I, Cekuoliene D, Kiltanaviciute V. Effects of video‐feedback correction of infant‐mother interaction on two‐year‐olds' behaviour [Motinos ir kūdikio sąveikos korekcijos, pagrįstos vaizdo analizės metodu, pov eikis dvimečių elgesio sunkumams]. Psichologija 2009b;40:53‐65. [DOI: 10.15388/Psichol.2009.0.2586] [DOI] [Google Scholar]
Klein Velderman 2006 {published and unpublished data}
- Bakermans‐Kranenburg M. Systematic review ‐ VIG [personal communication]. Email to: E Smith 24 March 2018.
- Bakermans‐Kranenburg MJ, Breddels‐Van Baardewijk P, Juffer F, Velderman MK, IJzendoorn MH. Insecure mothers with temperamentally reactive infants: a chance for intervention. In: Juffer F, Bakermans‐Kranenberug M, IJzendoorn M editor(s). Promoting Positive Parenting: An Attachment‐Based Intervention. New York (NY): Lawrence Erlbaum Associates/Taylor & Francis Group, 2008:75‐90. [Google Scholar]
- Bakermans‐Kranenburg MJ, Juffer F, Ijzendoorn MH. Interventions with video feedback and attachment discussions: does type of maternal insecurity make a difference?. Infant Mental Health Journal 1998;19(2):202‐19. [DOI: 10.1002/(SICI)1097-0355(199822)19:2%3C202::AID-IMHJ8%3E3.0.CO;2-P] [DOI] [Google Scholar]
- Klein Velderman M, Bakermans‐Kranenburg MJ, Jugger F, IJzendoorn MH. Effects of attachment‐based interventions on maternal sensitivity and infant attachment: differential susceptibility of highly reactive infants. Journal of Family Psychology 2006;20(2):266‐74. [DOI: 10.1037/0893-3200.20.2.266; PUBMED: 16756402] [DOI] [PubMed] [Google Scholar]
- Klein Velderman MK, Bakermans‐Kranenburg MJ, Juffer F, Ijzendoorn MH, Mangelsdorf SC, Zevalkink J. Preventing preschool externalizing behavior problems through video‐feedback intervention in infancy. Infant Mental Health Journal 2006;27(5):466‐93. [DOI: 10.1002/imhj.20104; PUBMED: 28640397] [DOI] [PubMed] [Google Scholar]
Koniak‐Griffin 1992 {published data only (unpublished sought but not used)}
- Koniak‐Griffin D, Verzemnieks I, Cahill D. Using videotape instruction and feedback to improve adolescents' mothering behaviors. Journal of Adolescent Health 1992;13(7):570‐5. [PUBMED: 1345129] [DOI] [PubMed] [Google Scholar]
Lam‐Cassettari 2015 {published and unpublished data}
- Lam‐Cassettari C. Cochrane review data request [personal communication]. Email to: E Smith 23 January 2018.
- Lam‐Cassettari C, Wadnerkar‐Kamble MB, James DM. Enhancing parent‐child communication and parental self‐esteem with a video‐feedback intervention: outcomes with prelingual deaf and hard‐of‐hearing children. Journal of Deaf Studies and Deaf Education 2015;20(3):266‐74. [DOI: 10.1093/deafed/env008; PMC4450156; PUBMED: 25819293] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moran 2005 {published data only (unpublished sought but not used)}
- Moran G. Re: Systematic review study data [personal communication]. Email to: L O'Hara 11 March 2017.
- Moran G, Pederson DR, Krupka A. Maternal unresolved attachment status impedes the effectiveness of interventions with adolescent mothers. Infant Mental Health Journal 2005;26(3):231‐49. [DOI: 10.1002/imhj.20045; PUBMED: 28682506] [DOI] [PubMed] [Google Scholar]
Moss 2011 {published data only (unpublished sought but not used)}
- Dubois‐Comtois K. Cochrane review: data request [personal communication]. Email to: E Smith 9 February 2018.
- Moss E, Dubois‐Comtois K, Cyr C, Tarabulsy GM, St‐Laurent D, Bernier A. Efficacy of a home‐visiting intervention aimed at improving maternal sensitivity, child attachment, and behavioral outcomes for maltreated children: a randomized control trial. Development and Psychopathology 2011;23(1):195‐210. [DOI: 10.1017/S0954579410000738; PUBMED: 21262048] [DOI] [PubMed] [Google Scholar]
Negrão 2014 {published and unpublished data}
- Negrão M, Pereira M, Soares I, Mesman J. Enhancing positive parent‐child interactions and family functioning in a poverty sample: a randomized control trial. Attachment & Human Development 2014;16(4):315‐28. [DOI: 10.1080/14616734.2014.912485; PUBMED: 24972101] [DOI] [PubMed] [Google Scholar]
- Pereira M. Systematic review ‐ data request [personal communication]. Email to: E Smith 28 February 2018.
- Pereira M, Negrão M, Soares I, Mesman J. Decreasing harsh discipline in mothers at risk for maltreatment: a randomized control trial. Infant Mental health Journal 2014;35(6):604‐13. [DOI: 10.1002/imhj.21464; PUBMED: 25798509] [DOI] [PubMed] [Google Scholar]
Platje 2018 {published data only}
- Overbeek MM, Sterkenburg PS, Kef S, Schuengel C. The effectiveness of VIPP‐V parenting training for parents of young children with a visual or visual‐and‐intellectual disability: study protocol of a multicenter randomized controlled trial. Trials 2015;16:401. [DOI: 10.1186/s13063-015-0916-6; PMC4565007 ; PUBMED: 26353825] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Platje E, Sterkenburg P, Overbeek M, Kef S, Schuengel C. The efficacy of VIPP‐V parenting training for parents of young children with a visual or visual‐and‐intellectual disability: a randomized controlled trial. Attachment & Human Development 2018;20(5):455‐72. [DOI: 10.1080/14616734.2018.1428997; 29359632] [DOI] [PubMed] [Google Scholar]
- Sterkenburg PS, Platje E, Overbeek MM, Kef S, Schuengel C. Studying the effect of Video‐feedback Intervention to promote Positive Parenting for parents of children with a visual or visual and intellectual disability (VIPP‐V): a randomized controlled trial. Journal of Mental Health Research in Intellectual Disabilities 2017;10(Suppl 1):206. [DOI: 10.1080/19315864.2017.1368259] [DOI] [Google Scholar]
Poslawsky 2015 {published data only (unpublished sought but not used)}
- Poslawsky IE, Naber FB, Bakermans‐Kranenburg MJ, Daalen E, Engeland H, Ijzendoorn MH. Video‐feedback Intervention to promote Positive Parenting adapted to Autism (VIPP‐AUTI): a randomized controlled trial. Autism 2015;19(5):588‐603. [DOI: 10.1177/1362361314537124; PUBMED: 24919961] [DOI] [PubMed] [Google Scholar]
- Poswlawsky I. Systematic review data request [personal communication]. Email to: E Smith 17 January 2018.
Seifer 1991 {published data only}
- Seifer R, Clark GN, Sameroff AJ. Positive effects of interaction coaching on infants with developmental disabilities and their mothers. American Journal of Mental Retardation 1991;96(1):1‐11. [PUBMED: 1878184] [PubMed] [Google Scholar]
Stein 2006 {published and unpublished data}
- Stein A. Data for our 2006 paper [personal communication]. Email to: J Barlow 11 June 2018.
- Stein A, Woolley H, Senior R, Hertzmann L, Lovel M, Lee J, et al. Treating disturbances in the relationship between mothers with bulimic eating disorders and their infants: a randomized, controlled trial of video feedback. American Journal of Psychiatry 2006;163(5):899‐906. [DOI: 10.1176/ajp.2006.163.5.899; PUBMED: 16648333] [DOI] [PubMed] [Google Scholar]
- Woolley H, Hertzmann L, Stein A. Video‐feedback intervention with mothers with postnatal eating disorders and their infants. In: Juffer F, Bakermans‐Kranenbrg MJ, IJzendoorn MH editor(s). Promoting Positive Parenting: An Attachment‐Based Intervention. New York (NY): Lawrence Erlbaum Associates/Taylor & Francis Group, 2008:111‐38. [Google Scholar]
Van Zeijl 2006 {published data only}
- Bakermans‐Kranenburg MJ, IJzendoorn MH, Pijlman FT, Mesman J, Juffer F. Experimental evidence for differential susceptibility: dopamine D4 receptor polymorphism (DRD4 VNTR) moderates intervention effects on toddlers' externalizing behavior in a randomized controlled trial. Developmental Psychology 2008;44(1):293‐300. [DOI: 10.1037/0012-1649.44.1.293; PUBMED: 18194028] [DOI] [PubMed] [Google Scholar]
- Bakermans‐Kranenburg MJ, Ijzendoorn MH, Mesman J, Alink LR, Juffer F. Effects of an attachment‐based intervention on daily cortisol moderated by dopamine receptor D4: a randomized control trial on 1‐ to 3‐year‐olds screened for externalizing behavior. Development and Psychopathology 2008;20(3):805‐20. [DOI: 10.1017/S0954579408000382; PUBMED: 18606032] [DOI] [PubMed] [Google Scholar]
- Mesman J, Stolk MN, Zeijl J, Alink LR, Juffer F, Bakermans‐Kranenburg MJ, et al. Extending the video‐feedback intervention to sensitive discipline: the early prevention of antisocial behavior. In: Juffer F, Bakermans‐Kranenbrg MJ, IJzendoorn MH editor(s). Promoting Positive Parenting: An Attachment‐Based Intervention. New York (NY): Lawrence Erlbaum Associates/Taylor & Francis Group, 2008:171‐92. [Google Scholar]
- Stolk MN, Mesman J, Zeijl J, Alink LR, Bakermans‐Kranenburg MJ, IJzendoorn MH, et al. Early parenting intervention: family risk and first‐time parenting related to intervention effectiveness. Journal of Child and Family Studies 2008;17:55. [DOI: 10.1007/s10826-007-9136-3] [DOI] [Google Scholar]
- Van Zeijl. Externalizing Problems in 1‐ to 3‐Year‐Old Children: Screening, Intervention, and the Role of Child Temperament [PhD thesis]. Leiden (NL): Leiden University, 2006. [Google Scholar]
- Zeijl J, Mesman J, IJzendoorn MH, Bakermans‐Kranenburg MJ, Juffer F, Stolk MN, et al. Attachment‐based intervention for enhancing sensitive discipline in mothers of 1‐ to 3‐year‐old children at risk for externalizing behavior problems: a randomized controlled trial. Journal of Consulting and Clinical Psychology 2006;74(6):994‐1005. [DOI: 10.1037/0022-006X.74.6.994; PUBMED: 17154730] [DOI] [PubMed] [Google Scholar]
Yagmur 2014 {published data only}
- Yagmur S, Mesman J, Malda M, Bakermans‐Kranenburg MJ, Ekmekci H. Video‐feedback intervention increases sensitive parenting in ethnic minority mothers: a randomized control trial. Attachment & Human Development 2014;16(4):371‐86. [DOI: 10.1080/14616734.2014.912489; PUBMED: 24972105] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Akai 2008 {published data only}
- Akai CE, Guttentag CL, Baggett KM, Willard Noria CC, Centers for the Prevention of Child Neglect. Enhancing parenting practices of at‐risk mothers. Journal of Primary Prevention 2008;29(3):223‐42. [DOI: 10.1007/s10935-008-0134; PMC6060617 ; PUBMED: 18543105] [DOI] [PMC free article] [PubMed] [Google Scholar]
Aldred 2001 {published data only}
- Aldred C, Pollard C, Phillips R, Adams C. Multidisciplinary social communication intervention for children with autism and persuasive developmental disorder: the Child's Talk project. Educational and Child Psychology 2001;18(2):76‐87. [Google Scholar]
Aldred 2004 {published data only}
- Aldred C, Green J, Adams C. A new social communication intervention for children with autism: pilot randomised controlled treatment study suggesting effectiveness. Journal of Child Psychology and Psychiatry 2004;45(8):1420‐30. [DOI: 10.1111/j.1469-7610.2004.00848.x; PUBMED: 15482502] [DOI] [PubMed] [Google Scholar]
Bernard 2012 {published data only}
- Bernard K, Dozier M, Bick J, Lewis‐Morrarty E, Lindhiem O, Carlson E. Enhancing attachment organization among maltreated children: results of a randomized clinical trial. Child Development 2012;83(2):623‐36. [DOI: 10.1111/j.1467-8624.2011.01712.x; PMC3305815 ; PUBMED: 22239483] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bilszta 2012 {published data only}
- Bilszta JL, Buist AE, Wang F, Zulkefli NR. Use of video feedback intervention in an inpatient perinatal psychiatric setting to improve maternal parenting. Archives of Women's Mental Health 2012;15(4):249‐57. [DOI: 10.1007/s00737-012-0283-1; PUBMED: 22588508] [DOI] [PubMed] [Google Scholar]
- Buist AE, Bilszta JLC, Zulkefi NR, Wang F. The use of video feedback in women with postnatal depression. Archive of Women’s Mental Health 2011;14(1 Suppl):S11‐2. [DOI: 10.1007/s00737-010-0203-1] [DOI] [Google Scholar]
Borghini 2014 {published data only}
- Borghini A, Habersaat S, Forcada‐Guex M, Nessi J, Pierrehumbert B, Ansermet F, et al. Effects of an early intervention on maternal post‐traumatic stress symptoms and the quality of mother‐infant interaction: the case of pre‐term birth. Infant Behavior & Development 2014;37(4):624‐31. [DOI: 10.1016/j.infbeh.2014.08.003; PUBMED: 25222614] [DOI] [PubMed] [Google Scholar]
Brisch 2003 {published data only}
- Brisch KH, Bechinger D, Betzler S, Heinemann H. Early preventive attachment‐oriented psychotherapeutic intervention program with parents of a very low birthweight premature infant: results of attachment and neurological development. Attachment & Human Development 2003;5(2):120‐35. [DOI: 10.1080/1461673031000108504; PUBMED: 12791563] [DOI] [PubMed] [Google Scholar]
Bunder 2011 {published data only}
- Bünder P. Enhancing development of children at risk and their parents by video counselling according to the Marte Meo method [Entwicklungsförderung von risikokindern und ihren eltern mit hilfe von videoberatung nach der Marte‐Meo‐Methode]. Praxis der Kinderpsychologie und Kinderpsychiatrie 2011;60(5):333‐50. [DOI: 10.13109/prkk.2011.60.5.333; PUBMED: 21751531] [DOI] [PubMed] [Google Scholar]
Cassiba 2015 {published data only}
- Cassibba R, Castoro G, Costantino E, Sette G, IJzendoorn MH. Enhancing maternal sensitivity and infant attachment security with video feedback: an exploratory study in Italy. Infant Mental Health Journal 2015;36(1):53‐61. [DOI: 10.1002/imhj.21486; PUBMED: 25445216] [DOI] [PubMed] [Google Scholar]
Cates 2012 {published data only}
- Berkule SB, Cates CB, Dreyer BP, Huberman HS, Arevalo J, Burtchen N, et al. Reducing maternal depressive symptoms through promotion of parenting in pediatric primary care. Clinical Pediatrics 2014;53(5):460‐9. [DOI: 10.1177/0009922814528033; PMC4435690 ; PUBMED: 24707022] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Canfield CF, Weisleder A, Cates C, Huberman HS, Dreyer BP, Legano LA, et al. Primary care parenting intervention and its effects on use of physical punishment among low‐income parents of toddlers. Journal of Developmental and Behavioral Pediatrics 2015;36(8):586‐93. [DOI: 10.1097/DBP.0000000000000206; PMC4586371 ; PUBMED: 26375804] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cates CB, Dreyer BP, Berkule SB, White LJ, Arevalo JA, Mendelsohn AL. Infant communication and subsequent language development in children from low‐income families: the role of early cognitive stimulation. Journal of Developmental and Behvioral Pediatrics 2012;33(7):577‐85. [DOI: 10.1097/DBP.0b013e318264c10f; PMC3434454 ; PUBMED: 22947884] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cates CB, Weisleder A, Berkule Johnson S, Seery AM, Canfield CF, Huberman H, et al. Enhancing parent talk, reading, and play in primary care: sustained impacts of the Video Interaction Project. Journal of Pediatrics 2018;199:45‐56.e1. [DOI: 10.1016/j.jpeds.2018.03.002; PMC6063788 ; PUBMED: 29703577] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cates CB, Weisleder A, Dreyer BP, Johnson SB, Vlahovicova K, Ledesma J, et al. Leveraging healthcare to promote responsive parenting: impacts of the Video Interaction Project on parenting stress. Journal of Child and Family Studies 2016;25(3):827‐35. [DOI: 10.1007/s10826-015-0267-7; PMC4847426; PUBMED: 27134514] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendelsohn AL, Dreyer BP, Brockmeyer CA, Berkule‐Silberman SB, Huberman HS, Tomopoulos S. Randomized controlled trial of primary care pediatric parenting programs: effect on reduced media exposure in infants, mediated through enhanced parent‐child interaction. Archives of Pediatrics & Adolescent Medicine 2011;165(1):42‐8. [DOI: 10.1001/archpediatrics.2010.266; PMC3083922 ; PUBMED: 21199979] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendelsohn AL, Huberman HS, Berkule SB, Brockmeyer CA, Morrow LM, Dreyer BP. Primary care strategies for promoting parent‐child interactions and school readiness in at‐risk families: the Bellevue project for early language, literacy, and education success. Archives of Pediatrics & Adolescent Medicine 2011;165(1):33‐41. [DOI: 10.1001/archpediatrics.2010.254; PMC3095489 ; PUBMED: 21199978] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weisleder A, Cates CB, Dreyer BP, Johnson SB, Huberman HS, Seery AM, et al. Promotion of positive parenting and prevention of socioemotional disparities. Pediatrics 2016;137(2):e20153239. [DOI: 10.1542/peds.2015-3239] [DOI] [PMC free article] [PubMed] [Google Scholar]
Dozier 2006 {published data only}
- Dozier M, Peloso E, Lindhiem O, Gordon KM, Manni M, Sepulveda S, et al. Developing evidence‐based interventions for foster children: an example of a randomized clinical trial with infants and toddlers. Journal of Social Issues 2006;62(4):767‐85. [DOI: 10.1111/j.1540-4560.2006.00486.x] [DOI] [Google Scholar]
Durett 1984 {published data only}
- Durrett ME, Otaki M, Richards P. Attachment and the mother's perception of support from the father. International Journal of Behavioral Development 1984;7(2):167‐76. [DOI: 10.1177/016502548400700205] [DOI] [Google Scholar]
Feeley 2012 {published data only}
- Feeley N, Zelkowitz P, Shrier I, Stremler R, Westreich R, Dunkley D, et al. Follow‐up of the Cues and Care Trial: mother and infant outcomes at 6 months. Journal of Early Intervention 2012;34(2):65‐81. [DOI: 10.1177/1053815112453767] [DOI] [Google Scholar]
Glanemann 2013 {published data only}
- Glanemann R, Reichmuth K, Matulat P, Zehnhoff‐Dinnesen AA. Muenster Parental Programme empowers parents in communication with their infant with hearing loss. International Journal of Pediatric Otorhinolaryngology 2013;77(12):2023‐9. [DOI: 10.1016/j.ijporl.2013.10.001; PUBMED: 24210293] [DOI] [PubMed] [Google Scholar]
- am Zehnhoff‐Dinnesen A, Glanemann R, Embacher A, Matulat P, Reichmuth K. Muenster parental training for improving parents' communication behaviour towards their hearing‐impaired toddlers and infants. Journal of Hearing Sciences 2011;1(1):93. [FP‐097; journalofhearingscience.com/media/attachments/2017/08/01/896141.pdf] [Google Scholar]
Groeneveld 2011 {published data only}
- Groeneveld MG, Vermeer HJ, IJzendoorn MH, Linting M. Enhancing home‐based child care quality through video‐feedback intervention: a randomized trial. Journal of Family Psychology 2011;25(1):86‐96. [DOI: 10.1037/a0022451; PUBMED: 21355649] [DOI] [PubMed] [Google Scholar]
Groeneveld 2016 {published data only}
- Groeneveld MG, Vermeer HJ, IJzendoorn MH, Linting M. Randomized video‐feedback intervention in home‐based childcare: improvement of children's wellbeing dependent on time spent with trusted caregiver. Child Youth Care Forum 2016;45:587‐606. [DOI: 10.1007/s10566-015-9344-8; PMC4923105; PUBMED: 27429535] [DOI] [PMC free article] [PubMed] [Google Scholar]
Guttentag 2014 {published data only}
- Guttentag CL, Landry SH, Williams JM, Baggett KM, Noria CW, Borkowski JG, et al. "My Baby & Me": effects of an early, comprehensive parenting intervention on at‐risk mothers and their children. Developmental Psychology 2014;50(5):1482‐96. [DOI: 10.1037/a0035682; PMC5609813 ; PUBMED: 24447116] [DOI] [PMC free article] [PubMed] [Google Scholar]
Huber 2016 {published data only}
- Huber A, McMahon C, Sweller N. Improved parental emotional functioning after Circle of Security 20‐week parent–child relationship intervention. Journal of Child and Family Studies 2016;25(8):2526‐40. [DOI: 10.1007/s10826-016-0426-5] [DOI] [Google Scholar]
Juffer 1997 {published data only}
- Juffer F, Hoksbergen RA, Riksen‐Walraven JM, Kohnstamm GA. Early intervention in adoptive families: supporting maternal sensitive responsiveness, infant‐mother attachment, and infant competence. Journal of Child Psychology and Psychiatry 1997;38(8):1039‐50. [PUBMED: 9413801] [DOI] [PubMed] [Google Scholar]
Juffer 2005 {published data only}
- Juffer F, Bakermans‐Kranenburg MJ, IJzendoorn MH. The importance of parenting in the development of disorganized attachment: evidence from a preventive intervention study in adoptive families. Journal of Child Psychology and Psychiatry 2005;46(3):263‐74. [DOI: 10.1111/j.1469-7610.2004.00353.x; PUBMED: 15755303] [DOI] [PubMed] [Google Scholar]
Kim 2005 {published data only}
- Kim JM, Mahoney G. The effects of relationship focused intervention on Korean parents and their young children with disabilities. Research in Developmental Disabilities 2005;26(2):117‐30. [DOI: 10.1016/j.ridd.2004.08.001; PUBMED: 15590243] [DOI] [PubMed] [Google Scholar]
Krupka 1995 {published data only}
- Krupka A. The Quality of Mother‐infant Interactions In Families at Risk for Maladaptive Parenting [PhD thesis]. Ontario (TO): University of Western Ontario, 1995. [Google Scholar]
Lambermon 1989 {published data only}
- Lambermon MW, IJzendoorn MH. Influencing mother‐infant interaction through video‐taped or written instruction: evaluation of a parent education program. Early Childhood Research Quarterly 1989;4(4):449‐58. [DOI: 10.1016/0885-2006(89)90003-3] [DOI] [Google Scholar]
Landry 2006 {published data only}
- Landry SH, Smith KE, Swank PR. Responsive parenting: establishing early foundations for social, communication, and independent problem‐solving skills. Developmental Psychology 2006;42(4):627‐42. [DOI: 10.1037/0012-1649.42.4.627; PUBMED: 16802896] [DOI] [PubMed] [Google Scholar]
Lindheim 2009 {published data only}
- Lindheim OJ. Modeling Change: An Attachment‐Based Intervention with High‐Risk Birth Mothers [PhD Thesis]. Newark (DE): University of Delaware, 2009. [Google Scholar]
Magill‐Evans 2007 {published data only}
- Magill‐Evans J, Harrison MJ, Benzies K, Gierl M, Kimak C. Effects of parenting education on first‐time fathers' skills in interactions with their infants. Fathering 2007;5(1):42‐57. [DOI: 10.3149/fth.0501.42] [DOI] [Google Scholar]
Mendelsohn 2005 {published data only}
- Mendelsohn AL, Dreyer BP, Flynn V, Tomopoulos S, Rovira I, Tineo W, et al. Use of videotaped interactions during pediatric well‐child care to promote child development: a randomized, controlled trial. Journal of Developmental and Behavioral Pediatrics 2005;26(1):34‐41. [PMC4435697; PUBMED: 15718881] [PMC free article] [PubMed] [Google Scholar]
- Mendelsohn AL, Valdez PT, Flynn V, Foley GM, Berkule SB, Tomopoulos S, et al. Use of videotaped interactions during pediatric well‐child care: impact at 33 months on parenting and on child development. Journal of Developmental and Behavioral Pediatrics 2007;28(3):206‐12. [DOI: 10.1097/DBP.0b013e3180324d87; 17565287; PUBMED: PMC3083927] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT03397719 {published data only}
- NCT03397719. Parent video feedback intervention study [Parent feedback intervention study: a randomized controlled trial]. clinicaltrials.gov/show/nct03397719 2018 (first received 13 December 2017).
Sheese 2007 {published data only}
- Sheese BE, Voelker PM, Rothbart MK, Posner MI. Parenting quality interacts with genetic variation in dopamine receptor D4 to influence temperament in early childhood. Development and Psychopathology 2007;19(4):1039‐46. [DOI: 10.1017/S0954579407000521; PUBMED: 17931433] [DOI] [PubMed] [Google Scholar]
Smith 2013 {published data only}
- Smith JD, Dishon TJ, Moore KJ, Shaw DS, Wilson MN. Effects of video feedback on early coercive parent‐child interactions: the intervening role of caregivers' relational schemas. Journal of Clinical Child and Adolescent Psychology 2013;42(3):405‐17. [DOI: 10.1080/15374416.2013.777917; PMC3651905; PUBMED: 23534831] [DOI] [PMC free article] [PubMed] [Google Scholar]
Solomon 2014 {published data only}
- Solomon R, Egeren LA, Mahoney G, Quon Huber MS, Zimmerman P. PLAY Project Home Consultation intervention program for young children with autism spectrum disorders: a randomized controlled trial. Journal of Developmental and Behavioral Paediatrics 2014;35(8):475‐85. [DOI: 10.1097/DBP.0000000000000096; PMC4181375 ; PUBMED: 25264862] [DOI] [PMC free article] [PubMed] [Google Scholar]
Spieker 2012 {published data only}
- Spieker SJ, Oxford ML, Kelly JF, Nelson EM, Fleming CB. Promoting first relationships: randomized trial of a relationship‐based intervention for toddlers in child welfare. Child Maltreatment 2012;17(4):271‐86. [DOI: 10.1177/1077559512458176; PMC3552521 ; PUBMED: 22949743] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sprang 2009 {published data only}
- Sprang G. The efficacy of a relational treatment for maltreated children and their families. Child and Adolescent Mental Health 2009;14(2):81‐8. [DOI: 10.1111/j.1475-3588.2008.00499.x] [DOI] [Google Scholar]
Svanberg 2010 {published data only}
- Svanberg PO, Mennet L, Spieker S. Promoting a secure attachment: a primary prevention practice model. Clinical Child Psychology and Psychiatry 2010;15(3):363‐78. [DOI: 10.1177/1359104510367584; PUBMED: 20603424] [DOI] [PubMed] [Google Scholar]
Van Balkom 2010 {published data only}
- Balkom H, Verhoeven L, Weerdenburg M, Stoep J. Effects of parent‐based Video Home Training in children with developmental language delay. Child Language Teaching and Therapy 2010;26(3):221‐37. [DOI: 10.1177/0265659009349978] [DOI] [Google Scholar]
Van Doesum 2008 {published data only}
- Doesum KT, Riksen‐Walraven JM, Hosman CM, Hoefnagels C. A randomized controlled trial of a home‐visiting intervention aimed at preventing relationship problems in depressed mothers and their infants. Child Development 2008;79(3):547‐61. [DOI: 10.1111/j.1467-8624.2008.01142.x; PUBMED: 18489412] [DOI] [PubMed] [Google Scholar]
Weiner 1994 {published data only}
- Weiner A, Kuppermintz H, Guttmann D. Video home training (the Orion project): a short‐term preventive and treatment intervention for families with young children. Family Process 1994;33(4):441‐53. [DOI: 10.1111/j.1545-5300.1994.00441.x; PUBMED: 7698307] [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Mendelsohn 2008 {published data only}
- Mendelsohn A. An RCT of the Video Interaction Project (VIP) and Building Blocks (BB): primary care based parenting interventions. Pediatric Academic Societies Annual Meeting; 2008, May 3‐6; Honolulu (HI). 2008.
References to ongoing studies
Euser 2016 {published data only}
- Euser S, Bakermans‐Kranenburg MJ, Bulk BG, Linting M, Damsteegt RC, Vrijhof CI, et al. Efficacy of the Video‐feedback Intervention to promote Positive Parenting and Sensitive Discipline in Twin Families (VIPP‐Twins): study protocol for a randomized controlled trial. BMC Psychology 2016;4(1):33. [DOI: 10.1186/s40359-016-0139; PMC4895801 ; PUBMED: 27268415] [DOI] [PMC free article] [PubMed] [Google Scholar]
Firk 2015 {published data only}
- Firk C, Dahmen B, Lehmann C, Niessen A, Koslowski J, Rauch G, et al. A mother‐child intervention program in adolescent mothers and their children to improve maternal sensitivity, child responsiveness and child development (the TeeMo study): study protocol for a randomized controlled trial. Trials 2015;16:230. [DOI: 10.1186/s13063-015-0747-5; PMC4446828 ; PUBMED: 26012585] [DOI] [PMC free article] [PubMed] [Google Scholar]
ISRCTN92360616 {published data only}
- 10.1186/ISRCTN92360616. Preterm Infant‐Parent Programme for Attachment (PIPPA Study). Preterm Infant Parent Programme for Attachment (PIPPA study): a randomised controlled trial of the preterm infant‐parent relationship‐focused intervention programme to support attachment and social‐emotional development of preterm infants (first received 1 May 2012). [DOI: 10.1186/ISRCTN92360616] [DOI]
NCT03052374 {published data only}
- NCT03052374. Video‐feedback interaction guidance for improving interactions between depressed mothers and their infants ("VID‐KIDS") (VID‐KIDS). clinicaltrials.gov/ct2/show/nct03052374 (first received 2 February 2017).
Schoemaker 2018 {published data only}
- Schoemaker NK, Jagersma G, Stoltenborgh M, Maras A, Vermeer HJ, Juffer F, et al. The effectiveness of Video‐feedback Intervention to promote Positive Parenting for Foster Care (VIPP‐FC): study protocol for a randomized controlled trial. BMC Psychology 2018;6(1):38. [DOI: 10.1186/s40359-018-0246; PMC6091108 ; PUBMED: 30075813] [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Aber 1985
- Aber JL, Slade A, Berger B, Bresgi I, Kaplan M. The parent development interview. Unpublished manuscript 1985.
Abidin 1983
- Abidin RR. Parenting Stress Index: Manual, Administration Booklet, (and) Research Update. Charlottesville (VA): Pediatric Psychology Press, 1983. [Google Scholar]
Abidin 1995
- Abidin RR. Parenting Stress Index: Professional Manual. 3rd Edition. Odessa (FL): Psychological Assessments, 1995. [Google Scholar]
Achenbach 1992
- Achenbach TM. Manual for the Child Behavior Checklist/2‐3 and 1992 profile. Burlington: University of Vermont, Department of Psychiatry 1992.
Achenbach 2000
- Achenbach TM, Rescorla LA. Manual for the ASEBA Preschool Forms and Profiles. Burlington (VT): University of Vermont, 2000. [Google Scholar]
Ainsworth 1974
- Ainsworth MD, Bell SM, Stayton DF. Infant‐mother attachment and social development: socialization as a product of reciprocal responsiveness to signals. In: Richards MPM editor(s). The Integration of a Child into a Social World. London (UK): Cambridge University Press, 1974:99‐135. [Google Scholar]
Ainsworth 1978
- Ainsworth MD, Blehar MC, Waters E, Wall S. Patterns of Attachment: A Psychological Study of the Strange Situation. Hillsdale (NJ): Lawrence Erlbaum Associates, Inc, 1978. [Google Scholar]
Alink 2009
- Alink LR, Mesman J, Zeijl J, Stolk MN, Juffer F, Bakermans‐Kranenburg MJ, et al. Maternal sensitivity moderates the relation between negative discipline and aggression in early childhood. Social Development 2009;18(1):99‐120. [DOI: 10.1111/j.1467-9507.2008.00478.x] [DOI] [Google Scholar]
Bakermans‐Kranenburg 2003
- Bakermans‐Kranenburg MJ, Ijzendoorn MH, Juffer F. Less is more: meta‐analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin 2003;129(2):195‐215. [DOI: 10.1037/0033-2909.129.2.195; PUBMED: 12696839] [DOI] [PubMed] [Google Scholar]
Bakermans‐Kranenburg 2018 [pers comm]
- Bakermans‐Kranenburg M. Systematic review ‐ VIG [personal communication]. Email to: E Smith 24 March 2018.
Balldin 2018
- Balldin S, Fisher PA, Wirtberg I. Video feedback intervention with children: a systematic review. Research on Social Work Practice 2018;28(6):682‐95. [DOI: 10.1177/1049731516671809] [DOI] [Google Scholar]
Barlow 2018 [pers comm]
- Barlow J. Quick query [personal communication]. Email to: A Stein 22 May 2018.
Barnard 1978
- Barnard KE. Nursing Child Assessment Teaching Scale Manual. Seattle, University of Washington, NCAST Office 1978.
Barone 2019 [pers comm]
- Barone L. Re: Cochrane systematic review: data request [personal communication]. Email to: E Smith 10 July 2019.
Bayley 1969
- Bayley N. Bayley Scales of Infant Development. New York (NY): Psychological Corporation, 1969. [Google Scholar]
Bayley 2006
- Bayley N. Bayley Scales of Infant and Toddler Development (Bayley‐III). 3rd Edition. San Antonio (TX): Pearson, 2006. [Google Scholar]
Beebe 2010
- Beebe B, Jaffe J, Markese S, Buck K, Chen H, Cohen P, et al. The origins of 12‐month attachment: a micro‐analysis of 4‐month mother‐infant interaction. Attachment & Human Development 2010;12(1‐2):3‐141. [DOI: 10.1080/14616730903338985; PMC3763737; PUBMED: 20390524] [DOI] [PMC free article] [PubMed] [Google Scholar]
Belsky 2002
- Belsky J, Fearon RM. Infant‐mother attachment security, contextual risk, and early development: a moderational analysis. Development and Psychopathology 2002;14(2):293‐310. [PUBMED: 12030693] [DOI] [PubMed] [Google Scholar]
Berry 1995
- Berry JO, Jones WH. The Parental Stress Scale: initial psychometric evidence. Journal of Social and Personal Relationships 1995;12(3):463‐72. [DOI: 10.1177/0265407595123009] [DOI] [Google Scholar]
Biringen 2000a
- Biringen Z. Emotional availability: conceptualization and research findings. The American Journal of Orthopsychiatry 2000;70(1):104‐14. [DOI: 10.1037/h0087711; PUBMED: 10702855] [DOI] [PubMed] [Google Scholar]
Biringen 2000b
- Biringen Z, Robinson JL, Emde RN. Appendix B: the Emotional Availability Scales (3rd ed.; an abridged Infancy/Early Childhood Version). Attachment & Human Development 2000;2(2):256‐70. [DOI: 10.1080/14616730050085626] [DOI] [PubMed] [Google Scholar]
Biringen 2008
- Biringen Z. The Emotional Availability (EA) scales and the Emotional Attachment & Emotional Availability (EA2) Clinical Screener (4th edition): Infancy/Early Childhood version. www.emotionalavailability.com (accessed 20 July 2019).
Bovenschen 2019 [pers comm]
- Bovenschen I. Systematic review ‐ study data [personal communication]. Email to: E Smith 26 March 2019.
Bowlby 1969
- Bowlby J. Attachment and Loss, Volume 1: Attachment. New York (NY): Basic Books, 1969. [Google Scholar]
Cassibba 2015
- Cassibba R, Castoro G, Costantino E, Sette G, Ijzendoorn MH. Enhancing maternal sensitivity and infant attachment security with video feedback: an exploratory study in Italy. Infant Mental Health Journal 2015;36(1):53‐61. [DOI: 10.1002/imhj.21486; PUBMED: 25445216] [DOI] [PubMed] [Google Scholar]
Cates 2016 [pers comm]
- Cates C (UK Cochrane Centre, Oxford), O'Mathuna D (Cochrane Ireland, Dublin). [personal communication]. Unpublished handout: RA3 & RA4 workshops delivered to Cochrane HRB/R&D Fellows 27‐28 April 2016; Vol. Located at Dublin.
Ciciolla 2013
- Ciciolla L, Crnic KA, West SG. Determinants of change in maternal sensitivity: contributions of context, temperament, and developmental risk. Parenting: Science and Practice 2013;13(3):178‐95. [DOI: 10.1080/15295192.2013.756354; PMC3772787 ; PUBMED: 24044007] [DOI] [PMC free article] [PubMed] [Google Scholar]
Crittenden 2001
- Crittenden PM. CARE‐INDEX Infants and Toddlers Coding Manual. Unpublished scales. Miami (FL): Family Relations Institute, 2001. [Google Scholar]
Crnic and Greenberg 1990
- Crnic KA, Greenberg MT. Minor parenting stresses with young children. Child Development 1990;61:1628‐37. [DOI] [PubMed] [Google Scholar]
Cyr 2010
- Cyr C, Euser EM, Bakermans‐Kranenburg MJ, Ijzendoorn MH. Attachment security and disorganization in maltreating and high‐risk families: a series of meta‐analyses. Development and Psychopathology 2010;22(1):87‐108. [DOI: 10.1017/S0954579409990289; PUBMED: 20102649] [DOI] [PubMed] [Google Scholar]
De Brock 1992
- Brock AJ, Vermulst AA, Gerris, JR, Abidin RR. Nijmeegse Ouderlijke Stress Index [Nijmege Parental Stress Index]. Lisse (NL): Swets and Zeitlinger, 1992. [Google Scholar]
De Wolff 1997
- Wolff MS, Ijzendoorn MH. Sensitivity and attachment: a meta‐analysis on parental antecedents of infant attachment. Child Development 1997;68(4):571‐91. [PUBMED: 9306636] [PubMed] [Google Scholar]
Deeks 2017
- Deeks JJ, Higgins JP, Altman DG (editors), on behalf of the Cochrane Statistical Methods Group. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Donner 1980
- Donner A, Koval JJ. The estimation of intraclass correlation in the analysis of family data. Biometrics 1980;36(1):19‐25. [DOI: 10.2307/2530491; PUBMED: 7370372] [DOI] [PubMed] [Google Scholar]
Dubois‐Comtois 2018 [pers comm]
- Dubois‐Comtois K. Cochrane review: data request [personal communication]. Email to: E Smith 9 February 2018.
Egeland 1990
- Egeland B, Erickson MF, Clemenhagen‐Moon JC, Hiester MK, Korfmacher J. 24 months tools coding manual. Project STEEP revised 1990 from mother–child project scales. Unpublished manuscript 1990, issue University of Minnesota, Minneapolis.
Egeland and Heister 1993
- Egeland B, Hiester M. Teaching Task Rating Scales. Unpublished scales 1993.
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315(7109):629‐34. [DOI: 10.1136/bmj.315.7109.629; PMC2127453; PUBMED: 9310563] [DOI] [PMC free article] [PubMed] [Google Scholar]
Eiden 2014
- Eiden RD, Godleski S, Colder CR, Schuetze P. Prenatal cocaine exposure: the role of cumulative environmental risk and maternal harshness in the development of child internalizing behavior problems in kindergarten. Neurotoxicology and Teratology 2014;44:1‐10. [DOI: 10.1016/j.ntt.2014.04.002; PMC4099285 ; PUBMED: 24803425] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fearon 2010
- Fearon RP, Bakermans‐Kranenburg MJ, Ijzendoorn MH, Lapsley AM, Roisman GI. The significance of insecure attachment and disorganization in the development of children's externalizing behavior: a meta‐analytic study. Child Development 2010;81(2):435‐56. [DOI: 10.1111/j.1467-8624.2009.01405.x; PUBMED: 20438450] [DOI] [PubMed] [Google Scholar]
Feldman 1998
- Feldman R. Coding Interactive Behaviour Manual. Ramat Gan (IL): Bar‐Ilan University, 1998. [Google Scholar]
Fukkink 2008
- Fukkink RG. Video feedback in widescreen: a meta‐analysis of family programs. Clinical Psychology Review 2008;28(6):904‐16. [DOI: 10.1016/j.cpr.2008.01.003; PUBMED: 18359136] [DOI] [PubMed] [Google Scholar]
Gilliom 2002
- Gilliom M, Shaw DS, Beck JE, Schonberg MA, Lukon JL. Anger regulation in disadvantaged preschool boys: strategies, antecedents, and the development of self‐control. Developmental Psychology 2002;38(2):222‐35. [DOI: 10.1037/0012-1649.38.2.222; PUBMED: 11881758] [DOI] [PubMed] [Google Scholar]
Goodman 1997
- Goodman R. The Strengths and Difficulties Questionnaire: a research note. Journal of Child Psychology and Psychiatry 1997;38(5):581‐6. [DOI: 10.1111/j.1469-7610.1997.tb01545.x; PUBMED: 9255702] [DOI] [PubMed] [Google Scholar]
Goodman 2011
- Goodman A, Heiervang E, Collishaw S, Goodman R. The ‘DAWBA bands’ as an ordered‐categorical measure of child mental health: description and validation in British and Norwegian samples. Social Psychiatry and Psychiatric Epidemiology 2011;46(6):521‐32. [DOI: 10.1007/s00127-010-0219-x; PUBMED: 20376427] [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 20 July 2019. Hamilton (ON): McMaster University (developed by Evidence Prime).
Hallers‐Haalboom 2014
- Hallers‐Haalboom ET, Mesman J, Groeneveld MG, Endendijk JJ, Berkel SR, Pol LD, et al. Mothers, fathers, sons and daughters: parental sensitivity in families with two children. Journal of Family Psychology 2014;28(2):138‐47. [DOI: 10.1037/a0036004; PUBMED: 24635666] [DOI] [PubMed] [Google Scholar]
Hannesdottir 2007
- Hannesdottir DK, Ollendick TH. The role of emotion regulation in the treatment of child anxiety disorders. Clinical Child and Family Psychology Review 2007;10(3):275‐93. [DOI: 10.1007/s10567-007-0024-6; PUBMED: 17705098] [DOI] [PubMed] [Google Scholar]
Heerman 1994
- Heerman JA, Jones LC, Wikoff RL. Measurement of parent behaviour during interactions with their infants. Infant Behaviour & Development 1994;17(3):311‐21. [DOI: 10.1016/0163-6383(94)90011-6] [DOI] [Google Scholar]
Higgins 2002
- Higgins JP, Thompson SG. Quantifying heterogeneity in meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. [DOI: 10.1002/sim.1186; PUBMED: 12111919] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Deeks JJ, Altman DG, editor(s). Chapter 16: Special topics in statistics. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Higgins 2017
- Higgins JP, Altman DG, Sterne JA (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Hoff 2004
- Hoff B, Munck H, Greisen G. Assessment of parental sensitivity towards pre‐school children born with very low birth weight. Scandinavian Journal of Psychology 2004;45(1):85‐9. [DOI: 10.1111/j.1467-9450.2004.00382.x] [DOI] [PubMed] [Google Scholar]
Hoivik 2018 [pers comm]
- Hoivik M. Cochrane review [personal communication]. Email to: E Smith 15 April 2018.
Jacobvitz 1997
- Jacobvitz D, Hazen NL, Riggs S. Disorganised mental processes in mothers, frightened/frightening behaviour in caregivers and disorientated, disorganised behaviour in infancy. Biennial meeting of the Society for Research in Child Development; 1997 April 3‐6; Washington (DC). Washington (DC), 1997.
Jones 2003
- Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, The Bellagio Child Survival Study Group. How many child deaths can we prevent this year?. Lancet 2003;362(9377):65‐71. [DOI: 10.1016/S0140-6736(03)13811-1; PUBMED: 12853204] [DOI] [PubMed] [Google Scholar]
Juffer 2008
- Juffer F, Bakermans‐Kranenburg MJ, Ijzendoorn MH, editor(s). Promoting Positive Parenting: An Attachment‐Based Intervention. New York (NY): Lawrence Erlbaum Associates/Taylor & Francis Group, 2008. [Google Scholar]
Juffer 2018
- Juffer F, Bakermans‐Kranenburg MJ, Ijzendoorn MH. Video‐feedback intervention to promote positive parenting and sensitive discipline: development and meta‐analytic evidence for Its effectiveness. In: Steele H, Steele M editor(s). Handbook of Attachment‐Based Interventions. New York (NY): The Guilford Press, 2018:1‐28. [Google Scholar]
Kanner 1981
- Kanner AD, Coyne JC, Schaffer C, Lazarus RS. Comparison of two models of stress measurement: daily hassles and uplifts versus major life events. Journal of Behavioral Medicine 1981;4(1):1‐39. [PUBMED: 7288876] [DOI] [PubMed] [Google Scholar]
Karl 1995
- Karl D. Maternal responsiveness of socially high‐risk mothers to the elicitation cues of their 7‐month‐old infants. Journal of Pediatric Nursing 1995;10(4):254‐63. [DOI: 10.1016/S0882-5963(05)80022-3; PUBMED: 7562382] [DOI] [PubMed] [Google Scholar]
Kelly 2005
- Kelly K, Slade A, Grienenberger JF. Maternal reflective functioning, mother‐infant affective communication, and infant attachment: exploring the link between mental states and observed caregiving behavior in the intergenerational transmission of attachment. Attachment & Human Development 2005;7(3):299‐311. [DOI: 10.1080/14616730500245963; PUBMED: 16210241] [DOI] [PubMed] [Google Scholar]
Kennedy 2010
- Kennedy H, Landor M, Todd L. Video Interaction Guidance as a method to promote secure attachment. Educational and Child Psychology 2010;27(3):59‐72. [ISSN (print): 0267‐1611] [Google Scholar]
Kennedy 2011
- Kennedy H, Landor M, Todd L, editor(s). Video Interaction Guidance: A Relationship‐Based Intervention to Promote Attunement, Empathy and Wellbeing. London (UK): Jessica Kingsley Publishers, 2011. [Google Scholar]
Kiang 2004
- Kiang L, Moreno AJ, Robinson JL. Maternal preconceptions about parenting predict child temperament, maternal sensitivity, and children's empathy. Developmental Psychology 2004;40(6):1081‐92. [DOI: 10.1037/0012-1649.40.6.1081; PUBMED: 15535758] [DOI] [PubMed] [Google Scholar]
Kivijärvi 2004
- Kivijärvi M, Räihä H, Virtanen S, Lertola K, Piha J. Maternal sensitivity behavior and infant crying, fussing and contented behaviour: the effects of mother's experienced social support. Scandinavian Journal of Psychology 2004;45(3):239‐46. [DOI: 10.1111/j.1467-9450.2004.00400.x] [DOI] [PubMed] [Google Scholar]
Klein Velderman 2006a
- Klein Velderman M, Bakermans‐Kranenburg MJ, Juffer F, IJzendoorm MH, Manglesdorf SC, Zevalkink J. Preventing preschool externalizing behavior problems through video‐feedback intervention in infancy. Infant Mental Health Journal 2006;27(5):466‐93. [DOI: 10.1002/imhj.20104; PUBMED: 28640397] [DOI] [PubMed] [Google Scholar]
Lam‐Cassettari 2018 [pers comm]
- Lam‐Cassettari C. Cochrane review data request [personal communication]. Email to: E Smith 23 January 2018.
Laulik 2013
- Laulik S, Chou S, Browne KD, Allam J. The link between personality disorder and parenting behaviours: a systematic review. Aggression and Violent Behaviour 2013;18(6):644‐55. [DOI: 10.1016/j.avb.2013.07.017] [DOI] [Google Scholar]
Leerkes 2002
- Leerkes EM, Crockenberg SC. The development of maternal self‐efficacy and its impact on maternal behavior. Infancy 2002;3(2):227‐47. [DOI: 10.1207/S15327078IN0302_7] [DOI] [PubMed] [Google Scholar]
Leerkes 2010
- Leerkes EM. Predictors of maternal sensitivity to infant distress. Parenting: Science and Practice 2010;10(3):219‐39. [DOI: 10.1080/15295190903290840; PMC2930822; PUBMED: 20824194] [DOI] [PMC free article] [PubMed] [Google Scholar]
Levendosky 2006
- Levendosky AA, Leahy KL, Bogat GA, Davidson WS, Eye A. Domestic violence, maternal parenting, maternal mental health, and infant externalizing behavior. Journal of Family Psychology 2006;20(4):544‐52. [DOI: 10.1037/0893-3200.20.4.544; PUBMED: 17176188] [DOI] [PubMed] [Google Scholar]
Liberati 2009
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta‐analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009;339:b2700. [DOI: 10.1136/bmj.b2700; PMC2714672 ; PUBMED: 19622552] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lovas 2005
- Lovas GS. Gender and patterns of emotional availability in mother‐toddler and father‐toddler dyads. Infant Mental Health Journal 2005;26(4):327‐53. [DOI: 10.1002/imhj.20056; PUBMED: 28682464] [DOI] [PubMed] [Google Scholar]
Lundy 2003
- Lundy BL. Father– and mother–infant face‐to‐face interactions: differences in mind‐related comments and infant attachment?. Infant Behavior and Development 2003;26(2):200‐12. [DOI: 10.1016/S0163-6383(03)00017-1] [DOI] [Google Scholar]
Lyons‐Ruth 2005
- Lyons‐Ruth K, Yellin C, Melnick S, Atwood G. Expanding the concept on unresolved mental states: hostile/helpless states of mind on the Adult Attachment Interview are associated with the disrupted mother‐infant communication and infant disorganization. Developmental Psychopathology 2005;17(1):1‐23. [15971757; PUBMED: 15971757] [DOI] [PMC free article] [PubMed] [Google Scholar]
Madigan 2006
- Madigan S, Bakermans‐Kranenburg MJ, Ijzendoorn MH, Moran G, Pederson DR, Benoit D. Unresolved states of mind, anomalous parenting behavior, and disorganized attachment: a review and meta‐analysis of a transmission gap. Attachment & Human Development 2006;8(2):89‐111. [DOI: 10.1080/14616730600774458; PUBMED: 16818417] [DOI] [PubMed] [Google Scholar]
Magnusson 2014
- Magnusson K. Interpreting Cohen's d effect size. R Psychologist, available from rpscyhologist.com/d3/cohend (accessed 1 October 2019).
Main 1990a
- Main M. Cross‐cultural studies of attachment organization: recent studies, changing methodologies, and the concept of conditional strategies. Human Development 1990;33(1):48‐61. [DOI: 10.1159/000276502] [DOI] [Google Scholar]
Main 1990b
- Main M, Hesse E. Parents' unresolved traumatic experiences are related to infant disorganised attachment status: is frightened and/or frightening behaviour the linking mechanism?. In: Greenberg MT, Cicchetti D, Cummings EM editor(s). Attachment in the Preschool Years: Theory, Research and Intervention. Chicago (USA): The University of Chicago Press, 1990:161‐82. [Google Scholar]
Meins 2001
- Meins E, Fernyhough C, Fradley E, Tuckey M. Rethinking maternal sensitivity: mothers' comments on infants' mental processes predict security of attachment at 12 months. Journal of Child Psychology and Psychiatry 2001;42(5):637‐48. [PUBMED: 11464968] [PubMed] [Google Scholar]
Meins 2012
- Meins E, Fernyhough C, Rosnay M, Arnott B, Leekham SR, Turner M. Mind‐mindedness as a multidimensional construct: appropriate and non‐attuned mind‐related comments independently predict infant–mother attachment in a socially diverse sample. Infancy 2012;17(4):393‐415. [DOI: 10.1111/j.1532-7078.2011.00087.x] [DOI] [PubMed] [Google Scholar]
Michalopoulos 2019
- Michalopoulos C, Faucetta K, Hill C, Portilla XA, Burrell L, Lee H, et al. Impacts on family outcomes of evidence‐based early childhood home visiting: results from the Mother and Infant Home Visiting Program evaluation. OPRE Report 2019‐07. Washington, DC: Office of Planning, Research, and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services, 2019. [Google Scholar]
Moran 2017 [pers comm]
- Moran G. Re: systematic review study data [personal communication]. Email to: L O'Hara 11 March 2017.
Moullin 2014
- Moullin S, Waldfogel J, Washbrook E. Baby bonds: parenting, attachment and a secure base for children. www.suttontrust.com/researcharchive/baby‐bonds/ (accessed 3 December 2015).
Mundy 2003
- Mundy P, Delgado C, Block J, Venezia M, Hogan A, Siebert J. A Manual for the Abridged Early Social Communication Scales (ESCS). Coral Gables (FL): University of Miami, 2003. [Google Scholar]
Murray 1996
- Murray L, Fiori‐Cowley A, Hooper R, Cooper P. The impact of postnatal depression and associated adversity on early mother‐infant interactions and later infant outcome. Child Development 1996;67(5):2512‐26. [DOI: 10.1111/j.1467-8624.1996.tb01871.x; PUBMED: 9022253] [DOI] [PubMed] [Google Scholar]
Murray 1997
- Murray L, Cooper PJ. Effects of postnatal depression on infant development. Archives of Disease in Childhood 1997;77(2):99‐101. [DOI: 10.1136/adc.77.2.99; PMC1717268 ; PUBMED: 9301345] [DOI] [PMC free article] [PubMed] [Google Scholar]
NICE 2015
- National Institute for Health and Care Excellence. Children’s attachment: attachment in children and young people who are adopted from care, in care or at high risk of going into care. www.nice.org.uk/guidance/ng26 (accessed 23 September 2019). [PubMed]
NICE 2016
- National Institute for Health and Care Excellence. Children's attachment. www.nice.org.uk/guidance/qs133 (accessed 23 September 2019).
NICHD Early Child Care Research Network 1999
- NICHD Early Child Care Research Network. Chronicity of maternal depressive symptoms, maternal sensitivity and child functioning at 36 months. Developmental Psychology 1999;35(5):1297‐310. [DOI: 10.1037/0012-1649.35.5.1297; PUBMED: 10493655] [DOI] [PubMed] [Google Scholar]
NICHD Early Child Care Research Network 2005
- NICHD Early Child Care Research Network. Child care and mother–child interaction in the first 3 years of life. The NICHD Early Child Care Research Network. New York, London: The Guildford Press, 2005:231‐245. [Google Scholar]
NIHCD Early Child Care Research Network 2003
- NIHCD Early Child Care Research Network. Early child care and mother–child interaction from 36 months through first grade. Infant behavior and Development 2003;26(3):345‐70. [DOI: 10.1016/S0163-6383(03)00035-3] [DOI] [Google Scholar]
O'Hara 2017a [pers comm]
- O'Hara L. Systematic review study data [personal communication]. Email to: H Van Bakel 16 January 2017.
O'Hara 2017b [pers comm]
- O'Hara L. Systematic review study data [personal communication]. Email to: G Moran 6 March 2017.
Pederson 1995
- Pederson DR, Moran G. A categorical description of attachment relationships in the home and its relation to q‐sort measures of infant– mother interaction. Monographs of the Society for Research in Child Development 1995;60:247–54. [Google Scholar]
Pederson 1999
- Pederson DR, Moran G. The relationship imperative: arguments for a broad definition of attachment. Journal of Family Psychology 1999;13(4):496‐500. [DOI: 10.1037/0893-3200.13.4.496] [DOI] [Google Scholar]
Pelchat 2003
- Pelchat D, Bisson J, Bois C, Saucier J‐F. The effects of early relational antecedents and other factors on the parental sensitivity of mothers and fathers. Infant and Child Development 2003;12(1):27‐51. [DOI: 10.1002/icd.335] [DOI] [Google Scholar]
Pereira 2012
- Pereira J, Vickers K, Atkinson L, Gonzalez A, Wekerle C, Levitan R. Parenting stress mediates between maternal maltreatment history and maternal sensitivity in a community sample. Child Abuse & Neglect 2012;36(5):433‐7. [DOI: 10.1016/j.chiabu.2012.01.006; PUBMED: 22633056] [DOI] [PubMed] [Google Scholar]
Pereira 2018 [pers comm]
- Pereira M. Systematic review ‐ data request [personal communication]. Email to: E Smith 28 February 2018.
Poswlawsky 2018 [pers comm]
- Poswlawsky I. Systematic review data request [personal communication]. Email to: E Smith 17 January 2018.
R 2018 [Computer program]
- R Foundation for Statistical Computing. R: A language and environment for statistical computing. Version 3.6.1. Vienna (AT): R Foundation for Statistical Computing, 2018.
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Ryan 2016
- Ryan R, Hill S. How to GRADE the quality of the evidence. cccrg.cochrane.org/author‐resources (accessed 20 July 2019).
Samarakkody 2010
- Samarakkody DC, Fernando DN, Perera H, McClure RJ, Silva H. The Child Behaviour Assessment Instrument: development and validation of a measure to screen for externalising child behaviour problems in community setting. International Journal of Mental Health Systems 2010;4:13. [DOI: 10.1186/1752-4458-4-13; PMC2897774 ; PUBMED: 20529304] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schünemann 2017
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Akl E, et al. on behalf of the Cochrane GRADEing Methods Group and the Cochrane Statistical Methods Group. Chapter 11: Completing ‘Summary of findings’ tables and grading the confidence in or quality of the evidence. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Shin 2008
- Shin H, Park YJ, Ryu H, Seomun GA. Maternal sensitivity: a concept analysis. Journal of Advanced Nursing 2008;64(3):304‐14. [DOI: 10.1111/j.1365-2648.2008.04814.x; PUBMED: 18764848] [DOI] [PubMed] [Google Scholar]
Singer 1999
- Singer LT, Salvator A, Guo S, Collin M, Lilien L, Baley J. Maternal psychological distress and parenting stress after the birth of a very low‐birth‐weight infant. JAMA 1999;281(9):799‐805. [DOI: 10.1001/jama.281.9.799; PUBMED: 10071000] [DOI] [PMC free article] [PubMed] [Google Scholar]
Slade 2004
- Slade A, Aber JL, Bresgi I, Berger B, Kaplan M. The Parent Development Interview—revised. Unpublished protocol 2004.
Slade 2005
- Slade A, Grienenberger J, Bernbach E, Levy D, Locker A. Maternal reflective functioning attachment, and the transmission gap: a preliminary study. Attachment & Human Development 2005;7(3):283‐98. [DOI: 10.1080/14616730500245880; PUBMED: 16210240] [DOI] [PubMed] [Google Scholar]
Smith 2017a [pers comm]
Smith 2017b [pers comm]
- Smith E. Cochrane review data request [personal communication]. Email to: C Lam‐Cassettari 2 June 2017.
Smith 2018a [pers comm]
- Smith E. Cochrane review on video interaction guidance [personal communication]. Email to: A Mendelsohn 1 February 2018.
Smith 2018b [pers comm]
- Smith E. Systematic review ‐ study data [personal communication]. Email to: I Bovenschen 12 January 2018.
Smith 2018c [pers comm]
- Smith E. Cochrane review [personal communication]. Email to: M Hoivik 8 February 2018.
Smith 2018d [pers comm]
- Smith E. Cochrane review [personal communication]. Email to: D Koniak 8 February 2018.
Smith 2018e [pers comm]
- Smith E. Systematic review ‐ data request [personal communication]. Email to: I Soares 12 January 2018.
Smith 2018f [pers comm]
- Smith E. Systematic review data request [personal communication]. Email to: I Poswlawsky 12 January 2018.
Smith 2018g [pers comm]
- Smith E. Systematic review ‐ VIG [personal communication]. Email to: M Bakermans‐Kranenburg 21 February 2018.
Smith 2018h [pers comm]
- Smith E. Cochrane review: data request [personal communication]. Email to: E Sheiner‐Moss 12 January 2018.
Smith 2018i [pers comm]
- Smith E. Cochrane review on video interaction guidance [personal communication]. Email to: A Mendelsohn 1 February 2018.
Smith 2019a [pers comm]
- Smith ER. Cochrane systematic review: data request [personal communication]. Email to: L Barone 9 July 2019.
Smith 2019b [pers comm]
- Smith E. Cochrane review: data request [personal communication]. Email to: R Seifer 22 July 2019.
Sparrow 2005
- Sparrow S, Cicchetti D, Balla D. Vineland Adaptive Behavior Scales. 2nd Edition. Minneapolis (MN): Pearson Assessment, 2005. [Google Scholar]
Spielberger 1983
- Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the State–Trait Anxiety Inventory. Palo Alto (CA): Consulting Psychologists Press, 1983. [Google Scholar]
Squires 2002
- Squires J, Bricker D, Twombly E, Yockelson S, Schoen Davis M, et al. Ages & Stages Questionnaires®: Socio‐Emotional. A parent‐completed, child‐monitoring system for socio‐emotional behaviors. Baltimore (ML): Paul H Brookes Publishing Co, 2002. [clas.uiowa.edu/nrcfcp/sites/clas.uiowa.edu.nrcfcp/files/Ages%20and%20Stages%20Questionnaires%20ASQSE.PDF] [Google Scholar]
Sroufe 2005
- Sroufe LA, Egeland B, Carlson EA, Collins WA. The Development of the Person: The Minnesota Study of Risk and Adaptation from Birth to Adulthood. New York (NY): The Guilford Press, 2005. [Google Scholar]
Steele 2010
- Steele H, Siever L. An attachment perspective on borderline personality disorder: advances in gene‐environment considerations. Current Psychiatry Reports 2010;12(1):61‐7. [DOI: 10.1007/s11920-009-0091-0; PUBMED: 20425312] [DOI] [PubMed] [Google Scholar]
Stein 2018 [pers comm]
- Stein A. Data for our 2006 paper [personal communication]. Email to: J Barlow 11 June 2018.
Sterne 2017
- Sterne JA, Egger M, Moher D, Boutron I (editors). Chapter 10: Addressing reporting biases. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Stolk 2008
- Stolk MN, Mesman J, Zeijl J, Alink LR, Bakersman‐Kranenburg MJ, Ijzendoorn MH, et al. Early parenting intervention aimed at maternal sensitivity and discipline: a process evaluation. Journal of Community Psychology 2008;36(6):780‐97. [DOI: 10.1002/jcop.20280] [DOI] [Google Scholar]
Sumner 1994
- Sumner G, Spietz A. NCAST Caregiver/Parent‐Child Interaction Teaching Manual. Seattle (WA): NCAST Publictions, 1994. [Google Scholar]
Terry 1991
- Terry DJ. Stress, coping and adaptation to new parenthood. Journal of Social and Personal Relationships 1991;8:527‐47. [Google Scholar]
UNICEF 2008
- UNICEF. The Child Care Transition. Innocenti Report Card 8. Florence (IT): UNICEF Innocenti Research Centre, 2008. [www.unicef‐irc.org/publications/pdf/rc8_eng.pdf] [Google Scholar]
Uzgiris 1975
- Uzgiris IC, Hunt JM. Assessment in Infancy: Ordinal Scales of Psychological Development. Champaign (IL): University of Illinois Press, 1975. [Google Scholar]
Van Bakel 2017 [pers comm]
- Bakel H. Re: quick query [personal communication]. Email to: J Barlow 12 June 2017.
Van den Boom 1988
- Boom DC. Neonatal Irritability and the Development of Attachment: Observation and Intervention [PhD thesis]. Leiden (NL): Leiden University, 1988. [Google Scholar]
Van den Boom 1991
- Boom DC. The influence of infant irritability on the development of the mother‐infant relationship in the first six months of life. In: Nugent JK, Lester BM, Brazelton TB editor(s). The Cultural Context of Infancy. Vol. 2, Norwood (NJ): Ablex Publishing Corporation, 1991:63‐89. [Google Scholar]
Van den Broek 2017
- Broek E, Eijden AJ, Overbeek MM, Kef S, Sterkenburg PS, Scheungel C. A systematic review of the literature on parenting of young children with visual impairments and the adaptions for Video‐feedback Intervention to promote Positive Parenting (VIPP). Journal of Developmental and Physical Disabilities 2017;29(3):503‐45. [DOI: 10.1007/s10882-016-9529-6; PMC5403903; PUBMED: 28496296] [DOI] [PMC free article] [PubMed] [Google Scholar]
Van Ijzendoorn 1995
- IJzendoorn MJ, Juffer F, Duyvesteyn MG. Breaking the intergenerational cycle of insecure attachment: a review of the effects of attachment‐based interventions on maternal sensitivity and infant security. Journal of Child Psychology and Psychiatry 1995;36(2):225‐48. [DOI: 10.1111/j.1469-7610.1995.tb01822.x; PUBMED: 7759588] [DOI] [PubMed] [Google Scholar]
Veroniki 2019
- Veroniki AA, Jackson D, Bender R, Kuss O, Langan D, Higgins JP, et al. Methods to calculate uncertainty in the estimated overall effect size from a random effects meta‐analysis. Research Synthesis Methods 2019;10(1):23‐43. [DOI: 10.1002/jrsm.1319; PUBMED: 30129707] [DOI] [PubMed] [Google Scholar]
Viechtbauer 2010
- Viechtbauer W. Conducting meta‐analyses in R with the metafor package. Journal of Statistical Software 2010;36(3):1‐48. [DOI: 10.18637/jss.v036.i03] [DOI] [Google Scholar]
Vik 2006
- Vik K, Hafting M. Video interaction guidance offered to mothers with postnatal depression: experiences from a pilot study. Nordic Journal of Psychiatry 2006;60(3):234‐8. [DOI: 10.1080/08039480600636593; PUBMED: 16720515] [DOI] [PubMed] [Google Scholar]
Wan 2017
- Wan MW, Brooks A, Green J, Abel K, Elmadih A. Psychometrics and validation of a brief rating measure of parent‐infant interaction Manchester assessment of caregiver–infant interaction. International Journal of Behavioral Development 2017;41(4):542‐9. [DOI: 10.1177/0165025416631835] [DOI] [Google Scholar]
Waters 1985
- Waters E, Deane KE. Defining and assessing individual differences in attachment relationships: Q‐methodology and the organization of behavior in infancy and early childhood. Monographs of the Society for Research in Child Development 1985;50(1‐2):41‐65. [DOI: 10.2307/3333826] [DOI] [PubMed] [Google Scholar]
Waters 1987
- Waters E. The Attachment Q‐set (Version 3). In: Waters E, Vaughn BE, Posada G, Kondo‐Ikemura K editor(s). Caregiving, Cultural, and Cognitive Perspectives on Secure‐Base Behavior and Working Models. Monographs of the Society for Research in Child Development. Hoboken, JN, USA: Wiley‐Blackwell, (accessed 20 August 2015):247‐54. [Google Scholar]
Webster‐Stratton 2015
- Webster‐Stratton C. The Incredible Years Parent Programs: methods and principles that support fidelity of program delivery. In: Ponzetti J editor(s). Evidence‐Based Parenting Education: A Global Perspective. Routledge, 2015. [Google Scholar]
Weinfield 2004
- Weinfield NS, Whaley GJ, Egeland B. Continuity, discontinuity and coherence in attachment from infancy to late adolescence: sequelae of organization and disorganization. Attachment & Human Development 2004;6(1):73‐97. [DOI: 10.1080/14616730310001659566; PUBMED: 14982680] [DOI] [PubMed] [Google Scholar]
Zeanah 1993
- Zeanah CH, Mammen OK, Lieberman AF. Disorders in attachment. In: Zeanah CH Jr editor(s). Handbook of Infant Mental Health. New York (NY): The Guilford Press, 1993:332‐49. [Google Scholar]
Zigmond 1983
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica 1983;67(6):361‐70. [DOI: 10.1111/j.1600-0447.1983.tb09716.x; PUBMED: 6880820] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
O'Hara 2016
- O’Hara L, Barlow J, Livingstone N, Macdonald G. Video feedback for improving parental sensitivity and attachment. Cochrane Database of Systematic Reviews 2016, Issue 9. [DOI: 10.1002/14651858.CD012348] [DOI] [PMC free article] [PubMed] [Google Scholar]