

Abstract
Diabetes mellitus is a chronic disease of aging that affects more than 20% of people over 65. In older patients with diabetes, comorbidities are highly prevalent and their presence may alter the relative importance, effectiveness, and safety of treatments for diabetes. Randomized controlled trials have shown that intensive glucose control produces microvascular and cardiovascular benefits but typically after extended treatment periods (five to nine years) and with exposure to short term risks such as mortality (in one trial) and hypoglycemia. Decision analysis, health economics, and observational studies have helped to illustrate the importance of acknowledging life expectancy, hypoglycemia, and treatment burden when setting goals in diabetes. Guidelines recommend that physicians individualize the intensity of glucose control and treatments on the basis of the prognosis (for example, three tiers based on comorbidities and functional impairments) and preferences of individual patients. Very few studies have attempted to formally implement and study these concepts in clinical practice. To better meet the treatment needs of older patients with diabetes and comorbidities, more research is needed to determine the risks and benefits of intensifying, maintaining, or de-intensifying treatments in this population. This research effort should extend to the development and study of decision support tools as well as targeted care management.
Introduction
Caring for older patients with diabetes mellitus is a major public health and policy challenge. The age at which someone is identified as “older” has evolved with advances in medicine, but it is currently set at 65 years for most developed countries. The prevalence of diabetes is high; more than 20% of adults aged over 65 have a diagnosis of diabetes.1 Compared with their non-diabetic peers, older adults with diabetes have a higher risk of microvascular and cardiovascular diseases, geriatric conditions (such as falls and dementia), and hypoglycemia. Despite the considerable burden of diabetes in older adults, the management of the disease has been controversial; recurring debates have taken place about the appropriate intensity of glucose control and the role of glucose lowering medicines in this population.
This review provides a comprehensive summary of the evidence supporting contemporary recommendations for managing older patients with diabetes and comorbidities. Diabetes care guidelines from multiple clinical organizations now emphasize the concepts of individualization of goal setting and treatment plans, as well as maximizing everyday quality of life. A primary aim of this review is to ensure that clinicians are aware of these guidelines, which have had modest adoption according to national studies of diabetes care. The second aim of the review is to identify gaps in evidence and outline a research agenda for the field of geriatric diabetes, which continues to be relatively understudied.
Sources and selection criteria
To establish the evidence base for intensive glucose control, I identified randomized controlled trials, published in English in core medical journals, involving older adults (>65 years of age) with type 2 diabetes, and evaluating the clinical effects of intensive glucose control using drugs in the outpatient setting. I searched PubMed (12 May 2005 to 12 May 2015) with the term “intensive glucose control” and filtered results by study design, language, medical journals, and age groups. I also included landmark studies before that date. Because of the limited availability of clinical trial evidence of glucose control in the oldest and sickest patients, I also included studies from the fields of epidemiology, decision science, and health economics. I did a separate search of PubMed for the same time period and population to identify trials evaluating approaches to providing diabetes care management. I also searched the clinical trial repository (ClinicalTrials.gov) for ongoing trials of diabetes management focused on older adults. These searches were augmented with a review of the bibliographies of systematic reviews, meta-analyses, and scientific position statements.2 3 4 5 I prioritized interventions that included goal setting, decision making, self care management, and care of geriatric conditions, rather than specific drugs or surgical therapies. I reviewed and collated the recommendations from practice guidelines and consensus statements from the American Geriatrics Society,6 7 the American Diabetes Association,8 the European Diabetes Working Party for Older People,9 and other major clinical organizations.
Prevalence and pathophysiology
Diabetes is a chronic disease of aging. The prevalence of diabetes increases sharply with age,10 affecting 1.6% of people under 45 years, 12.2% of adults aged 45-64 years, and 21.8% of those aged 65-74 years.1 In the United States, 11.2 million adults over the age of 65 are estimated to be affected by the disease.11 The vast majority of older adults with diabetes have type 2 diabetes (96%) owing to a combination of increased insulin resistance and impaired insulin secretion.12 13 Insulin resistance associated with advancing age is believed to be due to a combination of adiposity, sarcopenia (decreased muscle mass), and physical inactivity.14
The prevalence of diabetes in older adults is a reflection of the general growth in diabetes that has been observed in all age groups over three decades. With the aging of the baby boomer generation and high rates of obesity in the United States, the subpopulation of older people with diabetes is expected to double in the next two decades.15 This morbidity will contribute to an expected tripling of Medicare costs for diabetes care in the next 25 years (increasing from $45bn (£31bn; €40bn) to $171bn a year).15 The United States is not alone in its struggle with this burgeoning epidemic. The International Diabetes Federation anticipates that the global prevalence of diabetes is expected to increase from 415 million people in 2015 to 642 million by 2040, with nearly 50% of these people being over the age of 65.16
Diabetes and comorbid conditions
One of the great clinical challenges of managing diabetes is that the disease rarely occurs in isolation.17 Nearly 60% of older adults with diabetes have at least one comorbid chronic disease,18 19 20 and as many as 40% have four or more comorbid diseases.21 The rising prevalence of older people with multiple chronic diseases can be attributed to progress in public health and medicine, which has increased the number of people in the population reaching older ages,22 23 24 25 as well as improvements in chronic disease management that have extended the time that people are living with their chronic diseases.15 26
Comorbid conditions often occur in combination.27 To describe naturally occurring clusters of comorbid conditions, one study used latent class analysis to identify subgroups of a nationally representative sample (National Social Life, Health, and Aging Project (NSHAP)) of community dwelling adults (aged 57-85 years) with diabetes (n=750) based on 14 highly prevalent comorbid conditions in the older population.28 A three class model was chosen on the basis of specified model fit criteria. All classes had estimated probabilities of obesity, hypertension, and arthritis of 40% or more. Class 1 (67%) had the lowest probabilities of most conditions. Class 2 (29%) had the highest probabilities of incontinence, kidney disease, and cancer. Class 3 (9%) had the highest probabilities of congestive heart failure and myocardial infarction (>95%). Only respondents in classes 2 and 3 had six or more comorbid conditions (fig 1). Respondents in classes 2 (17%) and 3 (33%) had markedly higher five year mortality rates than did respondents in class 1 (9%) (P<0.001). Classifying the older population with diabetes on the basis of comorbid conditions produced three distinct subgroups. Cardiovascular disease history and high comorbid condition counts may distinguish subgroups that are less likely to benefit from intensive glycemic control.
Fig 1.

Distribution of patients by number of comorbid conditions, according to comorbidity classes in the National Social Life, Health, and Aging Project (2005-06)
A separate analysis of the Health and Retirement Study supports the concept that considering older patients with diabetes to fall into three unique classes is rational. People with diabetes were classified on the basis of the presence and number of comorbidities or impairments of functional status.29 This prescriptive approach produced three major classes of older patients: those who are relatively healthy; those with complex medical histories, for whom self care may be difficult; and those with very important comorbid illness and functional impairment. Whereas most patients were in the relatively healthy group, nearly 22% of adults with diabetes (about 3 million people) had health characteristics that could make self management of diabetes difficult (fig 2). Another 10% (1.4 million) may receive limited benefit from some diabetes management. As with the NSHAP analysis, the three classes corresponded to increasing levels of mortality risk.30
Fig 2.

Frequencies of adults with diabetes in clinical groups by age in Health and Retirement Study
Apart from these efforts to classify older patients living with diabetes, several well established comorbidity classification systems exist that predict the risk of mortality in older adults. These include the Charlson comorbidity index,31 32 the Elixhauser comorbidity index developed for administrative claims data,33 and the total illness burden index (TIBI).34 Investigators have also found that impairments in activities of daily living (ADLs) are independent predictors of mortality. This has led to the development and validation of mortality prediction models that include age, sex, comorbid conditions, and functional measures to estimate a mortality index score.35 36
Geriatricians have also long recognized that some older patients seem to be particularly vulnerable to external insults and have defined this clinical syndrome as frailty. Frailty is thought to be due to cumulative declines across multiple physiologic systems over time. Markers of frailty include age associated declines in lean body mass, strength, endurance, balance, walking performance, and activity.37 Older patients who are frail are at increased risk for incident falls, worsening mobility or ADL disability, hospital admission, and death.
Evidence about glucose control in older people
Randomized controlled trials
Older patients living with diabetes and comorbidities have historically been excluded from clinical trials of diabetes care.38 The landmark United Kingdom Prospective Diabetes Study (UKPDS) excluded people over the age of 65.39 40 Subsequent major clinical trials, such as ACCORD (Action to Control Cardiovascular Risk in Diabetes), ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation), and VADT (Veterans Affairs Diabetes Trial), included adults over 65 years of age but did not include many participants over 75 years of age at the time of enrollment. Another limitation of these trials is that they focused on selected outcomes, such as microvascular complications, cardiovascular complications, and mortality, which may not encompass the entire experience of patients with treatments (see below). Despite these limitations, these trials still provide important insights into the timing, magnitude, and direction of effects of glucose lowering for older patients. The trials have heterogeneous results that may be due to differences in patient populations, available treatments, treatment protocols, and glycemic targets (table 1).
Table 1.
Major randomized controlled trials of intensive glucose control
| Characteristic | UKPDS39 40 | ACCORD41 | ADVANCE42 43 | VADT44 45 |
|---|---|---|---|---|
| Mean age, years | 53.3 | 62.2 | 66 | 60.4 |
| Duration of diabetes, years | Newly diagnosed | 10 (median) | 8 (mean) | 11.5 (mean) |
| Achieved HbA1c
(intensive v standard) |
7.9% v 7.0% | 7.5% v 6.4% | 7.3% v 6.5% | 8.4% v 6.9% |
| Trial follow-up time, years | 10 | 3.5 | 5 | 5 |
| Within trial findings | Mortality: RR 0.94 (95% CI 0.80 to 1.10) | Mortality: HR 1.22 (95% CI 1.01 to 1.46) | Mortality: HR 0.93 (95% CI 0.83 to 1.06) | Mortality: HR 1.07 (95% CI 0.81 to 1.42) |
| Microvascular complications: RR 0.75 (0.60 to 0.93) | Primary outcome (non-fatal and fatal cardiovascular disease): HR 0.90 (0.78 to 1.04) | Microvascular complications: HR 0.86 (0.77 to 0.97) | Cardiovascular events: HR 0.88 (0.74 to 1.05) | |
| Myocardial infarction: RR 0.84 (0.71 to 1.00) | Non-fatal myocardial infarction: HR 0.76 (0.62 to 0.92) | Macrovascular complications: HR 0.94 (0.84 to 1.06) | ||
| Post-trial follow-up time | 10 years | 0.2 years of additional intervention period; 1.2 years | 6 years | 5 years |
| Post-trial follow-up findings | Mortality: RR 0.87 (0.79 to 0.96) | Mortality: HR 1.19 (1.03 to 1.38) | Mortality: HR 1.00 (0.92 to 1.08)) | Mortality: HR 1.05 (0.89 to 1.25) |
| Microvascular complications: RR 0.76 (0.64 to 0.89) | Primary outcome (non-fatal and fatal cardiovascular disease): HR 0.91 (0.81 to 1.03) | Microvascular complications: HR 0.92 (0.80 to 1.05) | Cardiovascular events: HR 0.83 (0.70 to 0.99) | |
| Myocardial infarction: RR 0.85 (0.74 to 0.97) | Non-fatal myocardial infarction: HR 0.82 (0.70 to 0.96) | Macrovascular complications: HR 1.00 (0.92 to 1.08) |
HR=hazard ratio; RR=relative risk.
The UKPDS provides some of the most important observations regarding the variable timing and heterogeneous effects of intensive glucose control (glycated hemoglobin (HbA1c) of 7.9% v 7.0%) in middle aged patients with recent onset of diabetes. During the original observation period of 10 years, intensive glucose control significantly lowered rates of microvascular disease (risk reduction 25%; P=0.001); however, the Kaplan-Meier plots separated significantly only after nine years of follow-up.46 47 During the post-trial follow-up of an additional 10 years, the benefits of intensive glycemic control on microvascular complications persisted, and benefits for reducing mortality and myocardial infarctions emerged.40 These findings have been called the legacy effect or metabolic memory and suggest that the effects of hyperglycemia on diabetes outcomes may differ according to the history of HbA1c control. With nearly 20 years of follow-up, surviving patients were, on average, in their early 70s in the most recent observational studies.
In the ACCORD trial, 10 251 participants with type 2 diabetes were randomly assigned to intensive glucose therapy (HbA1c<6.0%) or standard therapy (HbA1c 7.0-7.9%).41 Compared with UKPDS, patients were older, had longer duration of diabetes (median duration 10 years), and had a high risk of cardiovascular disease. On average, the intensive therapy group achieved an HbA1c of 6.4% and the standard therapy group achieved an HbA1c of 7.5%. The trial was ended early after a mean follow-up of 3.5 years, because the intensive therapy group had a higher mortality rate than the standard therapy group (hazard ratio 1.22, 95% confidence interval 1.01 to 1.46). The point estimate for the primary cardiovascular composite outcome suggested a benefit of intensive glucose control, but the finding was not significant (hazard ratio 0.90, 0.78 to 1.04). At five years’ follow-up, the ACCORD trial re-confirmed a higher mortality rate in the intensive glucose therapy group (hazard ratio 1.19, 1.03 to 1.38) and a lower rate of non-fatal myocardial infarction (0.82, 0.70 to 0.96).48 In age stratified analyses, ACCORD investigators have found that the excess mortality associated with intensive therapy occurred primarily in patients under 65 years of age.49
The ADVANCE trial included 11 140 participants with type 2 diabetes aged 55 years or older and randomized them to intensive glucose therapy (HbA1c<6.5%) or standard glucose therapy.42 Like ACCORD, ADVANCE enrolled patients at high risk for cardiovascular events and patients had an established history of diabetes (mean duration eight years). The intensive therapy and standard therapy groups in ADVANCE achieved HbA1c levels of 6.5% and 7.3%, respectively, at five years’ follow-up. However, unlike in the ACCORD trial, the intensive glucose therapy group had a 10% relative reduction in the combined outcome of major macrovascular and microvascular events (hazard ratio 0.90, 0.82 to 0.98), mostly due to a 21% relative reduction in nephropathy (0.79, 0.66 to 0.93), and no significant effects on major macrovascular events or death were seen. During six years of post-trial follow-up, there continued to be no significant effects on major macrovascular events or death.43
The VADT randomized 1791 veterans to intensive glucose therapy (an absolute reduction of 1.5% in HbA1c) versus standard therapy.44 Patients had a mean duration of diabetes of 11.5 years, and 40% had a history of cardiovascular disease. The intensive therapy group achieved a mean HbA1c of 6.9%, and the standard therapy group achieved a mean of 8.4%. At a median of 5.6 years’ follow-up, the primary outcome of major cardiovascular events was non-significantly lower in the intensive therapy group (hazard ratio 0.88, 0.74 to 1.05). No significant differences in death were seen between the two groups.44 In an erratum, VADT investigators reported that progression of albuminuria was lower in the intervention therapy group than the standard therapy group.50 In post-trial follow-up (total of 10 years’ observation), the intensive therapy arm had a significantly lower risk of major cardiovascular events (hazard ratio 0.83, 0.70 to 0.99) but had no mortality benefit.45
The trial results from ACCORD, ADVANCE, and VADT are most applicable to patients in their 60s and early 70s. Some trial investigators studying intensive diabetes management have attempted to enroll patients in their 80s but faced unexpected difficulties. The ACCORD trial attempted to enroll patients over the age of 80 but found that patients in this age group had very high hypoglycemia rates when randomized to the intervention arms. The study protocol was later revised to exclude patients over 80.49 In the Japan Elderly Diabetes Intervention Trial, investigators attempted to evaluate a multiple risk factor intervention in patients aged 65-85 years.51 52 More than a thousand (1173) patients were randomized to intensive or conventional treatment. Despite a structured protocol, investigators were unable to achieve separation in achieved HbA1c across study arms. This was attributed to concerns about treatment related hypoglycemia in older patients.
Simulated trials
Because of the strict exclusion criteria of controlled trials, investigators have used microsimulation models and observational methods to gain more insight into the expected effect of intensive glucose control in the oldest and sickest patients.53 In simulation models, predictions for patients’ outcomes are calculated from transition probabilities that are generated from results of randomized controlled trials, epidemiologic studies, and meta-analyses.54 55 56 57
One such microsimulation model evaluated how comorbidities and functional impairment would affect the potential benefits of intensive glucose control achieved in UKPDS (HbA1c level of 7.0% v 7.9%).58 This decision analytic study used a hypothetical population of adults 60-80 years of age with type 2 diabetes and no history of diabetes related complications. For this analysis, the UKPDS outcomes model was revised by replacing the background mortality module with a previously developed geriatric mortality prediction model.35 54
The revised diabetes model showed that the expected benefits of intensive control were inversely related to the level of comorbid illness and functional impairment for all age groups (fig 3).58 For example, for adults aged 60-64 years with new onset of diabetes, the benefits declined from 106 (95% confidence interval 95 to 117) quality adjusted days of good health at baseline to 44 (38 to 50) days with 3 additional mortality index points and 8 (5 to 10) days with 7 additional index points. For patients with longer duration of diabetes, the expected benefits of intensive glucose control were also negatively associated with life expectancy. For adults 60-64 years of age with diabetes for 10-15 years, the expected benefit of intensive glucose control decreased from 116 (103 to 129) quality adjusted days to 36 (29 to 43) days with 4 additional index points and 8 (6 to 11) days with 8 additional index points.
Fig 3.

Expected quality of life benefits of intensive glucose control for 60-64 year old and 75-79 year old patients with newly diagnosed diabetes, with increasing levels of comorbid illness and functional impairment
A subsequent observational study of 3074 patients with type 2 diabetes characterized participants into high and low-moderate comorbidity groups (TIBI score) at baseline and observed them for five years.59 Patients in the low-moderate comorbidity group with baseline HbA1c levels of 6.5% or less had a lower five year incidence of cardiovascular events (adjusted hazard ratio 0.60, 0.42 to 0.85; P=0.005). However, patients in the high comorbidity group gained no significant benefit from HbA1c levels of 6.5% or less. Similarly, only the low-moderate comorbidity group had fewer cardiovascular events after attaining an HbA1c level of 7.0% (adjusted hazard ratio 0.61, 0.44 to 0.83; P=0.001). Together, these studies suggest that less stringent glucose targets may be reasonable in patients with diabetes and limited life expectancy.
Quality of life
An important challenge in research focused on older patients with multiple chronic conditions is determining the right outcomes to assess. Biomeasure outcomes used in short term drug and device trials for diabetes (such as HbA1c) are convenient and more easily modifiable by treatments but may not have immediate clinical salience to patients. Clinical outcomes such as mortality and microvascular and cardiovascular complications are important to patients but may not be modifiable in the short term and may not capture the full spectrum of experience of patients. Thought leaders in aging research have recommended that researchers begin using health related quality of life (HRQL) measures such as the Medical Outcomes Study 8 (SF-8) and 36 (SF-36) item Short-Form Survey and the Patient Reported Outcomes Measurement Information System 29 item Health Profile.60 Unfortunately, a recent review of clinical trials in diabetes found that a minority of studies included outcomes important to patients.61
Making the shift from traditional clinical outcomes to outcomes important to patients raises questions about what interventions or conditions have the largest effects on patient centered outcomes. One study evaluated associations between HRQL and geriatric syndromes (chronic pain, depression, urinary incontinence, underweight, and falls), diabetic complications, and hypoglycemia in older adults with diabetes. Data came from a race stratified random sample of adults aged 60-75 years with type 2 or type 1 diabetes, who completed a survey that included an HRQL instrument based on the SF-8 (n=6317). In combined exposure models, geriatric syndromes (−5.3, 95% confidence interval −5.8 to −4.8; P<0.001) and diabetic complications (−3.5, −4.0 to −2.9; P<0.001) were associated with lower physical HRQL. The lowest mental HRQL was associated with depression, underweight (body mass index<18), amputation, and hypoglycemia. In combined exposure models, only hypoglycemia was associated with lower mental HRQL (−4.0, −7.0 to −1.1; P=0.008). Geriatric syndromes and hypoglycemia are associated with lower HRQL to a comparable degree to traditional complications of diabetes. These results suggest that tackling geriatric syndromes and avoiding hypoglycemia should be given as high a priority as preventing diabetic complications in older adults with diabetes.
Although this study highlighted the importance of geriatric syndromes, it did not include cognitive impairment and dementia. Cognitive impairment and dementia, which are strongly associated with diabetes,62 frequently lead to loss of independence in ADLs and instrumental ADLs, important elements of quality of life.
Hypoglycemia
Hypoglycemia has long been viewed as a barrier to achieving intensive glycemic control. In trials of intensive glucose control, rates of major hypoglycemia needing medical attention have always been consistently higher in the intensive control arms.41 42 44 46 Although previously considered a secondary outcome, hypoglycemia has become a primary outcome of basic and clinical diabetes research.63 From a policy perspective, hypoglycemia has been proposed as a key adverse drug event and performance measure for healthcare systems.64
Several recent studies support the growing importance of hypoglycemia relative to traditional complications of diabetes. A natural history study of a contemporary cohort of older patients with diabetes assessed how the incidence and ranking of complications differed by age and duration of diabetes.65 Among older adults with diabetes of short duration, cardiovascular complications followed by hypoglycemia were the most common non-fatal complications. Among patients aged 70-79 years with a short duration of diabetes, rates of coronary artery disease and hypoglycemia were higher (11.47 per 1000 person years and 5.03 per 1000 person years, respectively) than rates of end stage renal disease (2.60 per 1000 person years), lower limb amputation (1.28 per 1000 person years), and acute hyperglycemic events (0.82 per 1000 person years).
The contemporary rankings of diabetes related complications in today’s older adults are a reflection of secular trends in the management of diabetes. A retrospective observational study used data from 33 952 331 Medicare fee-for-service beneficiaries 65 years or older from 1999 to 2011. During this time, rates of admissions for hyperglycemia declined by 38.6% (from 114 to 70 admissions per 100 000 person years), whereas admissions for hypoglycemia increased by 11.7% (from 94 to 105 admissions per 100 000 person years). Hospital admission rates for hypoglycemia now exceed those for hyperglycemia among older adults.
The findings from these two studies suggest that as long term survival with diabetes increases and as the population ages, more research and public health efforts to reduce hypoglycemia will be needed to complement ongoing efforts to reduce cardiovascular and microvascular complications.
Burden of everyday treatments
Related to hypoglycemia is the burden of everyday treatments, an underappreciated aspect of quality of life. The accumulation of tasks of taking medicines, following diets and exercise programs, and monitoring blood glucose concentrations, while also adhering to recommendations for other comorbid conditions, can be overwhelming.27 Although this concept is important, it has been difficult to quantify with traditional measures of quality of life. One study used health state utility methods (a measure of preference) to ascertain the relative burden of diabetes related complications and treatments. It elicited utilities (ratings on a 0-1 scale, where 0 represents death and 1 represents perfect health) for nine complication states and 10 treatment states in 701 patients with diabetes. End stage complications had lower mean utilities than intermediate complications (for example, blindness 0.38 (SD 0.35) v retinopathy 0.53 (0.36); P<0.01), and end stage complications had the lowest ratings among all health states. Intensive treatments had lower mean utilities than conventional treatments (for example, intensive glucose control 0.67 (0.34) v conventional glucose control 0.76 (0.31); P<0.01), and the lowest rated treatment state was comprehensive diabetes care (0.64 (0.34)). On average, patients rated comprehensive treatment states similarly to intermediate complication states. Importantly, patients’ ratings of health states were highly heterogeneous, with some patients viewing comprehensive diabetes care as near perfect health whereas a significant minority (18%) viewed the same therapy as equivalent to death.
The perceived burden of treatments has important implications for determining the goals and treatments of diabetes in older patients. In cost effectiveness analyses, the incorporation of patients’ preferences regarding life with treatments has shown that the value of intensive glucose control in older patients is highly sensitive to assumptions about quality of life with treatments.66 67 This is because the effects of treatments on quality of life that are experienced routinely by all exposed patients can easily exceed the expected long term benefits of glycemic control that are experienced by a minority of patients.
Guidelines
Over the past 15 years, guidelines on diabetes care from multiple clinical organizations have now almost all adopted concepts of individualized goal setting and care management to maximize quality of life, but they differ in the details of their recommendations (table 2).
Table 2.
Comparison of clinical recommendations for HbA1c goals in older patients with type 2 diabetes
| American Geriatrics Society68 | Department of Veterans Affairs69 | American Diabetes Association8 | European Diabetes Working Party for Older People9 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Description of patient stratum | HbA1c goal | Description of patient stratum | HbA1c goal | Description of patient stratum | HbA1c goal | Description of patient stratum | HbA1c goal | |||
| Healthy | 7.0-7.5% | None or very mild microvascular complications; life expectancy of 10-15 years | <7.0% | Healthy (few coexisting chronic illnesses; intact cognitive and functional status) | <7.5% | Without major comorbidities | 7.0-7.5% | |||
| Moderate comorbidities | 7.5-8.0% | Long duration of diabetes (>10 years); requires combination drug regimen including insulin | <8.0% | Complex/intermediate (examples: multiple coexisting chronic illnesses*, ≥2 instrumental ADL impairments, or mild-moderate cognitive impairment) | <8.0% | Frail patients (dependent; multi-system disease; care home residency, including those with dementia) | 7.6-8.5% | |||
| Multiple comorbidities | 8.0-9.0% | Advanced microvascular complications and/or major comorbid illness; life expectancy <5 years | 8.0-9.0% | Very complex/poor health (examples: long term care, end stage chronic illnesses†, moderate-severe cognitive impairment, or ≥2 ADL dependencies) | <8.5%‡ | |||||
ADL=activities of daily living.
*Conditions serious enough to require drugs or lifestyle management; may include arthritis, cancer, congestive heart failure, depression, emphysema, falls, hypertension, incontinence, stage 3 or worse chronic kidney disease, myocardial infarction, and stroke (multiple means ≥3, but many patients may have ≥5).
†Presence of single end stage chronic illness such as stages III-IV congestive heart failure or oxygen dependent lung disease, chronic kidney disease requiring dialysis, or uncontrolled metastatic cancer may cause considerable symptoms or impairment of functional status and significantly reduce life expectancy.
‡HbA1c of 8.5% equates to estimated average glucose of ~200 mg/dL; less strict glycemic targets than this may expose patients to acute risks from glycosuria, dehydration, hyperglycemic hyperosmolar syndrome, and poor would healing.
Since 2003 the American Geriatrics Society (AGS) has endorsed the concept of individualizing diabetes care on the basis of life expectancy.6 The original guidelines stratified older patients into those with life expectancy above and below five years. The AGS updated these guidelines in 2013 and endorsed a three tier stratification scheme for glycemic targets (“healthy”: HbA1c 7.0-7.5; “moderate comorbidities”: 7.5-8.0; and “multiple comorbidities”: 8.0-9.0).
The Department of Veterans Affairs and Department of Defense diabetes guideline was updated in 2010.69 For glycemic goals, the guideline has three categories of patients based on duration of diabetes, complications, and life expectancy. Patients with either no or very mild microvascular complications of diabetes, who are free of major concurrent illnesses, and who have a life expectancy of at least 10-15 years, should have an HbA1c target of below 7%, if it can be achieved without risk. Patients with longer duration of diabetes (>10 years), or with comorbid conditions, and who require a combination drug regimen including insulin, should have an HbA1c target of below 8%. Patients with advanced microvascular complications, major comorbid illness, and/or a life expectancy of less than five years are unlikely to benefit from aggressive glucose lowering management and should have an HbA1c target of 8-9%. Lower targets (<8%) can be established on an individual basis.
In 2011 the European Diabetes Working Party for Older People published guidelines for treating people aged over 70 years with diabetes.70 These include recommendations to carry out annual evaluations of functional status (global/physical, cognitive, affective) using validated instruments, to avoid use of glibenclamide owing to its high risk of hypoglycemia in this population, and to calculate cardiovascular risk in all patients aged under 85 years. Suggested HbA1c targets are based on age and comorbidity. A range of 7-7.5% is suggested for older patients with type 2 diabetes without major comorbidities and 7.6-8.5% for frail patients (dependent, multisystem disease, care home residency, including those with dementia) whose risk of hypoglycemia may be high and likelihood of benefit relatively low.
In 2012 the American Diabetes Association (ADA) published a consensus statement on the care of older patients that emphasized individualization of diabetes care based on life expectancy, self care abilities, and patients’ preferences.8 The authors of the statement made specific recommendations for glycemic and blood pressure control targets and provided a framework for stratifying patients by health status into classes labeled “healthy,” “complex,” or “very complex,”8 with HbA1c goals of below 7.5%, 8.0%, and 8.5%, respectively. The three classes were identified on the basis of a combination of comorbid conditions and impairments in ADLs and instrumental ADLs.28 29 These recommendations were formally incorporated into the ADA’s annual standards of medical care by 2014.71
Current state of care
Despite the availability of guidelines on geriatric diabetes since 2003, considerable evidence suggests that recommendations to individualize care have not been adopted in clinical practice. Multiple studies of care of older patients with diabetes in national datasets have shown that the intensity of treatments does not differ by health status.64 72 73 One study described the intensity of diabetes treatment among older patients classified by health status in the National Health and Nutrition Examination Survey (NHANES) (2001-10).74 The proportion of older patients achieving an HbA1c below 7.0% was 61% overall and no different across the three tiers of health status. Among patients with HbA1c below 7.0%, 54.9% were treated with either insulin or sulfonylureas, and this proportion was similar across the three tiers of health status.
Integrating comorbidities into diabetes care
The apparent lack of individualized care in national studies may be due to the fact that many of the recommendations in guidelines have not been transformed into clinical management protocols for busy practices. A search of the diabetes management literature and ongoing registered clinical trials found relatively few studies dedicated to studying patients over 65 years of age (two out of 232 ongoing diabetes management trials). Trials of diabetes self management have proliferated,75 but, with rare exceptions, these interventions have been not tailored to the goals or special needs of geriatric populations.76 More importantly, most diabetes management trials are still motivated by the underlying assumption that all patients share the same goals for blood glucose. The paucity of trial evidence for this population may be attributed to the fragmentation of disease oriented research funding agencies, the slow adoption of outcomes important to patients as primary outcomes, and the historical emphasis in diabetes health services research and healthcare policy on achieving uniform population level targets (for example, HbA1c<7.0%).
Despite the shortcomings of the existing literature, the components of a care management program for older patients with comorbidities have been studied individually and, if successfully integrated, could improve the quality of life of these patients. These basic components include personalized decision support for goal setting and treatment planning and personalized care management designed for the social and clinical circumstances of older patients.
Decision support
Establishing a patient’s prognosis and treatment preferences in order to set goals takes valuable time; without systematic processes in place to personalize and track goals, individualized goals may be difficult to recall and adhere to in complex patients. Completing and documenting these tasks accurately, quickly, and over time might be greatly enhanced with clinical decision support. Beyond the technical aspects of making better decisions, the acknowledgment of comorbidities in diabetes care is fundamentally about confronting the realities of life expectancy in medical decision making. In many ways, the clinical and ethical challenges of diabetes management in older patients are the same as those for end of life care, with the important difference that they occur far earlier in the life course of patients.77 78
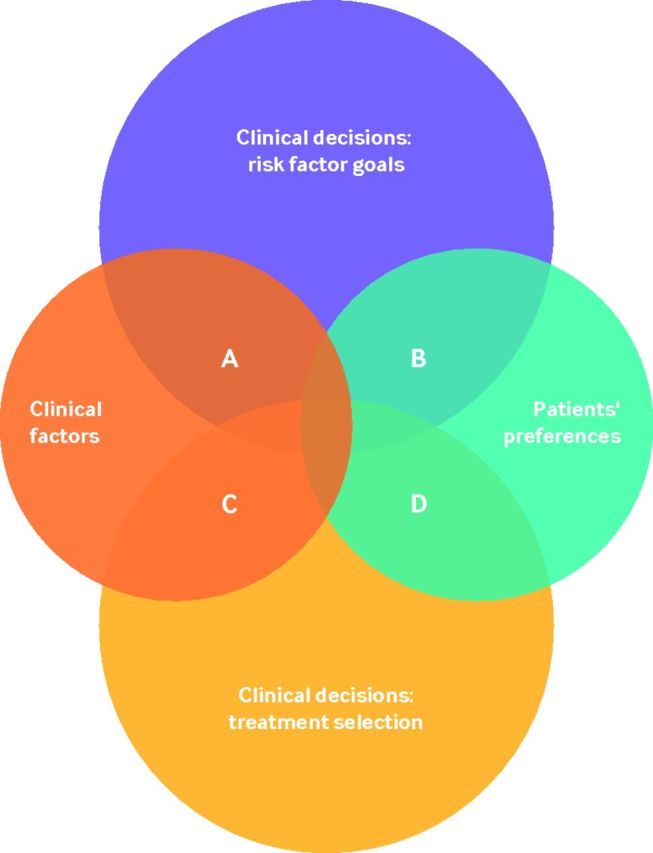
A systematic review created a conceptual framework of personalized diabetes care that illustrates the extent to which diabetes care can be personalized within the clinical decision making process (fig 4).3 The two main areas of clinical decision making are setting risk factor goals (for example, HbA1c, blood pressure, cholesterol) and making treatment selections. These two areas of decision making can be personalized on the basis of clinical factors (such as pharmacogenomics, comorbidity, life expectancy, stage of disease) and patients’ preferences. Within this framework, four main areas of overlap exist where a decision can be personalized. In categories A and C in figure 4, clinical decisions are personalized on the basis of clinical factors; for categories B and D, clinical decisions are personalized on the basis of patients’ preferences. Decision support is personalized when a decision aid or tool incorporates patients’ clinical characteristics and/or treatment preferences into the clinical decision making process. The systematic review found that, among 13 decision support tools, only three were designed to involve the patient in diabetes decision making.79 80 81 These tools attempted to elicit and incorporate patients’ preferences about the selection of treatments (category D79 81) and, in one case, the selection of management goals (category B80). In general, these tools improved patients’ knowledge, reduced decisional conflict, and increased patients’ involvement in decisions.
Fig 4.
Conceptual model of personalized decision support.
From this review, decision support interventions that encourage providers to consider both prognosis and preferences still seem to be rare.82 An example of integration of categories A and B decision support involved a web based decision support tool designed to encourage goal setting based on patients’ prognosis and treatment preferences. Unique features of this tool included a geriatric diabetes simulation model, to calculate life expectancy and complication rates, and formal elicitation of patients’ preferences.35 58
A pilot study at the University of Chicago clinics randomized physicians (n=28) and their patients (n=100) to the decision support tool, with a three to one recruitment ratio (75 intervention patients; 25 control patients). Before a clinic visit, intervention patients interacted with the tool, which generated a summary for their physician that included individual patients’ life expectancy estimates, treatment preferences, and screening results for geriatric conditions. Control patients received an educational HbA1c pamphlet. Ninety one per cent of intervention patients had their physician report that an HbA1c discussion took place during a visit compared with 76% for controls (P=0.19). Intervention patients had larger declines in the Informed Subscale of Decisional Conflict (−20.0 v 0; P=0.04). No significant differences were seen in proportions of patients with changes in goals (49% v 28%; P=0.08), although the proportion was higher in the intervention group. Most intervention patients reported that the tool was easy to use (91%) and helped them to communicate with their physician (84%).
Care management
In conjunction with personalized goal setting, provision of support for self care is important for improving clinical outcomes, as merely establishing goals is not sufficient for patients to achieve their goals.83 A randomized controlled trial evaluated whether assessment of barriers to self care and strategies to cope with these barriers, implemented telephonically by a diabetes educator, was superior to usual care with control for attention time.76 The intervention group received a model of care in which a geriatric diabetes team assessed barriers and developed strategies to help patients to cope with barriers. The program included tackling comorbid conditions of older patients such as cognitive impairment, depression, visual impairment, mobility/dexterity issues, and swallowing problems. The strategies were implemented via phone calls by a diabetes educator to the patients. The active intervention was implemented for the first six months, with a subsequent “no contact” follow-up period (total 12 months). The control group received equal amounts of attention time. After the active intervention period, HbA1c decreased by 0.45% in the intervention group compared with 0.31% in the attention control group. At 12 months, HbA1c decreased further in the intervention group by 0.21% compared with 0% in the control group (P<0.03). The intervention group showed additional statistically significant benefits in scores on measures of self care (Self-Care Inventory-R), gait and balance (Tinetti), and endurance (six minute walk test) compared with controls.
One potential approach to improve care and outcomes for older patients with diabetes is to enhance both goal setting and care management, using population management techniques at a clinic level. A clinic could potentially use the electronic medical record to establish goals of diabetes care with automated prognostic calculators using existing data on demographics, comorbidities, and functional impairments. The electronic medical record could also help to encourage clinics and physicians to document goals of diabetes care on an annual basis. These documented goals could influence subsequent treatment decisions and help to improve coordination of care among multiple providers. However, once goals are established for a population, additional support for some patients may be needed to help them to achieve their goals. Clinics could target specialized care management programs to those older patients not achieving their personal goals and at high risk for barriers to self care. In concert with these efforts, clinics could target care specialized management for older patients who may be over-treated and may benefit from de-intensification of care.
Conclusions
An important segment of the global obesity/diabetes epidemic is the growing population of older people with diabetes. Despite the considerable clinical and economic burden of this diabetes subpopulation, clinical trials have historically excluded the oldest patients and those with comorbidities. The major randomized controlled trials of intensive glucose control relevant to older patients indicate that treatment produces microvascular and cardiovascular benefits but typically after extended treatment periods (five to nine years) and with exposure to short term risks such as mortality (in one trial) and hypoglycemia. These trial data and complementary research from decision analysis, health economics, and observational studies have shaped contemporary clinical care guidelines. These guidelines almost all recommend that physicians and patients individualize the intensity of glucose control and treatments on the basis of the prognosis and preferences of older patients. Although general agreement exists on these broad concepts, very few studies have attempted to formally study them in clinical practice. Without formal study, the long term clinical effects of personalized goal setting and management will remain unknown.
To better meet the treatment needs of older patients with diabetes, more research is needed to determine the risks and benefits of intensifying, maintaining, or de-intensifying treatments in the oldest patients with multiple chronic illnesses. These risks and benefits may be altered by the availability of newer classes of glucose lowering agents (dipeptidyl peptidase 4 inhibitors, glucagon-like peptide 1 agonists, sodium-glucose co-transporter 2 inhibitors). Because of the challenges of conducting trials in older patients with multiple illnesses, shortened life expectancy, and/or cognitive impairment, both observational studies and controlled trials are needed to answer basic questions for this population. This research effort should extend to the development and study of decision support tools as well as targeted care management programs. The integration of both functions into clinical practice may improve health outcomes of this population.
Questions for further research
How can busy clinicians elicit patients’ preferences? Does eliciting patients’ preferences make a difference in outcomes?
How can busy clinicians stratify risk in older patients with diabetes mellitus? Does risk stratification make a difference in outcomes?
What are the clinical consequences of a comprehensive model of care that actively personalizes diabetes goals and treatments in older patients?
What are the clinical consequences of de-intensification of glucose lowering drugs in older, sicker patients?
How patients were involved
I consulted with two older patients with type 2 diabetes and multiple comorbid illnesses. One patient endorsed the recommendation that tackling geriatric syndromes and avoiding hypoglycemia should be given as high a priority as preventing diabetic complications in older adults with diabetes. This patient also identified the importance of frequent communication between patients, primary care physicians, and specialists. The second patient recommended that the article be shortened. Both patients strongly endorsed the concept of treating all patients with diabetes with individually designed treatment. I have incorporated the comments about clinical team communication into the section on emerging treatments, and I shortened the manuscript. Both patients reviewed the manuscript before submission.
Competing interests: I have read and understood the BMJ policy on declaration of interests and declare the following interests: none.
Provenance and peer review: Commissioned; externally peer reviewed.
References
- 1.Centers for Disease Control and Prevention. Rate per 100 of civilian, noninstitutionalized population with diagnosed diabetes, by age, United States, 1980–2014. 2015. http://www.cdc.gov/diabetes/statistics/prev/national/figbyage.htm.
- 2.Coca SG, Ismail-Beigi F, Haq N, Krumholz HM, Parikh CR. Role of intensive glucose control in development of renal end points in type 2 diabetes mellitus: systematic review and meta-analysis intensive glucose control in type 2 diabetes. Arch Intern Med 2012;172:761-9. 10.1001/archinternmed.2011.2230 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wilkinson MJ, Nathan AG, Huang ES. Personalized decision support in type 2 diabetes mellitus: current evidence and future directions. Curr Diab Rep 2013;13:205-12. 10.1007/s11892-012-0348-6 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Halter JB, Musi N, McFarland Horne F, et al. Diabetes and cardiovascular disease in older adults: current status and future directions. Diabetes 2014;63:2578-89. 10.2337/db14-0020 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ray KK, Seshasai SR, Wijesuriya S, et al. Effect of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes mellitus: a meta-analysis of randomised controlled trials. Lancet 2009;373:1765-72. 10.1016/S0140-6736(09)60697-8 . [DOI] [PubMed] [Google Scholar]
- 6.Brown AF, Mangione CM, Saliba D, Sarkisian CA. California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes. Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc 2003;51(Suppl Guidelines):S265-80. 10.1046/j.1532-5415.51.5s.1.x . [DOI] [PubMed] [Google Scholar]
- 7.Moreno G, Mangione CM, Kimbro L, Vaisberg E. American Geriatrics Society Expert Panel on Care of Older Adults with Diabetes Mellitus. Guidelines abstracted from the American Geriatrics Society Guidelines for Improving the Care of Older Adults with Diabetes Mellitus: 2013 update. J Am Geriatr Soc 2013;61:2020-6. 10.1111/jgs.12514 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kirkman MS, Briscoe VJ, Clark N, et al. Diabetes in older adults. Diabetes Care 2012;35:2650-64. 10.2337/dc12-1801 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sinclair AJ, Paolisso G, Castro M, Bourdel-Marchasson I, Gadsby R, Rodriguez Mañas L. European Diabetes Working Party for Older People. European Diabetes Working Party for Older People 2011 clinical guidelines for type 2 diabetes mellitus. Executive summary. Diabetes Metab 2011;37(Suppl 3):S27-38. 10.1016/S1262-3636(11)70962-4 . [DOI] [PubMed] [Google Scholar]
- 10.Selvin E, Coresh J, Brancati FL. The burden and treatment of diabetes in elderly individuals in the u.s. Diabetes Care 2006;29:2415-9. 10.2337/dc06-1058 . [DOI] [PubMed] [Google Scholar]
- 11. Centers for Disease Control and Prevention. National Diabetes Statistics Report: estimates of diabetes and its burden in the United States, 2014.US Department of Health and Human Services, 2014. [Google Scholar]
- 12.Morley JE. The elderly Type 2 diabetic patient: special considerations. Diabet Med 1998;15(Suppl 4):S41-6. 10.1002/(SICI)1096-9136(1998120)15:4+<S41::AID-DIA747>3.3.CO;2-5 . [DOI] [PubMed] [Google Scholar]
- 13.Laiteerapong N, Karter AJ, Liu JY, et al. Correlates of quality of life in older adults with diabetes: the diabetes & aging study. Diabetes Care 2011;34:1749-53. 10.2337/dc10-2424 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Amati F, Dubé JJ, Coen PM, Stefanovic-Racic M, Toledo FG, Goodpaster BH. Physical inactivity and obesity underlie the insulin resistance of aging. Diabetes Care 2009;32:1547-9. 10.2337/dc09-0267 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Huang ES, Basu A, O’Grady M, Capretta JC. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care 2009;32:2225-9. 10.2337/dc09-0459 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. International Diabetes Federation. IDF diabetes atlas. 7th ed International Diabetes Federation, 2015. [Google Scholar]
- 17.Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci 2004;59:255-63. 10.1093/gerona/59.3.M255 . [DOI] [PubMed] [Google Scholar]
- 18.Druss BG, Marcus SC, Olfson M, Tanielian T, Elinson L, Pincus HA. Comparing the national economic burden of five chronic conditions. Health Aff (Millwood) 2001;20:233-41. 10.1377/hlthaff.20.6.233 . [DOI] [PubMed] [Google Scholar]
- 19.Lee PG, Cigolle C, Blaum C. The co-occurrence of chronic diseases and geriatric syndromes: the health and retirement study. J Am Geriatr Soc 2009;57:511-6. 10.1111/j.1532-5415.2008.02150.x . [DOI] [PubMed] [Google Scholar]
- 20.Schneider KM, O’Donnell BE, Dean D. Prevalence of multiple chronic conditions in the United States’ Medicare population. Health Qual Life Outcomes 2009;7:82. 10.1186/1477-7525-7-82 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med 2002;162:2269-76. 10.1001/archinte.162.20.2269 . [DOI] [PubMed] [Google Scholar]
- 22.Vincent GK, Velkoff VA. The next four decades, the older population in the United States: 2010 to 2050.US Census Bureau, 2010. [Google Scholar]
- 23.Preis SR, Hwang SJ, Coady S, et al. Trends in all-cause and cardiovascular disease mortality among women and men with and without diabetes mellitus in the Framingham Heart Study, 1950 to 2005. Circulation 2009;119:1728-35. 10.1161/CIRCULATIONAHA.108.829176 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Xu J, Kochanek KD, Murphy SL, Tejada-Vera B. Deaths: final data for 2007. Natl Vital Stat Rep 2010;58 (19):1-19.. [PubMed] [Google Scholar]
- 25.Tierney EF, Cadwell BL, Engelgau MM, et al. Declining mortality rate among people with diabetes in North Dakota, 1997-2002. Diabetes Care 2004;27:2723-5. 10.2337/diacare.27.11.2723 . [DOI] [PubMed] [Google Scholar]
- 26.Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303:235-41. 10.1001/jama.2009.2014 . [DOI] [PubMed] [Google Scholar]
- 27.Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA 2005;294:716-24. 10.1001/jama.294.6.716 . [DOI] [PubMed] [Google Scholar]
- 28.Laiteerapong N, Iveniuk J, John PM, Laumann EO, Huang ES. Classification of older adults who have diabetes by comorbid conditions, United States, 2005-2006. Prev Chronic Dis 2012;9:E100.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Blaum C, Cigolle CT, Boyd C, et al. Clinical complexity in middle-aged and older adults with diabetes: the Health and Retirement Study. Med Care 2010;48:327-34. 10.1097/MLR.0b013e3181ca4035 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cigolle CT, Kabeto MU, Lee PG, Blaum CS. Clinical complexity and mortality in middle-aged and older adults with diabetes. J Gerontol A Biol Sci Med Sci 2012;67:1313-20. 10.1093/gerona/gls095 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373-83. 10.1016/0021-9681(87)90171-8 . [DOI] [PubMed] [Google Scholar]
- 32.Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 1992;45:613-9. 10.1016/0895-4356(92)90133-8 . [DOI] [PubMed] [Google Scholar]
- 33.Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care 1998;36:8-27. 10.1097/00005650-199801000-00004 . [DOI] [PubMed] [Google Scholar]
- 34.Litwin MS, Greenfield S, Elkin EP, Lubeck DP, Broering JM, Kaplan SH. Assessment of prognosis with the total illness burden index for prostate cancer: aiding clinicians in treatment choice. Cancer 2007;109:1777-83. 10.1002/cncr.22615 . [DOI] [PubMed] [Google Scholar]
- 35.Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006;295:801-8. 10.1001/jama.295.7.801 . [DOI] [PubMed] [Google Scholar]
- 36.Yourman LC, Lee SJ, Schonberg MA, Widera EW, Smith AK. Prognostic indices for older adults: a systematic review. JAMA 2012;307:182-92. 10.1001/jama.2011.1966 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Fried LP, Tangen CM, Walston J, et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001;56:M146-56. 10.1093/gerona/56.3.M146 . [DOI] [PubMed] [Google Scholar]
- 38.Saunders C, Byrne CD, Guthrie B, et al. Scottish Diabetes Research Network Epidemiology Group. External validity of randomized controlled trials of glycaemic control and vascular disease: how representative are participants?Diabet Med 2013;30:300-8. 10.1111/dme.12047 . [DOI] [PubMed] [Google Scholar]
- 39. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53. 10.1016/S0140-6736(98)07019-6 . [DOI] [PubMed] [Google Scholar]
- 40.Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008;359:1577-89. 10.1056/NEJMoa0806470 . [DOI] [PubMed] [Google Scholar]
- 41.Gerstein HC, Miller ME, Byington RP, et al. Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008;358:2545-59. 10.1056/NEJMoa0802743 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Patel A, MacMahon S, Chalmers J, et al. ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560-72. 10.1056/NEJMoa0802987 . [DOI] [PubMed] [Google Scholar]
- 43.Zoungas S, Chalmers J, Neal B, et al. ADVANCE-ON Collaborative Group. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med 2014;371:1392-406. 10.1056/NEJMoa1407963 . [DOI] [PubMed] [Google Scholar]
- 44.Duckworth W, Abraira C, Moritz T, et al. VADT Investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 2009;360:129-39. 10.1056/NEJMoa0808431 . [DOI] [PubMed] [Google Scholar]
- 45.Hayward RA, Reaven PD, Wiitala WL, et al. VADT Investigators. Follow-up of glycemic control and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015;372:2197-206. 10.1056/NEJMoa1414266 . [DOI] [PubMed] [Google Scholar]
- 46. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53. 10.1016/S0140-6736(98)07019-6 . [DOI] [PubMed] [Google Scholar]
- 47. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998;352:854-65. 10.1016/S0140-6736(98)07037-8 . [DOI] [PubMed] [Google Scholar]
- 48.Gerstein HC, Miller ME, Genuth S, et al. ACCORD Study Group. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med 2011;364:818-28. 10.1056/NEJMoa1006524 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Miller ME, Williamson JD, Gerstein HC, et al. ACCORD Investigators. Effects of randomization to intensive glucose control on adverse events, cardiovascular disease, and mortality in older versus younger adults in the ACCORD Trial. Diabetes Care 2014;37:634-43. 10.2337/dc13-1545 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Moritz T, Duckworth W, Abraira C. Veterans Affairs diabetes trial--corrections. N Engl J Med 2009;361:1024-5. 10.1056/NEJMc096250 . [DOI] [PubMed] [Google Scholar]
- 51.Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008;358:580-91. 10.1056/NEJMoa0706245 . [DOI] [PubMed] [Google Scholar]
- 52.Araki A, Iimuro S, Sakurai T, et al. Japanese Elderly Diabetes Intervention Trial Study Group. Long-term multiple risk factor interventions in Japanese elderly diabetic patients: the Japanese Elderly Diabetes Intervention Trial--study design, baseline characteristics and effects of intervention. Geriatr Gerontol Int 2012;12(Suppl 1):7-17. 10.1111/j.1447-0594.2011.00808.x . [DOI] [PubMed] [Google Scholar]
- 53.Rutter CM, Zaslavsky AM, Feuer EJ. Dynamic microsimulation models for health outcomes: a review. Med Decis Making 2011;31:10-8. 10.1177/0272989X10369005 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Clarke PM, Gray AM, Briggs A, et al. UK Prospective Diabetes Study (UKDPS) Group. A model to estimate the lifetime health outcomes of patients with type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004;47:1747-59. 10.1007/s00125-004-1527-z . [DOI] [PubMed] [Google Scholar]
- 55. CDC Diabetes Cost-effectiveness Group. Cost-effectiveness of intensive glycemic control, intensified hypertension control, and serum cholesterol level reduction for type 2 diabetes. JAMA 2002;287:2542-51. 10.1001/jama.287.19.2542 . [DOI] [PubMed] [Google Scholar]
- 56.Schlessinger L, Eddy DM. Archimedes: a new model for simulating health care systems--the mathematical formulation. J Biomed Inform 2002;35:37-50. 10.1016/S1532-0464(02)00006-0 . [DOI] [PubMed] [Google Scholar]
- 57.Zhou H, Isaman DJ, Messinger S, et al. A computer simulation model of diabetes progression, quality of life, and cost. Diabetes Care 2005;28:2856-63. 10.2337/diacare.28.12.2856 . [DOI] [PubMed] [Google Scholar]
- 58.Huang ES, Zhang Q, Gandra N, Chin MH, Meltzer DO. The effect of comorbid illness and functional status on the expected benefits of intensive glucose control in older patients with type 2 diabetes: a decision analysis. Ann Intern Med 2008;149:11-9. 10.7326/0003-4819-149-1-200807010-00005 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Greenfield S, Billimek J, Pellegrini F, et al. Comorbidity affects the relationship between glycemic control and cardiovascular outcomes in diabetes: a cohort study. Ann Intern Med 2009;151:854-60. 10.7326/0003-4819-151-12-200912150-00005 . [DOI] [PubMed] [Google Scholar]
- 60. Working Group on Health Outcomes for Older Persons with Multiple Chronic Conditions. Universal health outcome measures for older persons with multiple chronic conditions. J Am Geriatr Soc 2012;60:2333-41. 10.1111/j.1532-5415.2012.04240.x . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Gandhi GY, Murad MH, Fujiyoshi A, et al. Patient-important outcomes in registered diabetes trials. JAMA 2008;299:2543-9. 10.1001/jama.299.21.2543 . [DOI] [PubMed] [Google Scholar]
- 62.Biessels GJ, Staekenborg S, Brunner E, Brayne C, Scheltens P. Risk of dementia in diabetes mellitus: a systematic review. Lancet Neurol 2006;5:64-74. 10.1016/S1474-4422(05)70284-2 . [DOI] [PubMed] [Google Scholar]
- 63.Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Diabetes Care 2013;36:1384-95. 10.2337/dc12-2480 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tseng CL, Soroka O, Maney M, Aron DC, Pogach LM. Assessing potential glycemic overtreatment in persons at hypoglycemic risk. JAMA Intern Med 2014;174:259-68. 10.1001/jamainternmed.2013.12963 . [DOI] [PubMed] [Google Scholar]
- 65.Huang ES, Laiteerapong N, Liu JY, John PM, Moffet HH, Karter AJ. Rates of complications and mortality in older patients with diabetes mellitus: the diabetes and aging study. JAMA Intern Med 2014;174:251-8. 10.1001/jamainternmed.2013.12956 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Huang ES, Shook M, Jin L, Chin MH, Meltzer DO. The impact of patient preferences on the cost-effectiveness of intensive glucose control in older patients with new-onset diabetes. Diabetes Care 2006;29:259-64. 10.2337/diacare.29.02.06.dc05-1443 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Vijan S, Sussman JB, Yudkin JS, Hayward RA. Effect of patients’ risks and preferences on health gains with plasma glucose level lowering in type 2 diabetes mellitus. JAMA Intern Med 2014;174:1227-34. 10.1001/jamainternmed.2014.2894 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Moreno G, Mangione CM. Management of cardiovascular disease risk factors in older adults with type 2 diabetes mellitus: 2002-2012 literature review. J Am Geriatr Soc 2013;61:2027-37. 10.1111/jgs.12513 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.US Department of Veterans Affairs. VA/DOD clinical practice guidelines: management of diabetes mellitus in primary care (2010), 2010. http://www.healthquality.va.gov/guidelines/CD/diabetes/.
- 70.Sinclair AJ, Paolisso G, Castro M, Bourdel-Marchasson I, Gadsby R, Rodriguez Mañas L. European Diabetes Working Party for Older People. European Diabetes Working Party for Older People 2011 clinical guidelines for type 2 diabetes mellitus. Executive summary. Diabetes Metab 2011;37(Suppl 3):S27-38. 10.1016/S1262-3636(11)70962-4 . [DOI] [PubMed] [Google Scholar]
- 71. American Diabetes Association. Standards of medical care in diabetes--2014[Is there an author for this?]. Diabetes Care 2014;37(Suppl 1):S14-80. 10.2337/dc14-S014 . [DOI] [PubMed] [Google Scholar]
- 72.Lipska KJ, Ross JS, Miao Y, Shah ND, Lee SJ, Steinman MA. Potential overtreatment of diabetes mellitus in older adults with tight glycemic control. JAMA Intern Med 2015;175:356-62. 10.1001/jamainternmed.2014.7345 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Thorpe CT, Gellad WF, Good CB, et al. Tight glycemic control and use of hypoglycemic medications in older veterans with type 2 diabetes and comorbid dementia. Diabetes Care 2015;38:588-95.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Lipska KJ, Ross JS, Miao Y, Shah ND, Lee SJ, Steinman MA. Potential overtreatment of diabetes mellitus in older adults with tight glycemic control. JAMA Intern Med 2015;175:356-62. 10.1001/jamainternmed.2014.7345 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Naik AD, Palmer N, Petersen NJ, et al. Comparative effectiveness of goal setting in diabetes mellitus group clinics: randomized clinical trial. Arch Intern Med 2011;171:453-9. 10.1001/archinternmed.2011.70 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Munshi MN, Segal AR, Suhl E, et al. Assessment of barriers to improve diabetes management in older adults: a randomized controlled study. Diabetes Care 2013;36:543-9. 10.2337/dc12-1303 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Christakis NA. Death foretold: prophecy and prognosis in medical care.University of Chicago, 1999. [Google Scholar]
- 78.Silveira MJ, Wiitala W, Piette J. Advance directive completion by elderly Americans: a decade of change. J Am Geriatr Soc 2014;62:706-10. 10.1111/jgs.12736 . [DOI] [PubMed] [Google Scholar]
- 79.Mullan RJ, Montori VM, Shah ND, et al. The diabetes mellitus medication choice decision aid: a randomized trial. Arch Intern Med 2009;169:1560-8. 10.1001/archinternmed.2009.293 . [DOI] [PubMed] [Google Scholar]
- 80.Corser W, Holmes-Rovner M, Lein C, Gossain V. A shared decision-making primary care intervention for type 2 diabetes. Diabetes Educ 2007;33:700-8. 10.1177/0145721707304086 . [DOI] [PubMed] [Google Scholar]
- 81.Weymiller AJ, Montori VM, Jones LA, et al. Helping patients with type 2 diabetes mellitus make treatment decisions: statin choice randomized trial. Arch Intern Med 2007;167:1076-82. 10.1001/archinte.167.10.1076 . [DOI] [PubMed] [Google Scholar]
- 82.Huang ES, Nathan AG, Cooper J, et al. A pilot RCT of personalized decision support for older patients with diabetes. Diabetes 2013;62(suppl 1):336..23349538 [Google Scholar]
- 83.Denig P, Schuling J, Haaijer-Ruskamp F, Voorham J. Effects of a patient oriented decision aid for prioritising treatment goals in diabetes: pragmatic randomised controlled trial. BMJ 2014;349:g5651. 10.1136/bmj.g5651 . [DOI] [PubMed] [Google Scholar]