

Abstract
Using latent profile analysis (LPA), this study empirically identified dual-factor mental health subtypes, with a goal of examining structural stability of emerging latent classes over three high school years. Profiles’ relations with distal indicators of well-being, psychosocial distress, and self-reported grades were examined to explore the validity of emerging classes. A sample of 332 high school students reported on their social-emotional strengths and psychological distress during the fall term of their ninth-, tenth-, and eleventh-grade years. In Grade 12, students reported on measures assessing their grades and social-emotional experiences. Independent LPAs for each grade year yielded four mental health subtypes – complete mental health, moderately mentally healthy, symptomatic but content, and troubled – and provided evidence for the structural stability of the dual-factor mental health construct. Across high school years, most students were in the complete or moderately mentally healthy classes, with the troubled class consistently representing the smallest proportion of the sample. Students in classes with higher levels of strengths and lower levels of distress reported higher grades, prosocial contribution to community, and higher life satisfaction, and fewer symptoms of anxiety and depression. Implications and future directions for research and school-based practice are discussed.
Keywords: dual-factor mental health, adolescents, classification, latent profile analysis (LPA)
An approach to universal screening, complete mental health screening (You et al., 2014), offers a comprehensive picture of youth’s mental health functioning by assessing youth’s wellness and distress. This approach is based on dual-factor (Suldo & Shaffer, 2008) or two-continua (Westerhof & Keyes, 2010) models that consider psychological distress and social-emotional wellness as separate, yet related dimensions. The empirical literature substantiating a dual-factor model has most often relied on predetermined decision points when forming mental health groups that vary along indicators of distress and wellness (Kim, Dowdy, Furlong, & You, 2017). However, limitations associated with the use of rational cut-score approaches to classification call for the exploration of alternative approaches (Kim et al., 2017). The aims of the current study are to: (a) explore an empirically based, latent profile approach to complete mental health classification; (b) investigate the structural stability of emerging groups over three years; and (c) explore the validity of emerging mental health groups via examining the relation of the empirically derived groups to self-reported grades and social-emotional outcomes.
Defining Complete Mental Health
Mental health is often defined as a bipolar dimension with mental health and mental illness on opposite ends of one continuum (e.g., Greenspoon & Saklofske, 2001). This model conceptualizes mental health in relation to mental illness, such that mental illness indicates the presence of emotional or behavioral distress or psychological disorder (e.g., as defined using the Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association, 2013), whereas mental health implies an absence of these conditions (e.g., Keyes, 2005). However, definitions of mental health are shifting to emphasize positive health indicators, including subjective well-being and social emotional assets (e.g., Scales 1999). For example, the World Health Organization defines mental health as, “a state of well-being in which every individual realizes his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her or his community” (2016). Contemporary mental health models that simultaneously consider psychosocial distress and wellness have emerged as an alternative to traditional bipolar models. These dual-factor or two-continua models propose that mental wellness and mental illness comprise separate continua, with levels of both wellness and distress varying within an individual. In these models, logically defined groups are formed based on responses to wellness and distress measures (Antaramian Huebner, Hills, & Valois, 2010), with youth who are described to have complete mental health exhibiting higher levels of well-being and lower levels of distress (Moore et al., 2015). In this paper, the term “mental health” is used to refer to an individual’s general psychological state of well-being, encompassing both their degree of mental health and degree of mental illness. The term “complete mental health” refers specifically to a dual-factor or two-continua model of mental health that calls direct attention to well-being and psychological distress. Specifically, individuals with complete mental health have high levels of strengths and low levels of distress.
The dual-factor, complete mental health model has been supported for use with children (Greenspoon & Saklofske, 2001) and adolescents in middle (Antaramian et al., 2010; Suldo & Shaffer, 2008) and high school (Suldo, Thalji-Raitano, Kiefer, & Ferron, 2016). Although the tools used to define complete mental health and the constructs of well-being and distress have varied across empirical investigations, similar trends have emerged in the relation of dual-factor mental health groups to outcomes of interest. For example, adolescents with complete mental health have been found to have superior school engagement, academic achievement, school attendance, social relationships and functioning, physical health, and identity development (Lyons, Huebner, & Hills, 2013; Suldo et al., 2016). Moreover, among youth who experience distress, the presence of well-being has a buffering effect on outcomes. Despite findings of differential functioning based upon dual-factor mental health group membership, the criteria used to form dual-factor mental health groups are not a settled matter because cut points are researcher defined and vary across studies. Thus, a primary goal of this study was to explore an alternative, person-centered empirical classification approach that allows groups to emerge based upon similarities among members within a sample. An empirical approach lends itself to cross-study standardization (Masyn, 2013) and could refine the understanding of the characteristics of adolescent dual-factor mental health groups (Nylund, Bellmore, Nishina, & Graham, 2007).
Classification of Complete Mental Health
The majority of research on dual-factor mental health has classified individuals based upon a rationally formed dichotomous categorization scheme for each of the well-being and distress dimensions (e.g., Kim et al., 2017). That is, cut points are specified to distinguish individuals who are considered to be experiencing high versus low levels of well-being and distress. Using a dichotomous cut-score approach to classification, four mental health groups are logically formed across all investigations (e.g., Greenspoon & Saklofske, 2001; Lyons et al., 2012; Venning, Wilson, Kettler, & Eliott, 2013) and include groups of individuals with (a) high well-being and low distress (e.g., complete mental health), (b) high well-being and high distress (e.g., symptomatic but content), (c) low well-being and low distress (e.g., vulnerable or languishing), and (d) low well-being and high distress (e.g., troubled). A variety of criteria have been used for categorization based upon differing cut points. For example, some research used established decision points for norm-referenced measures (e.g., T-scores of 60 and above to indicate elevated risk), whereas others used values based upon individuals’ raw scores, sample means, or standardized scores (Kim et al., 2017). Others have used predetermined criteria in selecting raw- or mean-score cut points (e.g., such that 30% of the sample is classified as having low well-being; e.g., Antaramian et al., 2010; Suldo & Shaffer, 2008). Assigning youth to either high or low well-being and high or low distress categories forms the four mental health groups.
Although the cut score approach forms unique mental health groups, the resulting membership in the four groups is just one of many possible group assignments that are dependent upon the number of cut points selected and the criteria used. An inherent disadvantage of this approach to classification is that most often there are no clear criteria regarding where to set cut points or if four groups is the optimal number of groups (e.g., Nylund Asparouhov, & Muthén, 2007). Classification via the cut score approach can be insensitive to the degree of variation in mental health among youth (Kim et al., 2017). For example, when dichotomous classification criteria are specified such that youth scoring above the 30th percentile on a well-being measure are indicated to have high well-being, individuals exhibiting moderate levels of well-being (e.g., 40th percentile) are regarded as having similar levels of well-being as those individuals with the highest levels of well-being (e.g., 90th percentile; Kim et al., 2017). As such, the mental health groups formed are treated as homogenous when they have substantial heterogeneity, which incompletely captures the complexity of youths’ mental health experiences.
Additionally, when sample-dependent criteria are used across studies, an individual classified into one mental health group when one set of criteria are used, may be in a different group when using another set of criteria; hence, replication is problematic. For example, considering the four complete mental health groups, the majority of adolescents have been classified as experiencing complete mental health [42% (Venning et al., 2013) to 64% (Lyons et al., 2012)], followed by symptomatic but content [9% (Lyons et al., 2012) to 36% (Venning et al., 2013)], troubled [8% (Antaramian et al., 2010) to 20% (Lyons et al., 2012)], and languishing [5% (Venning et al., 2013) to 13% (Suldo & Shaffer, 2008)]. The observed differences in the proportion of youth who are classified into each mental health group within each study’s sample might be an artifact of sample-specific characteristics; however, they could also indicate disparities in classification that are observed when criteria used to classify individuals’ mental health vary across investigations. A person-centered, empirical approach to classification that identifies groups (i.e., latent classes or profiles) based upon individual observed response pattern provides an alternative approach for identifying emerging groups (Nylund et al., 2007b).
Latent Profile Analysis: Person-Centered Approach to Classification
Latent profile analysis (LPA) is a person-centered, empirical approach to classifying the heterogeneity within groups of people (Masyn, 2013; Vermunt, 2004). LPA identifies differences and similarities among individuals with respect to how variables measuring constructs of interest are related to each other. LPA is performed in an exploratory manner and assumes that the underlying population is heterogeneous but also that the population consists of a finite number of meaningful, more homogenous groups (Laursen & Hoff, 2006; Masyn, 2013). A categorical latent variable, indicative of group membership, is specified to identify unobserved (latent) groups (also called classes or profiles) based upon similarities in their response patterns across indicators. Through a model building process wherein numerous models specify increasingly more classes, statistical criteria are used to evaluate the resulting models and to decide on the number of latent groups. Rather than predetermining the number of groups to be formed using cut points, LPA allows for meaningful classes to be empirically identified, and then evaluated for accuracy and validity. Thus, when well-being and distress are examined concurrently, LPA allows for groups to emerge that may differ in both dimension (i.e., presence of well-being but absence of distress) and relative severity (i.e., varying levels of well-being and/or distress).
Two previous studies (Kim et al., 2017; Rebelez-Ernst, 2015) examined dual-factor mental health using an LPA approach to classification. In each study, separate latent class models were specified for social-emotional strengths and psychological distress, with classes from the best-fitting strength and distress models being cross-tabulated to form complete mental health groups. Kim and colleagues (2017) identified five profiles of strengths and three profiles of distress whereas Rebelez-Ernst (2015) identified four profiles of strengths and four profiles of distress. When the emerging strength and distress profiles were cross-tabulated, Kim et al. (2017) and Rebelez-Ernst (2015) identified 15 and 16 complete mental health groups, respectively. However, when examining the proportion of students in each of these samples in each emerging mental health group, many of the emerging groups described fewer than 5% of the study’s participants, calling into question the practicality of each group for informing prevention or intervention efforts. In addition, although these previous LPA investigations examined both positive and negative indicators of mental health using a dual-factor approach, adolescents’ characteristics on each element of mental health were considered separately and then cross-tabulated to form the final groups, as has been done with the traditional cut score classification approach. Research examining parsimonious approaches to LPA classification, specifying models that examine well-being and distress simultaneously, is needed to better inform use of data to identify youths’ mental health subtypes. Research investigating whether the number of emerging mental health groups is consistent over time (i.e., structural stability) is also needed.
Study Aims
LPA was used to empirically define complete mental health groups assessed via universal screening data. Across three years, adolescents reported on their social-emotional strengths and psychological distress. LPAs performed for adolescents in each of Grades 9–11 were designed to examine whether patterns in dual-factor mental health were consistent at different points. Research that empirically identifies dual-factor mental health groups is limited; there are only a few investigations that examined emerging classes and these examinations were cross-sectional (e.g., Kim et al., 2017). Thus, the repeated LPAs of this study are intended to provide important information about the nature of empirically derived dual-factor mental health groups within the high school period, including whether the observed dual-factor mental health construct emerges similarly (i.e., consistent number of groups, consistent characteristics or structure of groups) with repeated measurements within this developmental period. Given the exploratory nature of LPAs, no hypotheses were specified a priori regarding the number and characteristics of emerging mental health groups. However, similar dual-factor mental health groups emerging over each grade year would provide information about the nature of dual-factor mental health in high school students in addition to providing preliminary validation evidence for empirically-derived, person-centered dual-factor mental health. Thus, the LPAs that are the focus of this study were intended to examine whether dual-factor mental health profiles are consistent at different time points during high school (i.e., structural stability), and were not designed to track changes in individual students’ mental health group membership over time. Finally, the current study sought to examine the validity of emerging classes via exploring the relation of group membership with later self-reported grades and social-emotional outcomes. In particular, the relation between adolescents’ mental health class in each of Grades 9–11 with Grade 12 self-reported grades and positive and negative social-emotional outcomes was explored. Thus, the present study seeks to contribute to the youth mental health literature by (a) identifying subtypes of dual-factor mental health using an empirically derived latent class approach to classification, (b) examining the structural stability of these classes at three different time points across three years of high school, and (c) assessing how empirically derived mental health classes predict Grade 12 self-reports of grades and social-emotional outcomes.
Method
Participants
Participants attended one high school in central California that participated in an ongoing screening project occurring over four consecutive years. Participants for this study first completed the study survey as ninth graders and annually thereafter. Of the 497 students who completed the Grade 9 survey, 334 (67%) had parent consent and youth assent to complete the Grade 12 survey. Individuals who had at least three years of data across the four possible years when the survey was conducted were included in the present analyses (N = 332). Two students who completed only the Grade 9 and Grade 12 surveys were excluded from these analyses. Using these criteria, the final sample for each year was: 332 (Grade 9), 324 (Grade 10), and 291 (Grade 11). Information obtained from students’ archival school records in Grade 9 indicated that the participating sample was 48.5% female, 43.9% Latinx or Hispanic, 37.9% non-Hispanic White, 7.5% Asian or Pacific Islander, 1.2% African American, and 0.9% American Indian or Alaska Native. Race or ethnicity information was unavailable for 8.4% of the participants. In the current study, 47.3% of students were classified as socioeconomically disadvantaged and 8.4% were eligible to receive special education services. No significant differences with respect to these demographic characteristics were observed between participants included in the final sample and those who were not included due to attrition (χ2 > .05).
Procedures
Each year, for four consecutive years, all students in Grades 9–12 were invited to participate in universal screening. During the first month of each academic year, following approval by the university’s institutional review board, district approval, passive parental consent, and youth assent, school personnel administered the screening surveys to participating students in a group format during one period of a regular school day. The screening survey included all self-report measures. Administration scripts were provided to all classroom teachers.
Data were collected in the fall semester of 2013–2014 (Grade 9), 2014–2015 (Grade 10), 2015–2016 (Grade 11), and 2016–2017 (Grade 12). Students completed a survey electronically via an online format during Grades 9, 11, and 12. At the request of the school’s administration, surveys were completed using paper-and-pencil format during Grade 10 data collection. Each year, within the two weeks following initial data collection, students who were absent on their class’s initial screening day were provided with up to five additional opportunities to complete the survey. During the fall of Grades 9–11, the well-being and distress measures used in the LPAs were administered. In order to examine the validity of students’ emerging complete mental health class, five additional self-report measures of grades or social-emotional outcomes were administered concurrently with the screening survey, in the first month of Grade 12.
Measures
The following section provides a summary of the measures used in this study. Table 1 shows the alpha internal consistency coefficients and the item response range for each measure.
Table 1.
Measures Mean Item Response and Standard Deviations of Mental Health Indicators and Outcomes
| Grade 9 |
Grade 10 |
Grade 11 |
Grade 12 |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Score Range1 |
α2 | M | SD | M | SD | M | SD | M | SD | |
| SEHS-S (Grades 9–11) | ||||||||||
| Belief in Self | 1–4 | .76–.81 | 2.87 | 0.50 | 3.05 | 0.44 | 3.04 | 0.53 | — | — |
| Belief in Others | 1–4 | .80–.87 | 3.14 | 0.56 | 3.34 | 0.50 | 3.29 | 0.59 | — | — |
| Emotional Competence | 1–4 | .78–.84 | 2.98 | 0.48 | 3.22 | 0.44 | 3.24 | 0.49 | — | — |
| Engaged Living | 1–4.673 | .86–.91 | 3.31 | 0.68 | 3.39 | 0.60 | 3.36 | 0.68 | — | — |
|
SDQ (Grades 9–11) | ||||||||||
| Internalizing | 1–3 | .67–.75 | 1.64 | 0.44 | 1.51 | 0.42 | 1.57 | 0.48 | — | — |
| Externalizing | 1–3 | .55–.67 | 1.72 | 0.42 | 1.50 | 0.45 | 1.45 | 0.45 | — | — |
|
Psychosocial Outcomes (Grade 12) | ||||||||||
| Prosocial Contribution | 1–6 | .91 | — | — | — | — | — | — | 4.66 | 0.99 |
| Life Satisfaction | 1–5 | .80 | — | — | — | — | — | — | 4.97 | 0.85 |
| Depression symptoms | 1–4 | .87 | — | — | — | — | — | — | 1.58 | 0.59 |
| Anxiety symptoms | 1–4 | .90 | — | — | — | — | — | — | 1.57 | 0.68 |
| Self-reported grades | 1–8 | — | — | — | — | — | — | — | 6.44 | 1.53 |
Note. SEHS-S = Social Emotional Health Survey – Secondary; SDQ = Strengths and Difficulties Questionnaire. Contribution = Contribution to Community subscale of the Positive Youth Development Inventory. Life Satisfaction = Brief Multidimensional Students’ Life Satisfaction Scale. Depression symptoms = Patient Health Questionnaire. Anxiety symptoms = Generalized Anxiety Disorder Scale. Course grades = Self-reported past year grades 1 = mostly F’s 6 = mostly B’s…8 = Mostly A’s. See online supplemental material for additional measure information.
Item response range for each measure.
SEHS-S and SDQ reliabilities show the range across Grade 9, 10, and 11 administrations. Other reliabilities are for measures administered in Grade 12.
The Engaged Living domain is the combination of gratitude (item response range = 1–4), zest (item response range = 1–5), and optimism (item response range = 1–5).
Complete mental health measures
Social Emotional Health Survey-Secondary (SEHS-S)
The 36-item SEHS-S (You et al., 2014) assesses four positive mental health domains each comprised of three strength dispositions: belief-in-self (comprised of self-efficacy, self-awareness, persistence), belief-in-others (school support, peer support, family coherence), emotional competence (emotional regulation, empathy, self-control), and engaged living (optimism, gratitude, zest). Students responded to statements related to their social-emotional functioning using an ordinal-response scale. On the gratitude and zest subscales, a 5-point response scale is used (1 = not at all, 2 = very little, 3 = somewhat, 4 = quite a lot, 5 = extremely). For each of the other ten dispositions, adolescents indicated how true each statement is for them (1 = not at all true of me, 2 = a little true of me, 3 = pretty much true of me, 4 = very much true of me). Mean scores for the four belief-in-self, belief-in-others, emotional competence, engaged living domains were computed and used as indicators of well-being for each year of data collection and used in the LPAs.
Strengths and Difficulties Questionnaire (SDQ)
The SDQ is a 25-item self-report measure of youths’ behavior and feelings (past six months; Goodman, 1997). Respondents use a three-point response scale (1 = not true, 2 = somewhat true, 3 = certainly true). A three-factor structure (emotional distress/withdrawal, behavioral reactivity/conduct problems, and prosocial behaviors/peer competence; Ruchkin, Jones, Vermeiren, & Schwab-Stone, 2008) supports better reliability estimates over the original five SDQ factors (Goodman, 1997). The five highest loading items in the Ruchkin et al. (2008) study, were used for emotional distress/withdrawal (items 3, 6, 8, 13 and 16; λ = .47 to .60) and behavioral reactivity/conduct problems (items 2, 5, 10, 15, and 22; λ = .56 to .62; contact first author for additional information). Mean internalizing (i.e., emotional distress/withdrawal items) and externalizing (i.e., behavioral reactivity/conduct problems items) scores for each year were used as indicators in the LPAs.
Grade 12 psychosocial outcomes
Self-reported grades
Adolescents reported on their grades over the previous 12 months via one item from the California Healthy Kids Survey (“During the past 12 months, how would you describe the grades you mostly received in school?”; California Department of Education, n.d.). Students used an eight-point response scale (1 = mostly F’s … 8 = mostly A’s). Self-reported grades are often used (Kuncel, Credé, & Thomas, 2005) with some research showing their acceptable reliability for high school students (Sticca et al., 2017) and other research indicating that these data are to be interpreted with caution (Kuncel et al., 2005).
Brief Multidimensional Students’ Life Satisfaction Scale (BMSLSS)
The BMSLSS has five items measuring five domains of life satisfaction (friends, family, self, school, and living environment; Seligson, Huebner, & Valois, 2003). The BMSLSS scores have acceptable convergent validity with other life satisfaction measures and positive affect (Seligson et al., 2003). A five-point response scale (1 = very dissatisfied to 5 = very satisfied) was used in this study. A mean score, indicating total life satisfaction, was computed with higher scores indicating greater overall life satisfaction.
Contribution to community
The Contribution subscale (Pilkauskaite-Valickiene, 2015) of the Positive Youth Development Inventory (PYDI; Arnold, Nott, & Meinhold, 2012) is a seven-item measure of youths’ perception of community contribution (e.g., “I am someone who gives to benefit others”). A four-point response scale is used (1 = strongly disagree to 4 = strongly agree). In this study, a mean contribution score was computed, with higher scores indicating greater degrees of competence in this domain.
Patient Health Questionnaire (PHQ-9)
The PHQ-9 (Kroenke, Spitzer, & Williams, 2010) is a self-report measure of depressive symptoms corresponding to the nine Diagnostic and Statistical Manual (DSM) criteria for major depression. Using a four-point response scale (1 = not at all, 2 = several days, 3 = more than half the days, 4 = nearly every day), respondents indicated how often they experienced symptoms within the previous two weeks. The PHQ-9 has support for use with adolescents (Richardson, McCauley, & Katon, 2009) and has demonstrated adequate psychometric properties, including good sensitivity and specificity (Kroenke et al., 2010). Eight items were used in this study. One item (item 9, “Thoughts that you would be better off dead of or hurting yourself in some way”) was not included because of school administrators’ concerns about their ability to promptly respond to students who endorsed this item. A mean score was computed, with higher scores indicating greater severity of depressive symptoms.
Generalized Anxiety Disorder Scale (GAD-7)
The GAD-7 is a seven-item self-report anxiety measure (Kroenke et al., 2010; Spitzer, Kroenke, Williams, & Löwe, 2006). Using a four-point response scale identical to the PHQ-9, respondents indicated how often they had experienced symptoms related to anxiety within the previous two weeks. A mean score was computed, with higher scores indicating greater severity of anxiety symptoms.
Data Analytic Strategy
A series of LPAs were performed to examine the underlying number of latent groups among dual-factor mental health indicators for adolescents in each of Grades 9, 10, and 11 using Mplus version 7.4 (Muthén & Muthén, 1998–2015). Models were specified using mean scores from the four domains of the SEHS-S [belief-in-self (BIS), belief-in-others (BIO), engaged living (EL), emotional competence (EC)] and two domains of the SDQ [internalizing risk (INT) and externalizing risk (EXT)] as indicators of well-being and distress, respectively. Given the continuous nature of the indicators used in this study, a subset of latent class analysis (LCA), LPA, was used (Vermunt, 2004). Both LCA and LPA specify an underlying categorical latent variable which identifies classes, thus we use the term “classes” to refer to the emergent latent groups or profiles. The model building process requires fitting several possible LPAs for each grade and then comparing the model fit information and substantive interpretation of each model so as to determine which is the most appropriate (Nylund et al., 2007a). In LPA, classes can vary with respect to their indicator means, indicator variances, and covariances between indicators. In this study, two model structures were examined for each number of latent classes across each year: (a) Model 1 in which item variances are freely estimated but constrained to be equal across classes (i.e., class-invariant) with no within-class indicator covariances (i.e., diagonal), and (b) Model 2 in which indicator variances are freely estimated and are not constrained to be equal across classes (i.e., class-varying) with no within-class indicator covariances (i.e., diagonal).
A small percentage of individuals had missing responses on items contributing to SEHS-S, SDQ, or distal outcome composite score indicators. Missing item responses were accounted for within each subscale before computing composites. Mean composite scores were calculated only for individuals for whom at least 75% of items were answered within a given composite, which only resulted in 1.2% of the sample having indicator-level missingness across all grade years. Patterns of item-level missing data were examined, and no systematic pattern of missing data emerged. Additionally, independent samples t-tests did not yield significant differences in Grade 9 on SEHS-S or SDQ indicators for students who did and did not complete the survey in Grades 10 or 11. Chi-square tests also did not yield significant differences between these individuals on demographic indicators. Thus, data were assumed to be missing at random (MAR). Indicator level missingness is accounted for via Full Information Maximum Likelihood (FIML; Enders & Bandalos, 2001) used in the Mplus LPAs, which allows for item-level (i.e., indicator level) missingness under the MAR assumption.
Class enumeration and retention
A series of LPA models were fit in an effort to select a model with a number of classes that sufficiently describe the heterogeneity in the indicators (Masyn, 2013; Nylund, 2007). The number of latent classes was systematically increased by one until empirical support was not evidenced for additional classes, for example due to failures in model convergence or emergence of small or conceptually opaque classes (Nylund et al., 2007b). The model judged to most adequately capture the sample’s heterogeneity was selected as the best fitting model for each LPA. In determining the appropriate number of latent classes, Masyn (2013) recommends examining (a) evaluations of absolute fit, (b) evaluations of relative fit, and (c) evaluations of classification. Evaluations of absolute fit are not applicable to LPA, thus, relative fit indices were relied upon in the current study.
Evaluations of relative fit assess model fit by comparing a target model to an alternative model with a different number of latent classes and include the information criteria statistics, such as the Bayesian Information Criteria (BIC; Schwartz, 1978), Bayes Factor (BF), correct model probability (cmP), Bootstrap Likelihood Ratio Test (BLRT; McLachlan & Peel, 2000), and Vuong Lo Mendel Rubin LRT (VLMR-LRT; Vuong, 1989). When interpreting the BF, values between 1 and 3 offer weak evidence, between 3 and 10 offer moderate evidence, and greater than 10 offer strong evidence for the current model (Wasserman, 1997). Larger cmP values indicate a greater likelihood of the model being the correct model out of all models tested (Masyn, 2013). The BLRT and the VLMR-LRT tests examine the fit of a k-class model with a k-1 class solution, with non-significant p-values indicating support for the k-1 class solution. With regard to information criteria statistics, superior model fit is indicated by lower values. Accuracy of classification of individuals to latent classes within a given model was examined based upon estimates of posterior class probability (i.e., the likelihood of each individual’s membership in a given class, based upon his or her pattern of responses) and relative entropy (Ramaswamy, DeSarbo, Reibstein, & Robinson, 1993). High entropy has been associated with values close to .80 (Clark & Muthén, 2009), with values closer to 1 indicating superior classification precision (Masyn, 2013). Each of the above criteria was evaluated in selecting and interpreting all models.
Specification of conditional models with demographic covariates and distal outcomes
Following specification of unconditional, cross-sectional LPA models for Grades 9, 10, and 11, and selection of the final model for each grade year, covariates of gender and ethnicity (Latinx, non-Latinx) and distal self-reports of grades and social-emotional outcomes were included in the model to explore the validity of emerging latent classes. Gender and ethnicity covariates were included to account for significant associations between these demographic indicators and the distal psychosocial outcomes of interest in this study and for significant associations with well-being and psychopathology that have been documented in previous research (e.g., Merikangas et al., 2010, Merikangas, Nakamura, & Kessler, 2009). When covariates and distal outcomes are examined concurrently, the manual BCH method, a three-step approach, is current best practice (Asparouhov & Muthén, 2015). Using this method, (a) the latent class indicator is regressed onto the demographic covariates, (b) the distal outcomes are regressed onto the latent class indicator, and (c) the distal outcomes are regressed onto the covariates. When examining the relation between the latent classes and the covariates, the covariates maintain their dichotomous coding (i.e., 0, 1). However, when examining the direct relation between the distal outcomes and the covariates, the covariates are mean centered to allow for ease of interpretation of the conditional means produced for each outcome. That is, means, conditioned on (i.e., controlling for) the covariates, are estimated for each outcome for each emerging complete mental health class for each of Grades 9–11. The estimated means are then compared across class to identify any significant differences between classes on the distal outcomes measured. Contact first author for example syntax for these analyses.
Results
Latent Profile Analyses: Identification of Dual-Factor Mental Health Classes
Mean item responses for the mental health indicators and predictive validity outcomes are presented in Table 1. Cross-sectional LPA models were run for Grades 9, 10, and 11. A one-class model was tested first and then additional models with additional latent classes were explored. Given the LPA framework, both the class-invariant, diagonal (Model 1) and class-varying, diagonal (Model 2) model structures were tested. Table 2 presents the information used to evaluate each model, including fit statistics, entropy values, and class prevalence proportions. Examining the results for Grade 9, the BIC, cmP, and BF indicate that the four-class class-invariant, diagonal model fit best. Although the five-class solution also had support (BIC = 2589.87, BF = 23.80), examination of class prevalence information indicated that the additional fifth class explained variance in an unreliably small percentage of people (1.0% or 3.32 people). Thus, the four-class solution was chosen as the best fitting model. Model 2 structures for Grade 9, 10, and 11 models with greater than four, three, or two classes, respectively across years, demonstrated failed log likelihood convergence for 20% to 82% of runs, indicating model instability despite the produced fit criteria. Thus, best fitting models were selected with Model 1 structure for each grade year. Further examination of fit criteria across each grade year also supported a four-class solution for Grades 10 and 11. The observed entropy values of the best-fitting four-class solutions approximated high levels of entropy, with values ranging from .78 (Grades 9 and 10) to .82 (Grade 11) and indicate that for at least 78% to 82% of the time, individuals were correctly classified in latent classes (Clark & Muthén, 2009). Therefore, a four-class model was deemed the optimal model for Grades 9, 10, and 11.
Table 2.
Information Used to Evaluate Tested LPA Dual-Factor Mental Health Models
| Model | Number of classes |
Log likelihood |
BIC |
p-value of BLRT |
p-value of LMRT |
BF | cmP | Entropy | Class Prevalence |
|---|---|---|---|---|---|---|---|---|---|
| Grade 9 - Model 1 (n = 332) | 1 | −1464.48 | 2998.61 | - | - | <.001 | <.001 | - | 1.00 |
| 2 | −1299.40 | 2709.10 | <.001 | <.001 | <.001 | <.001 | 0.74 | .44, .55 | |
| 3 | −1231.61 | 2614.15 | <.001 | 0.01 | <.001 | <.001 | 0.85 | .05, .35, .60 | |
| 4 | −1197.99 | 2587.56 | <.001 | 0.55 | 3.18 | 0.75 | 0.78 | .06, .31, .20, .43 | |
| 5 | −1178.83 | 2589.87 | <.001 | 0.10 | 23.80 | 0.24 | 0.81 | .01, .09, .19, .27, .44 | |
| 6 | −1161.69 | 2596.21 | <.001 | 0.31 | <.001 | 0.01 | 0.81 | .01, .08, .12, .12, .28, .39 | |
|
Grade 9 - Model 2 (n = 332) |
1 |
−1464.48 |
2998.61 |
- |
- |
<.001 |
<.001 |
- |
1.00 |
| 2 | −1264.67 | 2674.46 | <.001 | <.001 | <.001 | <.001 | 0.82 | .33, .67 | |
| 3 | −1195.92 | 2612.43 | <.001 | 0.03 | 0.23 | 0.10 | 0.75 | .23, .33, .44 | |
| 4* | −1156.72 | 2609.50 | <.001 | 0.20 | 0.98 | 0.45 | 0.79 | .05, .25, .32, .39 | |
| 5* | −1118.97 | 2609.47 | <.001 | 0.26 | >100 | 0.45 | 0.82 | .05, .09, .23, .23, .41 | |
| 6* | −1095.71 | 2638.41 | 0.01 | 0.62 | <.001 | <.001 | 0.81 | .05, .07, .11, .18, .27, .32 | |
|
Grade 10 - Model 1 (n = 324) |
1 |
−1283.37 |
2636.10 |
- |
- |
<.001 |
<.001 |
- |
1.00 |
| 2 | −1101.50 | 2312.83 | <.001 | <.001 | <.001 | <.001 | 0.75 | .49, .51 | |
| 3 | −1040.96 | 2232.21 | <.001 | 0.02 | 0.09 | 0.08 | 0.82 | .07, .41, .53 | |
| 4 | −1018.37 | 2227.50 | <.001 | 0.39 | 11.42 | 0.85 | 0.78 | .06, .21, .32, .41 | |
| 5 | −1000.57 | 2232.37 | <.001 | 0.38 | 799.91 | 0.07 | 0.76 | .07, .09, .17, .32, .35 | |
| 6 | −987.02 | 2245.74 | 0.01 | 0.54 | <.001 | <.001 | 0.78 | .02, .07, .09, .16, .32, .34 | |
|
Grade 10 - Model 2 (n = 324) |
1 |
−1283.37 |
2636.10 |
- |
- |
<.001 |
<.001 |
- |
1.00 |
| 2 | −1058.99 | 2262.49 | <.001 | <.001 | <.001 | <.001 | 0.80 | .42, .58 | |
| 3* | −990.87 | 2201.41 | <.001 | 0.05 | 0.01 | 0.01 | 0.79 | .15, .35, .51 | |
| 4* | −948.16 | 2191.13 | <.001 | <0.001 | >100 | 0.99 | 0.80 | .09, .13, .38, .40 | |
| 5* | −919.23 | 2208.43 | <.001 | 0.11 | 40.49 | <.001 | 0.84 | .10, .12, .13, .29, .36 | |
| 6* | −885.36 | 2215.83 | <.001 | 0.03 | <.001 | <.001 | 0.84 | .05, .09, .12, .13, .24, .37 | |
|
Grade 11 - Model 1 (n = 291) |
1 |
−1379.66 |
2827.40 |
- |
- |
<.001 |
<.001 |
- |
1.00 |
| 2 | −1161.17 | 2430.13 | <.001 | <.001 | <.001 | <.001 | 0.83 | .38, .62 | |
| 3 | −1104.56 | 2356.62 | <.001 | 0.21 | <.001 | <.001 | 0.86 | .05, .43, .52 | |
| 4 | −1059.07 | 2305.36 | <.001 | 0.01 | 0.03 | <.001 | 0.82 | .04, .21, .31, .44 | |
| 5 | −1035.57 | 2298.07 | <.001 | 0.39 | 0.17 | 0.14 | 0.81 | .03, .10, .20, .22, .44 | |
| 6 | −1013.92 | 2294.49 | <.001 | 0.67 | <.001 | 0.85 | 0.82 | .03, .09, .12, .18, .22, .36 | |
|
Grade 11 - Model 2 (n = 291) |
1 |
−1379.66 |
2827.40 |
- |
- |
<.001 |
<.001 |
- |
1.00 |
| 2* | −1127.24 | 2396.32 | <.001 | <0.001 | <.001 | <.001 | 0.80 | .44, .56 | |
| 3* | −1033.93 | 2283.45 | <.001 | 0.20 | <.001 | <.001 | 0.86 | .19, .33, .48 | |
| 4* | −979.96 | 2249.26 | <.001 | 0.37 | - | 1.00 | 0.87 | .06, .16, .30, .48 |
Note. Bolded values = preferred model for a given fit index and shaded rows = model selected for each year.
log likelihood starting values did not converge, indicating model instability.
The profile plots of the estimated mean values for each mental health domain are presented in Figure 1. Based on the pattern of mean scores across the well-being (i.e., SEHS-S) and distress (i.e., SDQ) domains, the following labels are offered for the four emerging classes across each year: complete mental health (30.5%, Grade 9; 40.8%, Grade 10; 20.5%, Grade 11) with the highest means on the well-being domains and the lowest means on the distress domains, moderately mentally healthy (43.4%, 32.0%, 44.3%, respectively) with high-average means on the well-being indicators and low means on the distress domains, symptomatic but content (20.3%, 21.2%, 31.3%, respectively) also with high-average well-being but with higher mean scores on the distress indicators, and troubled (5.7%, 6.0%, 3.8%, respectively) with below-average well-being and average to above-average scores on the distress indicators. When naming the classes, we aimed to be descriptive and also consistent with the dual-factor nomenclature presently used. When examining the size of each class across years, the troubled class consistently had the smallest percentage of students. Most students exhibited high or high-average scores on the well-being indicators with low levels of reported distress on the distress indicators (i.e., complete mental health or moderately mentally healthy). Overall, a larger percentage of students fell into mental health classes characteristic of higher levels of distress by Grade 11 (i.e., troubled or symptomatic but content). Youth in mental health classes characteristic of higher levels of distress, particularly in Grades 10 and 11, tended to report higher levels of internalizing distress as compared to externalizing distress.
Figure 1.
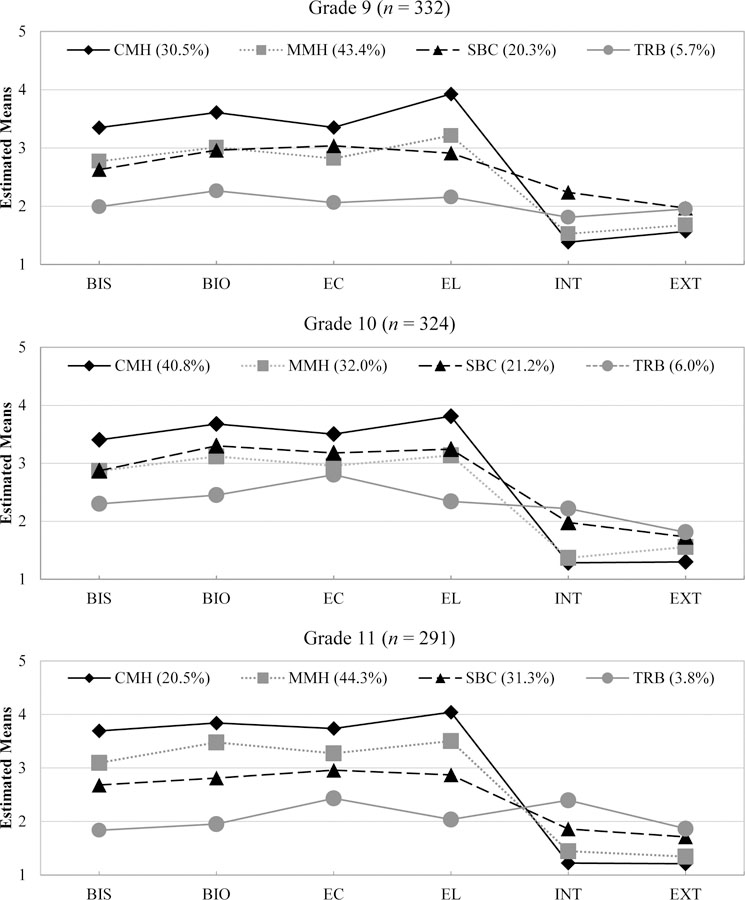
Dual-factor mental health profile plots for the four-class models for Grade 9 through Grade 11. Class size information is presented in the legend. (Note. BIS = belief in self, BIO = belief in others, EC = emotional competence, EL = engaged living, INT = internalizing distress, EXT = externalizing distress. CMH = complete mental health class, MMH = moderately mentally healthy class, SBC = symptomatic but content class, TRB = troubled class.) The mean-value range for BIS, BIO, and EC was 1 to 4; for EL was 1 to 4.67; and for INT and EXT was 1 to 3.
Table 3 presents the average posterior class probability (AvePP; Masyn, 2013) of students being classified into each mental health class, given their classification into one mental health class. For example, in Grade 9, the probability of individuals in the moderately mentally healthy class being classified into the complete mental health class was .08. The values in the shaded cells presented on the diagonal for each grade level illustrate the probability that members of a given class would be classified into that class (i.e., classification accuracy). The accuracy of classification for each mental health class across years was high (> .80).
Table 3.
Average Posterior Class Probability of Most Likely Latent Class Membership by Latent Mental Health Class
| Classification Probability |
|||||
|---|---|---|---|---|---|
| Grade | Most Likely Class Membership | 1 | 2 | 3 | 4 |
| Grade 9 | 1. Complete Mental Health | 0.94 | 0.06 | 0.01 | 0.00 |
| 2. Moderately Mentally Healthy | 0.08 | 0.86 | 0.05 | 0.01 | |
| 3. Symptomatic but Content | 0.01 | 0.16 | 0.83 | 0.01 | |
| 4. Troubled |
0.00 |
0.08 |
0.07 |
0.85 |
|
| Grade 10 | 1. Complete Mental Health | 0.94 | 0.04 | 0.02 | 0.00 |
| 2. Moderately Mentally Healthy | 0.08 | 0.85 | 0.08 | 0.00 | |
| 3.Symptomatic but Content | 0.04 | 0.15 | 0.81 | 0.01 | |
| 4. Troubled |
0.00 |
0.04 |
0.09 |
0.85 |
|
| Grade 11 | 1. Complete Mental Health | 0.86 | 0.14 | 0.00 | 0.00 |
| 2. Moderately Mentally Healthy | 0.05 | 0.90 | 0.05 | 0.00 | |
| 3. Symptomatic but Content | 0.00 | 0.08 | 0.91 | 0.01 | |
| 4. Troubled | 0.00 | 0.00 | 0.02 | 0.98 | |
Note. Shaded cells indicate accuracy of classification
Predictive Validity of the LPA Classes
To examine the predictive validity of the LPA classes, we examined if self-reported grades and social-emotional indicators differed across the four mental health classes. Prosocial contribution to community, life satisfaction, depression symptoms, anxiety symptoms, and self-reported grades, measured in Grade 12, were distal outcomes in these analyses. We examined differences between mental health classes in each of Grades 9–11 using the five outcome indicators. Moreover, because both covariates and distal outcomes were examined in the current analyses, the manual BCH method was used so that the relation between the covariates and distal outcomes was controlled when examining differences on the distal outcomes based on latent class membership. Thus, the results presented reflect the effect of latent class membership on each distal outcome at the average level of the gender and ethnicity covariates while controlling for the direct relation between the distal outcomes and gender and ethnicity.
Table 4 presents the class specific means and standard errors on each outcome for the Grade 9, 10, and 11 analyses, after controlling for the direct relations between the outcomes and the gender and ethnicity covariates. To test which mental health classes differed in their mean outcome scores, a Wald Test was conducted on all between-group comparisons. A conservative p-value (.01) was used to adjust for increased error due to multiple tests. Few differences between classes in each of Grades 9, 10, and 11 were observed with respect to self-reported grades. No significant differences were observed for Grade 9, with the Grade 10 and 11 differences reflecting higher grades for students in the complete mental health or moderately mentally healthy classes with respect to the symptomatic but content class.
Table 4.
Mean Item Responses and Standard Errors of Academic and Social-Emotional Distal Outcomes in Grade 12 Across Mental Health Classes
| Grade 12 Outcomes (Response Scale) |
||||||
|---|---|---|---|---|---|---|
| Grade | Mental Health Class (% in class) | Self-Reported Grades (range 1–8) | Contribution to Community (range 1–6) | Life Satisfaction (range 1–6) | Depression Symptoms (range 1–3) | Anxiety Symptoms (range 1–3) |
| Grade 9 (n = 332) | Complete Mental Health (30.5%) | 6.47 (.16)a | 5.04 (.11)a | 5.18 (.10)a | 1.58 (.07)a | 1.54 (.08)a |
| Moderately Mentally Healthy (43.4%) | 6.63 (.12)a | 4.61 (.09)a | 5.07 (.07)a | 1.48 (.05)a | 1.42 (.06)a | |
| Symptomatic but Content (20.3%) | 6.03 (.20)a | 4.37 (.13)b | 4.58 (.14)b | 1.91 (.10)b | 2.02 (.13)b | |
| Troubled (5.7%) | 6.45 (.44)a | 4.15 (.20)b | 4.57 (.30)ab | 1.37 (.14)a | 1.52 (.17)ab | |
|
Grade 10 (n = 324) |
Complete Mental Health (40.8%) |
6.72 (.12)a |
4.96 (.09)a |
5.35 (.07)a |
1.39 (.05)a |
1.32 (.05)a |
| Moderately Mentally Healthy (32.0%) | 6.44 (.16)ab | 4.56 (.11)b | 4.83 (.10)b | 1.45 (.07)ac | 1.55 (.08)ab | |
| Symptomatic but Content (21.2%) | 6.03 (.22)b | 4.39 (.15)c | 4.63 (.14)b | 2.12 (.11)b | 2.01 (.13)b | |
| Troubled (6.0%) | 6.00 (.44)ab | 4.16 (.19)bc | 4.50 (.21)b | 1.84 (.15)bc | 2.03 (.20)b | |
|
Grade 11 (n = 291) |
Complete Mental Health (20.5%) |
6.79 (.21)a |
5.32 (.13)a |
5.47 (.12)a |
1.29 (.07)a |
1.34 (.10)a |
| Moderately Mentally Healthy (44.3%) | 6.60 (.12)a | 4.88 (.08)b | 5.20 (.06)a | 1.44 (.05)a | 1.43 (.06)a | |
| Symptomatic but Content (31.3%) | 6.29 (.14)ab | 4.12 (.10)c | 4.52 (.09)b | 1.82 (.07)b | 1.82 (.07)b | |
| Troubled (3.8%) | 5.10 (.51)b | 3.64 (.29)c | 3.57 (.33)c | 2.36 (.20)b | 2.51 (.24)c | |
Note. Means that do not share subscripts differ at p < .01.
Class specific differences were observed for the positive mental health outcomes of prosocial contribution to community and life satisfaction. Students in the complete mental health and moderately mentally healthy classes had significantly greater prosocial contribution than the symptomatic but content and troubled classes. The Grade 9 and Grade 11 complete mental health and moderately mentally healthy classes similarly reported higher average levels of life satisfaction in Grade 12 than the symptomatic but content and troubled classes. The Grade 10 complete mental health class had significantly greater life satisfaction than all other classes. In Grade 11, adolescents in the symptomatic but content and troubled classes significantly differed, with students in the symptomatic but content class who reported higher levels of well-being also reporting greater levels of life satisfaction.
Students in the symptomatic but content and troubled classes tended to report more frequent symptoms of depression and anxiety, on average, than did students in the complete mental health and moderately mentally healthy classes. Patterns were largely consistent across both depression and anxiety outcomes for classes in each of Grades 9–11. However, minor variations were observed between classes for each grade year. For example, when Grade 12 outcomes were examined for Grade 9 classes, contrary to classes in the other grade years, students in the Grade 9 symptomatic but content class had significantly higher levels of depression in Grade 12, but not anxiety, than students in the troubled class. However, of the Grade 11 classes, students in the troubled class had significantly higher levels of anxiety in Grade 12, but not depression, than did students in the symptomatic but content class.
Groups reporting higher levels of well-being with low levels of distress tended to exhibit more positive outcomes on both the positive mental health and negative mental health indicators. Similarly, groups reporting higher levels of distress tended to experience poorer outcomes on the negative indicators of mental health. The complete mental health class was generally associated with the most positive outcomes up to three years later (i.e., better self-reported grades, higher average scores on positive mental health outcomes, lower average scores on negative mental health outcomes). However, the complete mental health class did not unanimously experience more positive outcomes than the moderately mentally healthy class, which had slightly lower average well-being. Similarly, though not always exhibiting significant differences between one another or with the other two classes, the symptomatic but content and troubled classes tended to experience poorer outcomes, especially with regard to negative mental health outcomes.
Discussion
Previous dual-factor research has most often classified youth into four groups based on logically determined cut points for well-being and distress indicators. In the current study, we relied on patterns in adolescents’ reports about their own mental health functioning to inform the most relevant mental health grouping. In each of Grades 9–11 the LPA results supported a four-class solution. These latent classes were examined at three points across the high school years to evaluate if the construct of dual-factor mental health was stable over time. We found structural stability in the latent dual-factor mental health construct over three years. The four-class solution consisting of a complete mental health (i.e., high well-being and low distress), moderately mentally healthy (i.e., high-average well-being, low distress), symptomatic but content (i.e., high-average well-being, average to above-average distress), and troubled (i.e., below-average wellbeing, average to above-average distress) class was replicated for each of Grade 9, 10, and 11 Despite minor fluctuations observed in the average scores for the well-being and distress indicators for each class, the substantive interpretation for each solution is consistent over time.
Consistent with previous dual-factor research, classes fitting each of a complete mental health, troubled, and symptomatic but content profile emerged in the current study. However, inconsistent with previous cut score and empirical classification work (e.g., Rebelez-Ernst, 2015), a languishing or vulnerable group, indicative of low well-being and low distress, did not emerge in the current study. Rather, the fourth emerging mental health group (i.e., students who are moderately mentally healthy) reported average to above average well-being and below average distress. As can be seen in the profile plots in Figure 1, this fourth emerging group reported similar levels of well-being as the symptomatic but content class in Grades 9 and 10 (although it was more differentiated from the symptomatic but content group in level of well-being in Grade 11), but markedly lower levels of distress, particularly as related to internalizing problems. The inability to detect a languishing group in the current study may indicate that a small number of students fit this profile making them statistically unreliable and difficult to detect within an LPA framework. Replication with larger, independent samples is warranted.
The patterns observed in levels of strengths in the current study indicate that understanding adolescents’ well-being may be more nuanced than described in previous dual-factor work. For example, rather than simply indicating lower versus higher well-being via a predetermined cut point, the LPA results reveal a gradient of well-being, with three of the four emerging mental health groups consistently differing in their average levels of social-emotional strengths. Empirically defining complete mental health groups allows for a group of youth with the highest levels of well-being and the lowest levels of distress (i.e., complete mental health) to be distinguished from those youth with high-average levels of well-being and low levels of distress (moderately mentally healthy). Within the cut-point classification approach, youth in the moderately mentally healthy class may have been considered to have complete mental health.
Although the same four classes emerged across the exploratory LPAs for each of Grades 9, 10, and 11, indicating consistency in the construct of dual-factor mental health over time, the proportions of students comprising each mental health class were variable. In each grade year, the majority of students were classified into the complete mental health and moderately mentally healthy classes. However, in Grades 9 and 11 moderately mentally healthy students represented over 40% of the sample, whereas the complete mental health group was largest (41%) in Grade 10. The troubled class exhibited consistency in size; whereas the symptomatic but content group increased over time, reaching 31% by Grade 11 compared to 20% in Grade 9. Similarly, the complete mental health class was smallest (21%) in Grade 11, compared to 31% in Grade 9 and 41% in Grade 10. These fluctuations in class prevalence observed over time suggest that movement is occurring across classes from year to year. Additional research is needed to examine factors (e.g., individual level, school-context level) contributing to movement among classes and associated fluctuations in class proportions. The proportions of students in the complete mental health and moderately mentally healthy classes in the current study are similar to rates reported by Keyes (2006) who found that, among adolescents aged 15 to 18, most reported being moderately mentally healthy (55%) followed by flourishing (40%; i.e., complete mental health). However, the percentage of students in emerging complete mental health classes in the current study (Grade 9 = 31%, Grade 10 = 41%, Grade 11 = 21%) is consistently smaller than percentages reported in previous dual-factor research using a cut-score approach [e.g., 42% (Venning et al., 2013) to 64% (Lyons et al., 2012)]. This suggests that the number of youth exhibiting complete mental health may be overestimated when cut-point criteria are applied rather than when groups are formed based on patterns in observed data.
This study examined the validity of the complete mental health classes via their relations with Grade 12 outcomes. Our findings identified class differences in self-reported grades and positive (prosocial contribution to community and life satisfaction) and negative (depression symptoms and anxiety symptoms) mental health indicators. Students in classes indicative of higher average scores on well-being indicators and lower average scores on distress indicators tended to have higher scores on positive indicators of mental health and lower scores on negative indicators of mental health over time, which provides validation evidence for the four emerging classes and of the dual-factor mental health construct. Consistent with previous research, we found that students in the complete mental health class experienced the most favorable outcomes across grade years, followed by students in the moderately mentally healthy class, with these two groups differing significantly from one another in approximately half of the comparisons made. Also consistent with previous research, students in the troubled class tended to experience the least favorable outcomes, although their self-reported outcomes were not always statistically significantly different from youth in the symptomatic but content class or from the moderately mentally healthy and complete mental health classes. However, given the much smaller size of the troubled class in the current study (i.e., approximately 6% or 20 people in Grade 9 and 10, and 4% or 12 people in Grade 11), comparisons made between the troubled group and the other mental health groups were likely underpowered. Replication with larger samples is needed. Overall, more differences between latent classes on Grade 12 outcomes were observed in Grade 11, indicating that the predictive power of latent mental health classes is strongest within a one year prior, as opposed to two or three years prior to measurement of the outcomes of interest.
Previous dual-factor mental health research has also indicated that, among youth experiencing distress, those with higher levels of well-being tend to exhibit more positive outcomes (e.g., Antaramian et al., 2010). In the current study, this effect was observed in relation to anxiety symptoms and life satisfaction (particularly in Grade 11), such that youth in the symptomatic but content class, exhibited more positive outcomes than youth in the troubled class. However, students in the symptomatic but content class also, on average, reported lower levels of internalizing distress than did youth in the troubled class. It is unclear if the presence of higher levels of well-being or lower levels of distress led to more positive outcomes for this group of students. An advantage of the empirical approach to classification, however, is that it allows meaningful differences in average responses on a given indicator to emerge across mental health groups; differences that are not acknowledged when groups are created by cut scores.
Implications for Research and Practice
The present study contributes to research supporting a comprehensive approach to mental health assessment that includes indicators of both well-being and distress. Using an empirical approach to complete mental health classification enabled identification of variability in well-being and distress observed for four emerging mental health groups. Although, on the surface, confirming the presence of four empirically defined mental health groups parallels what has been illustrated in previous dual-factor research, empirically identifying groups as opposed to using logically determined cut points allowed for meaningful variation in levels of well-being and distress indicators to be observed across groups. These results indicate that the cut-point approach to forming mental health groups may incompletely capture the complexity in youth’s dual-factor mental health profiles. Thus, the current results extend previous research on dual-factor mental health and offer continued support for examining both well-being and distress in universal screening efforts that can be used to inform prevention and early intervention.
Results highlight limitations of a binary cut-score approach to classification. Although there is error associated with both LPA and cut-point classification, cut-point approaches do not allow for examination of the probability of members of one class being classified into (i.e., being similar to) another class. Using empirically defined classification allows us to examine the accuracy with which youth are placed into groups via estimates of the likelihood of being classified into a given class based on one’s most likely latent class membership. Forming groups via latent classes, in this study we were able to model the error associated with classification and could examine the likelihood of individuals identified as members in one mental health class being classified into another class on an aggregate level (Table 3). Results supported strong accuracy in classification for the empirically defined mental health groups. However, future research is needed to compare differences in classification that may arise when a cut-score versus empirical approach is used. For example, investigations can compare the distribution of students assigned to LPA produced mental health classes as compared to group assignment based on cut scores as well as any differences in the predictive validity of each mental health class with later outcomes. In addition, examining the likelihood of membership in each empirically defined mental health class on an individual level (rather than at an aggregate level, as done in this study) can be used to further examine accuracy of various classification approaches.
Overall, the results call for further examination of cut-score approaches to classification used to interpret universal complete mental health screening data. Although school-based mental health practitioners may lack the resources needed to evaluate screening assessment data using LPA, the results of this study highlight that a dichotomous, cut-score approach to complete mental health classification may obscure meaningful variation in youths’ complete mental health profiles. If limited to using cut-score approaches due to the ease and efficiency of this approach, mental health practitioners may wish to utilize additional cut points, especially with regard to youth’s well-being, resulting in more than four groups. For example, Moore et al. (2015) used universal complete mental health screening results to form nine triage groups informed by three psychological risk and four social-emotional strength groups. Concurrently, scholars, mental health practitioners, and other school mental health stakeholders are called upon to investigate and develop techniques for translating LPA classification parameters into a usable format for organizing dual-factor mental health data that are collected and intended to guide intervention. The LPA examinations in this study are thus viewed as an initial step necessary for informing classification approaches that may be easily accessible to and applied by practitioners.
This study’s results support dual-factor mental health assessment and intervention. Through universal complete mental health screening, schools obtain a comprehensive, dynamic picture of their students’ mental health functioning (e.g., Moore et al., 2015). Information from universal screening offers predictive information about youths’ later mental health functioning and thus should be used to inform a range of interventions implemented at multiple tiers of support (von der Embse, Iaccarino, Mankin, Kilgus, & Magen, 2016). Therefore, practitioners interested in universal screening are encouraged to identify and co-administer screening tools that measure psychological strengths in addition to emotional/behavioral risk, psychological distress, or mental illness. When using screening data to link students to relevant interventions, practitioners should collaborate with their school and community colleagues to provide interventions that focus on supporting youths’ complete mental health. For example, Suldo and Shaffer (2008) explain that all youth would benefit from schoolwide approaches to support wellness (e.g., social-emotional learning curricula, promoting positive school climate), whereas youth with symptomatic but content mental health may benefit from small-group interventions that address symptoms of distress while continuing to support wellbeing (e.g., mentoring partnerships, check-in/check-out). Youth fitting a troubled profile would receive individualized, intensive interventions that are designed to reduce symptoms of mental illness, and to increase well-being (e.g., individual counseling, referral for special education evaluation). Through assessment and interventions tailored toward wellness promotion and risk prevention and treatment, schools can support all students’ complete mental health.
Limitations and Future Directions
Although adequate in size for the current analyses, the present sample was restricted in geographic diversity, which limits the generalizability of our findings. The sample consisted of students attending one school in central California and was limited in size by attrition between Grade 9 and 12, when the outcome measures were administered. Additionally, although the percentage of students representing the smallest troubled group was consistent with estimates of the proportion of youth who are identified as having severe mental health concerns via universal screening (Moore et al., 2015), the sample size of the current study resulted in a small number of students comprising the troubled group, thus limiting the power to detect differences between this group and the other mental health groups. Additional research is needed with larger, geographically diverse samples. Although the profiles observed in the current study provided support for the structural stability of dual-factor mental health classes, variability was observed in class sizes over the high school years. Research is needed to explore the relative size of emerging classes and factors that contribute to shifts in these proportions over time.
The well-being and distress measures, grades, and social-emotional outcomes relied on self-report. Results may have been influenced by mono-method and social desirability bias. Moreover, research recommends caution in interpreting self-reported grades (e.g., Kuncel et al., 2005); hence, additional research examining academic achievement is needed. The use of self-reported grades in the current study is further limited by their retrospective nature. In addition, although adolescents are recognized as ideal informants of their own internal states (e.g., Smith, 2007), some research suggests that adolescents may underreport their externalizing behavior (e.g., Smith, Pelham, Gnagy, Molina, & Evans, 2000). The lower rates of externalizing problems observed may reflect participants’ underestimation of their externalizing behaviors.
There are limitations in the naming of classes. Most research describing dual-factor mental health logically created groups using study-specific well-being and distress criteria. The labels adopted for these groups in many studies — complete mental health (also referred to as well-adjusted, thriving, mentally healthy), symptomatic but content (inconsistent, externally maladjusted), languishing (vulnerable, asymptomatic yet discontent), and troubled (highest risk, distressed, mentally unhealthy) — have served as a heuristic for each group’s core well-being and distress characteristics. Nonetheless, there is incomplete uniformity among dual-factor studies in how measures and cut-point criteria are used to form groups, as well as the labels of the groups themselves (Kim et al., 2017). In naming the emerging latent classes in the current study, we attempted to balance recommendations for use of consistent language to facilitate communication among dual-factor mental health stakeholders with recognition that operational definitions of complete mental health, moderately mentally healthy, symptomatic but content, and troubled mental health vary in the existing research base. The names given to emerging classes in this study were selected to parallel seminal research in this area (e.g., Keyes 2006; Suldo & Shaffer, 2008), yet represent only one way profiles of wellbeing and distress could be labeled. Cross study communication and collaboration among scholars interested in dual-factor mental health to operationally define variations in dual-factor mental health is needed.
The analyses of this study make an important contribution to dual-factor mental health research by validating the structural stability of empirically defined mental health classes based upon indicators of both well-being and distress. An important next step will be to investigate the stability of individuals’ patterns of dual-factor mental health over the high school years. Future research should investigate longitudinal trends in youths’ mental health via latent transition analysis, which provides estimates of the probabilities of transitioning between classes. Further, research examining how individual and contextual factors influence transitions to and from identified mental health classes (e.g., factors that influence transition into the troubled class from a more flourishing mental health class during the previous year) is important to further inform mental health screening and intervention efforts. In addition, research comparing classification and predictive validity of empirically derived versus cut-score defined dual-factor mental health groups is important for informing applied classification efforts that impact intervention.
Understanding mental health as comprised of indicators of well-being and distress is important in comprehensive efforts to address risk and promote youth thriving. When used as part of universal mental health screening, information gained from assessment of youths’ complete mental health can be used to inform intervention at each level of a comprehensive service delivery system, including schoolwide, small-group, and individualized interventions intended to ameliorate psychopathology and support development of social-emotional strengths and youths’ well-being. The current study, using an empirical classification approach provided initial information that can inform continuing research into how to classify youth into distinct mental health groups for intervention and follow-up efforts after screening assessments that foster youths’ positive mental health and well-being.
Supplementary Material
Funding and Acknowledgements
Support for this study was provided in part by a grant from the U.S. Department of Education, Institute of Education Sciences (#R305A160157). The preparation of this article was supported in part by the National Institute of Mental Health (#T32MH109436-02). The opinions expressed are those of the authors and do not represent views of the Institute of Education Sciences, the U.S. Department of Education, or the National Institutes of Health.
Footnotes
Conflict of Interest
The authors declare that they have no conflict of interest.
Compliance with Ethical Standards
The authors declare that they have no conflict of interest. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Contributor Information
Stephanie A. Moore, Johns Hopkins Bloomberg School of Public Health
Erin Dowdy, University of California, Santa Barbara.
Karen Nylund-Gibson, University of California, Santa Barbara.
Michael J. Furlong, University of California, Santa Barbara
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. [Google Scholar]
- Antaramian SP, Huebner ES, Hills KJ, & Valois RF (2010). A dual-factor model of mental health: Toward a more comprehensive understanding of youth functioning. American Journal of Orthopsychiatry, 80, 462–472. doi: 10.1111/j.1939-0025.2010.01049.x [DOI] [PubMed] [Google Scholar]
- Arnold ME, Nott BD, & Meinhold JL (2012). The Positive Youth Development Inventory Full Version Corvallis, OR: Oregon State University. [Google Scholar]
- Asparouhov T, & Muthén B (2015). Auxiliary variables in mixture modeling: Using the BCH method in Mplus to estimate a distal outcome model and an arbitrary secondary model. Mplus Web Notes, 21(2), 1–22. [Google Scholar]
- California Department of Education. (n.d.). California school district secondary school survey results fall 2009/spring 2010: Core module A Retrieved from http://chks.wested.org/resources/a-text_0910.pdf
- Clark SL, & Muthén B (2009). Relating latent class analysis results to variables not included in the analysis. Unpublished manuscript, University of California Los Angeles. [Google Scholar]
- Enders CK, & Bandalos DL (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling: A Multidisciplinary Journal, 8, 430–457. doi: 10.1207/S15328007SEM0803_5 [DOI] [Google Scholar]
- Goodman R (1997). The Strengths and Difficulties Questionnaire: A research note. Child Psychology & Psychiatry & Allied Disciplines, 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x [DOI] [PubMed] [Google Scholar]
- Greenspoon PJ, & Saklofske DH (2001). Toward an integration of subjective well-being and psychopathology. Social Indicators Research, 54, 81–108. doi: 10.1023/A:1007219227883 [DOI] [Google Scholar]
- Keyes CLM (2005). Mental illness and/or mental health? Investigating axioms of the complete state model of health. Journal of Counseling and Clinical Psychology, 73, 539–548. doi: 10.1037/0022-006X.73.3.539 [DOI] [PubMed] [Google Scholar]
- Keyes CLM, (2006). Mental health in adolescence: Is America’s youth flourishing? American Journal of Orthopsychiatry, 76, 395–402. doi: 10.1037/0002-9432.76.3.395 [DOI] [PubMed] [Google Scholar]
- Kim EK, Dowdy E, Furlong MJ, & You S (2017). Mental health profiles and quality of life among Korean adolescents. School Psychology International, 38, 98–116. doi: 10.1177/0143034316682296 [DOI] [Google Scholar]
- Kroenke K, Spitzer RL, Williams JBW, & Löwe B (2010). The Patient Health Questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. General Hospital Psychiatry, 32, 345–359. doi: 10.1016/j.genhosppsych.2010.03.006 [DOI] [PubMed] [Google Scholar]
- Kuncel NR, Credé M, & Thomas LL (2005). The validity of self-reported grade point averages, class ranks, and test scores: A meta-analysis and review of the literature. Review of Educational Research, 75, 63–82. doi: 10.3102/00346543075001063 [DOI] [Google Scholar]
- Laursen B, & Hoff E (2006). Person-centered and variable centered approaches to longitudinal data. Merrill-Palmer Quarterly, 52, 377–389. doi: 10.1353/mpq.2006.0029 [DOI] [Google Scholar]
- Lyons MD, Huebner ES, Hills KJ, & Shinkareva SV (2012). The dual-factor model of mental health: Further study of the determinants of group differences. Canadian Journal of School Psychology, 27, 183–196. doi: 10.1177/0829573512443669 [DOI] [Google Scholar]
- Masyn KE (2013). Latent class analysis and finite mixture modeling. In Little TD (Ed.), The Oxford handbook of quantitative methods (pp. 551–611). New York, NY: Oxford University Press. [Google Scholar]
- McLachlan G, & Peel D (2000). Finite mixture models New York, NY: Wiley. [Google Scholar]
- Merikangas KR, Jian-ping H, Burstein M, Swanson SA, Avenevoli S, Lihong C, … & Swendsen J (2010). Lifetime prevalence of mental disorders in US adolescents: Results from the National Comorbidity Study-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49, 980–989. doi: 10.1016/j.jaac.2010.05.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merikangas KR, Nakamura E, & Kessler RC (2009). Epidemiology of mental disorders in children and adolescents. Dialogues in Clinical Neuroscience, 11, 7–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore SA, Widales-Benitez O, Carnazzo KW, Kim EK, Moffa K, & Dowdy E (2015). Conducting universal complete mental health screening via student self-report. Contemporary School Psychology, 19, 253–267. doi: 10.1007/s40688-015-0062-x [DOI] [Google Scholar]
- Muthén LK, & Muthén BO (1998–2015). Mplus user’s guide (7th Ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Nylund KL, 2007. Latent transition analysis: modeling extensions and an application to peer victimization. Doctoral dissertation, University of California Los Angeles. [Google Scholar]
- Nylund K, Asparouhov T, & Muthén B (2007a). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: An Interdisciplinary Journal, 14, 535–569. doi: 10.1080/10705510701575396 [DOI] [Google Scholar]
- Nylund K, Bellmore A, Nishina A, Graham S (2007b). Subtypes, severity, and structural stability of peer victimization: What does latent class analysis say? Child Development, 78(6), 1706–1722. doi: 10.1111/j.1467-8624.2007.01097.x [DOI] [PubMed] [Google Scholar]
- Pilkauskaite-Valickiene R The role of character, confidence, and connection on contribution and subjective well-being. Procedia – Social and Behavioral Sciences, 197, 265–270. doi: 10.1016/j.sbspro.2015.07.134 [DOI] [Google Scholar]
- Ramaswamy V, Desarbo WS, Reibstein DJ, & Robinson WT (1993). An empirical pooling approach for estimating marketing mix elasticities with PIMS data. Marketing Science, 12(1), 103–124. doi: 10.1287/mksc.12.1.103 [DOI] [Google Scholar]
- Rebelez-Ernst JL (2015). Capturing complete mental health among adolescents: Investigation of covitality latent class typologies. Doctoral Dissertation, University of California Santa Barbara. [Google Scholar]
- Richardson L, McCauley E, Katon W (2009). Collaborative care for adolescent depression: a pilot study. General Hospital Psychiatry, 31, 36–45. doi: 10.1016/j.genhosppsych.2008.09.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruchkin V, Jones S, Vermeiren R, & Schwab-Stone M (2008). The Strengths and Difficulties Questionnaire: The self-report version in American urban and suburban youth. Psychological Assessment, 20, 175–182. doi: 10.1037/1040-3590.20.2.175 [DOI] [PubMed] [Google Scholar]
- Scales PC (1999). Reducing risks and building developmental assets: Essential actions for promoting adolescent health. Journal of School Health, 69, l13–119. doi: 10.1111/j.l746-1561.l999.tb07219.x [DOI] [PubMed] [Google Scholar]
- Schwartz G (1978). Estimating the dimension of a model. The Annals of Statistics, 6, 461–464. doi: 10.1214/aos/1176344136 [DOI] [Google Scholar]
- Seligson J, Huebner ES, & Valois RF (2003). Preliminary validation of the Brief Multidimensional Students’ Life Satisfaction Scale (BMSLSS). Social Indicators Research, 61, 121–145. doi: 10.1023/A:1021326822957 [DOI] [Google Scholar]
- Smith SR (2007). Making sense of multiple informants in child and adolescent psychopathology: A guide for clinicians. Journal of Psychoeducational Assessment, 25, 139–149. doi: 10.1177/0734282906296233 [DOI] [Google Scholar]
- Smith BH, Pelham WE Jr., Gnagy E, Molina B, & Evans S (2000). The reliability, validity, and unique contributions of self-report by adolescents receiving treatment for attention-deficit/hyperactivity disorder. Journal of Consulting and Clinical Psychology, 68, 489–499. doi: 10.1037//0022-006X.68.3.489 [DOI] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, Williams JBW, Löwe B (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166, 1092–1097. doi: 10.1001/archinte.166.10.1092 [DOI] [PubMed] [Google Scholar]
- Sticca F, Goetz T, Bieg M, Hall NC, Eberle F, & Haag L (2017). Examining the accuracy of students’ self-reported academic grades from a correlational and a discrepancy perspective: Evidence from a longitudinal study. PLoS ONE, 12(11), e0187367. doi: 10.1371/journal.pone.0187367 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suldo SM, & Shaffer EJ (2008). Looking beyond psychopathology: The dual-factor model of mental health in youth. School Psychology Review, 37, 52–68. [Google Scholar]
- Suldo SM, Thalji-Raitano A, Kiefer SM, & Ferron JM (2016). Conceptualizing high school students’ mental health through a dual-factor model. School Psychology Review, 45, 434–457. [Google Scholar]
- Venning A, Wilson A, Kettler L, & Eliott J (2013). Mental health among youth in South Australia: A survey of flourishing, languishing, struggling, and floundering. Australian Psychologist, 48, 299–310. doi: 10.1111/j.1742-9544.2012.00068.x [DOI] [Google Scholar]
- Vermunt JK (2004). Latent profile model. In Lewis-Beck MS, Bryman A, & Liao TF (Eds.), The Sage encyclopedia of social sciences research methods (pp. 554–555). Thousand Oakes, CA: Sage. [Google Scholar]
- von der Embse NP, Iaccarino S, Mankin A, Kilgus SP, & Magen E (2016). Development and validation of the Social, Academic, and Emotional Behavior Risk Screener – Student Rating Scale. Assessment for Effective Intervention, 42, 186–192. doi: 10.1177/1534508416679410 [DOI] [Google Scholar]
- Vuong QH (1989). Likelihood ratio tests for model selection and non-nested hypotheses. Econometrica, 57, 307–333. doi: 10.2307/1912557 [DOI] [Google Scholar]
- Wasserman L (1997). Bayesian model selection and model averaging. Presented at Mathematical Psychology Symposium “Methods for Model Selection,” Bloomington, IN. [DOI] [PubMed] [Google Scholar]
- Westerhof GB, & Keyes CLM (2010). Mental illness and mental health: The two-continua model across the lifespan. Journal of Adult Development, 17, 110–119. doi: 10.1007/s10804-009-9082-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. (2016, April). Mental health: Strengthening our response (Fact Sheet) Retrieved from www.who.int/mediacentre/factsheets/fs220/en/
- You S, Furlong MJ, Dowdy E, Renshaw T, Smith DC, & O’Malley MD (2014). Further validation of the Social and Emotional Health Survey for high school students. Applied Quality of Life Research, 9, 997–1015. doi: 10.1007/s11482-013-9282-2 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.