

Abstract
Background
Garlic is widely used by patients for its blood pressure lowering effects. A meta‐analysis published in 2008 concluded that garlic consumption lowers blood pressure in hypertensive and normotensive patients. Therefore, it is important to review the currently available evidence to determine whether garlic may also have a beneficial role in the reduction of cardiovascular events and mortality rates in patients with hypertension.
Objectives
To determine whether the use of garlic as monotherapy, in hypertensive patients, lowers the risk of cardiovascular morbidity and mortality compared to placebo.
Search methods
A systematic search for trials was conducted in the Cochrane Hypertension Group Specialised Register, CENTRAL, MEDLINE, EMBASE, AGRICOLA, AMED, and CINAHL up to November 2011. A hand search of reference lists of identified reviews was conducted. Experts in the area were also contacted to identify trials not found in the electronic search. Clinicaltrials.gov was searched for ongoing trials.
Selection criteria
Randomized, placebo‐controlled trials of any garlic preparation versus placebo for the treatment of hypertension were included.
Data collection and analysis
Two reviewers independently extracted data and assessed trial quality using the risk of bias tool. Data synthesis and analysis was performed using RevMan 5.
Main results
The search identified two randomized controlled trials for inclusion. One trial included 47 hypertensive patients and showed that garlic significantly reduces mean supine systolic blood pressure by 12 mmHg (95% CI 0.56 to 23.44 mmHg, p=0.04) and mean supine diastolic blood pressure by 9 mmHg (95% CI 2.49 to 15.51 mmHg, p=0.007) versus placebo. The authors state that garlic was "free from side effects" and that no serious side effects were reported. There were 3 cases "where a slight smell of garlic was noted."
The second trial could not be meta‐analysed as they did not report the number of people randomized to each treatment group. They did report that 200 mg of garlic powder given three times daily, in addition to hydrochlorothiazide‐triamterene baseline therapy, produced a mean reduction of systolic blood pressure by 10‐11 mmHg and of diastolic blood pressure by 6‐8 mmHg versus placebo.
Neither trial reported clinical outcomes and insufficient data was provided on adverse events.
Authors' conclusions
There is insufficient evidence to determine if garlic provides a therapeutic advantage versus placebo in terms of reducing the risk of mortality and cardiovascular morbidity in patients diagnosed with hypertension. There is also insufficient evidence to determine the difference in withdrawals due to adverse events between patients treated with garlic or placebo.
Based on 2 trials in 87 hypertensive patients, it appears that garlic reduces mean supine systolic and diastolic blood pressure by approximately 10‐12 mmHg and 6‐9 mmHg, respectively, over and above the effect of placebo but the confidence intervals for these effect estimates are not precise and this difference in blood pressure reduction falls within the known variability in blood pressure measurements. This makes it difficult to determine the true impact of garlic on lowering blood pressure.
Keywords: Humans, Antihypertensive Agents, Antihypertensive Agents/therapeutic use, Blood Pressure, Blood Pressure/drug effects, Cardiovascular Diseases, Cardiovascular Diseases/prevention & control, Drug Combinations, Garlic, Garlic/chemistry, Hydrochlorothiazide, Hydrochlorothiazide/therapeutic use, Hypertension, Hypertension/drug therapy, Hypertension/mortality, Phytotherapy, Phytotherapy/methods, Randomized Controlled Trials as Topic, Supine Position, Triamterene, Triamterene/therapeutic use
Plain language summary
Garlic for Hypertension
Garlic is widely used by patients for its blood pressure lowering effects. In this analysis, we reviewed the currently available evidence to determine the impact of garlic on cardiovascular events and mortality in patients with hypertension. Based on data from two randomized controlled trials that compared garlic to placebo in patients with hypertension it appears that garlic may have some blood pressure lowering effect, as compared to placebo but the evidence currently available is insufficient to determine whether garlic provides a therapeutic advantage versus placebo in terms of reducing the risk of cardiovascular morbidity and mortality. Data on the safety of garlic, as a therapeutic entity, in this population is also lacking. More (and large enough) trials comparing several doses of garlic with placebo are needed to detect possible differences in mortality, serious adverse events, and cardiovascular morbidity.
Background
Description of the condition
Hypertension is associated with structural changes in the heart and blood vessels which may lead to cardiovascular mortality and morbidity (i.e. cardiovascular disease, stroke, peripheral vascular disease, and renal disease). Hypertension is typically defined as having a systolic blood pressure (SBP) > 140 mmHg and a diastolic blood pressure (DBP) > 90 mmHg (CHEP 2008, Chobanian 2003). Worldwide, approximately 1 billion people are affected by hypertension (Chobanian 2003) and seven million deaths per year may be attributed to hypertension (WHO 2003). In addition, for every 20 mmHg increase in SBP and 10 mmHg increase in DBP (through the range from 115/75 to 185/115 mmHg) in people aged 40 to 70 years, the risk of cardiovascular disease (CVD) morbidity doubles (Chobanian 2003). This emphasizes the importance of finding safe and effective treatments for the prevention of the associated mortality and morbidity in hypertensive patients. Thus, with a vast number of patients being diagnosed with this disease, it is not surprising that alternative and complementary therapy for hypertension are being explored (Rahman 2006). According to a survey of 900 people conducted by the US Food and Drug Administration in 2002, garlic is the second most utilized complementary therapy (after Echinacea) with 17% of the population using this supplement within the preceding 12 month period (Timbo 2006). Garlic is considered one of the most popular complementary therapies for blood pressure control and is thought to be used by 50% of patients with hypertension (Bongiorno 2008).
Description of the intervention
Garlic (Allium sativum) is a member of the family Alliaceae, and is believed to have originated from Central Asia (Jellin 2006, Rahman 2006). The use of garlic for medicinal purposes is well documented in history. The Egyptians, Romans, Chinese, and Indians used garlic for a variety of medical ailments. Garlic was thought to be effective for respiratory and gastrointestinal illnesses, in the treatment of certain infectious diseases, and for increasing performance in labourers (Rivlin 2001).
There are several different types of garlic preparations that are available: garlic cloves, essential garlic oil (0.2 to 0.5% of garlic cloves), garlic powder (which contains the same compounds as garlic cloves but in different amounts), garlic oil macerates (garlic cloves ground into vegetable oils), garlic extract (primarily made up of the water‐soluble constituents of garlic cloves), and aged garlic extract (aging converts the harsh compounds into stable, less toxic sulphur compounds) (Harunobu 2001).
How the intervention might work
The blood pressure lowering properties of garlic appear to come from the bulb portion of the plant and have been attributed to the production of sulphur containing compounds. Allicin (allyl 2‐propenethiosulfinate) is thought to be one of the principle bioactive compounds, with the highest sulphur content. Allicin is produced from the breakdown of S‐allyl cysteine‐S‐oxide (alliin)(Jellin 2006). Allicin, a vasodilating agent, has also been shown in vitro to inhibit angiotensin‐converting enzyme (which aids in the production of angiotensin, a potent vasoconstrictor) and therefore reduces blood pressure in individuals with hypertension (Banerjee 2002). The effectiveness of garlic products on blood pressure is thought to be determined primarily by their ability to yield allicin. This ability, however, can be affected by the method of preparation since the enzyme alliinase, responsible for the conversion of alliin to allicin, is inactivated by heat (Jellin 2006). As a result, not all garlic products have the same amount of allicin and thus, it is thought that the effectiveness of the products vary depending on how they were prepared (Jellin 2006). Ongoing research suggests that the medicinal properties of garlic are due to other compounds in addition to allicin. Phenolic and steroidal compounds in garlic have pharmacological effects, are odour free, and, unlike allicin, are heat‐stable (Harunobu 2001, Lanzotti 2006, Matsuura 2001).
Why it is important to do this review
Evidence from randomized controlled trials suggests that garlic may be beneficial in the treatment of hypertension. Results from a 1994 meta‐analysis that included eight trials and 415 patients reported an overall 7.7 mmHg greater reduction in systolic blood pressure and 5.0 mmHg greater reduction in diastolic blood pressure in all subjects treated with garlic. Upon review of the two placebo‐controlled trials within the meta‐analysis specifically looking at hypertensive patients, an 11.1 mmHg greater reduction in systolic blood pressure and 6.5 mmHg greater reduction in diastolic blood pressure was found in the garlic treated patients. Overall, however, this review concluded there was insufficient evidence to recommend garlic as clinical therapy for the treatment of hypertension (Silagy 1994). On the other hand, a more recent 2008 systematic review that included 25 studies (n=1298), eleven of which were eligible for meta‐analysis (503 patients included in the SBP analysis and 565 in the DBP analysis), concluded that garlic preparations are, in fact, superior to placebo for lowering blood pressure in a mixed population of normotensive and hypertensive patients. The result of a regression analysis showed a statistically significant association between blood pressure at the start of the intervention and blood pressure reduction following use of garlic (SBP: R = 0.057; p = 0.03; DBP: R = ‐0.315; p = 0.02) (Ried 2008).
Since garlic is widely used by patients for its blood pressure lowering effects, it is important to review the currently available evidence to determine whether garlic may, in fact, have a beneficial role in the reduction of these cardiovascular events and/or reduce mortality rates in patients with hypertension. The recent meta‐analysis (Ried 2008) provides evidence that garlic consumption lowers blood pressure in a mixed population of hypertensive and normotensive patients. However, it remains to be determined whether the consumption of garlic reduces the risk of morbidity or mortality associated with elevated blood pressure. The aim of our systematic review is to determine the effect of garlic consumption on morbidity and mortality in hypertensive patients. The secondary aim is to quantify the blood pressure lowering effect of garlic consumption specifically in hypertensive patients.
Objectives
Primary objective
To determine whether garlic monotherapy provides a therapeutic advantage over placebo for the treatment of adults with hypertension, as determined by a hierarchy of clinically important outcomes:
All cause mortality
Cardiovascular events (fatal or non‐fatal myocardial infarction)
Cerebrovascular events (fatal or non fatal strokes)
Secondary objectives
To determine whether garlic monotherapy provides a therapeutic advantage over placebo in reduction of systolic and diastolic blood pressure in adults with hypertension.
To determine the incidence of withdrawal due to adverse effects associated with garlic monotherapy.
Methods
Criteria for considering studies for this review
Types of studies
Randomized controlled trials, either parallel group or crossover, were considered.
Types of participants
Trials with human participants who are at least 18 years of age, with a diagnosis of primary hypertension (defined as having a systolic blood pressure > 140 mmHg or a diastolic blood pressure of > 90mmHg, or both) were reviewed. Participants could be on other therapies for hypertension as long as this additional therapy was used by participants in all arms of the trial (i.e. all groups would receive the same additional antihypertensive therapy).
Types of interventions
Interventions using garlic (allium sativum) monotherapy in a preparation without any other ingredients known or thought to have an antihypertensive effect. Studies that use manufactured, cooked, or raw garlic preparations were considered. No restrictions were placed on the quantity of garlic administered or the frequency of garlic administration.
Trials with a placebo comparator were considered for inclusion.
Types of outcome measures
Primary outcomes
The primary outcomes are death due to any cause, serious adverse events (an event that is life‐threatening, causes death, leads to hospitalization, prolongs hospitalization, leads to persistent or significant disability/incapacity, or leads to a congenital anomaly/birth defect), and cardiovascular events including myocardial infarction and stroke.
Secondary outcomes
The secondary outcomes are blood pressure reduction, as well as breath and body odour, mouth and gastrointestinal burning or irritation, or any other adverse events severe enough to cause withdrawal from treatment.
Search methods for identification of studies
The Database of Abstracts of Reviews of Effectiveness (DARE) and the Cochrane Database of Systematic Reviews were searched for related reviews.
Electronic searches
The following electronic databases were searched for primary studies:
a) The Cochrane Hypertension Group Specialised Register (1948‐November 2011), Cochrane Central Register of Controlled Trials (2011, Issue 4), MEDLINE (1950‐November 2011), EMBASE (1980‐November 2011), AGRICOLA (1970‐November 2011), Allied and Complementary Medicine (AMED) (1985‐November 2011), BIOSIS (1969‐2011), and CINAHL (1981‐November 2011). The Hypertension Group Specialised Register includes controlled trials from searches of AGRICOLA, Allied and Complementary Medicine (AMED), BIOSIS, CAB Abstracts, CINAHL, Cochrane Central Register of Controlled Trials, EMBASE, Food Science and Technology Abstracts (FSTA), Global Health, International Pharmaceutical Abstracts (IPA), LILACS, MEDLINE, ProQuest Dissertations & Theses, PsycINFO, SCIRUS, and Web of Science.
b) ClinicalTrials.gov
Electronic databases were searched using a strategy combining the Cochrane Highly Sensitive Search Strategy for identifying randomized trials in MEDLINE: sensitivity‐maximizing version (2008 revision) with selected MeSH terms and free text terms relating to garlic and hypertension. No language restrictions were used. The MEDLINE search strategy (Appendix 1) was translated into EMBASE (Appendix 2), CENTRAL (Appendix 3), the Hypertension Group Specialised Register (Appendix 4), AGRICOLA (Appendix 5), AMED (Appendix 6), BIOSIS (Appendix 7), and CINAHL (Appendix 8) using the appropriate controlled vocabulary as applicable.
Searching other resources
Citations of reviews and meta‐analyses on the treatment of hypertension with garlic were examined. Experts in the field were contacted to identify any other trials missed in our search.
Data collection and analysis
Selection of studies
Two reviewers independently assessed all studies identified to determine whether they met the predefined inclusion criteria. All references that mentioned the use of garlic from articles identified in the search were reviewed and were included if they met the criteria. The reasons for excluding a study were documented. A third independent reviewer resolved any differences that arose on whether a trial should be included.
Data extraction and management
Studies which fulfilled the inclusion criteria were examined in detail by two independent reviewers. Two independent reviewers extracted data using a standardized data extraction form.
Assessment of risk of bias in included studies
The following parameters were assessed:
Method and/or security of randomization,
Whether or not the individuals involved in the study (including health care provider, assessor, and patient) were blinded to the treatment allocation,
Whether analysis by intention‐to‐treat was performed,
How many participants completed the study.
Any differences in interpretation of the data were resolved through consensus between the four reviewers. If additional information was required, an attempt to contact the original authors of the study was made.
Study characteristics and the outcome measures of interest were collected independently by the two reviewers using a pre‐formed data extraction sheet. All data, regardless of compliance or completion of follow up was collected in order to allow for analysis by intention to treat.
Measures of treatment effect
For evaluation of the primary outcomes (all cause mortality, cardiovascular events, and cerebrovascular events), the total number of patients with at least one event within each trial were to be recorded as a percent. Proportions were to be calculated for these dichotomous outcomes, and comparisons between groups. However none of the included trials reported on clinical outcomes.
Data for blood pressure reduction was combined using a weighted mean difference method. This combines a weight based on the number of individuals in the trial and the within study variance. If the trial did not report the within study variance for decrease in blood pressure, the standard deviation was to be imputed from the average standard deviation from the other trials. Imputation was not necessary as all relevant information was present in the included trials.
Unit of analysis issues
Data from all patients individually randomized to each intervention was used in the analysis. Care was taken to identify situations in which data has been censored/excluded or if data presented was the total number of events or the total number of patients with a first event.
Dealing with missing data
An attempt was made to contact the authors of the study for clarification if there was missing data.
Assessment of heterogeneity
Assessment of heterogeneity was not done as there was only one study included in the meta‐analysis component of this review.
Assessment of reporting biases
Assessment of reporting bias was not necessary as we were unable to assess if there was data missing from the outcomes reported by the authors in the studies. None of the results reported in this study were imputed or assumed.
Data synthesis
Cochrane Review Manager software, RevMan 5, was used for all data analyses. No dichotomous outcome data was reported in the included trials. Data for blood pressure reduction was combined using a weighted mean difference method with standard deviations.
Subgroup analysis and investigation of heterogeneity
The following subgroup analyses were planned but were not performed due to the lack of data available in the included trials:
Trials of less than 6 months duration, 6 to 12 months duration, and those more than 6 months duration
Trials of mild‐to‐moderate hypertension, severe hypertension and isolated systolic hypertension
Sensitivity analysis
The following sensitivity analyses were planned but were not performed due to the lack of available data in the included trials:
Trials with proper randomization or concealment of allocation compared to those without these characteristics
Trials preformed with intention‐to‐treat analysis compared to those without an intention‐to‐treat analysis
Unblinded versus blinded trials
Trials using unmanufactured raw or cooked garlic versus manufactured garlic trials
For any crossover trial, the pre‐crossover versus post‐crossover results
The effects of garlic with the inclusion of trials where blood pressure standard deviations are imputed versus the exclusion of data from trials that did not report blood pressure standard deviations
Results
Description of studies
Results of the search
See Figure 1 for flow chart describing the search results. Two reviewers (CF and FH) independently reviewed titles and abstracts from the initial search results in 2009. The search was then updated in November 2011 and abstracts and titles were screened by two reviewers (SS and AT). Two additional trials were identified through screening of the updated search (Han 2011, Ried 2010). No on‐going trials were identified through a search of the clinicaltrials.gov database.
1.
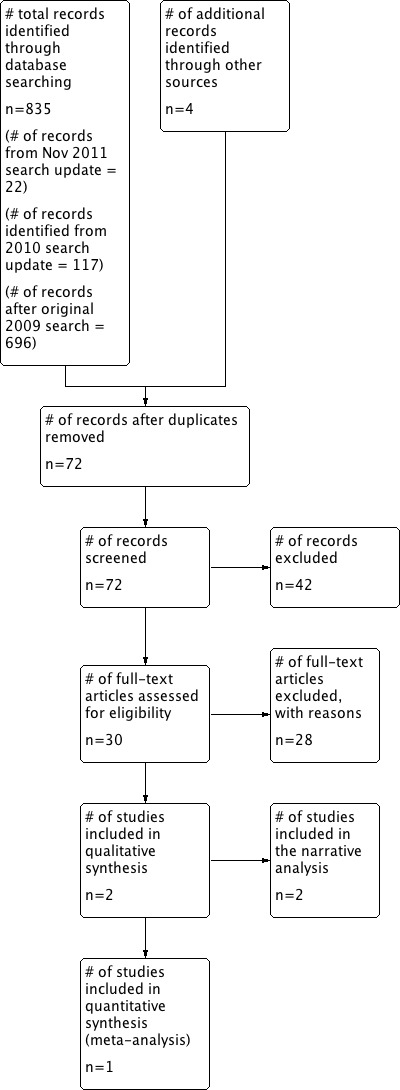
Study Flow Diagram
Included studies
Two studies were identified that met all of the inclusion criteria (Auer 1990 and Kandziora 1988). See Characteristics of included studies.
Excluded studies
A total of nine studies (Barrie 1987; Gardner 2001; Jain 1993; Kieswetter 1991; Rotzsch 1992; Saradeth 1994; Simons 1995; Superko 2000; Turner 2004; Zhang 2000) were excluded from this analysis as they included healthy volunteers or patients who did not have a diagnosis of hypertension. Czerny 1996 and Lutomski 1984 were excluded as the group randomized to receive garlic also received another herbal preparation (lecithin and rutin respectively). As well, not all patients in the Lutomski 1984 trial had hypertension. De A Santos 1995, Kandaziora 1988 (2), and Holzgartner 1992 did not have a placebo comparator arm, but compared garlic to another active antihypertensive medication. Eight studies (De A Santos 1993; Han 2011; Holzgartner 1992; Isaacsohn 1998; Kiesewetter 1993; Steiner 1996; Vorberg 1990) included some patients who had hypertension, but it ws unclear if randomization was stratified based on a diagnosis of hypertension. We were unable to extract the data on the hypertensive patients from these studies. Ried 2010 randomized patients with hypertension but these patients were on other anti‐hypertensive agents, and the use of these other agents was not standardized or equal between groups. The intent of the Ried 2010 study was to assess the effects of add‐on garlic therapy for hypertension. Mrozikiewicz 1989 was excluded because the only available information was in abstract form only. Four trials (Luley 1986, Mansell 1996, Satitvipawee 2003; Schiewe 1995) were excluded as they were primarily lipid lowering trials and didn't include or report adequate information on blood pressure. McMahon 1992 was excluded as no numerical data was available. Mousa 2007 was excluded because the patients were not randomized to the various interventions and a crossover design was not used. Two trials (Sobenin 2007 and Williams 2005) included patients with known ischemic heart disease or coronary artery disease. Presumably, some of these patients did have a diagnosis of hypertension, but we were unable to extract data for the hypertensive patients included in these studies.
Risk of bias in included studies
Both Auer 1990 and Kandziora 1988 did not report details for sequence generation, allocation concealment, or blinding. No details were given to account for patients through the trial period in order to assess for loss to follow up. No trial protocol was cited to rule out selective outcome reporting. Very limited information was provided on harm. It was not possible to contact the author for clarification as no contact information was provided in the trial report. A Google search was conducted for the name of the lead authors however no useful contact information was retrieved. (See Figure 2; Figure 3).
2.
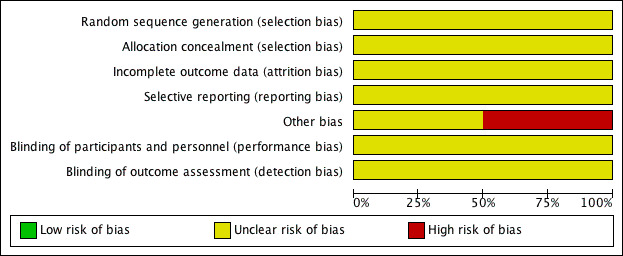
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
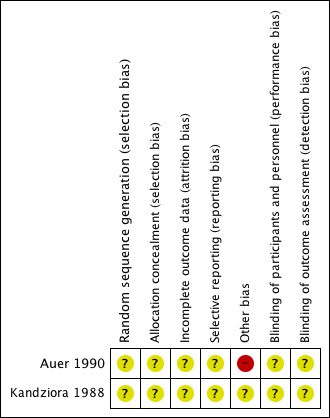
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Effects of interventions
Auer 1990 did not report on clinical outcomes or adverse events. However it had a relatively small sample size that would have been insufficient to demonstrate differences in these outcomes. Auer 1990 compared 200 mg garlic powder (Kwai(r)) three times daily (n=24) to placebo (n=23) in patients with WHO class I and II (mild) hypertension. After 12 weeks of study treatment garlic produced a reduction in mean supine systolic blood pressure of 19 mmHg (from 171 to 152 mmHg) and a reduction in mean supine diastolic blood pressure of 13 mmHg (from 102 to 89 mmHg). Non‐significant reductions in mean supine systolic (8 mmHg), mean supine diastolic (4 mmHg) blood pressure, mean standing systolic blood pressure (10 mmHg) or mean standing diastolic blood pressure (4 mmHg) were reported in the placebo‐treated patients. Garlic produced a reduction in mean standing systolic blood pressure of 21 mmHg (from 171 to 150 mmHg) and a reduction in mean standing diastolic blood pressure of 11 mmHg (from 101 to 90 mmHg). No details for standard error of the mean or standard deviations with respect to blood pressure changes were reported but the information was imputable from figure 1 on page 10 of Auer 1990. Information from the graph was used to calculate standard deviations and to subsequently compare the difference in mean reduction of supine systolic and diastolic blood pressure between garlic and placebo (see Analysis 1.1, Figure 4 and Analysis 1.2, Figure 5). Our analysis suggests garlic significantly reduces mean supine systolic blood pressure by 12 mmHg (95% CI 0.56 to 23.44 mmHg, p=0.04)) and mean supine diastolic blood pressure by 9.00 mmHg (95%CI 2.49 to 15.51 mmHg, p=0.007) versus placebo. The trial reports state both that garlic was "free from side effects" and that no serious adverse effects were reported. They reported 3 cases "where a slight smell of garlic was noted."
1.1. Analysis.
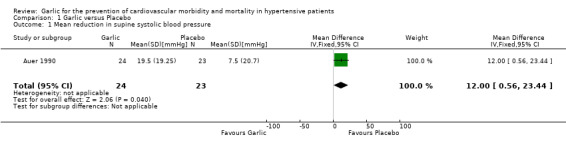
Comparison 1 Garlic versus Placebo, Outcome 1 Mean reduction in supine systolic blood pressure.
4.

Forest plot of comparison: 1 Garlic versus Placebo, outcome: 1.1 Mean reduction in supine systolic blood pressure [mmHg].
1.2. Analysis.
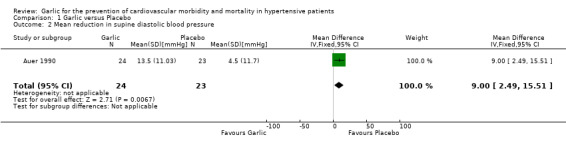
Comparison 1 Garlic versus Placebo, Outcome 2 Mean reduction in supine diastolic blood pressure.
5.

Forest plot of comparison: 1 Garlic versus Placebo, outcome: 1.2 Mean reduction in supine diastolic blood pressure [mmHg].
Kandziora 1988 enrolled 40 patients with hypertension who were all given hydrochlorothiazide‐triameterene therapy for their hypertension. These patients were then randomized to either 2 X 100 mg tablets of high potency garlic powder or matching placebo three times daily for 12 weeks. It should be noted that the data from this trial could not be used in the meta‐analysis as authors did not report the number of patients randomized to each treatment group. In this trial, the authors report that garlic produced a statistically significant mean reduction in supine SBP of 16 mmHg (from 178 to 162 mmHg) and supine DBP of 15 mmHg (from 100 to 85 mmHg). Garlic produced a statistically significant mean reduction in standing SBP of 16 mmHg (from 174 to 158 mmHg) and standing DBP of 16 mmHg (from 99 to 83 mmHg). Placebo produced a mean reduction in supine SBP of 5 mmHg (from 178 to 173 mmHg) and supine DBP of 9 mmHg (from 100 to 91 mmHg). Placebo produced a mean reduction in standing SBP of 6 mmHg (from 175 to 169 mmHg) and standing DBP of 8 mmHg (from 98 to 90 mmHg). This study reported that no patients experienced any cardiovascular outcomes, pulse changes, tachycardia, bradycardia, or other undesired effects. These results were present in addition to any effects of the use of hydrochlorothiazide‐triamterene therapy that was given to all patients in the trial.
Discussion
Summary of main results
Two trials (Auer 1990, Kandziora 1988) met the inclusion criteria for this review. In Auer 1990, 47 hypertensive individuals used 200 mg of garlic powder three times daily versus placebo. Garlic powder significantly reduced mean supine systolic and diastolic blood pressure by 12 mmHg and 9 mmHg, respectively. No cardiovascular event data or harm data were reported.
The data from Kandziora 1988 could not be meta‐analysed as they did not report the number of people randomized to each treatment group. They did report that 200 mg of garlic powder given three times daily, in addition to hydrochlorothiazide‐triamterene baseline therapy, produced a 10‐11 mmHg mean reduction in systolic blood pressure and a 6‐8 mmHg mean reduction in diastolic blood pressure versus placebo. No clinical outcomes were reported and insufficient data was provided on the safety of garlic powder for the treatment of hypertension.
Overall completeness and applicability of evidence
There is a paucity of clinical trials that randomize hypertensive patients to either garlic or placebo. It is important to demonstrate the impact of clinical and harm outcomes for interventions that reduce blood pressure. Based on the available data, it appears that garlic reduces blood pressure versus placebo however the magnitude of this effect cannot be accurately quantified. There is currently insufficient data regarding clinical outcomes or harm to support the use of garlic therapy in the management of hypertension.
Quality of the evidence
The two included trials (Auer 1990, Kandziora 1988) had small sample sizes and did not report important details regarding study methodology. As such, the amount of bias in these trials remains unclear. In addition, the effect sizes are relatively imprecise and only give an indication of the possible blood pressure lowering effects of garlic. Further research in this area is needed.
Potential biases in the review process
Many trials were excluded because they did not randomize patients with hypertension at baseline. Some may argue that important data was therefore not utilized. In our opinion, the impacts of garlic on blood pressure and clinical outcomes may differ between non‐hypertensive and hypertensive patients based on pathophysiology and risk of clinical morbidity due to underlying disease processes.
Agreements and disagreements with other studies or reviews
Ried 2008 conducted a meta‐analysis of garlic intervention trials to determine the effect of garlic on blood pressure. This review did not specify that trials had to randomize patients with objectively diagnosed hypertension. Rather, the authors included all randomized controlled trials of garlic that measured blood pressure changes. They did conduct a subgroup analysis of trials that had patients with baseline blood pressures in the hypertensive range and reported that garlic did significantly reduce systolic blood pressure by 8.4 ± 2.8 mmHg (n = 4; p < 0.001), and diastolic blood pressure by 7.3 ± 1.5 mmHg versus placebo. We compared the trials in that subgroup analyses to those trials that were identified in our search. We had also found Auer 1990 and Kandziora 1988 which were included in our review. We identified Vorberg 1990 as well but excluded this trial because patients were selected for the trial based on elevated cholesterol and not due to a diagnosis of hypertension. The original trial publication was reviewed and it was not possible to extract the data for the patients who may have been hypertensive at baseline. We also assessed Holzgartner 1992, however this trial compared garlic to bezafibrate and not placebo. This trial also included patients with and without hypertension, the patients were not stratified based on a diagnosis, and we were unable to extract the data for the hypertensive subgroup, therefore this trial was excluded from this analysis.
In addition, the intent of the Ried 2008 analysis was simply to identify the blood pressure lowering effect of garlic versus placebo. Our intent was different, in that we also wanted to know if garlic reduced morbidity and mortality in hypertensive patients. In our opinion this is the more important clinical question as simply lowering blood pressure using an intervention doesn't necessarily mean that the clinical morbidity and mortality due to hypertension will also go down (Wright 2009). In addition we also wanted to establish if there was any significant harm for garlic versus placebo, which was also not described in the Ried 2008 meta‐analysis.
Authors' conclusions
Implications for practice.
There is insufficient evidence currently available to determine if garlic provides a therapeutic advantage versus placebo in terms of reducing the risk of mortality and cardiovascular morbidity. There is insufficient evidence to determine the difference in withdrawals due to adverse events between patients treated with garlic or placebo.
Based on 2 trials in 87 hypertensive patients, it appears that garlic reduces mean supine systolic and diastolic blood pressure by approximately 10‐12 mmHg and 6‐9 mmHg, respectively, over and above the effect of placebo. However the confidence intervals for these effect estimates are not precise and this difference in blood pressure reduction falls within the known variability in blood pressure measurements (Musini 2009). This makes it difficult, if not impossible, to determine the true impact of garlic on reducing blood pressure.
Implications for research.
Garlic appears to have a blood pressure lowering effect based but the precise estimate of blood pressure reduction specifically in hypertensive individuals remains unknown. In addition, evidence is lacking on the possible impact of garlic on mortality or cardiovascular morbidity. Future trials should randomize hypertensive patients to several doses of garlic versus placebo. These trials should be large enough and report the differences in mortality, serious adverse events and cardiovascular morbidity.
Acknowledgements
The Cochrane Hypertension Review Group.
The UBC Therapeutics Initiative Drug Assessment Working Group.
Stephen Adams for assistance with the statistical analysis.
Ciprian Jauca for assistance with translation of non‐English trials.
Greg Rowell for help in refining the search strategy.
Appendices
Appendix 1. Medline Search Strategy
Database: Ovid MEDLINE(R) 1948 to Present with Daily Update Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 garlic/ 2 garlic.tw. 3 (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund).tw. 4 or/1‐3 5 hypertension/ 6 hypertens$.tw. 7 exp blood pressure/ 8 (blood pressure or bloodpressure).tw. 9 or/5‐8 10 randomized controlled trial.pt. 11 controlled clinical trial.pt. 12 randomized.tw. 13 placebo.tw. 14 drug therapy/ 15 randomly.tw. 16 trial.tw. 17 groups.tw. 18 or/10‐17 19 animals/ not (humans/ and animals/) 20 18 not 19 21 4 and 9 and 20
Appendix 2. EMBASE search strategy
Database: EMBASE <1980 to 2011 November 22> Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 garlic/ 2 garlic extract/ 3 garlic oil/ 4 garlic.tw. 5 (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund).tw. 6 or/1‐5 7 exp hypertension/ 8 hypertens$.tw. 9 exp blood pressure/ 10 (blood pressure or bloodpressure).mp. 11 or/7‐10 12 randomized controlled trial/ 13 crossover procedure/ 14 double‐blind procedure/ 15 random$.tw. 16 (crossover$ or cross‐over$).tw. 17 placebo$.tw. 18 (doubl$ adj blind$).tw. 19 allocat$.tw. 20 comparison.ti. 21 trial.ti. 22 or/12‐21 23 11 and 22 24 (animal$ not (human$ and animal$)).mp. 25 23 not 24 26 6 and 11 and 25
Appendix 3. CENTRAL search strategy
Database: Wiley ‐ Cochrane Central Register of Controlled Trials <2011 Issue 4> Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ #1 MeSH descriptor Garlic, explode all trees #2 garlic:ti,ab #3 (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund):ti,ab #4 #1 or #2 or #3 #5 MeSH descriptor Hypertension, this term only #6 hypertens*:ti,ab #7 MeSH descriptor Blood Pressure explode all trees #8 (blood pressure or bloodpressure):ti,ab #9 #5 or #6 or #7 or #8 #10 #4 AND #9
Appendix 4. Hypertension Group Specialised Register search strategy
Database: Hypertension Group Specialised Register Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 All fields (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund)
Appendix 5. AGRICOLA search strategy
Database: AGRICOLA <1970 to November 2011> Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 garlic.hw. 2 allium.hw. 3 garlic.tw. 4 (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund).tw. 5 or/1‐4 6 hypertension.hw. 7 hypertens$.tw. 8 blood pressure.hw. 9 (blood pressure or bloodpressure).tw. 10 or/6‐9 11 random$.ti,ab,id,sh,mp. 12 (control$ adj2 clinical).ti,ab,id,sh,mp. 13 placebo$.ti,ab,id,sh,mp. 14 trial.ti,ab,id,sh,mp. 15 groups.ab. 16 (doubl$ adj3 blind$).ti,ab,id,sh,mp. 17 allocat$.ti,ab,id,sh,mp. 18 assign$.ti,ab,id,sh,mp. 19 or/11‐18 20 5 and 10 and 19
Appendix 6. AMED search strategy
Database: AMED (Allied and Complementary Medicine) <1985 to November 2011> Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 allium sativum/ 2 garlic.tw. 3 (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund).tw. 4 or/1‐3 5 hypertension/ 6 hypertens$.tw. 7 blood pressure/ 8 (blood pressure or bloodpressure).tw. 9 or/5‐8 10 exp clinical trials/ 11 double blind method/ 12 random allocation/ 13 random$.tw. 14 placebo$.tw. 15 trial.tw. 16 groups.ab. 17 assign$.tw. 18 allocat$.tw. 19 or/10‐18 20 4 and 9 and 19
Appendix 7. BIOSIS search strategy
Database: BIOSIS Previews <1969 to 2011> Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 TS=garlic 2 TS=(allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund) 3 #2 or #1 4 TS=hypertens* 5 TS=("blood pressure" or bloodpressure) 6 #5 or #4 7 TS=random* 8 TS=("clinical control" or "clinical controlled" or "controlled clinical") 9 TS=placebo* 10 TI=trial* 11 TS="doubl*‐blind*" 12 TS=allocat* 13 TS=assign* 14 #13 OR #12 OR #11 OR #10 OR #9 OR #8 OR #7 15 #14 and #6 and #3
Appendix 8. CINAHL search strategy
Database: EBSCO CINAHL Search Date: 23 November 2011 ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ S20 S4 and S9 and S19 S19 S10 or S11 or S12 or S13 or S14 or S15 or S16 or S17 or S18 S18 AB groups S17 TI trial* S16 TI allocat* or AB allocat* S15 TI assign* or AB assign* S14 TI doubl* n2 blind* or AB doubl* n2 blind* S13 TI placebo* or AB placebo* S12 TI random* or AB random* S11 (MH "Random Assignment") S10 (MH "Clinical Trials") S9 S5 or S6 or S7 or S8 S8 TI ( (blood pressure or bloodpressure) ) or AB ( (blood pressure or bloodpressure) ) S7 (MH "Blood Pressure+") S6 TI hypertens* or AB hypertens* S5 (MH "Hypertension+") S4 S1 or S2 or S3 S3 TI ( (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund) ) or AB ( (allium or allibessen or allisantin or allisat or alloton or carisano or kwai or kyolic or salicaps or sanhelios or sapec or xund) ) S2 TI garlic or AB garlic S1 (MH "Garlic")
Data and analyses
Comparison 1. Garlic versus Placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean reduction in supine systolic blood pressure | 1 | 47 | Mean Difference (IV, Fixed, 95% CI) | 12.0 [0.56, 23.44] |
| 2 Mean reduction in supine diastolic blood pressure | 1 | 47 | Mean Difference (IV, Fixed, 95% CI) | 9.0 [2.49, 15.51] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Auer 1990.
| Methods | Randomized, placebo‐controlled, double‐blind | |
| Participants | Non‐hospitalized patients, recruited from general practices, with mild hypertension (WHO stage I and II, diastolic pressure between 95‐104 mmHg on "two control measurements with 14 days between each."The trial excluded patients on antihypertensives and antihyperlipidemic drugs, those with severe hypertension and hyperlipidemia, and those thought to be seriously ill or those that might suffer complications during the trial. | |
| Interventions | Fourteen days of "acclimatization"then given active treatment or placebo. Two capsules of 100mg each garlic powered preparation three times daily and the control group received "a similar looking placebo." | |
| Outcomes | Pulse, triglycerides, total cholesterol, supine/standing systolic and diastolic blood pressure, aspartate aminotransferase, alanine aminotransferase, gamma glutamyl transpeptidase, and blood sugar. | |
| Notes | Treatment lasted 12 weeks. Blood pressure, total cholesterol and pulse measure 2 weeks before treatment, at randomization, and at 4, 8, 12 weeks. aspartate aminotransferase, alanine aminotransferase, gamma glutamyl transpeptidase, and blood sugar were measured at randomization and at 12 weeks. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The patients were allocated to treatment groups at random."Given the small sample size, randomization was unlikely to balance groups for known and unknown characteristics even if an appropriate method of sequence generation was used. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No details are reported on the number of people in each group that were analysed for any particular outcome nor were any details on loss to follow‐up/withdrawals reported. |
| Selective reporting (reporting bias) | Unclear risk | No trial protocol was cited nor could a published protocol be found. It is unclear whether the pre‐specified plan matches what was reported in the published trial report. |
| Other bias | High risk | No reporting of any harm data or any clinical outcome data. No reporting of sample size calculations or p‐value adjustment for multiple comparisons. It is also unclear what the primary and secondary outcomes measures were. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Stated as "double‐blind"in the abstract but no mention of exactly which 2 groups were blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details were reported with regards to who measured the outcomes, who analysed the data, and no mention if any of those parties were blinded to treatment allocation. |
Kandziora 1988.
| Methods | Randomized, double‐blind, placebo controlled | |
| Participants | 40 hypertensive adults between the ages of 43 to 65 years with mild hypertension (WHO class I and II) with no evidence of diabetes, lipid disorders, serious coronary, renal or cerebral organ damage. | |
| Interventions | 200 mg of high potency garlic powder given orally three times daily for 12 weeks versus matching placebo. | |
| Outcomes | Electrolytes, electrocardiograms, blood pressure, serum creatinine, blood sugar, and cholesterol. | |
| Notes | Article published in German, was translated for us by Ciprian Jauca. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No details given and the number of patients randomized to each group was not reported. |
| Selective reporting (reporting bias) | Unclear risk | No trial protocol cited. |
| Other bias | Unclear risk | n/a |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details reported |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Barrie 1987 | Patients did not have hypertension. |
| Czerny 1996 | Group randomized to receive garlic also received lecithin, no lecithin was given in the placebo arm. |
| De A Santos 1993 | Not all patients had hypertension at baseline. It is unclear if randomization was stratified based on diagnosis of hypertension. Unable to extract data on hypertensive patients. |
| De A Santos 1995 | Compared garlic powder to garlic oil. No placebo comparator. Not all patients had hypertension at baseline. It is unclear if randomization was stratified based on diagnosis of hypertension. Unable to extract data on hypertensive patients. |
| Gardner 2001 | Patients did not have hypertension |
| Han 2011 | Patients with diagnosis of hypertension at baseline could not be separated from those with pre‐hypertension. Authors were contacted by email in June 2012 but sufficient detail was not provided. |
| Holzgartner 1992 | Compared garlic to bezafibrate. Not all patients had hypertension at baseline. It is unclear if randomization was stratified based on diagnosis of hypertension. Unable to extract data on hypertensive patients. |
| Isaacsohn 1998 | Only some (11/50) had a diagnosis of hypertension. We were unable to extract the data from the hypertensive patients. Randomization was not stratified based on blood pressure at baseline. |
| Jain 1993 | Patients did not have hypertension. |
| Kandaziora 1988 (2) | Compared garlic preparation to diuretic‐reserpin combination. No placebo comparator. |
| Kiesewetter 1993 | Of the 60 randomized patients, only 4 had hypertension at baseline and the data for these subjects are not reported separately. And even if randomization was stratified for hypertension, it was unlikely balanced between groups. |
| Kieswetter 1991 | Not all patients had hypertension at baseline. It is unclear if randomization was stratified based on diagnosis of hypertension. Unable to extract data on hypertensive patients. |
| Luley 1986 | Patients did not have hypertension. Lipid lowering trial. |
| Lutomski 1984 | Not all patients had a diagnosis of hypertension. Individual data for patients with hypertension could not be obtained. Garlic was given in combination with rutin, no rutin was given in the placebo arm. |
| Mansell 1996 | Basline BP data not available. Lipid lowering trial in diabetic patients. |
| McMahon 1992 | Identified through hand search of Simons S et al review in Netherlands Journal of Medicine 2009. In this review it was stated that "no numerical data provided." |
| Mousa 2007 | Not a randomized or crossover study. |
| Mrozikiewicz 1989 | Abstract only, no baseline data available |
| Ried 2010 | Enrolled people who were on a variety of other anti‐hypertensive prior to being randomized to garlic or placebo. More importantly, patients in both study groups were on different proportions of antihypertensives compared to each other (i.e. use of other classes was not standardized). Note: email communication with Dr. Ried on June 26 2012 confirmed that the uncontrolled hypertension group was categorized after the randomization process. Also confirmed that "Group allocation was randomized and double‐blinded and trial IDs provided to eligible patients in consecutive order as they enrolled." |
| Rotzsch 1992 | Patients did not have hypertension. |
| Saradeth 1994 | Patients did not have hypertension. |
| Satitvipawee 2003 | Lipid lowering trial, no blood pressure data available. |
| Schiewe 1995 | Lipid lowering trial, no blood pressure data available. |
| Simons 1995 | Patients did not have hypertension. |
| Sobenin 2007 | Patients had known coronary artery diease but information on hypertension and blood pressure data were not available. |
| Steiner 1996 | Not all patients had hypertension at baseline. It is unclear if randomization was stratified based on diagnosis of hypertension. Unable to extract data on hypertensive patients. |
| Superko 2000 | Patients did not have hypertension. |
| Turner 2004 | Patients did not have hypertension. |
| Vorberg 1990 | Not all patients had hypertension at baseline. It is unclear if randomization was stratified based on diagnosis of hypertension. Unable to extract data on hypertensive patients. |
| Williams 2005 | Ischemic heart disease patients, only some had hypertension but could not extract data for these patients. Randomization was not stratified based on hypertension |
| Zhang 2000 | Patients did not have hypertension. |
Contributions of authors
Sarah Stabler was be responsible for searching for trials, data extraction, data analyses, interpretation of data, and writing/editing of the final report.
Aaron M Tejani was be responsible for verifying analyses, interpretation of data, writing/editing of the final report.
Claire Fowkes was be responsible for searching for trials, data extraction, data analyses, interpretation of data.
Fong Hyunh was be responsible for searching for trials, data extraction, data analyses, interpretation of data.
Sources of support
Internal sources
None, Not specified.
External sources
None, Not specified.
Declarations of interest
None known.
New
References
References to studies included in this review
Auer 1990 {published data only}
- Auer W, Eiber A, Hertkorn E, Koehrle U, Lorenz A, Mader F, Merx W, Otto G, Schmidt‐Otto B, Taubenheim H. Hypertension and hyperlipidaemia: garlic helps in mild cases. Br J Clin Pract 1990;Supplement 69:3‐6. [PubMed] [Google Scholar]
Kandziora 1988 {published data only}
- Kandaziora J. Blood pressure and lipid lowering effect of garlic preparations in combination with a diuretic [Blutdruk‐ und lipidsenkende Wirkung eines Knoblauch‐Praparates in Kombination mit einem Diuretikum]. Artzliche Forschung 1988;35:1‐8. [Google Scholar]
References to studies excluded from this review
Barrie 1987 {published data only}
- Barrie S, Wright J, Pizzorno JE. Effects of garlic oil on platelet aggregation, serum lipids and blood pressure in humans. Journal of Orthomol Med 1987;2(1):15‐21. [Google Scholar]
Czerny 1996 {published data only}
- Czerny B, Sarnochowiec S. Clinical Investigations with a Garlic‐Lecithin Preparation [Klinishce Untersuchungen mit einem Knoblauch‐Lezithin‐Praparat]. Arztezellschrift for Naturheltvorfahren 1996;37(2):126‐136. [Google Scholar]
De A Santos 1993 {published data only}
- A Santos OS, Grunwald J. Effect of garlic powder tablets on blood lipids and blood pressure‐a six month placebo controlled, double blind trial. Br J Clin Res 1993;4:37‐44. [Google Scholar]
De A Santos 1995 {published data only}
- A Santos OS, Johns RA. Effects of garlic powder and garlic oil preparations on blood lipids, blood pressure and well‐being.. Br J Clin Res 1995;6:91‐100. [Google Scholar]
Gardner 2001 {published data only}
- Gardner CD, Chatterjee LM, Carlson JJ. The effect of a garlic preparation on plasma lipid levels in moderately hypercholesterolemic adults. Atherosclerosis 2001;154:213‐220. [DOI] [PubMed] [Google Scholar]
Han 2011 {published and unpublished data}
- Han CH, Liu JC, Lin YS, et al. Antihypertensive activities of processed garlic on spontaneously hypertensive rats and hypertensive humans. Botanical Studies 2011;52:277‐283. [Google Scholar]
Holzgartner 1992 {published data only}
- Holzgartner H, Schmidt U, Kuhn U. Comparison of the efficacy and tolerance of a garlic preparation vs. bezafibrate. Arzneimittelforschung 1992;42(12):1473–1477. [PUBMED: 1288512] [PubMed] [Google Scholar]
Isaacsohn 1998 {published data only}
- Isaacsohn JL, Moser M, Stein EA, Dudley K, Davey J, Liskov E, Black HR. Garlic Powder and Plasma Lipids and Lipoproteins. Arch Intern Med 1998;138:1189‐1194. [DOI] [PubMed] [Google Scholar]
Jain 1993 {published data only}
- Jain AK, Vargas R, Gotzkowsky S, McMahon FG. Can Garlic Reduce Levels of Serum Lipids? A Controlled Clinical Study. Am J Med 1993;94:632‐635. [DOI] [PubMed] [Google Scholar]
Kandaziora 1988 (2) {published data only}
- Kandziora J. Antihypertensive efficacy and tolerability of garlic preparations [Antihypertensive Wirksamkeit und Vertraglichkeit eines Knoblauch‐Praparates (Study 2)]. Artzliche Forschung 1988;35:1‐8. [Google Scholar]
Kiesewetter 1993 {published data only}
- Kiesewetter H, Jung F, Jung EM, Blume J, Mrowietz C, Birk A, Koscienly J, Wenzel E. Effects of garlic coated tablets in peripheral arterial occlusive disease. Clin Invetsig 1993;71(5):383‐386. [DOI] [PubMed] [Google Scholar]
Kieswetter 1991 {published data only}
- Kieswetter H, Jung F, Pindur EM, Mrowietz C, Wenzel E. Effect of garlic on thrombocyte aggregation, microcirculation and other risk factors. Int J Clin Pharmacol Therapy and Tox 1991;29(4):151‐155. [PubMed] [Google Scholar]
Luley 1986 {published data only}
- Luley C, Lehmann‐Leo W, Moller B, Martin T, Schwatrzkopf W. Lack of efficacy of dried garlic in patients with hyperlipoproteinemia. Arzneimittelforschung 1986;36(4):766‐8. [PubMed] [Google Scholar]
Lutomski 1984 {published data only}
- Lutomski J, Poznan, Polen. Clinical investigations of the therapeutic efficacy of Ilja Rogogg(R) garlic pills with rutin [Klinische Untersuchungen zur therapeutischen Wirksamkeit von Ilja Rogogg(r) Knoblauchpillen mit Rutin]. Zeutschrift fur Phytotherapie 1984;5(15):938‐942. [Google Scholar]
Mansell 1996 {published data only}
- Mansell P, Reckless JPD, Lloyd J, Leatherdale B. The Effect of Dried Garlic Powder Tablets On Serum Lipids in Non‐Insulin Dependent Diabetic Patients. Eur J Clin Res 1996;8:25‐26. [Google Scholar]
McMahon 1992 {published data only}
- McMahon FG, Jain A, Vargas R, Kadowitz P, McNamara D. Clinical Effects of a Garlic Powder Preparation on Various Cardiovascular Risk Factors. Eur J Clin Res 1992;3A:8‐9. [Google Scholar]
Mousa 2007 {published data only}
- Mousa AS, Mousa SA. Cellular effects of garlic supplements and antioxidants on high blood pressure in humans: pilot study. Nutr Res 2007;27(2):119‐123. [Google Scholar]
Mrozikiewicz 1989 {published data only}
- Mrozikiewicz VA, Lutomski J. Efficacy of Some Garlic Preparations. Pharmacological and Clinical Studies in Poland. [Wirkungseffekte einiger Knoblauchpraparate. Pharmakologische und klinische Untersuchungen in Polen]. Deutsche Apotheker‐Zeitung 1989;129:16. [Google Scholar]
Ried 2010 {published data only}
- Ried K, Frank OR, Stocks NP. Aged garlic extract lowers blood pressure in patients with treated but uncontrolled hypertension: A randomised controlled trial. Maturitas 2010;67:144‐150. [DOI] [PubMed] [Google Scholar]
Rotzsch 1992 {published data only}
- Rotzsch W, Richter V, Rassoul F, Walper A. Postprandial Lipamie with medication of Allium sativum [Postprandiale Lipamie unter Medikation von Allium sativum]. Lipidsenker Lipid Reducers 1992;42 (II)(10):1223‐1226. [PubMed] [Google Scholar]
Saradeth 1994 {published data only}
- Saradeth T, Seidl S, Resch KL, Ernst E. Does garlic alter the lipid pattern in normal volunteers?. Phytomedicine 1994;1:183‐185. [DOI] [PubMed] [Google Scholar]
Satitvipawee 2003 {published data only}
- Satitvipawee P, Indrabhakti S, Getn‐Gern P, Rawdaree P, Ratanasuwan, T, Viwatwongkasem C. No effect of garlic extract supplement on serum lipid levels in hypercholesterolemic subjects. J Med Assoc Thai 2003;86:750‐757. [PubMed] [Google Scholar]
Schiewe 1995 {published data only}
- Schiewe FP, Hein T, Koln. Garlic in hyperlipidemia [Knoblauch bei Hyperlipidamie]. Zeitschrift fur Phytotherapie 1995;16:343‐348. [Google Scholar]
Simons 1995 {published data only}
- Simons L, Balasubramaniam S, Konigsmark M, Parfitt A, Simons J, Peters W. On the effect of garlic on plasma lipids and lipoproteins in mild hypercholesterolaemia. Atherosclerosis 1995;113(2):219‐225. [DOI] [PubMed] [Google Scholar]
Sobenin 2007 {published data only}
- Sobenin IA, Prianishnikov VV, Kunnova LM, Rabinovich EA, Orekhov AN. Use of allicor to lower the risk of myocardial infarction (Article in Russian). Ter Arkh 2007;85(3):25‐28. [PubMed] [Google Scholar]
Steiner 1996 {published data only}
- Steiner A, Khan A, Holbert D, Lin R. A double‐blind crossover study in moderately hypercholesterolemic men that compared the effect of aged garlic extract and placebo administration on blood lipids. Am J Clin Nutr 1996;64(6):866‐870. [DOI] [PubMed] [Google Scholar]
Superko 2000 {published data only}
- Superko HR, Krauss RM. Garlic Powder, Effect on Plasma Lipids, Postprandial Lipemia, Low‐Density Lipoprotein Particle Size, High‐Density Lipoprotein Subclass Distribution and Lipoprotein(a). J Am Coll Cardiol 2000;35(2):321‐326. [DOI] [PubMed] [Google Scholar]
Turner 2004 {published data only}
- Turner B, Molgaard C, Marckmann P. Effect of garlic (Allium sativum) powder tablets on serum lipids, blood pressure and arterial stiffness in normo‐lipidaemic volunteers: a randomised, double‐blind, placebo‐controlled trial. Br J of Nutr 2004;92:701‐706. [DOI] [PubMed] [Google Scholar]
Vorberg 1990 {published data only}
- Vorberg G, Schneider B. Therapey with Garlic: Results of a Placebo‐Controlled, Double‐Blind Study. Br J Clin Pract 1009;68:7‐11. [PubMed] [Google Scholar]
Williams 2005 {published data only}
- Williams MJA, Sutherland WJF, McCormick MP, Yeoman DJ, Jong SA. Aged garlic extract improves endothelial function in men with coronary artery disease. Phytother Res 2005;19:314‐319. [DOI] [PubMed] [Google Scholar]
Zhang 2000 {published data only}
- Zhang XH, Lowe D, Giles P, Fell S, Board AR, Baughan JA, Connock MJ, Maslin DJ. A randomized trial of the effects of garlic oil upon coronary heart disease risk factors in trained male runners. Blood Caogul Fibrin 2000;11:67‐74. [DOI] [PubMed] [Google Scholar]
Additional references
Banerjee 2002
- Banerjee Sk, Maulik SK. Effect of garlic on cardiovascular disorders: a review. Nutr J 2002;1:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bongiorno 2008
- Bongiorno PB, Fratellone PM, LoGiudice P. Potential health benefits of garlic (allium staivum): a narrative review. Journal of Complement and Int Med 2008;5:1‐15. [Google Scholar]
CHEP 2008
- Canadian Hypertension Education Program (CHEP) Guidelines 2008. Available from: URL: http://hypertension.ca/chep/wp‐content/uploads/2008/03/2008‐chepspiral‐booklet‐final_jan28.pdf.
Chobanian 2003
- Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report.. JAMA 2003;289(19):2560‐2572. [DOI] [PubMed] [Google Scholar]
Harunobu 2001
- Harunobu A, Petesch B, Matsuura H, et al. Intake of garlic and its bioactive components. J Nutr 2001;131(3):955S‐962S. [DOI] [PubMed] [Google Scholar]
Jellin 2006
- Jellin Jm, Gregory PJ, Batz F, Hitchens K, et al. Garlic [Garlic]. Pharmacists Letter / Prescribers Letter Natural Medicine Comprehensive Database. 8th Edition. Stockton CA: Therapeutic Research Faculty, 2006:556‐61. [Google Scholar]
Lanzotti 2006
- Lanzotti V. The analysis of onion and garlic. J CHROMATOGR A 2006;1112(1‐2,21):3‐22. [DOI] [PubMed] [Google Scholar]
Matsuura 2001
- Matsuura H. Saponins in Garlic as Modifiers of the Risk of Cardiovascular Disease. J Nutr 2001;31(3):1000S‐1005. [DOI] [PubMed] [Google Scholar]
Musini 2009
- Musini V, Wright J. Factors Affecting Blood Pressure Variability: Lessons Learned from Two Systematic Reviews of Randomized Controlled Trials.. PLoS One 2009;4(5):e5673. [DOI: 10.1371/journal.pone.0005673] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rahman 2006
- Rahman K, Lowe G. Garlic and Cardiovasular Disease: A Critical Review. J Nutr. 2006;136:736S‐740S. [DOI] [PubMed] [Google Scholar]
Ried 2008
- Ried K, Frank OR, Stocks NP, et al. Effect of garlic on blood pressure: a systematic review and meta‐analysis. BMC Cardiovascular Disorders 2008;8(13):1‐12. [DOI: 10.1186/1471-2261-8-13] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rivlin 2001
- Rivlin R. Historical perspective on the use of garlic. J Nutr 2001;31(3):951S‐954S. [DOI] [PubMed] [Google Scholar]
Silagy 1994
- Silagy CA, Neil HA. A meta‐analysis of the effect of garlic on blood pressure. J Hypertens 1994;12:463‐468. [PubMed] [Google Scholar]
Timbo 2006
- Timbo BB, Ross MP, McCarthy PV, et al. Dietary supplements in a national survey: prevalence of use and reports of adverse events. Am Diet Assoc 2006;106:1966‐1974.. [DOI] [PubMed] [Google Scholar]
WHO 2003
- World Health Organization, International Society of Hypertension Writing Group. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens 2003;21:1983‐1992. [DOI] [PubMed] [Google Scholar]
Wright 2009
- Wright JM, Musini VM. First‐line drugs for hypertension. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD001841.pub2] [DOI] [PubMed] [Google Scholar]