

Abstract
Introduction:
Color Doppler and CT angiography are diagnostic methods commonly used to determine the degree of carotid stenosis.
Aim:
To evaluate how the degree of carotid stenosis determined by the Color Doppler correlates with the degree of stenosis determined by the CT angiography.
Material and Methods:
The study was designed as a retrospective study. It included 42 patients with carotid stenosis. From medical records we collected anamnestic data (gender, age and risk factors - hypertension, hyperlipidemia, diabetes, smoking and obesity) and the results regarding the degree of carotid stenosis determined by Color Doppler and CT angiography.
Results:
Out of the total number of patients (n=42), 73.8% were males and 26.2% were females. Average age of examined patients was 65.24±8.61. Most frequent risk factor of atherosclerosis was hypertension, followed by hyperlipidemia and smoking. NASCET grading distinguishes: first (0-29%), second (30-69%) and third (70-99%) degree of carotid stenosis. According to the Color Doppler evaluation findings, the second degree had 8 patients and 34 patients had the third degree of carotid stenosis. CT angiography have shown that 35 patients had third degree carotid stenosis, while 7 patients had the second degree carotid stenosis. In only one case results of evaluated methods differed regarding assessment of carotid stenosis. We have found that there is a significant positive correlation of the degree of carotid stenosis determined by the Color Doppler with the degree of stenosis determined by CT angiography (p=0.0002). Risk factors of atherosclerosis did not have a significant correlation with the degree of carotid stenosis (p>0.05).
Conclusion:
The degree of carotid stenosis estimated by the Color Doppler positively correlates with the degree of stenosis estimated by CT angiography.
Keywords: carotid stenosis, CT angiography, Color Doppler, atherosclerosis
1. INTRODUCTION
Stroke represents one of the leading causes of death in the world and a leading cause of disability within adult population (1). The cause of ischemic stroke may be thrombosis formed at the site of atherosclerotic plaque or thrombus embolization into the distal arteries of the cerebral circulation. Extracranial cerebrovascular diseases cause 75% of all ischemic stroke (2).
Carotid stenosis is a narrowing of carotid arteries, which is mainly a consequence of atherosclerosis and accumulation of atherosclerotic plaques in the carotid bifurcation and the initial part of the internal carotid artery. A timely diagnosis of the patient and reliable determination of the degree of carotid stenosis provides important step in the process of adequate treatment and prevention of stroke.
In clinical practice, determination of the degree of carotid stenosis by Color Doppler is based on the results of the two prospective studies The North American Symptomatic Carotid Endarterectomy Trial (NASCET) and European Carotid Surgery Trial (ECST). Even though they used different methods of measuring the degree of carotid stenosis, they have both shown that there is a significant benefit of carotid endarterectomy in patients with severe carotid stenosis (NASCET for stenosis of ≥70%; ECST for stenosis of ≥80%) in reducing the risk of stroke (3, 4).
Today, there are different diagnostic methods available for determining the degree of carotid stenosis and evaluation of the severity of the carotid stenosis, such as Color Doppler ultrasound examination, computed tomography angiography (CT angiography), magnetic resonance angiography (MRA) and digital subtraction angiography (DSA). The choice of diagnostic method depends on the indication and availability of these methods in the hospital. Today Color Doppler is used as an initial diagnostic method since it is readily available, cost-effective, and non-invasive. Since it is also partly a subjective method, interpretation of the carotid stenosis significantly depends on the opinion and experience of the physician, therefore, when Color Doppler verifies the presence of significant stenosis, it is advisable to perform additional diagnostic evaluation using CT angiography or MRA, which have replaced DSA. CT angiography provides tool for objective estimation of the degree of carotid stenosis and it has gained popularity in current clinical practice because it is a minimal invasive diagnostic procedure and gives reliable result about the condition of carotid arteries.
The use of different diagnostic methods may show mismatch in the estimation of the carotid stenosis degree, as may be the case with diagnostic evaluation of the patient by Color Doppler and CT angiography. In this study, we have compared the results of these two methods in estimation of the degree of carotid stenosis.
2. AIM
To examine whether the degree of carotid stenosis determined by Color Doppler ultrasound correlates with the degree of stenosis determined by CT angiography. Additional aims were to examine the correlation between the patient’s age and the occurrence of carotid stenosis, to examine whether more male or female patients suffer from carotid stenosis, to determine the frequency of risk factors in patients with carotid stenosis and to identify is there any association between the risk factors and degree of carotid stenosis.
3. MATERIAL AND METHODS
The study was designed as a retrospective, cross-sectional, observational study. Data for this study were collected from patient medical records of the Clinic for Cardiovascular Surgery of the Clinical Center University of Sarajevo.
We have included male and female patients who had a degree of carotid stenosis determined both by Color Doppler ultrasound and CT angiography. We analyzed data of 297 patients with carotid stenosis who were hospitalized at the Clinic during the period from 2014 to 2018. A total of 42 patients were included in this study. We have excluded from the study all patients with incomplete diagnostic results, all patients with fibromuscular dysplasia, giant cell arteritis, patients with malignancies, traumas and patients with previously surgically treated carotid stenosis. The following anamnestic data were collected: gender, age and risk factors for carotid stenosis (hypertension, hyperlipidemia, diabetes, smoking, and obesity). The diagnostic data referred to the degree of carotid stenosis determined by the Color Doppler and CT angiography. The degree of carotid stenosis was classified according to NASCET criteria into the first degree of carotid stenosis (0-29%), second degree (30-69%) and third degree (70-99%). All patients were examined using Color Doppler ultrasound, blood flow velocity parameters were measured, and the degree of stenosis was determined according to NASCET criteria. During CTA examination images of the cross-section of arteries were obtained, including the diameter at the site of maximum stenosis along with the diameter of distal normal arterial segment.
For statistical data analyses, we used Statistical Package for the Social Sciences (SPSS) program (version 25.0, IBM Corporation, New York, USA) and Microsoft Excel (version 16.24, Microsoft Corporation, Redmond, Washington, USA). The following methods were used: demographic statistics to describe the sample, X2 test and Fisher’s Exact Test to calculate the difference between individual risk factors with CT angiography findings. We have determined the correlation between the findings of Color Doppler and CT angiography using non-parametric Spearman’s correlation. P-value less than 0.05 represents a significant value (p<0.05).
4. RESULTS
A total of 42 patients diagnosed with carotid stenosis were included in the study, 31 males (73.8%) and 11 females (26.2%). The average age of the patients was 65.24±8.61 years. The youngest patients was 50 and the oldest 80 years old. Out of the total number of patients, the largest number of patients (n=20) were between 60-69 years of age, 14 were between 70-80 years of age and 8 were in the range 50-59 years of age.
An analysis of risk factors in the total sample (n=42) revealed that the majority of patients had hypertension (n=39; 92.9%). The second most common risk factor was hyperlipidemia (n=34; 81%), followed by smoking (n=18; 42.9%). 9 patients had diabetes (21.4%) and 15 patients were obese (35.7%) (Table 1).
Table 1. Distribution of risk factors in patients.
| Risk factors | N | % |
|---|---|---|
| Hypertension | 39 | 92.9% |
| Hyperlipidemia | 34 | 81.0% |
| Diabetes mellitus | 9 | 21.4% |
| Smoking | 18 | 42.9% |
| Obesity | 15 | 35.7% |
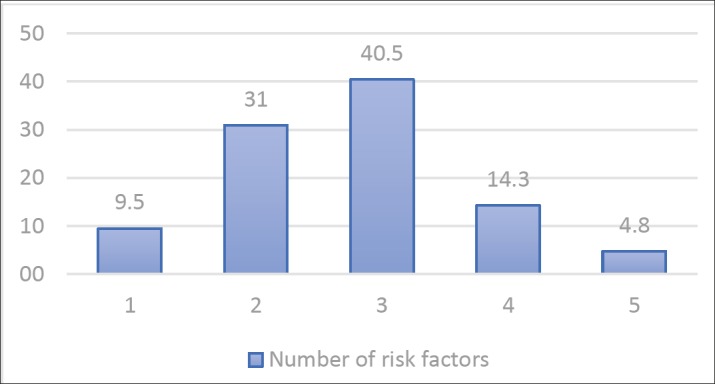
The analysis of risk factors of atherosclerosis have shown the following results: The highest number of patients had three risk factors (n=17; 40.5%), 13 patients had two risk factors (n=13; 31%), 6 patients had four risk factors (n=6; 14.3%), and 4 patients had only one risk factor (n=4, 9.5%). There were only 2 patients with all 5 risk factors (4.8%), while there were no patients without risk factors (Figure 1).
Figure 1. Distribution of the sum of risk factors.
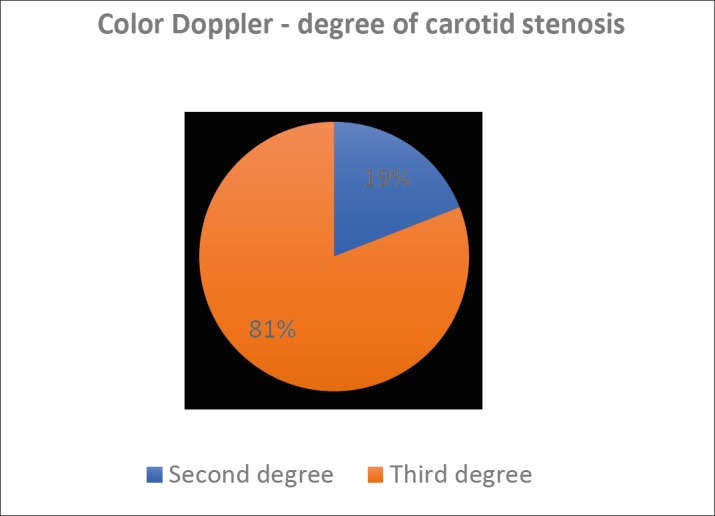
Analyzing the degree of carotid stenosis according to NASCET criteria as determined by Color Doppler we found that none of them had a first degree of stenosis, 8 patients (19%) had a second degree of stenosis, and 34 patients (81%) had a third degree of carotid stenosis (Figure 2). The average value of the degree of carotid stenosis determined by the Color Doppler was 77.97%.
Figure 2. Distribution of the degree of carotid stenosis according to Color Doppler.
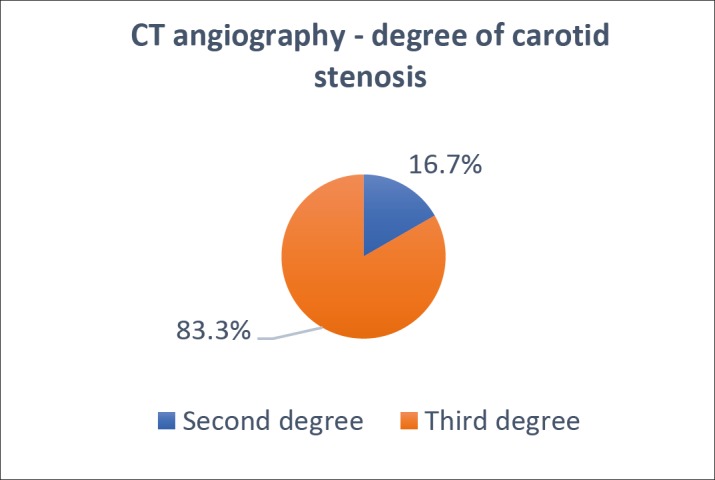
Analyzing the degree of carotid stenosis according to NASCET criteria determined by CT angiography in the total number of patients (n=42), we found that none of the patients had a first degree of stenosis, 7 patients (16.7%) had a second degree of stenosis, and 35 patients (83.3 %) had a third degree of carotid stenosis (Figure 3). The average value of carotid stenosis determined by CT angiography was 76.69%.
Figure 3. Distribution of the degree of carotid stenosis according to CT angiography.
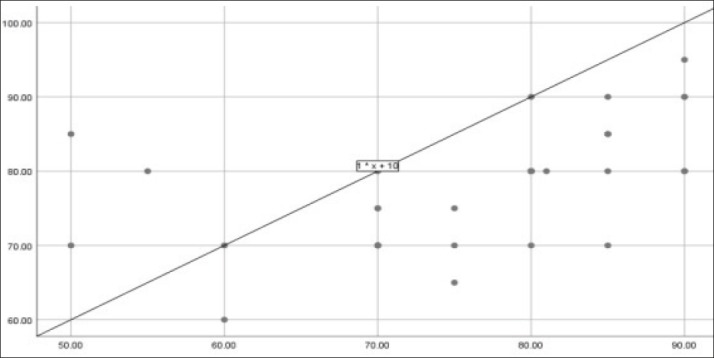
Comparing the degree of carotid stenosis estimated by Color Doppler with degree of stenosis determined by CT angiography, we have found that the correlation between Color Doppler examination and CT angiography was significantly positive, i.e., the degree of carotid stenosis estimated by Color Doppler and CT angiography significantly correlates (rho=0.536; p=0.0002) (Figure 4).
Figure 4. Correlation of CT angiography and Color Doppler.
Comparing the degree of carotid stenosis by risk factors, we found that there was no statistically significant correlation between risk factors and the degree of stenosis (p>0.05) (Table 2).
Table 2. The association of the risk factors with the degree of carotid stenosis.
| Risk factors | N | P value |
|---|---|---|
| Hypertension | 39 | 0.430 |
| Hyperlipidemia | 34 | 0.113 |
| Diabetes mellitus | 9 | 0.630 |
| Smoking | 18 | 0.438 |
| Obesity | 15 | 0.978 |
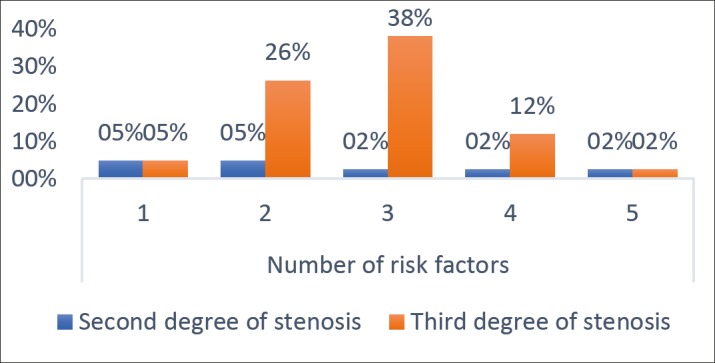
We also found that there was no statistically significant association between the sum of the risk factors present in patients and the degree of carotid stenosis χ2 (4, n=42)=6.239a, p=0.182 (Figure 5).
Figure 5. The association of the sum of risk factors with the degree of carotid stenosis.
5. DISCUSSION
In our study, gender analysis have shown that out of the total number of patients, 73.8% (n=31) were male and 26.2% female (n=11). A study that conducted Mathiesen et al have also pointed out that carotid stenosis caused due to atherosclerosis is more common in males than females (5). O´Leary et al concluded that carotid stenosis is more common in males, where 75% out of the total number of evaluated patients with carotid stenosis were male (6).
The average age of our patients was 65.24±8.61 which is similar with results of other authors who observed that advanced age is one of important risk factors for development of carotid stenosis (7, 8). Jackson et al, study included a group of patients with an average age of 68.4 years, but they observed that carotid stenosis caused by severe atherosclerosis is common among patients of 55 years and older (9).
The leading risk factor of atherosclerosis in our group of patients was hypertension, followed by hyperlipidemia and smoking. Other studies suggest that hypertension is one of the most present risk factors among patients diagnosed with carotid stenosis, while it is well known that hyperlipidemia favors the formation of atherosclerotic plaque and consequent narrowing of the carotid arteries (5, 10-12). Also, a high percentage of smokers in our study population (42.9%) strongly support findings of the past researches who observed that smoking causes thickening of the carotid artery wall along with the narrowing of the lumen of the arteries (13). Mathiesen et al, concluded that a higher incidence of carotid stenosis is related to advanced age, male sex, high blood pressure, hyperlipidemia, and smoking (5). Many other studies suggest that diabetes and obesity are increasing the risk of developing carotid stenosis and stroke (8).
We also analyzed whether these risk factors have correlation with the the degree of carotid stenosis, as well as whether there was an association between the number of risk factors present in patients and the value of the degree of carotid stenosis. The results have shown that risk factors, as well as the presence of their total number in the patients, did not have a statistically significant effect on the degree of carotid stenosis. Such results are comparable with the findings of other studies that evaluated the association of risk factors with the progression of carotid stenosis and which concluded that there was no correlation between the risk factors and the progression of the degree of carotid stenosis (14, 15).
In our research, we primarily analyzed the correlation of Color Doppler and CT angiography findings in their assessment of the degree of carotid stenosis. Comparing these two diagnostic methods we have observed a significant linear correlation between the degree of carotid stenosis assessed by Color Doppler followed by CT angiography (r=0.536; p=0.0002, p<0.05). The only mismatch of results between these two diagnostic methods was present in one case, where Color Doppler assessed second degree carotid stenosis (30-69%), while CT angiography finding stated it was carotid stenosis amounting to 70-99%. Numerous studies that have compared Color Doppler and CT angiography in the assessment of the degree of carotid stenosis indicated the high level correlation between these two methods. Vit et al examined a total of 35 carotid arteries, and in 91.6% cases where CT angiography detected the degree of stenosis higher than 60% Color Doppler showed the same result, while in cases where CT angiography showed stenosis less than 60%, Color Doppler assessed the same degree of stenosis in 89.5% cases (16). They concluded that these diagnostic methods significantly correlate in the evaluation of the degree of carotid stenosis, which is also consistent with our results. On the other hand, Titi et al examined a total of 187 carotid arteries with Color Doppler and CT angiography, and in 26 cases Color Doppler underestimated and in 13 cases overestimated the degree of carotid stenosis. They also concluded that Color Doppler is initial method for the diagnosis of carotid stenosis and reliably determines the degree of carotid stenosis, but they suggest that all doubts should be resolved by CT angiography because it has stood the test of time to be a reliable method of carotid stenosis assessment (17). Research that was conducted by Abul-Kasim also showed good correlation of CT angiography and Color Doppler in detection of the narrowing of the carotid arteries and in the estimation of the degree of carotid stenosis; it also concluded that these two diagnostic methods can be used separately or as complementary to each other in diagnosis of carotid artery disease (18). The results of our study are in agreement with the studies mentioned above since we have also proved that Color Doppler and CT angiography had positive correlation in the assessment of the degree of carotid stenosis.
There are some limitations to our study. First, the sample size was small, and a larger number of patients involved would raise the impact of this study. In addition to that, many different examiners performed color doppler examinations which increases the subjectivity of obtained results.
6. CONCLUSION
This This study confirmed that the majority of patients diagnosed with carotid stenosis are male and that the prevalence of patients diagnosed with carotid stenosis is higher in advanced age. We also confirmed that most common risk factors in patients diagnosed with carotid stenosis are hypertension, hyperlipidemia, and smoking and that there is no significant correlation between the presence of risk factors and the degree of carotid stenosis.
In this study, we have shown that the degree of carotid stenosis assessed by Color Doppler significantly correlates with the degree of carotid stenosis assessed by CT angiography. In modern clinical practice, the availability of the diagnostic methods in the hospitals plays an important role in the process of diagnosing carotid stenosis. CT angiography is a more expensive method than Color Doppler, but it is objective and accurate in determining the degree of carotid stenosis, while Color Doppler is a non-invasive and easily available diagnostic method. So, in everyday clinical practice, determining the degree of carotid artery stenosis and planning further actions regarding patient medical treatment can be reliably based on the use of Color Doppler. It would contribute to reducing the occurrence of complications by using CT angiography, such as adverse reaction to contrast agent and exposing patients to ionizing radiation. However, in cases where Color Doppler shows uncertain results, CT angiography remains a reliable method for determination of the degree of carotid stenosis.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent forms
Author’s contribution:
NR and MG gave a substantial contribution to the conception and design of the work and in the acquisition, analysis and interpretation of data for the work. NR had a part in drafting the work and revising it critically for important intellectual content. Each author gave final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of interest:
None declared.
Financial support:
None.
REFERENCES
- 1.European Registers of Stroke (EROS) Investigators. Heuschmann PU, Di Carlo A, Bejot Y, Rastenyte D, Ryglewicz D. Incidence of stroke in Europe at the beginning of the 21st century. Stroke. 2009;40:1557–1563. doi: 10.1161/STROKEAHA.108.535088. [DOI] [PubMed] [Google Scholar]
- 2.Rockman CB, Jacobowitz GR, Gagne PJ, Adelman MA, Lamparello PJ, Landis R, et al. Focused screening for occult carotid artery disease: Patients with known heart disease are at high risk. J Vasc Surg. 2004;39(1):44–51. doi: 10.1016/j.jvs.2003.07.008. [DOI] [PubMed] [Google Scholar]
- 3.Barnett HJM, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1998;339(20):1415–1425. doi: 10.1056/NEJM199811123392002. [DOI] [PubMed] [Google Scholar]
- 4.European Carotid Surgery Trialists’ Collaborative Group. Randomized trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST) Lancet. 1998;351(9113):1379–1387. [PubMed] [Google Scholar]
- 5.Mathiesen EB, Joakimsen O, Bonaa KH. Prevalence of and risk factors associated with carotid artery stenosis: the Tromso Study. Cerebrovasc Dis. 2001;12(1):44–51. doi: 10.1159/000047680. [DOI] [PubMed] [Google Scholar]
- 6.O’Leary D, Polak J, Kronmal R, Kittner S, Bond M, Wolfson S, et al. Distribution and correlates of sonographically detected carotid artery disease in the Cardiovascular Health Study. The CHS Collaborative Research Group. Stroke. 1992;23(12):1752–1760. doi: 10.1161/01.str.23.12.1752. [DOI] [PubMed] [Google Scholar]
- 7.Pinto A, Tuttolomondo A, Di Raimondo D, Fernandez P, Licata G. Cerebrovascular risk factors and clinical classification of strokes. Seminars in Vascular Medicine. 2004;4(3):287–303. doi: 10.1055/s-2004-861497. [DOI] [PubMed] [Google Scholar]
- 8.Prasad K. Pathophysiology and Medical Treatment of Carotid Artery Stenosis. International Journal of Angiology. 2015;24(03):158–172. doi: 10.1055/s-0035-1554911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jackson VP, Bendick PJ. Duplex ultrasound screening for carotid arteriosclerotic disease in asymptomatic patients. J Ultrasound Med. 1985;4(8):411–415. doi: 10.7863/jum.1985.4.8.411. [DOI] [PubMed] [Google Scholar]
- 10.Prati P, Vanuzzo D, Casaroli M, Di Chiara A, De Biasi F, Feruglio GA, et al. Prevalence and determinants of carotid atherosclerosis in a general population. Stroke. 1992;23(12):1705–1711. doi: 10.1161/01.str.23.12.1705. [DOI] [PubMed] [Google Scholar]
- 11.Kerenyi L, Mihalka L, Csiba L, Bacso H, Bereczki D. Role of hyperlipidemia in atherosclerotic plaque formation in the internal carotid artery. Journal of Clinical Ultrasound. 2006;34(6):283–288. doi: 10.1002/jcu.20233. [DOI] [PubMed] [Google Scholar]
- 12.Duncan G, Lees R, Ojemann R, David S. Concomitants of atherosclerotic carotid artery stenosis. Stroke. 1977;8(6):665–669. doi: 10.1161/01.str.8.6.665. [DOI] [PubMed] [Google Scholar]
- 13.Tell G, Polak J, Ward B, Kittner S, Savage P, Robbins J. Relation of smoking with carotid artery wall thickness and stenosis in older adults. The Cardiovascular Health Study. Circulation. 1994;90(6):2905–2908. doi: 10.1161/01.cir.90.6.2905. [DOI] [PubMed] [Google Scholar]
- 14.Garvey L, Makaroun M, Muluk V, Webster M, Muluk S. Etiologic factors in progression of carotid stenosis: A 10-year study in 905 patients. Journal of Vascular Surgery. 2000;31(1):31–38. doi: 10.1016/s0741-5214(00)70065-6. [DOI] [PubMed] [Google Scholar]
- 15.Liapis C, Kakisis J, Papavassiliou V, Ntanou A, Kontopoulou S, Kaperonis E, et al. Internal Carotid Artery Stenosis: Rate of Progression. European Journal of Vascular and Endovascular Surgery. 2000;19(2):111–117. doi: 10.1053/ejvs.1999.0951. [DOI] [PubMed] [Google Scholar]
- 16.Vit A, de Candia A, Piccoli G, Como G, Pielizzo F, Bazzaocchi M. Color-Doppler sonography vs CT-angiography in discriminating carotid atherosclerotic plaques for surgical treatment. A prospective study. Radiol Med. 2003;106(4):382–390. [PubMed] [Google Scholar]
- 17.Titi M, George C, Bhattacharya D, Rahi A, Woodhead P, Stevenson W, et al. Comparison of carotid Doppler ultrasound and computerised tomographic angiography in the evaluation of carotid artery stenosis. The Surgeon: journal of the Royal Colleges of Surgeons of Edinburgh and Ireland. 2007;5(3):132–136. doi: 10.1016/s1479-666x(07)80039-4. [DOI] [PubMed] [Google Scholar]
- 18.Abul-Kasim K. CT-angiography and doppler ultrasonography in atherosclerotic carotid artery disease. A comparative study. The New Iraqi Journal of Medicine. 2009;5(3):35–40. [Google Scholar]