

Abstract
Lumbar spinal stenosis (LSS) affects more than 200 000 adults in the United States, resulting in substantial pain and disability. It is the most common reason for spinal surgery in patients over 65 years. Lumbar spinal stenosis is a clinical syndrome of pain in the buttocks or lower extremities, with or without back pain. It is associated with reduced space available for the neural and vascular elements of the lumbar spine. The condition is often exacerbated by standing, walking, or lumbar extension and relieved by forward flexion, sitting, or recumbency. Clinical care and research into lumbar spinal stenosis is complicated by the heterogeneity of the condition, the lack of standard criteria for diagnosis and inclusion in studies, and high rates of anatomic stenosis on imaging studies in older people who are completely asymptomatic. The options for non-surgical management include drugs, physiotherapy, spinal injections, lifestyle modification, and multidisciplinary rehabilitation. However, few high quality randomized trials have looked at conservative management. A systematic review concluded that there is insufficient evidence to recommend any specific type of non-surgical treatment. Several different surgical procedures are used to treat patients who do not improve with non-operative therapies. Given that rapid deterioration is rare and that symptoms often wax and wane or gradually improve, surgery is almost always elective and considered only if sufficiently bothersome symptoms persist despite trials of less invasive interventions. Outcomes (leg pain and disability) seem to be better for surgery than for non-operative treatment, but the evidence is heterogeneous and often of limited quality.
Introduction
Lumbar spinal stenosis (LSS) is a degenerative condition in which changes in the discs, ligamentum flavum, and facet joints with aging cause narrowing of the spaces around the neurovascular structures of the spine. These changes lead to pain in the legs and back, as well as impaired ambulation and other disabilities.1
LSS is the most common indication for spinal surgery in people older than 65 years.2 However, there is no single objective standard for identifying LSS and diagnosis relies on complex judgments that integrate symptoms, signs, imaging findings, and comorbid conditions. Clinical care and research in LSS are complicated by the heterogeneity of the condition and the lack of standard criteria for diagnosis and for inclusion in studies.3
Central stenosis with associated neurogenic claudication, lateral stenosis with radiculopathy, and combined syndromes are sometimes included under the label of LSS or evaluated separately, which can make interpretation of the literature challenging. Similarly, subgroups of LSS can be lumped together to create heterogeneous cohorts. Such subgroups include—but are not limited to—LSS related to degenerative changes but with normal spinal alignment, LSS associated with isolated degenerative spondylolisthesis, and LSS with some associated degenerative scoliosis. Recent studies have begun to focus on more clearly defined cohorts but much more work is needed to obtain the most clinically relevant data to guide care. The aims of this review are to organize and summarize the vast and diverse literature on the diagnosis and management of LSS. The impact of this condition is expected to grow as the aging population rises, while overall the available evidence remains of low to moderate quality at best.
Incidence and prevalence
LSS affects more than 200 000 people in the United States, resulting in substantial pain and disability, and it is the most common reason for spinal surgery in patients over 65 years.4 In 2007 more than 37 000 laminectomies for spinal stenosis were performed in Medicare alone with an aggregated hospital bill for these procedures of nearly $1.65bn (£1.1bn; €1.55bn).5 Data from the national ambulatory medical care survey and the National Spine Network indicate that 13-14% of patients with low back problems who see a specialist and 3-4% who see a general physician may have spinal stenosis.6 In the Framingham population study, 19-47% of Americans over age 60 had evidence of anatomic spinal stenosis on cross sectional imaging, depending on the criteria used.7 The prevalence of diagnosed LSS is expected to continue to increase with the aging of the population and increased use of advanced imaging.8
Sources and selection criteria
We searched the Cochrane Library and PubMed database using the search term “lumbar spinal stenosis”, with a filter for systematic reviews in PubMed. We identified systematic reviews published from January 2000 to May 2015 and screened the reference lists from these reviews for additional relevant articles. Clinical articles with lumbar spinal stenosis in the title were considered for inclusion. The breadth of the topic precluded a formal systematic review.
Definition
LSS may have been described as early as the 1880s,9 but the modern description dates back to 1949, when Verbiest reported “a particular form of narrowing of the lumbar vertebral canal not associated with any other anomaly of the spine . . . On walking and standing these patients presented signs of disturbance of the cauda equina: bilateral radicular pains, disturbances of sensation and impairment of motor power in the legs. When the patient was recumbent the symptoms immediately disappeared and neurological examination during rest revealed nothing abnormal . . . Myelography showed a block with the appearance of extradural compression.”10 LSS is currently recognized as “a clinical syndrome of buttock or lower extremity pain, which may occur with or without back pain, associated with diminished space available for the neural and vascular elements in the lumbar spine” associated with certain characteristic provocative and palliative features.11
Causes
In LSS a narrowing of the central spinal canal, lateral recesses, or intervertebral foramen (or a combination thereof) causes compression of associated neurovascular structures. LSS can be classified as congenital (developmental) or acquired (or both).
Congenital stenosis is an uncommon condition (2.6-4.7% in the Framingham study),7 which involves spinal canal narrowing caused by abnormalities or disorders in postnatal development.12 Most cases of LSS are degenerative, resulting from changes in the spine with aging.13 Changes of the spine that may lead to LSS include facet joint hypertrophy, loss of intervertebral disc height, disc bulging, osteophyte formation, and hypertrophy of the ligamentum flavum (fig 1).
Fig 1 .
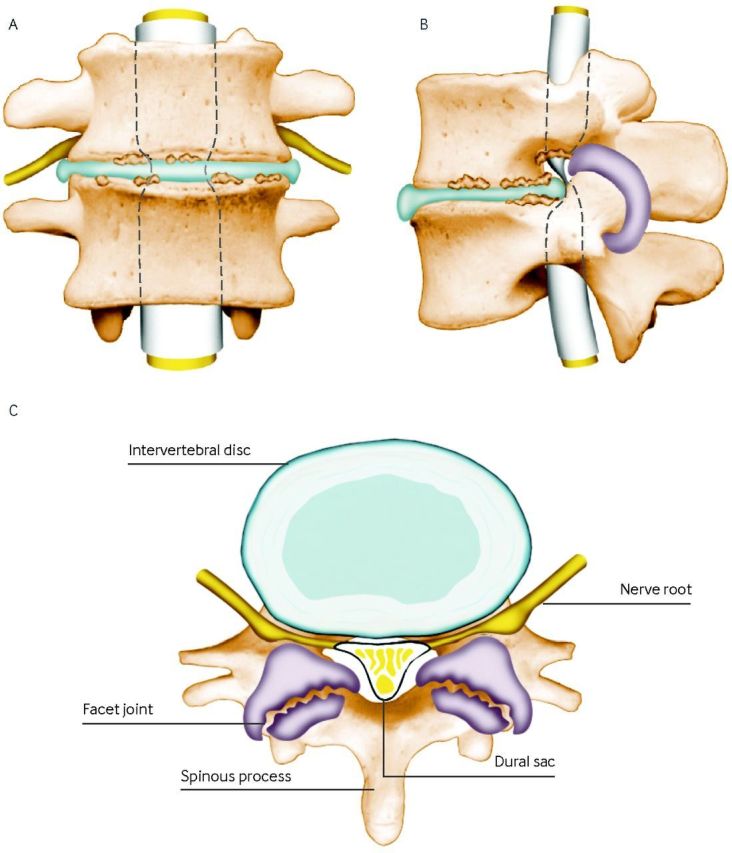
Degenerative spinal stenosis: frontal (A), sagittal (B), and axial views (C). Thickening of the tissue surrounding the dural sac is shown in purple. The axial figure depicts only a relatively minor degree of stenosis to allow visualization of the different structures. Reproduced with permission from the department of orthopedic surgery at Dartmouth-Hitchcock Medical Center
It has been suggested that the degenerative process underlying stenosis often begins with changes in the intervertebral discs (loss of disc height and bulging) and then moves to the facet joints.14 Acquired degenerative stenosis can also be caused by excess scar tissue or proliferation of bone after surgery, or as a result of infection or trauma.12 Although anatomic narrowing of the spinal canal or foramen is a necessary component of LSS, it is not sufficient for the clinical syndrome to be expressed—the degree of narrowing must be such that the compression of the neurovascular structures compromises nerve or vascular function.13
LSS also has an important dynamic component.15 The association between standing or walking and leg symptoms and relief of symptoms when sitting down or bending forward correlate with dynamic changes in the spine with positioning. This is because extension of the lumbar spine reduces the size of the lumbar spinal canal, as does axial loading.16 These changes occur in normal spines and the effects are magnified in degenerated spines with baseline narrowing.17
Symptoms and signs
Pain is often the main symptom and main reason for seeking care.18 19 20 The most common sites of reported pain are the lower back, buttocks, thighs, and legs. The discomfort associated with LSS is often described as a cramping or burning feeling.13 Symptom patterns vary from a gradual onset of dull aching pain in the sacroiliac area and posterolateral thighs to sharp radicular pain in the thighs, legs, and feet.21 In people with central canal LSS the pain may be bilateral but usually not entirely symmetrical. By contrast, patients with exclusively foraminal or lateral recess stenosis often report symptoms resembling unilateral radiculopathy.22
Patient also commonly report problems with balance,23 sensory loss (numbness or tingling), and weakness of the muscles of the lower extremities.19 24 Patients with LSS nearly always have low back pain, but low back pain alone, with no leg symptoms, is usually not thought to be caused by LSS even in the presence of severe anatomic stenosis, although in some cases this is controversial. Nearly all the studies considered here required patients to have leg symptoms, either neurogenic claudication or radicular pain, and confirmation of stenosis by imaging.
The cardinal manifestation and most specific symptom of central LSS is neurogenic claudication.25 Neurogenic claudication consists of the progressive onset of pain, numbness, weakness, and tingling in the low back, buttocks, and legs, which is initiated by standing, walking, or lumbar extension.26 Symptoms are posture dependent, appearing with standing and lumbar extension, exacerbated by walking, and relieved by sitting or forward flexion.21 The “shopping cart sign,” with the patient walking in a flexed or stooped position to relieve or reduce symptoms, is a common indicator of neurogenic claudication. This stooped posture or the inability to stand fully upright may be the presenting problem.
A key diagnostic challenge is differentiating neurogenic claudication caused by LSS from vascular claudication related to peripheral vascular disease, both of which present with leg pain during walking. In general, the distinction centers around the difference between exacerbation of symptoms with posture versus exertion. Patients with vascular claudication often improve with rest while standing, whereas those with neurogenic claudication need to sit down or lean over. A recent study found that the combination of triggering of symptoms with standing, relief with sitting, symptoms located above the knees, and a positive shopping cart sign provided strong evidence for neurogenic claudication (likelihood ratio of 13). Conversely, the alleviation of symptoms with standing (stopping walking but remaining upright) and symptoms located below the knees provided strong evidence for vascular claudication (likelihood ratio of 20).27
The symptoms of LSS can have a substantial impact on mobility, functional autonomy, and performance (physical activity in daily life). Most people with symptomatic LSS have limited walking capacity; they may require walking aids and may even avoid walking altogether.28 29 30 31 This limitation can have repercussions for overall health and physical performance, with most patients exhibiting varying degrees of sedentary behavior.32
Natural course of LSS
The natural course of untreated LSS is largely unknown, given that most people with the condition, particularly those with severe symptoms, seek some sort of treatment.33 However, the frequent misconception that LSS is a “degenerative” condition that inexorably worsens over time is not supported by evidence.
The North American Spine Society (NASS) clinical guidelines concluded that the natural course is favorable in a third to a half of patients with clinically mild to moderate LSS.11 Other reviews suggest that the condition may deteriorate in some patients and improve in about a third, with most patients remaining unchanged for up to eight years of follow-up.33 34 35 Rapid or catastrophic neurological decline seems to be rare in mild to moderate stenosis.11 A recent study that followed 34 patients with LSS diagnosed by magnetic resonance imaging for 10 years concluded that 60% of patients did not progress dramatically, despite progressive anatomic changes.36 Others suggest that clinical spinal stenosis is a fluctuating and potentially improving continuum,37 where the current function of patients predicts their future function.
Pathophysiology
The physiological mechanism behind neurogenic claudication is unclear. The two main theories are the ischemic theory and the venous stasis theory,13 which are both based to some degree on the mechanical compression of nervous and vascular structures during lumbar extension.
The ischemic theory suggests that compression of the microvasculature causes nerve root ischemia, which leads to symptoms including paresthesias, pain, and weakness.38 39 By contrast, the venous stasis theory suggests that the underlying mechanism is inadequate oxygenation and accumulation of metabolites in the cauda equina due to venous pooling in multilevel stenosis.26 40 41 In addition to neurogenic claudication, LSS may present with postural aggravation of radiculopathy as a direct result of compression of the neural elements.42 Of note, there is no strong evidence for acute inflammation as a cause for the symptoms of spinal stenosis.43
As discussed in more detail below, anatomic narrowing and neurovascular compression are fundamental to the pathogenesis of LSS; however, these imaging findings are often seen in asymptomatic people and the association between anatomic narrowing and clinical symptoms is unclear.44 Similarly, symptoms typically wax and wane over time, whereas the degree of anatomic narrowing, with the exception of the dynamic components related to posture, remains relatively stable or gradually worsens over time.
A possible link between venous congestion from cardiovascular disease and symptoms of stenosis has been suggested.45 Overall, the lack of a detailed understanding of the underlying pathophysiology linking anatomic stenosis to patients’ symptoms remains a key barrier to advancing research and clinical care in LSS.
Diagnosis
There is no objective standard for the clinical diagnosis of LSS.46 In the absence of valid objective criteria it has been suggested that expert opinion be considered the “gold standard” in diagnosis.29 The clinical syndrome of LSS is generally diagnosed using a combination of clinical signs from the history, physical examination, and imaging.47
The most useful findings from the history are age, radiating leg pain that is exacerbated by standing up or walking, the absence of pain when seated, the improvement of symptoms when bending forward, and a wide based gait.48 Balance impairment, neuromuscular deficits in the lower extremities including decreased strength (weakness), sensory deficits (numbness), and absent or decreased reflexes (Achilles tendon and patellar) are also highly associated with LSS.29 Although neurogenic claudication is the cardinal symptom of LSS, it is usually seen when a patient is walking. In the past, observational tests of walking have not been used in clinical diagnosis, but this type of assessment is becoming more popular when assessing functional capacity. Tests used for this purpose include treadmill protocols,31 49 50 51 52 53 54 55 the gait loading test,56 and the self paced walking test.55 Tests of lumbar extension loading have also been proposed for use in the diagnosis of LSS.57
Researchers have also recently begun to assess the impact of LSS on daily physical activities and on gait characteristics using accelerometry. Preliminary reports suggest that changes in gait parameters, including postural sway, associated with claudication during continuous walking, can be detected using accelerometers.58 Although the gait and performance parameters specific to LSS have yet to be fully defined, these techniques may be useful for diagnosis in the future.59
Electrodiagnostics
Electrodiagnostic methods including electromyography may also be used in the differential diagnosis of LSS,60 and in assessing the physiological consequences of stenosis. Electromyography is not used routinely but is most useful when the clinical picture and imaging results do not correlate and in differentiating the condition from diseases with a similar presentation, including peripheral vascular disease (vascular claudication), hip osteoarthritis, and spinal cord lesions.61
One quantitative electromyographic protocol called paraspinal mapping has been shown to be useful in the diagnosis of LSS, showing statistically significant differences between people with clinical stenosis and those with mechanical back pain and asymptomatic volunteers.62 In one study, this technique was found to be 93% sensitive in the diagnosis of radiologically confirmed symptomatic LSS.63 A recent study focusing on lateral stenosis found that paraspinal electromyographic findings correlate significantly with lateral stenosis seen on magnetic resonance imaging (MRI) and with patient symptoms, including pain and disability.64 This study concluded that electromyography may be useful in detecting lateral LSS.
However, several other conditions can increase paraspinal mapping scores, including inflammatory radiculopathy, polyneuropathy, myopathy, motor neuron diseases, and previous surgery, thereby decreasing the specificity in clinical practice.63 To date, the diagnostic accuracy of other techniques, including dermatomal somatosensory evoked potentials and magnetic stimulation remain unclear.48
Imaging
Current LSS guidelines state that imaging provides the most definitive diagnostic information for patients with symptoms thought to be related to LSS.48 Yet imaging is generally reserved for diagnostic confirmation and procedure planning for patients considering invasive interventions for LSS rather than as a routine part of the initial evaluation.
MRI, which allows examination of the size, shape, and anatomic associations between spinal and neural elements,21 is currently the recommended method for confirming the diagnosis of LSS.48 Computed tomography is recommended when MRI is contraindicated or unavailable. MRI is used because of its outstanding soft tissue contrast, but a systematic review found no evidence that it was more accurate than computed tomography in the diagnosis of LSS.65 Myelography has been used extensively in the past, but it is not recommended because it is invasive and is no more accurate than MRI.48
Although a Delphi study conducted in 2012 found that there are no standard quantitative criteria for defining anatomic LSS on imaging,66 a systematic review found 10 parameters that are currently used to quantify LSS.67 The parameters reported most often for central stenosis were anteroposterior diameter (<10 mm) and cross sectional area (<70 mm2) of the spinal canal, whereas height and depth of the lateral recess were measured for lateral stenosis and neuroforaminal diameter for foraminal stenosis.67 The two qualitative imaging criteria rated most important as diagnostic indicators in the Delphi study were disc protrusion and perineural intraforaminal fat.66 A study conducted to determine clinically relevant MRI measurements at the spinal level defined developmental LSS as anteroposterior diameter of <20 mm at L1, <19 mm at both L2 and L3, <17 mm at L4, and <16 mm at L5 and S1.68
A review found that MRI had a sensitivity of 87-96% and specificity of 68-75% for the diagnosis of LSS.69 One study found that MRI showed substantial reliability for assessment of the central canal, but poor to substantial reliability for assessment of the subarticular and foraminal zones, respectively.70 Newer semi-quantitative grading schemes based on dural sac morphology and the relation of cerebrospinal fluid to nerve roots in the central canal have shown initial promise for assessing the severity of LSS.71 72
Recent research has found that the “sedimentation sign”—the absence of posterior nerve root settling on supine MRI—has excellent reliability and may be useful in the diagnosis of severe LSS, although more research is needed to fully understand its role in the evaluation of LSS.73 74 75 A systematic review identified 14 different qualitative and semi-quantitative criteria that have been used with remarkable variability in individual definitions.76 Standardization and vigorous evaluation of the clinical and prognostic significance of imaging parameters with respect to treatment outcomes should be a high research priority.77
Although the presence of anatomic narrowing and neurovascular compression on imaging is needed for the diagnosis of LSS, it is not sufficient. Spinal stenosis is a clinical syndrome, not an anatomic or radiological finding. An estimated 21% of people with anatomic stenosis on MRI are asymptomatic.78 In fact, although a large proportion of older people show some degree of spinal stenosis on imaging, most are symptom free.78 Imaging must therefore be combined with history and clinical presentation before a diagnosis can be made.13 46
To date, research on the relation between clinical symptoms and findings on imaging has produced inconsistent results, with some studies finding an association,49 and others not.52 79 80 81 82 The lack of association might partly be explained by most imaging studies being conducted with the patient supine, whereas symptoms of LSS generally present during standing or walking.46 Nonetheless, the exact mechanism by which a constrained canal or nerve foramina manifests itself in symptoms has yet to be elucidated.
Clinical prediction rules
Three clinical prediction rules have been developed for LSS.83 84 85 86 A systematic review found that older age, pain with standing and walking, and relief with sitting or bending were common independent predictors of LSS across all prediction rules.87 Only one of these prediction rules has been validated.84 85 Using this tool, a score of 7 or more provides a positive likelihood ratio of just 1.6 (95% confidence interval 1.3 to 2.0), suggesting that this rule would have little effect in clinical practice.87
A consensus on criteria to define and classify lumbar spinal stenosis is needed.48 Preliminary findings from a Delphi study involving an international group of 68 experts suggest that the six most important factors in the diagnosis of LSS are “leg pain while walking,” “flex forward while walking to relieve symptoms,” “sit down or bend forward to relieve pain,” “normal foot pulses,” “relief with rest, and “lower extremity weakness.”88
Management
Non-surgical options
The many options for non-surgical management of LSS include drugs, physiotherapy, spinal injections, lifestyle modification, and multidisciplinary rehabilitation. Few high quality randomized trials have investigated these non-operative management strategies for LSS. A systematic review published in 2013 on non-operative treatments for patients with neurogenic claudication and imaging confirmed LSS concluded that there was insufficient evidence to recommend any specific type of non-surgical treatment for LSS.89 It also concluded that a lack of clear descriptions of non-surgical treatment protocols hinders proper analysis of treatment outcomes. There is a clear need for large well designed trials examining different non-surgical management strategies for LSS, with clearly articulated treatment protocols. Several ongoing trials may provide greater insight to guide appropriate recommendations. One trial is comparing usual medical care with individualized manual therapy and rehabilitative exercise versus community based group exercise.90 The other is examining the effects of a pedometer and nutrition lifestyle intervention compared with usual care.91 92
Despite the lack of consensus around treatment recommendations, most patients who seek care for neurogenic claudication are treated conservatively, and a course of conservative treatment is typically recommended before surgical intervention.89 The main categories of non-surgical treatment are drugs, physiotherapy, and injections.
Drugs
Although various over-the-counter and prescription drugs are used to treat LSS, the evidence to guide choices is limited. Single small trials suggest that some drugs, including prostaglandins, gabapentin, and vitamin B1 improve pain and walking distance, although evidence is of low or very low quality.90 Evidence from several small trials and a recent meta-analysis suggests that calcitonin is no better than placebo or acetaminophen (paracetamol) in the treatment of LSS.93 94 95 96
Given their analgesic and anti-inflammatory properties, non-steroidal anti-inflammatory drugs (NSAIDs) ought to be effective in LSS, but the evidence suggests they are no more effective than acetaminophen.25 97 Opioids and muscle relaxants are also prescribed for pain control in LSS, although they have not been shown to be more effective than acetaminophen or NSAIDs in well controlled studies.25 97
The role of long term opioid use in LSS is currently unclear.25 It has also been suggested that prostaglandin E1 may improve symptoms by improving blood flow to the cauda equina and nerve roots through vasodilation and antiplatelet aggregation effects. A recent review concluded that overall prostaglandin E1 improved clinical outcome measures including pain, Japanese Orthopedic Association score, and walking distance, although most of the studies had only short term follow-up.98
Finally, although both corticosteroids and antidepressants are often prescribed for patients with LSS, their efficacy remains unclear because of the lack of well controlled studies.
Physiotherapy
Physiotherapy is an accepted treatment for LSS. Physiotherapy related treatments include, but are not limited to:
Exercise (aerobic, strength, flexibility)
Specific exercises in lumbar flexion (cycling)
Body weight supported treadmill walking
Muscle coordination training
Balance training
Lumbar semi-rigid orthosis
Braces and corsets
Pain relieving treatments (heat, ice, electrical stimulation, massage, ultrasound)
Spinal manipulation
Postural instruction.
One study found that treatments most commonly used by patients are massage (27%), strengthening exercises (23%), flexibility exercises (18%), and heat or ice (14%), whereas physiotherapists most often advocate flexibility exercises (87%), stabilization exercises (86%), strengthening exercises (83%), heat or ice (76%), acupuncture (63%), and joint mobilization (62%).99
Unfortunately, there has been very little rigorous research into the efficacy of physiotherapy for LSS. A recent systematic review of non-operative treatments for patients with neurogenic claudication and imaging confirmed LSS found low quality evidence from a single trial that exercise provides short term benefit for leg pain and function compared with no treatment.93 The review also found that walking and stationary cycling provide similar, limited results. No trials have shown a strong effect of physiotherapy on walking capacity or performance. To date, evidence that physiotherapy is better than no treatment, oral diclofenac (non-steroidal anti-inflammatory) plus home exercises, or combined manual therapy plus exercise at improving walking ability is of very low to low quality.93
A systematic review published in 2013 found that no conclusions could be drawn about which physiotherapy treatments are best for LSS.100 The review found low quality evidence that physiotherapy interventions have no additional effect over exercise alone.100 When physiotherapy was compared with surgical interventions, surgery led to better long term (two year) outcomes for pain and disability but not walking distance.
Finally, a secondary analysis of the non-randomized Spine Patient Outcomes Research Trial (SPORT) found that use of physiotherapy was associated with no improvement in pain but some improvement in self reported physical function and a reduced likelihood of patients receiving surgery within one year.101
A subsequent randomized trial published in 2015 compared surgical decompression with a standardized physiotherapy regimen of lumbar flexion, conditioning exercises, and patient education.102 It found no difference in results at one or two years; however, 57% of the patients assigned to physiotherapy crossed over to surgery, which made it difficult to interpret the effects of physiotherapy.
Given the dynamic aspects of posture relative to spinal canal diameter, flexion exercise may improve the underlying pathophysiology of LSS; alternatively, the main role of physiotherapy may be to improve patients’ function with LSS rather than improve the LSS itself. Although the therapeutic effects may not be manifested at the level of the spinal pathology directly, the effects of these interventions may be sufficient to meet the goals and expectations of some patients with LSS. To this end, preliminary results from an ongoing randomized controlled trial (RCT) investigating a lifestyle intervention for LSS suggest that increased physical activity and weight loss may improve function and reduce symptoms in people with LSS. Although the mechanisms of these effects are unclear, this type of treatment warrants further investigation.
Injections
The results of trials on the effects of epidural injections for LSS vary. A systematic review published in 2013 found very low quality evidence from a single trial that epidural steroid injections improve pain, function, and quality of life for two weeks after injection when compared with home exercise or inpatient physiotherapy.103 However, two trials showed no effect compared with placebo.103 A more recent meta-analysis published in 2015 found that epidural steroid injections provide limited short term and long term improvement in pain and walking distance in patients with LSS.104 Minimal evidence shows that epidural steroid injections are better than local anesthetic injections alone, regardless of the mode of epidural injection.104 Another review of injections for central LSS concluded that epidural injections with local anesthetic alone, or local anesthetic with steroids, offer some relief of low back pain and lower extremity pain for central LSS. It also suggested that the interlaminar approach is superior to the caudal approach although the caudal approach is superior to the transforaminal one.105
A randomized trial published in 2014 that investigated epidural injections for LSS received much attention in the media and in the scientific community.106 This large double blinded controlled trial found no evidence of a treatment effect at six weeks with injection of glucocorticoids plus lidocaine, compared with lidocaine alone. These results suggest that the addition of glucocorticoids does not improve short term outcome, although it can increase the risks, as highlighted by an outbreak of fungal meningitis caused by contamination of a steroid preparation used for epidural injections.107 The most recent systematic review found immediate improvements in pain and function with epidural corticosteroid injections for radiculopathy but limited evidence of a lack of effectiveness in spinal stenosis (fig 2).108
Fig 2.
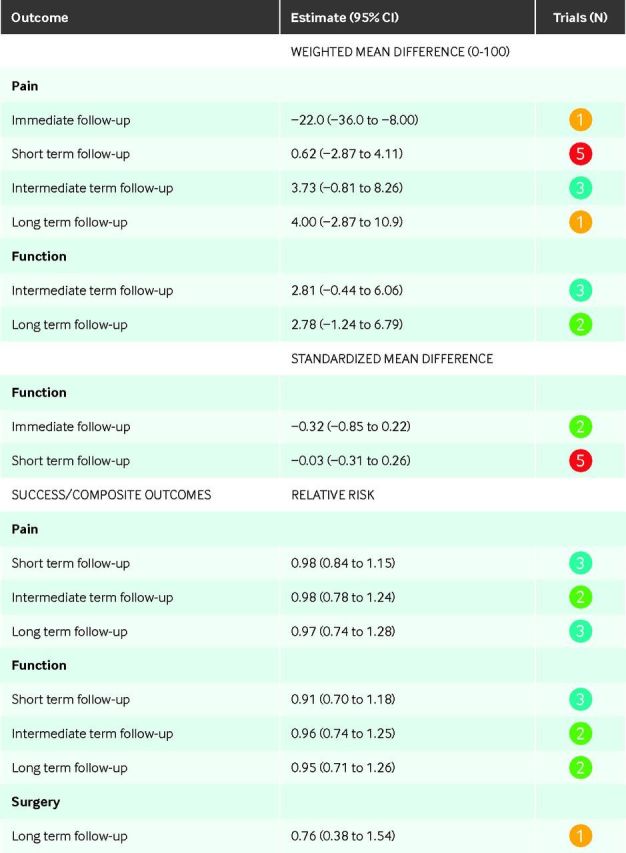
Pooled results of epidural steroid injections versus placebo interventions for spinal stenosis108
Other non-surgical options
Many older people with low back pain seek out complementary and alternative medicine, and although studies have not always clearly defined the diagnoses some of these people probably have spinal stenosis. However, little rigorous data are available on the efficacy of these alternative treatments in LSS. In the past, LSS with severe degenerative changes was considered to be a contraindication to spinal manipulation.15 However, several studies have recently looked at the effects of flexion distraction manipulation in LSS. A review of chiropractic treatment in LSS from 2009 found limited evidence of potential benefit but the evidence was of extremely low quality.109 More rigorous comparative studies are looking at this question,110 111 but currently there is no high quality evidence of the efficacy of spinal manipulation in LSS. Similarly, a systematic review published in 2013 of acupuncture in LSS found “that current evidence for the use of acupuncture in patients with LSS is limited, due to the scarcity of existing clinical trials and high risk of bias” and was therefore unable to draw any conclusions regarding its effectiveness.112
Surgical options
Several different surgical procedures are used to treat patients with LSS who do not improve with non-operative treatments. Given the rarity of rapid deterioration and that the disease often waxes and wanes then gradually improves, surgery is almost always an elective procedure that is considered only if sufficiently bothersome symptoms persist despite trials of less invasive interventions,113 and clinical practice varies widely.
Between 1979 and 1992, the rate of surgery for LSS increased almost eightfold and then plateaued.5 114 In recent years, although overall rates of surgery have been fairly stable, at one to two per 1000, the rates of operations that include lumbar fusion have increased dramatically.115 116 Rates vary widely across geographic regions—an eightfold variation in rates of decompression surgery and 14-20-fold variation in the use of fusion surgery.115 116 This variability occurs within the context of a lack of consensus among surgeons regarding indications for surgery and evidence that decision making in practice is often driven by surgeons’ preferences and enthusiasm rather than patient characteristics.8 In addition, there is no evidence of benefit for fusion in LSS without spondylolisthesis or scoliosis.117 118
Decompression
The primary goal of surgical intervention in LSS is to decompress the neural structures that are being encroached upon, theoretically relieving symptoms and improving function.
The specific details of the surgical approach vary according to the location of the stenosis, number of segments affected, associated deformity or spinal instability, history of previous surgery, and the surgeon’s preferences.113 The various approaches to achieving decompression include traditional laminectomy, bilateral laminotomies, bilateral decompression through unilateral laminotomy, and different forms of laminoplasty.113
Current evidence does not allow strong conclusions to be drawn about the comparative effectiveness of these approaches.119 A systematic review of three newer techniques for surgical decompression in LSS found no significant difference in self care abilities and leg pain compared with conventional laminectomy. However, the quality of evidence was low or very low because of the limited number of studies available for review and the poor study designs.120 The studies considered here typically involved different sites of stenosis; in addition, the exact method and extent of decompression was determined by the operating surgeon. This reflects the heterogeneity that complicates the interpretation of the literature in LSS.
Decompression of the neural structures generally focuses on relieving the leg symptoms (claudication or radiculopathy) associated with LSS and less on improving any accompanying back pain. Therefore, although back pain does improve, the improvement in leg pain is usually greater.121 Patients with LSS and predominant leg pain have better surgical outcomes and a greater relative improvement in surgical rather than non-operative outcomes than do patients with predominant back pain or equally bothersome pain in the legs and the back.122
Several randomized trials and systematic reviews have compared the efficacy of surgery versus non-operative treatment for LSS. A small RCT of patients with moderate sciatic symptoms and stenosis confirmed by imaging found a small persistent advantage for the surgery group at 10 years but provided no formal statistical analysis.18 The long term outcomes of a high quality RCT of moderate LSS found a significant early advantage for surgery; this advantage narrowed by six years but was still significant when viewed over the entire six years.123 SPORT was the largest study to compare surgery and non-operative treatment in LSS. It found no differences in the intent to treat analyses in the randomized component of the study, but high rates of treatment crossover greatly limited the conclusions that could be drawn.121 124 As-treated analyses of both the randomized and concurrent observational cohorts from SPORT showed a significant early benefit to surgery, although in the randomized cohort this advantage decreased over time and was no longer significant at six to eight years of follow-up.125
A recent review of reviews evaluating surgery compared with non-operative treatment for LSS concluded that “surgery appears to result in better outcomes (leg pain and disability) with regard to conservative interventions, but the evidence is heterogeneous and the underlying methodology is of low quality.”105 Similarly, an updated systematic review found very low quality evidence from a meta-analysis of two trials that compared direct decompression (with or without fusion) with multimodal non-operative care for the outcome of pain related disability, as measured by the Oswestry disability index.121 126 There was no significant difference at six months (mean difference −3.66, −10.12 to 2.80) or one year (−6.18, −15.03 to 2.66), but at 24 months a significant difference was found favoring decompression (−4.43, −7.91 to −0.96). Longer term follow-up data were available but a combined analysis could not be performed for those end points.127
A recent trial, published since these reviews, compared surgical decompression with a standardized physiotherapy regimen of lumbar flexion, conditioning exercises, and patient education.102 This trial reported no difference in results between the surgery and physiotherapy groups at one or two years; however, 57% of the patients assigned to physiotherapy crossed over to surgery, which is even higher than the 43% seen in SPORT.102 128 These crossover rates complicate the comparison of outcomes between the two treatment groups. However, all patients in both studies were considered candidates for surgery before randomization, which suggests that expert non-operative therapy in patients with LSS who are considered to be suitable for surgery could reduce the rate of surgery with good patient outcomes.
A systematic review of predictors of postoperative outcomes in LSS found that depression, cardiovascular comorbidity, disorders that affected walking ability, and scoliosis predicted poorer subjective outcomes. By contrast, better walking ability, better self rated health, higher income, less overall comorbidity, and pronounced central stenosis predicted better subjective outcomes.129 However, it is unclear whether these same factors would also predict non-operative outcomes. In a study of predictors of the treatment effect of surgery, smoking emerged as a major predictor of worse surgical outcomes and a smaller surgical treatment effect. Other predictors of a poor response included baseline disability, neuroforaminal stenosis, predominant leg pain, not lifting at work, and presence of a baseline neurological deficit.130
Role of postoperative rehabilitation
Although the general consensus is that surgery probably has better outcomes than non-operative treatment for LSS, only 60-70% of patients are satisfied with their symptoms after surgery.124 A systematic review of postoperative rehabilitation in LSS found moderate quality evidence that postoperative active rehabilitation after decompression surgery for lumbar spinal stenosis is more effective than usual care in improving both short term and long term (back related) functional status. Similar findings were noted for secondary outcomes, including short term improvement in low back pain and long term improvement in both low back pain and leg pain.131
Role of fusion
One of the major controversies about surgery for spinal stenosis is the role of spinal fusion. Spinal arthrodesis with the goal of achieving spinal fusion has generally been recommended for spinal stenosis associated with degenerative spondylolisthesis, recurrent stenosis after previous decompression, instability, or scoliosis.113 A recent clinical practice guideline recommended that “in the absence of deformity or instability, lumbar fusion has not been shown to improve outcomes in patients with isolated stenosis, and therefore it is not recommended (grade C recommendation).132 Similarly, guidelines from the North American Spine Society recommend that in the absence of associated scoliosis or spondylolisthesis, “decompression alone is suggested for patients with leg predominant symptoms without instability (grade B).”133
Despite this lack of evidence of an advantage for fusion in the absence of deformity or instability, and recommendations against it, epidemiological data suggest marked increases in the use of fusion in patients receiving surgery for isolated spinal stenosis, and a 14-fold variation in rates across the US.115 Increases and variability in rates are even more marked for complex fusions involving multiple levels or combinations of anterior and posterior fusion.5 Fusions, particularly complex fusions, however, are also independently associated with increased perioperative mortality, major complications, readmission to hospital, and cost.5 134
Interspinous spacers
Interspinous spacer devices are an alternative intervention in spinal stenosis designed to separate the spinous processes at the stenotic levels, thereby preventing the narrowing associated with loading and lumbar extension. They are inserted between the spinous processes using a minimally invasive technique and are designed to limit extension and decompress the nerves.
Biomechanical studies in cadaveric spines have shown a significant reduction in the motion from flexion into extension at levels implanted with a spacer with no significant effect on the kinematics of the adjacent levels.135 Additional studies in cadaveric spines showed that the device increased the spinal canal area during extension of the spine by 18%, the foraminal area by 25%, and the foraminal width by 41%.136 A neurophysiologic study showed similar improvement in transcranial motor evoked potential with interspinous distraction in severe single level spinal stenosis to that seen with decompressive laminectomy.137 A claims based analysis in the US showed that a spacer was inserted in about 6% of US Medicare beneficiaries receiving surgery for LSS.
One large randomized clinical trial compared an interspinous spacer device with continued non-operative therapy consisting of at least one epidural injection and drugs or physiotherapy (or both) in 191 patients.138 At two years, 48% of the spacer group and only 5% of the non-operative group met a composite success measure of improved symptom severity, improved physical function scores, and satisfaction with the treatment. Side effects were reported by 11% of those who underwent interspinous spacer implantation and 1.1% of the control group; these included spinous process fracture, coronary ischemia, respiratory distress, hematoma, and death from pulmonary edema.139
Recently, three RCTs from the Netherlands, Sweden, and Norway compared interspinous spacer implantation with decompressive surgery for LSS.140 141 142 They all found lower rates of complications but higher rates of re-operation in the spacer group (25-29% v 5-8% in the laminectomy group), although outcomes were similar between groups at two years. In the US claims analysis, patients receiving a spacer alone had fewer major medical complications than those undergoing decompression or fusion surgery (1.2% v 1.8% and 3.3%, respectively), but had significantly higher rates of further inpatient lumbar surgery (16.7% v 8.5% for decompression and 9.8% for fusion at two years).143 Two recent systematic reviews and meta-analyses both found that although interspinous spacers may provide some benefit, they are associated with a higher incidence of reoperation and higher cost compared with decompressive laminectomy, and that the indications, risks, and benefits of using these devices should be carefully considered before surgery.144 145
The MILD procedure
The minimally invasive lumbar decompression (MILD) procedure is an image guided minimally invasive procedure for treatment of degenerative central canal LSS with ligamentum flavum hypertrophy through percutaneous decompression of the hypertrophic ligamentum flavum.146 A randomized study of 38 patients showed no significant difference at six weeks in the Oswestry disability index for patients treated with MILD versus those treated with epidural steroid injections (mean difference 5.70, 0.57 to 10.83), although improvements in pain were greater in the MILD decompression group (2.40, 1.92 to 2.88). At 12 weeks there were many crossovers, which prevented further analysis, and no safety differences were observed.147 A systematic review found that current evidence on MILD is of low quality with risk of bias, although the procedure seems to be relatively safe in the treatment of symptomatic LSS.148 However, evidence for the relative safety and comparative effectiveness of MILD compared with standard decompression is lacking.
Associated conditions affecting treatment
Degenerative spondylolisthesis
Degenerative spondylolisthesis is a type of degenerative spinal deformity in which one vertebral body slips forward relative to the one below (fig 3) although the neural arch remains intact.149 This malalignment can cause narrowing of the central canal, lateral recesses, and neuroforamina, resulting in symptomatic spinal stenosis. Degenerative spondylolisthesis is more likely than LSS with normal vertebral alignment to occur in women and to present with stenosis at a single level.150 Evidence on the efficacy or comparative effectiveness of different non-operative treatments for this condition is limited and there are no rigorous guidelines. Generally recommended non-operative treatments for LSS with associated degenerative spondylolisthesis include patient education, analgesics, flexion strengthening and stabilizing exercises, and physical and cognitive treatments focused on function and activities of daily living.149
Fig 3 .

Degenerative spondylolisthesis: frontal (A) and sagittal (B) views. Forward slippage of one vertebra over the other may cause narrowing of the central canal, lateral recesses, and neuroforamina, thereby contributing to lumbar spinal stenosis. Reproduced with permission from the department of orthopedic surgery at Dartmouth-Hitchcock Medical Center
Many studies of LSS include patients with degenerative spondylolisthesis but only SPORT evaluated the outcomes of surgery versus non-operative treatment in patients with LSS and degenerative spondylolisthesis and those with normal alignment separately.121 151 As with LSS, the study found no difference in intention to treat analyses between randomized groups, but the high rates of crossover complicated the interpretation of the results. Observational analyses (as treated) in the randomized and observational cohorts showed a significant advantage for surgery at two and four years.151 152 A combined analysis directly comparing results between the degenerative spondylolisthesis and isolated LSS cohorts found similar baseline levels of symptom severity and disability between the groups, greater improvement with surgery in the degenerative spondylolisthesis cohort, and similar non-operative outcomes between the two cohorts. It concluded that surgical treatment had a greater effect in patients with degenerative spondylolisthesis.150
As mentioned above, in contrast to isolated LSS, current recommendations on the surgical treatment of degenerative spondylolisthesis include decompression and fusion.133 This recommendation is mainly based on a prospective study from 1991 that showed better outcomes in people treated with laminectomy and arthrodesis rather than laminectomy alone.153 However, with the development of less extensive decompression techniques, interest in the use of decompression alone has been renewed.154 In SPORT, 6% of patients with degenerative spondylolisthesis had decompression alone.155
Another controversy in the surgical treatment of degenerative spondylolisthesis is the appropriate role of instrumentation when an arthrodesis is performed. A randomized trial comparing instrumented and non-instrumented fusion in degenerative spondylolisthesis found a significant increase in fusion rate with instrumentation but no difference in clinical outcomes.156 Long term follow-up of patients having non-instrumented posterolateral fusion found that those with a pseudo-arthrosis had a worse outcome than those who achieved solid fusion. However, because this case series had no comparison group with instrumented fusion, it provides no direct evidence on the question of instrumentation.157 In SPORT, 21% of patients with degenerative spondylolisthesis had non-instrumented fusion, 56% had fusion with the use of posterior instrumentation, and 17% had a circumferential fusion; clinical outcomes were similar between the three groups.155 Current clinical practice guideline recommendations (grade B) on the use of instrumentation in the treatment of degenerative spondylolisthesis state that the addition of instrumentation is thought to improve fusion rates but not clinical outcomes in patients with symptomatic LSS and degenerative spondylolisthesis.133
In a study of predictors of surgical treatment effect in degenerative spondylolisthesis, age less than 67 years, female sex, absence of stomach problems, neurogenic claudication, baseline reflex deficit, opioid use, not taking antidepressants, dissatisfaction with symptoms, and patient anticipation of a high likelihood of being pain free after surgery predicted a greater relative benefit from surgery.158 These predictors, however, have not been replicated or validated in other studies. An international panel attempted to define criteria for surgery in degenerative spondylolisthesis using the Rand appropriateness criteria. The main criteria associated with a clinical scenario being rated as appropriate for surgery were the presence of severe disability, severe neurological abnormalities, and the absence of severe psychosocial comorbidities. Few scenarios with back pain only—that is, without accompanying neurogenic claudication or radiculopathy—were considered appropriate for surgery.159 However, these criteria need to be validated in clinical practice.
Degenerative scoliosis
Adult scoliosis, which includes patients with curvature of the spine of varying degrees that is caused or affected by degenerative disc and joint disease, is a common disorder in the aging population. It has an important effect on quality of life and may be contribute to symptomatic spinal stenosis in some cases. Both the prevalence and severity of lumbar scoliosis increase steadily with age. Evidence based guidelines for the treatment of adult degenerative scoliosis are lacking and treatment decisions largely depend on the healthcare provider’s clinical expertise and practice patterns as well as the patient’s preferences. An ongoing clinical trial sponsored by the National Institutes of Health comparing surgical and non-operative treatments for adult symptomatic lumbar scoliosis (Clinicaltrials.gov; NCT00854828) may help provide some insight into the management of this complex disorder in the future. Complication rates approaching 60% have been reported for long fusion procedures used to treat degenerative scoliosis.160 The pros and cons of extensive reconstructive surgery with high complication rates versus more limited intervention with the risk of progressive deformity and the need for further surgery are controversial. However, discussion of the management of LSS patients with severe concurrent scoliosis is beyond the scope of this review.
Conclusion
LSS is a common and often debilitating condition in older people. It is characterized by degenerative changes that cause encroachment of the soft tissues into spaces around the neural structures and lead to symptoms of neurogenic claudication or radiculopathy, or both. The high rate of anatomic spinal stenosis on imaging in asymptomatic older people, the often vague and variable symptoms of spinal stenosis, and the heterogeneity across the spectrum of LSS make this condition complex to diagnose and treat. Over-reliance on imaging findings probably results in overdiagnosis of LSS so should be avoided.
Many of the treatments lack a strong evidence base and even those with the strongest evidence base, such as decompressive surgery, may be only modestly successful and carry potential risks. Given the marked heterogeneity in LSS and the trade-offs involved in different treatment approaches, a shared decision making approach is needed. This should focus on providing patients with standardized information on the treatment options, eliciting and clarifying patients’ personal values and goals, and tailoring treatment to achieve patients’ symptomatic and functional goals. Key information for patients includes the typical waxing and waning but generally favorable natural course of the disease, in contrast to the rapid and progressive deterioration that many of them fear, along with the expected outcomes and risks of the various treatment options. Formal decision aids for spinal stenosis, both video161 and paper based,115 are available to help inform and engage patients in decision making. More evidence on well defined homogeneous phenotypes within the broad spectrum of LSS could provide more tailored evidence on the likely outcomes for individual patients.
Contributors: Both authors participated fully in the planning, conduct, and reporting of the work described in the article, and are responsible for the overall content as guarantors.
Competing interests: We have read and understood BMJ policy on declaration of interests and declare the following interests: CTL: none; JDL: consulting for FzioMed and the Informed Medical Decisions Foundation and stock options from NewVert; FzioMed and NewVert produce products related to surgery for intervertebral disc herniation but not for spinal stenosis. This work was supported in part by the Multidisciplinary Clinical Research Center in Musculoskeletal Diseases at Dartmouth, funded by NIAMS (P60-AR048094 and P60-AR062799).
Provenance and peer review: Commissioned; externally peer reviewed.
Cite this as: BMJ 2016;352:h6234
References
- 1.Katz JN, Harris MB. Clinical practice. Lumbar spinal stenosis. N Engl J Med 2008;358:818-25. [DOI] [PubMed] [Google Scholar]
- 2.Deyo RA. Treatment of lumbar spinal stenosis: a balancing act. Spine J 2010;10:625-7. [DOI] [PubMed] [Google Scholar]
- 3.Genevay S, Atlas SJ, Katz JN. Variation in eligibility criteria from studies of radiculopathy due to a herniated disc and of neurogenic claudication due to lumbar spinal stenosis: a structured literature review. Spine 2010;35:803-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Deyo RA, Gray DT, Kreuter W, et al. United States trends in lumbar fusion surgery for degenerative conditions. Spine 2005;30:1441-5; discussion 1446-7. [DOI] [PubMed] [Google Scholar]
- 5.Deyo RA, Mirza SK, Martin BI, et al. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 2010;303:1259-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.ECRI Health Technology Assessment Group. Treatment of degenerative lumbar spinal stenosis: summary. 2001. www.ncbi.nlm.nih.gov/books/NBK11855/. [PMC free article] [PubMed]
- 7.Kalichman L, Cole R, Kim DH, et al. Spinal stenosis prevalence and association with symptoms: the Framingham Study. Spine J 2009;9:545-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Deyo RA. Treatment of lumbar spinal stenosis: a balancing act. Spine J 2010;10:625-7. [DOI] [PubMed] [Google Scholar]
- 9.Szpalski M, Gunzburg R. Lumbar spinal stenosis in the elderly: an overview. Eur Spine J 2003;12:S170-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Verbiest H. A radicular syndrome from developmental narrowing of the lumbar vertebral canal. J Bone Joint Surg Br 1954;36-B:230-7. [DOI] [PubMed]
- 11.Watters WC, Baisden J, Gilbert TJ, et al. Degenerative lumbar spinal stenosis: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis. Spine J 2008;8:305-10. [DOI] [PubMed] [Google Scholar]
- 12.Ciricillo SF, Weinstein PR. Lumbar spinal stenosis. West J Med 1993;158:171-7. [PMC free article] [PubMed] [Google Scholar]
- 13.Chad DA. Lumbar spinal stenosis. Neurol Clin 2007;25:407-18. [DOI] [PubMed] [Google Scholar]
- 14.Arbit E, Pannullo S. Lumbar stenosis: a clinical review. Clin Orthop 2001;384:137-43. [PubMed] [Google Scholar]
- 15.Fritz JM, Delitto A, Welch WC, et al. Lumbar spinal stenosis: a review of current concepts in evaluation, management, and outcome measurements. Arch Phys Med Rehabil 1998;79:700-8. [DOI] [PubMed] [Google Scholar]
- 16.Schönström N, Lindahl S, Willén J, et al. Dynamic changes in the dimensions of the lumbar spinal canal: an experimental study in vitro. J Orthop Res 1989;7:115-21. [DOI] [PubMed] [Google Scholar]
- 17.Penning L. Functional pathology of lumbar spinal stenosis. Clin Biomech (Bristol Avon) 1992;7:3-17. [DOI] [PubMed] [Google Scholar]
- 18.Amundsen T, Weber H, Nordal HJ, et al. Lumbar spinal stenosis: conservative or surgical management?: a prospective 10-year study. Spine 2000;25:1424-35; discussion 1435-6. [DOI] [PubMed] [Google Scholar]
- 19.Iversen MD, Katz JN. Examination findings and self-reported walking capacity in patients with lumbar spinal stenosis. Phys Ther 2001;81:1296-306. [PubMed] [Google Scholar]
- 20.Lin S-I, Lin R-M. Disability and walking capacity in patients with lumbar spinal stenosis: association with sensorimotor function, balance, and functional performance. J Orthop Sports Phys Ther 2005;35:220-6. [DOI] [PubMed] [Google Scholar]
- 21.Binder DK, Schmidt MH, Weinstein PR. Lumbar spinal stenosis. Semin Neurol 2002;22:157-66. [DOI] [PubMed] [Google Scholar]
- 22.Lee CK, Rauschning W, Glenn W. Lateral lumbar spinal canal stenosis: classification, pathologic anatomy and surgical decompression. Spine 1988;13:313-20. [DOI] [PubMed] [Google Scholar]
- 23.Tomkins-Lane CC, Battié MC. Predictors of objectively measured walking capacity in people with degenerative lumbar spinal stenosis. J Back Musculoskelet Rehabil 2013;26:345-52. [DOI] [PubMed] [Google Scholar]
- 24.Johnsson KE, Rosén I, Udén A. Neurophysiologic investigation of patients with spinal stenosis. Spine 1987;12:483-7. [DOI] [PubMed] [Google Scholar]
- 25.Atlas SJ, Delitto A. Spinal stenosis: surgical versus nonsurgical treatment. Clin Orthop 2006;443:198-207. [DOI] [PubMed] [Google Scholar]
- 26.Porter RW. Spinal stenosis and neurogenic claudication. Spine 1996;21:2046-52. [DOI] [PubMed] [Google Scholar]
- 27.Nadeau M, Rosas-Arellano M, Gurr K, et al. The reliability of differentiating neurogenic claudication from vascular claudication based on symptomatic presentation. Can J Surg 2103;56:372-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Conway J, Tomkins CC, Haig AJ. Walking assessment in people with lumbar spinal stenosis: capacity, performance, and self-report measures. Spine J 2011;11:816-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Katz JN, Dalgas M, Stucki G, et al. Degenerative lumbar spinal stenosis. Diagnostic value of the history and physical examination. Arthritis Rheum 1995;38:1236-41. [DOI] [PubMed] [Google Scholar]
- 30.Tomkins-Lane CC, Conway J, Hepler C, et al. Changes in objectively measured physical activity (performance) after epidural steroid injection for lumbar spinal stenosis. Arch Phys Med Rehabil 2012;93:2008-14. [DOI] [PubMed] [Google Scholar]
- 31.Whitehurst M, Brown LE, Eidelson SG, et al. Functional mobility performance in an elderly population with lumbar spinal stenosis. Arch Phys Med Rehabil 2001;82:464-7. [DOI] [PubMed] [Google Scholar]
- 32.Tomkins-Lane CC, Holz SC, Yamakawa KS, et al. Predictors of walking performance and walking capacity in people with lumbar spinal stenosis, low back pain, and asymptomatic controls. Arch Phys Med Rehabil 2012;93:647-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Benoist M. The natural history of lumbar degenerative spinal stenosis. J Bone Spine Rev Rhum 2002;69:450-7. [DOI] [PubMed] [Google Scholar]
- 34.Hurri H, Slätis P, Soini J, et al. Lumbar spinal stenosis: assessment of long-term outcome 12 years after operative and conservative treatment. J Spinal Disord 1998;11:110-5. [PubMed] [Google Scholar]
- 35.Johnsson KE, Rosén I, Udén A. The natural course of lumbar spinal stenosis. Clin Orthop 1992;279:82-6. [PubMed] [Google Scholar]
- 36.Minamide A, Yoshida M, Maio K. The natural clinical course of lumbar spinal stenosis: a longitudinal cohort study over a minimum of 10 years. J Orthop Sci 2013;18:693-8. [DOI] [PubMed] [Google Scholar]
- 37.Haig AJ, Tong HC, Yamakawa KSJ, et al. Predictors of pain and function in persons with spinal stenosis, low back pain, and no back pain. Spine 2006;31:2950-7. [DOI] [PubMed] [Google Scholar]
- 38.Evans JG. Neurogenic intermittent claudication. BMJ 1964;2:985-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Watanabe R, Parke WW. Vascular and neural pathology of lumbosacral spinal stenosis. J Neurosurg 1986;64:64-70. [DOI] [PubMed] [Google Scholar]
- 40.Ooi Y, Mita F, Satoh Y. Myeloscopic study on lumbar spinal canal stenosis with special reference to intermittent claudication. Spine 1990;15:544-9. [DOI] [PubMed] [Google Scholar]
- 41.Porter RW, Ward D. Cauda equina dysfunction. The significance of two-level pathology. Spine 1992;17:9-15. [PubMed] [Google Scholar]
- 42.Binder DK, Schmidt MH, Weinstein PR. Lumbar spinal stenosis. Semin Neurol 2002;22:157-66. [DOI] [PubMed] [Google Scholar]
- 43.Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol 2010;24:253-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Andreisek G, Hodler J, Steurer J. Uncertainties in the diagnosis of lumbar spinal stenosis. Radiology 2011;261:681-4. [DOI] [PubMed] [Google Scholar]
- 45.Frymoyer JW. Degenerative spondylolisthesis: diagnosis and treatment. J Am Acad Orthop Surg 1994;2:9-15. [DOI] [PubMed] [Google Scholar]
- 46.Haig AJ, Tomkins CC. Diagnosis and management of lumbar spinal stenosis. JAMA 2010;303:71-2. [DOI] [PubMed] [Google Scholar]
- 47.Suri P, Rainville J, Kalichman L, et al. Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis? JAMA 2010;304:2628-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.De Schepper EIT, Overdevest GM, Suri P, et al. Diagnosis of lumbar spinal stenosis: an updated systematic review of the accuracy of diagnostic tests. Spine 2013;38:E469-81. [DOI] [PubMed] [Google Scholar]
- 49.Barz T, Melloh M, Staub L, et al. The diagnostic value of a treadmill test in predicting lumbar spinal stenosis. Eur Spine J 2008;17:686-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Deen HG, Zimmerman RS, Lyons MK, et al. Measurement of exercise tolerance on the treadmill in patients with symptomatic lumbar spinal stenosis: a useful indicator of functional status and surgical outcome. J Neurosurg 1995;83:27-30. [DOI] [PubMed] [Google Scholar]
- 51.Deen HG, Zimmerman RS, Lyons MK, et al. Use of the exercise treadmill to measure baseline functional status and surgical outcome in patients with severe lumbar spinal stenosis. Spine 1998;23:244-8. [DOI] [PubMed] [Google Scholar]
- 52.Herno A, Saari T, Suomalainen O, et al. The degree of decompressive relief and its relation to clinical outcome in patients undergoing surgery for lumbar spinal stenosis. Spine 1999;24:1010-4. [DOI] [PubMed] [Google Scholar]
- 53.Jensen OH, Schmidt-Olsen S. A new functional test in the diagnostic evaluation of neurogenic intermittent claudication. Clin Rheumatol 1989;8:363-7. [DOI] [PubMed] [Google Scholar]
- 54.Tenhula J, Lenke LG, Bridwell KH, et al. Prospective functional evaluation of the surgical treatment of neurogenic claudication in patients with lumbar spinal stenosis. J Spinal Disord 2000;13:276-82. [DOI] [PubMed] [Google Scholar]
- 55.Tomkins CC, Battié MC, Rogers T, et al. A criterion measure of walking capacity in lumbar spinal stenosis and its comparison with a treadmill protocol. Spine 2009;34:2444-9. [DOI] [PubMed] [Google Scholar]
- 56.Kim Y-S, Park S-J, Oh I-S, et al. The clinical effect of gait load test in two level lumbar spinal stenosis. Asian Spine J 2009;3:96-100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Takahashi N, Kikuchi S, Yabuki S, et al. Diagnostic value of the lumbar extension-loading test in patients with lumbar spinal stenosis: a cross-sectional study. BMC Musculoskelet Disord 2014;15:259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Nagai K, Aoyama T, Yamada M, et al. Quantification of changes in gait characteristics associated with intermittent claudication in patients with lumbar spinal stenosis. J Spinal Disord Tech 2014;27:E136-42. [DOI] [PubMed] [Google Scholar]
- 59.Tomkins-Lane CC, Haig AJ. A review of activity monitors as a new technology for objectifying function in lumbar spinal stenosis. J Back Musculoskelet Rehabil 2012;25:177-85. [DOI] [PubMed] [Google Scholar]
- 60.Kalff R, Ewald C, Waschke A, et al. Degenerative lumbar spinal stenosis in older people. Dtsch Ärztebl Int 2013;110:613-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Haig AJ, Tong HC, Yamakawa KSJ, et al. The sensitivity and specificity of electrodiagnostic testing for the clinical syndrome of lumbar spinal stenosis. Spine 2005;30:2667-76. [DOI] [PubMed] [Google Scholar]
- 62.Haig AJ, Tong HC, Yamakawa KS, et al. Spinal stenosis, back pain, or no symptoms at all? A masked study comparing radiologic and electrodiagnostic diagnoses to the clinical impression. Arch Phys Med Rehabil 2006;87:897-903. [DOI] [PubMed] [Google Scholar]
- 63.Yagci I, Gunduz OH, Ekinci G, et al. The utility of lumbar paraspinal mapping in the diagnosis of lumbar spinal stenosis. Am J Phys Med Rehabil 2009;88:843-51. [DOI] [PubMed] [Google Scholar]
- 64.Kuittinen P, Sipola P, Aalto TJ, et al. Correlation of lateral stenosis in MRI with symptoms, walking capacity and EMG findings in patients with surgically confirmed lateral lumbar spinal canal stenosis. BMC Musculoskelet Disord 2014;15:247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.De Graaf I, Prak A, Bierma-Zeinstra S, et al. Diagnosis of lumbar spinal stenosis: a systematic review of the accuracy of diagnostic tests. Spine 2006;31:1168-76. [DOI] [PubMed] [Google Scholar]
- 66.Mamisch N, Brumann M, Hodler J, et al. Radiologic criteria for the diagnosis of spinal stenosis: results of a Delphi survey. Radiology 2012;264:174-9. [DOI] [PubMed] [Google Scholar]
- 67.Steurer J, Roner S, Gnannt R, et al. Quantitative radiologic criteria for the diagnosis of lumbar spinal stenosis: a systematic literature review. BMC Musculoskelet Disord 2011;12:175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Cheung JP-Y, Samartzis D, Shigematsu H, et al. Defining clinically relevant values for developmental spinal stenosis: a large-scale magnetic resonance imaging study. Spine 2014;39:1067-76. [DOI] [PubMed] [Google Scholar]
- 69.Wassenaar M, van Rijn RM, van Tulder MW, et al. Magnetic resonance imaging for diagnosing lumbar spinal pathology in adult patients with low back pain or sciatica: a diagnostic systematic review. Eur Spine J 2012;21:220-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Lurie JD, Tosteson AN, Tosteson TD, et al. Reliability of readings of magnetic resonance imaging features of lumbar spinal stenosis. Spine 2008;33:1605-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Lee S, Lee JW, Yeom JS, et al. A practical MRI grading system for lumbar foraminal stenosis. AJR Am J Roentgenol 2010;194:1095-8. [DOI] [PubMed] [Google Scholar]
- 72.Schizas C, Theumann N, Burn A, et al. Qualitative grading of severity of lumbar spinal stenosis based on the morphology of the dural sac on magnetic resonance images. Spine 2010;35:1919-24. [DOI] [PubMed] [Google Scholar]
- 73.Barz T, Melloh M, Staub LP, et al. Nerve root sedimentation sign: evaluation of a new radiological sign in lumbar spinal stenosis. Spine 2010;35:892-7. [DOI] [PubMed] [Google Scholar]
- 74.Moses RA, Zhao W, Staub LP, et al. Is the sedimentation sign associated with spinal stenosis surgical treatment effect in SPORT? Spine 2015;40:129-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Tomkins-Lane CC, Quint DJ, Gabriel S, et al. Nerve root sedimentation sign for the diagnosis of lumbar spinal stenosis: reliability, sensitivity, and specificity. Spine 2013;38:E1554-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Andreisek G, Imhof M, Wertli M, et al. A systematic review of semiquantitative and qualitative radiologic criteria for the diagnosis of lumbar spinal stenosis. Am J Roentgenol 2013;201:W735-46. [DOI] [PubMed] [Google Scholar]
- 77.Andreisek G, Deyo RA, Jarvik JG, et al. Consensus conference on core radiological parameters to describe lumbar stenosis—an initiative for structured reporting. Eur Radiol 2014;24:3224-32. [DOI] [PubMed] [Google Scholar]
- 78.Boden SD, Davis DO, Dina TS, et al. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 1990;72:403-8. [PubMed] [Google Scholar]
- 79.Amundsen T, Weber H, Lilleås F, et al. Lumbar spinal stenosis. Clinical and radiologic features. Spine 1995;20:1178-86. [DOI] [PubMed] [Google Scholar]
- 80.Geisser ME, Haig AJ, Tong HC, et al. Spinal canal size and clinical symptoms among persons diagnosed with lumbar spinal stenosis. Clin J Pain 2007;23:780-5. [DOI] [PubMed] [Google Scholar]
- 81.Herno A, Airaksinen O, Saari T. Computed tomography after laminectomy for lumbar spinal stenosis. Patients’ pain patterns, walking capacity, and subjective disability had no correlation with computed tomography findings. Spine 1994;19:1975-8. [PubMed] [Google Scholar]
- 82.Lohman CM, Tallroth K, Kettunen JA, et al. Comparison of radiologic signs and clinical symptoms of spinal stenosis. Spine 2006;31:1834-40. [DOI] [PubMed] [Google Scholar]
- 83.Cook C, Brown C, Michael K, et al. The clinical value of a cluster of patient history and observational findings as a diagnostic support tool for lumbar spine stenosis. Physiother Res Int J Res Clin Phys Ther 2011;16:170-8. [DOI] [PubMed] [Google Scholar]
- 84.Kato Y, Kawakami T, Kifune M, et al. Validation study of a clinical diagnosis support tool for lumbar spinal stenosis. J Orthop Sci 2009;14:7118. [DOI] [PubMed] [Google Scholar]
- 85.Konno S, Hayashino Y, Fukuhara S, et al. Development of a clinical diagnosis support tool to identify patients with lumbar spinal stenosis. Eur Spine J 2007;16:1951-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Sugioka T, Hayashino Y, Konno S, et al. Predictive value of self-reported patient information for the identification of lumbar spinal stenosis. Fam Pract 2008;25:237-44. [DOI] [PubMed] [Google Scholar]
- 87.Haskins R, Osmotherly PG, Rivett DA. Diagnostic clinical prediction rules for specific subtypes of low back pain: a systematic review. J Orthop Sports Phys Ther 2015;45:61-76. [DOI] [PubMed] [Google Scholar]
- 88.Sandella DE, Haig AJ, Tomkins-Lane C, et al. Defining the clinical syndrome of lumbar spinal stenosis: a recursive specialist survey process. PM R 2013;5:491-5; quiz 495. [DOI] [PubMed] [Google Scholar]
- 89.Ammendolia C, Stuber KJ, Rok E, et al. Nonoperative treatment for lumbar spinal stenosis with neurogenic claudication. Cochrane Database Syst Rev 2013;8;CD010712. [DOI] [PMC free article] [PubMed]
- 90.Schneider M, Ammendolia C, Murphy D, et al. Comparison of non-surgical treatment methods for patients with lumbar spinal stenosis: protocol for a randomized controlled trial. Chiropr Man Ther 2014;22:19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Tomkins-Lane CC, Lafave LMZ, Parnell JA, et al. The spinal stenosis pedometer and nutrition lifestyle intervention (SSPANLI) randomized controlled trial protocol. BMC Musculoskelet Disord 2013;14:322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Tomkins-Lane CC, Lafave LMZ, Parnell JA, et al. The spinal stenosis pedometer and nutrition lifestyle intervention (SSPANLI): development and pilot. Spine J 2014; published online 22 Oct. [DOI] [PubMed]
- 93.Ammendolia C, Stuber K, de Bruin LK, et al. Nonoperative treatment of lumbar spinal stenosis with neurogenic claudication: a systematic review. Spine 2012;37:E609-16. [DOI] [PubMed] [Google Scholar]
- 94.Coronado-Zarco R, Cruz-Medina E, Arellano-Hernández A, et al. Effectiveness of calcitonin in intermittent claudication treatment of patients with lumbar spinal stenosis: a systematic review. Spine 2009;34:E818-22. [DOI] [PubMed] [Google Scholar]
- 95.Podichetty VK, Segal AM, Lieber M, et al. Effectiveness of salmon calcitonin nasal spray in the treatment of lumbar canal stenosis: a double-blind, randomized, placebo-controlled, parallel group trial. Spine 2004;29:2343-9. [DOI] [PubMed] [Google Scholar]
- 96.Peng K, Chen L, Peng J, et al. Effects of calcitonin on lumbar spinal stenosis: a systematic review and meta-analysis. Int J Clin Exp Med 2015;8:2536-44. [PMC free article] [PubMed] [Google Scholar]
- 97.Van Tulder MW, Scholten RJ, Koes BW, et al. Non-steroidal anti-inflammatory drugs for low back pain. Cochrane Database Syst Rev 2000;2:CD000396. [DOI] [PubMed] [Google Scholar]
- 98.Yoshihara H. Prostaglandin E1 treatment for lumbar spinal canal stenosis: review of the literature. Pain Pract 2015; published online 7 Jan. [DOI] [PubMed]
- 99.Tomkins CC, Dimoff KH, Forman HS, et al. Physical therapy treatment options for lumbar spinal stenosis. J Back Musculoskelet Rehabil 2010;23:31-7. [DOI] [PubMed] [Google Scholar]
- 100.Macedo LG, Hum A, Kuleba L, et al. Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review. Phys Ther 2013;93:1646-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Fritz JM, Lurie JD, Zhao W, et al. Associations between physical therapy and long-term outcomes for individuals with lumbar spinal stenosis in the SPORT study. Spine J 2014;14:1611-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Delitto A, Piva SR, Moore CG, et al. Surgery versus nonsurgical treatment of lumbar spinal stenosis: a randomized trial. Ann Intern Med 2015;162:465-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Ammendolia C, Stuber KJ, Rok E, et al. Nonoperative treatment for lumbar spinal stenosis with neurogenic claudication. Cochrane Database Syst Rev 2013;8:CD010712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Liu K, Liu P, Liu R, et al. Steroid for epidural injection in spinal stenosis: a systematic review and meta-analysis. Drug Des Dev Ther 2015;9:707-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Manchikanti L, Singh V, Pampati V, et al. Comparison of the efficacy of caudal, interlaminar, and transforaminal epidural injections in managing lumbar disc herniation: is one method superior to the other? Korean J Pain 2015;28:11-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Friedly JL, Comstock BA, Turner JA, et al. A randomized trial of epidural glucocorticoid injections for spinal stenosis. N Engl J Med 2014;371:11-21. [DOI] [PubMed] [Google Scholar]
- 107.Centers for Disease Control and Prevention (CDC). Multistate outbreak of fungal infection associated with injection of methylprednisolone acetate solution from a single compounding pharmacy—United States, 2012. MMWR Morb Mortal Wkly Rep 2012;61:839-42. [PubMed] [Google Scholar]
- 108.Chou R, Hashimoto R, Friedly J, et al. Epidural corticosteroid injections for radiculopathy and spinal stenosis: a systematic review and meta-analysis. Ann Intern Med 2015;163:373-81. [DOI] [PubMed] [Google Scholar]
- 109.Stuber K, Sajko S, Kristmanson K. Chiropractic treatment of lumbar spinal stenosis: a review of the literature. J Chiropr Med 2009;8:77-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Cambron JA, Schneider M, Dexheimer JM, et al. A pilot randomized controlled trial of flexion-distraction dosage for chiropractic treatment of lumbar spinal stenosis. J Manipulative Physiol Ther 2014;37:396-406. [DOI] [PubMed] [Google Scholar]
- 111.Schneider M, Ammendolia C, Murphy D, et al. Comparison of non-surgical treatment methods for patients with lumbar spinal stenosis: protocol for a randomized controlled trial. Chiropr Man Ther 2014;22:19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Kim KH, Kim T-H, Lee BR, et al. Acupuncture for lumbar spinal stenosis: A systematic review and meta-analysis. Complement Ther Med 2013;21:535-56. [DOI] [PubMed] [Google Scholar]
- 113.Sengupta DK, Herkowitz HN. Lumbar spinal stenosis. Treatment strategies and indications for surgery. Orthop Clin North Am 2003;34:281-95. [DOI] [PubMed] [Google Scholar]
- 114.Ciol MA, Deyo RA, Howell E, et al. An assessment of surgery for spinal stenosis: time trends, geographic variations, complications, and reoperations. J Am Geriatr Soc 1996;44:285-90. [DOI] [PubMed] [Google Scholar]
- 115.Dartmouth Institute. Variation in the care of surgical conditions: spinal stenosis. 2014. www.dartmouthatlas.org/downloads/reports/Spinal_stenosis_report_10_29_14.pdf. [PubMed]
- 116.Weinstein JN, Lurie JD, Olson PR, et al. United States’ trends and regional variations in lumbar spine surgery: 1992-2003. Spine 2006;31:2707-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Kreiner DS, Shaffer WO, Baisden JL, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J 2013;13:734-43. [DOI] [PubMed] [Google Scholar]
- 118.Resnick DK, Watters WC III, Mummaneni PV, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 10: Lumbar fusion for stenosis without spondylolisthesis. J Neurosurg Spine 2014;21:62-6. [DOI] [PubMed] [Google Scholar]
- 119.Jacobs WCH, Rubinstein SM, Koes B, et al. Evidence for surgery in degenerative lumbar spine disorders. Best Pract Res Clin Rheumatol 2013;27:673-84. [DOI] [PubMed] [Google Scholar]
- 120.Overdevest GM, Jacobs W, Vleggeert-Lankamp C, et al. Effectiveness of posterior decompression techniques compared with conventional laminectomy for lumbar stenosis. Cochrane Database Syst Rev 2015;3:CD010036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 2008;358:794-810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Pearson A, Blood E, Lurie J, et al. predominant leg pain is associated with better surgical outcomes in degenerative spondylolisthesis and spinal stenosis: results from the Spine Patient Outcomes Research Trial (SPORT). Spine 2011;36:219-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Slätis P, Malmivaara A, Heliövaara M, et al. Long-term results of surgery for lumbar spinal stenosis: a randomised controlled trial. Eur Spine J 2011;20:1174-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the Spine Patient Outcomes Research Trial. Spine 2010;35:1329-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Lurie JD, Tosteson TD, Tosteson A, et al. Long-term outcomes of lumbar spinal stenosis: eight-year results of the Spine Patient Outcomes Research Trial (SPORT). Spine 2015;40:63-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Malmivaara A, Slätis P, Heliövaara M, et al. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine 2007;32:1-8. [DOI] [PubMed] [Google Scholar]
- 127.Zaina F, Tomkins-Lane C, Carragee E, et al. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev [forthcoming]. [DOI] [PMC free article] [PubMed]
- 128.Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 2008;358:794-810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Aalto TJ, Malmivaara A, Kovacs F, et al. Preoperative predictors for postoperative clinical outcome in lumbar spinal stenosis: systematic review. Spine 2006;31:E648-63. [DOI] [PubMed] [Google Scholar]
- 130.Pearson A, Lurie J, Tosteson T, et al. Who should have surgery for spinal stenosis? Treatment effect predictors in SPORT. Spine 2012;37:1791-802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.McGregor AH, Probyn K, Cro S, et al. Rehabilitation following surgery for lumbar spinal stenosis. A Cochrane review. Spine 2014;39:1044-54. [DOI] [PubMed] [Google Scholar]
- 132.Resnick DK, Watters WC III, Mummaneni PV, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 10: lumbar fusion for stenosis without spondylolisthesis. J Neurosurg Spine 2014;21:62-6. [DOI] [PubMed] [Google Scholar]
- 133.Kreiner DS, Shaffer WO, Baisden JL, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J 2013;13:734-43. [DOI] [PubMed] [Google Scholar]
- 134.Carragee EJ. The increasing morbidity of elective spinal stenosis surgery: is it necessary? JAMA 2010;303:1309. [DOI] [PubMed] [Google Scholar]
- 135.Lindsey DP, Swanson KE, Fuchs P, et al. The effects of an interspinous implant on the kinematics of the instrumented and adjacent levels in the lumbar spine. Spine 2003;28:2192-7. [DOI] [PubMed] [Google Scholar]
- 136.Richards JC, Majumdar S, Lindsey DP, et al. The treatment mechanism of an interspinous process implant for lumbar neurogenic intermittent claudication. Spine 2005;30:744-9. [DOI] [PubMed] [Google Scholar]
- 137.Schizas C, Pralong E, Tzioupis C, et al. Interspinous distraction in lumbar spinal stenosis: a neurophysiological perspective. Spine 2013;38:2113-7. [DOI] [PubMed] [Google Scholar]
- 138.Zucherman JF, Hsu KY, Hartjen CA, et al. A prospective randomized multi-center study for the treatment of lumbar spinal stenosis with the X STOP interspinous implant: 1-year results. Eur Spine J 2004;13:22-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Zucherman JF, Hsu KY, Hartjen CA, et al. A multicenter, prospective, randomized trial evaluating the X STOP interspinous process decompression system for the treatment of neurogenic intermittent claudication: two-year follow-up results. Spine 2005;30:1351-8. [DOI] [PubMed] [Google Scholar]
- 140.Lønne G, Johnsen LG, Aas E, et al. Comparing cost-effectiveness of X-stop to minimally invasive decompression in lumbar spinal stenosis: a randomized controlled trial. Spine 2015; published online 20 Jan. [DOI] [PubMed]
- 141.Strömqvist BH, Berg S, Gerdhem P, et al. X-stop versus decompressive surgery for lumbar neurogenic intermittent claudication: randomized controlled trial with 2-year follow-up. Spine 2013;38:1436-42. [DOI] [PubMed] [Google Scholar]
- 142.Moojen WA, Arts MP, Jacobs WCH, et al. Interspinous process device versus standard conventional surgical decompression for lumbar spinal stenosis: randomized controlled trial. BMJ 2013;347:f6415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Deyo RA, Martin BI, Ching A, et al. Interspinous spacers compared with decompression or fusion for lumbar stenosis: complications and repeat operations in the Medicare population. Spine 2013;38:865-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Hong P, Liu Y, Li H. Comparison of the efficacy and safety between interspinous process distraction device and open decompression surgery in treating lumbar spinal stenosis: a meta analysis. J Investig Surg 2015;28:40-9. [DOI] [PubMed] [Google Scholar]
- 145.Wu A-M, Zhou Y, Li Q-L, et al. Interspinous spacer versus traditional decompressive surgery for lumbar spinal stenosis: a systematic review and meta-analysis. PloS One 2014;9:e97142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Deer TR, Kapural L. New image-guided ultra-minimally invasive lumbar decompression method: the mild procedure. Pain Physician 2010;13:35-41. [PubMed] [Google Scholar]
- 147.Brown LL. A double-blind, randomized, prospective study of epidural steroid injection vs the mild procedure in patients with symptomatic lumbar spinal stenosis. Pain Pract 2012;12:333-41. [DOI] [PubMed] [Google Scholar]
- 148.Kreiner DS, MacVicar J, Duszynski B, et al. The mild procedure: a systematic review of the current literature. Pain Med Malden Mass 2014;15:196-205. [DOI] [PubMed] [Google Scholar]
- 149.Kalichman L, Hunter DJ. Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J 2008;17:327-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Pearson A, Blood E, Lurie J, et al. Degenerative spondylolisthesis versus spinal stenosis: does a slip matter? Comparison of baseline characteristics and outcomes (SPORT). Spine 2010;35:298-305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonsurgical treatment for lumbar degenerative spondylolisthesis. N Engl J Med 2007;356:2257-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am 2009;91:1295-304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-8. [PubMed] [Google Scholar]
- 154.Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg 2014;22:203-13. [DOI] [PubMed] [Google Scholar]
- 155.Abdu WA, Lurie JD, Spratt KF, et al. Degenerative spondylolisthesis: does fusion method influence outcome? Four-year results of the spine patient outcomes research trial. Spine 2009;34:2351-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Fischgrund JS, Mackay M, Herkowitz HN, et al. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-12. [DOI] [PubMed] [Google Scholar]
- 157.Kornblum MB, Fischgrund JS, Herkowitz HN, et al. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective long-term study comparing fusion and pseudarthrosis. Spine 2004;29:726-33; discussion 733-4. [DOI] [PubMed] [Google Scholar]
- 158.Pearson AM, Lurie JD, Tosteson TD, et al. Who should undergo surgery for degenerative spondylolisthesis? Treatment effect predictors in SPORT. Spine 2013;38:1799-811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Mannion AF, Pittet V, Steiger F, et al. Development of appropriateness criteria for the surgical treatment of symptomatic lumbar degenerative spondylolisthesis (LDS). Eur Spine J 2014;23:1903-17. [DOI] [PubMed] [Google Scholar]
- 160.Wang G, Hu J, Liu X, et al. Surgical treatments for degenerative lumbar scoliosis: a meta analysis. Eur Spine J 2015;24:1792-9. [DOI] [PubMed] [Google Scholar]
- 161.Phelan EA, Deyo RA, Cherkin DC, et al. Helping patients decide about back surgery: a randomized trial of an interactive video program. Spine 2001;26:206-11; discussion 212. [DOI] [PubMed] [Google Scholar]