

Abstract
Background:
Scapula fractures are uncommon in sports and are poorly understood in this patient group.
Purpose:
To report on scapula fractures in contact and collision athletes and assess the injury patterns of different mechanisms of injury.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective case series was performed of all sports-related scapula fractures treated at a single institution between 2007 and 2015. The mechanisms of injury were divided into direct lateral impact, fall onto an outstretched arm, or abduction/external rotation.
Results:
A total of 11 patients were identified: 9 professional rugby players, 1 professional soccer player, and 1 amateur soccer player. The mean age was 28 years (range, 18-35 years). The mean return to play was 127 days in those treated nonoperatively and 163 days in those treated operatively. A direct impact mechanism occurred in 7 patients, all of whom sustained glenoid neck and body fractures and were treated nonoperatively. Two rugby players had a concomitant suprascapular nerve injury. An outstretched arm mechanism occurred in 2 cases, leading to posterior and inferior glenoid fractures. Both patients were treated operatively. An abduction/external rotation mechanism occurred in 2 cases, resulting in an anteroinferior and an anterior glenoid rim fracture. One case was treated operatively and the other was treated nonoperatively. Of those with glenoid fractures, 75% were not visible on plain radiographs and required further imaging.
Conclusion:
Scapula fractures acquired in sports are a serious injury with a prolonged recovery period. The mechanism of injury can help predict the injury pattern and highlight the need for further imaging. There is a high association with suprascapular nerve injuries.
Keywords: contact athletes, scapula fracture, rugby, football, soccer, diagnosis
Scapula fractures are infrequent, representing 1% of all fractures.9,14,15 They are often secondary to high-energy trauma and have significant associated injuries.14 Over 50% of scapula fractures occur as a result of road traffic collisions, with almost 20% involving a pedestrian being struck by a car. A simple fall accounts for only 12% of scapula fractures in the population.14 While the majority of these fractures can be successfully managed nonoperatively,1,4 intra-articular glenoid fractures11 and a superior shoulder suspensory mechanism injury7,11 may require surgical intervention.
Almost 90% of scapula fractures are attributed to high-energy mechanisms. These are well reported in the literature, with associated injuries.1,7,11,16 Anterior glenoid rim fractures associated with dislocation have also been reported.14 However, scapula fractures attributed to sports injuries are not well reported in the literature. Approximately 0.5% of all sports-related fractures are scapula fractures.5 Case reports on scapula fractures in professional American football players have previously been published2,3,13; the largest of these is a report of 5 cases.3 No studies were identified that focused on scapula fractures in rugby or European football (soccer).
Elite rugby players are a unique population in that they are often subjected to high-energy collisions.6 Each player can expect to routinely receive 1.95 to 2.13 times their bodyweight during tackles and collisions.15 With the mean weight of a front row player approaching 220 lb,15 the forces involved become substantial. Predictably, these common events during any match lead to a high rate of injury and time off play.3 Specifically, shoulder injuries are thought to occur every 17,000 player-hours of a match, although only 1% of those result in a fracture.8 Scapula fractures in elite rugby players are rarer, representing only 8% of significant shoulder injuries requiring specialist orthopaedic management.8 Given its significance, there is little in the literature specifically addressing this injury.
In the current study, we report our experience of the largest series of field sports–associated scapula fractures to date. In addition to describing the management of these cases, we aimed to identify the patterns of scapula fracture related to specific injury mechanisms and to report any associated injuries that require attention.
Methods
A retrospective cohort study was performed examining patients treated at The Wilmslow Hospital, HCA UK (Hospital Corporations of America United Kingdom), between 2007 and 2015. From our practice clinical database, which was set up in 2007, the total number of scapula fractures was identified by filtering all “athletes” with shoulder injuries and then “scapula fractures” from the diagnosis field. All patients in the database had signed consent forms for their anonymized data to be utilized for scientific and research purposes. Data were analyzed retrospectively, and there was no change in the patients’ standard of care or decision-making.
Only national amateur or professional contact athletes sustaining a scapula fracture while participating in a match or training were included. These were all cases referred to the senior author (L.F.), and they were identified from an electronic database. The rational was to look at players who were either professional or semiprofessional rather than people who sporadically played for recreation, without regular training and matches. Consequently, our results could be compared with the published case series examining American football players.2,3,13
The case notes and radiographs of all identified patients were examined for age, occupation, mechanism of injury, type of scapula fracture sustained, associated injuries, treatment provided, and time away from profession. The mechanism of injury was divided into 3 categories: direct impact, outstretched arm, and abduction/external rotation (ABER). A direct impact was defined as a direct lateral or posterior blow to the shoulder, either from a collision or by landing directly onto a shoulder during a fall/tackle. An outstretched arm mechanism was described as falling onto an outstretched arm in an attempt to prevent injury such that the load is transferred up the arm to the scapula. Finally, an ABER mechanism was defined as forced hyperexternal rotation and abduction of the arm during a fall, tackle, or collapsing scrum. The different patterns of scapula fractures were compared with the responsible mechanism. Isolated glenoid rim fractures associated with dislocations (bony Bankart lesions) were excluded, as we believe that these are shoulder dislocation injuries and not true glenoid fractures.
Results
During the 8-year study review period, the senior author saw 829 shoulder injuries in competitive rugby players and 103 shoulder injuries in competitive soccer players. Eleven patients with scapula fractures were identified (Table 1). Of these, 9 patients were professional rugby players (4 rugby league and 5 rugby union); 1 patient was a professional soccer player; and 1 patient was an amateur soccer player. The proportion of scapula fractures presenting in collision athletes with shoulder injuries was therefore 1.1% in rugby players and 1.9% in soccer players. The mean age at the time of injury was 28 years (range, 18-35 years) (Table 2). The mean return to play was 127 days in patients who were treated nonoperatively and 163 days in those who underwent operative treatment. The time of injury in relation to the off-season was not recorded. Return to play was probably longer in athletes injured toward the end of the competitive season, which may have altered the results. However, we did not perform a subanalysis of this group.
TABLE 1.
Descriptions of Each Patient in the Seriesa
| No. | Profession | Injury Occurrence | Age, y | Previous Surgery | Injury Mechanism | Diagnosis Modality | Scapula Fracture | Treatment | Return to Activity, d |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Rugby league: center | Rugby match | 25 | DI | XR | Scapula neck/body | Nonoperative | 59 | |
| 2 | Rugby league: hooker | Rugby match | 22 | Stabilization | OA | MRA | Glenoid (Ideberg 1B) | Arthroscopic guided fixation and labral repair | 148 |
| 3 | Rugby league: hooker | Rugby training | 23 | ACJ reconstruction and coracoid fixation | ABER | MRA | Coracoid base fracture extending into glenoid | Open fixation | 172 |
| 4 | Rugby league: prop | Rugby match | 18 | DI | XR | Scapula neck/body | Nonoperative | 163 | |
| 5 | Rugby union: flanker | Rugby match | 33 | Latarjet | DI | XR | Scapula neck/bodyb | Nonoperative | Retired |
| 6 | Rugby union: fullback | Rugby match | 35 | OA | MRI | Glenoid (Ideberg 2) | Arthroscopic guided fixation | 169 | |
| 7 | Rugby union: fullback | Rugby match | 33 | DI | XR | Scapula neck/body | Nonoperative | 146 | |
| 8 | Rugby union: hooker | Rugby match | 28 | DI | XR | Scapula neck/bodyb | Nonoperative | ||
| 9 | Rugby union: wing | Rugby match | 30 | Previous stabilization then Latarjet | ABER | XR | Acromion and glenoid (Ideberg 3) | Nonoperative | 90 |
| 10 | Professional soccer: goalkeeper | Soccer training | 22 | DI | XR | Scapula neck/body | Nonoperative | 179 | |
| 11 | Surveyor | Soccer match | 28 | DI | XR | Scapula neck/body | Nonoperative | 37 |
aABER, abduction and external rotation; ACJ, acromioclavicular joint; DI, direct impact; MRA, magnetic resonance imaging arthrography; MRI, magnetic resonance imaging; OA, outstretched arm; XR, radiograph.
bAssociated injury: suprascapular nerve palsy.
TABLE 2.
Characteristics and Management of Patients Sustaining Sports-Related Scapula Injuries (N = 11)
| Mean (Range) or n (%) | |
|---|---|
| Age, y | 28 (18-35) |
| Time to presentation, d | 8 (2-22) |
| Injury identified on initial radiographs | 8 (73) |
| Associated injuries | 2 (18)a |
| Previous surgery | 4 (36) |
| Nonoperative treatment | 8 (73) |
| Operative management | 3 (27) |
| Return to play, d | |
| Nonoperative | 127 |
| Operative | 163 |
| Unable to return to activity | 1 (9) |
aSuprascapular nerve injury.
Four patients had previous surgery on the injured shoulder. One of the professional rugby players had a previous acromioclavicular joint (ACJ) injury requiring reconstruction and then a separate scapula fracture requiring surgical fixation several years later. One player had a previous anterior labral stabilization, and another 2 had previous Latarjet procedures.
Eight rugby players experienced their injury during a match, 1 during training, and the professional soccer player also had an injury in training. The amateur soccer player sustained his injury during a match. Seven patients sustained extra-articular fractures of the scapula neck and body, while 4 sustained intra-articular fractures involving the glenoid. All scapula neck and body fractures were identified on simple radiographs, while only 1 of the 4 intra-articular glenoid injuries was identified on plain radiographs. These injuries were detected on further magnetic resonance imaging (MRI) and MRI arthrography (MRA).
Mechanism of Injury
A total of 7 patients sustained their injury via a direct impact mechanism, either during a tackle or by diving for the ball (Figure 1). Five were rugby players and 2 were soccer players. All the patients in this group sustained fractures to the scapula neck and/or body. The injuries were all extra-articular and did not involve the superior shoulder suspensory mechanism (ie, clavicle, acromion, coracoid, or ACJ). These patients were all treated nonoperatively with a short period of symptomatic immobilization and early physical therapy. Within this group, 2 rugby players were found to clinically have suprascapular nerve injuries, which were subsequently confirmed by electromyography. Both patients initially complained of shoulder weakness. Clinically, they had weakness of shoulder ABER, with MRI findings of neurogenic edema. One was simple neurapraxia, which resolved with time. The other injury was more serious, leading to muscle wasting and persisting shoulder weakness. The individual retired from professional sport.
Figure 1.

Images demonstrating a scapula fracture pattern associated with a direct injury mechanism. Panel (A) is from one patient and panels (B) and (C) from another. (A) Three-dimensional computer tomography reconstruction. (B) Anteroposterior radiograph. (C) Axial magnetic resonance image.
There were 2 patients who sustained their injuries by outstretched arm mechanism (Figure 2); both intra-articular glenoid fractures involving >25% of the articular surface. Of note, 1 patient had an inferior rim fracture (Ideberg 2)12 associated with a large anterior and inferior labral tear. The second patient sustained a large posterior rim fracture with a significant SLAP (superior labrum anterior and posterior) and posterior labral tear. Both these patients were treated operatively with arthroscopic-assisted internal fixation and arthroscopic treatment of the associated soft tissue injuries. There was no evidence of dislocation in these patients at the time of injury.
Figure 2.
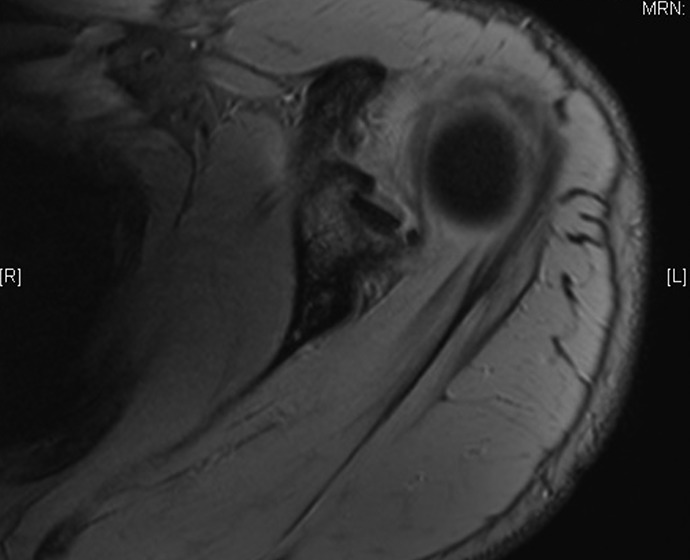
Axial T2-weighted magnetic resonance image demonstrating a scapula fracture pattern associated with an outstretched arm mechanism of injury.
Two patients sustained fractures via an ABER mechanism. One patient sustained a coracoid base fracture that extended into the anterior glenoid rim. Approximately 10% of the glenoid articular surface was involved. This patient was treated with open reduction and internal fixation with cannulated screws (Figure 3). The second patient sustained an oblique fracture through the glenoid articular surface that traversed the body to the acromial base and involved the acromion, similar to an Ideberg 3 (Figure 4).12 The fracture in this case was minimally displaced and was successfully treated with nonoperative immobilization and subsequent physical therapy. The indications for surgery were displaced intra-articular fractures as well as undisplaced intra-articular fractures with an associated labral tear. All these fractures were fixed within 6 weeks of injury.
Figure 3.

Images demonstrating a scapula fracture pattern and management associated with an abduction and external rotation mechanism of injury. (A) Axial computer tomography image. (B) Glenoid open reduction internal fixation in the same patient.
Figure 4.
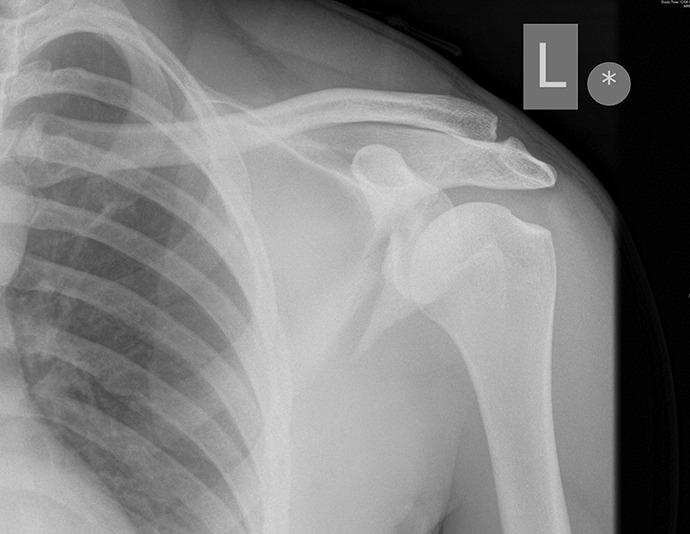
Anteroposterior radiograph demonstrating a scapula fracture pattern associated with an abduction and external rotation mechanism of injury.
Return to Play
Professional players who were treated nonoperatively had a mean return to play of 127 days (range, 59-179 days). The 1 patient in this series who was an amateur soccer player was able to return to his nonphysical profession within 37 days, but it is not known if he has returned to playing soccer. One professional patient with a nonoperatively treated scapula fracture attended only his first appointment, and there is no information regarding when he returned to play. Professional players who were treated operatively had a slightly longer time to return to play of 163 days (range, 148-172 days). Of note, 1 rugby player with a scapular neck fracture was forced to retire from professional sport owing to persisting weakness and muscle wasting from a suprascapular nerve palsy.
Discussion
The results of this study demonstrated that scapula fractures in rugby or soccer players are associated with a prolonged recovery time of 4 to 5 months. As the mechanism of injury is highly predictive of the injury patterns, a detailed history of the exact mechanism is important in identifying the injury. This is particularly true, as 75% of glenoid fractures were not identified on radiographs but on MRI and MRA. There was also an increased incidence of suprascapular nerve injuries in rugby players with scapula fractures. While all of the scapula neck and body fractures were managed nonoperatively, 18% of cases overall and 22% of rugby players (2 patients) had an associated suprascapular nerve injury. Furthermore, 4 patients had a previous shoulder injury. These included an ACJ injury requiring reconstruction and then a separate scapula fracture requiring surgical fixation several years later. One player had a previous anterior labral stabilization, and another 2 had previous Latarjet procedures. This is important to note, as it may be a risk factor for a recurrent injury/fracture.
There is little in the literature focusing on scapula injuries in professional rugby players other than its incidence10 and little with regard to soccer players. Scapula fractures are associated with a 13% chance of a concomitant brachial plexus injury in road traffic collisions and a suprascapular injury rate of 7%.10 The rate of suprascapular nerve injury in rugby players was 22% in our study. The literature also reports high rates of ongoing pain after scapula neck and body injuries treated nonoperatively, with rates of exertional weakness approaching 40% to 60% of cases.1 A scapula fracture can therefore be a career-ending injury for a professional sportsperson, and this was the case in 1 of our patients. It is not clear if this patient cohort should have a lower threshold for surgical treatment.
There are 6 cases reported in the literature that were sustained during American football.2,3,13 Cain and Hamilton3 presented a series of 4 cases. Two players sustained a direct blow to the scapula and extra-articular body fractures. One player sustained an anterior dislocation with a glenoid rim fracture, while the final player had a coracoid and anterior intra-articular glenoid body fracture. No information was reported with regard to the arm position during injury. All patients were treated nonoperatively and sustained a full recovery. Brown et al2 reported a case of bilateral fractures sustained by separate injuries. The first was a direct blow leading to a body fracture, which was treated nonoperatively; the second was sustained with the arm in ABER, leading to an anterior intra-articular glenoid fracture extending to the coracoid base, which was united at the time of surgery. The final case was reported by Kaminsky and Pierce13 and involved a delayed presentation of a scapula body nonunion via an unclear mechanism.
The current report brings the number of case reports of scapula fractures in contact field sports to 17. Based on our data and those in the reports mentioned so far, there is evidence to demonstrate an association between the mechanism of injury, including arm position, and the fracture patterns sustained by the patient, which we have classified into 3 categories (Figure 5). We propose that direct lateral and posterior scapula impact (type A) leads to scapula body and neck fractures. Although most are managed nonoperatively, a careful neurological examination is required. An injury sustained via an outstretched arm (type B) leads to Ideberg type 1B or type 2 fracture of the posterior glenoid and is associated with posterior labral tears. Forced loading in ABER (type C) leads to Ideberg 1A and an anterior fracture that includes the coracoid base. Type B and type C injury mechanisms are difficult to detect on radiographs, and a low threshold for further imaging is required. By noting the exact mechanism and arm position at the time of injury, these classifications can aid timely diagnosis of these shoulder injuries and their sequelae.
Figure 5.

Mechanism of injury and the proposed scapula fracture classification. Type A: Extra-articular fracture involving the scapula neck and body. Type B: Intra-articular glenoid fracture involving >25% of the articular surface. Type C: Intra-articular glenoid fracture extending into the base of the coracoid.
Limitations
This study has a few limitations. As not all athletes in our clinical database had imaging beyond plain radiographs, it may be that some injuries were missed, which would have increased the size of this case series. Despite this center receiving a high volume of sports-related shoulder injuries in professional athletes, this remains a relatively small retrospective case series. The small numbers did not allow any statistical comparison beyond descriptive analysis. However, this is a rare injury poorly described in the rugby and soccer player populations, and to our knowledge, this case series remains the largest in the literature of scapula fractures in contact field sports.
Conclusion
Scapula fractures acquired in sports are a serious injury with a prolonged recovery period, and they can have career-ending effects. The mechanism of injury can help predict the fracture pattern and highlight the need for further imaging. There is a high association of these fracture patterns with suprascapular nerve injuries, which must be examined during clinical assessment. These high-energy injuries are rarely described in athletes and classically relate to major trauma, highlighting the forces associated with rugby and other contact sports.
Acknowledgment
The authors thank Catherine Sulzmann for her talented illustrations.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
- 1. Ada JR, Miller ME. Scapular fractures: analysis of 113 cases. Clin Orthop Relat Res. 1991;269:174–180. [PubMed] [Google Scholar]
- 2. Brown MA, Sikka RS, Guanche CA, Fischer DA. Bilateral fractures of the scapula in a professional football player: a case report. Am J Sports Med. 2004;32(1):237–242. [DOI] [PubMed] [Google Scholar]
- 3. Cain TE, Hamilton WP. Scapular fractures in professional football players. Am J Sports Med. 1992;20(3):363–365. [DOI] [PubMed] [Google Scholar]
- 4. Cole PA, Gauger EM, Schroder LK. Management of scapular fractures. J Am Acad Orthop Surg. 2012;20(3):130–141. [DOI] [PubMed] [Google Scholar]
- 5. Court-Brown CM, Wood AM, Aitken S. The epidemiology of acute sports-related fractures in adults. Injury. 2008;39(12):1365–1372. [DOI] [PubMed] [Google Scholar]
- 6. Crichton J, Jones DR, Funk L. Mechanisms of traumatic shoulder injury in elite rugby players. Br J Sports Med. 2012;46(7):538–542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF. The floating shoulder: clinical and functional results. J Bone Joint Surg Am. 2001;83(8):1188–1194. [DOI] [PubMed] [Google Scholar]
- 8. Fuller CW, Brooks JH, Cancea RJ, Hall J, Kemp SP. Contact events in rugby union and their propensity to cause injury. Br J Sports Med. 2007;41(12):862–867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Goss TP. Scapular fractures and dislocations: diagnosis and treatment. J Am Acad Orthop Surg. 1995;3(1):22–33. [DOI] [PubMed] [Google Scholar]
- 10. Headey J, Brooks JH, Kemp SP. The epidemiology of shoulder injuries in English professional rugby union. Am J Sports Med. 2007;35(9):1537–1543. [DOI] [PubMed] [Google Scholar]
- 11. Herscovici D, Jr, Fiennes AG, Allgower M, Ruedi TP. The floating shoulder: ipsilateral clavicle and scapular neck fractures. J Bone Joint Surg Br. 1992;74(3):362–364. [DOI] [PubMed] [Google Scholar]
- 12. Ideberg R, Grevsten S, Larsson S. Epidemiology of scapular fractures: incidence and classification of 338 fractures. Acta Orthop Scand. 1995;66(5):395–397. [DOI] [PubMed] [Google Scholar]
- 13. Kaminsky SB, Pierce VD. Nonunion of a scapula body fracture in a high school football player. Am J Orthop (Belle Mead NJ). 2002;31(8):456–457. [PubMed] [Google Scholar]
- 14. McGahan JP, Rab GT, Dublin A. Fractures of the scapula. J Trauma. 1980;20(10):880–883. [DOI] [PubMed] [Google Scholar]
- 15. Usman J, McIntosh AS, Frechede B. An investigation of shoulder forces in active shoulder tackles in rugby union football. J Sci Med Sport. 2011;14(6):547–552. [DOI] [PubMed] [Google Scholar]
- 16. Zlowodzki M, Bhandari M, Zelle BA, Kregor PJ, Cole PA. Treatment of scapula fractures: systematic review of 520 fractures in 22 case series. J Orthop Trauma. 2006;20(3):230–233. [DOI] [PubMed] [Google Scholar]