

Abstract
Objectives:
To describe causes of blindness and visual impairment (VI) in children in Eastern province, Saudi Arabia.
Methods:
A record-based descriptive cross-sectional study was conducted. Medical records of patients aged 2 to 16 years who were following up in the Pediatric Ophthalmology Clinics, Dhahran Eye Specialist Hospital, Dhahran, Saudi Arabia between September and December 2018 were reviewed. Causes of vision loss according to visual acuity (VA) with best correction were recorded. Blindness was defined as VA <20/400, VI as VA from 20/400 to 20/60, and visual loss as VA of ≤20/60.
Results:
Of 818 patients, 39% had visual loss, 22.9% were blind, and 71.2% had VI. Common etiologies of bilateral blindness were retinal dystrophy disease and Leber’s congenital amaurosis, whereas unilateral blindness was most common due to trauma and refractive error (RE). Common etiologies of bilateral VI were RE, esotropia, and retinal dystrophy. Unilateral VI was mainly due to RE, cataract, congenital esotropia, and trauma. Of all patients, 58.8% had treatable causes, 22.6% had preventable causes, and 19.5% had non-preventable and non-treatable causes; mostly genetic or congenital (59.7%) rather than acquired (40.2%).
Conclusion:
Genetic or congenital causes are major factors causing blindness. Most causes are treatable and preventable, emphasizing on early detection and treatment of those causes.
Childhood blindness is a health condition that has a major impact on different aspects of children’s lives. It can adversely affect future learning, job opportunities, and quality of life. Mortality rate is noted to be higher in blind than in sighted children.1-3 Blindness is a disability that affects not only the child, rather it extend to their family and community as it has an impact on person’s productivity.3 As reported by the 2018 International Classification of Disease (ICD 11), blindness is defined as presented visual acuity (VA) less than 3/60 (20/400); visual impairment (VI) is divided into severe-presented VA that is worse than 6/60 (20/200), moderate-presented VA that is worse than 6/18 (20/60), and mild-presented VA that is worse than 6/12 (20/40).4 In the Kingdom of Saudi Arabia (KSA), blindness is very common and considered a main disability. The prevalence of blindness is 1.5% and VI 7.8% in KSA.5 The causes of childhood blindness are mostly from ocular or systemic diseases that differ between countries.6 There has been limited studies on reversible and irreversible causes of visual loss in the pediatric population in the eastern province of KSA. The main objective of this research was to elucidate the causes of visual loss in a pediatric age group at a tertiary healthcare center in eastern province of Saudi Arabia.
Methods
A record-based descriptive cross-sectional study was carried out to identify the reasons of visual loss in a pediatric group aged between 2 to 16 years at a tertiary healthcare center in eastern province of KSA. Total of 818 patients who were following up at the Pediatric Ophthalmology Clinic in Dhahran Eye Specialist Hospital, Dhahran, KSA (DESH) were reviewed. Only patients who were blind or visually impaired according to the 2018 ICD 11 definition were enrolled.4 The differentiation of blind and visually impaired patients (either unilateral or bilateral) was performed according to VA with best correction.
Visual loss was defined as VA of blindness <20/400, and VI is VA from 20/400 to 20/60. In total, 323 patients were enrolled in this study. Data were retrospectively gathered from patients’ medical records between January 2014 to December 2018 in DESH, including age (2-16 years), gender, nationality, VA for both eyes with best correction, causes of unilateral and bilateral blindness or VI, and underlying causes of poor vision (genetic, congenital, or acquired), and whether the cause was preventable or treatable depending on the nature of the diseases encountered. Records not showing any of the mentioned parameters were excluded. In this study, ethical approval was obtained from DESH for access to the data.
All categorical data were approached by frequency with percentage, and continuous data were approached by mean with standard deviation. All the analysis was carried out by using IBM SPSS for Windows, version 21 (IBM Corp, Armonk, NY, USA). Institutional Review Board approval was obtained.
Results
Of 818 patients, 323 (39%) had visual loss (VA of ≤20/60). The study included 323 patients who were between 2 to 16 years (average age, 5.6±2.8 years). There were 154 (47.7%) females and 169 (52.3%) males. In the sample, 126 (39%) patients were younger than 4 years, 121 (37.5%) were between 5 to 7 years, 58 (18%) were between 8-10 years, 15 (4.6%) were between 11 to 13 years, and 3 (0.9%) were between 14 to 16 years. Saudi constitute for 97.5% while only 2.5% were non-Saudi.
The most frequent etiologies of blindness among 74 (22.9%) patients were trauma in 12 (16.2%) cases and refractive errors (RE) in 10 (13.5%) cases. Specifically, the most frequent etiologies of bilateral blindness were retinal dystrophy disease in 3 (18.8%) cases and Leber’s congenital amaurosis (LCA) in 3 (18.8%) cases. The most frequent etiologies of unilateral blindness were trauma in 12 (20.7%) cases and RE in 9 (15.5%) cases (Table 1). The most frequent etiologies of VI among 230 (71.2%) patients were RE in 58 (25.2%) cases and congenital esotropia in 29 (12.6%) cases. Specifically, the most frequent etiologies of bilateral VI were RE in 19 (19.3%) cases, followed by congenital esotropia and retinal dystrophy accounting for 12 (12.2%) cases each. The most frequent etiologies of unilateral VI were RE in 39 (29.5%) cases, followed by cataract, congenital esotropia, and trauma accounting for 17 (12.9%) cases each (Table 1). Furthermore, 19 (5.9%) of the 323 patients were blind in one eye associated with VI in the other eye. The most frequent causes were retinal dystrophy in 3 (15.8%) cases and RE in 3 (15.8%) cases.
Table 1.
Causes of unilateral and bilateral blindness among 74 children.
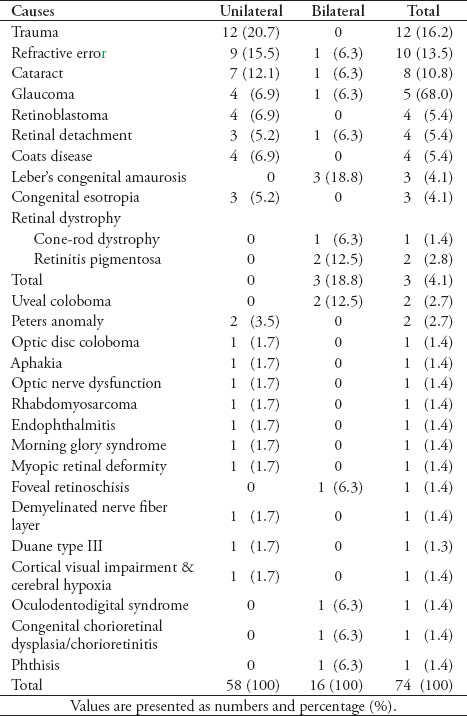
Table 2.
Causes of unilateral and bilateral visual impairment among 230 children.
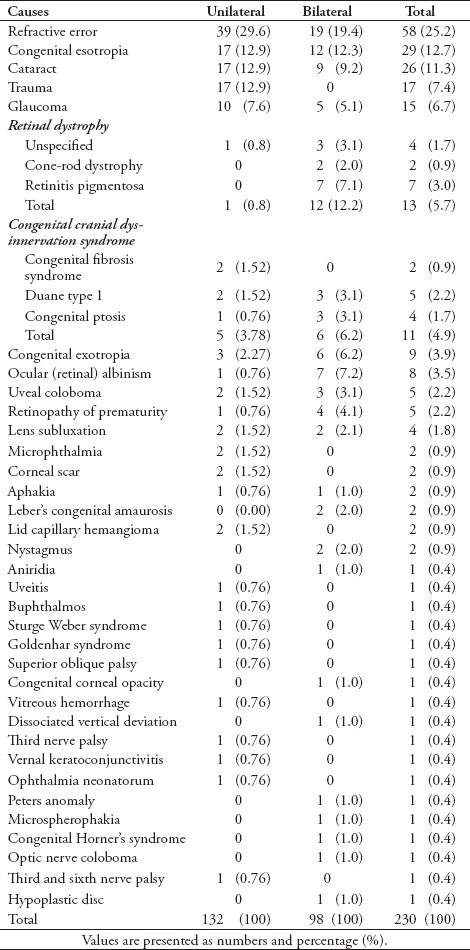
Of the 74 blind cases, 12 were traumatic. The most common cause was globe rupture in 4 (33.3%) cases. Moreover, among the 230 VI cases, 19 were traumatic. The most common cause was cataract in 6 (35.3%) cases. Most of the patients had treatable causes 187 (57.8%) while the others had preventable 73 (22.6%) or non-preventable/non-treatable causes 63 (19.5%) of 323 patients.
Genetic or congenitally determined factors were the primary causes, accounting for 193 (59.7%) of 323 patients. In contrast, acquired causes accounted for 130 (40.2%) of 323 patients. Patients with blindness comprised 45 of 74 patients with genetic or congenitally determined causes accounting for 60.8%, compared to 29 of 74 patients with acquired causes accounting for 39.2%. Furthermore, 135 of 230 patients with VI had genetic or congenitally determined causes, accounting for 58.7%, whereas 95 of 230 patients had acquired causes, accounting for 41.3%. Moreover, 13 of 19 patients with both blindness in a single eye and VI in the other had genetic or congenitally determined causes, accounting for 68.4%; whereas 6 of 19 patients had acquired causes, accounting for 31.6%.
Discussion
The prevalence of childhood blindness varies between nations due to socioeconomic factors.2,7,8 Gross domestic product per capita (GDP) and less than 5-year mortality rate have been identified as major socioeconomic factors. In the Eastern Mediterranean region, 23 countries were divided based on GDP into 3 groups and are coded as: 1-high, 2-medium, and 3-low-income. Similar causes of childhood blindness were noted in groups one and 2, including perinatal and genetic causes, retinopathy of prematurity (ROP), and cataract being the most common. Furthermore, among these groups infectious and nutritional causes were rare. In contrast, group 3 showed a higher incidence of nutritional and infectious causes, with major causes.2
Another study that considered all Middle East countries as a single entity and defined them as middle-income countries produced similar conclusions, with the most common causes of childhood blindness being cataract, ROP, glaucoma, and teratogens.7 In this study KSA is considered a middle income country.7 Whereas, in the previously mentioned study, it was one of the high income countries.2
Results of a community-based survey conducted in 1986, from a random multi-stage stratified cluster sample of the Saudi population indicated that the prevalence of blindness was 1.5%, and VI 7.8% in KSA, as defined by WHO.5
Several researches on childhood blindness have been carried out in Riyadh, KSA. One of the earliest studies in 1985, revealed a change in the pattern of childhood blindness causes. The author compared causes of childhood blindness among those who were born before 1962 to those who were born during or after 1962. The results showed a major shift from acquired to congenital causes during the years following 1962.9 Two further studies conducted in Riyadh, KSA during 2005 and 2006, and a study in Jazan in 2016 showed similar results.3,5,10
In our study, the most encountered causes of blindness were trauma and RE. Specifically, the most encountered causes of bilateral blindness were retinal dystrophy disease and LCA, while the most encountered causes of unilateral blindness were trauma and RE. Furthermore, the most encountered causes of VI were RE and congenital esotropia. Specifically, the most encountered causes of bilateral VI were RE, congenital esotropia, and retinal dystrophy, while the most encountered causes of unilateral VI were RE, cataract, congenital esotropia, and trauma. These results indicate that congenital causes accounted for 59.7% of cases. Infection-related causes were not observed in this study, possible due to the substantial reduction in cases of measles and rubella following the implementation of mandatory vaccinations.11
These results are consistent with those of Tabbara et al,3 which indicate that congenital etiology is primarily the cause of visual loss. In the study, it was also evident that there is a relation between consanguinity and genetic/congenital causes.3 This could not be proven in our study due to the lack of data concerning this matter.
Collectively, preventable factors comprised 22.6% of the causes of visual loss. Hence, efforts should be enacted to control these etiologies. This could be achieved by investing in screening and early detection of such factors. Suggested recommendations include early neonatal eye examination before home discharge, screening campaigns for children in schools, and early management of cataract to prevent amblyopia. Trauma was the primary cause of unilateral blindness among children; this could be prevented by increasing community awareness regarding the adverse outcomes of leaving hazardous toys, fireworks, and sharp objects in the reach of children.
It is worth mentioning that the Ministry of Health and Ministry of Education in KSA, have implemented programs for early detection of visual defects especially RE in children. These include, mandatory vision assessment before entering school and a national screening program for school students which also includes vision check-ups.
In this study, more than half of the causes were treatable (57.8%), which emphasizes the importance of early neonatal examination for detecting and treating these causes. For instance, RE were the second cause of blindness and the primary cause of VI. This condition is easily corrected using spectacles, which is a cost-effective measure and improves children’s education experience.2,12
Study limitations
This study include biased sample as it comprised referred patients at a tertiary healthcare center; which does not fully reflect the wider community. As such, our study may not fully recapitulate the true prevalence of blindness and VI in pediatric population in the eastern province of KSA. In this regard, we recommend conducting community-based studies reflecting the true prevalence of blindness and VI in KSA.
In conclusion, the most encountered causes of blindness were trauma and RE. The most encountered causes of VI were RE, and congenital esotropia. Furthermore, in patients who had blindness in one eye with VI in the other causes include retinal dystrophy and RE. In this study, genetic/congenitally determined causes were identified as major causes of visual loss. Most of the identified etiologies are treatable or preventable, which emphasizes the importance of early detection and treatment of those causes.
Acknowledgment
We authors gratefully acknowledge the Ophthalmology and Medical Record Department at Dhahran Eye Specialist Hospital in the Eastern Province of Saudi Arabia that helped us to conduct this study and data collection. We would also like to thank Editage (https://www.editage.com/) for English language editing.
Footnotes
References
- 1.Gilbert C, Awan H. Blindness in children. BMJ. 2003;327:760–761. doi: 10.1136/bmj.327.7418.760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Khandekar R, Kishore H, Mansu R, Awan H. The status of childhood blindness and functional low vision in the eastern Mediterranean region in 2012. Middle East Afr J Ophthalmol. 2014;21:336–343. doi: 10.4103/0974-9233.142273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tabbara K, El-Sheikh H, Shawaf S. Pattern of childhood blindness at a referral center in Saudi Arabia. Ann Saudi Med. 2005;25:18–21. doi: 10.5144/0256-4947.2005.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Health Orghanization, International. Vision impairment and blindness. 2018. [Cited 12 January 2019]. Available from: http://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment .
- 5.Kotb A, Hammouda E, Tabbara KF. Childhood blindness at a school for the blind in Riyadh, Saudi Arabia. Ophthalmic Epidemiol. 2006;13:1–5. doi: 10.1080/09286580500477317. [DOI] [PubMed] [Google Scholar]
- 6.Alghamdi H. Causes of irreversible unilateral or bilateral blindness in the Al Baha region of the Kingdom of Saudi Arabia. Saudi J Ophthalmol. 2016;30:189–193. doi: 10.1016/j.sjopt.2016.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Foster A. Childhood blindness. Eye. 1988;2:S27–36. doi: 10.1038/eye.1988.131. [DOI] [PubMed] [Google Scholar]
- 8.Zeidan Z, Hashim K, Muhit M, Gilbert C. Prevalence and the causes of childhood blindness in camps for displaced persons in Khartoum:Results of a household survey. East Mediterr Health J. 2007;13:580–585. [PubMed] [Google Scholar]
- 9.Tabbara K, Badr I. Changing pattern of childhood blindness in Saudi Arabia. Br J Ophthalmol. 1985;69:312–315. doi: 10.1136/bjo.69.4.312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Darraj A, Barakat W, Kenani M, Shajry R, Khawaji A, Bakri S, et al. Common eye diseases in children in Saudi Arabia (Jazan) Ophthalmol Eye Dis. 2016;8:33–39. doi: 10.4137/OED.S39055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tufenkeji H, Rattan H. Childhood immunization in the kingdom of Saudi Arabia. Ann Saudi Med. 1994;14:91–93. doi: 10.5144/0256-4947.1994.91. [DOI] [PubMed] [Google Scholar]
- 12.Al-Tamimi E, Shakeel A, Yassin S, Ali S, Khan U. A clinic-based study of refractive errors, strabismus, and amblyopia in pediatric age-group. J Family Community Med. 2015;22:158–162. doi: 10.4103/2230-8229.163031. [DOI] [PMC free article] [PubMed] [Google Scholar]