

Abstract
Rationale:
Crossed renal ectopia (CRE) is a rare congenital anomaly that is frequently associated with gastrointestinal, cardiovascular, genital and bone malformations. To the best of our knowledge, only 35 cases of crossed renal ectopia involving calculi and 30 cases of CRE associated with renal carcinoma have been reported to date.
Patient concerns:
Here, we present 2 cases of crossed renal ectopia. A 59-year-old woman with diabetes presented to our hospital with abdominal pain. The second patient was a 24-year-old woman who complained with abdominal pain with a duration of 1 day.
Diagnoses:
On the basis of abdominal ultrasonography, we suspected a solitary kidney both in the two patients. Combined with retrograde pyelography and 3D computed tomography, case 1 was diagnosed as an S-shaped right-to-left crossed-fused ectopic kidney with many stones in the left (normal) renal pelvis and case 2 was confirmed to have lump right-to-left crossed-fused renal ectopia with two 3-mm stones in the renal pelvis of the 2 kidneys.
Interventions:
Case 1 underwent percutaneous nephrolithotomy while case 2 refused to undergo surgery and underwent conservative treatment for pain relief.
Outcomes:
Two patients have been followed up and have no stones recurrence.
Lessons:
Crossed fused renal ectopia is easily misdiagnosed as a solitary kidney. CRE is so rare that the recognition of the disease needs to be improved and effective treatment should be taken timely. According to the two cases and literature review, minimally invasive surgery has become increasingly common to treat CRE with stones and carcinoma.
Keywords: calculi, crossed-fused renal ectopia, percutaneous nephrolithotomy, renal carcinoma
1. Introduction
Crossed renal ectopia is a rare congenital anomaly in which the kidneys are located on the same side, whereas the ureter of the ectopic kidney still descends to the normal location on the bladder. The anomaly consists of two types: crossed-unfused renal ectopia and crossed-fused renal ectopia, the latter of which is more common. The incidence of crossed-fused renal ectopia on autopsy and live birth has been reported to be approximately 1:7500 and 1:1000, respectively, with a male predominance.[1–3] The symptoms of the anomaly are not obvious, and most individuals cannot be diagnosed until they undergo a medical examination. According to available published studies, the anomaly is associated with many malformations, including nephrolithiasis, ureteropelvic junction obstruction, renal tumors and cystic dysplasia.[4–6] Hence, early diagnosis and effective therapeutic methods are beneficial. We searched PubMed from 1937 to 2018 with key words such as crossed fused ectopic kidney, crossed-fused renal ectopia, crossed renal ectopia, crossed renal ectopia calculi or stones, and crossed renal ectopia carcinoma or cancer. To date, only 35 cases of in crossed ectopic kidneys involving stones and 30 cases associated with renal carcinoma have been reported. The clinical data are presented in Tables 1 and 2. Although a few cases managed by surgery have been reported, there are no standard guidelines for treating crossed-fused ectopic kidneys with stones or renal carcinoma.
Table 1.
Review of reported crossed renal ectopia cases associated with stones.
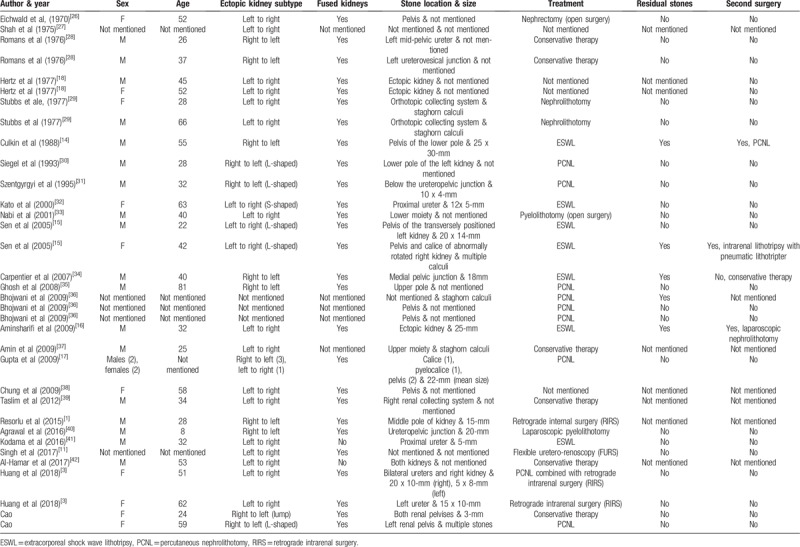
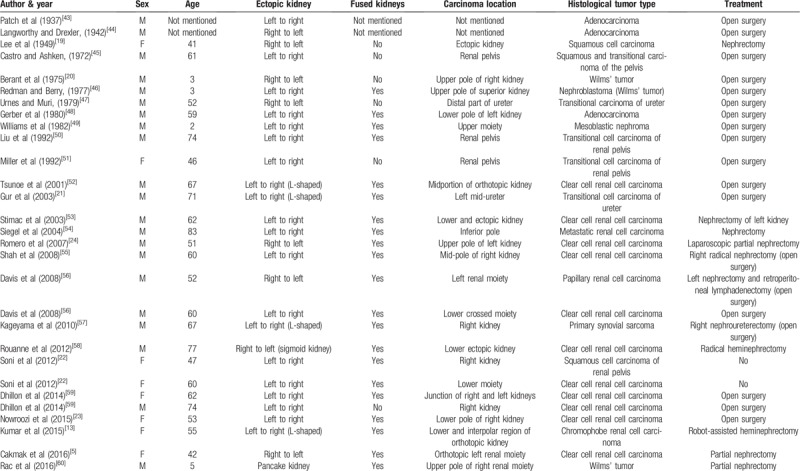
Table 2.
Review of reported cases of crossed renal ectopia associated with renal carcinoma.
Here, we report 2 cases of crossed-fused ectopic kidney with stones managed by percutaneous nephrolithotomy and medicine and review the available English literature.
2. Case report
2.1. Case 1
A 59-year-old woman with diabetes presented to our hospital with abdominal pain. Her physical examination showed dull pain in the abdomen and no fever or flank pain on percussion. The laboratory findings revealed pyuria (white blood cell count in urine: 87.8 HPF). The renal function and other laboratory tests showed no abnormalities. Abdominal ultrasonography revealed the absence of the right kidney and a solitary left kidney with two ureters. For further examination, plain film of kidney-ureter-bladder (KUB), retrograde pyelography and 3D computed tomography were used to confirm the anomaly. 3D computed tomography showed an S-shaped right-to-left crossed-fused ectopic kidney with many stones in the left (normal) renal pelvis. (Fig. 1A) The crossed ectopic kidney was located inferior to the left kidney with fusion. Vascular anomalies were also found that the right renal artery was supplied by the anterior wall of the abdominal aorta, while the lower right renal vein passed up into the left renal vein. After considering the benefits and risks, the patient agreed to undergo PCNL owing to her rare anomaly and aberrant renal anatomy (Fig. 1B).
Figure 1.
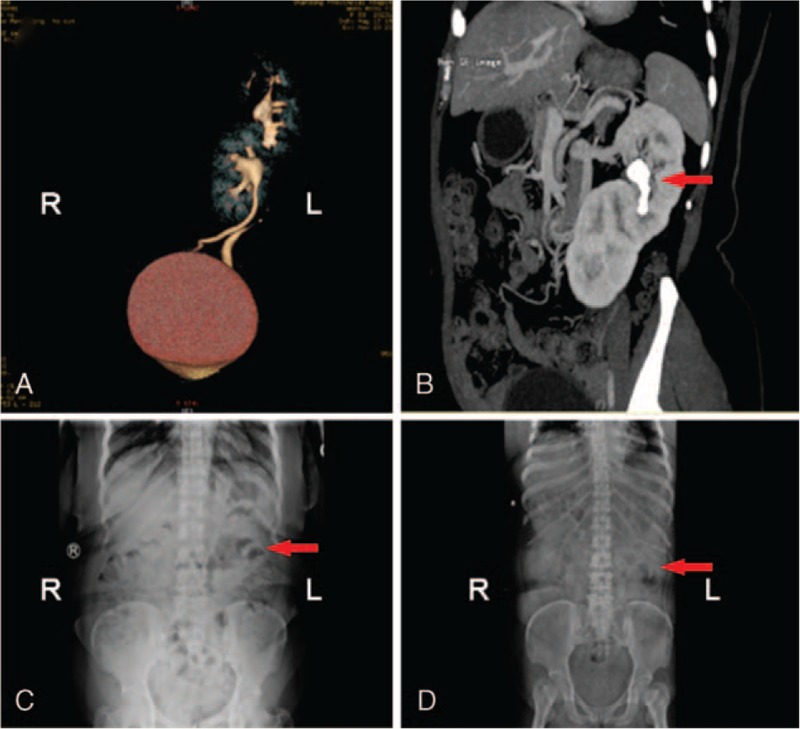
3D computed tomography and X-ray images of patient 1. (A) 3D computed tomography revealed S-shaped right-to-left crossed-fused renal ectopia. (B) CT demonstrated the vascular anomaly and calculi in the left renal pelvis (arrow). (C) Preoperative abdominal X-ray revealed stone shadows (arrow) in the left abdominal area. (D) Postoperative KUB showed no stone shadows.
After the induction of general anesthesia, the patient was placed in the lithotomy position for inspection of the bladder and ureters using a rigid ureteroscope, and abnormities were found. Then, 2 5-F ureteral stents were placed in the left ureter and an 18-F catheter was placed before the patient was moved into the right lateral decubitus position. Under ultrasound guidance, the left renal pelvis was accessed, and the guide wire was placed in the tract. The stones were confirmed and visualized by the ureteroscope going through the tract. The biggest diameter of these stones was about 9-mm. After dilating the tract to 24-F, we combined the rigid nephroscope with a pneumatic lithotripter to fragment and eliminate the stones. Finally, a double-J tube was placed in the left ureter, and a 14-F nephrostomy tube was routinely placed in the tract after complete stone clearance. The procedure lasted 80 minutes and was successful without the need for blood transfusion or the occurrence of any complications. The patient underwent renal ultrasound before the 14-F nephrostomy tube was removed 6 days after the surgery. We compared the pre- and postoperative KUB findings to ensure complete stone clearance (Fig. 1C and D). After a year of follow-up, the patient stayed asymptomatic with no stone recurrence detected by abdominal ultrasonography.
2.2. Case 2
In the second case, the patient was a 24-year-old woman. She presented with abdominal pain with a duration of 1 day. The physical examination showed acute pain in the left flank. The laboratory tests revealed pyuria and hematuria (white blood cell count in urine: 33.7 HPF; red blood cell count in urine: 258.4 HPF). Abdominal ultrasonography showed absence of right kidney on the right side. 3D computed tomography revealed right-to-left crossed renal ectopia and two 3-mm stones in the renal pelvis of the two kidneys. (Fig. 2) The ectopic kidney fused with the normal kidney and the ureter of the ectopic kidney descended and crossed the midline, just anterior to the fifth lumbar vertebra. The patient refused to undergo surgery and underwent conservative treatment for pain relief. At length, the stones were completely cleared without surgery, which was confirmed by abdominal ultrasonography. The symptoms of flank pain, pyuria and hematuria disappeared. She remained asymptomatic after 12 months of follow-up. The patient underwent abdominal ultrasonography during the follow-up because she refused the expense of the CT scan.
Figure 2.
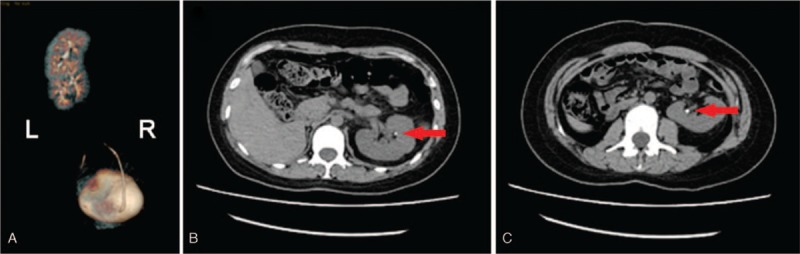
3D CT images of patient 2. (A) 3D CT image revealed lump right-to-left crossed-fused renal ectopia. (B, C) CT demonstrated two 3-mm stones in both renal pelvises.
3. Discussion
The incidence of crossed-fused renal ectopia on autopsy has been reported to be approximately 1:7500, which is about 10 times higher than that of the unfused ectopia.[1–3] In crossed-unfused renal ectopia, the ectopic kidney crosses the midline but the renal parenchyma of ectopic kidney does not fuse with that of normal kidney. The ureter of the ectopic kidney descends and crosses the midline and enters the urinary bladder at its normal position. In crossed-fused renal ectopia, the ectopic kidney crosses to the opposite side and fuses with the normal kidney. The ectopic kidney is usually located inferior to the normal kidney with fusion. Crossed-fused renal ectopia is a rare congenital abnormal development of the urinary system. There are 6 subtypes of the anomaly:
-
(1)
inferior ectopia, in which the ectopic kidney lies inferior to the normal kidney;
-
(2)
superior ectopia, in which the upper pole of the normal kidney fuses with the lower pole of the ectopic kidney;
-
(3)
sigmoid or S-shaped;
-
(4)
lump or pancake;
-
(5)
L-shaped; and
- (6)
Zhuo Yin et al, however, reported a new subtype of crossed-fused renal ectopia named the “Y” type, in which the ureters of the kidneys are fused.[2] In our report, a 59-year-old woman presented with the S-shaped subtype and a 24-year-old woman presented with the lump subtype.
The diagnosis of crossed-fused renal ectopia can be confirmed by abdominal ultrasonography, KUB, retrograde pyelography and 3D computed tomography before surgery. First, ultrasonography can reveal the absent kidney. KUB and retrograde pyelography can help determine the size and location of any stones present. Attention should be paid to the 3D CT findings because the identification of essential vessels will allow access while avoiding bleeding and unnecessary mishaps.[5] Vascular anomalies are always associated with crossed-fused renal ectopia. In patient 1 in the present study, the right renal artery was supplied by the anterior wall of the abdominal aorta, while the lower right renal vein passed up into the left renal vein, and the two veins then joined the inferior vena cava (Fig. 1B). Moreover, CRE may be associated with urinary abnormalities, such as urinary tract infection, renal calculi and ureteropelvic junction obstruction, principally due to mechanical reasons.[1,9]
This anomaly is so uncommon that there are no standard guidelines for treating associated stones or carcinoma. Minimally invasive measures have been increasingly reported to be helpful in managing this anomaly in association with nephrolithiasis, UPJO, and carcinoma, among others.[3,10–13] After reviewing the available literature, we found 35 cases of crossed renal ectopia associated with stones. The female-to-male ratio was 10:21, and the ratio of the side of the ectopic kidney was 13:20 (left:right). The treatment methods included open surgery in 4 patients, conservative therapy in 5, extracorporeal shock wave lithotripsy (ESWL) in 7, percutaneous nephrolithotomy (PCNL) in 10, retrograde intrarenal surgery (RIRS) in 4 and laparoscopic pyelolithotomy in 1. However, the treatment method in 5 cases was not mentioned, and in 3 patients, ESWL failed, and a second surgery was required.[1,14–18] In our report, patient 1 was completely cleared of stones with PCNL, and patient 2 underwent conservative treatment. After reviewing available studies in the literature thoroughly, we found 30 cases of renal cancer in CRE.[5,19–22] We also found that CRE associated with renal cancer mainly occurs in adults, most commonly as clear cell renal cell carcinoma.[23] Only 4 cases of renal carcinoma in CRE in children have been reported, 3 of which were cases of Wilms’ tumor (Table 2).
The choice of treatment in CRE with stones depends on the vascular anatomy and the size of the stone. As far as we are concerned, patients with small stones without hydronephrosis, such as patient 2, may be treated with conservative therapy. However, those with large calculi and hydronephrosis, such as patient 1, should be treated with surgery to achieve stone clearance. Watchful waiting and close follow-up should be recommended for patients without symptoms because they may be asymptomatic throughout their life. The treatment methods for stones in CRE include open surgery, ESWL, PCNL, RIRS and laparoscopic surgery. With the development of surgical instruments, minimally invasive surgery has become increasingly common and feasible, while the selection of open surgery is gradually decreasing (Table 1). ESWL is an alternative treatment, although it was reported to have failed in 3 patients who had residual stones and required a second surgery.[14–16] Sen et al reported the use of ESWL to treat 2 patients with an L-shaped renal anomaly with stones. The first patient was free of stones after three sessions, while the second patient was treated with retrograde intrarenal lithotripsy after ESWL failed.[15] Aminsharifi et al reported the use of laparoscopic nephrolithotomy to treat a patient with a 25-mm opaque renal stone in left-to-right crossed-fused renal ectopia who had undergone two sessions of ESWL that failed.[16]
Percutaneous nephrolithotomy (PCNL) is another alternative, especially in patients with a large stone burden; however, the risks of bleeding and gastrointestinal injury may increase due to the aberrant vascular supply and the location of the ectopic kidney. Gupta et al reported the use of PCNL to treat 46 patients (52 renal units) with abnormal kidneys, including 4 patients with crossed-fused ectopic kidneys. The mean size of the stones was 22 mm, and the mean operating time was 80 minutes (range, 70–100).[17] Huang et al reported 2 cases of crossed-fused renal ectopia, one with 20-mm stones and one with 15-mm stones. One of the patients underwent PCNL and achieved total stone clearance.[3]
Additionally, to the best of our knowledge, Resorlu et al reported the first use of RIRS in a patient with crossed-fused renal ectopia with a 15-mm stone, which confirmed that RIRS is a safe and feasible minimally invasive choice for application in cases of this anomaly.[1]
Concerning the reports of renal cancer in crossed renal ectopia, clear cell renal cell carcinoma was the most common, and the main surgical method for treatment was open surgery (Table 2). Romero et al were the first to apply laparoscopic heminephrectomy to treat a patient with clear cell renal cell carcinoma associated with right-to-left crossed-fused renal ectopia.[24] Kumar et al reported the first use of robot-assisted heminephrectomy to treat chromophobe renal cell carcinoma in a case of L-shaped renal ectopia. According to the location, size and clinical stage of the renal tumor, radical or partial nephrectomy should be performed as soon as possible to preserve the functional and uninvolved kidney. Crossed-fused ectopic kidneys can even be utilized as donor organs for transplantation.[25]
4. Conclusion
Because of the rarity of crossed renal ectopia, detailed and accurate preoperative examinations and assessments must be emphasized for the diagnosis of the anomaly. The choice of treatment in CRE with stones relies on the vascular anatomy, the size of the stones, the extent of hydronephrosis and the experience of the urologist. Based on the cases provided from the literature, minimally invasive surgery has become increasingly common to treat CRE with stones and carcinoma. Urologists should choose safe, sufficient and feasible methods to cure CRE with abnormalities involving stones, carcinoma and other malformations.
Author contributions
Conceptualization: Yalei Cao, Yinan Zhang, Weiting Kang, Yuanman Luo, Xunbo Jin.
Data curation: Yalei Cao, Yinan Zhang, Weiting Kang, Ning Suo, Zilian Cui, Yuanman Luo.
Funding acquisition: Zilian Cui, Xunbo Jin.
Methodology: Weiting Kang, Ning Suo, Yuanman Luo, Xunbo Jin.
Supervision: Yinan Zhang, Weiting Kang, Ning Suo, Zilian Cui.
Visualization: Ning Suo, Zilian Cui, Yuanman Luo, Xunbo Jin.
Writing – original draft: Yalei Cao.
Writing – review & editing: Yalei Cao.
Yalei Cao orcid: 0000-0002-4197-5547.
Footnotes
Abbreviations: CRE = crossed renal ectopia, ESWL = extracorporeal shock wave lithotripsy, KUB = plain film of kidney-ureter-bladder, PCNL = percutaneous nephrolithotomy, RIRS = retrograde intrarenal surgery, UPJO = ureteropelvic junction obstruction.
How to cite this article: Cao Y, Zhang Y, Kang W, Suo N, Cui Z, Luo Y, Jin X. Crossed-fused renal ectopia with renal calculi: Two Case Reports and a Review of the Literature. Medicine. 2019;98:48(e18165).
Patient has provided informed consent for publication of the case.
Funding disclosure: This work was supported by the 59-class General Financial Grant from the China Postdoctoral Science Foundation; under Grant [number 2016M590638]; The National Natural Science Foundation of China under Grant [number 81572534].
The authors report no conflicts of interest.
References
- [1].Resorlu M, Kabar M, Resorlu B, et al. Retrograde intrarenal surgery in cross-fused ectopic kidney. Urology 2015;85:e5–6. [DOI] [PubMed] [Google Scholar]
- [2].Yin Z, Yang JR, Wei YB, et al. A new subtype of crossed fused ectopia of the kidneys. Urology 2014;84:e27. [DOI] [PubMed] [Google Scholar]
- [3].Huang L, Lin Y, Tang Z, et al. Management of upper urinary tract calculi in crossed fused renal ectopic anomaly. Exp Ther Med 2018;15:371–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Tang L, Koshy J, Spevak MR, et al. Diagnosis of rare association of orthotopic multicystic dysplasia with crossed fused renal ectopia. Case Rep Urol 2014;2014:140850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Cakmak O, Isoglu CS, Peker EA, et al. Renal cell carcinoma in patient with crossed fused renal ectopia. Arch Ital Urol Androl 2016;87:330–1. [DOI] [PubMed] [Google Scholar]
- [6].Hajji F, Moufid K, Ghoundale O, et al. A rare case of pelviureteric junction obstruction in the uncrossed kidney of a crossed fused renal ectopia. Ann R Coll Surg Engl 2018;e1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Wein AJ, Kavoussi LR, Novick AC, Partin AW, CA. P. Campbell-Walsh urology. 9th ed. 2007. [Google Scholar]
- [8].Liu L, Yang J, Zhu L, et al. Crossed-fused renal ectopia associated with inverted-Y ureteral duplication, ectopic ureter, and bicornuate uteruses. Urology 2010;75:1175–7. [DOI] [PubMed] [Google Scholar]
- [9].Saini S, Yadav S, Nayak B. Double trouble: pelvi-ureteric junction obstruction and renal cell carcinoma in right to left crossed fused ectopia. BMJ Case Rep 2016;2016: [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Giani A, Garancini M, Delitala A, et al. 3D-laparoscopic anterior rectal resection in a patient with crossed fused renal ectopia: the importance of 3D imaging. Minerva Chir 2017;72:546–7. [DOI] [PubMed] [Google Scholar]
- [11].Singh AG, Chhabra JS, Sabnis R, et al. Role of flexible uretero-renoscopy in management of renal calculi in anomalous kidneys: single-center experience. World J Urol 2017;35:319–24. [DOI] [PubMed] [Google Scholar]
- [12].Muruganandham K, Kumar A, Kumar S. Laparoscopic pyeloplasty for ureteropelvic junction obstruction in crossed fused ectopic pelvic kidney. Korean J Urol 2014;55:764–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Kumar S, Singh S, Jain S, et al. Robot-assisted heminephrectomy for chromophobe renal cell carcinoma in L-shaped fused crossed ectopia: Surgical challenge. Korean J Urol 2015;56:729–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Culkin DJ, Wheeler JS, Jr, Karasis M, et al. Treatment of renal calculus in inferior crossed renal ectopia. Urology 1988;32:424–6. [DOI] [PubMed] [Google Scholar]
- [15].Tokgoz H, Sen I, Tan MO, et al. Extracorporeal shock wave lithotripsy in L-shaped kidneys: report of two cases. Int Urol Nephrol 2005;37:685–9. [DOI] [PubMed] [Google Scholar]
- [16].Aminsharifi A, Niroomand R, Kroup M, et al. Laparoscopic nephrolithotomy in a patient with crossed fused renal ectopia. Nature reviews. Urology 2009;6:675–9. [DOI] [PubMed] [Google Scholar]
- [17].Gupta NP, Mishra S, Seth A, et al. Percutaneous nephrolithotomy in abnormal kidneys: single-center experience. Urology 2009;73:710–4. discussion 714-715. [DOI] [PubMed] [Google Scholar]
- [18].Hertz M, Rubinstein ZJ, Shahin N, et al. Crossed renal ectopia: clinical and radiological findings in 22 cases. Clin Radiol 1977;28:339–44. [DOI] [PubMed] [Google Scholar]
- [19].Lee HP. Crossed unfused renal ectopia with tumor. J Urol 1949;61:333–9. [DOI] [PubMed] [Google Scholar]
- [20].Berant M, Jacob ET, Pevzner S. Wilms’ tumor in the crossed ectopic kidney. J Pediatr Surg 1975;10:555–6. [DOI] [PubMed] [Google Scholar]
- [21].Gur U, Yossepowitch O, Baniel J. Transitional cell carcinoma in a fused crossed ectopic kidney. Urology 2003;62:748. [DOI] [PubMed] [Google Scholar]
- [22].Soni HC, Jadav VJ, Sumariya B, et al. Primary malignancy in crossed fused ectopic kidney. Abdom Imaging 2012;37:659–63. [DOI] [PubMed] [Google Scholar]
- [23].Nowroozi MR, Ghorbani H, Amini E, et al. Unusual presentation of renal cell carcinoma in crossed ectopic kidney. Nephrourol Mon 2015;7:e26760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Romero FR, Chan DY, Muntener M, et al. Laparoscopic heminephrectomy for renal cell carcinoma in cross-fused ectopic kidney. Urology 2007;69:779.e711-773. [DOI] [PubMed] [Google Scholar]
- [25].Lee SK, Mwipatayi BP, Abbas M, et al. Transplantation of crossed fused renal ectopia. Asian J Surg 2007;30:82–4. [DOI] [PubMed] [Google Scholar]
- [26].Eichwald M, Wolfe LE. Nephrolithiasis connected with hydronephrosis of a crossed renal ectopia. JAMA 1970;211:117–8. [PubMed] [Google Scholar]
- [27].Shah MH. Solitary crossed renal ectopia. Br J Urol 1975;47:512. [DOI] [PubMed] [Google Scholar]
- [28].Romans DG, Jewett MA, Robson CJ. Crossed renal ectopia with colic. A clinical clue to embryogenesis. Br J Urol 1976;48:171–4. [DOI] [PubMed] [Google Scholar]
- [29].Stubbs AJ, Resnick MI. Struvite staghorn calculi in crossed fused ectopia. J Urol 1977;118:369–71. [DOI] [PubMed] [Google Scholar]
- [30].Siegel YI, Lingeman JE. Percutaneous transilial access for stone removal in crossed fused renal ectopia. Urology 1993;42:82–5. [DOI] [PubMed] [Google Scholar]
- [31].Szentgyorgyi E. Spontaneous rupture of an L-shaped kidney. Int Urol Nephrol 1995;27:521–5. [DOI] [PubMed] [Google Scholar]
- [32].Kato M, Ioritani N, Aizawa M, et al. Extracorporeal shock wave lithotripsy for a ureteral stone in crossed fused renal ectopia. Int J Urol 2000;7:270–3. [DOI] [PubMed] [Google Scholar]
- [33].Nabi G, Kasana I, Khan M. Management of nephrolithiasis in crossed renal ectopia. J Postgrad Med 2001;47:66–7. [PubMed] [Google Scholar]
- [34].Larre S, Carpentier X, Sebe P, et al. A report of unusual crossed fused renal ectopia and minimal invasive management of calculi. Surg Radiol Anat 2007;29:393–5. [DOI] [PubMed] [Google Scholar]
- [35].Ghosh BC, DeSantis M, Kleyner Y, et al. Crossed fused renal ectopia with calculi. J Am Coll Surg 2008;206:753. [DOI] [PubMed] [Google Scholar]
- [36].Rana AM, Bhojwani JP. Percutaneous nephrolithotomy in renal anomalies of fusion, ectopia, rotation, hypoplasia, and pelvicalyceal aberration: uniformity in heterogeneity. J Endourol 2009;23:609–14. [DOI] [PubMed] [Google Scholar]
- [37].Amin MU, Khan S, Nafees M. Crossed fused renal ectopia with staghorn calculus and gross hydronephrosis. J Coll Physicians Surg Pak 2009;19:69–70. [PubMed] [Google Scholar]
- [38].Chung S, Chueh S, Chiang H, et al. L-shaped cross-fused kidney with stone. Urology 2009;73:61–2. [DOI] [PubMed] [Google Scholar]
- [39].Taslim B, Abdulwasiu B, Olusegun S, et al. Crossed renal ectopia coexisting with nephrolithiasis in a young Nigerian man. Arab J Nephrol Transplant 2012;5:107–10. [PubMed] [Google Scholar]
- [40].Agrawal S, Chipde SS, Kalathia J, et al. Renal stone in crossed fused renal ectopia and its laparoscopic management: case report and review of literature. Urol Ann 2016;8:236–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Kodama K, Takase Y AT Management of ureterolithiasis in a patient with crossed unfused renal ectopia. Case Rep Urol 2016;2016:1847213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Al-Hamar NE, Khan K. Crossed nonfused renal ectopia with variant blood vessels: a rare congenital renal anomaly. Radiol Case Rep 2017;12:59–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Patch FS. Carcinoma in a crossed heterolateral ectopic kidney without fusion. Brit J Urol 1937;9:339–59. [Google Scholar]
- [44].Langworthy HT, Drexler LS. Carcinoma in crossed renal ectopia. J Urol 1942;47:776. [Google Scholar]
- [45].Castro JE, Ashken MH. Crossed renal ectopia without fusion associated with carcinoma of the renal pelvis. Br J Surg 1972;59:235–7. [DOI] [PubMed] [Google Scholar]
- [46].Redman JF, Berry DL. Wilms’ tumor in crossed fused renal ectopia. J Pediatr Surg 1977;12:601–3. [DOI] [PubMed] [Google Scholar]
- [47].Urnes T, Muri O., Jr Crossed, non-fused renal ectopia and ipsilateral ureteral carcinoma. A case report. Scand J Urol Nephrol 1979;13:213–5. [DOI] [PubMed] [Google Scholar]
- [48].Gerber WL, Culp DA, Brown RC, et al. Renal mass in crossed-fused ectopia. J Urol 1980;123:239–44. [DOI] [PubMed] [Google Scholar]
- [49].Williams GB. Mesoblastic nephroma in crossed renal ectopia. J Urol 1982;128:801–2. [DOI] [PubMed] [Google Scholar]
- [50].Liu S, Leung H, Considine J. Urothelial tumour of renal pelvis in patient with crossed ectopia. Br J Urol 1992;69:215–6. [DOI] [PubMed] [Google Scholar]
- [51].Miller DC, Kropp KA. Transitional cell carcinoma associated with crossed renal ectopia and previous cyclophosphamide therapy. J Urol 1992;148:1244–6. [DOI] [PubMed] [Google Scholar]
- [52].Tsunoe H, Yasumasu T, Tanaka M, et al. Resection of an L-shaped kidney with renal cell carcinoma using a microwave tissue coagulator. Int J Urol 2001;8:459–62. [DOI] [PubMed] [Google Scholar]
- [53].Stimac G, Dimanovski J, Ruzic B, et al. Tumors in kidney fusion anomalies--report of five cases and review of the literature. Scand J Urol Nephrol 2004;38:485–9. [DOI] [PubMed] [Google Scholar]
- [54].Siegel HJ, Casillas MA., Jr Crossed fused renal ectopia with metastatic renal cell carcinoma. Clin Nucl Med 2004;29:765–6. [DOI] [PubMed] [Google Scholar]
- [55].Shah SS, Ahmed K, Smith R, et al. Chylous ascites following radical nephrectomy: a case report. J Med Case Rep 2008;2:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [56].Davis CM, Rao MV, Flanigan RC, et al. Renal cell carcinoma in two patients with crossed fused ectopic kidneys. Urol Int 2008;81:370–2. [DOI] [PubMed] [Google Scholar]
- [57].Kageyama S, Tsuru T, Okamoto K, et al. Primary synovial sarcoma arising from a crossed ectopic kidney with fusion. Int J Urol 2010;17:96–8. [DOI] [PubMed] [Google Scholar]
- [58].Rouanne M, Legrand G, Renard-Penna R, et al. Management of renal cell carcinoma in sigmoid kidney. Urol Int 2012;88:483–5. [DOI] [PubMed] [Google Scholar]
- [59].Dhillon J, Mohanty SK, Kim T, et al. Spectrum of renal pathology in adult patients with congenital renal anomalies-a series from a tertiary cancer center. Ann Diagn Pathol 2014;18:14–7. [DOI] [PubMed] [Google Scholar]
- [60].Rac G, Ellet JD, Sarkissian H, et al. Open partial nephrectomy for Wilms’ tumor in a cross-fused pelvic ectopic kidney. Urology 2016;93:188–90. [DOI] [PubMed] [Google Scholar]