

Abstract
Objective The aim of this study was to assess changes in micro-hardness level of enamel after it was exposed to thymoquinone (TQ).
Materials and Methods Sixteen enamel blocks were prepared and divided into two groups (each group received eight blocks, n = 8); Gp 1 (control): enamel blocks kept in 100 mL artificial saliva (AS) for 24 hours and Gp 2: enamel blocks kept in a mixture of TQ powder (1 g) and AS (100 mL) for 24 hours. Post-immersion they were subjected to simulated brushing with each sample receiving 8,000 linear strokes. For brushing, 3 mL of AS and TQ oil was used for groups 1 and 2, respectively. Enamel surfaces were analyzed for changes in values of surface micro-hardness (pre-immersion, post-immersion, and post-brushing) by obtaining Vickers hardness number (VHN).
Results The present study indicated improvement in micro-hardness levels for both groups although experimental group showed more enhancement. The mean baseline VHN for control group was 498.6, 500.4 for post-immersion, and 503.5 for post-brushing. The mean baseline VHN for experimental group was 448.7, 531 for post-immersion, and 610.3 for post-brushing. Statistically significant differences ( p < 0.05) were observed when post-brushing VHN values of both groups were compared and also within the experimental group when post-brushing values were compared with baseline values.
Statistical Analysis Wilcoxon signed-rank test was applied for the evaluation of pre- and post-exposure hardness values. Level of significance was ≤0.05.
Conclusion The exposure of enamel to TQ led to an improvement in its micro-hardness levels. Further studies are required to understand the mechanism of action of TQ on human tissues.
Keywords: enamel, micro-hardness, Nigella sativa, thymoquinone
Introduction
Human oral mouth is a host to around 700 bacterial species 1 living in equilibrium. A disease only occurs when there is a disturbance in this equilibrium and the balance shifts toward pathogenic species. 2 Human tooth is made up of three hard tissues (enamel, dentin, and cementum). Enamel that covers the anatomical crown of the tooth and is hardest among these tissues. It covers only the dentin in the crown, and dentin in the root is covered by a thin layer of calcified cementum. Enamel is a highly mineralized hard tissue that is 4 wt% organic and 96 wt% inorganic in composition. The presence of high inorganic content makes it the hardest tissue in the human body. Enamel once lost cannot be regenerated or biologically repaired. 3 Dental caries initiates from the surface of the enamel as it is clinically exposed to oral environment, 4 and the microbes and oral plaque play an important role in its etiology. 5
Dental caries is one of the most prevalent diseases and is caused by destruction of tooth structure by acids produced from cariogenic bacteria after they ferment dietary carbohydrates. 6 Streptococcus mutans are gram positive bacteria that are usually found in biofilms attached to surfaces of the teeth. 7 Streptococcus mutans is considered the major cariogenic species because of its ability to produce large amounts of acids, thus surpassing noncariogenic organisms and causing demineralization of hard tissues of teeth. 8 9 When the demineralization continues, it causes cavitation that provides cariogenic bacteria with a protected space in which dental caries can grow progressively. 10
Nigella sativa is a medicinal plant also commonly called black seed, black cumin, and/or Habbatul Barakah. 11 It is used extensively by millions of Muslims around the world and has a religious significance attached to its use 12 Historically, Nigella sativa seeds have been used for the treatment of body aches, nose congestion, and intestinal worms. 13 These seeds are considered to be an active source of providing ions like calcium, 14 which could be useful in remineralization of tooth structure.
One of the active components of Nigella sativa is thymoquinone (TQ) that has been reported to be anticarcinogenic, 15 anti-inflammatory, analgesic, and antimicrobial. 16 TQ has also shown promising results in a previous animal study where Shaker and Al-Wafi evaluated TQ for the prevention of gingival inflammation in a rat model. 17 It was concluded that gingival inflammation and periodontal indices were significantly lower in rats treated with TQ as compared with the control groups. The role of TQ in healing oral ulcers is also present in the literature. 18 Al-Thobity et al demonstrated in a previous study that the addition of TQ in acrylic denture base could be useful in preventing adhesion of Candida albicans to it, thus resulting in prevention of denture stomatitis. 19
There is a deficit of literature dealing with the effects of TQ on the hardness of dental enamel. Therefore, the aim of the present study was to evaluate changes in the micro-hardness of enamel after it is exposed to TQ (by simple immersion and by simulated tooth brushing).
Materials and Methods
Ethical approval was obtained from the Scientific Research Unit of the institute (Ref: EA 2018001) and all the ethical protocols were strictly followed. Dry powder extract of TQ (Sigma-Aldrich) and TQ oil was obtained and used in the experiments.
Artificial Saliva Preparation
Artificial saliva (AS) was prepared by mixing NaCl: 0.400 g, KCl: 0.400 g, NaH 2 PO4. H 2 O: 0.69 g; CaCl 2 . H 2 O: 0.795 g; Na 2 S. 9H 2 O: 0.005 g in 1000 mL of deionized water, as suggested by Fusayama et al. 20 The pH of freshly prepared AS was 5.5 that was adjusted to a neutral pH of 7.0 by adding aliquots of 1 M of NaOH as proposed by Farooq et al. 21
Preparation of Enamel Blocks and Grouping of Specimens
Sixteen extracted teeth ( n = 16) were obtained from oral and maxillofacial surgery clinics of the institute. Teeth that were free from caries, restorations, or any other obvious defects were selected. Enamel blocks were prepared by cutting these teeth mesiodistally over cementoenamel junction with a water-cooled diamond saw (Isomet 5000 Linear Precision Saw; Buehler Ltd, Illinois, United States) at a blade speed of 3,000 rpm and a feed rate of 10 mm/min. The root portion was discarded and the crown was then embedded in an acrylic block in such a manner that the buccal surface was exposed. Before the experiments, enamel surfaces were serially polished with a water-cooled carbide paper of up to 1200 grit fineness (3M; St. Paul, Minnesota, United States). These sixteen enamel blocks were then randomly divided into two groups (each group received eight blocks, n = 8); Gp 1 (control): enamel blocks kept in AS for 24 hours and Gp 2: enamel blocks kept in a mixture of TQ (1 g) and AS (100 mL) for 24 hours.
The mixture of AS and TQ was prepared first by weighing it using a motorized analytical balance scale (Sgm Laboratory Solutions, India) and then mixing it using a magnetic stirrer (Hot Plate stirrer LabTech, Italy).
Surface Micro-Hardness Analysis
The enamel blocks were analyzed for changes in the values of surface micro-hardness and the data were collected pre- and post-immersion in AS for Gp 1. For Gp 2 containing a mixture of AS + TQ the data were again collected before and after immersion in the mixture. The Vickers hardness number (VHN) values were measured using a digital micro-hardness tester (FM-ARS 9000; Future-Tech Corp, Kawasaki, Japan). In each sample, an area was marked with a nail varnish and three indents were made inside that marked area using a Vickers diamond indenter under a 100-g load applied for 10 seconds.
Simulated Tooth Brushing with Thymoquinone
Post-immersion, enamel blocks belonging to groups 1 and 2 were subjected to simulated brushing that was performed inside a toothbrush simulation machine (Toothbrush simulator; model ZM-3.8, Germany), under a load of 250 g for 2,000 linear strokes per day for 4 days (each sample received 8,000 strokes that is equivalent to 5 months of in vivo brushing). 6 For brushing of group 1 specimens, 3 mL of AS and for group 2, 3 mL of TQ oil were used. After every brushing cycle, all the specimens were washed with distilled water thoroughly. After fourth day of brushing, specimens were washed with distilled water and were left to air dry prior to surface micro-hardness analysis again.
Statistical Analysis
Data analysis was performed by using SPSS-20.0 (IBM product; Chicago, Illinois, United States). Wilcoxon signed-rank test was applied to evaluate significance of mean within the control and experimental groups comparing baseline values versus post-immersion and post-brushing values. A p -value ≤0.05 was considered statistically significant difference of means.
Results
The micro-hardness level of enamel surfaces was assessed by Vickers indentation ( Fig. 1 ). The results of the present study indicated improvement in micro-hardness levels for both groups. For the control group in which enamel blocks were only exposed to AS, the improvement was less than the experimental group in which enamel blocks were exposed to a mixture of AS + TQ ( Fig. 2 ). The mean baseline VHN for the control group was 498.6 that improved to 500.4 post-immersion, and 503.5 post-brushing. The mean baseline VHN for the experimental group was 448.7 that improved to 531 post-immersion, 610.3 post-brushing ( Table 1 ). Statistically significant differences ( p < 0.05) were perceived when post-brushing VHN values of both groups were compared and were also observed within the experimental group when post-brushing values were compared with baseline values.
Fig. 1.
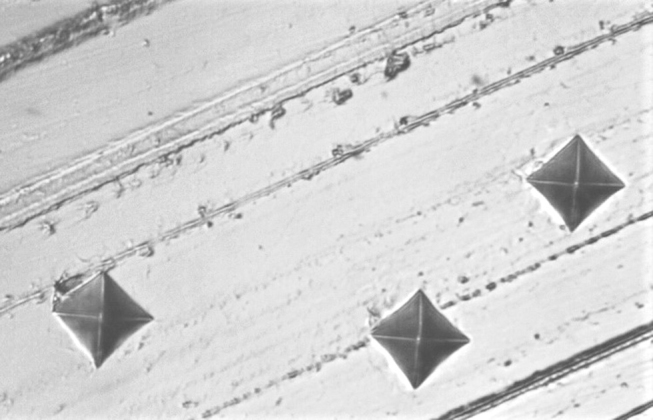
Image showing indentations performed on enamel surfaces to obtain Vickers hardness number values.
Fig. 2.
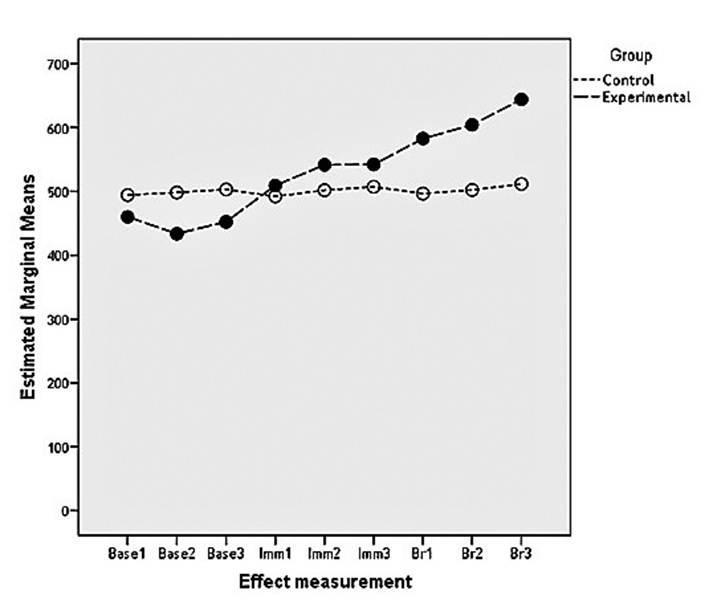
Image showing a comparison of Vickers hardness number values between the two groups at baseline, post-immersion, and post-brushing.
Table 1. Mean VHN for both groups measured at baseline, post-immersion, and post-brushing.
| Groups | Control group (mean ± SD) | Experimental group (mean ± SD) | p -Value |
|---|---|---|---|
| Abbreviations: AS, artificial saliva; SD, standard deviation; TQ, thymoquinone; VHN, Vickers hardness number. Note: Baseline: Mean VHN of eight enamel blocks after three indentations in each sample for both the groups, Post-immersion: Mean VHN of eight enamel blocks after three indentations each sample in both the groups post-24 hour exposure to AS and TQ for group 1 and 2 respectively, Post-brushing: Mean VHN of eight enamel blocks after three indentations in each sample for both the groups post simulated brushing with AS and TQ for groups 1 and 2 respectively. Wilcoxon sign-rank test. a Significant mean difference between control and experimental groups. b Significant mean difference within the group baseline versus post brushing. | |||
| Baseline | 498.63 ± 83.85 | 448.73 ± 103.39 | 0.307 |
| Post-immersion | 500.46 ± 85.89 | 531.02 ± 104.86 | 0.534 |
| Post-brushing | 503.50 ± 85.65 | 610.36 ± 68.67 a,b | 0.016 |
Discussion
The results of our study show improved hardness level of enamel blocks when they were exposed to TQ (post-immersion and post-brushing), whereas, in the control group containing AS, there was only a slight improvement in the hardness level. Dental enamel is a mineralized tooth tissue that is mostly inorganic (96 wt%) and forms the outer protective covering of teeth. 22 The enamel is exposed to various acidic and masticatory challenges throughout its existence; therefore, it is important to analyze hardness levels of enamel and how they are affected by various elements. 23 24
Human saliva could act as a medium and also as a chief source of transporting essential ions like calcium and phosphate to the tooth structure. 25 However, the role played only by saliva in hardening of dental enamel is debatable. Enamel is open to an active oral environment and it has the ability to adsorb minerals from its environment by mechanism of simple diffusion. 26 Alencar et al performed an in situ study to understand hardening of acid-softened enamel by saliva at different time intervals and concluded that it takes at least 2 hours to achieve partial hardening of enamel only. 27 In another similar in vitro study, Wang et al reported that application of AS for several hours could only lead to limited recovery of apatite enamel structure. 28 Our study revealed similar results where enamel hardness was only slightly increased after exposure to AS, although in our study enamel blocks were not demineralized before being exposed to AS and to the mixture of AS + TQ.
It is noteworthy to mention that even after stirring the mixture for 2 hours in our study, TQ was only partially dissolved in AS. This could be attributed to the physicochemical nature of TQ that is identical to hydrophobic materials that may well lead to its poor bioavailability. 29 Nevertheless, the mixture of AS + TQ showed significantly higher micro-hardness levels of enamel surface post-immersion. TQ is chemically 2-methyl-5-isopropyl-1, 4-benzoquinone. 30 It is the main bioactive component of Nigella sativa and TQ could be accountable for its main biological actions. 31 Many researchers also believe that all benefits of Nigella sativa are actually due to the presence of TQ in its composition. 32 33 34 35 36 37
Post-brushing, micro-hardness values of the experimental group were significantly increased. It could not be said with authority what led to an increase in micro-hardness level of enamel surfaces in our study but the only variable changed between the groups was brushing enamel blocks with TQ oil in the experimental group. This could have possibly improved the hardness of enamel surfaces in that group.
One limitation of our study is its in vitro nature as actual in vivo conditions but to overcome this, every attempt was made to standardize all the variables (teeth number of both groups, exposure time, quantity of exposed solution). Another limitation of our study was that it is almost impossible to take baseline, post-immersion, and post-brushing hardness values from exactly the same area of enamel’s surface. To minimize the variation, the area from that we aimed to take hardness values was marked first and then micro-hardness was analyzed in only that particular area. The same area was brushed during simulated brushing with AS and TQ for our control and experimental groups. In the future, comparison of TQ with a fluoride containing toothpaste could prove useful to determine efficacy of both products in remineralizing enamel.
To the best of the author’s knowledge, this is the first in vitro study that has tested TQ’s effect on the micro-hardness level of dental enamel. The positive results of our study could lead to future in vivo studies to understand TQ’s effect in a more vigorous dynamic oral environment.
Conclusion
Exposure to TQ led to an increased micro-hardness of enamel surfaces as compared with the enamel blocks exposed to AS only. Future clinical studies are indicated to test TQ under intense in vivo oral conditions.
Acknowledgments
The authors are grateful to Vice Deanship of Post-Graduate Studies and Research at the College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia for facilitating us with the micro-hardness analysis.
Footnotes
Authors’ ContributionConflict of Interest All authors have made substantive contribution to this study and/or manuscript, and all have reviewed the final paper prior to its submission.
None declared.
References
- 1.Dewhirst F E, Chen T, Izard J. The human oral microbiome. J Bacteriol. 2010;192(19):5002–5017. doi: 10.1128/JB.00542-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kuboniwa M, Tribble G D, Hendrickson E L, Amano A, Lamont R J, Hackett M. Insights into the virulence of oral biofilms: discoveries from proteomics. Expert Rev Proteomics. 2012;9(03):311–323. doi: 10.1586/epr.12.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zafar M S, Ahmed N. Nano-mechanical evaluation of dental hard tissues using indentation technique. World Appl Sci J. 2013;28(10):1393–1399. [Google Scholar]
- 4.Zafar M S, Ahmed N. The effects of acid etching time on surface mechanical properties of dental hard tissues. Dent Mater J. 2015;34(03):315–320. doi: 10.4012/dmj.2014-083. [DOI] [PubMed] [Google Scholar]
- 5.Alfaroukh R, ElEmbaby A, Almas K. Oral biofilm formation and retention on commonly used dental materials: an update. Odontostomatol Trop. 2018;41(164):28–34. [Google Scholar]
- 6.Alhussain A M, Alhaddad A A, Ghazwi M M, Farooq I. Remineralization of artificial carious lesions using a novel fluoride incorporated bioactive glass dentifrice. Dent Med Probl. 2018;55(04):379–382. doi: 10.17219/dmp/97311. [DOI] [PubMed] [Google Scholar]
- 7.Zero D TFM, Fontana M, Martínez-Mier E A. The biology, prevention, diagnosis and treatment of dental caries: scientific advances in the United States. J Am Dent Assoc. 2009;140 01:25S–34S. doi: 10.14219/jada.archive.2009.0355. [DOI] [PubMed] [Google Scholar]
- 8.Lemos J A, Quivey R G, Jr., Koo H, Abranches J.Streptococcus mutans: a new gram-positive paradigm? Microbiology 2013159(Pt 3)436–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Raja M, Hannan A, Ali K. Association of oral candidal carriage with dental caries in children. Caries Res. 2010;44(03):272–276. doi: 10.1159/000314675. [DOI] [PubMed] [Google Scholar]
- 10.Rouabhia M, Chmielewski W. Diseases associated with oral polymicrobial biofilms. Open Mycol J. 2012;6:27–32. [Google Scholar]
- 11.Al-Attass S A, Zahran F M, Turkistany S A. Nigella sativa and its active constituent thymoquinone in oral health. Saudi Med J. 2016;37(03):235–244. doi: 10.15537/smj.2016.3.13006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rahmani A H, Aly S M. Nigella Sativa and its active constituents thymoquinone shows pivotal role in the diseases prevention and treatment. Asian J Pharm Clin Res. 2015;8(01):48–53. [Google Scholar]
- 13.Gaur S, Shrivastava B, Gaur S, Bhardwaj R, Khanchandani R. Medicinal and therapeutical potential of Nigella sativa. Int J Med App Sci Res. 2014;1:32–39. [Google Scholar]
- 14.Ahmad A, Husain A, Mujeeb M. A review on therapeutic potential of Nigella sativa: a miracle herb. Asian Pac J Trop Biomed. 2013;3(05):337–352. doi: 10.1016/S2221-1691(13)60075-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Padhye S, Banerjee S, Ahmad A, Mohammad R, Sarkar F H. From here to eternity - the secret of Pharaohs: therapeutic potential of black cumin seeds and beyond. Cancer Ther. 2008;6b:495–510. [PMC free article] [PubMed] [Google Scholar]
- 16.Ahmad I, Tripathi J, Sharma M, Karchulli M S, Umer L. Nigella sativa - a medicinal herb with immense therapeutic potential (a systematic review) Int J Bio Pharm Res. 2014;5:755–762. [Google Scholar]
- 17.Shaker A, Al-Wafi H.Benefits of thymoquinone, a Nigella Sativa extract in preventing dental caries initiation and improving gingival health ProQuest 2014. LLC72 [Google Scholar]
- 18.Al-Douri A, Al-Kazaz S. The effect of Nigella Sativa oil (black seed) on the healing of chemically induced oral ulcer in rabbit (experimental study) Al-Rafidain Dent J. 2010;10:151–157. [Google Scholar]
- 19.Al-Thobity A M, Al-Khalifa K S, Gad M M, Al-Hariri M, Ali A A, Alnassar T. In vitro evaluation of the inhibitory activity of thymoquinone in combatting Candida albicans in denture stomatitis prevention. Int J Environ Res Public Health. 2017;14(07):743. doi: 10.3390/ijerph14070743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fusayama T, Katayori T, Nomoto S. Corrosion of gold and amalgam placed in contact with each other. J Dent Res. 1963;42:1183–1197. doi: 10.1177/00220345630420051301. [DOI] [PubMed] [Google Scholar]
- 21.Farooq I, Moheet I A, AlShwaimi E. In vitro dentin tubule occlusion and remineralization competence of various toothpastes. Arch Oral Biol. 2015;60(09):1246–1253. doi: 10.1016/j.archoralbio.2015.05.012. [DOI] [PubMed] [Google Scholar]
- 22.Zafar M S. A comparison of dental restorative materials and mineralized dental tissues for surface nanomechanical properties. Life Sci J. 2014;1110s:19–24. [Google Scholar]
- 23.Gutiérrez-Salazar M, Reyes-Gasga J. Microhardness and chemical composition of human tooth. Mater Res. 2003;6(03):367–373. [Google Scholar]
- 24.Hassan U, Farooq I, Moheet I A, AlShwaimi E. Cutting efficiency of different dental materials utilized in an air abrasion system. Int J Health Sci (Qassim) 2017;11(04):23–27. [PMC free article] [PubMed] [Google Scholar]
- 25.Shaikh K, Pereira R, Gillam D G, Phad S. Comparative evaluation of desensitizing dentifrices containing BioMin®, Novamin® and fluoride on dentinal tubule occlusion before and after a citric acid challenge– a scanning electron microscope in-vitro Study. J Odontol. 2018;2(01):105. [Google Scholar]
- 26.Zafar M S, Ahmed N. Nanomechanical characterization of exfoliated and retained deciduous incisors. Technol Health Care. 2014;22(06):785–793. doi: 10.3233/THC-140852. [DOI] [PubMed] [Google Scholar]
- 27.Alencar C R, Mendonça F L, Guerrini L B. Effect of different salivary exposure times on the rehardening of acid-softened enamel. Braz Oral Res. 2016;30(01):e104. doi: 10.1590/1807-3107BOR-2016.vol30.0104. [DOI] [PubMed] [Google Scholar]
- 28.Wang X, Mihailova B, Klocke A, Heidrich S, Bismayer U.Effect of artificial saliva on the apatite structure of eroded enamel Int J Spectrosc 2011 2011. Available at:http://www.hindawi.com/journals/ijs/2011/236496/.doi:10.1155/2011/236496
- 29.Lebwohl M, Ali S. Treatment of psoriasis. Part 2. Systemic therapies. J Am Acad Dermatol. 2001;45(05):649–661, quiz 662–664. doi: 10.1067/mjd.2001.117047. [DOI] [PubMed] [Google Scholar]
- 30.Kishwar F, Mahmood T, Mahmood I, Anwar A, Parween R, Mustafa S. Complexation of active ingredient thymoquinone of nigella sativa (black seed) with chromium(vi) Fuuast J BIOL. 2016;6(01):65–72. [Google Scholar]
- 31.Ermumcu M SK, Sanher N. Black cumin (Nigella sativa) and its active component of thymoquinone: effects on health. J Food Health Sci. 2017;3(04):170–183. [Google Scholar]
- 32.Mehta B K, Pandit V, Gupta M. New principles from seeds of Nigella sativa. Natural product research. Part A. 2009;23:138–148. doi: 10.1080/14786410801892078. [DOI] [PubMed] [Google Scholar]
- 33.Akram Khan M, Afzal M. Chemical composition of Nigella sativa Linn: Part 2 recent advances. Inflammopharmacology. 2016;24(02)(03):67–79. doi: 10.1007/s10787-016-0262-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Khazdair M R. The protective effects of Nigella sativa and its constituents on induced neurotoxicity. J Toxicol. 2015;2015:841823. doi: 10.1155/2015/841823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Beheshti F, Khazaei M, Hosseini M. Neuropharmacological effects of Nigella sativa. Avicenna J Phytomed. 2016;6(01):104–116. [PMC free article] [PubMed] [Google Scholar]
- 36.Darakhshan S, Bidmeshki Pour A, Hosseinzadeh Colagar A, Sisakhtnezhad S. Thymoquinone and its therapeutic potentials. Pharmacol Res. 2015;95-96:138–158. doi: 10.1016/j.phrs.2015.03.011. [DOI] [PubMed] [Google Scholar]
- 37.El-Dakhakhny M, Madi N J, Lembert N, Ammon H P. Nigella sativa oil, nigellone and derived thymoquinone inhibit synthesis of 5-lipoxygenase products in polymorphonuclear leukocytes from rats. J Ethnopharmacol. 2002;81(02):161–164. doi: 10.1016/s0378-8741(02)00051-x. [DOI] [PubMed] [Google Scholar]