

Endoscopic submucosal dissection (ESD) of sizable early gastric cancers located in the upper third of the stomach is exceedingly demanding technically.1, 2 This case report demonstrates a challenging gastric ESD that was efficiently executed by the effective use of tissue traction (Video 1, available online at www.VideoGIE.org).
A 62-year-old woman underwent screening EGD, and an 80-mm elevated, laterally spreading lesion suggestive of cancer was found involving the greater curvature of the upper gastric body. Examination of a biopsy specimen showed a well-differentiated tubular adenocarcinoma. A CT scan was negative for nodal and distant metastasis. After discussing the various treatment options, the patient opted for endoscopic resection.
It was difficult to see the entire lesion because of puddle formation when the patient was in the left lateral position (Fig. 1). Changing her position from left to right lateral allowed much better visualization of the lesion by shifting the puddle to the cardia with the assistance of gravity (Fig. 2). There was no limitation on endoscope manipulation in the right lateral position. After completing circumferential mucosal incision, we added 3 clip-line tractions to the distal side of the lesion to expose the submucosa, making dissecting much more efficient in retroflexion (Figure 3, Figure 4, Figure 5, Figure 6). Both the patient’s position and multiple clip-line traction allowed satisfactory tissue traction to be maintained until the end of the procedure. En bloc resection was achieved in 160 minutes (Fig. 7). Complete defect closure was accomplished with 3 endoloops and multiple endoclips (Fig. 8). The resected specimen measured 118-mm × 99-mm and revealed well-differentiated tubular adenocarcinoma, with the deepest invasion confined to the mucosa. There was no evidence of ulceration, and the margins were negative, with the cancer measuring up to 86 mm × 70 mm (Fig. 9). Second-look endoscopy confirmed sustained complete closure.
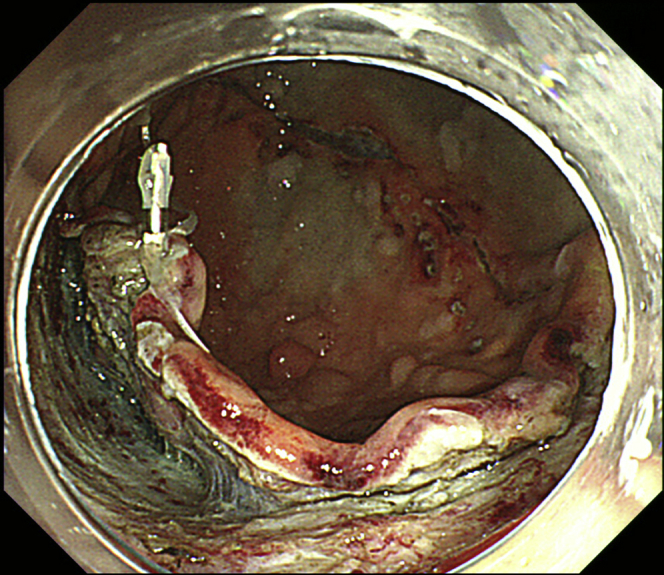
Figure 1.

Identification of a large elevated lesion in the greater curvature of the upper gastric body, although visualization of the entire lesion is difficult because of puddle formation with the patient in the left lateral position.
Figure 2.

A change in patient’s position from left to right lateral allows much better visualization of the lesion by shifting the puddle to the cardia using gravity. Marking around the lesion has been performed.
Figure 3.

Endoscopic submucosal dissection strategy before multiple clip line traction. 1, Mucosal incision of the distal side with dual knife. 2, Submucosal dissection of the distal side with dual knife (KD-650U; Olympus Medical Systems Corp, Tokyo, Japan). 3, Circumferential mucosal incision completed with IT 2 knife (KD-612U; Olympus Medical Systems Corp. Tokyo, Japan).
Figure 4.

Completion of circumferential mucosal incision.
Figure 5.
Addition of clip-line traction to the left side of the lesion to expose the submucosa, making dissecting much more efficient.
Figure 6.

Patient’s position and multiple clip-line traction allow satisfactory tissue traction to be maintained until the end of the procedure.
Figure 7.

Achievement of en bloc resection.
Figure 8.

Closure of the large mucosal defect with 3 endoloops and endoclips, and complete closure of the defect.
Figure 9.

Resected specimen (118 mm × 99 mm), revealing well-differentiated tubular adenocarcinoma, with deepest invasion confined to the mucosa, no evidence of ulceration, and negative margins, with the cancer measuring up to 86 mm × 70 mm.
Altering the patient’s position allowed better visualization of the submucosal plane of the lesion, which was in a tremendously challenging location. Multiple clip-line traction maintained sufficient traction, even for the sizable lesion in the greater curvature of the upper stomach.3 It would have been difficult to manage post-ESD bleeding from the mucosal defect endoscopically if it had occurred. Therefore, prophylactic closure was performed.4 This patient was able to avoid invasive gastrectomy because of this technique.
Disclosure
All authors disclosed no financial relationships relevant to this publication.
Acknowledgements
The authors thank Dr Satoru Nonaka and Shih Yea Sylvia Wu (Endoscopy Division, National Cancer Center Hospital) for their kind support of this article. The development of this advanced endoscopy was supported by the National Cancer Center Research and Development Fund (29-A-13).
Footnotes
If you would like to chat with an author of this article, you may contact Dr Abe at seabe@ncc.go.jp.
Supplementary data
Endoscopic submucosal dissection of a sizable cancer through alteration of patient’s position and multiple clip-line traction.
References
- 1.Chung I.K., Lee J.H., Lee S.H. Therapeutic outcomes in 1000 cases of endoscopic submucosal dissection for early gastric neoplasms: Korean ESD Study Group multicenter study. Gastrointest Endosc. 2009;69:1228–1235. doi: 10.1016/j.gie.2008.09.027. [DOI] [PubMed] [Google Scholar]
- 2.Imagawa A., Okada H., Kawahara Y. Endoscopic submucosal dissection for early gastric cancer: results and degrees of technical difficulty as well as success. Endoscopy. 2006;38:987–990. doi: 10.1055/s-2006-944716. [DOI] [PubMed] [Google Scholar]
- 3.Yoshida M., Takizawa K., Suzuki S. Conventional versus traction-assisted endoscopic submucosal dissection for gastric neoplasms: a multicenter, randomized controlled trial (with video) Gastrointest Endosc. 2018;87:1231–1240. doi: 10.1016/j.gie.2017.11.031. [DOI] [PubMed] [Google Scholar]
- 4.Abe S., Oda I., Mori G. Complete endoscopic closure of a large gastric defect with endoloop and endoclips after complex endoscopic submucosal dissection. Endoscopy. 2015;47:E374–E375. doi: 10.1055/s-0034-1392594. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Endoscopic submucosal dissection of a sizable cancer through alteration of patient’s position and multiple clip-line traction.