

Abstract
Objective:
Low educational attainment is a risk factor for more rapid cognitive aging, but there is substantial variability in cognitive trajectories within educational groups. The aim of this study was to determine the factors that confer resilience to memory decline within educational strata.
Method:
We selected 2,573 initially non-demented White, African American, and Hispanic participants from the longitudinal community-based Washington Heights/Inwood Columbia Aging Project who had at least two visits. We estimated initial memory (intercept) and the rate of memory decline (slope) using up to five occasions of measurement. We classified groups according to educational attainment groups as Low (≤5 years), Medium (6–11 years) and High (≥12 years). We used a multiple-group Latent Growth Model (LGM) to identify the baseline predictors of initial memory performance and rate of memory decline across groups. The model specification considered the influence of demographic, socioeconomic, biomedical, and cognitive variables on the intercept and the slope of memory trajectory.
Results:
Our results indicated that the three educational groups do not benefit from the same factors. When allowed to differ across groups, the predictors were related to cognitive outcomes in the highly educated group, but we found no unique predictor of cognition for the low educated older adults.
Conclusions:
These findings highlight that memory-protective factors may differ across older adults with distinct educational backgrounds, and the need to evaluate a broader range of potential resilience factors for older adults with few years of school.
Keywords: cognitive aging, episodic memory, resilience factors, educational attainment, statistical modeling, longitudinal study
Introduction
Most research on factors that maintain cognition in aging comes from cohorts with relatively high educational attainment. For populations with low educational attainment, the literature has not widely examined factors that promote cognitive resilience in the face of age and dementia risk. In this study, our goal was to identify cognitive resilience factors among people with very few years of school.
Previous literature has established educational attainment, defined as years of formal education and credential, as a major protective factor for cognitive decline, risk of developing dementia and clinical expression of dementia in the face of neurodegeneration (Albert et al., 1995; Amieva et al., 2014; Meng & D’Arcy, 2012; Prince et al., 2013; Stern, 2009). However, its impact on episodic memory is not always clear. While education influences baseline episodic memory performance, its effect on memory trajectories is inconsistent (Zahodne et al., 2011).
Beyond education, studies show other demographic factors such as sex/gender, race/ethnicity, and occupation, as well as biological factors such as cardiovascular health and genetic risk factors impact memory performance and, potentially, decline among older adults. A recent study shows that older women have lower rates of episodic memory decline compared with older men, in a highly educated sample (Lundervold et al., 2014). Whites tend to obtain higher baseline episodic memory scores compared to African Americans and Hispanics even after controlling for age, gender and self-reported years of education (Early et al., 2013; Wilson et al., 2015). Using longitudinal data, some studies report no racial differences in rate of episodic memory decline (Wilson et al., 2015) while others suggest faster rates of cognitive decline among the African Americans when compared with Whites in face of educational disparities across race in the U.S. (Early et al., 2013; Sachs-Ericsson & Blazer, 2005). Some investigators suggest that socioeconomic factors, such as family income and poverty status, account for racial differences in memory decline (Sachs-Ericsson & Blazer, 2005; Sisco et al., 2013). Having a cognitively demanding occupation is related to better cognitive performance in highly educated subjects (Foubert-Samier et al., 2012) even in the face of neurodegeneration (Stern, 2012). Lower family income and financial inadequacy are associated with increased dementia risk, and may act mechanistically through reduced access to educational, financial, and health resources, amplifying physiological stress that can lead to multisystem biological dysregulation (Yaffe et al., 2013).
In terms of biological factors, hypertension is associated with cognitive impairment in older adults even in the absence of dementia or stroke history (Knopman et al., 2001). Hypertension confers higher risk for developing Alzheimer’s disease (Bermejo-Pareja et al., 2010), potentially by affecting the brain’s vascular integrity. Furthermore, hypertension is more strongly correlated with poor episodic memory performance compared to the other cognitive domains such as attention and language, even when controlling for education (Gifford et al., 2013). APOE-ε4 is the best-known and most robust genetic risk factor for Alzheimer’s disease, but it has been a weak predictor for African Americans and Hispanics, and its association with older adults’ cognitive performance in cross-sectional data has been inconsistent (Foster et al., 2013). There is longitudinal evidence that relates the presence of the ε4 allele to a faster episodic memory decline, even in non-demented older adults (Albrecht et al., 2015). The available literature on risk and protective factors in older adults with low education is limited as most of these studies were based on highly educated samples and little is known about how these factors function in older adults with lower education.
As the brain ages, it is possible that non-memory cognitive abilities help to compensate for memory decline, particularly among people with few years of school who lack other potential sources of resilience such as high level occupational status or income. In recent studies, executive function and verbal knowledge were the domains most related to memory functioning (Bouazzaoui et al., 2013; Hertzog et al., 2003; Rast, 2011). Better cognitive performance on verbal knowledge may be related to superior learning of verbal information, while better executive function may facilitate efficient retrieval of the stored material (Bouazzaoui et al., 2013; Hertzog et al., 2003; Rast, 2011). There is a lack of literature examining cognitive resilience and its possible mechanisms such as non-memory cognitive compensation in older adults with low levels of education (<5 years of schooling). Research among individuals with low literacy shows that they are more likely to recruit parietal areas during cognitive tasks than those with high literacy (Julayanont & Ruthirago, 2016; Petersson et al., 2007). (Petersson, Reis & Ingvar, 2001). In response to cognitive aging, individuals with low levels of education may recruit and rely on cognitive domains in different ways than individuals with more formal schooling.
The majority of research on protective factors in memory decline comes from samples with at least 12 or more years of education, and most cohorts have an average of 15 years of school or higher. The main aim of this study is to examine whether risk and resilience factors for memory decline differ across educational groups when participants with less than a high school education are included. We hypothesized that older adults with low education would be more likely to recruit language and executive skills as compensatory resources than better educated participants. Therefore, we expected that despite having lower baseline language and executive function scores, these skills would be stronger predictors of memory trajectory in lower educated older adults than among higher educated adults.
Method
Participants
We included data from 2573 ethnically diverse and initially non-demented participants from the prospective, community-based Washington/Hamilton Heights Inwood Columbia Aging Project (WHICAP) in Northern Manhattan, New York City. At each visit, participants underwent a medical interview and comprehensive neuropsychological evaluation, performed in English or Spanish. After each WHICAP visit, a consensus group of neuropsychologists and neurologists utilize DSM-III criteria to determine dementia diagnosis. WHICAP recruitment initially occurred in two waves (1992 and 1999), and follow-up visits occur every 18–24 months. We included participants that had at least two and up to five assessments. The Institutional Review Board at Columbia University Medical Center approved the recruitment, informed consent, and study procedures.
Independent variables
Age at time of assessment was determined via self-reported date of birth. Gender and race/ethnicity were self-reported using the 2000 U.S Census format. Income was categorized dichotomously at the median by annual family income (< $9,000; ≥ $9,000). Occupation was classified dichotomously as manual labor/housework or having a skilled career including skilled trade/craft, clerical/office worker, manager business/government, or professional/technical.
Hypertension was coded as present if the participant self-reported the condition during a medical interview or if they reported taking any medication prescribed to lower high blood pressure. Presence of at least one APOE-ε4 allele was determined by standard genotyping (Mayeux et al., 1995).
We assessed baseline cognitive functioning with a comprehensive neuropsychological battery, with comparable English and Spanish measures, described previously (Siedlecki et al., 2010; Stern et al., 1992). The WHICAP neuropsychological measures have demonstrated measurement invariance across English and Spanish speakers, as well as across racial/ethnic, sex/gender and racial/ethnic by sex/gender subgroups (Avila et al., in press; Siedlecki et al., 2010). Measurement invariance analyses were conducted to ensure construct comparability across educational groups in the current study. Results from invariance analyses suggested that full scalar invariance held across the groups.
We calculated composite scores by grouping the neuropsychological tasks by domain, as represented in the factor analysis of the battery performed by Siedlecki et al., 2010. Individual test scores were first standardized to a z-score metric based on sample means and standard deviations at baseline. Z-scores for each test within each cognitive domain resulted in four composite measures: episodic memory, language, executive, and visuospatial functioning. Episodic memory composites were derived at baseline and each follow-up assessment.
Total recall, delayed recall and delayed recognition trials from the Selective Reminding Test (Buschke and Fuld, 1974) comprised the episodic memory composite score. Tests of naming, repetition, and comprehension measured language ability. Correctly spontaneously recognized objects from a modified 15-item Boston Naming Test (Kaplan, Goodglass, & Weintraub, 1983) assessed naming ability. Subtests of the Boston Diagnostic Aphasia Examination (Goodglass, 1983) evaluated repetition and comprehension. Tasks of abstract reasoning, categorization, and letter fluency assessed executive function. A similarities subtest of the Wechsler Adult Intelligence Scale – Revised (Wechsler, 1981), and the total score on the Identities and Oddities subtest of the Mattis Dementia Rating Scale (Mattis, 1976) evaluated abstract reasoning and categorization. Letter fluency consisted of the total of named words beginning with three specific letters (C, F, L for English-speakers or P, S, V for Spanish-speakers). Finally, the total number of correct items from a task of matching and recognition of figures from the Benton Visual Retention Test (BVRT; Benton, 1955) and the copying of five visual designs from the Rosen Drawing Test (Rosen, 1981) determined visuospatial ability.
Statistical Analysis
We used episodic memory composite scores for baseline and each follow-up visit to determine memory trajectories. Sample sizes for the five episodic memory assessments were: 2573, 2556, 1988, 1405 and 898. We conducted a multiple-group Latent Growth Model (LGM) to identify the baseline predictors of initial memory performance (intercept) and rate of memory decline (slope) across the groups.
The model (Figure 1) was specified considering the influence of demographic (age, gender, race/ethnicity), socioeconomic (occupation and income), biomedical (hypertension status and APOE-ε4 status), and baseline cognitive (language, executive function, and visuospatial) variables on the intercept and the slope of memory trajectory. Additionally, we included age squared in the model to account for the non-linear effect of age with the independent variables. Assumptions of the model, including linear vs. quadratic slope, variability of intercept and slope within the education subgroups and constancy of residuals, and use of between-person predictors to explain the variance in memory intercept and slope, were tested and are reported in the supplementary material.
Figure 1.
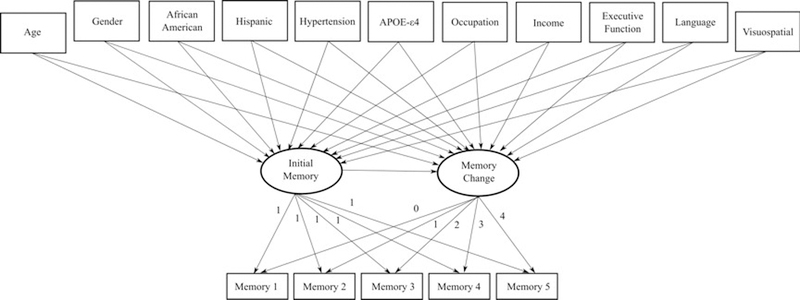
Model specification for multiple group comparisons
We divided participants into three educational attainment groups, based on self-reported years of schooling (Appendix A describes how educational level was coded in WHICAP): low (≤5 years), medium (6–11 years), and high (≥12 years). We based these cut-points on the sample distribution and the arrangement of grades as primary, secondary, and completed high school or more, and these cut-points are also consistent with education quartiles of this sample. We conducted descriptive statistics and group comparisons in SPSS version 23. We compared educational groups with ANOVA for continuous variables with Bonferroni post hoc tests, and categorical variables were compared using chi-square tests.
We performed multiple-group LGM analyses in MPlus Version 7.31 (Muthén & Muthén, Los Angeles, CA) to examine trajectories across education groups. We used the full information maximum likelihood missing data method, using all available data to estimate the model. The constrained model was built with all regression parameters to the intercept and slope fixed between educational groups. We tested improvement of the model fit by freeing a single regression path for a potential memory predictor per model, while all the others remained fixed. This approach allowed us to test the equal-fit hypothesis for each of the 10 predictors of memory trajectory. We compared the Akaike Information Criteria (AIC), the Bayesian Information Criteria (BIC), the sample-size adjusted BIC (aBIC) and the Likelihood Ratio Test (LTR) of each model to the fully constrained model. Considering that the BIC penalizes models with added complexity (additional degrees of freedom), we prioritized decreases in AIC, aBIC and LTR when comparing hierarchically nested models.
We additionally conducted an age-adjusted model examining the composite scores corrected for age by regressing baseline memory composite score on baseline age. The regression constant and slope were used to adjust baseline and follow-up composite scores for all time points. The age-adjusted model did not result in different results (data not shown). We also conducted a joint modeling combining latent growth model with discrete-time survival model to examine attrition due to death. The results from the joint discrete time survival and growth model in the overall sample indicated that the risk of death was not related to memory performance. Separate joint models were estimated for each education group. Risk of death was only associated with slope for the high education group (OR = 5.63 [1.13, 10.13]), suggesting that individuals in this group who demonstrated less cognitive decline over time were less likely to die during the study (data not shown).
Results
The descriptive characteristics of the sample are shown in Table 1. Educational groups did not differ by age, gender distribution, or frequency of APOE-ε4 carriers. The low education group had more Hispanics, fewer African Americans and Whites, fewer participants with skilled occupations and higher income, and had a lower cognitive performance at baseline in all three non-memory domains and episodic memory when compared with the medium and high education groups. The medium education group also had more Hispanics, fewer participants with skilled occupations and higher income, and lower baseline cognitive scores when compared with the high education group. The high education group had fewer participants with hypertension when compared with the other two groups. The intercept and slope of memory also differed across groups, with one exception: the low and medium educated groups showed similar slopes (Table 1).
Table 1.
Descriptive and comparison of the three educational attainment groups
| Low (L) N = 541 |
Medium (M) N = 824 |
High (H) N = 1208 |
Group Comparisons |
|
|---|---|---|---|---|
| Mean (SD) | ||||
| Age | 76.13 (6.00) | 76.24 (6.22) | 75.71 (6.22) | L = M = H |
| Language | −0.54 (0.82) | −0.10 (0.71) | 0.32 (0.55) | L < M < H |
| Executive Function | −0.65 (0.57) | −0.25 (0.62) | 0.46 (0.68) | L < M < H |
| Visuospatial | −0.80 (0.80) | −0.09 (0.72) | 0.40 (0.57) | L < M < H |
| Memory 1 | −0.04 (0.58) | 0.14 (0.60) | 0.49 (0.68) | L < M < H |
| Memory 2 | −0.33 (0.74) | −0.06 (0.76) | 0.36 (0.80) | L < M < H |
| Memory 3 | −0.25 (0.75) | −0.11 (0.78) | 0.27 (0.83) | L < M < H |
| Memory 4 | −0.32 (0.77) | −0.12 (0.79) | 0.31 (0.80) | L < M < H |
| Memory 5 | −0.45 (0.74) | −0.18 (0.79) | 0.17 (0.82) | L < M < H |
| Intercept | −0.01 (0.46) | 0.14 (0.50) | 0.45 (0.56) | L < M < H |
| Slope | −0.16 (0.07) | −0.15 (0.07) | −0.12 (0.07) | L = M > H |
| N (%) | ||||
| Female | 388 (71.7) | 564 (68.4) | 815 (67.5) | L = M = H |
| African American | 66 (12.1) | 311 (37.7) | 456 (37.7) | L < M = H |
| Hispanic | 447 (82.6) | 386 (46.8) | 176 (14.6) | L > M > H |
| White | 28 (5.3) | 127 (15.5) | 576 (47.7) | L < M < H |
| Hypertension | 351 (65.9) | 532 (64.6) | 696 (57.6) | L = M > H |
| Skilled Occupation | 43 (7.9) | 171 (20.8) | 847 (70.1) | L < M < H |
| Higher Income | 100 (18.5) | 331 (40.2) | 822 (68.0) | L < M < H |
| APOE-ε4 present | 143 (26.4) | 212 (25.7) | 299 (24.8) | L = M = H |
Table 2 displays the dropout and death rates, as well as assessment time interval differences between groups. The high education group had a longer time lapse between visits compared to the low and medium groups for intervals between time 2 and 3 and time 3 and 4.
Table 2.
Dropout and death rates, and interval differences between groups.
| Low | Medium | High | |
|---|---|---|---|
| Missing | Before time 5 – N(%) | ||
| Participated in all | 232(43) | 330 (40) | 445 (37) |
| Died | 170 (31) | 304 (37) | 407 (34) |
| Dropped out | 139 (26) | 192 (23) | 356 (29) |
| Intervals | Years between intervals | ||
| Time 1 to Time 2* | 1.91 | 1.88 | 2.00 |
| Time 2 to Time 3** | 2.00 | 2.11 | 2.33 |
| Time 3 to Time 4** | 2.49 | 2.55 | 2.75 |
| Time 4 to Time 5* | 2.62 | 2.45 | 2.68 |
In the full-constrained model (Table 3), the low education group demonstrated a steeper decline in memory compared to the high education group. Groups were similar in baseline memory performance in this model.
Table 3.
Multiple-group latent growth models for three group comparison
| Model | AIC | BIC | aBIC | Loglikelihood | LRT |
|---|---|---|---|---|---|
| Full Constrain | 10510.098 | 10794.874 | 10629.674 | −5203.049 | - |
| Freely estimated | |||||
| Age | 10515.879 | 10822.561 | 10644.653 | −5201.939 | 2.220 |
| Gender | 10513.973 | 10820.656 | 10642.748 | −5200.987 | 4.124 |
| African American | 10515.798 | 10822.480 | 10644.573 | −5201.899 | 2.300 |
| Hispanic | 10504.345 | 10811.027 | 10633.120 | −5196.172 | 13.754* |
| Income | 10514.104 | 10820.786 | 10642.879 | −5201.052 | 3.994 |
| Occupation | 10507.210 | 10813.892 | 10635.985 | −5197.605 | 10.888* |
| Hypertension | 10511.011 | 10817.693 | 10639.786 | −5199.505 | 7.088 |
| APOE e4 | 10514.245 | 10820.928 | 10643.020 | −5201.123 | 3.852 |
| Language | 10504.116 | 10810.798 | 10632.891 | −5196.058 | 13.982* |
| Executive Function | 10496.942 | 10803.624 | 10625.717 | −5192.471 | 21.156* |
| Visuospatial | 10484.104 | 10790.786 | 10612.879 | −5186.052 | 33.994* |
p<0.05
Multiple-Group Comparisons
The multiple group models revealed that, when freely estimated separately, executive function, language, visuoconstruction, occupation and being Hispanic improved model fit compared to the fully constrained model (Table 3). Table 4 shows fit statistic values for each group for each of the freely estimated parameters.
Table 4.
Constrained model estimates
| Predictor | Intercept | Slope |
|---|---|---|
| Hispanic | Low (0.039) > High (−0.240)* Med (−0.101) > High (−0.240)* |
|
| Occupation | Low (0.230) > Med (−0.025) | Med (0.006) > High (−0.024)* |
| Language | Low (0.030) < High (0.212)* Med (0.109)* < High (0.212)* |
|
| Executive Function | Low (0.098) < Med (0.240)* Low (0.098) < High (0.317)* |
|
| Visuospatial | Low (−0.051) < Med (0.120)* Low (−0.051) < High (0.219)* Med (0.120)* < High (0.219)* |
Med: Medium;
Significantly related
Higher scores on executive function and visuospatial ability at baseline were stronger predictors of baseline memory performance for the medium education group than for the low education group. No differences were found for predictors of episodic memory decline across the low and medium education groups.
Comparing low and high education groups revealed that being non-Hispanic and having higher non-memory performance at baseline (executive function, language and visuospatial abilities) were important predictors for the high education group (Table 4). No free estimated predictor distinctly influenced episodic memory decline between these two groups.
Comparing the medium and high education groups revealed that being non-Hispanic was a predictor of memory intercept only for the high educated participants. Better language and visuospatial cognitive performances at baseline were predictors of memory intercept in both medium and high education groups. Having a skilled occupation was associated with less decline in memory only in the highly educated group.
The differences in predicted trajectories for the groups is illustrated in figure 2.
Figure 2.
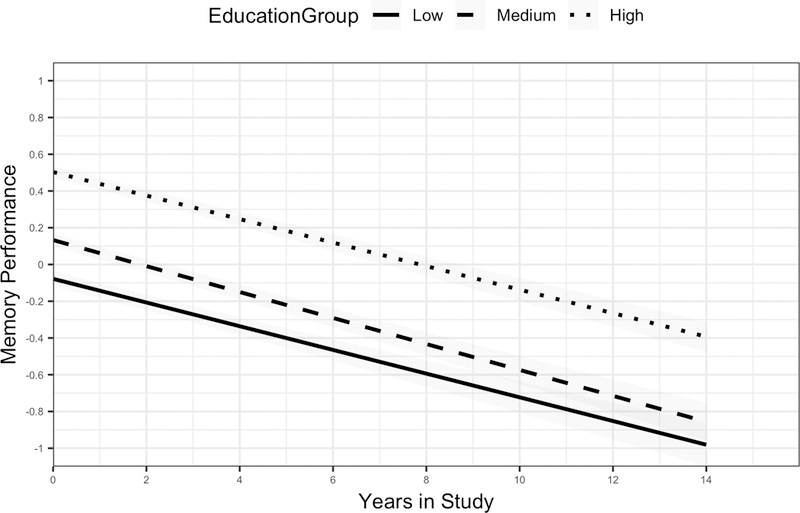
Differences in episodic memory predicted trajectories for the groups. Y-axis accounts for the episodic memory composite score, X-axis accounts for the years in the study. Low education group in solid line, medium education group in dashed line and high education group in dotted line.
Discussion
In this study, we aimed to determine if risk and resilience factors for episodic memory trajectory differed across educational strata. In this diverse cohort of older adult residents of the Washington Heights neighborhood of New York City, for many participants, early childhood rural residence, non-existent or unenforced compulsory school laws, and governmental neglect of schools led to a lack of opportunity to attend school during childhood. This educational diversity allowed us to create three educational strata: less than 5 years, 6–11 years, and 12+ years of school. We found that memory trajectories within the three educational groups differentially related to potential demographic, socioeconomic, biomedical, and cognitive factors of risk and resilience. Overall, we found a higher number of factors that influenced memory trajectory in the medium and high education groups than in the low education group.
Contrary to our expectations that language and executive function would be better predictors of memory trajectory in the low educated group, visuospatial ability at baseline was a consistent predictor of initial memory performance only for the medium and high education groups. Our hypothesis was based on research showing that illiterates recruit more parietal areas compared to literates during cognitive tasks (Julayanont & Ruthirago, 2016; Petersson et al., 2007). Also, prior research has shown that retrieval of episodic information and forced-choice recognition are related to parietal cortex function (Buckner & Wheeler, 2001; Wagner et al., 2005). However, our results suggest that executive and visuospatial skills do not provide a unique resource for maintaining memory function for older adults with low education.
Executive function and language performance at baseline predicted the initial memory performance for the high education group, but not the low education group. The memory task used is a verbal list learning measure, and thus, the association between language skills such as semantic retrieval and generative fluency and initial memory performance (but not decline) is unsurprising. The availability of a superior verbal knowledge system is related to an increased capacity for learning words by relying on an existing network and using categorization strategies (Bouazzaoui et al., 2013; Rast, 2011). Executive function may also predict memory performance by increasing the efficiency of the recall process and by monitoring the already recalled information (Hertzog et al., 2003; Rast, 2011). Tasks that tap frontal lobe function are also related to efficient memory recall and encoding, and lesions in these brain areas are capable of resulting in clinical memory deficit (Buckner & Wheeler, 2001). The frontoparietal control network was associated with successful memory performance (Franzmeier et al., 2017) in a sample with high education. Our results, suggest that integrated connectivity may be present in participants with high level of education, but not in those with low education.
Perhaps integrated cognitive systems are tied to literacy acquisition, which is related to visual processing improvement, ventral occipito-temporal pathway reorganization, and better fractional anisotropy of the left arcuate fasciculus, leading to a reinforcement of the left temporo-parietal connections (Julayanont & Ruthirago, 2016; Petersson et al., 2007; Thiebaut de Schotten et al., 2012;).
Independent of performance in non-memory cognitive domains, not being Hispanic was also a strong predictor of better initial memory performance for the high education group when compared to the low education group. 15% of the participants from the high education group identified as Hispanic, and from these, 90% were educated in their birth countries before immigrating to the United States of America (USA). Distinct educational quality may impact initial memory performance in Hispanics compared with Whites and African Americans highly-educated in the USA. Socioeconomic and legal systems related to education may account for a discrepancy in educational quality between Hispanics and other ethnic groups. Educational quality can impact cognitive performance more than the self-reported years of school attendance (Manly et al. 2002; Sisco et al., 2013). It is possible that quality of education has an impact on brain network organization, leading to a distinct cognitive compensatory mechanism for those with higher educational quality.
Our study also had several limitations. One limitation of our study is the absence of an education quality measure. This is a methodological challenge considering the diversity of educational experiences present in the current sample, many of whom were educated in strikingly dissimilar contexts across the US or for 90% of our cohort of Hispanics who received their primary education outside of the USA. Due to this broad linguistic, geographic, and cultural variety, the development and validation of a single or psychometrically equivalent measure of education quality across our cohort remains a difficult task. Another limitation was our assessment of hypertension. We defined hypertension through self-report or use of medication prescribed to lower high blood pressure. This may result in some uncertainty about current level of hypertension. Furthermore, our study did not include neuroimaging variables as baseline predictors given that neuroimaging data was not available for the majority of participants in this sample. Future studies should do so given structural brain imaging research showing potential cognitive trajectory predictors (e.g. greater baseline gray and white matter volume) (Carmichael et al., 2012).
Several biomedical, socioeconomic and demographic factors predicted memory trajectory in the overall model (all education groups included), but when comparing education groups, only Hispanic ethnicity differed as a predictor of baseline memory score. Furthermore, the predictors that differed across groups influenced initial memory performance only, but not longitudinal change. Our results are in accordance with other studies that, despite identifying multiple demographic predictors of baseline cognitive performance, identified only a few predictors of cognitive trajectory (Early et al., 2013; Farias et al., 2011). This finding may be partially explained by the fact that distinct rates of cognitive decline are not consistently found across educational groups (Zahodne et al., 2011).
In conclusion, this study tested a unified model of predictors of memory trajectory among older adults with a broad range of educational backgrounds. Given that most previous research assessing longitudinal memory and cognitive trajectories rely on highly educated participants, predictors of trajectory generated from those studies may not be applicable to people with low educational attainment. Considering that older adults with low educational level are at higher risk for developing dementia, and the high prevalence of low education among older adults around the world, there is a critical need for researchers to determine if there are unique risk and resilience factors for cognitive decline in this group. The goal of this line of research within observation studies is to point to potential modifiable sources of protection or risk for cognitive decline that could be incorporated into interventions to maintain cognitive function with aging. Our results suggest that if causal relationships were established, interventions on social, medical, and biological factors would equally benefit memory performance (but not memory decline) across educational groups.
Supplementary Material
Acknowledgements
This work was supported by the National Institutes of Health (NIA AG R01 AG037212 & RF1 AG054023).
Appendix A – Educational Level WHICAP coding
The WHICAP coding for educational level combines self-reported years of formal academic education and credential and the final number range from 0 to 20. This coding system does not consider partial years.
If the participant did not receive a high school degree or equivalent degree (e.g. GED), their education level is coded from 0 to 11. This number represents the highest grade completed.
If the participant received a high school diploma as a terminal degree, 12 years is coded regardless of number of years required to complete it. If the participant received an equivalent degree (e.g. GED) as a terminal degree, the actual number of years of formal education is coded.
If the participant attended college and did not graduate, their education level is coded from 13–15, based on the number of years completed. If the participant received an Associate’s degree, 14 years is coded. If the participant received a Bachelor’s degree, 16 years is coded, regardless of the number of years required to do so. If the participant attended a trade or technical school, these years are counted towards years of education.
If the patient received a Master’s degree, 18 years is coded. If the participant received a JD degree or attended three or more years of education (e.g., PhD, MD, DDS) for a doctoral degree, 19 years is coded. If the participant received a doctoral degree, 20 years is coded. If a participant has multiple graduate degrees including a doctorate (e.g., MS and MD), their education level remains coded as 20 years.
Footnotes
The authors report no conflicts of interest.
References
- Albert MS, Jones K, Savage CR, Berkman L, Seeman T, Blazer D, & Rowe JW (1995). Predictors of cognitive change in older persons: MacArthur studies of successful aging. Psychology and Aging, 10(4), 578–589. doi: 10.1037/0882-7974.10.4.578 [DOI] [PubMed] [Google Scholar]
- Albrecht MA, Szoeke C, Maruff P, Savage G, Lautenschlager NT, Ellis KA, … Group, A. R. (2015). Longitudinal cognitive decline in the AIBL cohort: The role of APOE epsilon4 status. Neuropsychologia, 75, 411–419. doi: 10.1016/j.neuropsychologia.2015.06.008 [DOI] [PubMed] [Google Scholar]
- Amieva H, Mokri H, Le Goff M, Meillon C, Jacqmin-Gadda H, Foubert-Samier A, … Dartigues J-F (2014). Compensatory mechanisms in higher-educated subjects with Alzheimer’s disease: a study of 20 years of cognitive decline. Brain, 137(4), 1167–1175. doi: 10.1093/brain/awu035 [DOI] [PubMed] [Google Scholar]
- Avila JF, Rentería M. Arce, Witkiewitz K, Verney SP, Vonk JMJ, & Manly JJ (2019). Measurement invariance of neuropsychological measures of cognitive aging across race/ethnicity by sex/gender groups. Neuropsychology. doi: 10.1037/neu0000584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benton AL (1955). The Visual Retention Test. New York: The Psychological Corporation. [Google Scholar]
- Bermejo-Pareja F, Benito-Leon J, Louis ED, Trincado R, Carro E, Villarejo A, & de la Camara AG (2010). Risk of incident dementia in drug-untreated arterial hypertension: a population-based study. J Alzheimers Dis, 22(3), 949–958. doi: 10.3233/JAD-2010-101110 [DOI] [PubMed] [Google Scholar]
- Bouazzaoui B, Fay S, Taconnat L, Angel L, Vanneste S, & Isingrini M (2013). Differential involvement of knowledge representation and executive control in episodic memory performance in young and older adults. Canadian Journal of Experimental Psychology/, 67(2), 100–107. doi: 10.1037/a0028517 [DOI] [PubMed] [Google Scholar]
- Buckner RL, & Wheeler ME (2001). The cognitive neuroscience of remembering. Nat Rev Neurosci, 2(9), 624–634. doi: 10.1038/35090048 [DOI] [PubMed] [Google Scholar]
- Buschke H, & Fuld PA (1974). Evaluating storage, retention, and retrieval in disordered memory and learning. Neurology, 24, 1019–1025. [DOI] [PubMed] [Google Scholar]
- Carmichael O, Mungas D, Beckett L, Harvey D, Tomaszewski Farias, S., Reed B, … Decarli C. (2012). MRI predictors of cognitive change in a diverse and carefully characterized elderly population. Neurobiol Aging, 33(1), 83–95. doi: 10.1016/j.neurobiolaging.2010.01.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Early DR, Widaman KF, Harvey D, Beckett L, Park LQ, Farias ST, … Mungas D. (2013). Demographic predictors of cognitive change in ethnically diverse older persons. Psychol Aging, 28(3), 633–645. doi: 10.1037/a0031645 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farias ST, Mungas D, Hinton L, & Haan M (2011). Demographic, neuropsychological, and functional predictors of rate of longitudinal cognitive decline in Hispanic older adults. Am J Geriatr Psychiatry, 19(5), 440–450. doi: 10.1097/JGP.0b013e3181e9b9a5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster JK, Albrecht MA, Savage G, Lautenschlager NT, Ellis KA, Maruff P, … Group, A. R. (2013). Lack of reliable evidence for a distinctive epsilon4-related cognitive phenotype that is independent from clinical diagnostic status: findings from the Australian Imaging, Biomarkers and Lifestyle Study. Brain, 136(Pt 7), 2201–2216. doi: 10.1093/brain/awt127 [DOI] [PubMed] [Google Scholar]
- Foubert-Samier A, Catheline G, Amieva H, Dilharreguy B, Helmer C, Allard M, & Dartigues JF (2012). Education, occupation, leisure activities, and brain reserve: A population-based study. Neurobiology of Aging, 33(2). 10.1016/j.neurobiolaging.2010.09.023 [DOI] [PubMed] [Google Scholar]
- Franzmeier N, Hartmann J, Taylor ANW, Araque-Caballero MÁ, Simon-Vermot L, Kambeitz-Ilankovic L, … Ewers M (2018). The left frontal cortex supports reserve in aging by enhancing functional network efficiency. Alzheimer’s Research & Therapy, 10(1), 28 10.1186/s13195-018-0358-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gifford KA, Badaracco M, Liu D, Tripodis Y, Gentile A, Lu Z, … Jefferson AL (2013). Blood Pressure and Cognition Among Older Adults: A Meta-Analysis. Archives of Clinical Neuropsychology, 28(7), 649–664. doi: 10.1093/arclin/act046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodglass H (1983). The assessment of aphasia and related disorders (2nd ed.), Philadelphia: Lea & Febiger. [Google Scholar]
- Hertzog C, Dixon RA, Hultsch DF, & MacDonald SWS (2003). Latent Change Models of Adult Cognition: Are Changes in Processing Speed and Working Memory Associated With Changes in Episodic Memory? Psychology and Aging, 18(4), 755–769. doi: 10.1037/0882-7974.18.4.755 [DOI] [PubMed] [Google Scholar]
- Julayanont P, & Ruthirago D (2018). The illiterate brain and the neuropsychological assessment: From the past knowledge to the future new instruments. Applied Neuropsychology:Adult. 10.1080/23279095.2016.1250211 [DOI] [PubMed] [Google Scholar]
- Kaplan E, Goodglass H, & Weintraub S (1983). The Boston Naming Test. Philadelphia: Lea & Febiger. [Google Scholar]
- Knopman D, Boland LL, Mosley T, Howard G, Liao D, Szklo M, … Atherosclerosis Risk in Communities Study, I. (2001). Cardiovascular risk factors and cognitive decline in middle-aged adults. Neurology, 56(1), 42–48. [DOI] [PubMed] [Google Scholar]
- Lundervold AJ, Wollschläger D, & Wehling E (2014). Age and sex related changes in episodic memory function in middle aged and older adults. Scandinavian Journal of Psychology, 55(3), 225–232. doi: 10.1111/sjop.12114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattis S (Ed.). (1976). Mental status examination for organic mental syndrome in the elderly patient. New York: Grune & Stratton. [Google Scholar]
- Manly JJ, Jacobs DM, Sano M, Bell K, Merchant CA, Small SA, & Stern Y (1999). Effect of literacy on neuropsychological test performance in nondemented, education-matched elders. J Int Neuropsychol Soc, 5(3), 191–202. [DOI] [PubMed] [Google Scholar]
- Manly JJ, Jacobs DM, Touradji P, Small SA, & Stern Y (2002). Reading level attenuates differences in neuropsychological test performance between African American and White elders. Journal of the International Neuropsychological Society, 8(03), 341–348. doi: 10.1017/S1355617702813157 [DOI] [PubMed] [Google Scholar]
- Mayeux R, Ottman R, Maestre G, Ngai C, Tang MX , Ginsberg H, et al. (1995). Synergistic effects of traumatic head injury and apolipoprotein-epsilon 4 in patients with Alzheimer’s disease. Neurology, 45 (3 Pt 1), pp. 555–557. [DOI] [PubMed] [Google Scholar]
- Meng X & D’Arcy C (2012). Education and Dementia in the Context of the Cognitive Reserve Hypothesis: A Systematic Review with Meta-Analyses and Qualitative Analyses. PLoS ONE 7(6): e38268. doi: 10.1371/journal.pone.0038268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK & Muthén BO (1998-2012). Mplus User’s Guide. Seventh Edition Los Angeles, CA: Muthén & Muthén [Google Scholar]
- Petersson KM, Reis A, & Ingvar M (2001). Cognitive processing in literate and illiterate subjects: a review of some recent behavioral and functional neuroimaging data. Scand J Psychol, 42(3), 251–267. [DOI] [PubMed] [Google Scholar]
- Petersson KM, Silva C, Castro-Caldas A, Ingvar M, & Reis A (2007). Literacy: A cultural influence on functional left-right differences in the inferior parietal cortex. European Journal of Neuroscience. 10.1111/j.1460-9568.2007.05701.x [DOI] [PubMed] [Google Scholar]
- Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, & Ferri CP (2013). The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement, 9(1), 63–75 e62. doi: 10.1016/j.jalz.2012.11.007 [DOI] [PubMed] [Google Scholar]
- Rast P (2011). Verbal knowledge, working memory, and processing speed as predictors of verbal learning in older adults. Developmental Psychology, 47(5), 1490–1498. doi: 10.1037/a0023422 [DOI] [PubMed] [Google Scholar]
- Rosen W (1981). The Rosen Drawing Test. Bronx, NY: Veterans Administration Medical Center. [Google Scholar]
- Sachs-Ericsson N, & Blazer DG (2005). Racial differences in cognitive decline in a sample of community-dwelling older adults: the mediating role of education and literacy. Am J Geriatr Psychiatry, 13(11), 968–975. doi: 10.1176/appi.ajgp.13.11.968 [DOI] [PubMed] [Google Scholar]
- Siedlecki KL, Manly JJ, Brickman AM, Schupf N, Tang MX, & Stern Y (2010). Do neuropsychological tests have the same meaning in spanish speakers as they do in english speakers? Neuropsychology, 24(3), 402–411. 10.1037/a0017515 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sisco S, Gross AL, Shih RA, Sachs BC, Glymour M, Bangen KJ, Benitez A, Skinner J, Schneider BC, & Manly JJ (2013). The role of early-life educational quality and literacy in explaining racial disparities in cognition in late life. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, doi: 10.1093/geronb/gbt133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stern Y, Andrews H, Pittman J, Sano M, Tatemichi T, Lantigua R, & Mayeux R (1992). Diagnosis of Dementia in a Heterogeneous Population: Development of a Neuropsychological Paradigm-Based Diagnosis of Dementia and Quantified Correction for the Effects of Education. Archives of Neurology, 49(5), 453–460. 10.1001/archneur.1992.00530290035009 [DOI] [PubMed] [Google Scholar]
- Stern Y (2009). Cognitive reserve. Neuropsychologia, 47, 2015–2028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stern Y (2012). Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol, 11(11), 1006–1012. doi: 10.1016/S1474-4422(12)70191-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thiebaut de Schotten, M., Cohen L, Amemiya E, Braga LW, & Dehaene S (2014). Learning to read improves the structure of the arcuate fasciculus. Cereb Cortex, 24(4), 989–995. doi: 10.1093/cercor/bhs383 [DOI] [PubMed] [Google Scholar]
- Wagner AD, Shannon BJ, Kahn I, & Buckner RL (2005). Parietal lobe contributions to episodic memory retrieval. Trends in Cognitive Sciences, 9(9), 445–453. [DOI] [PubMed] [Google Scholar]
- Wechsler D (1981). Wechsler Adult Intelligence Scale-Revised. New York: The Psychological Corporation. [Google Scholar]
- Wilson RS, Capuano AW, Sytsma J, Bennett DA, & Barnes LL (2015). Cognitive aging in older Black and White persons. Psychology and Aging, 30(2), 279–285. doi: 10.1037/pag0000024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yaffe K, Falvey C, Harris TB, Newman A, Satterfield S, Koster A, … Health, A. B. C. S. (2013). Effect of socioeconomic disparities on incidence of dementia among biracial older adults: prospective study. BMJ, 347, f7051. doi: 10.1136/bmj.f7051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zahodne LB, Glymour MM, Sparks C, Bontempo D, Dixon RA, MacDonald SWS, & Manly JJ (2011). Education Does Not Slow Cognitive Decline with Aging: 12-Year Evidence from the Victoria Longitudinal Study. Journal of the International Neuropsychological Society, 17(06), 1039–1046. doi: 10.1017/S1355617711001044 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.