

Abstract
Background
Historically, students with intellectual disability were not expected to learn to read, and thus were excluded from reading instruction. Over the past decades, societal expectations for this group of learners have changed in that children and adolescents with intellectual disability are now expected to be provided with, and benefit from, literacy instruction. This shift in societal expectations has also led to an increase in research examining effective interventions for increasing beginning reading skills for students with intellectual disability.
Objectives
To assess the effectiveness of interventions for teaching beginning reading skills to children and adolescents with intellectual disability.
Search methods
We searched the following electronic databases up to October 2019: CENTRAL; MEDLINE, including Epub Ahead of Print and In‐Process and Other Non‐Indexed Citations, Embase, 13 other databases, and two trials registers. We contacted authors of included studies, examined reference lists, and used Google Scholar to search for additional studies.
Selection criteria
We included randomized controlled trials (including trials that use quasi‐random methods of allocation such as date of birth), involving children and adolescents with intellectual disability (defined as an intelligence quotient (IQ) two standard deviations or more below the population mean) between the ages of 4 and 21 years, that evaluated the efficacy of a beginning reading intervention compared to a control intervention, including no treatment control, wait‐list control, treatment as usual, attention control, or alternate non‐reading instruction control.
Data collection and analysis
Two review authors independently screened titles and abstracts yielded by the search against the inclusion criteria, and extracted data from each trial using a piloted data extraction form to collect information about the population, intervention, randomization methods, blinding, sample size, outcome measures, follow‐up duration, attrition and handling of missing data, and methods of analysis. When data were missing, one review author contacted the study authors to request additional information. Two review authors assessed the risk of bias of each included study and rated the quality of the evidence using the GRADE approach (a systematic method for rating the certainty of evidence in meta‐analyses). We conducted random‐effect meta‐analyses, with inverse‐variance weighting to combine effect sizes for each of our primary and secondary outcomes. We presented effect sizes as standardized mean differences (SMD) with 95% confidence intervals (CI).
Main results
We identified seven studies involving 352 children and adolescents with intellectual disabilities that met the inclusion criteria. All studies provided the intervention in school settings. Four studies were conducted in the USA, one in Canada, and two in the UK. Three studies were funded by grants from the US Department of Education, Institute of Education Sciences; one study by the Canadian Language and Literacy Research Network and the Nova Scotia Health Research Foundation; and three studies did not indicate a funding source.
We identified some concerns with risk of bias, mainly due to the difficulty of blinding of participants and personnel, and the lack of blinding of outcome assessors.
Meta‐analyses of the data demonstrated small‐to‐moderate effects of beginning reading interventions delivered to children and adolescents with intellectual disability across four dependent variables. We found medium effect sizes in favor of the beginning reading interventions for the primary outcomes of phonologic awareness (SMD 0.55, 95% CI 0.23 to 0.86; 4 studies, 178 participants; moderate‐quality evidence), word reading (SMD 0.54, 95% CI 0.05 to 1.03; 5 studies, 220 participants; moderate‐quality evidence), and decoding (SMD 0.40, 95% CI 0.12 to 0.67; 5 studies, 230 participants; low‐quality evidence). The studies reported no adverse events. We also found a moderate effect for the secondary outcomes of oral reading fluency (SMD 0.65, 95% CI –0.12 to 1.42; 2 studies, 84 participants; low‐quality evidence) and language skills (SMD 0.28, 95% CI 0.03 to 0.54; 3 studies, 222 participants; moderate‐quality evidence).
Authors' conclusions
Results from this review provide evidence that beginning reading interventions that include elements of phonologic awareness, letter sound instruction, and decoding, delivered to children and adolescents with intellectual disability, are associated with small‐to‐moderate improvements in phonologic awareness, word reading, decoding, expressive and receptive language, and oral reading fluency. These findings are aligned with previously conducted studies that examined the effects of reading interventions for people without intellectual disability.
Plain language summary
Beginning reading interventions for children and adolescents with intellectual disability
What was the aim of the review?
Children and adolescents with an intellectual disability have below average cognitive abilities and everyday skills. In the past, no‐one expected them to learn to read, but that has now changed. This review aimed to find out if specialized reading instruction (for example, small group instruction on letter‐sound awareness) could help children and adolescents who have an intellectual disability learn to read.
What did the review study?
We examined beginning reading interventions (methods) provided in schools to children and adolescents with intellectual disabilities. We examined the effects of the intervention on beginning reading skills, including phonologic awareness (blending sounds into words), reading words, decoding (correctly pronouncing written words), and language skills such as vocabulary.
What are the main results of the review?
We located seven studies that examined beginning reading interventions for children and adolescents with intellectual disability. Four studies were conducted in the USA, one in Canada, and two in the UK. These studies compared beginning reading interventions to standard reading instruction. The studies included 352 children and adolescents with intellectual disabilities. All studies provided the intervention in school settings. The findings of the review suggest that beginning reading interventions probably improve phonologic awareness, word reading, and language skills (moderate‐quality evidence) and may improve decoding skills and oral reading fluency (low‐quality evidence). Three studies were funded by grants from the US Department of Education, Institute of Education Sciences; one study by the Canadian Language and Literacy Research Network and the Nova Scotia Health Research Foundation; and three studies did not indicate a funding source.
Key messages
The results of this review show that beginning reading interventions are moderately effective for improving phonologic awareness, word reading, decoding skills, oral reading fluency, and language skills in children and adolescents with intellectual disability. The quality of the evidence was low and moderate across the five outcomes we analyzed. No study reported side effects of treatment.
How up‐to‐date is this review?
We included studies published up to October 2019.
Summary of findings
Background
Description of the condition
The International Classification of Diseases describes intellectual disability as "a condition of arrested or incomplete development of the mind, which is especially characterized by impairment of skills manifested during the developmental period, skills which contribute to the overall level of intelligence (i.e. cognitive, language, motor, and social abilities)" (WHO 2010). Intellectual disability is "characterized by significant limitations both in intellectual functioning (reasoning, learning, problem solving) and in adaptive behavior, which covers a range of everyday social and practical skills….[and] originates before the age of 18" (AAIDD 2011; p 1). Significant limitation is most commonly defined as a score (with measurement error considered) on a standardized, norm‐referenced assessment that is approximately two standard deviations (SD) or more below the population mean (e.g. an intelligence quotient (IQ) of 70 or less; Luckasson 2002). Other definitions have been adopted by various organizations (e.g. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM‐IV; APA 2000); International Classification of Functioning, Disability and Health (ICF; WHO 2001)), although most emphasize three dimensions, including intellectual functioning, adaptive behavior, and early manifestation (Polloway 2011).
Globally, an array of terms is used to describe the condition of intellectual disability. Across 147 countries, the most commonly used terms include 'mental retardation' (76%), 'intellectual disabilities' (56.8%), 'mental handicap' (39.7%), 'learning disabilities' (32.3%), 'developmental disabilities' (22.6%), 'mental deficiency' (17.2%), and 'mental subnormality' (11.6%) (WHO 2007). The term 'general learning difficulties' is often used in education and health fields in the UK. However, many professional and governmental organizations and the broader professional community have shifted to the use of 'intellectual disability' (Schalock 2011), and advocates remain focused on increasing the consistent use of the term 'intellectual disability' by governmental and professional organizations worldwide. Schalock 2007 provided the rationale for the change:
"The term intellectual disability (a) reflects the changed construct of disability proposed by AAIDD [American Association of Intellectual and Developmental Disabilities] and WHO [World Health Organization]; (b) aligns better with current professional practices that are focused on functional behaviors and contextual factors; (c) provides a logical basis for individualized supports provision due to its basis in a social‐ecological framework; (d) is less offensive to persons with disabilities; and (e) is more consistent with international terminology" (Schalock 2007, p 120). Although the increasing consensus on the preferred use of the term 'intellectual disability' has occurred in the last decade, the essential elements of the condition formerly called 'mental retardation', specifically, limitations in intellectual functioning, deficits in adaptive behavior, and early age of onset, have not changed in over 50 years.
The prevalence of intellectual disability is estimated to be 10.37 in 1000 people, globally (Maulik 2011). Maulik 2011 reported variation in prevalence rates across studies, with higher incidences of intellectual disability found when samples were drawn from low‐ and middle‐income countries, rural and urban slum populations, and child or adolescent populations. However, the overall prevalence rate is similar to previous estimates that approximately 1% of students from high‐income countries are identified as having intellectual disability (Polloway 2010). Although the prevalence rate is low, it is worth noting that this represents a substantial number of people worldwide who are in need of educational services – approximately 31 million children, adolescents, and young adults up to 24 years of age (US Census Bureau 2013).
Causation is often unknown, particularly for people with intellectual disability who have higher IQ scores (i.e. slightly below the cut‐off of two SDs below the mean; Snell 2009). Cases with an identified cause result in various levels of intellectual disability but are most often associated with more significant cognitive impairment (Polloway 2006). Known causes include specifiable biologic causes such as chromosomal abnormalities (e.g. Down syndrome, fragile X syndrome), metabolic disorders (e.g. phenylketonuria), and postnatal brain disease (e.g. neurofibromatosis). Additionally, early infection (e.g. congenital rubella), trauma (e.g. oxygen deprivation during birth, severe head injury), and exposure to toxins (e.g. lead poisoning) are causally connected to intellectual disability. Poverty and cultural deprivation have also been associated with an increased risk of intellectual disability, possibly due to deficits in nutrition, education, and health care, and increased environmental risks (Hardman 2014). However, the relationship between biologic and environmental causes of intellectual disability is complex. For many people, the precise contribution of possible causes cannot be confirmed (Polloway 2011). Additional research is needed to understand better the interactions between environmental and biologic causes (Dykens 1995; Tunnicliffe 2011).
Quality of life of people with intellectual disability has improved in many countries since the last half of the 20th century (Weymeyer 2013). This improvement is due, in part, to changes in how societies view people with intellectual disability (Spooner 2011). Representative of this changing view is the number of people with intellectual disability who live in large institutions. Beadle‐Brown and colleagues conducted a review of the literature and found that many countries (e.g. Canada, England, Norway, Sweden, USA) have substantially decreased the numbers of people with intellectual disability who live in institutionalized settings since the 1980s (Beadle‐Brown 2007). Other countries (e.g. Belgium, Germany, Greece, Spain, The Netherlands) have only begun the process of deinstitutionalization more recently, and institutional care continues to be the most common living condition for people with intellectual disability. Legal protections for people with intellectual disability have also changed since the 1950s in many countries (Weymeyer 2013). The WHO surveyed 147 participating countries and documented that 59.2% had a national policy or program specifically related to intellectual disability, and that 22.4% referred to intellectual disability in other policies (WHO 2007). However, 18.4% of respondents indicated that intellectual disability was not covered by any policy or program. In terms of education, 77.8% of countries addressed intellectual disability in a specific education policy or program. These improvements are not, however, uniform across countries. A small number of countries (e.g. Taiwan) continue to advocate for increased institutionalization (Beadle‐Brown 2007). In addition, the level of change in living conditions varies greatly within and across countries, largely dependent on support from local and national organizations and the availability of resources (IASSID 2001). For example, lower‐income countries were less likely than high‐income countries to address intellectual disability in their education policies or programs (66.7% with low income versus 90.5% with high income).
There is high variability in outcomes for adults with intellectual disability, often moderated by the level of cognitive impairment and the availability of resources to provide intervention and ongoing support (Stein 2011). Levels of employment range from 37% to 70% of adults with intellectual disability; however, people work, on average, only 20 hours per week to 28 hours per week at wages substantially below median income (Huang 2010). Intellectual disability is also associated with an increased risk for physical (e.g. obesity, mobility impairments) and mental (e.g. psychiatric disorders, anxiety disorders) health problems (Stein 2011). Further, adults with intellectual disability often have smaller social networks whose members are most often family members, care providers, or disabled peers (Huang 2010). Additional research is needed to document how ongoing changes in how people with intellectual disability are viewed by society have affected adult outcomes.
It is not surprising that people with intellectual disability are less skilled readers than their typically developing peers since reading is a complex cognitive skill and poorer performance on cognitive tasks is a defining characteristic of intellectual disability (Stanovich 1985). Reading difficulty has been reported as the most common secondary condition that causes significant limitation for people with intellectual disability (Koritsas 2011). As would be expected, people with intellectual disability consistently underperform compared to typically developing peers who are matched on verbal ability on key reading skills (e.g. word recognition, phonologic decoding; Channell 2013). Wei 2011 demonstrated that the reading skills of students with intellectual disability are also substantially less developed than peers with other disabilities (e.g. autism, specific learning disabilities). The study authors estimated longitudinal growth trajectories on letter‐word identification and passage comprehension for 3421 students with various disabilities across the ages of 7 to 17 years. At all points in time, the mean performance of students with intellectual disability was lower than that of students in all other disability categories. Katims 2000 examined the reading skills of a group of 132 elementary, middle‐, and high‐school students with intellectual disability (IQ between 29 and 76). The study author reported that only 22.2% had obtained minimum literacy, defined as 1. reading and comprehending connected text at the primer level, 2. being able to write at least two graphemes representing spoken sounds, and 3. being able to write at least two words correctly. Further, Lemons and colleagues estimated the reading skill of a sample of 7440 students with disabilities using curriculum‐based measurement (CBM; Deno 1985) (Lemons 2013). In this sample, only 1.9% of students with intellectual disability in grade eight (n = 663) and 3.5% of students with intellectual disability in grade 11 (n = 498) were able to read a passage at a fifth grade (equivalent to an eight‐year‐old) level.
Despite evidence of substantial impairment in reading ability for people with intellectual disability, individual differences in reading skill have also been documented. Severity of intellectual impairment has been frequently cited as a significant predictor of variation in academic performance for people with intellectual disability. For example, Turner 2008 examined longitudinal predictors of academic attainment in a sample of 71 people with intellectual disability (i.e. Down syndrome). Mental age assessed at the beginning of the study (when participants had a mean age of nine years) accounted for the largest portion of variance in academic attainment (i.e. a composite of reading, writing, and numeracy skill) assessed 14 years later. Additionally, researchers have explored relationships between cognitive ability and reading skill for a variety of alphabetic languages (i.e. languages in which phonemes (individual spoken sounds) are represented by graphemes (written symbols used to represent the sounds)). Across an array of languages, intelligence is statistically significantly correlated with a range of readings skills for people with intellectual disability (French: Cohen 2001; Hebrew: Levy 2011; Persian: Soltani 2013).
Description of the intervention
Literacy, broadly defined, encompasses "using printed and written information to function in society, to achieve one's goals, and to develop one's knowledge and potential" (Kirsch 2002, p 2). Beginning reading instruction focuses on teaching students to identify printed letters and words. The process of learning to read entails "coming to know how one's writing system works" (Perfetti 1998, p 6). In other words, reading involves learning how spoken language is encoded in the printed form of the writing system. This learning is a necessary component in developing higher‐level reading skills, including reading comprehension and being able to get meaning from print. The focus of this review will be on beginning reading interventions that target initial acquisition of reading skills, not on interventions targeting higher‐level reading skills such as reading comprehension, reading vocabulary, and oral reading fluency.
Traditionally, for people with intellectual disability, two approaches have been used to teach beginning reading skills to children and adolescents with intellectual disability: sight word and phonics.
Sight word approach
The most common approach for teaching students with intellectual disability has been a sight word approach, by which students memorize a set of words (Browder 1998). Often, words are selected for their functional use (e.g. words that facilitate grocery shopping or safety), and a visual (e.g. photograph, icon) or physical (e.g. real or artificial object) representation may be paired with the printed word to facilitate learning. Students with intellectual disability who have been provided systematic sight word instruction have learned to identify a fairly large number of words (Browder 2006). Traditionally, this approach has been preferred over phonics‐based approaches (described below), based on the presumption that attempting to teach people with intellectual disability to read by understanding relationships between phonemes and graphemes would be too cognitively taxing and thus unsuccessful (Browder 2009). Despite its effectiveness at increasing the ability to read a set number of taught words, a sight word approach is limited. People who learn to read via sight word instruction have only a limited understanding of how the writing system encodes spoken language (i.e. focusing on whole words rather than graphemes limits a learner's ability to benefit from the connection between print and sounds). Thus, students do not learn how to generalize their learning beyond directly taught words. More specifically, students do not develop the ability to read novel, non‐taught words, which is a critical component of literacy acquisition.
Phonics‐based approach
Due to the limitations of a sight word approach, several researchers have begun to explore phonics‐based approaches to reading interventions for people with intellectual disability (Allor 2010; Browder 2012; Lemons 2010). These approaches focus on teaching students to identify and manipulate phonemes in spoken language and to connect these with printed graphemes. Two core components include: phonologic awareness and phonics. Phonologic awareness is the ability to hear and manipulate sounds in spoken language (Carnine 2010). The continuum of skills included under the broader category includes the ability to identify rhyme and alliteration; to segment a spoken sentence into words; to blend and segment syllables; to manipulate onset and rime; and to segment, blend, and manipulate individual phonemes in words. Phonics involves teaching students to make connections between the sounds in spoken language and the letters used to represent the sounds in print (Hougen 2012). Instruction involves teaching students letter sounds, decoding (converting print to spoken language), and encoding (converting spoken language into print).
Perfetti 1998 explained how learning a writing system occurs across different languages. They specify that, for alphabetic languages (e.g. English, Italian, Russian), the key principle to be learned is the alphabetic principle – an understanding of the association of meaningless printed units (i.e. letters or graphemes) to meaningless units of the spoken language (individual sounds or phonemes). In modified alphabetic languages (e.g. Hebrew, Egyptian), print is used to represent consonants, but not often vowels. Perfetti and Marron further explain how the process is similar for almost all languages, with some variation in the 'size' of the spoken language unit; that is, associated with the printed graphic. For example, Japanese relies on the syllabic principle whereby graphic units are associated with spoken syllables; Chinese is based on a morphologic principle in which the written units encode morphemes. (Chinese is additionally complex in that graphic symbols also encode syllables, thus identifying it as morphosyllabic language may be more appropriate; see Perfetti 1998; Perfetti 2003.) Regardless of language, the critical aspect of learning to read is to recognize that written language represents speech, and to understand the relationship between the two.
Phonics‐based approaches to teaching children to read in English are supported by three decades of research (Adams 1990; National Reading Panel 2000; Snow 1998). Due to strong empirical support, this type of reading instruction is mandated in Australia (Rowe 2005), the UK (Rose 2009), and the USA (No Child Left Behind Act of 2001). However, people with intellectual disability were predominately excluded from empirical evaluations of phonics‐based approaches. Further, one meta‐analysis evaluating phonics instruction for English‐speaking poor readers was unable to draw conclusions about the efficacy of phonics instruction for people with intellectual disability due to the limited number of people with intellectual disability included in the reviewed studies (McArthur 2018). Thus, it remains unclear how effective phonics‐based approaches are for people with intellectual disability.
Syntheses on reading instruction for people with intellectual disability
Browder and colleagues have completed the most recent systematic review on teaching people with intellectual disability to read in English (Browder 2006). The authors identified 128 studies (88 were single‐subject design; 40 were group design) involving 1123 participants. Studies predominantly targeted acquisition of functional sight words; fewer examined phonologic awareness (five) or phonics instruction (13). Following an evaluation of study quality based on previously published indicators (Gersten 2005; Horner 2005), the reviewers concluded that the evidence base supports the teaching of sight words using systematic prompting techniques in a repeated trial format. The reviewers were unable to identify a sufficient number of high‐quality studies to verify other evidence‐based approaches for teaching reading to students with intellectual disability (e.g. phonologic awareness, phonics). In the most recently published systematic review focused on phonics‐based approaches for people with intellectual disability, the reviewers identified seven studies (two were single‐subject design; one was a randomized, post‐test‐only design; four were non‐randomized design; Joseph 2004). Findings from the studies indicated that students with intellectual disability were able to benefit from phonics‐based instruction. However, many of the studies were focused on limited aspects of phonics (e.g. classifying letters as consonants or vowels) and the reviewers did not evaluate studies for risk of bias of experimental design.
How the intervention might work
We presume that interventions focused on the targeted components of reading will work in much the same manner for students with intellectual disabilities as they do for students who are typically developing. Instruction assists learners in 1. understanding that spoken language consists of units (e.g. words, syllables, and phonemes) that can be broken apart and manipulated, and 2. associating these spoken units with the graphic units used to represent them in speech. A student is most often first exposed to a new skill (e.g. learning the sound of the letter 't') with a model by an instructor. The instructor then provides multiple opportunities for the student to practice the skill while receiving immediate, corrective feedback. Instructor support or scaffolding is purposefully decreased until the student is able to perform the task independently. Then, the student is provided with multiple opportunities to practice the skill independently and to work on improving automaticity or fluency. Various instructional strategies have been demonstrated to be effective in accomplishing these learning objectives (direct, explicit instruction (Allor 2010); systematic prompting and fading (Browder 2006)). Further, emergent language skills, which are often delayed in people with intellectual disability, are highly predictive of response to beginning reading intervention for people with (Steele 2013) and without intellectual disability (Scarborough 1990). Thus, as proposed by Burgoyne 2009, interventions that incorporate an oral language component may be more effective at increasing beginning reading skills than interventions that do not.
We expect that the rate of learning may be slower for students with intellectual disability compared to other types of learners and that instruction may need to be provided for a longer period of time (e.g. multiple school years) or at a greater level of intensity (e.g. one‐on‐one instruction, additional minutes per week), or both. We also believe that several important features may moderate learning. First, as demonstrated in previous studies (Snell 2009), we expect student outcomes to be associated with severity of impairment. Higher IQ scores will likely be associated with better intervention effects. Second, as learning to read involves developing an understanding of how spoken language is represented in print, we would hypothesize that response to reading intervention will be influenced by language skills (e.g. receptive vocabulary). Third, type of instruction (sight word, phonics) may influence outcomes. Studies that focus on acquisition of functional sight words will likely demonstrate stronger effects in sight word learning, whereas interventions targeting phonics skills (e.g. letter sound knowledge) would be presumed to have stronger effects on targeted skills. Fourth, increases in the intensity of intervention (e.g. frequency, duration, group size) would be hypothesized to be associated with greater outcomes (Vaughn 2012). Fifth, variations in environment may moderate treatment effects. We aim to code for and, if possible, examine moderator effects for, educational setting of the study (e.g. special school, general education setting) and education quality of the country in which the study was conducted as indexed by the United Nation's Education Index (United Nations Development Programme 2013). Sixth, differences in language (alphabetic versus syllabic; opaque versus transparent) may moderate outcomes. Previous work has demonstrated for typically developing children that learning to read is easier in alphabetic languages that are more transparent (i.e. consistent sound‐symbol correspondences; e.g. Finnish, Hungarian) compared to languages that are more opaque (i.e. less consistency between sound‐symbol correspondences; e.g. French, English) (Ellis 2004; Ziegler 2010). We hypothesize that people with intellectual disability may also have more success in learning to read when their language is more transparent.
Why it is important to do this review
Historically, many educators assumed that people with intellectual disability were not capable of learning to read; thus, reading instruction was not considered appropriate (Katims 2000). However, across a number of countries (e.g. Australia, the UK, and the USA), societal expectations for people with intellectual disability have drastically changed in the last 20 years and schools are now expected to teach academic content (e.g. reading, mathematics, science) to students with intellectual disability (Browder 2009).
Previous reviews were limited to English language instruction and conducted more than 10 years ago (Browder 1998; Browder 2006; Joseph 2004). Our aim was to conduct a more comprehensive, up‐to‐date synthesis by examining the effectiveness of beginning reading interventions across languages and instructional methods. This review will allow us to explore the effects of various types of reading interventions and may allow us to examine important moderating factors that may affect student outcomes, including severity of impairment, method of instruction, intensity of instruction, or characteristics of the spoken language.
Our focus included beginning reading interventions. We included studies in which interventions targeted one or more elements of reading instruction, including 1. phonologic awareness, 2. letter‐sound or grapheme‐phoneme correspondences, 3. decoding or phonics, 4. encoding or spelling, or 5. reading of words or connected text, was targeted by the intervention, and was included as a dependent variable. There are no exclusionary criteria related to intervention language or instructional method (e.g. sight word, phonics, other).
Objectives
To assess the effectiveness of interventions for teaching beginning reading skills to children and adolescents with intellectual disability.
Methods
Criteria for considering studies for this review
Types of studies
Randomized controlled trials (RCTs), including trials that used quasi‐random methods of allocation (e.g. day of week, date of birth, case number presentation).
Types of participants
Children and adolescents aged 4 to 21 years with intellectual disabilities, defined as an IQ two SDs or more below the population mean, irrespective of language. When a specific IQ was not provided but a descriptive term was used, we accepted studies that described the sample as having 'intellectual disability' or 'mental retardation', which are the two most common terms used to refer to intellectual disabilities, according to the WHO Intellectual Disability Atlas (WHO 2007).
Types of interventions
Literacy interventions, irrespective of instructional method (e.g. sight word, phonics, other), comprising one or more elements of reading acquisition, including:
phonologic awareness;
letter‐sound or grapheme‐phoneme correspondences;
decoding or phonics;
encoding or spelling;
sight word learning;
word recognition;
storybook reading; and
text reading.
Control interventions: no treatment control; wait‐list control; treatment as usual (TAU); attention control; or alternate, non‐reading instruction control (e.g. mathematics instruction).
We excluded other treatment control designs; that is, where only two reading interventions were compared one to another.
Types of outcome measures
Primary outcomes
Phonologic awareness (e.g. ability to blend individual phonemes into a word), measured by standardized measures such as the Comprehensive Test of Phonological Processing (CTOPP; Wagner 1999) or Test of Phonological Awareness (TOPA; Torgesen 1994).
Sound‐symbol correspondence (e.g. ability to produce phonemes correctly when presented with isolated graphemes).
Word reading (e.g. ability to pronounce a written word correctly), measured by assessments of reading efficiency such as the Sight Word Efficiency subscale of the Test of One Word Reading Efficiency (TOWRE; Torgesen 1999) or the Word Identification subscale of the Woodcock Reading Mastery Test (WRMT; Woodcock 1987).
Decoding (e.g. ability to use sound‐symbol knowledge to decode novel words or pseudo‐words), measured by assessments of reading efficiency such as the Phonemic Decoding Efficiency subscale of the TOWRE (Torgesen 1999), or the Word Attack subscale of the WRMT (Woodcock 1987); or curriculum‐based measures of non‐word reading fluency (NWF) such as Dynamic Indicators of Basic Early Literacy Skills (DIBELS; Good 2002).
Adverse events (e.g. problem behavior, social stigmatism).
Secondary outcomes
Supplemental measures of literacy, including vocabulary, comprehension, spelling, writing, oral reading fluency, or a combination of these.
Supplemental measures of language skills, treatment acceptability, attitudes towards reading, self‐efficacy related to reading, and behavioral outcomes, if reported.
Outcomes could have been measured using standardized assessments, qualitative data (e.g. social validity), parent or teacher rating scales (or both), and behavioral observation. Table 6 shows the measures used for each outcome by study.
1. Summary of outcome assessments used by outcome for each study.
| Study | Phonologicawarenessa | Word reading | Decoding | Language/vocabulary skills | Oral reading fluencya |
| Ahlgrim‐Delzell 2016 | Phonemic identification; blending sounds | Not measured | Decoding | Not measured | Not measured |
| Allor 2014 | CTOPP: Blending Words; CTOPP: Blending Non‐words; CTOPP: Segmenting Words; DIBELS‐PSF | TOWRE: Sight Word Efficiency subscale | TOWRE: Phonemic Decoding Efficiency subscale; DIBELS‐NWF | EVT; PPVT: Receptive subscale | DIBELS‐ORF |
| Browder 2012 | Not measured | Not measured | Not measured | PPVT: Receptive subscale | Not measured |
| Burgoyne 2012 | Phoneme blending | EWR: Single Word Reading subscale | Non‐word reading | EOWPVT: Expressive Vocabulary; ROWPVT: Receptive Vocabulary | Not measured |
| Cleave 2011 | Rhyme task; TOPA: initial; TOPA: final | WRMT: Word Identification subscale | WRMT: Word Attack subscale | Not measured | Not measured |
| Finnegan 2011 | Not measured | Not measured | WJ‐III: Word Attack subscale; Training word identification; Transfer word identification | Not measured | Not measured |
| Roberts‐Tyler 2019 | Not measured | WRaPS | Not measured | Not measured | DIBELS‐ORF; DRA |
aWhen more than one measure was reported for a single outcome, the effect size estimate used in the meta‐analysis represents an averaged effect size estimate across all reported measures that were functionally equivalent.
CTOPP: Comprehensive Test of Phonological Processing (Wagner 1999); DIBELS‐NWF: Dynamic Indicators of Basic Early Literacy Skills: Nonsense Word Fluency (Good 2002); DIBELS‐ORF: Dynamic Indicators of Basic Early Literacy Skills: Oral Reading Fluency (Good 2002); DIBELS‐PSF: Dynamic Indicators of Basic Early Literacy Skills: Phoneme Segmentation Fluency (Good 2002); DRA: Diagnostic Reading Analysis (Crumpler 2007); EOWPVT: Expressive One‐word Picture Vocabulary Test (Brownell 2000); EVT: Expressive Vocabulary Test (Williams 1997); EWR: Early Word Recognition (Hulme 2009); PPVT: Peabody Picture Vocabulary Test (Dunn 1997); ROWPVT: Receptive One‐word Picture Vocabulary Test (Brownell 2000); TOPA: Test of Phonological Awareness (Torgesen 1994); TOWRE: Test of One Word Reading Efficiency (Torgesen 1999); WRaPS: Word Recognition and Phonic Skills Assessment (Carver 1994); WJ‐III: Woodcock‐Johnson III: Diagnostic Reading Battery (Shrank 2004); WRMT: Woodcock Reading Mastery Test (Woodcock 1987).
We only located data for the time point immediately after intervention. Had we located follow‐up data, we would have handled these data as described in Table 7.
2. Additional methods that were not used.
| Analysis | Description of method | Reason not used |
| Time point of outcome measurement | We had intended to group outcome time points as follows: immediately postintervention; 1–5 months' postintervention; 6–11 months' postintervention; 12–23 months' postintervention; 24–35 months' postintervention; and so on. | We did not locate any follow‐up data. |
| Measurement of treatment effect |
Continuous data Had outcomes been measured on a consistent scale across studies, we would have calculated the effect of each study using the MD, and presented it with 95% CI. |
Outcomes were not reported on a consistent scale across studies, so we chose to use the SMD. |
|
Dichotomous data Had we located dichotomous data, we would have calculated an odds ratio with 95% CI for each outcome in each trial (Deeks 2011). |
We did not locate dichotomous data. | |
| Unit of analysis |
Cluster‐randomized trials Had we located cluster‐randomized trials, we would have adhered to the advice provided on statistical methods for cluster‐randomized trials in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b). If trialists had failed to adequately control for the clustering effect in their analyses, we would have requested individual participant data to calculate an estimate of the ICC. If these data were not available, or could not be obtained, we would have identified external estimates of the ICC from similar studies or other resources. Having established an appropriate ICC, we would have reanalyzed the data in Review Manager 2014, to calculate effect sizes and CI using the generic inverse variance method (Higgins 2011b). If insufficient information was available to control for clustering in this way, we would have entered the data into Review Manager 2014 using participants as the unit of analyses, and performed sensitivity analyses to assess the potential bias that may have occurred as a result of the inadequately controlled clustered trials. We would also have performed sensitivity analyses if we had obtained the ICCs from external sources. Cross‐over trials In the event that we had located cross‐over trials, we would have combined the results of the cross‐over trials with the results of the parallel‐group trials. If data from a cross‐over trial were restricted or could not be obtained from the authors, we would have used the presented data within the first phase up to the point of cross‐over, and pooled data from cross‐over trials according to the methods described by Higgins 2011b and Elbourne 2002. Multiple treatment groups If a study had compared 2 types of reading interventions and a third group not receiving treatment, we would have first confirmed that each intervention individually would have met the inclusion criteria. Had we located studies of multiple treatment group, we would have determined whether the 2 intervention groups received equivalent or different treatments. If the groups received equivalent treatments, we would have combined the data from the 2 treatment groups to form 1 pair‐wise comparison with the control group. If the study contained groups receiving different interventions, we would have formed 2 pair‐wise comparisons by splitting the sample size of the control group and comparing each intervention group separately with the reduced sample control (Higgins 2011b). |
We did not locate any cluster‐randomized trials, cross‐over trials, or trials with multiple treatment groups. |
| Assessment of reporting bias | If we had identified ≥ 10 studies reporting the same outcome, we would have drawn funnel plots (estimated differences in treatment effects against their standard error). Asymmetry could be due to publication bias, but could also be due to a real relation between trial and effect size, such as when larger trials have lower compliance and compliance is positively related to effect size (Sterne 2011). If such a relation was found, we would have examined clinical variation between the studies (Sterne 2011, Section 10.4). As a direct test for publication bias, we would have conducted sensitivity analyses to compare the results from published data with data from other sources. | We did not locate sufficient studies (10) to assess reporting bias. |
| Subgroup analyses | If we had located enough studies, we would have explored moderator effects for chronologic age, level of severity of intellectual disability, language skills, and intervention density (e.g. session duration, session frequency, intervention duration). We may also have conducted further investigation of the causes of heterogeneity using subgroup analyses. Possible subgroups that we might have examined, if present, were: intervention setting and type of trial (e.g. parallel or cross‐over). | We did not conduct subgroup analyses due to the small number of included trials. |
| Sensitivity analyses | To explore the impact of studies with high risk of bias on the robustness of the results of the review, we would have conducted sensitivity analyses by removing studies with a high risk of bias (e.g. sequence generation, incomplete outcome data, blinding of outcome assessment), and reanalyzing the remaining studies to determine whether these factors affected the results. Also, we would have reanalyzed the data using different statistical approaches (e.g. using a fixed‐effect instead of a random‐effects model), to explore the impact of our choice of effect model (Higgins 2011b). Had we included RCTs and quasi‐RCTs together in a synthesis, we would have explored the impact through sensitivity analyses, by removing the quasi‐RCTs. Moreover, we would have examined the influence of different procedural decisions that we had taken (e.g. use of different dependent variables, exclusion of outlying studies) through sensitivity analyses, to determine the impact of the decisions on the overall results. | We did not conduct sensitivity analyses due to the small number of included trials. |
CI: confidence interval; ICC: intracluster correlation coefficient; IQ: intelligence quotient; MD: mean difference; SMD: standardized mean difference.
We reported the primary and secondary outcomes in 'the Summary of findings' tables (see Table 1; Table 2; Table 3; Table 4; Table 5).
Summary of findings for the main comparison. Beginning reading interventions for phonologic awareness in children and adolescents with intellectual disability.
| Beginning reading interventions for phonologic awareness in children and adolescents with intellectual disability | ||||||
| Patient or population: children and adolescents with intellectual disability Settings: schools Intervention: beginning reading interventions Control: treatment as usual | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Beginning reading interventions | |||||
|
Phonologic awareness
Measured with: standardized measures of phonologic awareness Assessed at: immediately postintervention |
— | The mean phonologic awareness score in the intervention group was 0.55 standard deviations higher (0.23 to 0.86 higher) | — | 178 (4 studies) | ⊕⊕⊕⊝ Moderatea | An effect size of 0.55 is considered to be a medium effect size. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
aDowngraded one level due to low number of studies with small samples sizes (largest trial contributing data for this outcome had 76 participants) and wide CIs around point estimates of study effects.
Summary of findings 2. Beginning reading interventions for word reading in children and adolescents with intellectual disability.
| Beginning reading interventions for word reading in children and adolescents with intellectual disability | ||||||
| Patient or population: children and adolescents with intellectual disability Settings: schools Intervention: beginning reading interventions Control: treatment as usual | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Beginning reading interventions | |||||
|
Word reading
Measured with: standardized and researcher‐created measures of sight word reading Assessed at: immediately postintervention |
— | The mean word reading score in the intervention group was 0.54 standard deviations higher (0.05 to 1.03 higher) | — | 220 (5 studies) | ⊕⊕⊕⊝ Moderatea | An effect size of 0.54 is considered to be a medium effect size. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
aDowngraded one level due to low number of studies with small samples sizes (largest trial contributing data for this outcome had 76 participants) and wide CIs around point estimates of study effects.
Summary of findings 3. Beginning reading interventions for decoding in children and adolescents with intellectual disability.
| Beginning reading interventions for decoding in children and adolescents with intellectual disability | ||||||
| Patient or population: children and adolescents with intellectual disability Settings: schools Intervention: beginning reading interventions Control: treatment as usual | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Beginning reading interventions | |||||
|
Decoding
Measured with: standardized and researcher‐created measures of nonsense word decoding Assessed at: immediately postintervention |
— | The mean decoding score in the intervention groups was 0.40 standard deviations higher (0.12 to 0.67 higher) | — | 230 (5 studies) | ⊕⊕⊝⊝ Lowa,b | An effect size of 0.40 is considered to be a medium‐to‐small effect size. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
aDowngraded one level due to wide range of point estimate of study effects. bDowngraded one level due to low number of studies with small samples sizes (largest trial contributing data for this outcome had 76 participants) and wide CIs around point estimates of study effects.
Summary of findings 4. Beginning reading interventions for oral reading fluency in children and adolescents with intellectual disabilities.
| Beginning reading interventions for oral reading fluency in children and adolescents with intellectual disabilities | ||||||
| Patient or population: children and adolescents with intellectual disabilities Settings: schools Intervention: beginning reading interventions Control: treatment as usual | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Beginning reading interventions | |||||
|
Oral reading fluency
Measured with: standardized measures of oral reading fluency Assessed at: immediately postintervention |
— | The mean oral reading fluency in the intervention groups was 0.65 standard deviations higher (0.12 lower to 1.42 higher) | — | 84 (2 studies) | ⊕⊕⊝⊝ Lowa,b | An effect size of 0.65 is considered to be a medium effect size. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
aDowngraded one level due to wide range of point estimate of study effects. bDowngraded one level due to low number of studies with small samples sizes (largest trial contributing data for this outcome had 62 participants) and wide CI around point estimates of study effects.
Summary of findings 5. Supplemental measures of language skills in children and adolescents with intellectual disability.
| Supplemental measures of language skills in children and adolescents with intellectual disability | ||||||
| Patient or population: children and adolescents with intellectual disability Settings: schools Intervention: supplemental measures of language skills Control: treatment as usual | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Supplemental measures of language skills | |||||
|
Expressive and receptive language
Measured with: standardized assessments of expressive and receptive language Assessed at: immediately postintervention |
— | The mean expressive and receptive language scores in the intervention groups was 0.28 standard deviations higher (0.03 to 0.54 higher) | — | 222 (3 studies) | ⊕⊕⊕⊝ Moderatea | An effect size of 0.28 is considered to be a small effect size. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
aDowngraded one level due to low number of studies with small samples sizes (largest trial contributing data for this outcome had 92 participants) and wide CIs around point estimates of study effects.
Search methods for identification of studies
We used a sensitive search strategy to reduce the risk of missing any potential studies. We did not limit the search by date or language, and we did not use a study methods filter.
Electronic searches
In April 2015, we searched all available years of the electronic databases and trial registers listed below, without using date limits or language restrictions. We updated our searches in November 2016, October 2017, August 2018, and October 2019. The search strategies for each database are shown in Appendix 1.
Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 10), in the Cochrane Library, and which includes the Cochrane Developmental, Psychosocial and Learning Problems Specialized Register (searched 3 October 2019).
MEDLINE Ovid (1946 to September week 3 2019).
MEDLINE Epub Ahead of Print (searched 2 October 2019).
MEDLINE In‐Process & Other Non‐Indexed Citations Ovid (searched 2 October 2019).
Embase Ovid (1974 to 1 October 2019).
CINAHLPlus EBSCOhost (Cumulative Index to Nursing and Allied Health Literature; 1973 to 2 October 2019).
PsycINFO Ovid (1967 to September week 2 2019).
ERIC EBSCOhost (Education Resources Information Center; 1966 to 2 October 2019).
British Education Index EBSCOhost (BEI; searched 2 October 2019).
Science Citation Index Web of Science (SCI; 1970 to 1 October 2019).
Social Science Citation Index Web of Science (SSCI; 1970 to 1 October 2019).
Conference Proceedings Citation Index – Science Web of Science (CPCI‐S; 1970 to 1 October 2019).
Conference Proceedings Citation Index – Social Sciences & Humanities Web of Science (CPCI‐SS&H; 1970 to 1 October 2019).
Cochrane Database of Systematic Reviews (CDSR; 2019 Issue 10), part of the Cochrane Library (searched 2 October 2019)
Database of Abstracts of Reviews of Effects (DARE; 2015 Issue 2; final issue), in the Cochrane Library (searched 9 November 2016) .
EPPI‐Centre Database of Education Research (eppi.ioe.ac.uk/webdatabases; searched 11 October 2019).
OpenGrey (opengrey.eu; searched 11 October 2019).
National Technical Information Service (NTIS; ntis.gov; searched 11 October 2019).
ClinicalTrials.gov (clinicaltrials.gov; searched 11 October 2019).
ICTRP (who.int/ictrp/en; searched 3 October 2019).
Searching other resources
We checked the reference lists of relevant publications to find additional studies that may have been missed by the electronic searches. We contacted the authors of eligible studies to ask if they knew of other relevant unpublished or ongoing trials. In addition, we used Google Scholar to search for papers that cited relevant studies, as well as searching for papers on similar topics by the authors of our included studies.
Data collection and analysis
Selection of studies
Two review authors (BR and DM) independently screened the titles and abstracts yielded by the search against the inclusion criteria listed above (Criteria for considering studies for this review). These authors retrieved and assessed the full texts of any reports about which there was uncertainty. We sought additional information from study authors, as necessary, to resolve questions about the relevance or methodology of a study. We resolved disagreements about eligibility through discussion and, when disagreements could not be resolved, we sought advice from a mediator (CL). We recorded the reasons for excluding trials. Neither review author was blind to the journal titles or to the study authors and institutions. We recorded our decisions in a study flow diagram (Moher 2009).
Data extraction and management
Two review authors (DH and CL) independently extracted data from each trial using a data extraction form that was piloted using paper and pencil extraction and then transferred to REDCap. We collected information about the population, interventions, randomization methods, blinding, sample size, outcome measures, follow‐up duration, attrition and handling of missing data, and methods of analysis. When data were missing, one review author (CL) contacted the study authors to request additional information. If further information could not be obtained, we coded the variables in question as 'missing'. We resolved disagreements through consensus between the two data extractors.
Assessment of risk of bias in included studies
Two review authors (CL and DH) independently assessed the risk of bias of each included trial using Cochrane's 'Risk of bias' tool (Higgins 2011a). We resolved any disagreements by discussion; no third party (BR) was needed to resolve disagreements.
We present the 'Risk of bias' assessments in 'Risk of bias' tables, where we provide our judgment (low, high, or unclear risk of bias) and, in a separate text box, details on the available information that led to each judgment.
We assessed the following sources of bias: sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective outcome reporting; and any other potential sources of bias.
See Table 8 for descriptions of the criteria we used to reach our judgments on risk of bias.
3. Assessment of risk of bias.
| Risk of bias item | Questions | Criteria for assigning 'Risk of bias' judgments |
| Sequence generation | Was the sequence generation method used adequate? | We judged the risk of bias as follows:
|
| Allocation concealment | Was allocation adequately concealed? | We judged the risk of bias as follows:
|
| Blinding of participants and personnel | Were participants and personnel blind to which participants were in the treatment group? | We judged the risk of bias as follows:
|
| Blinding of outcome assessment | Were outcome assessors blind to which participants were in the treatment group? | We judged the risk of bias as follows:
|
| Incomplete outcome data | Did the trial authors deal adequately with missing data? | We judged the risk of bias as follows:
|
| Selective outcome reporting | Did the authors of the trial omit to report on any of their outcomes? | We judged the risk of bias as follows:
|
| Other potential sources of bias | Were any other bias' present in the trial, such as changing methods during the trial, or other anomalies? | We judged the risk of bias as follows:
|
Measures of treatment effect
Dichotomous data
We found no studies that included dichotomous data. See our protocol, Reichow 2014, and Table 7 for methods that we would have used to handle dichotomous data.
Continuous data
We analyzed continuous data when means and SDs were presented in the study papers, were made available by the authors of the trials, or were calculable from the available data. No study reported individual data, so we were unable to analyze the data to see if they were skewed and to correct them according to the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011). Where similar outcomes were measured using different scales, we calculated a standardized mean difference (SMD) using Hedges g with small sample correction (Hedges 1985), and presented this with 95% confidence intervals (CI).
Multiple outcomes
When a study included two or more functionally equivalent measures, we estimated a mean effect size (ES) using the formula provided by Borenstein and colleagues, for combining multiple outcomes or time points within a study (Borenstein 2009).
Unit of analysis issues
We found no cluster‐randomized trials or studies with multiple treatment groups. See our protocol, Reichow 2014, and Table 7 for methods that we will use to handle these studies should we find them in updates of this review.
Dealing with missing data
For studies in which missing data were not available, we conducted analyses using only the available data; that is, we did not impute missing data. If a greater number of studies were located, allowing us to conduct sensitivity analyses, we would have considered the extent to which missing data may have impacted the results of the review and assessed the sensitivity of any primary meta‐analysis to missing data using the strategy recommended by Higgins and colleagues (Higgins 2011b).
Assessment of heterogeneity
We assessed clinical variation across studies (e.g. participant factors, curricula used in trial, outcome assessment) and trial factors (e.g. randomization concealment, type of intervention, type of comparison group). We examined heterogeneity among included studies through the use of the Chi2 test, where a low P value indicates heterogeneity of treatment effects. We also used the I2 statistic to determine the percentage of variability that was due to heterogeneity rather than sampling error or chance (Higgins 2002). We examined estimates of the between studies' variance components using Tau2. Had data permitted, we would have conducted subgroup analyses and sensitivity analyses (see Reichow 2014 and Table 7).
Assessment of reporting biases
We did not assess reporting bias as we did not include 10 or more studies. See our protocol, Reichow 2014, and Table 7 for further details of analyses that we will use if we locate an adequate number of studies in updates of this review.
Data synthesis
The primary analyses focused on the effectiveness of beginning reading interventions for children and adolescents with intellectual disability. We combined the means of the studies by conducting a meta‐analysis using a random‐effects model, which assumes that the variability across studies represents factors that are beyond participant‐level sampling error alone, with inverse variance weighting. We used a random‐effects model because studies had several differences related to the samples (e.g. IQ level, etiology, age), settings (e.g. country effects, educational environment), and interventions (e.g. duration, length, intensity), which may not be readily reported in the studies.
'Summary of findings' tables
We created a 'Summary of findings' table per comparison using GRADEprofiler GDT software (GRADEpro GDT). We created three 'Summary of findings' tables for the primary outcomes of phonologic awareness, word reading and decoding, and two 'Summary of findings' table for the secondary outcomes of oral reading fluency and language skills, at postintervention.
Two review authors (CL and DH) independently assessed the quality of the evidence for these outcomes as high, moderate, low or very low, using the criteria outlined by the GRADE approach: limitations in the design and implementation of available of studies; indirectness; inconsistency; imprecision; and publication bias (Schünemann 2011). We reported these quality ratings in the 'Summary of findings' tables. We resolved disagreements by discussion and reached consensus; a third party was not needed to resolve any remaining disagreements.
Subgroup analysis and investigation of heterogeneity
We planned to conduct further investigations of the causes of methodologic and clinical heterogeneity using subgroup analyses. However, due to the small number of included studies, we decided that such analyses were not appropriate. See our protocol, Reichow 2014, and Table 7 for further details and examples of analyses that we will conduct should we locate more studies in updates of this review.
Sensitivity analysis
We only located a small number of studies, so we deemed sensitivity analyses inappropriate. Our protocol, Reichow 2014, and Table 7 provide further details and examples of analyses that we will conduct should we locate more studies in updates of this review.
Results
Description of studies
Results of the search
Figure 1 shows a flow diagram of our search results. The electronic searches conducted between April 2015 and October 2019 returned 13,687 records (13,203 records from Electronic searches and 484 records from Searching other resources); 6813 records remained after deduplication. Initial screening on title and abstract reduced the number to 136 potential reports. We retrieved and evaluated the full texts of 132 reports and identified seven studies (from 12 reports) as suitable for inclusion. We excluded 120 irrelevant reports (see Excluded studies). Even after utilizing interlibrary loan, we were unable to locate the remaining four reports, which are awaiting classification (Hughes 1982; Hughes 1984; Muter 1976; Salario 1960). We contacted the authors of all included studies; no author indicated having knowledge of any additional studies. See Figure 1.
1.

Study flow diagram.
Included studies
The review included seven studies examining beginning reading interventions for children and adolescents with intellectual disability (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Burgoyne 2012; Cleave 2011; Finnegan 2011; Roberts‐Tyler 2019).
Study location
Four studies were conducted in the USA (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Finnegan 2011). The remaining three studies were conducted in Canada (Cleave 2011) and the UK (Burgoyne 2012; Roberts‐Tyler 2019).
Study design
All studies were conducted using an RCT design that compared the treatment condition to a group receiving treatment‐as‐usual (TAU) reading instruction.
Participants
The seven studies included 352 participants with intellectual disability; 195 participants in the beginning reading intervention groups and 157 participants in the comparison group. Five of the seven studies reported mean chronologic ages at treatment entry (Allor 2014; Burgoyne 2012; Cleave 2011; Finnegan 2011; Roberts‐Tyler 2019); the mean age was 9.5 years (SD 2.7), with a range of 5.5 years to 18 years. The remaining two studies reported age as a categorical variable (Ahlgrim‐Delzell 2016; Browder 2012). Four of the studies provided age by treatment and control (Burgoyne 2012; Cleave 2011; Finnegan 2011; Roberts‐Tyler 2019). From these studies, the mean age of students in treatment groups was 9.98 years (SD 2.82) with a range of 5.5 years to 18 years. The mean age of students in control groups was 9.59 years (SD 2.81) with a range of 6.5 years to 18.7 years.
Five of the seven studies reported mean IQ (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Cleave 2011; Finnegan 2011). The mean IQ score across samples was 51.6 (SD 11.6), with a range of 42.5 to 57.1. Four studies reported IQ by treatment and control group (Ahlgrim‐Delzell 2016; Browder 2012; Cleave 2011; Finnegan 2011). The mean IQ score for the treatment groups was 49.47 (SD 11.19), with a range of 43.5 to 55.9. The mean IQ score for the control groups was 51.12 (SD 13.6) with a range of 41.5 to 56.2.
Six of seven studies reported the percentage of males and females in the samples. The mean proportion of males across the studies was 58% with a range of 41% to 74%. Two studies reported the percentage of males and females in intervention and control groups (Ahlgrim‐Delzell 2016; Browder 2012). In these studies, the proportion of males in the treatment group was 75% and the proportion of males in the control group was 59%.
Interventions
The duration of the beginning reading interventions ranged from 4 weeks (Finnegan 2011) to 100 weeks (Allor 2014), with a median of 24 weeks (interquartile range 9). The study authors did not provide explanations for the respective intervention durations of each study.
The mean intensity of the intervention was 4 (SD 1.3) sessions per week (range 3 to 5 sessions), with each session having a mean duration of 27.14 minutes (SD 11.4). The mean total duration of intervention was 5027.3 minutes (SD 7880.4), with a range of 210 minutes to 22,671 minutes.
School staff delivered the intervention in five studies (certified teachers in three studies: Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; paraprofessionals in one study: Burgoyne 2012; and a combination of certified teachers and paraprofessionals in one study: Roberts‐Tyler 2019). The remaining two studies delivered the intervention using research personnel (Cleave 2011; Finnegan 2011). Six studies implemented the interventions individually with participants (Ahlgrim‐Delzell 2016; Browder 2012; Burgoyne 2012; Cleave 2011; Finnegan 2011; Roberts‐Tyler 2019); the remaining study implemented the interventions with small groups of participants (Allor 2014).
Six of seven studies described the intervention as a phonologic awareness intervention (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Burgoyne 2012; Cleave 2011; Roberts‐Tyler 2019). All seven studies included content on letter‐sound correspondence, six included phonologic awareness (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Burgoyne 2012; Cleave 2011; Roberts‐Tyler 2019), and five included decoding (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Finnegan 2011; Roberts‐Tyler 2019). Four studies included content on sight word reading and word recognition (Allor 2014; Browder 2012; Finnegan 2011; Roberts‐Tyler 2019), and three studies included content on storybook reading (Browder 2012; Burgoyne 2012; Roberts‐Tyler 2019). One study used computers to deliver the intervention content (Roberts‐Tyler 2019).
Comparisons
The comparison group in all seven studies was TAU, which consisted of children's typical reading instruction delivered by their school. Most studies did not describe the focus of this instruction. Allor 2014 provided additional detail regarding the TAU group. Most students received a TAU intervention that focused on overlapping skill (i.e. letter‐sound knowledge, decoding). Browder 2012 reported that students in the TAU group predominantly received instruction in a sight word intervention that focused on teaching words paired with pictures. The duration of TAU was similar to treatment. However, studies did not clearly indicate the number of minutes or sessions of instruction students in the TAU group received.
Outcomes
The meta‐analysis focused on five reading outcomes reported across the eligible studies: phonologic awareness; word reading; decoding; oral reading fluency; and language and vocabulary skills. Not all studies reported each outcome. Below, we summarized which studies measured which primary and secondary outcome and how.
Primary outcomes
Phonologic awareness
Four studies measured phonologic awareness. Ahlgrim‐Delzell 2016 used curriculum based measures (CBM) of phoneme identification, blending sounds, and decoding for picture‐word matching; Allor 2014 used the CTOPP blending words subscale, CTOPP blending non‐words subscale, the CTOPP segmenting words subscale, and the DIBELS phoneme segmentation fluency subscale; Cleave 2011 used the TOPA initial letter subscale and the TOPA final letter subscale; and Burgoyne 2012 used a phoneme blending task that matched words to pictures.
Word reading
Four studies measured word reading. Allor 2014 used the TOWRE with the sight word efficiency subscale; Burgoyne 2012 used the Early Word Recognition (EWR) single word reading subscale; Cleave 2011 used the WRMT word identification subscale; and Roberts‐Tyler 2019 used the Word Recognition and Phonic Skills Assessment (WRaPS).
Decoding
Four studies measured decoding. Allor 2014 used the TOWRE phonemic decoding subscale and the DIBELS nonsense word fluency subscale; Burgoyne 2012 used a non‐word reading task; Cleave 2011 used the WRMT word attack subscale; and Finnegan 2011 used the Woodcock Johnson 3rd edition word attack, training word identification, and transfer word identification subscales.
Secondary outcomes
Oral reading fluency
Two studies measured oral reading fluency; Allor 2014 used the DIBELS oral reading fluency subscale and Roberts‐Tyler 2019 used the DIBELS oral reading fluency subscale and the Diagnostic Reading Analysis (DRA).
Language and vocabulary skills
Three studies measured language and vocabulary skills. Allor 2014 used the Expressive Vocabulary Test (EVT) receptive vocabulary subscale and the Peabody Picture Vocabulary Test (PPVT) receptive vocabulary subscale; Browder 2012 used the PPVT with the receptive vocabulary subscale; and Burgoyne 2012 used the Expressive One‐Word Picture Vocabulary Test (EOWPVT) and the Receptive One‐Word Picture Vocabulary Test.
We contacted study authors for missing or additional data. We received missing or additional data from Allor 2014, Browder 2012, Cleave 2011, and Finnegan 2011. We did not receive the requested data from Burgoyne 2012.
Funding sources
Three studies were funded by grants from the US Department of Education, Institute of Education Sciences (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012). One study was funded by research grants from the Canadian Language and Literacy Research Network and the Nova Scotia Health Research Foundation (Cleave 2011). Three studies did not indicate the funding source of the study (Burgoyne 2012; Finnegan 2011; Roberts‐Tyler 2019).
Excluded studies
We examined 132 full‐text reports and excluded 120. We excluded 53 reports because they were not RCTs, 46 because the participants did not have an intellectual disability, 18 because they did not contain an intervention meeting our inclusion criteria (see Criteria for considering studies for this review), two studies because the control group received the intervention in a different format, and one because the participants were not between the ages of 4 and 21 years.
We describe select characteristics of two, key excluded studies in the Characteristics of excluded studies table: Alfassi 2009; and Van der Bijl 2006. We excluded Alfassi 2009 because the study did not contain an intervention for beginning reading skills and we excluded Van der Bijl 2006 because the study was not an RCT. We chose to report the details of these studies because they needed a third party to reconcile discrepant opinions on inclusion after full‐text screening.
Risk of bias in included studies
Figure 2 shows the graphical representation of risk of bias across studies and Figure 3 shows the 'Risk of bias' summary for each study.
2.

Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgments about each risk of bias item for each included study.
Allocation
Random sequence generation
We deemed three studies at low risk of bias for sequence generation due to explicit description of the methods used to randomize participants to conditions (Ahlgrim‐Delzell 2016; Allor 2014; Roberts‐Tyler 2019). We judged the remaining four studies at unclear risk of bias for lack of description regarding randomization procedures (Browder 2012; Burgoyne 2012; Cleave 2011; Finnegan 2011).
Allocation concealment
We deemed allocation concealment as low in one study because randomization occurred after consent was obtained (Roberts‐Tyler 2019). The remaining six studies did not describe allocation concealment, so we deemed them at unclear risk of bias (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Burgoyne 2012; Cleave 2011; Finnegan 2011).
Blinding
Blinding of participants and personnel (performance bias)
Due to the nature of the intervention where participants and study personnel are often interacting, blinding of participants and personnel cannot always be controlled. We considered two studies at high risk of bias for blinding of participants and personnel because there was no indication that teachers or students were blind to treatment condition (Browder 2012), or a researcher with knowledge of group assignment and research hypotheses delivered treatment (Finnegan 2011). We judged the remaining five studies at unclear risk of performance bias because it was unclear if students had knowledge of treatment conditions and it was unclear if teachers knew study hypotheses (Ahlgrim‐Delzell 2016; Allor 2014; Burgoyne 2012; Cleave 2011; Roberts‐Tyler 2019).
Blinding of outcome assessment (detection bias)
We judged one study, which specified that outcome assessors were blind to treatment status, at low risk of bias (Cleave 2011). We judged two studies at high risk of bias because a researcher with knowledge of group assignment and study hypotheses were involved in collection of all outcome assessments (Finnegan 2011) or were involved in a majority the collection of outcome assessments (Roberts‐Tyler 2019). We judged the remaining four studies at unclear risk of detection bias for lack of a description of blinding procedures that might have been used (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Burgoyne 2012).
Incomplete outcome data
We rated five studies at low risk of attrition bias (Ahlgrim‐Delzell 2016; Browder 2012; Burgoyne 2012; Cleave 2011; Roberts‐Tyler 2019). We judged two studies to have unclear risk of bias; one study reported attrition but it was unclear if the missing data were related to the true outcome (Allor 2014), and one study did not clearly report the number of students who began and completed the trial (Finnegan 2011).
Selective reporting
We judged six studies at low risk of bias for selective outcome reporting (Ahlgrim‐Delzell 2016; Allor 2014; Browder 2012; Burgoyne 2012; Cleave 2011; Roberts‐Tyler 2019). We judged one study at unclear risk because information was not provided in the study report confirming that all outcomes that were assessed were reported (Finnegan 20110).
Other potential sources of bias
We did not detect any additional sources of bias and rated all studies at low risk of bias on this domain.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5
Primary outcomes
We estimated a mean ES using the formula provided by Borenstein and colleagues, for combining multiple outcomes or time points within a study (Borenstein 2009) to estimate ESs for phonologic awareness for Ahlgrim‐Delzell 2016; phonologic awareness, decoding, and language skills for Allor 2014; language skills for Burgoyne 2012; phonologic awareness for Cleave 2011; and word reading for Finnegan 2011.
Phonologic awareness
Four studies reported phonologic awareness outcomes (Ahlgrim‐Delzell 2016; Allor 2014; Burgoyne 2012; Cleave 2011). Measures included both standardized and non‐standardized assessments. Standardized measures included phonologic awareness subtests of the CTOPP, DIBELS, and TOPA. Non‐standardized measures included researcher‐developed assessments of phonemic identification, blending sounds, and phoneme blending. We conducted a meta‐analysis of ESs for these four studies using a random‐effects model and small sample correction (Hedges 1985). The mean ES between intervention and control groups was SMD 0.55 (95% CI 0.23 to 0.86; P < 0.001; 178 participants; moderate‐quality evidence; Analysis 1.1; Table 1). Heterogeneity was low (Chi2 = 1.63, degrees of freedom (df) = 3, P = 0.65; I2 = 0%; Tau2 = 0.00). See Figure 4.
1.1. Analysis.

Comparison 1 Phonologic awareness, Outcome 1 Phonologic awareness.
4.

Forest plot of comparison: 1 Phonologic awareness, outcome: 1.1 Phonologic awareness.
Sound‐symbol correspondence
No study reported the effects of beginning reading interventions on sound‐symbol correspondence.
Word reading
Five studies reported word reading outcomes (Allor 2014; Burgoyne 2012; Cleave 2011; Finnegan 2011; Roberts‐Tyler 2019). Measures included both standardized and non‐standardized assessments. Standardized measures included word reading subtests of the TOWRE, WJMRT, and WRaPS. Non‐standardized measures included a researcher‐developed single word reading assessment. We conducted a meta‐analysis of ESs for these five studies using a random‐effects model and small sample correction (Hedges 1985). The mean ES between intervention and control groups was SMD 0.54 (95% CI 0.05 to 1.03; P = 0.03; 220 participants; moderate‐quality evidence; Analysis 2.1; Table 2). Heterogeneity was high (Chi2 = 12.54, df = 4, P = 0.01; I2 = 68%; Tau2 = 0.19). See Figure 5.
2.1. Analysis.

Comparison 2 Word reading, Outcome 1 Word reading.
5.

Forest plot of comparison: 2 Word reading, outcome: 2.1 Word reading.
Decoding
Five studies reported decoding reading outcomes (Ahlgrim‐Delzell 2016; Allor 2014; Burgoyne 2012; Cleave 2011; Finnegan 2011). Measures included both standardized and non‐standardized assessments. Standardized measures included decoding subtests of DIBELS, TOWRE, WRMT, and Woodcock‐Johnson III. Non‐standardized measures included a researcher‐developed decoding assessment and a non‐word reading measure. We conducted a meta‐analysis of ESs for these five studies using a random‐effects model and small sample correction (Hedges 1985). The mean ES between intervention and control groups was SMD 0.40 (95% CI 0.12 to 0.67; P= 0.005; 230 participants; low‐quality evidence; Analysis 3.1; Table 3). Heterogeneity was low (Chi2 = 4.52, df = 4, P = 0.34; I2 = 11%; Tau2 = 0.01). See Figure 6.
3.1. Analysis.

Comparison 3 Decoding, Outcome 1 Decoding.
6.

Forest plot of comparison: 3 Decoding, outcome: 3.1 Decoding.
Adverse events
No study reported adverse events as a result of any treatment.
Secondary outcomes
Supplemental measures of literacy
Two studies reported oral reading fluency (Allor 2014; Roberts‐Tyler 2019). Measures included standardized subtests of DIBELS and the DRA. We conducted a meta‐analysis of ESs for both studies using a random‐effects model and small sample correction (Hedges 1985). The mean ES between intervention and control groups was SMD 0.65 (95% CI –0.12 to 1.42; P= 0.10; 84 participants; low‐quality evidence; Analysis 4.1; Table 4). Heterogeneity was high (Chi2 = 2.41, df = 1, P = 0.12; I2 = 59%; Tau2 = 0.19).
4.1. Analysis.

Comparison 4 Supplemental measures of literacy, Outcome 1 Oral reading fluency.
Supplemental measures of language skills
Three studies reported language or vocabulary skills (Allor 2014; Browder 2012; Burgoyne 2012). Measures included both standardized and non‐standardized assessments. Standardized measures included vocabulary subtests of the EVT and PPVT. Non‐standardized measures included a researcher‐developed expressive and receptive vocabulary assessments. We conducted a meta‐analysis of the ESs for these three studies using a random‐effects model and small sample correction (Hedges 1985). The mean ES between intervention and control groups was SMD 0.28 (95% CI 0.03 to 0.54; P = 0.03; 222 participants; moderate‐quality evidence; Analysis 5.1; Table 5). Heterogeneity was low (Chi2 = 0.89, df = 2, P = 0.64; I2 = 0%; Tau2 = 0.00).
5.1. Analysis.
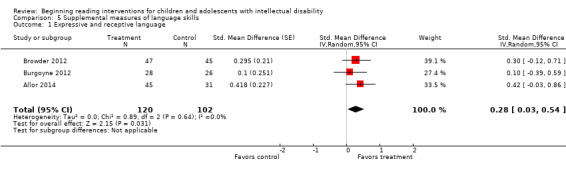
Comparison 5 Supplemental measures of language skills, Outcome 1 Expressive and receptive language.
Discussion
Summary of main results
From a search of 6831 unique records, we identified seven studies that met the inclusion criteria for this review (Criteria for considering studies for this review). Meta‐analyses of the data demonstrated small‐to‐moderate effects of reading interventions delivered to children and adolescents with intellectual disability across three primary outcomes (phonologic awareness: SMD ES 0.55; word reading: SMD ES 0.54; and decoding: SMD ES 0.40), and two secondary outcomes; oral reading fluency: SMD ES 0.65 and supplemental measures of language skills: SMD ES 0.28). There were insufficient data to evaluate effects on the other primary outcomes (sound‐symbol correspondence, adverse events). The limited number of identified studies precluded our examination of moderation effects of chronologic age, severity of impairment, language skills, intervention density (e.g. session duration, session frequency, intervention duration), intervention setting, and type of trial. As we did not locate enough studies to conduct moderator analyses, specific recommendations about which interventions work best for learners with specific characteristics could not be made. We rated the quality of the evidence as low to moderate using the GRADE system (Schünemann 2011). This, coupled with the limited number of identified studies, means that our findings could be influenced by additional research. Thus, caution is warranted in interpreting findings.
Overall completeness and applicability of evidence
The overall completeness of our review was reduced due to the low number of studies that met our inclusion criteria (Criteria for considering studies for this review). Data were available for meta‐analyses on only three of the five primary outcomes and one of the two secondary outcomes. Additionally, we were unable to estimate effects beyond immediate post‐test. In the small sample of included studies, interventions targeting phonologic awareness, word reading, and decoding were represented. Additional research evaluating interventions that target spelling and reading of connected text are needed. Interventions spanned a large range of durations, from four (Finnegan 2011) to 100 weeks (Allor 2014); however, the limited number of studies precluded our ability to evaluate outcomes related to intervention intensity. Regarding applicability of findings, all participants in the included studies were learning to read English. Additional research is necessary to evaluate beginning reading interventions in other languages. Further, the studies were conducted in Canada, the UK, and the USA. Additional research in other countries is warranted. The students in the included studies were primarily elementary‐aged students. Additional research exploring beginning reading intervention for preschool children, adolescents, and young adults is needed. Thus, our findings may not generalize to students who are learning to read in a language other than English, or to older adolescents or young adults with intellectual disability.
Quality of the evidence
Using the GRADE approach (Schünemann 2011), we rated the quality of the evidence as moderate for three outcomes (phonologic awareness, word reading, and supplemental measures of language skills; see Table 1, Table 2, and Table 5), and low for one outcome (decoding, see Table 3). The rating reflects our concerns with imprecision due to small sample sizes across all outcomes, which did not allow us to conduct robust moderator analyses. Given the high variability of the duration of interventions across studies (range 4 to 100 weeks, median 24 weeks), we conducted one exploratory moderator analysis by comparing the mean ESs with and without the study with a duration that was four times the median (Allor 2014); results of these analyses suggested that two outcomes (word reading, and expressive and receptive vocabulary) would no longer have a statistically significant mean ES if the Allor 2014 study was removed. We also had concerns with inconsistency for the decoding outcome due to inconsistent effects across studies. The risk of publication bias was unclear since it could not be assessed due to the small number of studies included in the review.
Potential biases in the review process
Many researchers who study reading interventions for children and adolescents with intellectual disability use experimental, single‐case research designs (Gast 2014). Had we included these types of designs, as did Browder and colleagues (Browder 2006), we would have identified additional studies and our conclusions may have been different. Additionally, we used reported means and SDs to estimate treatment effects. Our treatment estimates did not take into consideration covariates or other extraneous variables, and thus, our estimates may differ slightly from those reported by study authors who conducted more complex analyses.
Agreements and disagreements with other studies or reviews
Results from this review provide evidence that reading interventions for children and adolescents with intellectual disability are associated with small‐to‐moderate improvements in phonologic awareness, word reading, decoding, and expressive and receptive language. These findings are aligned with previously conducted meta‐analyses that examined the effects of reading interventions for people without intellectual disability (Scammacca 2015; Wanzek 2018).
The National Reading Panel 2000, which included peer‐reviewed studies conducted using experimental designs, quasi‐experimental design studies that included a control group, or multiple, baseline, single‐case designs, demonstrated moderate‐to‐large effects of reading interventions for children without disability. For example, phonologic awareness interventions led to improvements in phonemic awareness (SMD ES 0.86) and reading outcomes (SMD ES 0.53); phonics interventions were associated with gains in reading of regular (SMD ES 0.67) and nonsense (SMD ES 0.60) words. Effects were slightly reduced for children with identified reading disability in grades two through six. For this group of learners, the effects of phonologic awareness interventions were SMD ES 0.62 for phonemic awareness and 0.45 for reading outcomes; the effect of phonics interventions were SMD ES 0.49 for regular and 0.52 for nonsense word reading.
Findings are also in agreement with those of McArthur and colleagues (McArthur 2018). The McArthur 2018 review of phonics interventions for English‐speaking people without disabilities who had below average reading skills, included published and unpublished studies that allocated participants using randomization, minimization, or quasi‐randomized methods. The reviewers demonstrated statistically significant effects on word reading accuracy (SMD ES 0.47), non‐word reading accuracy (SMD ES 0.76), and letter sound knowledge (SMD ES 0.35). Suggate 2016 conducted a review of reading interventions delivered to school‐aged children and adolescents. This review, which included published and unpublished studies that utilized randomized designs and quasi‐experimental design studies that contained a comparison group, demonstrated that phonemic awareness interventions had a moderate effect on short‐term outcomes (SMD ES 0.43) and a slightly diminished effect on long‐term (i.e. on average, 11 months after intervention) outcomes (SMD ES 0.36). Phonics interventions had a small effect in the short term (SMD ES 0.29), which decreased substantially in the long term (SMD ES 0.07).
Our findings extend those of two systematic reviews of reading interventions specifically focused on people with intellectual disability (Browder 2006; Joseph 2004). Joseph 2004 identified seven studies that examined the effects of phonics interventions. Although the methodologic design (which included published, single‐case designs, quasi‐experimental comparative designs, and quasi‐experimental, one‐group pre/postdesigns), and rigor of included studies prohibited causal inferences from being drawn, the reviewers indicated that the results provided initial evidence that people with intellectual disability can benefit from phonics‐based approaches to reading instruction. Browder 2006 conducted a more comprehensive review of reading instruction for people with significant cognitive disabilities. In their review, which included peer‐reviewed studies that used experimental or quasi‐experimental designs, including single‐case designs, they examined the evidence base for interventions aligned with each of the National Reading Panel's components of reading by coding studies for quality and ES. Both reviews included group and single‐case design studies. Based on outcomes from single‐case designs, Browder and colleagues identified the use of sight word instruction, using systematic prompting and fading, as an evidence‐based practice for teaching students with intellectual disability to read. They concluded that additional research was needed to determine the efficacy of other approaches to teaching reading to this population of learners.
During the decade since the Browder 2006 review, additional research has been conducted focused on teaching students with intellectual disability to read. The six studies we identified were all conducted within this time frame and all evaluated the efficacy of multicomponent interventions that included a focus on phonologic awareness, letter‐sound correspondence, or decoding. We did not identify any interventions that focused on sight word instruction alone. This is likely due to our exclusion of single‐case design studies. Unfortunately, we were unable to compare the magnitude of effects between the Browder 2006 review and ours, due to the lack of comparability of ES estimates used in the two reviews (percentage of non‐overlapping data versus SMD). Advances are being made in methodologies to estimate SMD ES from single‐case designs, and thus, future reviews may be able to include single‐case design studies in meta‐analyses (Valentine 2016).
The present review extends upon the previously conducted systematic reviews, mentioned above, by synthesizing outcomes from RCTs using a meta‐analytic approach. Our findings provide evidence that reading interventions provided to children and adolescents with intellectual disability that include elements of phonologic awareness, letter sound instruction, and decoding are associated with small‐to‐moderate effects on beginning reading outcomes. The estimated effects are in alignment with effects demonstrated in previous meta‐analyses (Scammacca 2015; Wanzek 2018) for children and adolescents who are typically developing, at‐risk, or with reading disabilities. The estimates of effect for people with intellectual disability, however, appear to be slightly smaller in magnitude compared to the majority of effects reported for people without intellectual disability.
Authors' conclusions
Implications for practice.
Due to the limited number of studies that met our inclusion criteria, our implications for practice should be interpreted with caution. Our review suggests that integrating phonologic awareness and phonics into beginning reading instruction provided to children with intellectual disability may be appropriate for many students. Browder 2009 and Lemons 2016 provide additional guidance for practitioners on how to support the beginning reading development of students with intellectual disability. Findings from Allor 2014 also suggest that early reading intervention provided to this population of learners will need to be sufficiently intensive and delivered over an extended period of time. For example, Allor 2014 found that many learners required two years to four years of daily intervention to demonstrate one year's worth of progress in the reading curriculum. It is important to highlight the need to interpret this finding from a single study with caution. Further, additional individualization may be required for many children and adolescents with intellectual disability. Practitioners can use a process called data‐based individualization to guide ongoing adaptation and individualization. Lemons 2014 presented a case study of a teacher using this approach. Practitioners can also consult the National Center on Intensive Intervention (www.intensiveintervention.org), to learn how to implement data‐based individualization.
Implications for research.
The primary implication for research is that additional experimental studies in which the efficacy of beginning reading interventions for children and adolescents with intellectual disability are needed. We believe there are at least five factors that should be considered in this line of inquiry. First, studies should include a broader age range of participants than the studies included in this review. Evaluating effective methods to enhance reading outcomes for older adolescents and young adults could provide information to guide practitioners who provide services to individuals as they transition into postsecondary settings. Second, as highlighted by Allor 2014, additional evaluations of multi‐component reading interventions that span multiple years are needed. As students with intellectual disability may require several years of intensive intervention to demonstrate meaningful progress, studies should span multiple years to allow for better understanding of possible outcomes. Third, in the protocol for this review (Reichow 2014), we identified several features of instruction (e.g. type of instruction, language of instruction) and participant characteristics (e.g. severity of impairment, language skills) that may moderate treatment response. Unfortunately, the limited research base did not provide sufficient data to explore moderation of treatment effects in this review. Future studies that are designed to explore plausible moderators would extend understanding of how features of instruction and individual differences may align to enhance reading outcomes. Fourth, although our meta‐analysis identified statistically significant small‐to‐moderate effects on important beginning reading skills, there were participants in many of the studies who exhibited poor response to intervention. Additional experimental work to evaluate efficient, effective methods to individualize and intensify reading interventions for students with intellectual disability would increase practitioners' ability to improve reading outcomes for a broader segment of this population.
Acknowledgements
This review was produced within Cochrane Developmental, Psychosocial and Learning Problems (CDPLP). The authors would like to thank Margaret Anderson, Information Specialist of CDPLP for searching relevant databases. We would also like to thank Geraldine Macdonald (Co‐ordinating Editor), Joanne Duffield (Managing Editor), Steve Milan (Editor), Laura MacDonald (Former Managing Editor), and other members of CDPLP for their assistance and guidance throughout the review process.
Appendices
Appendix 1. Search strategies
CENTRAL in the Cochrane Library
Searched 20 April 2015, 9 November 2016, 17 October 2017, 29 August 2018, and 3 October 2019.
#1[mh "Mental Retardation"] #2[mh "Intellectual disability"] [Annotation:replaced mh "Mental Retardation" in 2015} #3[mh ^"Mentally Disabled Persons"] #4[mh ^" Developmental Disabilities"] #5[mh ^"Learning disorders"] #6((mental* or intellectual*) near/2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal*)) #7((learning* or cognit*) near/2 (impair* or retard* or disab* or defici* or difficulty or difficulties or disorder* or handicap* or subnormal* or sub‐normal*)) #8((profound* or mild* or moderate* or multiple or severe*) near/1 (handicap* or disab*)) #9feeble‐minded* #10moron* #11imbecil* #12(down* near/3 syndrome*) #13(prader near/3 willi*) #14(williams near/3 syndrome) #15"fragile X" or FRAXE or FRAXA #16("Martin Bell" near/3 syndrome*) #17((low or borderline) near/1 IQ) #18{or #1‐#17} #19[mh Reading] #20read or reading #21(literacy near/3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*)) #22[mh Phonetics] #23(phonetic* or phonic* or phonolog* or phonemic or phoneme*) #24grapheme* #25(word* near/3 (decod* or de next cod* or encod*)) #26(alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming) #27(sound near/1 symbol*) #28(letter near/1 (name* or knowledge or sound)) #29((word* or sound*) near/3 (blend* or connect* or segment* or onset* or rime*)) #30(sight near/1 (method* or vocabulary or word)) #31word next recognition #32orthograph* #33(rebus or story‐map*) #34{or #19‐#33} #35#18 and #34
MEDLINE Ovid
Searched 20 April 2015, 9 November 2016, 17 October 2017, 29 August 2018, and 2 October 2019.
1 exp Intellectual disability/ [Annotation: replaced Mental Retardation/ in 2015] 2 Mentally Disabled Persons/ 3 Developmental Disabilities/ 4 Learning disorders/ 5 ((mental$ or intellectual$) adj2 (impair$ or retard$ or disab$ or defici$ or handicap$ or subnormal$ or sub‐normal$)).tw. 6 ((learning$ or cognit$) adj2 (impair$ or retard$ or disab$ or defici$ or difficulty or difficulties or disorder$ or handicap$ or subnormal$ or sub‐normal$)).tw. 7 ((profound$ or mild$ or moderate$ or multiple or severe$) adj1 (handicap$ or disab$)).tw. 8 feeble‐minded$.tw. 9 moron$.tw. 10 imbecil$.tw. 11 (down$ adj3 syndrome$).tw. 12 (prader adj3 willi).tw. 13 (williams adj3 syndrome).tw. ) 14 (fragile X or FRAXE or FRAXA).tw. 15 (Martin Bell adj3 syndrome$).tw. 16 ((low or borderline) adj1 IQ).tw. 17 or/1‐16 18 Reading/ (218 19 (read or reading).tw. 20 (literacy adj3 (intervention$ or program$ or instruction$ or skill$ or activit$ or develop$ or strateg$)).tw. 21 Phonetics/ 22 (phonetic$ or phonic$ or phonolog$ or phonemic or phoneme$).tw. 23 grapheme$.tw. 24 (word$ adj3 (decod$ or de‐cod$ or encod$)).tw. 25 (alliteration or alphabeti#e or alphabeti#ation or rhyme or rhyming).tw. 26 (sound adj1 symbol$).tw. 27 (letter adj1 (name$ or knowledge or sound)).tw. 28 ((word$ or sound$) adj3 (blend$ or connect$ or segment$ or onset$ or rime$)).tw. 29 (sight adj1 (method or vocabulary or word)).tw. 30 word recognition.tw. 31 orthograph$.tw. 32 (rebus or story‐map$).tw. 33 or/18‐32 34 randomized controlled trial.pt. 35 controlled clinical trial.pt. 36 randomi#ed.ab. 37 placebo$.ab. 38 randomly.ab. 39 trial.ab. 40 groups.ab. 41 or/34‐40 42 exp animals/ not humans.sh. 43 41 not 42 44 17 and 33 and 43
MEDLINE Epub Ahead of Print Ovid
Searched 10 November 2016, 17 October 2017, 28 August 2018, and 2 October 2019
1 ((mental$ or intellectual$) adj2 (impair$ or retard$ or disab$ or defici$ or handicap$ or subnormal$ or sub‐normal$)).tw. 2 ((learning$ or cognit$) adj2 (impair$ or retard$ or disab$ or defici$ or difficulty or difficulties or disorder$ or handicap$ or subnormal$ or sub‐normal$)).tw. 3 ((profound$ or mild$ or moderate$ or multiple or severe$) adj1 (handicap$ or disab$)).tw. 4 feeble‐minded$.tw. 5 moron$.tw. 6 imbecil$.tw. 7 (down$ adj3 syndrome$).tw. 8 (prader adj3 willi).tw. 9 (williams adj3 syndrome).tw. 10 (fragile X or FRAXE or FRAXA).tw. 11 (Martin Bell adj3 syndrome$).tw. 12 ((low or borderline) adj1 IQ).tw. 13 or/1‐12 14 (read or reading).tw. 15 (literacy adj3 (intervention$ or program$ or instruction$ or skill$ or activit$ or develop$ or strateg$)).tw. 16 (phonetic$ or phonic$ or phonolog$ or phonemic$ or phoneme$).tw. 17 grapheme$.tw. 18 (word$ adj3 (decod$ or de‐cod$ or encod$)).tw. 19 (alliteration or alphabeti#e or alphabeti#ation or rhyme or rhyming).tw. 20 (sound adj1 symbol$).tw. 21 (letter adj1 (name$ or knowledge or sound)).tw. 22 ((word$ or sound$) adj3 (blend$ or connect$ or segment$ or onset$ or rime$)).tw. 23 (sight adj1 (method or vocabulary or word)).tw. 24 word recognition.tw. 25 orthograph$.tw. 26 (rebus or story‐map$).tw. 27 or/14‐26 28 13 and 27 29 (random$ or control$ or group$ or cluster$ or placebo$ or trial$ or assign$ or prospectiv$ or meta‐analysis or systematic review or longitudinal$).tw 30 28 and 29
MEDLINE In‐Process & Other Non‐Indexed Citations Ovid
Searched 10 November 2016, 17 October 2017, 28 August 2018, and 2 October 2019.
1 ((mental$ or intellectual$) adj2 (impair$ or retard$ or disab$ or defici$ or handicap$ or subnormal$ or sub‐normal$)).tw. 2 ((learning$ or cognit$) adj2 (impair$ or retard$ or disab$ or defici$ or difficulty or difficulties or disorder$ or handicap$ or subnormal$ or sub‐normal$)).tw. 3 ((profound$ or mild$ or moderate$ or multiple or severe$) adj1 (handicap$ or disab$)).tw. 4 feeble‐minded$.tw. 5 moron$.tw. 6 imbecil$.tw. 7 (down$ adj3 syndrome$).tw. 8 (prader adj3 willi).tw. 9 (williams adj3 syndrome).tw. 10 (fragile X or FRAXE or FRAXA).tw. 11 (Martin Bell adj3 syndrome$).tw. 12 ((low or borderline) adj1 IQ).tw. 13 or/1‐12 14 (read or reading).tw. 15 (literacy adj3 (intervention$ or program$ or instruction$ or skill$ or activit$ or develop$ or strateg$)).tw. 16 (phonetic$ or phonic$ or phonolog$ or phonemic$ or phoneme$).tw. 17 grapheme$.tw. 18 (word$ adj3 (decod$ or de‐cod$ or encod$)).tw. 19 (alliteration or alphabeti#e or alphabeti#ation or rhyme or rhyming).tw. 20 (sound adj1 symbol$).tw. 21 (letter adj1 (name$ or knowledge or sound)).tw. 22 ((word$ or sound$) adj3 (blend$ or connect$ or segment$ or onset$ or rime$)).tw. 23 (sight adj1 (method or vocabulary or word)).tw. 24 word recognition.tw. 25 orthograph$.tw. 26 (rebus or story‐map$).tw. 27 or/14‐26 28 13 and 27 29 (random$ or control$ or group$ or cluster$ or placebo$ or trial$ or assign$ or prospectiv$ or meta‐analysis or systematic review or longitudinal$).tw 30 28 and 29
Embase Ovid
Searched 20 April 2015, 10 November 2016, 17 October 2017, 28 August 2018, and 2 October 2019.
1 intellectual impairment/ 2 exp mental deficiency/ 3 developmental disorder/ ) 4 learning disorder/ 5 ((mental$ or intellectual$) adj2 (impair$ or retard$ or disab$ or defici$ or handicap$ or subnormal$ or sub‐normal$)).tw. 6 ((learning$ or cognit$) adj2 (impair$ or retard$ or disab$ or defici$ or difficulty or difficulties or disorder$ or handicap$ or subnormal$ or sub‐normal$)).tw. 7 ((profound$ or mild$ or moderate$ or multiple or severe$) adj1 (handicap$ or disab$)).tw. 8 feeble‐minded$.tw. 9 moron$.tw. 10 imbecil$.tw. 11 (down$ adj3 syndrome$).tw. 12 (prader adj3 willi$).tw. 13 (williams adj3 syndrome).tw. 14 (fragile X or FRAXE or FRAXA).tw. 15 (Martin Bell adj3 syndrome$).tw. 16 ((low or borderline) adj1 IQ).tw. 17 or/1‐16 18 reading/ 19 (read or reading).tw. 20 (literacy adj3 (intervention$ or program$ or instruction$ or skill$ or activit$ or develop$ or strateg$)).tw. 21 phonetics/ 22 (phonetic$ or phonic$ or phonolog$ or phonemic or phoneme$).tw. 23 grapheme$.tw. 24 (word$ adj3 (decod$ or de‐cod$ or encod$)).tw. 25 (alliteration or alphabeti#e or alphabeti#ation or rhyme or rhyming).tw. 26 (sound adj1 symbol$).tw. 27 (letter adj1 (name$ or knowledge or sound)).tw. 28 ((word$ or sound$) adj3 (blend$ or connect$ or segment$ or onset$ or rime$)).tw. 29 (sight adj1 (method or vocabulary or word)).tw. 30 word recognition.tw. 31 orthograph$.tw. 32 (rebus or story‐map$).tw. 33 or/19‐32 34 Randomized controlled trial/ 35 controlled clinical trial/ 36 Single blind procedure/ 37 Double blind procedure/ 38 triple blind procedure/ 39 Crossover procedure/ 40 (crossover or cross‐over).tw. 41 ((singl$ or doubl$ or tripl$ or trebl$) adj1 (blind$ or mask$)).tw. 42 Placebo/ 43 placebo.tw. 44 prospective.tw. 45 factorial$.tw. 46 random$.tw. 47 assign$.ab. 48 allocat$.tw. 49 volunteer$.ab. 50 or/34‐49 51 17 and 33 and 50
CINAHL Plus EBSCOhost
Searched 20 April 2015, 10 November 2016, 17 October 2017, 29 August 2018, and 2 October 2019.
S1(MH "Intellectual Disability+") S2(MH "Mentally Disabled Persons") S3(MH "Developmental Disabilities") S4(MH "Learning Disorders") S5((mental* or intellectual*) N2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal *)) S6((learning* or cognit*) N2 (impair* or retard* or disab* or defici* or difficulty or difficulties or disorder* or handicap* or subnormal* or sub‐normal*)) S7((profound* or mild* or moderate* or multiple or sever*) N1 (handicap* or disab*)) S8feeble‐minded* S9moron* S10imbecil* S11(down* N3 syndrome*) S12(prader N3 willi*) S13(williams N3 syndrome) S14(fragile X or FRAXE or FRAXA) S15(Martin Bell N3 syndrome*) S16((low or borderline) N1 IQ) S17S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 S18(MH "Reading+") S19(MH "Reading Disorders") S20(MH "Literacy") S21(read or reading) S22(literacy N3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*)) S23(MH "Phonology") S24(MH "Phonetics") S25(phonetic* or phonic* or phonolog* or phonemic or phoneme*) S26grapheme* S27(word* N3 (decod* or de‐cod* or encod*)) S28(alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming) S29(sound N1 symbol*) S30(letter N1 (name* or knowledge or sound)) S31((word* or sound*) N3 (blend* or connect* or segment* or onset* or rime*)) S32(sight N1 (method or vocabulary or word)) S33word recognition S34orthograph* S35(rebus or story‐map*) S36S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 S37S17 AND S36 S38(MH "Clinical Trials+") S39MH random assignment S40(MH "Meta Analysis") S41(MH "Crossover Design") S42(MH "Quantitative Studies") S43PT randomized controlled trial S44PT Clinical trial S45(clinical trial*) or (control* N2 trial*) S46("follow‐up study" or "follow‐up research") S47(prospectiv* study or prospectiv* research) S48(evaluat* N2 study or evaluat* N2 research) S49(MH "Program Evaluation") S50(MH "Treatment Outcomes") S51TI(single N2 mask* or single N2 blind*) OR AB(single N2 mask* or single N2 blind*) S52TI((doubl* N2 mask*) or (doubl* N2 blind*)) OR AB((doubl* N2 mask*) or (doubl* N2 blind*)) S53TI ((tripl* N2 mask*) or (tripl* N2 blind*)) or ((trebl* N2 mask*) or (trebl* N2 blind*)) OR AB((tripl* N2 mask*) or (tripl* N2 blind*)) or ((trebl* N2 mask*) or (trebl* N2 blind*) S54random* S55S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 OR S50 OR S51 OR S52 OR S53 OR S54 S56S37 AND S55
PsycINFO Ovid
Searched 20 April 2015, 10 November 2016, 17 October 2017, 29 August 2018, and 2 October 2019.
1 exp Intellectual Development Disorder/ 2 learning disorders/ 3 developmental disabilities/ 4 fragile x syndrome/ 5 prader willi syndrome/ 6 williams syndrome/ 7 fetal alcohol syndrome/ 8 microcephaly/ 9 ((mental$ or intellectual$) adj2 (impair$ or retard$ or disab$ or defici$ or handicap$ or subnormal$ or sub‐normal $)).tw. 10 ((learning$ or cognit$) adj2 (impair$ or retard$ or disab$ or defici$ or difficulty or difficulties or disorder$ or handicap$ or subnormal$ or sub‐normal$)).tw. 11 ((profound$ or mild$ or moderate$ or multiple or sever$) adj1 (handicap$ or disab$)).tw. 12 feeble‐minded$.tw. 13 moron$.tw. 14 imbecil$.tw. 15 (down$ adj3 syndrome$).tw. 16 (prader adj3 willi$).tw. 17 (williams adj3 syndrome).tw. 18 (fragile X or FRAXE or FRAXA).tw. 19 (Martin Bell adj3 syndrome$).tw. 20 ((low or borderline) adj1 IQ).tw. 21 or/1‐20 22 reading/ 23 reading achievement/ 24 reading comprehension/ 25 reading development/ 26 reading disabilities/ 27 reading education/ 28 reading materials/ 29 reading measures/ 30 reading skills/ 31 initial teaching alphabet/ 32 orthography/ 33 phonetics/ 34 phonemes/ 35 sight vocabulary/ 36 word recognition/ 37 (read or reading).tw. 38 (literacy adj3 (intervention$ or program$ or instruction$ or skill$ or activit$ or develop$ or strateg$)).tw. 39 (phonetic$ or phonic$ or phonolog$ or phonemic or phoneme$).tw. 40 grapheme$.tw. 41 (word$ adj3 (decod$ or de‐cod$ or encod$)).tw. 42 (alliteration or alphabeti#e or alphabeti#ation or rhyme or rhyming).tw. 43 (sound adj1 symbol$).tw. 44 (letter adj1 (name$ or knowledge or sound)).tw. 45 ((word$ or sound$) adj3 (blend$ or connect$ or segment$ or onset$ or rime$)).tw. 46 (sight adj1 (method or vocabulary or word)).tw. 47 word recognition.tw. 48 orthograph$.tw. 49 (rebus or story‐map$).tw. 50 or/22‐49 51 clinical trials/ 52 (randomis$ or randomiz$).tw. 53 (random$ adj3 (allocat$ or assign$)).tw. 54 ((clinic$ or control$) adj trial$).tw. 55 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 56 (crossover$ or "cross over$").tw. 57 random sampling/ 58 Experiment Controls/ 59 Placebo/ 60 placebo$.tw. 61 exp program evaluation/ 62 treatment effectiveness evaluation/ 63 ((effectiveness or evaluat$) adj3 (stud$ or research$)).tw. 64 or/51‐63 65 21 and 50 and 64
ERIC EBSCOhost
Searched 21 April 2015, 10 November 2016, 17 October 2017, 29 August 2018, and 2 October 2019.
S1DE "Mental Retardation" S2DE "Mild Mental Retardation" S3DE "Moderate Mental Retardation" S4DE "Severe Mental Retardation" S5DE "Developmental Disabilities" S6DE "Intellectual Disability" S7DE "Fetal Alcohol Syndrome" S8DE "Learning Problems" S9DE "Down Syndrome" S10TI((mental* or intellectual*) N2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal *)) or AB((mental* or intellectual*) N2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal *)) S11TI((learning* or cognit*) N2 (impair* or retard* or disab* or defici* or difficulty or difficulties or disorder* or handicap* or subnormal* or sub‐normal*)) OR AB((learning* or cognit*) N2 (impair* or retard* or disab* or defici* or difficulty or difficulties or disorder* or handicap* or subnormal* or sub‐normal*)) S12TI((profound* or mild* or moderate* or multiple or sever*) N1 (handicap* or disab*))OR AB((profound* or mild* or moderate* or multiple or sever*) N1 (handicap* or disab*)) S13feeble‐minded S14moron* S15imbecil* S16(down* N3 syndrome*) S17(prader N3 willi*) S18(williams N3 syndrome) S19(fragile X or FRAXE or FRAXA) S20("Martin Bell" N3 syndrome*) S21((low or borderline) N1 IQ) S22S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 S23DE "Reading" OR (DE "Beginning Reading") OR DE "Reading Ability" OR DE "Reading Achievement" OR DE "Reading Difficulties" OR DE "Reading Instruction" OR DE "Reading Programs" OR DE "Reading Skills" OR DE "Decoding (Reading)" OR DE "Sight Method" OR DE "Sight Vocabulary" S24DE "Literacy" OR DE "Literacy Education" S25TI(literacy N3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*))OR AB(literacy N3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*)) S26TI(read or reading) OR AB(read or reading) S27DE "Phonics" S28DE "Phonemes" S29DE "Phonemic Awareness" S30DE "Graphemes" S31DE "Orthographic Symbols" S32TI(phonetic* or phonic* or phonolog* or phonemic or phoneme*) or AB(phonetic* or phonic* or phonolog* or phonemic or phoneme*) S33TI (grapheme*) OR AB( grapheme*) S34TI(word* N3 (decod* or de‐cod* or encod*)) or AB(word* N3 (decod* or de‐cod* or encod*)) S35TI((alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming)) OR AB((alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming)) S36(sound N1 symbol*) S37TI(letter N1 (name* or knowledge or sound)) OR AB (letter N1 (name* or knowledge or sound)) S38TI ((word* or sound*) N3 (blend* or connect* or segment* or onset* or rime*))OR AB((word* or sound*) N3 (blend* or connect* or segment* or onset* or rime*)) S39TI (sight N1 (method or vocabulary or word)) OR AB (sight N1 (method or vocabulary or word)) S40TI(word recognition ) OR AB(word recognition ) ) S41TI (orthograph* ) OR AB(orthograph* ) S42TI(rebus or story‐map*) OR AB(rebus or story‐map*) S43S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 S44S22 AND S43 S45DE "Control Groups" OR DE "Evaluation Research" OR DE "Experimental Groups" OR DE "Program Effectiveness" OR DE "Program Evaluation" or DE "Intervention" OR DE "Teacher Effectiveness" OR DE "Program Effectiveness" OR DE "Instructional Effectiveness" OR DE "Comparative Analysis" OR DE "Meta Analysis" S46TI(random*) or AB (random*) S47AB(control* N1 (group* or trial or stud* OR subject* or participant* or experiment*)) OR TI (control* N1 (group* or trial or stud* OR subject* or participant* or experiment*)) S48S45 OR S46 OR S47 S49S44 AND S48
British Education Index EBSCOhost
Searched 21 April 2015, 9 November 2016, 17 October 2017, 29 August 2018, and 2 October 2019.
S1((DE "MENTAL retardation" OR DE "DOWN syndrome") OR(DE "DEVELOPMENTALLY disabled" OR DE "LEARNING disabilities")) OR (DE "DEVELOPMENTAL disabilities" )OR DE "MENTAL disabilities" S2DE "CHILDREN with mental disabilities" OR DE "LEARNING disabled children" OR DE "CHILDREN with mental disabilities ‐‐ Education" S3(DE "MENTAL retardation" OR DE "DOWN syndrome" OR DE "FETAL alcohol syndrome ‐‐ Study & teaching" ) S4((mental* or intellectual*) N2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal *)) S5((learning* or cognit*) N2 (impair* or retard* or disab* or defici* or difficulty or difficulties or disorder* or handicap* or subnormal* or sub‐normal*)) S6((profound* or mild* or moderate* or multiple or sever*) N1(handicap* or disab*)) S7feeble‐minded* OR moron* OR imbecil* S8(down* N3 syndrome*) S9(prader N3 willi*) S10(williams N3 syndrome) S11(fragile X or FRAXE or FRAXA ) S12(Martin Bell* N3 syndrome*) S13((low or borderline) N1 (INTELLIGENCE OR IQ)) S14S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 S15DE "READING readiness" OR DE "READING intervention" OR DE "READING ‐‐ Direct instruction approach" OR DE "READING" OR DE "BASAL reading instruction" OR DE "BEGINNING reading" OR DE "FUNCTIONAL reading" OR DE "INDEPENDENT reading" OR DE "INDIVIDUALIZED reading instruction" OR DE "INTENSIVE reading" OR DE "MISCUE analysis" OR DE "ORAL reading" OR DE "READING (Early childhood)" OR DE "READING (Elementary)" OR DE "READING (Middle school)" OR DE "READING (Preschool)" OR DE "READING (Secondary)" OR DE "READING ‐‐ Code emphasis approaches" OR DE "READING ‐‐ Language experience approach" OR DE "READING achievement" OR DE "SCORE reading & playing" OR DE "STRUGGLING readers" OR DE "READING ‐‐ Research" OR DE "READING disability" S16DE "LITERACY" S17read or reading S18(literacy N3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*)) S19DE "ALPHABETIC principle (Reading)" S20grapheme* S21(word* N3 (decod* or de‐cod* or encod*)) S22(alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming) S23(sound N1 symbol*) S24(DE "ORTHOGRAPHY & spelling" OR DE "PHONOLOGICAL decoding" OR DE "PHONOLOGICAL encoding") OR (DE "PHONETIC alphabet") OR DE "PHONETICS ‐‐ Study & teaching" S25(phonetic* or phonic* or phonolog* or phonemic* or phoneme*) S26(letter N1 (name* or knowledge or sound*)) S27((word* or sound*) N3 (blend* or connect* or segment* or onset* or rime*)) S28(sight N1 (method or vocabulary or word)) S29word recognition S30orthograph* S31(rebus or story‐map*) S32S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 S33S14 AND S32
Web of Science: SCI; SSCI; CPCI‐S; and CPCI‐SSH
Searched 21 April 2015, 10 November 2016, 17 October 2017, 29 August 2018, and 2 October 2019.
22 #21 AND #20 Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 21 TS=(random* or "control group" or "controlled trial " or RCT) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 20 #19 AND #13 Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 19 #18 OR #17 OR #16 OR #15 OR #14 Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 18 TS=((low or borderline) near/1 IQ) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 17 TS=("down* syndrome" or "prader willi*" or "fragile x" or FRAXA or FRAXE or "Martin Bell* syndrome" or "williams syndrome") Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 16 TS=((profound* or mild* or moderate* or multiple or severe*) near/2 (handicap* or disab*)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 15 TS=((learning* or cognit*) near/2 (impair* or retard* or disab* or defici* or difficulty or difficulties or disorder* or handicap* or subnormal* or sub‐normal*)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 14 TS=((mental* or intellectual*) near/2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal*)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 13 #12 OR #11 OR #10 OR #9 OR #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1 Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 12TS=(rebus or story‐map*) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 11 TS=(orthograph* ) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 10 TS=("word recognition") Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 9 TS=(sight near/1 (method* or vocabulary or word)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 8 TS=((word* or sound*) near/1 (blend* or connect* or segment* or onset* or rime*)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 7 TS=(letter near/1 (name* or knowledge or sound)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 6 TS=(sound near/1 symbol*) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 5 TS= (alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 4 TS=(word* near/3 (decod* or de‐cod* or encod*)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 3 TS=(phonetic* or phonic* or phonolog* or phonemic or phoneme*) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 2 TS=(literacy near/3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*)) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH # 1 TS=(read or reading) Indexes=SCI‐EXPANDED, SSCI, CPCI‐S, CPCI‐SSH
Cochrane Database of Systematic Reviews (CDSR)
Searched 20 April 2015, 9 November 2016, 17 October 2017, 28 August 2018, and 2 October 2019.
#1[mh "Mental Retardation"] #2[mh "Intellectual disability"] #3[mh ^"Mentally Disabled Persons"] #4[mh ^" Developmental Disabilities"] #5[mh ^"Learning disorders"] #6((mental* or intellectual*) near/2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal*)):ti,ab #7((learning* or cognit*) near/2 (impair* or retard* or disab* or defici* or difficulty or difficulties or handicap* or subnormal* or sub‐normal*)):ti,ab #8((profound* or mild* or moderate* or multiple or severe*) near/1 (handicap* or disab*)):ti,ab #9feeble‐minded*:ti,ab #10moron*:ti,ab #11imbecil*:ti,ab #12(down* near/3 syndrome*):ti,ab #13(prader near/3 willi*):ti,ab #14(williams near/3 syndrome):ti,ab #15("fragile X" or FRAXE or FRAXA):ti,ab #16("Martin Bell" near/3 syndrome*):ti,ab #17((low or borderline) near/1 IQ):ti,ab #18{or #1‐#17} #19[mh Reading] #20(read or reading):ti,ab #21(literacy near/3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*)):ti,ab #22[mh Phonetics] #23(phonetic* or phonic* or phonolog* or phonemic or phoneme*):ti,ab #24grapheme*:ti,ab #25(word* near/3 (decod* or de next cod* or encod*)):ti,ab #26(alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming):ti,ab #27(sound near/1 symbol*):ti,ab #28(letter near/1 (name* or knowledge or sound)):ti,ab #29((word* or sound*) near/3 (blend* or connect* or segment* or onset* or rime*)):ti,ab #30(sight near/1 (method* or vocabulary or word)):ti,ab #31(word next recognition):ti,ab #32orthograph* #33(rebus or story‐map*):ti,ab #34{or #19‐#33} #35MeSH descriptor: [Adolescent] explode all trees #36MeSH descriptor: [Child] 1 tree(s) exploded #37[mh ^"Young adult"] #38(child* or teen* or adolescen* or young next person* or young next people or young next adult* or youth*):ti,ab #39{or #35‐#38}
Database of Abstracts of Reviews of Effects (DARE)
Searched 20 April 2015 and 9 November 2016. No new content has been added to DARE since this date.
#1[mh "Mental Retardation"] #2[mh "Intellectual disability"] #3[mh ^"Mentally Disabled Persons"] #4[mh ^" Developmental Disabilities"] #5[mh ^"Learning disorders"] #6((mental* or intellectual*) near/2 (impair* or retard* or disab* or defici* or handicap* or subnormal* or sub‐normal*)):ti,ab #7((learning* or cognit*) near/2 (impair* or retard* or disab* or defici* or difficulty or difficulties or disorder* or handicap* or subnormal* or sub‐normal*)):ti,ab #8((profound* or mild* or moderate* or multiple or severe*) near/1 (handicap* or disab*)):ti,ab #9feeble‐minded*:ti,ab #10moron*:ti,ab #11imbecil*:ti,ab #12(down* near/3 syndrome*):ti,ab #13(prader near/3 willi*):ti,ab #14(williams near/3 syndrome):ti,ab #15("fragile X" or FRAXE or FRAXA):ti,ab #16("Martin Bell" near/3 syndrome*):ti,ab #17((low or borderline) near/1 IQ):ti,ab #18{or #1‐#17} #19[mh Reading] #20(read or reading):ti,ab #21(literacy near/3 (intervention* or program* or instruction* or skill* or activit* or develop* or strateg*)):ti,ab #22[mh Phonetics] #23(phonetic* or phonic* or phonolog* or phonemic or phoneme*):ti,ab #24grapheme*:ti,ab #25(word* near/3 (decod* or de next cod* or encod*)):ti,ab #26(alliteration or alphabeti*e or alphabeti*ation or rhyme or rhyming):ti,ab #27(sound near/1 symbol*):ti,ab #28(letter near/1 (name* or knowledge or sound)):ti,ab #29((word* or sound*) near/3 (blend* or connect* or segment* or onset* or rime*)):ti,ab #30(sight near/1 (method* or vocabulary or word)):ti,ab #31(word next recognition):ti,ab #32orthograph* #33(rebus or story‐map*):ti,ab #34{or #19‐#33} #35MeSH descriptor: [Adolescent] explode all trees #36MeSH descriptor: [Child] 1 tree(s) exploded #37[mh ^"Young adult"] #38(child* or teen* or adolescen* or young next person* or young next people or young next adult* or youth*):ti,ab in Other Reviews #39{or #35‐#38} #40#18 and #34 and #39
WorldCat
Searched 21 April 2015, 9 November 2016, 17 October 2017, 28 August 2018, and 3 October 2019.
(kw:intellectual disab* OR mental* retard* OR mental handicap* ) AND (kw:read*) AND (kw:random* OR evaluat* OR control* OR experiment*) Limited to Thesis/dissertation
EPPI‐Centre Database of Education Research
Searched 20 November 2016, 21 September 2018, and 11 October 2019.
("mental retardation" OR "intellectual disabilit*" OR "developmental disabilit*" OR "learning dis*" OR "down syndrome" OR "fragile X" OR "prader willi" OR "low IQ" OR "borderline IQ") AND (reading OR literacy OR read OR phonetics OR decoding OR grapheme OR alliteration OR rhyming OR "sight word" OR "word recognition" OR orthography OR story‐map OR rebus)
OpenGrey
Searched 20 November 2016, 21 September 2018, and 11 October 2019.
("mental retardation" OR "intellectual disabilit*" OR "developmental disabilit*" OR "learning dis*" OR "down syndrome" OR "fragile X" OR "trader willi" OR "low IQ" OR "borderline IQ") AND (reading OR literacy OR read OR phonetics OR decoding OR grapheme OR alliteration OR rhyming OR "sight word" OR "word recognition" OR orthography OR story‐map OR rebus)
National Technical Information Service (NTIS)
Searched 20 November 2016, 21 September 2018, and 11 October 2019.
("mental retardation" OR "intellectual disabilit*" OR "developmental disabilit*" OR "learning dis*" OR "down syndrome" OR "fragile X" OR "prader willi" OR "low IQ" OR "borderline IQ") AND (reading OR literacy OR read OR phonetics OR decoding OR grapheme OR alliteration OR rhyming OR "sight word" OR "word recognition" OR orthography OR story‐map OR rebus)
ClinicalTrials.gov
Searched 20 November 2016, 17 October 2017, 28 August 2018, and 3 October 2019.
("mental retardation" OR "intellectual disabilit*" OR "developmental disabilit*" OR "learning dis*" OR "down syndrome" OR "fragile X" OR "prader willi" OR "low IQ" OR "borderline IQ") AND (reading OR literacy OR read OR phonetics OR decoding OR grapheme OR alliteration OR rhyming OR "sight word" OR "word recognition" OR orthography OR story‐map OR rebus)
ICTRP
Searched 20 November 2016, 17 October 2017, 28 August 2018, and 3 October 2019.
("mental retardation" OR "intellectual disabilit*" OR "developmental disabilit*" OR "learning dis*" OR "down syndrome" OR "fragile X" OR "prader willi" OR "low IQ" OR "borderline IQ") AND (reading OR literacy OR read OR phonetics OR decoding OR grapheme OR alliteration OR rhyming OR "sight word" OR "word recognition" OR orthography OR story‐map OR rebus)
Data and analyses
Comparison 1. Phonologic awareness.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Phonologic awareness | 4 | 178 | Std. Mean Difference (Random, 95% CI) | 0.55 [0.23, 0.86] |
Comparison 2. Word reading.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Word reading | 5 | 220 | Std. Mean Difference (Random, 95% CI) | 0.54 [0.05, 1.03] |
Comparison 3. Decoding.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Decoding | 5 | 230 | Std. Mean Difference (Random, 95% CI) | 0.40 [0.12, 0.67] |
Comparison 4. Supplemental measures of literacy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Oral reading fluency | 2 | 84 | Std. Mean Difference (Random, 95% CI) | 0.65 [‐0.12, 1.42] |
Comparison 5. Supplemental measures of language skills.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Expressive and receptive language | 3 | 222 | Std. Mean Difference (Random, 95% CI) | 0.28 [0.03, 0.54] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ahlgrim‐Delzell 2016.
| Methods | Randomized controlled trial | |
| Participants |
Setting: school Sample size: 31 students with intellectual and multiple disabilities (treatment group: 17; control group: 14) Dropouts/withdrawals: 0 Mean age: not reported. Children were enrolled in grades K to 8. Sex: overall: 23/31 (74%) male; treatment group: 14/17 (82.4%) male; control group: 9/14 (64.3%) male Mean IQ: overall: 51.6 (SD 10.9; range 40–88); treatment group: 50.10 (SD 9.5); control group: 53.40 (SD 12.5) |
|
| Interventions |
Intervention: Early Reading Skills Builder, delivered by certified teachers in 5 × 17.5‐minute sessions per week, for 36 weeks Control: treatment as usual |
|
| Outcomes |
Primary outcomes:
|
|
| Notes |
Study start date: October 2012 Study end date: June 2013 Funding: US Department of Education, Institute of Education Sciences, awarded to The Attainment Company COI: none declared by the authors; The Attainment Company developed an iPad‐based technologic support device (GoTalk Now) that was used in the study. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: study used a randomized controlled trial design where students were randomly assigned to treatment and control conditions using simple random assignment blocked by teacher when multiple students in a classroom were determined eligible to participate. |
| Allocation concealment (selection bias) | Unclear risk | Comment: method of allocation concealment not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: teachers were not blind to group status of the participants; unclear if students knew group of their participation in the study. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: blinding of outcome assessors not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no evidence of attrition. |
| Selective reporting (reporting bias) | Low risk | Comment: all outcomes that were collected appeared to have been reported in study report. |
| Other bias | Low risk | Comment: no additional sources of bias detected. |
Allor 2014.
| Methods | Randomized controlled trial | |
| Participants |
Setting: school Sample size: 98 students with intellectual and multiple disabilities (treatment group: 59; control group: 39) Dropouts/withdrawals: 22 (treatment group: 14; control group: 8) Mean age: overall: 11.3 years (SD 1.3); treatment group: 11.5 (SD 1.9); control group: 11.2 (SD 0.4) Sex: overall: 49/76 (64%) male; data per group not reported Mean IQ: overall: 57.7 (SD 8.7; range 40–70); treatment group: 57.1 (SD 8.9); control group: 58.6 (SD 8.3) |
|
| Interventions |
Intervention: Early Interventions in Reading, delivered by certified teachers in 5 × 45‐minute sessions per week, for a mean of 100.8 weeks (SD 27.1; range 19–134) Control: treatment as usual |
|
| Outcomes |
Primary outcomes:
Secondary outcomes:
Other outcomes reported in the study but not included in this review:
|
|
| Notes |
Participant sample: study inclusion criteria specified IQ 40–80 to be eligible; however, only data from participants with IQs < 70 were included (data for sample with IQ < 70 obtained from study author). Study start date: not reported Study end date: not reported Funding: US Department of Education, Institute of Education Sciences COI: COI section not included in manuscript. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: students randomly assigned within school and IQ range. |
| Allocation concealment (selection bias) | Unclear risk | Comment: method of allocation concealment not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: teachers not blind to group status of participants; unclear if students knew group or their participation in the study. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: blinding of outcome assessors not described. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: 22 students did not complete study (treatment group: 14; control group: 8). Missing data: treatment group 11; control group: 5; unclear if missing data related to true outcome. |
| Selective reporting (reporting bias) | Low risk | Comment: all outcomes that were collected appeared to have been reported in study report. |
| Other bias | Low risk | Comment: no additional sources of bias detected. |
Browder 2012.
| Methods | Randomized controlled trial | |
| Participants |
Setting: school Sample size: 93 students with developmental and intellectual disabilities (treatment group: 47; control group: 46) Dropouts/withdrawals: 1 (treatment group: 0; control group: 1) Mean age: 8.8 years (SD 1.6); data per group not reported Sex: overall: 56/93 (60%) male; treatment group: 32/47 (67%) male; control group: 24/46 (53%) male Mean IQ: overall: 42.5 (SD 12.9); treatment group: 43.5 (SD 13.3); control group: 41.5 (SD 13.1) |
|
| Interventions |
Intervention: Early Literacy Skills Builder, delivered by certified teachers in 5 × 20‐minute sessions per week, for 24 weeks Control: treatment as usual |
|
| Outcomes |
Primary outcomes: none reported Secondary outcomes:
Other outcomes reported in the study but not included in this review:
|
|
| Notes |
Study start date: 2004 Study end date: 2007 Funding: US Department of Education, Institute of Education Sciences COI: first and second authors of the study are authors of the intervention (Early Literacy Skills Builder) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: randomization method not described. |
| Allocation concealment (selection bias) | Unclear risk | Comment: method of allocation concealment not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: no indication that the teachers or other participants were blind to study purpose or hypotheses. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: blinding of outcome assessors not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: participant section of method section indicated 93 participants, and data were reported on 92 participants in the table on the effects of the interventions; hence attrition seemed very low. |
| Selective reporting (reporting bias) | Low risk | Comment: all outcomes that were collected appeared in study report. |
| Other bias | Low risk | Comment: no additional sources of bias detected. |
Burgoyne 2012.
| Methods | Randomized controlled trial | |
| Participants |
Setting: school Sample size: 57 students with Down syndrome (treatment group: 29; control group: 28) Dropouts/withdrawals: 3 (treatment group 1; control group: 2) Mean age: 6.6 years (SD 1.3; range 5–10 years); treatment group: 6.7 years (SD 1.2); control group: 6.5 years (SD 1.3) Sex: overall: 28 (49%) male; data per group not reported Mean IQ: not reported |
|
| Interventions |
Intervention: phonemic awareness instruction, delivered by paraprofessional school staff in 5 × 40‐minute sessions per week, for 24 weeks Control: treatment as usual |
|
| Outcomes |
Primary outcomes:
Secondary outcome:
Other outcomes reported in the study but not included in this review:
|
|
| Notes |
Study start date: 2009 Study end date: 2010 Funding: Big Lottery Fund COI: none of the authors declared any COI; 3 authors were employees of DS Education International, which, as a registered charity, intended to market the program evaluated in this intervention, with any profits from the sales going back to the charity to support its work. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: method of random assignment to groups not described. |
| Allocation concealment (selection bias) | Unclear risk | Comment: method of allocation concealment not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: teachers were not blind to group status; unclear if students knew their group or participation in the study. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: blinding of outcome assessors not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: low attrition, with missing data for 1/29 student in treatment group and 2/28 students in control group. |
| Selective reporting (reporting bias) | Low risk | Comment: all outcomes that were collected appeared to have been reported. |
| Other bias | Low risk | Comment: no additional sources of bias detected. |
Cleave 2011.
| Methods | Randomized controlled trial | |
| Participants |
Setting: school Sample size: 17 students with Down syndrome (treatment group 8; control group: 9) Dropouts/withdrawals: 1 (treatment group: 0; control group: 1) Mean age: overall: 10.9 years (SD 3.0; range 5 years 10 months to 16 years 8 months); treatment group: 11.7 (SD 3.6); control group: 10.05 (SD 2.4) Sex: overall: 7/17 (41%) male; data per group not reported Mean IQ: overall: 50.8 (SD 9.2); treatment group: 48.40 (SD 9.4); control group: 53.4 (SD 13.9) |
|
| Interventions |
Intervention: phonemic awareness instruction, delivered by research personnel in 3 × 30‐minute sessions per week, for 22 weeks Control: treatment as usual |
|
| Outcomes |
Primary outcomes:
Secondary outcomes: none reported |
|
| Notes |
Study start date: not reported Study end date: not reported Funding: Canadian Language and Literacy Research Network, Nova Scotia Health Research Foundation COI: COI section not included in manuscript. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: method of random assignment to groups not described. |
| Allocation concealment (selection bias) | Unclear risk | Comment: method of allocation concealment not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: although instructors knew which group they were in, the interventionists were not told of the study's hypothesis, but the interventionists were aware of the goals of the intervention program they were administering. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: all testing completed by speech‐language pathologists who were blind to the child's group assignment. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no evidence of attrition. |
| Selective reporting (reporting bias) | Low risk | Comment: all outcomes that were collected appeared to have been reported. |
| Other bias | Low risk | Comment: no additional sources of bias detected. |
Finnegan 2011.
| Methods | Randomized controlled trial | |
| Participants |
Setting: school Sample size: 52 students with intellectual disability (treatment group: 35; control group: 17) Dropouts/withdrawals: no dropouts/withdrawals reported Mean age: overall: 8.7 years (SD 2.6; range 5–12 years); treatment group: 8.7 years (SD 2.5), control group: 8.5 years (SD 2.6) Sex: overall: 31/51 (60%) male; data per group not reported Mean IQ: overall: 56.0 (SD 13.4); treatment group: 55.9 (SD 12.6); control group: 56.2 (SD 15.2) |
|
| Interventions |
Intervention: phonemic awareness instruction delivered by research personnel in 3 × 17.5‐minute sessions per week, for 4 weeks Control: treatment as usual |
|
| Outcomes |
Primary outcomes:
Secondary outcomes: none reported |
|
| Notes |
Study start date: not reported Study end date: not reported Funding: no external funding reported COI: COI section not included |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: method of random assignment to groups not described. |
| Allocation concealment (selection bias) | Unclear risk | Comment: method of allocation concealment not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: researcher with knowledge of group assignment and study hypotheses was involved in providing the intervention to participants. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: researcher with knowledge of group assignment and study hypotheses was involved in outcome assessment. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: information regarding the number of students who began and completed the trial not provided in study report. |
| Selective reporting (reporting bias) | Unclear risk | Comment: information confirming that all outcomes that were assessed were reported not provided. |
| Other bias | Low risk | Comment: no additional sources of bias detected. |
Roberts‐Tyler 2019.
| Methods | Randomized controlled trial | |
| Participants |
Setting: school Sample size: 26 students with intellectual disability (13 per group) Dropouts/withdrawals: 2 treatment participants and 1 control participant excluded after pretest for non‐compliant behavior with baseline assessments, and 1 control participant with missing post‐test data Mean age: overall: 13.0 years (SD 3.3; range 5–19 years); treatment group: 12.8 (SD 4.0); control group: 13.2 (SD 2.5) Sex: not reported Mean IQ: not reported |
|
| Interventions |
Intervention: Headsprout Early Reading intervention with 80 online episodes delivered on school computers Control: treatment as usual |
|
| Outcomes |
Primary outcome:
Secondary outcome:
|
|
| Notes |
Study start date: not reported Study end date: not reported Funding: no external funding reported COI: no COIs reported for any author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: random number lists generated in Excel. |
| Allocation concealment (selection bias) | Low risk | Comment: participants randomly allocated prior to baseline assessment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: teachers not blind to group status; unclear if students knew their group or participation in study. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: researcher with knowledge of group assignment and study hypotheses involved in outcome assessment in 64% of post‐test assessments. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: attrition rate 84.6% and equal across groups. |
| Selective reporting (reporting bias) | Low risk | Comment: information confirming that all outcomes that were assessed were reported not provided. |
| Other bias | Low risk | Comment: no additional sources of bias detected. |
COI: conflict of interest; CTOPP: Comprehensive Test of Phonological Processing (Wagner 1999); DIBELS‐NWF: Dynamic Indicators of Basic Early Literacy Skills: nonsense word fluency (Good 2002); DIBELS‐ORF: Dynamic Indicators of Basic Early Literacy Skills: Oral Reading Fluency (Good 2002); DIBELS‐PSF: Dynamic Indicators of Basic Early Literacy Skills: Phoneme Segmentation Fluency (Good 2002); DRA: Diagnostic Reading Analysis (Crumpler 2007); EVT: Expressive Vocabulary Test (Williams 1997); IQ: intelligence quotient; NVLA: Nonverbal Literacy Assessment; PPVT: Peabody Picture Vocabulary Test (Dunn 1997); SD: standard deviation; TOPA: Test of Phonological Awareness (Torgesen 1994); TOWRE: Test of One Word Reading Efficiency (Torgesen 1999); WJ‐III: Woodcock‐Johnson III: Diagnostic Reading Battery (Shrank 2004); WRaPS: Word Recognition and Phonic Skills Assessment (Carver 1994); WLPB‐R: Woodcock Language Proficiency Battery – Revised: WRMT: Woodcock Reading Mastery Test (Woodcock 1987).
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Alfassi 2009 | Did not contain an intervention for beginning reading skills. |
| Van der Bijl 2006 | Not a randomized controlled trial. |
Characteristics of studies awaiting assessment [ordered by study ID]
Hughes 1982.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to locate the study report. |
Hughes 1984.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to locate the study report. |
Muter 1976.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to locate the study report. |
Salario 1960.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to locate the study report. |
Differences between protocol and review
We made minor edits to the Background section to improve clarity.
As specified under Types of outcome measures, we only located data for the time point immediately after intervention. If we had located follow‐up data, we would have handled these data as described in Table 7.
We no longer had access to the Australian Education Index so could not search it as part of the Electronic searches, We searched two additional segments of Ovid MEDLINE, which became available to us in 2016 and which are updated daily (MEDLINE E‐pub Ahead of Print and MEDLINE In‐Process and Other Non‐indexed Citations).
Under Measures of treatment effect, we specified the calculation by Borenstein 2009, which we used to combine results of functionally equivalent measures of an outcome within a study. We chose this calculation because alternative methods fail to account for the dependence between measures and therefore result in inflated variance estimate and introduce bias by giving studies with more effect sizes greater weight in the meta‐analysis. As such, the approach used to combine effect sizes accounts for the correlation between the dependent measures of interest, providing a more accurate and robust estimate of the intervention's effect (Scammacca 2014).
We constructed a table, which we populated with protocol decisions that were not needed or used in the final review (see Table 7), to help the reader distinguish between methods that were and were not used.
We added a new section, ' 'Summary of findings' tables', to comply with MECIR standards.
Contributions of authors
Protocol
BR, CL, DM, and DH contributed to the development of the protocol for this review; CL and DH drafted the introduction; and BR, CL, and DM drafted the methods. All review authors (BR, CL, DM, DH) reviewed and approved the full protocol.
Review
BR and DM screened the abstracts and titles, retrieved potentially eligible papers, and made decisions about eligibility. They resolved any disagreements by discussion until agreement was made; CL mediated in the case of ongoing disagreements.
CL and DH independently extracted data, resolving any disagreements by discussion until agreement was made.
CL and DH conducted the 'Risk of bias' assessments, with discrepancies, if needed, resolved by BR.
BR and DM conducted the GRADE assessments, with discrepancies, if needed, resolved by CL.
BR, CL, DM, and DH drafted and approved the full review.
BR is the guarantor for the review.
Sources of support
Internal sources
-
University of Florida, USA.
Salary support for BR
-
Vanderbilt University, USA.
Salary support for CL
-
University of Illinois at Chicago, USA.
Salary support for DM
-
University of Michigan‐Deerborn, USA.
Salary support for DH
External sources
None, Other.
Declarations of interest
BR receives royalties from Springer for the publications Handbook of Early Childhood Special Education, Evidence‐Based Practices and Treatments for Children with Autism, and Adolescents and Adults with Autism Spectrum Disorders. He also receives honoraria from Springer for his duties as Associate Editor of the Journal of Autism and Developmental Disorders, and from not‐for‐profit organizations for lectures on autism spectrum disorders and developmental disorders. BR receives salary support from the University of Florida, and funding from the Department of Education, USA. BR declares that none of these sources supported or influenced his work on this review.
CL receives honoraria from not‐for‐profit organizations for lectures on disabilities and education; former salary support from the University of Pittsburgh; current salary support from Peabody College of Vanderbilt University; and funding from the Department of Education, USA. CL also declares that he was not involved in any of the studies included in this review. CL receives an honorarium for his work as a Senior Advisor for the National Center on Intensive Intervention, a not‐for‐profit entity funded by the US Department of Education Office of Special Education Programs. Although CL conducts and publishes research on reading interventions for children and adolescents with intellectual disabilities, at the time of this review, he was not an author of any study that would have met eligibility requirements. CL declares that none of these sources supported or influenced his work on this review.
DM receives honoraria from not‐for‐profit organizations for lectures on disabilities and education; current salary support from the University of Illinois at Chicago; funding from the Department of Education, USA; and honorarium for his consultancy on behavioral interventions and progress monitoring for the National Center on Intensive Intervention, a not‐for‐profit entity funded by the US Department of Education Office of Special Education Programs. DM also receives honoraria from the Hammill Institute for serving as the Editor‐in‐Chief of Behavioral Disorders. DM declares that none of these sources supported or influenced his work on this review.
DH receives current salary support from the University of Michigan‐Dearborn, USA, which did not influence his work on this review.
New
References
References to studies included in this review
Ahlgrim‐Delzell 2016 {published data only}
- Ahlgrim‐Delzell L, Broder DM, Wood L, Stanger C, Preston AI, Kemp‐Inman A. Systematic instruction of phonics skills using an iPad for students with developmental disabilities who are AAC users. Journal of Special Education 2016;50(2):86‐97. [DOI: 10.1177/0022466915622140] [DOI] [Google Scholar]
Allor 2014 {published and unpublished data}
- Allor J. Re: Cochrane Review Request [personal communication]. Email to: C Lemons 21 January 2016.
- Allor J. Re: Cochrane Review request [personal communication]. Email to: C Lemons 1 March 2016.
- Allor JH, Mathes PG, Roberts JK, Cheatham JP, Al Otaiba S. Is scientifically‐based reading instruction effective for students with below‐average IQs?. Exceptional Children 2014;80(3):287‐306. [DOI: 10.1177/0014402914522208] [DOI] [Google Scholar]
- Allor JH, Mathes PG, Roberts JK, Cheatham JP, Champlin TM. Comprehensive reading instruction for students with intellectual disabilities: findings from the first three years of a longitudinal study. Psychology in the Schools 2010;47(5):445‐66. [DOI: 10.1002/pits.20482] [DOI] [Google Scholar]
- Allor JH, Mathes PG, Roberts JK, Jones FG, Champlin TM. Teaching students with moderate intellectual disabilities to read: an experimental examination of a comprehensive reading intervention. Education and Training in Autism and Developmental Disabilities 2010;45(1):3‐22. [www.jstor.org/stable/23880147] [Google Scholar]
- Lemons C. Cochrane Review request [personal communication]. Email to: J Allor 21 January 2016.
Browder 2012 {published data only}
- Browder D. Re: Cochrane Review request [personal communication]. Email to: C Lemons 17 February 2016.
- Browder D. Re: Cochrane Review request [personal communication]. Email to: C Lemons 22 January 2016.
- Browder D, Ahlgrim‐Delzell L, Flowers C, Baker J. An evaluation of a multicomponent early literacy program for students with severe developmental disabilities. Remedial and Special Education 2012;33(4):237‐46. [DOI: 10.1177/0741932510387305] [DOI] [Google Scholar]
- Browder DM, Ahlgrim‐Delzell L, Courtade G, Gibbs SL, Flowers C. Evaluation of the effectiveness of an early literacy program for students with significant developmental disabilities. Exceptional Children 2008;75(1):33‐52. [DOI: 10.1177/001440290807500102] [DOI] [Google Scholar]
- Lemons C. Cochrane Review request [personal communication]. Email to: D Browder 21 January 2016.
Burgoyne 2012 {published data only}
- Buckely S. Re: contact request to get a newer address for Kelly. Email to: C Lemons 9 November 2016.
- Burgoyne K, Duff FJ, Clarke PJ, Buckley S, Snowling MJ, Hulme C. Efficacy of a reading and language intervention for children with Down syndrome: a randomized controlled trial. Journal of Child Psychology and Psychiatry 2012;53(10):1044‐53. [DOI: 10.1111/j.1469-7610.2012.02557.x; PMC3470928; PUBMED: 22533801] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burgoyne K, Duff FJ, Clarke PJ, Buckley S, Snowling MJ, Hulme C. Reading and language intervention for children with Down syndrome: outcomes from a RCT. Journal of Intellectual Disability Research 2012;56(7‐8):696. [DOI: 10.1111/j.1365-2788.2012.01583_5.x] [DOI] [Google Scholar]
- Lemons C. Cochrane Review request [personal communication]. Email to: K Burgoyne 21 January 2016.
- Lemons C. Cochrane Review request [personal communication]. Email to: K Burgoyne 29 January 2016.
- Lemons C. Contact request to get a newer address for Kelly. Email to: S Buckley 9 November 2016.
Cleave 2011 {published data only}
- Cleave P. Re: Cochrane Review request [personal communication]. Email to: C Lemons 28 January 2016.
- Cleave PL, Bird EK, Bourassa DC. Developing phonological awareness skills in children with Down syndrome. Canadian Journal of Speech‐Language Pathology and Audiology 2011;35(4):332‐43. [cjslpa.ca/files/2011_CJSLPA_Vol_35/No_04_277‐371/Cleave_Kay‐Raining‐Bird_Bourassa_CJSLPA_2011.pdf] [Google Scholar]
- Lemons C. Cochrane Review request [personal communication]. Email to: P Cleave 21 January 2016.
Finnegan 2011 {published data only}
- Finnegan E. Re: Cochrane Review request [personal communication]. Email to: C Lemons 22 January 2016.
- Finnegan E. Re: Cochrane Review request [personal communication]. Email to: C Lemons 29 January 2016.
- Finnegan EG. Comparison of the Effects of Two Systematic Approaches of Phonics Instruction on the Ability of Children with Significant Cognitive Disabilities to Read Words [EdD thesis]. New York (NY): Teacher's College, Columbia University, 2011. [Google Scholar]
- Finnegan EG. Two approaches to phonics instruction: comparison of effects with children with significant cognitive disability. Education and Training in Autism and Developmental Disabilities 2012;47(3):269‐79. [DOI: ] [Google Scholar]
- Lemons C. Cochrane Review request [personal communication]. Email to: E Finnegan 21 January 2016.
Roberts‐Tyler 2019 {published data only}
- Roberts‐Tyler EJ, Hughes JC, Hastings RP. Evaluating a computer‐based reading programme with children with intellectual disabilities: feasibility and pilot research. JORSEN: Journal of Research in Special Education Needs 2019 Jun 10 [Epub ahead of print]. [DOI: 10.1111/1471-3802.12458] [DOI]
References to studies excluded from this review
Alfassi 2009 {published data only}
- Alfassi M, Weis I, Lifshitz H. The efficacy of reciprocal teaching in fostering the reading literacy of students with intellectual disabilities. European Journal of Special Needs Education 2009;24(3):291‐305. [DOI: 10.1080/08856250903016854] [DOI] [Google Scholar]
Van der Bijl 2006 {published data only}
- Bijl C, Alant E, Lloyd L. A comparison of two strategies of sight word instruction in children with mental disability. Research in Developmental Disabilities 2006;27(1):43‐55. [DOI: 10.1016/j.ridd.2004.12.001; PUBMED: 15939572] [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Hughes 1982 {published data only}
- Hughes JM, John MH. The design of schedules for the initial assessment of the phonic ability of primary ESN(M) pupils – followed by the development of appropriate teaching strategies – phase one of an IT/INSET project. Links 1982;8:29‐34. [Google Scholar]
Hughes 1984 {published data only}
- Hughes JM, John MH. The use of errorless discrimination procedures to help the severely mentally handicapped acquire a social sight vocabulary. Links 1984;9:14‐6. [Google Scholar]
Muter 1976 {published data only}
- Muter VA. An Investigation of Teaching Methods in an Operantly Based Remedial Spelling Programme [Masters thesis]. London (UK): University of London, Institute of Psychiatry, 1976. [Google Scholar]
Salario 1960 {published data only}
- Salario M. An Experimental Study to Determine the Value of an Extended Pre‐Reading Program with Primary Mentally Handicapped Children [Masters thesis]. Chicago (IL): Chicago Teachers College, 1960. [Google Scholar]
Additional references
AAIDD 2011
- American Association of Intellectual and Developmental Disabilities. Intellectual Disability: Definition, Classification, and Systems of Supports. 11th Edition. Washington (DC): American Association of Intellectual and Developmental Disabilities, 2011. [Google Scholar]
Adams 1990
- Adams MJ. Beginning to Read: Thinking and Learning about Print. Cambridge (MA): MIT Press, 1990. [Google Scholar]
Allor 2010
- Allor JH, Mathes PG, Roberts JK, Jones FG, Champlin TM. Teaching students with moderate intellectual disabilities to read: an experimental examination of a comprehensive reading intervention. Education and Training in Autism Spectrum Disorders 2010;45(1):3‐22. [www.jstor.org/stable/23880147] [Google Scholar]
APA 2000
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th Edition. Washington (DC): American Psychiatric Association, 2000. [Google Scholar]
Beadle‐Brown 2007
- Beadle‐Brown J, Mansell J, Kozma A. Deinstitutionalization in intellectual disabilities. Current Opinion in Psychiatry 2007;20(5):437‐42. [DOI: 10.1097/YCO.0b013e32827b14ab; PUBMED: 17762584] [DOI] [PubMed] [Google Scholar]
Borenstein 2009
- Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Chapter 24: multiple outcomes or time‐points within a study. In: Borenstein M, Hedges LV, Higgins JP, Rothstein HR editor(s). Introduction to Meta‐Analysis. London (UK): John Wiley & Sons, 2009:225‐38. [Google Scholar]
Browder 1998
- Browder DM, Xin YP. A meta‐analysis and review of sight word research and its implications for teaching functional reading to individuals with moderate and severe disabilities. Journal of Special Education 1998;32(3):130‐53. [DOI: 10.1177/002246699803200301] [DOI] [Google Scholar]
Browder 2006
- Browder DM, Wakeman SY, Spooner F, Ahlgrim‐Delzell L, Algozzine R. Research on reading instruction for individuals with significant cognitive disabilities. Exceptional Children 2006;72(4):392‐408. [Google Scholar]
Browder 2009
- Browder DM, Gibbs S, Ahlgrim‐Delzell L, Courtade GR, Mraz M, Flowers C. Literacy for students with severe developmental disabilities: what should we teach and what should we hope to achieve?. Remedial and Special Education 2009;30(5):269‐82. [DOI: 10.1177/0741932508315054] [DOI] [Google Scholar]
Brownell 2000
- Brownell R. Expressive and Receptive One Word Picture Vocabulary Tests. 2nd Edition. Novato (CA): Academic Therapy Publications, 2000. [Google Scholar]
Burgoyne 2009
- Burgoyne K. Reading interventions for children with Down syndrome. www.down‐syndrome.org/reviews/2128/reviews‐2128.pdf (accessed 1 April 2014).
Carnine 2010
- Carnine DW, Silbert J, Kame'enui EJ, Tarver SG. Direct Instruction Reading. Boston (MA): Merrill, 2010. [Google Scholar]
Carver 1994
- Carver C, Moseley D. A Group of Individual Diagnostic Test of Word Recognition and Phonic Skills (WRaPS). London (UK): Hodder & Stoughton, 1994. [Google Scholar]
Channell 2013
- Channell MM, Loveall SJ, Conners FA. Strengths and weaknesses in reading skills of youth with intellectual disabilities. Research in Developmental Disabilities 2013;34(2):776‐87. [DOI: 10.1016/j.ridd.2012.10.010; PMC4776650] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cohen 2001
- Cohen D, Riviére JP, Plaza M, Thompson C, Chauvin D, Hambourg N, et al. Word identification in adults with mild mental retardation: does IQ influence reading achievement?. Brain and Cognition 2001;46(1‐2):69‐73. [PUBMED: 11527367] [DOI] [PubMed] [Google Scholar]
Crumpler 2007
- Crumpler M, McCarthy C. Diagnostic Reading Analysis: Manual. 2nd Edition. Totten (UK): Hobbs the Printers Ltd, 2007. [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JP, Altman DG. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Deno 1985
- Deno SL. Curriculum‐based measurement: the emerging alternative. Exceptional Children 1985;52(3):219‐32. [PUBMED: 2934262] [DOI] [PubMed] [Google Scholar]
Dunn 1997
- Dunn LM. Peabody Picture Vocabulary Test. 4th Edition. Circle Pines (MN): American Guidance Service, 1997. [Google Scholar]
Dykens 1995
- Dykens EM. Measuring behavioral phenotypes: provocations from the "new genetics". American Journal on Mental Retardation 1995;99(5):522‐32. [PUBMED: 7779347] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne DR, Altman DG, Higgins JP, Curtin F, Worthington HV, Vail A. Meta‐analysis involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [PUBMED: 11914310] [DOI] [PubMed] [Google Scholar]
Ellis 2004
- Ellis NC, Natsume M, Stavropoulou K, Hoxhallari L, Daal VH, Polyzoe N, et al. The effects of orthographic depth on learning to read alphabetic, syllabic, and logographic scripts. Reading Research Quarterly 2004;39(4):438‐68. [DOI: 10.1598/RRQ.39.4.5] [DOI] [Google Scholar]
Gast 2014
- Gast DL, Ledford JR. Single Case Research Methodology: Applications in Special Education and Behavioral Sciences. 2nd Edition. New York (NY): Routledge, 2014. [Google Scholar]
Gersten 2005
- Gersten R, Fuchs LS, Compton DL, Coyne M, Greenwood C, Innocenti MS. Quality indicators for group experimental and quasi‐experimental research in special education. Exceptional Children 2005;71(2):149‐64. [DOI: 10.1177/001440290507100202] [DOI] [Google Scholar]
Good 2002
- Good RH, Kaminski RA. Dynamic Indicators of Basic Early Literacy Skills. 6th Edition. Eugene (OR): Institute for Development of Educational Achievement, 2002. [Google Scholar]
GRADEpro GDT [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 13 April 2017. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Hardman 2014
- Hardman ML, Drew CJ, Egan MW. Human Exceptionality: School, Community, and Family. 11th Edition. Belmont (CA): Wadsworth, 2014. [Google Scholar]
Hedges 1985
- Hedges L, Olkin I. Statistical Models for Meta‐analysis. New York (NY): Academic Press, 1985. [Google Scholar]
Higgins 2002
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. [DOI] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JP, Altman DG, Sterne JA. Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011b
- Higgins JP, Deeks JJ, Altman DG. Chapter 16: Special topics in statistics. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Horner 2005
- Horner RH, Carr EG, Halle J, McGee G, Odom S, Wolery M. The use of single‐subject research to identify evidence‐based practice in special education. Exceptional Children 2005;71(2):165‐79. [DOI: 10.1177/001440290507100203] [DOI] [Google Scholar]
Hougen 2012
- Hougen MC. Effective phonics instruction. In: Hougen MC, Smartt SM editor(s). Fundamentals of Literacy Instruction and Assessment, Pre‐K‐‐6. Baltimore (MD): Paul H Brookes Publishing Co, 2012. [Google Scholar]
Huang 2010
- Huang P, Blum NJ. Developmental and behavioral disorders grown‐up intellectual disability. Journal of Developmental and Behavioral Pediatrics 2010;31(1):61‐71. [DOI: 10.1097/DBP.0b013e3181c72401; PUBMED: 20081439] [DOI] [PubMed] [Google Scholar]
Hulme 2009
- Hulme C, Stothard SE, Clarke P, Bowyer‐Crane C, Harrington A, Truelove E, et al. York Assessment of Reading for Comprehension: Early Reading. London (UK): GL Assessment, 2009. [Google Scholar]
IASSID 2001
- International Association for the Scientific Study of Intellectual Disabilities. Mental health and intellectual disabilities: addressing the mental health needs of people with intellectual disabilities. Report to the World Health Organization. www.iassidd.org/ (accessed 12 May 2014).
Joseph 2004
- Joseph LM, Seery ME. Where is the phonics? A review of the literature on the use of phonetic analysis with students with mental retardation. Remedial and Special Education 2004;25(2):88‐94. [DOI: 10.1177/07419325040250020301] [DOI] [Google Scholar]
Katims 2000
- Katims DS. Literacy instruction for people with mental retardation: historical highlights and contemporary analysis. Education and Training in Mental Retardation and Developmental Disabilities 2000;35(1):3‐15. [Google Scholar]
Kirsch 2002
- Kirsch IS, Jungeblut A, Jenkins L, Kolstad A. Adult Literacy in America: a First Look at the Findings of the National Adult Literacy Survey. Washington (DC): National Center for Education Statistics, 2002. [Google Scholar]
Koritsas 2011
- Koritsas S, Iacono T. Secondary conditions in people with developmental disability. American Journal on Intellectual and Developmental Disabilities 2011;116(1):36‐47. [DOI: 10.1352/1944-7558-116.1.36; PUBMED: 21291309] [DOI] [PubMed] [Google Scholar]
Lemons 2010
- Lemons CJ, Fuchs D. Modeling response to reading intervention in children with Down syndrome: an examination of predictors of differential growth. Reading Research Quarterly 2010;45(2):134‐68. [DOI: 10.1598/RRQ.45.2.1] [DOI] [Google Scholar]
Lemons 2013
- Lemons CJ, Zigmond N, Kloo A, Hill DR, Mrachko AA, Paterra MF, et al. Performance of students with significant cognitive disabilities on early‐grade curriculum‐based measures of word and passage reading fluency. Exceptional Children 2013;79(4):408‐26. [DOI: 10.1177/001440291307900402] [DOI] [Google Scholar]
Lemons 2014
- Lemons CJ, Kearns DM, Davidson KA. Data‐based individualization in reading: intensifying intervention for students with significant reading disabilities. Teaching Exceptional Children 2014;46(4):20‐9. [DOI: 10.1177/0040059914522978] [DOI] [Google Scholar]
Lemons 2016
- Lemons CJ, Allor JH, Al Otaiba S, LeJeune LM. 10 research‐based tips for enhancing literacy instruction for students with intellectual disability. Teaching Exceptional Children 2016;49(1):18‐30. [DOI: 10.1177/0040059916662202] [DOI] [Google Scholar]
Levy 2011
- Levy Y. IQ predicts word decoding skills in populations with intellectual disabilities. Research in Developmental Disabilities 2011;32(6):2267‐77. [DOI: 10.1016/j.ridd.2011.07.043; PUBMED: 21862282] [DOI] [PubMed] [Google Scholar]
Luckasson 2002
- Luckasson R, Borthwick‐Duffy S, Buntinx WH, Coulter DL, Craig EM, Reeve A, et al. Mental Retardation: Definition, Classification, and Systems of Supports. Washington (DC): American Association on Mental Retardation, 2002. [Google Scholar]
Maulik 2011
- Maulik PK, Mascarenhas MN, Mathers CD, Dua T, Saxena S. Prevalence of intellectual disability: a meta‐analysis of population‐based studies. Research in Developmental Disabilities 2011;32(2):419‐36. [DOI: 10.1016/j.ridd.2010.12.018; PUBMED: 21236634] [DOI] [PubMed] [Google Scholar]
McArthur 2018
- McArthur G, Sheehan Y, Badcock NA, Francis DA, Wang HC, Kohnen S, et al. Phonics training for English‐speaking poor readers. Cochrane Database of Systematic Reviews 2018, Issue 11. [DOI: 10.1002/14651858.CD009115.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. PLoS Medicine 2009;6(7):e1000097. [DOI: 10.1371/journal.pmed.1000097; PMC2707599; PUBMED: 19621072] [DOI] [PMC free article] [PubMed] [Google Scholar]
National Reading Panel 2000
- National Reading Panel. Teaching Children to Read: an Evidence‐Based Assessment of the Scientific Research Literature on Reading and its Implications for Reading Instruction. Washington (DC): US Department of Health and Human Services, 2000. [Google Scholar]
No Child Left Behind Act of 2001
- No Child Left Behind Act of 2001. www.gpo.gov/fdsys/pkg/PLAW‐107publ110/html/PLAW‐107publ110.htm (accessed prior to 22 May 2017).
Perfetti 1998
- Perfetti CA, Marron MA. Learning to read: literacy acquisition by children and adults. In: Wagner DA editor(s). Advances in Adult Literacy Research and Development. New York (NY): Hampton Press, 1998. [Google Scholar]
Perfetti 2003
- Perfetti CA. The universal grammar of reading. Scientific Studies of Reading 2003;7(11):3‐24. [Google Scholar]
Polloway 2006
- Polloway EA, Smith JD. Biological aspects and the promises of prevention. In: Beirne‐Smith M, Patton JR, Kim SH editor(s). Mental Retardation: an Introduction to Intellectual Disability. 7th Edition. Columbus (OH): Pearson, 2006. [Google Scholar]
Polloway 2010
- Polloway EA, Lubin J, Smith JD, Patton JR. Mild intellectual disabilities: legacies and trends in concepts and educational practices. Education and Training in Developmental Disabilities 2010;45(1):54‐68. [Google Scholar]
Polloway 2011
- Polloway EA, Patton JR, Nelson MA. Intellectual and developmental disabilities. In: Kauffman JM, Hallahan DP editor(s). Handbook of Special Education. New York (NY): Routledge, 2011. [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rose 2009
- Rose J, Schools and Families Department for Children. The Independent Review of the Primary Curriculum: Final Report. Nottingham (UK): Department for Children, Schools and Families, 2009. [Google Scholar]
Rowe 2005
- Rowe KJ, National Inquiry into the Teaching of Literacy. Teaching Reading: Report and Recommendations. Barton (ACT): Australian Government Department of Education, Science, and Training, 2005. [Google Scholar]
Scammacca 2014
- Scammacca N, Roberts G, Stuebing KK. Meta‐analysis with complex research designs: dealing with dependence from multiple measures and multiple group comparisons. Review of Educational Research 2014;84(3):328‐64. [DOI: 10.3102/0034654313500826; PMC4191743; PUBMED: 25309002] [DOI] [PMC free article] [PubMed] [Google Scholar]
Scammacca 2015
- Scammacca NK, Roberts G, Vaughn S, Stuebing KK. A meta‐analysis of interventions for struggling readers in grades 4‐12: 1980‐2011. Journal of Learning Disabilities 2015;48(4):369‐90. [DOI: 10.1177/0022219413504995; PMC3975734; PUBMED: 24092916] [DOI] [PMC free article] [PubMed] [Google Scholar]
Scarborough 1990
- Scarborough HS. Very early language deficits in dyslexic children. Child Development 1990;61(6):1728‐43. [PUBMED: 2083495] [PubMed] [Google Scholar]
Schalock 2007
- Schalock RL, Luckasson RA, Shogren KA, Borthwick‐Duffy S, Bradley V, Buntinx WH, et al. The renaming of mental retardation: understanding the change to the term intellectual disability. Intellectual and Developmental Disabilities 2007;45(2):116‐24. [DOI: 10.1352/1934-9556(2007)45[116:TROMRU]2.0.CO;2; PUBMED: 17428134] [DOI] [PubMed] [Google Scholar]
Schalock 2011
- Schalock RL. The evolving understanding of the construct of intellectual disability. Journal of Intellectual and Developmental Disability 2011;36(4):227‐37. [DOI: 10.3109/13668250.2011.624087; PUBMED: 22029886] [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Vist GE, Higgins JP, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Shrank 2004
- Shrank FA, Mather N, Woodcock RW. Woodcock‐Johnson III Diagnostic Reading Battery. Rolling Meadows (IL): Riverside, 2004. [Google Scholar]
Snell 2009
- Snell ME, Luckasson R, Borthwick‐Duffy S, Bradley V, Buntinx WH, Coulter DL, et al. Characteristics and needs of people with intellectual disability who have higher IQs. Intellectual and Developmental Disabilities 2009;47(3):220‐33. [DOI: 10.1352/1934-9556-47.3.220; PUBMED: 19489667] [DOI] [PubMed] [Google Scholar]
Snow 1998
- Snow C, Burns MS, Griffin P. Preventing Reading Difficulties in Young Children. Washington (DC): National Academy Press, 1998. [Google Scholar]
Soltani 2013
- Soltani A, Roslan S. Contributions of phonological awareness, phonological short‐term memory, and rapid automated naming, toward decoding ability in students with mild intellectual disability. Research in Developmental Disabilities 2013;34(3):1090‐9. [DOI: 10.1016/j.ridd.2012.12.005; PUBMED: 23314249] [DOI] [PubMed] [Google Scholar]
Spooner 2011
- Spooner F, Brown F. Educating students with significant cognitive disabilities: historical overview and future projections. In: Kauffman JM, Hallahan DP editor(s). Handbook of Special Education. New York (NY): Routledge, 2011. [Google Scholar]
Stanovich 1985
- Stanovich KE. Cognitive determinants of reading in mentally retarded individuals. International Review of Research in Mental Retardation 1985;13:181‐213. [DOI: 10.1016/S0074-7750(08)60236-0] [DOI] [Google Scholar]
Steele 2013
- Steele A, Scerif G, Cornish K, Karmiloff‐Smith A. Learning to read in Williams syndrome and Down syndrome: syndrome‐specific precursors and developmental trajectories. Journal of Child Psychology and Psychiatry 2013;54(7):754‐62. [DOI: 10.1111/jcpp.12070; PUBMED: 23718731] [DOI] [PubMed] [Google Scholar]
Stein 2011
- Stein DS, Blum NJ, Barbaresi WJ. Developmental and behavioral disorders throughout the life span. Pediatrics 2011;128(2):365‐73. [DOI: 10.1542/peds.2011-0266] [DOI] [PubMed] [Google Scholar]
Sterne 2011
- Sterne JA, Egger M, Moher D. Chapter 10: Addressing reporting biases. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Suggate 2016
- Suggate SP. A meta‐analysis of the long‐term effects of phonemic awareness, phonics, fluency, and reading comprehension interventions. Journal of Learning Disabilities 2016;49(1):77‐96. [DOI: 10.1177/0022219414528540; PUBMED: 24704662] [DOI] [PubMed] [Google Scholar]
Torgesen 1994
- Torgesen JK, Bryant BR. Test of Phonological Awareness. Austin (TX): Pro‐Ed, 1994. [Google Scholar]
Torgesen 1999
- Torgesen JK, Wagner RK, Rashotte CA. The Test of Word Reading Efficiency. Austin (TX): Pro‐Ed, 1999. [Google Scholar]
Tunnicliffe 2011
- Tunnicliffe P, Oliver C. Phenotype‐environment interactions in genetic syndromes associated with severe or profound intellectual disability. Research in Developmental Disabilities 2011;32(2):404‐18. [DOI: 10.1016/j.ridd.2010.12.008; PUBMED: 21257289] [DOI] [PubMed] [Google Scholar]
Turner 2008
- Turner S, Alborz A, Gayle V. Predictors of academic attainments of young people with Down's syndrome. Journal of Intellectual Disability Research 2008;52(Pt 5):380‐92. [DOI: 10.1111/j.1365-2788.2007.01038.x; PUBMED: 18205756] [DOI] [PubMed] [Google Scholar]
United Nations Development Programme 2013
- United Nations Development Programme. Human Development Report 2013: the Rise of the South: Human Progress in a Diverse World. New York (NY): United Nations Development Programme, 2013. [Google Scholar]
US Census Bureau 2013
- United States Census Bureau. International programs: international data base. www.census.gov/programs‐surveys/international‐programs/about/idb.html (accessed 8 April 2019).
Valentine 2016
- Valentine JC, Tanner‐Smith EE, Pustejovsky JE, Lau TS. Between‐case standardized mean difference effect sizes for single‐case designs: a primer and tutorial using the scdhlm web application. Olso (NO): The Campbell Collaboration, 2016. [DOI: 10.4073/cmpn.2016.3] [DOI] [Google Scholar]
Vaughn 2012
- Vaughn S, Wanzek J, Murray CS, Roberts G. Intensive Interventions for Students Struggling in Reading and Mathematics: a Practice Guide. Portsmouth (NH): RMC Research Corporation, Center on Instruction, 2012. [Google Scholar]
Wagner 1999
- Wagner R, Torgesen J, Rashotte C. Comprehensive Test of Phonological Processing. Austin (TX): Pro‐Ed, 1999. [Google Scholar]
Wanzek 2018
- Wanzek J, Stevens EA, Williams KJ, Sammacca N, Vaughn S, Sargent K. Current evidence on the effects of intensive early reading interventions. Journal of Learning Disabilities 2018;51(6):612‐24. [DOI: 10.1177/0022219418775110; PMC6247899; PUBMED: 29779424] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wei 2011
- Wei X, Blackorby J, Schiller E. Growth in reading achievement of students with disabilities, ages 7 to 17. Exceptional Children 2011;78(1):89‐106. [DOI: 10.1177/001440291107800106] [DOI] [Google Scholar]
Weymeyer 2013
- Weymeyer ML. The Story of Intellectual Disability: an Evolution of Meaning, Understanding, and Public Perception. Baltimore (MD): Paul H Brookes Publishing Co, 2013. [Google Scholar]
WHO 2001
- World Health Organization. International Classification of Functioning, Disability and Health. Geneva (Switzerland): World Health Organization, 2001. [Google Scholar]
WHO 2007
- World Health Organization. Atlas: Global Resources for Persons with Intellectual Disabilities. Geneva (Switzerland): World Health Organization, 2007. [Google Scholar]
WHO 2010
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems. 10th Edition. Geneva (Switzerland): World Health Organization, 2010. [Google Scholar]
Williams 1997
- Williams KT. Expressive Vocabulary Test. Circle Pines (MN): American Guidance Services, 1997. [Google Scholar]
Woodcock 1987
- Woodcock RW. Woodcock Reading Mastery Tests. Revised. Circle Pines (MN): American Guidance Services, 1987. [Google Scholar]
Ziegler 2010
- Ziegler JC, Bertrand D, Tóth D, Csépe V, Reis A, Faísca L, et al. Orthographic depth and its impact on universal predictors of reading: a cross‐language investigation. Psychological Science 2010;21(4):551‐9. [DOI: 10.1177/0956797610363406; PUBMED: 20424101] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Reichow 2014
- Reichow B, Lemons CJ, Maggin DM, Hill DR. Beginning reading interventions for children and adolescents with intellectual disability. Cochrane Database of Systematic Reviews 2014, Issue 10. [DOI: 10.1002/14651858.CD011359] [DOI] [PMC free article] [PubMed] [Google Scholar]