

INTRODUCTION
Interventional EUS has seen exponential growth in its indications and applications in the last decade.[1,2,3] Dedicated endoscopic devices for EUS-guided interventions are still limited. Up until recently, the tools used have been borrowed from other procedures such as ERCP.
In interventional EUS, the linear-array echoendoscope allows a needle to be advanced under EUS-guidance from the upper gastrointestinal lumen to the biliary, pancreatic, or another adjacent intestinal lumen. Real-time puncture can be performed and provide the possibility of EUS-guided transluminal drainage (EUS-TLD). Plastic stents and conventional self-expandable metallic stents (SEMSs) were initially used but present several limitations due to their design.[1,4,5] They lack lumen-to-lumen anchorage and present migratory risks in the absence of stricture to hold them in place. Plastic stents are associated with potential pneumoperitoneum and bile peritonitis, whereas fully-covered SEMS (FCSEMS), despite preventing bile leak, will not maintain secure apposition between two nonadherent organs. Furthermore, their length often exceeds the anatomical requirement of a shorter transluminal anastomosis and predisposes them to obstruction as well as difficult positioning.
With the rise in new EUS-guided interventional techniques, new tools, in particular, new stent designs have evolved to facilitate the various applications. A few EUS-specific stents have now become available for EUS-TLD.[4,5] We hereby review the stent designs and discuss lacunae to be addressed to improve the efficacy, safety, and ease of procedures.
INDICATIONS OF EUS-TRANS-LUMINAL DRAINAGE
Until recently, the management of symptomatic peripancreatic fluid collections (PFCs), namely pancreatic pseudocysts (PP) and walled-off pancreatic necrosis (WON) included surgery and percutaneous drainage (PTD). These techniques although effective, incurred high rates of morbidity and mortality for surgery, and fistula formation as well as infection for PTD. EUS-guided drainage has become a minimally invasive standard first-line management of PFC.[2] Novel EUS-specific stent designs such as the lumen-apposing metal stents (LAMSs) are effective and safe in this indication.[6,7]
EUS-guided gallbladder drainage (EUS-GBD) was introduced for inoperable patients with acute cholecystitis and obstructive malignancies.[2] It is conceptually similar to PFC drainage; however, the noninflamed gallbladder is nonadherent to the bowel wall. Therefore, additional measures must be taken to avoid bile and gas leakage. Furthermore, the gallbladder is mobile, making it a difficult target for puncture. LAMSs appear to be safe and effective for EUS-GBD and avoid the complications of PTD such as hepatic hematoma, and pneumothorax. Furthermore, it can be performed despite perihepatic ascites and offers the advantage of direct therapy such as gallstone removal.[2,8]
ERCP is the standard of care for biliary drainage (BD) in a malignant biliary obstruction (MBO). Since the first report by Giovannini et al. in 2001,[9] EUS-BD has been developed as an alternative means of BD. EUS-BD can be performed through intrahepatic (transgastric-transhepatic) or extrahepatic (transenteric-transcholedochal) approaches.[2,10] Several methods have been described. Choledocoduodenostomy (EUS-CBD) and hepaticogastrostomy (EUS-HGS) are newer approaches which achieve extra-papillary drainage by transmural stenting. Distal MBO is the most frequent indication. Compared to percutaneous biliary drainage (PTBD) as salvage for failed ERCP, EUS-BD is as effective with less adverse events (AE), and lower reintervention rates.[11] A growing body of evidence suggests that EUS-BD may also be used as a first-line technique for BD with SEMS in MBO.[12,13] Compared to ERCP, it confers two important theoretical advantages: (1) it avoids papillary trauma and subsequent risk of pancreatitis; (2) it does not traverse the malignant stricture hence reducing the risk of tumor ingrowth that ultimately leads to stent dysfunction and reintervention. The use of LAMSs, in particular, electrocautery-enhanced (ECE) LAMSs has largely simplified the technique for EUS-choledochoduodenostomy (EUS-CDS) in distal MBO with the theoretical advantage of reducing bile leak and migration. Furthermore, LAMSs serve as a conduit for direct cholangioscopy and endoscopic therapy as required.[10] EUS-HGS enables transluminal stenting of the left biliary tree without traversing the stricture. It is a feasible choice for both distal and proximal MBO.[2,14] It can be combined with ERCP to drain both left and right hepatic ducts. The nonadherence of the liver to the stomach wall and constant motion may cause fatal migration and dislodgment of the trans-hepatic stent to occur.[14] Hybrid stents that are partially covered (PC) SEMS with a covered gastric portion and uncovered (UC) portion within the liver are recently developed specific stents for EUS-HGS.[1,14]
Indications and techniques for pancreatic duct drainage remain controversial.[1,2,5] EUS-guided pancreatic drainage as an alternative to surgery is an option when ERCP is not possible. The technique is challenging due to the small diameter and relatively short length of the pancreatic duct, as well as hard and nonadherent pancreatic parenchyma.[15] Dedicated devices are lacking; although, the use of novel plastic and FCSEMS has recently been described.[1,5,15]
Finally, off-label uses of LAMSs for EUS-guided trans-gastric ERCP (EDGE) in postbypass patients, gastrojejunostomy in gastric outlet obstruction, and the treatment of gastrointestinal strictures have been subject to recent publications, showing promising results.[3,4]
AVAILABLE DESIGNS OF EUS-SPECIFIC STENTS AND THEIR INDICATIONS
Lumen-apposing metal stents
LAMSs are a recently developed, revolutionary device, specifically designed for EUS-TLD with potential advantages compared to conventional stents. They are large in diameter facilitating both drainage and access to extraluminal structures and can appose 2 nonadherent structures, likely minimizing the risk of leakage. Finally, LAMSs offer a built-in single delivery system that simplifies stent placement. They have a short dumbbell-shaped design with wide flanges on either end. The stents are fully silicone covered, and made of a self-expanding nitinol (nickel-titanium alloy) mesh, which provides flexibility and excellent radial force. The thermal shape memory characteristics of nitinol cause the released stent to expand into its predetermined dimension at body temperature. The silicone membrane minimizes leakage. The flanges disperse pressure uniformly on the luminal wall with enough physical force to hold the tissue wall in apposition and create a secure anastomose between two nonadherent lumens.[16,17] LAMSs were initially designed for drainage of PFCs, and to offer access for performing direct endoscopic necrosectomy (DEN). Indications have expanded to the biliary and enteric system.[2,3,16]
There are different types of LAMSs commercially available. Their characteristics are summarized in Table 1.
Table 1.
Summary of features of lumen apposing metal stent all in nitinol fully silicone covered
| Stent brand | Stent (flange) diameter (mm) | Stent length (mm) | Catheter diameter (Fr) | Deployment | Studied applications | LAF (Newton) |
|---|---|---|---|---|---|---|
| AXIOS™ (Boston Scientific) | 6 (14), 8 (17), 10 (21), 15 (24), 20 (29) | 8, 10 | 10.8 | TTS, single-step delivery with ECE-LAMS | PFC, EUS-CDS, EUS-GBD, EUS-GJ, EUS-GG | 2.29 |
| SPAXUS™ (Taewoong Medical) | 8 (23), 10 (25), 16 (31) | 20 | 10 | TTS | PFC, EUS-GBD, EUS-GJ | 1.76 |
| NAGI™ (Taewoong Medical) | 10 (26), 12 (26), 14 (26), 16 (26) | 10, 20, 30 | 9, 10 | TTS | PFC, EUS-GBD | 1.08 |
| Aixstent® (Leufen Medical) | 10 (25), 15 (25) | 30 | 10 | TTS | PFC | |
| Plumber® stent (MI Tech) | 12 (24), 14 (26), 16 (28) | 10, 20, 30 | 10.2 | TTS | PFC |
LAMS: Lumen-apposing metal stents, TTS: Through-the-scope, ECE: Electrocautery-enhanced, PFC: Peripancreatic fluid collection, EUS-CDS: EUS-guided choledochoduodenostomy, EUS-GBD: EUS-guided gallbladder drainage, EUS-GG: EUS-guided gastro-gastrostomy, EUS-GJ: EUS-guided gastro-jejunostomy, LAF: Lumen-apposing force (only available for 3 LAMSs as per study by Teoh et al.)
Available lumen-apposing metal stents
AXIOS™ stent (Boston Scientific Marlborough, MA, USA)
The delivery part of the device consists of a handle mechanism that allows a two-step release of each flange under EUS and endoscopic guidance.[4] In “cold” AXIOS™, preliminary tract dilation by bougienage, balloon dilation, or cautery is needed to allow advancement of the catheter across tissue planes in the target lumen. A tapered “nosecone” at the catheter tip facilitates passage across the wall after dilation. The handle of the AXIOS™ delivery system is Luer-locked onto the echoendoscope instrumentation channel, similar to a fine-needle aspiration (FNA) needle, which allows full control by the operator on deployment with the right hand. The handle consists of a distal portion for catheter control and a proximal portion for stent control. Advancement of the “catheter control hub” along the distal portion advances the catheter into the target lumen. The catheter position is then secured when the desired position is achieved by activating the “catheter lock.” The stent deployment hub is retracted to the halfway park and retracts the catheter sheath to deploy the distal stent anchor in the target lumen. The “stent deployment hub” is then retracted to deploy the proximal anchor in the bowel lumen. Two radiopaque markers enable fluoroscopic control of stent position if needed. The ability to deploy the distal and proximal stent anchors independently of each other in a two-step sequence with a “block” after releasing the distal anchor is unique to the AXIOS stent. Thus, unintended deployment of the proximal anchor is prevented [Figure 1].
Figure 1.
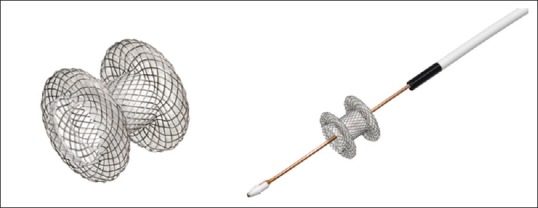
Hot AXIOS™ fully deployed (left) and with electrocautery- enhanced delivery system (right). Image provided by courtesy of Boston Scientific. ©2019 Boston Scientific Corporation or its affiliates. All rights reserved
The Hot AXIOS™ (an ECE-LAMSs) is the new version of the stent. The delivery system has an integrated cautery in the nosecone at the tip of the catheter. The cautery system consists of two radially distributed diathermic wires converging around the guide wire lumen to optimize current density and provide a clean, sharp cut with minimal coagulation effect. The result is a single-step puncture and release of the stent in the target lumen without the need for preliminary dilation, hence decreasing the number of accessory exchanges, and reducing the potential of complications.[4] The hot AXIOS™ can either be inserted over the wire after puncturing the target with a 19G FNA needle or placed directly without a guide wire.
Spaxus™ stent (Taewoong Medical Co., Ltd., Ilsan, Korea)
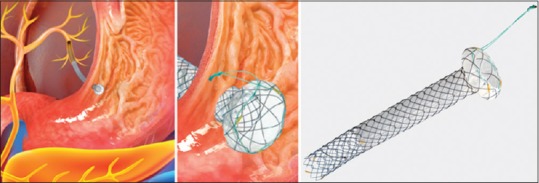
The unique feature of these stents is that the flanges fold back once fully deployed, which aims to enhance lumen apposition and prevent migration. When the outer X-ray marker overlaps with the inner X-ray marker, the distal flange is entirely open. Furthermore, there is a blue marker on the outer sheath to endoscopically confirm the complete deployment of the distal flange [Figure 2].
Figure 2.
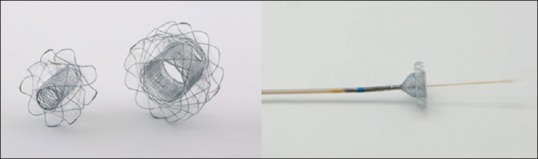
Spaxus™ stent fully deployed (left) and partially deployed (right) with outer sheath blue marker visible. Image provided by courtesy of Taewoong Medical
NAGI™ stent (Taewoong Medical Co., Ltd., Ilsan, Korea)
Eight radio-opaque markers located at both ends and in the middle allow accurate fluoroscopic positioning. A suture is attached at the distal flange to remove the stent [Figure 3].
Figure 3.

Nagi™ stent fully deployed (left) and partially deployed in the delivery catheter (right). Image provided by courtesy of Taewoong Medical
Plumber® stent (MI Tech, Seoul, Korea)
The wide lumen diameter allows effective drainage, and the short body length, as well as high stability, enables easy insertion of a standard upper endoscope into the cyst for DEN. The delivery system is similar to that of a conventional biliary metal stent. A strong lasso is attached to one end of the covered stent to enable accurate repositioning or removal with ease. Twelve gold radio-opaque markers are located at the distal, proximal, and central points of the stent to ensure excellent visualization under fluoroscopy for precise positioning. The delivery device has a soft and atraumatic radiopaque olive tip. Through the scope, delivery can be fully resheathed if required with clear “point of no return” markers [Figure 4].
Figure 4.
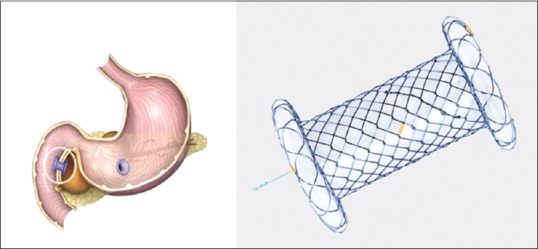
Plumber stent for peripancreatic fluid collection drainage (left), fully deployed stent (right). Image provided by courtesy of MI Tech
Aixstent® (Leufen Medical, Aachen, Germany)
The Aixstent® is a fully silicone covered nitinol stent with diabolo design and wide flanges on each end. Three tantalum radiopaque markers at either end of the stent ensure accurate fluoroscopic positioning.
Comparative lumen-apposing metal stents efficacy
Although it has been claimed that LAMSs have lumen-apposing properties, there are limited data objectively measuring such properties. Furthermore, the organs used for creating anastomoses could change the lumen-apposing effect of the stent. Teoh et al. performed an ex vivo study comparing the lumen-apposing force (LAF) of three LAMSs (AXIOS™ [Boston Scientific Marlborough, MA, USA], NAGI™ [Taewoong Medical Co., Ltd., Ilsan, Korea], Spaxus™ [Taewoong Medical Co., Ltd., Ilsan, Korea]) in four types of anastomosis (cholecystoduodenal, cholecystogastric, gastrogastric, and gastrojejunal) using porcine tissue.[17] These were compared to hand-sewn equivalent anastomoses. The outcome parameter was the LAF created by each type of stent. Sixty-four anastomoses were created. Regardless of the type of anastomosis, the difference between stents persisted with the AXIOS™ and the Spaxus™ stent showing higher LAF than the NAGI™ stent design. On the other hand, the LAF created by hand-sewn anastomoses was significantly higher than that for all stents across all types of anastomoses. The authors concluded that the AXIOS™ and Spaxus™ had a higher LAF and should be favored for performing EUS-guided trans-mural anastomoses in nonadherent organs.
Indications of lumen apposing metal stents
EUS-guided peri-pancreatic fluid collection drainage
The LAMSs length can accommodate combined GI tract and fluid collection wall thickness up to 10 mm as assessed by EUS during the procedure. The recommended stent size selection for PFC depends on the size and content of the latter. In the presence of necrotic material, a 15-mm diameter is better than 10 mm as an access port to perform debridement, irrigation, and cystoscopy. The stent is intended for implantation up to 60 days and should be removed on confirmation of pseudocyst or WON resolution. Contraindications are cystic neoplasms, pseudoaneurysms, duplication cysts, noninflammatory fluid collections, abnormal coagulopathy, altered anatomy, intervening gastric varices, and anaphylactic reaction to the stent material (nickel, titanium, and silicone).
A systematic review and meta-analysis by Hammad et al. evaluating the efficacy and safety of LAMSs in PFC[7] showed that among 11 studies (n = 688), weighted pool rate (WPR) for technical success was 98% (96, 99%), (I2 = 15%), and for clinical success 93% (89, 96), (I2 = 50%). There was no difference in clinical success for PP versus WON. WPR for AE was 13% (9; 20%), (I2 = 64%). AE were 10% more in WON compared to PP. The most common AE requiring intervention was stent migration (4.2%), infection (3.8%), bleeding (2.4%), and stent occlusion (1.9%). Six studies (n = 504) compared LAMSs to multiple plastic stents. Pooled RR for technical success was 1.71 (0.38, 7.37). Pooled RR for clinical success was 0.37 (0.2, 0.67) in favor of LAMSs. Pooled RR for AE was 0.39 (0.18, 0.84), (I2 = 50%). The authors concluded that LAMSs had a better clinical success and safety profile compared to plastic stents. In another recent large multicenter, international, retrospective study (n = 205), Yang et al. also showed better clinical success and AE profile of LAMSs compared to plastic stents.[18] Furthermore, an international multi-center consensus concluded that LAMSs was the most appropriate stent for EUS-drainage of WON and that larger LAMSs were preferred for this indication.[19] Itoi et al. showed that with the AXIOS stent, DEN could immediately be performed at the index procedure as anchoring flanges reduced the risk of migration.[20] However, other experts would allow a few days before performing such procedures.
Although several studies show the efficacy of LAMSs in PFC drainage, few reports have focused on AE. There is no standardized definition of complications in the various studies; however, the most commonly encountered AE with LAMSs in PFC drainage are bleeding, stent migration or dislodgment, buried stents, stent occlusion, and perforation.
In a randomized trial by Bang et al. (n = 31) comparing LAMSs to plastic stents in WON,[21] significant stent-related bleeding was observed at ≥3 weeks postintervention in the LAMSs cohort resulting in interim audit and protocol amendment. There was no significant difference in AE between cohorts after protocol amendment whereby a computed tomography scan was obtained at 3 weeks followed by LAMSs removal if WON had resolved. In this study, procedure time was shorter with LAMSs, but there was no significant difference between the two cohorts in the total number of procedures performed, clinical success, AE, readmission, length of hospital stay, and overall treatment costs. LAMSs-related early and late bleeding has been observed.[21,22] Bleeding may be due to the inherent property of LAMSs that confers its fixed lumen-apposing anchorage and rapid collapse of the PFC, resulting in impingement of vasculature within the wall of the PFC. Plastic stents, on the other hand, are softer and more flexible and tend to migrate to the gut lumen as WON resolves. Finally, the flanged ends of LAMSs are intended to anchor the stent in place; however, migration rates have been reported up to 19% and can occur either into the cyst cavity or back into the gut lumen. Migration can be immediate or deferred. Repeated DEN of WON can also cause displacement of the stent.
EUS-guided gallbladder drainage
A meta-analysis and systematic review by Kalva et al. evaluating the efficacy and safety of LAMSs in EUS-GBD, showed that pooled proportion of technical success was 93.86% (95% confidence interval [CI] = 90.56–96.49), and clinical success was 92.48% (95% CI = 88.9–95.42).[23] Overall complication rate was 18.31% (95% CI = 13.49–23.68), and stent-related complication rate was 8.16% (95% CI = 4.03–14.96) with perforation 6.71% and recurrent cholangitis/cholecystitis 4.05%. With Hot AXIOS™, which avoids tract dilation, a multicenter study by Dollhopf et al. (n = 75) showed that for the treatment of acute cholecystitis in patients with high surgical risk, technical and clinical successes were 98.7% and 95.9%, respectively.[24] Overall AE was 10.7%. For procedure-related AE, there was 1 perforation and 1 major bleed. Other short- and long-term AE were 3 recurrent cholecystitis, 2 stent migrations and 1 Bouveret syndrome. A recent systematic review by Anderloni et al. showed a safer outcome of EUS-GBD with LAMSs compared to SEMS or plastic stents.[8] EUS-GBD with LAMSs was shown to be as effective as PTD and may also result in shorter length of hospitalization, less repeat interventions and less adverse events.[25]
EUS-guided choledochoduodenostomy
In EUS-CDS, the most frequent complications are pneumoperitoneum and biliary leak predominantly occurring with plastic or UCSEMS.[26] PC and FCSEMS may still be complicated by bile or air leakage during track dilation. The AXIOS™ stent is the only LAMSs to have been evaluated in EUS-CDS. The AXIOS™ stents with diameters of 6 and 8 mm and saddle length of 8 mm are custom designed for EUS-CDS. In comparison to other drainage procedures, it confers the advantages of a significantly reduced procedure time, the possibility of fluoroless BD, and reduced adverse events, in particular for biliary leakage and migration. Selecting patients with a common bile duct dilation of at least 15-mm diameter, and distal MBO below mid common bile duct appears to be effective measures to reduce procedure-related complications.[27]
The Hot AXIOS™ also removes the need for tract dilation, and numerous guide-wire exchanges, potentially reducing complications. Data on LAMSs show excellent efficiency and safety profile EUS-CDS in distal MBO:
A multicenter, retrospective study by Kunda et al. (n = 57)[28] showed that EUS-CDS with AXIOS™ or Hot AXIOS™, had a technical success rate of 98.2% (56/57) and clinical success rate of 94.7% (54/57). Mean procedure time was 22.4 min. Overall AE rate was 7% with 2 duodenal perforations, 1 bleed, and 1 transient cholangitis. During follow-up, 9.3% (5/54) with clinical success required reintervention for 1 stent migration and 4 sump syndromes.
A recent multicenter, retrospective study by Jacques et al. (n = 52)[27] showed that EUS-CDS with Hot AXIOS™ had a technical success of 88.5% (46/52), and clinical success rate of 100% (46/46). Mean procedure time was 10.2 min. About 3.8% (2/46) of patients presented short-term complications (1 bleed and 1 cholangitis due to obstructive bezoar). Long-term AE were 13.5% including 6 (11.5%), recurrent jaundice due to 4 tumor obstructions, and 2 sump-syndromes. One patient experienced stent migration at 6 weeks. In univariate analyses, a small common bile duct diameter and not following the recommended procedure technique were significant risk factors for technical failure. Median survival time without biliary complications was 135 days. Interestingly, expert and nonexperts performed the procedure; however, no difference in technical or clinical success was found in the two groups. Finally, 2 patients underwent pancreaticoduodenectomy with no interference of the stent on the procedure.
EUS-guided entero-enteric anastomoses (off-label use)
Itoi et al. published the first prospective study (n = 20) using LAMSs for gastro-jejunostomy in malignant gastric outlet obstruction.[29] The technical success rate was 90%; however, 2 failures were due to mis-deployment of the distal flanges resulting in pneumoperitoneum and perforation. A multicenter retrospective study by Chen et al. also showed the high technical success of 96.2% and clinical success of 84% using LAMSs in benign gastric outlet obstruction.[30]3 AE were noted: 2 mis-deployments and 1 gastric leak. For gastro-gastric fistula as part of the EDGE procedure, Kedia et al. showed technical success in 5/5 cases.[31] ERCP could be performed through LAMSs during the index procedure in 3/5 cases. Two cases required re-stenting, but there were no major adverse events. In a larger multicenter study by Bukhari et al., comparing EDGE, to enteroscopy-assisted ERCP in Roux-en-Y bypass patients showed that EDGE had higher technical success and shorter procedure time with similar adverse events rate.[32]
In summary, LAMSs are EUS-specific stents with distinct design features: large diameter, a short length, and bi-flanged ends. Furthermore, their design is aimed to hold tissue wall in apposition, but currently, no definition of the force generated by LAMSs is available, in particular during peristalsis. LAF can vary due to differences in the design of flanges, such as angulation, size, and shape. The configuration and shape of the organ involved, as well as wall thickness, could also impact on LAF. LAMSs have been most extensively studied in the indications of PFC drainage and EUS-CDS. They appear to be an effective and safe option compared to conventional stents for draining PFC, although, by virtue of their design, they may carry an increased risk of bleeding. ECE-LAMSs are a significant milestone in EUS-CDS. The advantages are the reduction in leak and migration as well as reduced procedure time. Further randomized studies, comparing ECE-LAMSs with ERCP are required to validate its safety and efficacy as a first-line procedure for biliary decompression. Finally, further prospective studies examining the efficacy and safety profile of off-label uses of LAMSs such as enteral anastomosis are also necessary.
Hybrid stents
EUS-HGS is useful in the palliative drainage of distal or proximal MBO when ERCP is not suitable. Various stents have been tried in this technique. FCSEMS compared to plastic stents present the advantages of a larger caliber, reduced risk of bile leak, longer stent patency, and tamponade effect in case of intraprocedural bleeding. Disadvantages of FCSEMS are the cost, stent shortening, and obstruction of biliary side branches. On the other hand, UC SEMS present the disadvantages of bile leak, higher risk of tumor ingrowth, as well as being difficult to remove. Until recently, these limitations were overcome by inserting an FCSEMS into a UCSEMS with the drawback of multiple manipulations and costs.[14,33,34] These shortcomings led to the development of novel “hybrid” metal stents.[14,34] Hybrid stents are PC SEMS, which are fully covered at the distal portion to prevent bile leakage, and UC at the proximal portion to prevent biliary side branch obstruction. Furthermore, they have anti-migratory mechanisms (flaps or flares) and present sufficient stent length to prevent proximal migration into the peritoneum.
Available hybrid stents
There are a few hybrid metal stents, and their characteristics are summarized in Table 2.
Table 2.
Summary of features of hybrid stents all in nitinol partially silicone covered
| Stent brand | Stent diameter (mm) | Covered length (mm) | Stent length (cm) | Catheter diameter (mm) | Anchoring | Deployment | Studied applications | Comments |
|---|---|---|---|---|---|---|---|---|
| GIOBOR™ (Taewoong Medical) | 8, 10 | 40, 50 | 8, 10 | 8.5 | Flared gastric end | TTS | EUS-HGS | Lasso |
| Hanarostent BPD® (MI Tech) | 10 | 30 | 8, 10 | 8.5 | Flared gastric flap | TTS | EUS-HGS | Lasso |
| Hybrid Stent (Standard Sci Tech Inc) | 8, 10 | 35 | 5-10 | 8 | Anti-migratory flaps | TTS | EUS-HGS, EUS-CDS | |
| DEUS delivery + premounted stent (Standard Sci Tech Inc) | 6 | 35-85 | 5-10 | 3/4 tip 7 body | Anti-migratory flaps | TTS, all-in-one delivery system | EUS-HGS, EUS-CDS | Distal funnel-shaped uncovered wire mesh |
TTS: Through-the-scope, EUS-CDS: EUS-guided choledochoduodenostomy, EUS-HGS: EUS-guided hepaticogastrostomy
GIOBOR™ (Taewoong Medical Co., Ltd., Ilsan, Korea)
There are three radiopaque markers at both ends and two in the middle. The flexible design and material conforms to the curved track from the stomach to the left hepatic duct. It also has a single lasso for possible retrieval. The choice of stent length is decided according to patient anatomy and characteristics so that the intra-gastric portion is at least 2 cm to reduce the risk of stent migration [Figure 5].
Figure 5.
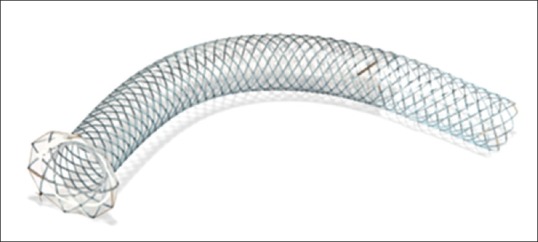
Giobor™ stent deployed with covered and uncovered portion as well as flared gastric end. Image provided by courtesy of Taewoong
Hanarostent BPD® (MI Tech, Seoul, Korea)
The UC intra-hepatic portion is 30 mm in length while the distal trans-gastric silicone-covered portion is 50 mm in length. The stent has a diameter of 10 mm × 10 mm with an anti-migration rivet-type flared flap of 20 mm at the gastric extremity. The 12 gold radio-opaque markers show each end and the margins of the covered section under fluoroscopy. The proximal repositioning lasso also aids repositioning if required (however it can potentially increase the risk of displacement during the procedure). The stent can be fully resheathed during delivery up to 70% deployment [Figure 6].
Figure 6.
Hanarostent BPD® depicted as deployed in situ of a hepatico-gastrostomy (left), stent deployed presenting a covered and uncovered portion as well as flared gastric end (right). Image provided by courtesy of Taewoong
Hybrid Stent (Standard Sci Tech Inc., Seoul, South Korea)
The hybrid stent has been commercially available in Korea since 2015. It is unavailable in Europe and the USA The hook and cross wire nitinol structure (polygon mesh surface) reduces the rate of shortening to achieve accurate positioning, reduce ingrowth in the small cavities, and to optimize radial and returning forces for conformability and for segmental compression. The hybrid stent is used for EUS-HGS and EUS-CDS. It has an UC part with a variable length of 15-65 mm, and silicone-covered part 35 mm long. Furthermore, there are four anti-migratory flaps to anchor around the covered portion to reduce inward migration and stent deviation. Finally, the radiopaque markers between covered and UC portions assist in accurate positioning.
DEUS delivery system (Standard Sci Tech Inc., Seoul, South Korea)
The one-step EUS-BD with a dedicated introducer, DEUS, was developed specifically for EUS-CDS and EUS-HGS.[35] The introducer has a 3Fr and 4Fr tapered pentagonal metal tip for simple one-step transluminal stenting after EUS-guided needle puncture. Neither graded dilatation nor cautery incision is necessary with this device as the tapered metal tip reduces wall resistance. The 7F outer sheath delivery catheter further enhances pushability during the one-step tract puncture over the guide wire. A preloaded hybrid stent is premounted on the DEUS delivery device. The stent has an UC portion 15 mm in length. The proximal anchoring flaps and distal funnel-shaped UC wire mesh in the bile duct portion are features to reduce stent migration.
Indications of hybrid stents
Hybrid stents are specifically used for EUS-BD, in particular, EUS-HGS. Although it is generally admitted that EUS-HGS is technically more challenging than EUS-CDS, it remains an attractive complementary technique particularly for BD of complex proximal MBO. In EUS-HGS, needle puncture into the peritoneal cavity increases the risk of pneumo-peritoneum and bile leak. The movement of the liver during respiration may contribute to stent migration, resulting in leak and bilio-enteric trauma.[14] Finally, the smaller intra-hepatic duct caliber precluding the placement of a wider metallic stent may also cause incomplete sealing of the bilio-enteric fistula. A systematic review by Alvarez-Sánchez et al.[27] showed that adverse event rates were higher for intrahepatic (18%) compared to the extrahepatic (14%) approach. EUS-HGS dedicated hybrid stents and one-step delivery systems have helped circumvent some of the difficulties in these procedures.[34,35,36,37]
In a retrospective study by De Cassan et al., the Giobor™ stent for EUS-HGS was evaluated in a single-center (n = 41).[34] The technical success was 90.2%, and the functional success was 65%. About 31.7% early complications were noted, mostly infection (21.9%) followed by stent migration (4.9%), and hemorrhage (4.9%). At 6 months follow-up, 27% required re-intervention due to stent migration in 1 patient and cholangitis in 9 patients (secondary to stent obstruction in 4 patients and obstruction other than stent in 4 patients and both in 1 patient). 29.7% of patients died of the underlying disease.
In a prospective study by Cho et al. (n = 54), the hybrid stent was used for EUS-BD.[36] The technical and clinical success was 100% and 94.4%, respectively. Immediate AE developed in 16.6% (3 cholangitis, 2 bleeding, 3 self-limited pneumoperitoneum, and 1 abdominal pain). Proximal or distal stent migration did not occur over the follow-up period (median 148.5 days). Stent patency was 166.3 days for EUS-HGS and 329.1 days for EUS-CDS.
In the multicenter randomized trial by Lee et al. (n = 66) comparing EUS-BD versus PTBD for distal MBO after failed ERCP, the all-in-one DEUS introducer with a premounted hybrid stent was used.[37] The study showed that technical and functional success in the EUS-BD group (94.1%, and 87.5%, respectively) was similar to the PTBD group. On the other hand, AE were less in the EUS-BD compared to the PTBD group (8.8% vs. 31.2%, P = 0.022). AE in the EUS-BD were mild in degree (1 pancreatitis, 1 self-limited pneumoperitoneum, 1 bile leak). Reintervention in the EUS-BD group was 25% versus 54.8% in the PTBD group (P = 0.015). Median stent patency was comparable in both groups (228 vs. 220d, P = 0.848). The authors attributed the low adverse events rate to the simplified procedure with the novel DEUS device, which did not require additional fistula tract dilation.
In a larger multicenter randomized noninferiority study by Paik et al. (n = 125), EUS-BD was compared to ERCP in palliative drainage of distal MBO.[13] The all in one DEUS introducer and a premounted stent was used. Technical success rates were 93.8% vs. 90.2% (P = 0.003), and clinical success rates 90% versus 94.5% (P = 0.49) for EUS-BD and ERCP respectively. EUS-BD had lower rates of overall AE (6.3% vs. 19.7% P = 0.03) including post-procedure pancreatitis (0 vs. 14.8%), and re-intervention (15.6 vs. 42.6%). EUS-BD had higher rates of stent patency (85.1% vs. 48.9%). Median procedure time was significantly shorter in EUS-BD (5 min vs. ERCP 11 min, P < 0.001).
In summary, data on EUS-HGS specific stents remain sparse. All-in-one dedicated devices could facilitate the application of this technique while reducing the risk of AE. Furthermore, certain devices can be used for both EUS-HGS and EUS-CDS. The development of effective all-in-one devices for EUS-BD as well as prospective comparative studies between available devices and ERCP should be a future goal.
Plastic stents for EUS-guided pancreatic duct drainage
There are few dedicated devices for EUS-guided pancreatic duct drainage. One such device is a newly designed plastic 7Fr single pigtail stent with a total length of 20 cm and an effective length of 15 cm (CX-T stent, TYPE IT, Gadelius Medical Co., Tokyo, Japan).[38] The stent has a pigtail anchor in the proximal end and four internal flanges (2 distal and 2 proximal). There are no holes in the middle part of the stent to prevent pancreatic juice leakage. This stent also has a straight and tapered tip to improve pushability compared to standard pancreatic stents and thus its ability to traverse strictures. A study by Matsunami et al. (n = 30),[39] evaluating this stent showed 100% technical and early clinical success rate. AE occurred in 23.3% patients, namely self-limited abdominal pain, mild pancreatitis, and bleeding. Two patients died of primary disease, and 3 were lost to follow-up. Patients were followed up for a median of 23 months, and spontaneous dislodgement was observed in 6 patients. Twelve patients (48%) had regular stent exchange 1 year after the initial intervention. Finally, 9 patients (36%) had complete stent removal either intentionally or by spontaneous dislodgement without any symptoms.
LACUNAE
Despite the excellent results of LAMSs in EUS-guided PFC drainage, these stents come with their own specific complications. Namely, the use of LAMSs in draining WON can cause significantly delayed bleeding and buried bump syndrome by virtue of their strong anchorage. This issue could be addressed with the development of nontraumatic flanges and improved flexibility of materials used.
With regard to EUS-BD, stent designs must consider that the stricture site is not traversed; hence, additional stabilizing measures are necessary. Despite the theoretical lumen-apposing ability of LAMSs, migration remains a complication that must be addressed. Future stent designs should also consider that LAMSs are placed perpendicularly in the bile duct and may this disturb the bile flow leading to the sump syndrome. EUS-CDS compatible hybrid stents appear to have reduced this complication as the stents are UC in the biliary portion and placed in the natural direction of the bile flow. Stent obstruction by alimentary debris may also require prophylactic measures in the design, such as a valve mechanism. Finally, the large and stiff delivery catheter of LAMSs is a technical drawback for EUS-CDS that is not seen with the smaller and more flexible all-in-one DEUS delivery system.
Concerning LAMSs for gastrojejunostomy, a wider lumen would appear to be an advantage to prevent food impaction. However, stent diameter is currently limited by the delivery system. Newer stent designs offering a larger diameter would be a future goal, but the main challenge is to stabilize the jejunum to allow the initial penetration of the system after passing through the stomach.
Concerning EUS-guided pancreatic duct drainage, all-in-one devices such as the DEUS used in EUS-HGS would facilitate this technically demanding procedure.
Data are lacking with regard to the learning curve for EUS-TLD. A prospective study by Oh et al. (n = 129)[40] showed that 33 EUS-BD procedures were required to reach a stabilization level in terms of AE and to reduce procedure time. Concerning Hot AXIOS™, a second follow-up study by Jacques et al. (n = 61) re-examined its efficacy in distal MBO after a year of further experience.[41] This study under abstract form showed 98.4% technical and clinical success, 1.6% procedure-related complication (1 bleed during fistulotomy, which was self-limited with the expansion of the stent), 0% early complications. Thus when experience with Hot AXIOS™ was acquired for EUS-CDS, this technique was effective and safe for BD.
EUS-TLD comprises a number of complex procedures. Some data indicate that all-in-one devices reduce complications as well as procedure time.[13,27] The widespread commercialization of certain devices currently limited to some countries would be necessary to confirm their efficacy and safety. Finally, the industry should focus on developing more all-in-one devices catered for specific EUS-TLD techniques.
CONCLUSION
EUS-TLD has revolutionized the approach to pancreato-biliary disease. With the advent of new EUS-specific devices, EUS-TLD has already replaced interventional radiology and surgery in centers with interventional endoscopic expertise. With improved EUS-specific stent designs and increasing experience, EUS-TLD is a promising technique with expanding indications. In addition to refining the design of EUS-specific devices to improve safety, and ease of application, emphasis should be placed on procedure standardization, appropriate training, and cost-effectiveness.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Dhir V, Isayama H, Itoi T, et al. Endoscopic ultrasonography-guided biliary and pancreatic duct interventions. Dig Endosc. 2017;29:472–85. doi: 10.1111/den.12818. [DOI] [PubMed] [Google Scholar]
- 2.Teoh AY, Dhir V, Kida M, et al. Consensus guidelines on the optimal management in interventional EUS procedures: Results from the Asian EUS group RAND/UCLA expert panel. Gut. 2018;67:1209–28. doi: 10.1136/gutjnl-2017-314341. [DOI] [PubMed] [Google Scholar]
- 3.Saumoy M, Yarber C, Kahaleh M. Novel uses of lumen-apposing metal stents. Gastrointest Endosc Clin N Am. 2018;28:197–205. doi: 10.1016/j.giec.2017.11.007. [DOI] [PubMed] [Google Scholar]
- 4.Weilert F, Binmoeller KF. Specially designed stents for translumenal drainage. Gastrointest Interv. 2015;4:40–5. [Google Scholar]
- 5.Mangiavillano B, Pagano N, Baron TH, et al. Biliary and pancreatic stenting: Devices and insertion techniques in therapeutic endoscopic retrograde cholangiopancreatography and endoscopic ultrasonography. World J Gastrointest Endosc. 2016;8:143–56. doi: 10.4253/wjge.v8.i3.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Binmoeller KF, Shah J. A novel lumen-apposing stent for transluminal drainage of nonadherent extraintestinal fluid collections. Endoscopy. 2011;43:337–42. doi: 10.1055/s-0030-1256127. [DOI] [PubMed] [Google Scholar]
- 7.Hammad T, Khan MA, Alastal Y, et al. Efficacy and safety of lumen-apposing metal stents in management of pancreatic fluid collections: Are they better than plastic stents? A systematic review and meta-analysis. Dig Dis Sci. 2018;63:289–301. doi: 10.1007/s10620-017-4851-0. [DOI] [PubMed] [Google Scholar]
- 8.Anderloni A, Buda A, Vieceli F, et al. Endoscopic ultrasound-guided transmural stenting for gallbladder drainage in high-risk patients with acute cholecystitis: A systematic review and pooled analysis. Surg Endosc. 2016;30:5200–8. doi: 10.1007/s00464-016-4894-x. [DOI] [PubMed] [Google Scholar]
- 9.Giovannini M, Moutardier V, Pesenti C, et al. Endoscopic ultrasound-guided bilioduodenal anastomosis: A new technique for biliary drainage. Endoscopy. 2001;33:898–900. doi: 10.1055/s-2001-17324. [DOI] [PubMed] [Google Scholar]
- 10.Minaga K, Kitano M. Recent advances in endoscopic ultrasound-guided biliary drainage. Dig Endosc. 2018;30:38–47. doi: 10.1111/den.12910. [DOI] [PubMed] [Google Scholar]
- 11.Sharaiha RZ, Khan MA, Kamal F, et al. Efficacy and safety of EUS-guided biliary drainage in comparison with percutaneous biliary drainage when ERCP fails: A systematic review and meta-analysis. Gastrointest Endosc. 2017;85:904–14. doi: 10.1016/j.gie.2016.12.023. [DOI] [PubMed] [Google Scholar]
- 12.Bang JY, Navaneethan U, Hasan M, et al. Stent placement by EUS or ERCP for primary biliary decompression in pancreatic cancer: A randomized trial (with videos) Gastrointest Endosc. 2018;88:9–17. doi: 10.1016/j.gie.2018.03.012. [DOI] [PubMed] [Google Scholar]
- 13.Paik WH, Lee TH, Park DH, et al. EUS-guided biliary drainage versus ERCP for the primary palliation of malignant biliary obstruction: A multicenter randomized clinical trial. Am J Gastroenterol. 2018;113:987–97. doi: 10.1038/s41395-018-0122-8. [DOI] [PubMed] [Google Scholar]
- 14.Ogura T, Higuchi K. Technical tips for endoscopic ultrasound-guided hepaticogastrostomy. World J Gastroenterol. 2016;22:3945–51. doi: 10.3748/wjg.v22.i15.3945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Giovannini M. Endoscopic ultrasound-guided pancreatic duct drainage: Ready for the prime time? Endosc Ultrasound. 2017;6:281–4. doi: 10.4103/eus.eus_86_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mussetto A, Fugazza A, Fuccio L, et al. Current uses and outcomes of lumen-apposing metal stents. Ann Gastroenterol. 2018;31:535–40. doi: 10.20524/aog.2018.0287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Teoh AY, Ng EK, Chan SM, et al. Ex vivo comparison of the lumen-apposing properties of EUS-specific stents (with video) Gastrointest Endosc. 2016;84:62–8. doi: 10.1016/j.gie.2015.11.041. [DOI] [PubMed] [Google Scholar]
- 18.Yang J, Chen YI, Friedland S, et al. Lumen-apposing stents versus plastic stents in the management of pancreatic pseudocysts: A large, comparative international, multicenter study. Endoscopy. 2018 doi: 10.1055/a-0759-1353. epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 19.Guo J, Saftoiu A, Vilmann P, et al. A multi-institutional consensus on how to perform endoscopic ultrasound-guided peri-pancreatic fluid collection drainage and endoscopic necrosectomy. Endosc Ultrasound. 2017;6:285–91. doi: 10.4103/eus.eus_85_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Itoi T, Binmoeller KF, Shah J, et al. Clinical evaluation of a novel lumen-apposing metal stent for endosonography-guided pancreatic pseudocyst and gallbladder drainage (with videos) Gastrointest Endosc. 2012;75:870–6. doi: 10.1016/j.gie.2011.10.020. [DOI] [PubMed] [Google Scholar]
- 21.Bang JY, Navaneethan U, Hasan MK, et al. Non-superiority of lumen-apposing metal stents over plastic stents for drainage of walled-off necrosis in a randomised trial. Gut. 2019;68:1200–9. doi: 10.1136/gutjnl-2017-315335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lang GD, Fritz C, Bhat T, et al. EUS-guided drainage of peripancreatic fluid collections with lumen-apposing metal stents and plastic double-pigtail stents: Comparison of efficacy and adverse event rates. Gastrointest Endosc. 2018;87:150–7. doi: 10.1016/j.gie.2017.06.029. [DOI] [PubMed] [Google Scholar]
- 23.Kalva NR, Vanar V, Forcione D, et al. Efficacy and safety of lumen apposing self-expandable metal stents for EUS guided cholecystostomy: A meta-analysis and systematic review. Can J Gastroenterol Hepatol. 2018;2018:7070961. doi: 10.1155/2018/7070961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dollhopf M, Larghi A, Will U, et al. EUS-guided gallbladder drainage in patients with acute cholecystitis and high surgical risk using an electrocautery-enhanced lumen-apposing metal stent device. Gastrointest Endosc. 2017;86:636–43. doi: 10.1016/j.gie.2017.02.027. [DOI] [PubMed] [Google Scholar]
- 25.Irani S, Ngamruengphong S, Teoh A, et al. Similar efficacies of endoscopic ultrasound gallbladder drainage with a lumen-apposing metal stent versus percutaneous transhepatic gallbladder drainage for acute cholecystitis. Clin Gastroenterol Hepatol. 2017;15:738–45. doi: 10.1016/j.cgh.2016.12.021. [DOI] [PubMed] [Google Scholar]
- 26.Alvarez-Sánchez MV, Jenssen C, Faiss S, et al. Interventional endoscopic ultrasonography: An overview of safety and complications. Surg Endosc. 2014;28:712–34. doi: 10.1007/s00464-013-3260-5. [DOI] [PubMed] [Google Scholar]
- 27.Jacques J, Privat J, Pinard F, et al. Endoscopic ultrasound-guided choledochoduodenostomy with electrocautery-enhanced lumen-apposing stents: A retrospective analysis. Endoscopy. 2019;51:540–7. doi: 10.1055/a-0735-9137. [DOI] [PubMed] [Google Scholar]
- 28.Kunda R, Pérez-Miranda M, Will U, et al. EUS-guided choledochoduodenostomy for malignant distal biliary obstruction using a lumen-apposing fully covered metal stent after failed ERCP. Surg Endosc. 2016;30:5002–8. doi: 10.1007/s00464-016-4845-6. [DOI] [PubMed] [Google Scholar]
- 29.Itoi T, Ishii K, Ikeuchi N, et al. Prospective evaluation of endoscopic ultrasonography-guided double-balloon-occluded gastrojejunostomy bypass (EPASS) for malignant gastric outlet obstruction. Gut. 2016;65:193–5. doi: 10.1136/gutjnl-2015-310348. [DOI] [PubMed] [Google Scholar]
- 30.Chen YI, James TW, Agarwal A, et al. EUS-guided gastroenterostomy in management of benign gastric outlet obstruction. Endosc Int Open. 2018;6:E363–8. doi: 10.1055/s-0043-123468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kedia P, Tyberg A, Kumta NA, et al. EUS-directed transgastric ERCP for roux-en-Y gastric bypass anatomy: A minimally invasive approach. Gastrointest Endosc. 2015;82:560–5. doi: 10.1016/j.gie.2015.03.1913. [DOI] [PubMed] [Google Scholar]
- 32.Bukhari M, Kowalski T, Nieto J, et al. An international, multicenter, comparative trial of EUS-guided gastrogastrostomy-assisted ERCP versus enteroscopy-assisted ERCP in patients with roux-en-Y gastric bypass anatomy. Gastrointest Endosc. 2018;88:486–94. doi: 10.1016/j.gie.2018.04.2356. [DOI] [PubMed] [Google Scholar]
- 33.Giovannini M, Dotti M, Bories E, et al. Hepaticogastrostomy by echo-endoscopy as a palliative treatment in a patient with metastatic biliary obstruction. Endoscopy. 2003;35:1076–8. doi: 10.1055/s-2003-44596. [DOI] [PubMed] [Google Scholar]
- 34.De Cassan C, Bories E, Pesenti C, et al. Use of partially covered and uncovered metallic prosthesis for endoscopic ultrasound-guided hepaticogastrostomy: Results of a retrospective monocentric study. Endosc Ultrasound. 2017;6:329–35. doi: 10.4103/2303-9027.209869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Park DH, Lee TH, Paik WH, et al. Feasibility and safety of a novel dedicated device for one-step EUS-guided biliary drainage: A randomized trial. J Gastroenterol Hepatol. 2015;30:1461–6. doi: 10.1111/jgh.13027. [DOI] [PubMed] [Google Scholar]
- 36.Cho DH, Lee SS, Oh D, et al. Long-term outcomes of a newly developed hybrid metal stent for EUS-guided biliary drainage (with videos) Gastrointest Endosc. 2017;85:1067–75. doi: 10.1016/j.gie.2016.09.010. [DOI] [PubMed] [Google Scholar]
- 37.Lee TH, Choi JH, Park do H, et al. Similar efficacies of endoscopic ultrasound-guided transmural and percutaneous drainage for malignant distal biliary obstruction. Clin Gastroenterol Hepatol. 2016;14:1011–9.e3. doi: 10.1016/j.cgh.2015.12.032. [DOI] [PubMed] [Google Scholar]
- 38.Itoi T, Sofuni A, Tsuchiya T, et al. Initial evaluation of a new plastic pancreatic duct stent for endoscopic ultrasonography-guided placement. Endoscopy. 2015;47:462–5. doi: 10.1055/s-0034-1391083. [DOI] [PubMed] [Google Scholar]
- 39.Matsunami Y, Itoi T, Sofuni A, et al. Evaluation of a new stent for EUS-guided pancreatic duct drainage: Long-term follow-up outcome. Endosc Int Open. 2018;6:E505–12. doi: 10.1055/s-0044-101753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Oh D, Park DH, Song TJ, et al. Optimal biliary access point and learning curve for endoscopic ultrasound-guided hepaticogastrostomy with transmural stenting. Therap Adv Gastroenterol. 2017;10:42–53. doi: 10.1177/1756283X16671671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Jacques J, Fumex F, Privat J, et al. EUS-guided choledocho-duodenostomy using Hot-AXIOS: A French multi-centric evaluation of its efficacy after training [abstract] JFHOD (French hepato-gastroenterology and digestif oncology meeting) 21-24th of March 2019, Paris [Google Scholar]