

Abstract
Background
This study aimed to assess adherence to oral nutrition supplements (ONS) among hospital outpatients and to assess patient characteristics, experiences of ONS, and the characteristics of ONS prescriptions in clinical practice.
Methods
Hospital outpatients aged ≥18 years and prescribed ONS by a dietitian at a Swedish hospital were referred to the study from September 2016 to February 2017. Data were collected from structured telephone interviews, medical records, and a register of ONS delivered. Adherence to ONS was measured by dividing self‐reported intake of ONS (frequency question and 24‐hour recall question) by the amount prescribed and using the medication possession ratio (MPR).
Results
Of the 96 patients included (mean age 67 ± 13 years), 52% were male. The 2 most frequent medical diagnoses were malignancy and digestive system disease. Mean adherence to ONS was 93% measured by the frequency question, 87% measured by the 24‐hour recall question, and 76% according to MPR. The majority of the patients (83%) were prescribed 1–3 bottles of ONS/day. The average number of flavors of ONS delivered was 4.2. Before prescription, 69% of the patients had been allowed to taste the ONS and 92% had chosen the flavors to be prescribed. Over 75% liked the taste of the ONS and considered them to be good for their health.
Conclusions
Adherence to ONS was high in this population, which might be explained by the individual tailoring of ONS prescriptions by a dietitian, positive experiences of ONS, and the relatively young mean age of the participants.
Keywords: malnutrition, medical nutrition therapy, oral nutrition supplements, patient compliance, treatment adherence and compliance
Background
The prevalence of disease‐related malnutrition is reportedly 20%–50% among patients admitted to hospital1 and 19% among hospital outpatients.2 The condition is associated with decreased quality of life3, 4 and increased length of hospital stay, morbidity, mortality1, 5 and cost of care.5, 6 If nutrition therapy comprising counselling on energy and nutrient‐dense food is considered to be insufficient, an approach that is commonly used is the addition of oral nutrition supplements (ONS). In meta‐analyses, ONS have been shown to be clinically effective in some patient groups,7, 8, 9, 10, 11 such as malnourished geriatric patients,9, 10 whereas a Cochrane review on disease‐related malnutrition found no major differences for morbidity or mortality between dietary advice and ONS.12 The use of ONS is, however, endorsed in several international guidelines on nutrition therapy.13, 14, 15, 16
The effectiveness of nutrition therapy using ONS varies because of patient adherence (or compliance) to the prescription. Adherence to therapy is defined by the World Health Organization (WHO) as “the extent to which a person's behavior – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider.”17 Higher adherence to ONS has been associated with a higher energy intake18, 19 and an increase in body weight19, 20, 21 and upper arm circumference.21 Regarding factors influencing ONS adherence, a positive association has previously been shown between energy density and ONS adherence, and a negative association has been found for age.18 Other influencing factors are suggested to be the duration of usage of ONS,22 variety of supplements prescribed,18, 22 how the supplement is taken,18 and if the patient is informed of the purpose of the ONS.23 All these potentially influencing factors can be found in the 5 different dimensions of adherence to therapy presented by WHO which are: (i) patient‐related factors, (ii) social and economic factors, (iii) healthcare team and system‐related factors, (iv) condition‐related factors, and (v) therapy‐related factors.17
Adherence to ONS has sometimes been acknowledged as being problematic because of low acceptance of the supplements10, 24 and side effects such as diarrhea and nausea.10, 25 However, in a systematic review by Hubbard et al, a relatively high compliance (78%) to ONS was found.18 In this review, patients in surveys of usage/clinical practice had a lower compliance to ONS than those in clinical trials.18 The patients in those surveys of usage were patients in elderly care homes and hospitals.26, 27, 28, 29, 30 It is noteworthy that a large number of studies in this review were excluded because of inadequate reporting of adherence to ONS.18 In Sweden, free‐living patients (ie, hospital outpatients and community‐dwelling patients) represent the principal group of ONS users, followed by residents in elderly care homes and finally hospitalized patients.31 In a study of ONS usage in an Irish community setting (n = 76, thereof 64% free‐living), 49% of the patients reported that they did not follow the ONS prescription most days of the week.32 Apart from this study, there is a lack of studies investigating adherence to ONS among free‐living patients and, more specifically, hospital outpatients prescribed ONS within clinical practice.
Swedish and international guidelines recommend that dietary counselling forms the basis of malnutrition treatment and should only be combined with ONS when considered necessary.14, 33, 34 Furthermore, ONS prescriptions are recommended to include variety and to be individually tailored regarding, for example, patient preferences for ONS type and timing.23 In many of the clinical trials with ONS, a standardized amount of 250–600 kcal/d of a multinutrient ONS is prescribed.18, 23 However, little has been reported about ONS prescription characteristics in clinical practice. The main aim of this study was to assess adherence to ONS among hospital outpatients. Additionally, we evaluated patient characteristics including patients’ experiences of ONS and the characteristics of ONS prescriptions in clinical practice.
Methods
Study Design and Participants
This was a cross‐sectional study on adherence to ONS among hospital outpatients who were prescribed ONS within clinical practice. Approval of the study protocol was received from the Regional Ethical Review Board in Uppsala (Reference No. 2015/55 and 2015/55/1). Written informed consent was obtained from all participants.
Study participants were recruited from a university hospital in a city in Sweden by 18 clinical dietitians working in the areas of oncology, surgery, gastroenterology, hematology, cardiology, rheumatology, neurology, allergy, endocrinology, lung medicine, hepatology, psychiatry, and intensive care. The majority of the dietitians worked with both inpatient and outpatient care within their field of expertise. Because of organizational issues, the geriatrics department declined participation in the recruitment, and hence no patients receiving care on the geriatric units were included.
Eligible patients met the following criteria: adult (≥18 years old), prescribed ONS with ≥2 macronutrients and added micronutrients by a hospital dietitian, free‐living, absence of dementia or cognitive impairment, not receiving enteral or parenteral nutrition, and able to communicate orally in Swedish. Eligible patients were asked if they would like to receive study information by mail when they attended a first or follow‐up visit or had a telephone contact with their dietitian. Those who were interested in participating returned a signed written consent form. Participants received a gift voucher for flowers equivalent to approximately $12 as compensation, or, alternatively, they could choose to donate the same amount to Medecins Sans Frontieres (Doctors Without Borders). Age and gender information were recorded about patients who declined being sent study information by mail. The inclusion period was from September 2016 to February 2017.
The county council of the region has local guidelines for the prescription of ONS.35 The guidelines state that an individual assessment and evaluation should always be performed before nutrition products are prescribed. It is advocated that clinical dietitians should be the primary prescribing healthcare professionals and the recommended amount of ONS prescribed is not >1–3 bottles per day. A patient qualifies for prescription of ONS if the ordinary food intake is not enough and there is a risk for disease‐related malnutrition in combination with a medical diagnosis where ONS have a scientifically documented positive effect.35 Prescribed ONS are delivered to the patient's home by a designated distribution company. The deliveries contain the products prescribed for 1 month's consumption, and refills can be prescribed for up to 6 months. A prescription is valid for delivery up to 12 months from the prescription date. ONS are subsidized by the county council and, when prescribed as a complement to the ordinary diet, the patient fee is approximately $29 for a single delivery (ie, 1 month's consumption). This system of prescription and delivery of ONS applies to free‐living patients (hospital outpatients and community‐dwelling patients). For hospitalized patients, ONS are provided by the hospital food service organization.
Data Collection
The data were collected through structured telephone interviews (TI) (average time 14 minutes, range 6–46 minutes), and from the dietetic notes in electronic medical records (EMR) and a register of delivered nutrition products (RDNP) held by the regional distribution company. Patients who had submitted a signed consent form to participate could choose to decline participation in the TI, and for these, only information from the EMR and the RDNP was collected. The 5 dimensions of the adherence model from WHO17 were taken into consideration when deciding which variables to include in the data collection, focusing mainly on the therapy‐related factors (ONS related). The first version of the TI questions was tested by 5 cognitive interviews using the verbal probing technique, with the aim of detecting sources of response error caused by problems with, for example, comprehension or recall.36 The subjects for the cognitive interviews were found by contacting 2 different patient associations (head‐neck cancer and gastrointestinal disease), which then disseminated information about the interviews in member magazines, at member meetings, and via e‐mail lists. Three of the cognitive interviews were held face‐to‐face and 2 by telephone, and interview duration ranged between 22 and 74 minutes. Changes made to the TI questions following 4 of the cognitive interviews were rephrasing (n = 4), splitting 1 question into 2 questions (n = 2), and deletion (n = 2) due to recall issues. The final cognitive interview was held using the revised questions, after which 2 questions were further clarified by rephrasing.
Assessment of patient characteristics, ONS experiences, and prescription characteristics
Information about the hospital outpatients’ medical diagnoses, age, and gender was collected from the EMRs. Prevalence of risk of malnutrition was assessed retrospectively by using the Malnutrition Universal Screening Tool (MUST), which includes body mass index (BMI; kg/m2), body weight change during the past 3–6 months, and acute clinical condition.37 Since the study population consisted of hospital outpatients, none were expected to be given the “acute disease effect score,” but consideration was given to whether their dietary intake was likely to be small or nonexistent for 5 days. A total score of 0 indicates low risk of malnutrition, a score of 1 indicates medium risk, and a score of ≥2 indicates high risk.37 The data on body weight, height, and body weight change were self‐reported during the TI. Duration of ONS use was obtained from the EMR and self‐reported during the TI. Duration was defined as the period from when the patient started consuming ONS until the measurement time. However, if the patients’ consumption of ONS ceased for >1 month during this period, we calculated the duration start date from when consumption of ONS resumed. Information about the amount, type (eg, high energy, fiber containing, etc), flavors, and date of delivery of the ONS was collected from the RDNP. Information about whether the patients were allowed to taste the supplements before prescription and if they participated in choosing flavors was collected during the TI. The patients were also asked during the TI to report, on a 4‐point Likert scale, to what extent they agreed with statements regarding health benefits and taste of ONS, the influence of support from others, and forgetfulness regarding consumption of ONS. In addition, they were asked if they viewed ONS as food or medicine and about their consumption of ONS in relation to other meals. Consistency between the ONS prescription documented by the dietitian in the EMR and the patient self‐reported prescription was assessed. Furthermore, 2 open‐ended questions included in the TI concerned reasons for occasionally finding it difficult to drink ONS and if they experienced anything that facilitated the consumption of ONS.
Assessment of adherence to ONS
Adherence to ONS was assessed by dividing the self‐reported intake of ONS by the prescribed amount and by using a medication refill adherence measure called the Medication Possession Ratio (MPR). Self‐reported intake of ONS was measured by a frequency question and a 24‐hour (24‐h) recall question. Information about the prescription of ONS was found in the dietetic notes in the patient's EMR. The 3 methods of assessing adherence to ONS in this study are further described in Table 1. Scores for the adherence rate ranged between 0% and 100%. If more than the prescribed amount of ONS was reported to have been consumed, the adherence rate score was truncated at 100%. Truncated adherence scales are commonly used in medication adherence studies.38 This approach was considered suitable since a higher intake of ONS than prescribed might, for those patients with malnutrition or at nutrition risk, be anticipated to be either good or at least not harmful.
Table 1.
Assessment of Adherence to ONS by the Frequency Question, 24‐Hour Recall Question, and MPR
| Procedure | Frequency Question | 24‐Hour Recall Question | MPR |
|---|---|---|---|
| Assigned as the prescribed amount | Amount written in the dietetic note in the EMR or delivered amount if information was missing | Amount written in the dietetic note in the EMR or delivered amount if information was missing | Amount delivered divided by 30 days (eg, if the patient received 60 bottles, the prescribed amount is 2 since 60 bottles/30 days equals 2) |
| Assigned as the consumed amount |
|
|
Amount delivered between 2 refill points |
| Calculation of adherence rate | Proportion of the prescribed amount of ONS consumed | Proportion of the prescribed amount of ONS consumed | Proportion of days when the prescribed number of ONS was consumed |
| Adherence rate | 0%–100% | 0%–100% | 0%–100% |
| Measurement time point | “Here and now.” Adherence rate by the time of the TI. | “Here and now.” Adherence rate by the day before the TI. | “Retrospectively.” From 1 to 6 months back in time. |
| Example of calculation | Prescribed amount was 1–2 bottles of ONS per day. The patient reported their usual consumption to be 1 bottle per day. 1/1 = 1. An adherence rate of 100% was assigned to this patient. | Prescribed amount was 1–2 bottles of ONS per day. The patient reported consumption of 2 bottles yesterday. 2/2 = 1. An adherence rate of 100% was assigned to this patient. | The patient was prescribed 60 bottles with 3 refills on May 1, 2016 (to be used for 4 months, ie, 120 days). The patient requested refills on July 15, August 20, and November 12, 2016. Number of days between May 1 and November 12 was 195. Within this observation period, the patient had access to the prescribed amount for 90 days (3 deliveries of ONS). 90/195 = 0.4615. An adherence rate of 46% was assigned to this patient. |
EMR, electronic medical record; MPR, medication possession ratio; ONS, oral nutrition supplement; TI, telephone interview.
When posing the 24‐h recall question, a technique inspired by the automated multiple pass method was used to provide several opportunities for the participants to remember all bottles of ONS consumed.39 The question “How many ONS did you drink yesterday?” was hence followed by questions such as “Did you drink any supplements during the night?” “What time did you drink the supplements yesterday?” and “What flavor was it?” etc.
MPR was calculated by the commonly used formula “Number of days’ supply obtained during observation period/Number of days in observation period times 100.” 40 In this study, the delivery date of the ONS was used as the refill date. MPR could be assessed for patients who had received >1 delivery of ONS. Data on the deliveries performed 6 months prior to the TI date were used. The ONS prescriptions for the last 6 months of ONS delivery had been signed by the dietitian from 1 to 12 months prior to the TI. Thus, the MPR covers multiple refill intervals (ie, several months) for some patients and single refill intervals (ie, 1 month) for other patients. MPR was not calculated for patients with an agreed interruption of ONS use (ie, patients were not supposed to consume ONS during this period) within the interval. In addition to the adherence measures, the participants were asked during the TI if they usually consumed the whole bottle of ONS.
Statistical Analysis
Results are reported as absolute and relative frequencies for categorical variables, and means and standard deviations (SD) for continuous variables. Descriptive univariate statistics were used to calculate the adherence measures. The differences between the adherence measures at group level were compared by paired Wilcoxon signed ranks test since the variables were non‐normally distributed and no transformation method was applicable. Spearman's ρ was used to assess relationships between the different adherence measures at individual level. A P‐value of ≤0.05 was required for the null hypothesis to be rejected. Analyses were performed using the Statistical Package for the Social Sciences (IBM Corp, Released 2016. IBM SPSS Statistics for Windows, Version 24.0, Armonk, NY, USA).
Results
Of 218 patients fulfilling the inclusion criteria, 148 agreed to being sent study information. The reasons for patients not being sent study information were, for the majority (n = 50/70), that the dietitians did not ask them because of reasons such as time constraints, patient in late palliative care, or patient's alcohol abuse. The remainder declined study information being sent to them (n = 20/70). From the feedback given by the recruiting dietitians, there may have been more patients fulfilling the inclusion criteria who were not asked to participate or not recorded due to a very high workload in the clinic. Of the 148 patients who were sent study information, 96 agreed to participate in the study. Of these 96, complete data were available for 78 since 18 declined to participate in the TI (Figure 1). There were no significant differences regarding age or gender proportions between the patients who were not sent information about the study (n = 70) and the included study participants (n = 96) (data not shown). There were also no significant differences for those characteristics between the included study patients who participated in the TI and those who did not (data not shown).
Figure 1.
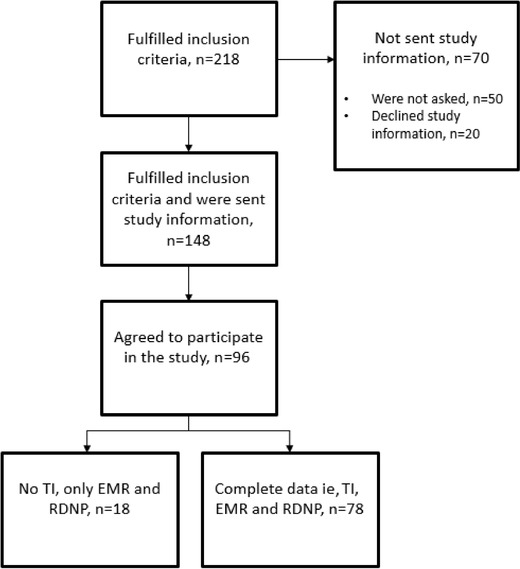
Flowchart of patient recruitment. EMR, electronic medical record; RDNP, register of delivered nutrition products; TI, telephone interview.
Patient Characteristics
The mean age of the patients was 67.4 years, and 52% were men. The 2 major medical diagnoses were malignancy being treated at the oncological or the surgical department (n = 51) and digestive system disease (n = 19), such as inflammatory bowel disease, liver disease, etc. BMI was on average within the normal range (22.1 ± 3.9). According to MUST, 70% were classified as having a medium or high risk of malnutrition. The majority (63%) were living in a household with >1 inhabitant, and 12% were receiving home care service. Patient characteristics are shown in Table 2.
Table 2.
Patient Characteristics
| Patient Characteristics | All Included Patients, n = 96 | Patients with TI, EMR and RDNP Data, n = 78 | Patients with EMR and RDNP Data, n = 18 |
|---|---|---|---|
| Age (y), mean ± SD (range) | 67.4 ± 13.2 (21–89) | 66.6 ± 13.1 (21–89) | 70.8 ± 13.7 (29–84) |
| 0–64 years, n (%) | 29 (30.2) | 26 (33.3) | 3 (16.7) |
| ≥65 years, n (%) | 67 (69.8) | 52 (66.7) | 15 (83.3) |
| Sex (men) n, (%) | 50 (52.1) | 41 (52.6) | 9 (50.0) |
| Medical diagnosis n, (%) | |||
| Malignancy | 51 (53.1) | 43 (55.1) | 8 (44.4) |
| Digestive system disease | 19 (19.8) | 15 (19.2) | 4 (22.2) |
| Lung disease | 10 (10.4) | 7 (9.0) | 3 (16.7) |
| Kidney disease | 9 (9.4) | 7 (9.0) | 2 (11.1) |
| Other, eg, neurological disease, rheumatic disease, cardiac disease | 7 (7.3) | 6 (7.7) | 1 (5.6) |
| Body mass index (kg/m2), mean ± SD | 22.1 ± 3.9a | 22.3 ± 3.9 | 21.2 ± 3.4b |
| Underweight (<18.5 kg/m2), n (%) | 10 (12.8) | ||
| Normal range (18.5–24.9 kg/m2), n (%) | 50 (64.1) | ||
| Overweight (25–29.9 kg/m2), n (%) | 14 (17.9) | ||
| Obese (≥30 kg/m2), n (%) | 4 (5.1) | ||
| Weight loss previous 3–6 monthsc, n (%) | |||
| <5% | 35 (46.1) | ||
| 5%–10% | 21 (27.6) | ||
| >10% | 20 (26.3) | ||
| Malnutrition Universal Screening Toolc n, (%) | |||
| 0 Low risk | 23 (30.3) | ||
| 1 Medium risk | 23 (30.3) | ||
| ≥ 2 High risk | 30 (39.5) | ||
| Residents in household n, (%) | |||
| Lives alone | 29 (37.2) | ||
| Two or more | 49 (62.8) | ||
| Home care service (yes) n, (%) | 9 (11.5) | ||
EMR, electronic medical record; RDNP, register of delivered nutrition products; TI, telephone interview.
n = 89.
n = 11.
n = 76.
Adherence to ONS
Mean adherence to ONS was 93% (SD 18) measured with the frequency question, 87% (SD = 28) measured with the 24‐h recall question, and 76% (SD = 21) measured with MPR (Figure 2). When measured with the frequency question, the proportion of patients with full adherence (ie, 100%) was 85% (n = 66/78). For the 24‐h recall question, the proportion of patients with full adherence was 78% (n = 61/78) and for MPR 26% (n = 11/42). Measured with the frequency question, 6 patients had an adherence rate above 100%, which was adjusted to 100% (range 116–200). Measured with the 24‐h recall question, the number was 9 (range 125–200) and with MPR 10 (range 101–143). All pairwise comparisons of the distribution of the adherence rate measured with the 3 methods differed significantly (Figure 2). Spearman's ρ tests were performed on pairs of the 3 adherence measures, and a significant positive correlation between the adherence rate measured with the frequency question and the 24‐h recall question was found (rs = 0.79, P = 0.000). Neither the adherence rate measured by the frequency question (rs = ‐0.081, P = 0.644) nor the 24‐h recall question (rs = 0.023, P = 0.898) correlated with MPR. Of the 78 patients, 100% reported that they usually consumed the whole bottle when consuming ONS. For the statement “I often forget to drink the ONS” only 1 person agreed to a large/very large extent (Figure 3).
Figure 2.
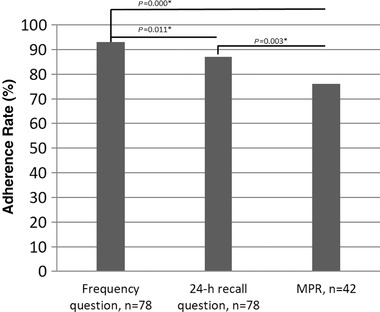
Adherence to oral nutrition supplements. *Significant at 0.05 level. Presented are the means and P‐values from paired Wilcoxon signed ranks test. 24‐h, 24‐hour; MPR, medical possession ratio.
Figure 3.
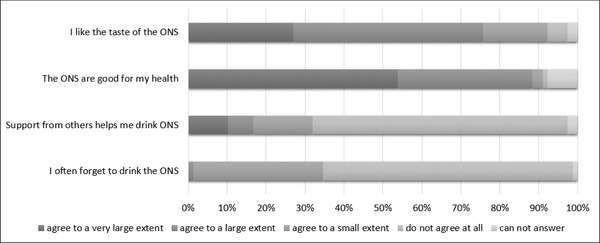
Proportions (%) of the patients’ level of agreement with different statements regarding oral nutrition supplements (ONS), n = 78.
Prescription Characteristics
Information about the prescribed amount was obtained from the dietetic notes in the EMR for 87 patients and from the RDNP for the remainder (n = 9). The prescriptions were commonly between 1 and 3 bottles of ONS per day (Table 3), and for the majority, they were combined with dietary counselling. As well as prescriptions of an exact number of bottles per day, a range of 1–2 bottles or 2–3 bottles per day was often prescribed. On average, the patients were prescribed 2.7 refills, which corresponds to a prescription time span of slightly over 2½ months. The average number of bottles delivered was approximately 2 per day (63 for 30 days of consumption), number of types of ONS was 1.8, and number of flavors 4.2. The average energy density of the delivered ONS was 1.6 kcal/mL, and 70% received a combination of supplements that had an average energy density of ≥1.5 kcal/mL. The majority of the patients were allowed to taste the supplements before prescription (69%) and participated in the choice of flavors (92%). The duration of ONS use was <6 months for 72% of the patients. Information on duration of ONS use was obtained from the EMR for 79 of the patients and was self‐reported for the remaining 16. The mean duration between the TI and the patient's last contact with the prescribing dietitian was 17.6 ± 13.2 days. On average, the patients had received 4.3 contacts (visits or telephone) with the dietitian during the past year. Fifty‐four percent of the population had received their first contact with the dietitian within 1 year. Of the 61 patients who acknowledged being prescribed a specific amount of ONS, 79% reported that they were only given an oral prescription, 18% reported the prescription was both written and oral, and 3% reported only being given a written prescription. For 60% (n = 47/78) of the patients, the patient‐reported prescribed amount of ONS was the same as the registered amount in the EMR. For the remaining 40% (n = 31/78), there was a discrepancy between the patient‐reported prescription and the prescription documented in the EMR. Of these (n = 11/31), 11 patients reported not being given a daily prescribed amount although a prescribed amount was documented in the EMR. For 18 patients (n = 18/31), the patient‐reported prescription deviated from the one documented by the dietitian in the EMR.
Table 3.
Prescription Characteristics, n = 96
| Prescription Characteristics | Descriptive Statistics |
|---|---|
| Prescribed amount (bottles per day), n (%) | |
| 1 | 12 (12.5) |
| 1–2 | 23 (24.0) |
| 2 | 25 (26.0) |
| 2–3 | 6 (6.3) |
| 3 | 14 (14.6) |
| 4 | 5 (5.2) |
| Non‐specified, eg, patient decides, <3, >2 | 11 (11.5) |
| Prescribed refills/deliveries of ONSa, mean ± SD | 2.7 ± 1.5 |
| 1, n (%) | 30 (33.3) |
| 2, n (%) | 10 (11.1) |
| 3, n (%) | 22 (24.4) |
| 4, n (%) | 21 (23.3) |
| 5, n (%) | 1 (1.1) |
| 6, n (%) | 6 (6.7) |
| Delivered number of bottles or portions per month, mean ± SD | 63.0 ± 22.6 |
| Number of types of ONS, mean ± SD | 1.8 ± 0.9 |
| Number of ONS flavors, mean ± SD | 4.2 ± 2.5 |
| Delivered volume in mL per day, mean ± SD | 401.4 ± 178.2 |
| Delivered amount of energy in kcal per day, mean ± SD | 636.8 ± 246.6 |
| Energy density (kcal/mL), mean ± SD | 1.6 ± 0.4 |
| 0–0.99 kcal/mL, n (%) | 2 (2.1) |
| 1–1.49 kcal/mL, n (%) | 27 (28.1) |
| 1.5–1.99 kcal/mL, n (%) | 47 (49.0) |
| ≥2 kcal/mL, n (%) | 20 (20.8) |
| Duration of ONS useb, n (%) | |
| <1 month | 31 (32.6) |
| 1–2 months | 17 (17.9) |
| 3–6 months | 21 (22.1) |
| 7–12 months | 8 (8.4) |
| 13–24 months | 7 (7.3) |
| >24 months | 11 (11.6) |
| Allowed to taste ONS before prescriptionc, n (%) | |
| Yes | 54 (69.2) |
| No | 19 (24.4) |
| Don't know | 5 (6.4) |
| Patient participated in choice of flavorsc, n (%) | |
| Yes | 72 (92.3) |
| No | 5 (6.4) |
| Don't know | 1 (1.3) |
ONS, oral nutrition supplements.
n = 90.
n = 95.
n = 78.
Experiences of ONS
The majority of the patients participating in the TI (n = 78) agreed to a very large or large extent with the statements “I like the taste of the ONS” (76%) and “The ONS are good for my health” (88%) (Figure 3). Less than one‐fifth of the patients (17%) agreed to a very large or large extent with the statement “Support from others helps me drink ONS.” Of those living alone, 4% agreed to a very large or large extent with the statement about support from others increasing their ONS consumption. Of those living with 1 or more cohabitants, 9% agreed with this statement. Support from others, therefore, does not seem to be of great importance for the consumption of ONS in this population irrespective of household size. More patients (54%) regarded ONS as food rather than medicine than those who regarded ONS as medicine rather than food (28%). However, a substantial number of patients (18%) declined to answer this question since they could not choose between the 2 alternatives. Regarding timing of ONS consumption, they were most commonly consumed between meals, whereas a quarter of patients alternated consuming ONS between meals, instead of meals, and together with meals (Figure 4). More than half of the patients (n = 42/78) reported no difficulties with consumption of ONS. The remaining 36 of 78 gave examples of different reasons that occasionally made the consumption of ONS difficult, such as nausea, satiety, fullness, the taste of ONS, texture, swallowing difficulties, stomach pain, etc. Procedures suggested to facilitate consumption were consuming the ONS cold (n = 12), mixing the ONS with other drinks or seasonings (n = 5), and serving them in a particular way (n = 5), for example with or without a straw, in a glass, or directly from the bottle, etc.
Figure 4.
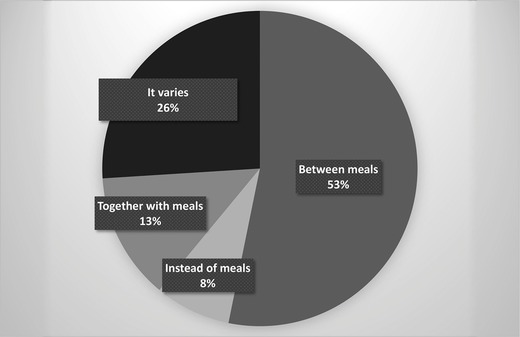
Oral nutrition supplement consumption in relation to meals, n = 77.
Discussion
This cross‐sectional study on hospital outpatients who had been prescribed ONS by dietitians in clinical practice demonstrates a very high adherence rate of 93% measured with the frequency question, 87% measured with the 24‐h recall question, and 76% with MPR. An adherence rate of ≥80% is generally considered satisfactory for medications41 and ≥73%–75% has been suggested in 2 different trials on ONS.19, 42 Despite previous indications of lower adherence to ONS in surveys of usage,18, 32 the 3 mean adherence rates demonstrated in this study were higher than or similar to the reported overall mean adherence rate (78%) in the systematic review of compliance to ONS by Hubbard et al in 2012 (n = 46 studies).18
There are several possible explanations for the high adherence to ONS in our population. This setting of free‐living outpatients receiving specialist care from dietitians at a hospital may give the patients certain prerequisites that affect the adherence rate to ONS in a positive way. The nutrition therapy and prescription characteristics demonstrated in this study are in line with the descriptions of and recommendations for ONS use in clinical practice.12, 23 First, ONS were primarily prescribed in combination with dietary counseling by a clinical dietitian. Second, a large number of patients were allowed to taste the ONS before prescription and patients participated in the choice of flavors, which confirms that prescriptions were individually tailored. It is also recommended that a variety of ONS are prescribed to enhance acceptance,23, 43 and an average of 4.2 prescribed ONS flavors covers this. The majority (>70%) also liked the taste of the ONS, whereas a dislike of the taste has been previously proposed as an explanation for low compliance to ONS treatment.44, 45 Furthermore, the treatment was monitored by healthcare professionals, which, in combination with individual tailoring, is considered to be the appropriate way of managing therapy with ONS.23 Also, when goals of ONS treatment are not met, the healthcare professional should decide on alternative treatments.23, 43 Since all patients were receiving individual nutrition therapy from a clinical dietitian, those with low acceptability of the supplements might never have been prescribed ONS or their prescription was stopped and replaced with other interventions. It is also possible that patients with lower acceptability of the supplements and/or adherence rate declined study participation to a greater extent or were never asked about participation because of sporadic contact with their prescribing dietitian.
It has previously been shown that compliance is higher for patients receiving ONS with an energy density of ≥2 kcal/mL than 1–1.5 kcal/mL.18 Since only a quarter of our population received a combination of supplements with an average energy density of ≥2 kcal/mL, this is not an explanation for the very high adherence rate. For the studied population, it was most common to consume the ONS in between meals rather than with meals or instead of meals. This might be of importance to achieve high adherence, but it is difficult to gain an overview of ONS intervention procedures since information about how the ONS were to be taken is often lacking in randomized controlled trials on ONS.46 In the review by Hubbard et al, no differences in compliance to ONS prescriptions were seen between studies reporting having given instructions about when to take the ONS compared with those that did not include such information.18
Even though adherence to ONS was very high in this study, another area of interest is the low consistency between the prescription documented in the EMR and the patient's self‐reported prescription for 40% of the population. One potential explanation might be that the dietitians sometimes did not explicitly give a recommended ONS amount but used a non‐prescriptive approach, which has been shown to be appreciated by patients in dietetic consultations.47 Another explanation could be patient recall, which has been shown as a factor for patients on hospital discharge with regard to prescribed medications.48 Earlier adherence research revealed that patients commonly adhere better to a medicine prescription during the 5 days before and after a visit to the healthcare professional, compared with 1 month after the visit.49 This phenomenon is known as “white coat adherence.”50, 51 Since the average time between the visit to the dietitian and the TI was 18 days, this could have had a positive effect on adherence. Because of privacy regulations, another recruitment strategy where study information was sent to all patients in the county council receiving ONS at home could not be applied. A recent contact with the prescribing dietitian was therefore unavoidable.
In addition to the discussion concerning aspects of the nutrition therapy and prescription characteristics, patient characteristics are also of importance. Hubbard et al found a negative association between compliance to ONS and age in their review of compliance to ONS.18 Our population had an average age of 67, which is relatively young in comparison to the populations in other surveys of usage of ONS (79–86 years) in which adherence was lower.26, 27, 28, 29, 30, 32 The majority of patients in our population were within the normal BMI range, and 72% were either at moderate or high risk of malnutrition according to MUST. Hubbard et al found no association between compliance to ONS and BMI,18 but Jobse et al observed a higher proportion of compliers to ONS prescriptions among patients categorized as malnourished by the Mini Nutritional Assessment short form in their clinical trial on ONS among nursing home residents.21 In our study, nutrition therapy for malnutrition had started at different time points before data collection, which should be taken into consideration when interpreting the data concerning risk of malnutrition.
This study contributes to the knowledge of adherence to ONS in clinical practice and, since the adherence rate was over 75% in this population, the patient and prescription characteristics including patient experiences might function as guidance regarding influencing factors to focus on in future intervention studies in which adherence to ONS is the primary outcome measure. Using WHO's 5 dimensions of adherence to therapy17 and the results from this study, the following areas may be of interest for forthcoming research on adherence to ONS: (i) patient‐related factors, such as attitudes toward and motivation for using ONS; (ii) social and economic factors, such as the reasons behind why age seems to be associated with adherence to ONS; (iii) healthcare team and system‐related factors, such as patient‐provider relationship and monitoring/follow‐up routines; (vi) condition‐related factors, such as severity of disease and treatment care level/setting; and (v) therapy‐related factors, such as variety of ONS, level of individual tailoring, and the combination of dietary counselling and ONS.
Methodological Considerations
There are 2 major drawbacks regarding the recruitment of the population in this study. The first is the non‐participation of the geriatrics department since older people are often regarded as a group with low adherence to ONS.24, 26 Second, the recruiting dietitians sometimes found it inappropriate to ask patients about study participation (eg, patients in late palliative care), and during periods of high workload, some patients fulfilling the inclusion criteria might have been missed. These factors may have affected the constitution of the study population. However, with regard to the medical diagnoses and age of the participants, they seem to represent the hospital outpatient population being prescribed ONS by the hospital dietitians fairly well.
We used self‐reported data on body weight and height, which has been shown to provide underestimated BMI values in previous research.52 However, in a study of people over 60 years of age, self‐reported data categorized people to their correct BMI category quite satisfactorily.53 Further, according to the instructions on malnutrition screening using MUST, self‐reported measures can be used as surrogates for measured weight, height, and weight change to calculate the MUST score.37
In our study, mean adherence was higher measured by self‐reported intake of ONS than with the medication refill adherence measure MPR. Well‐known challenges with retrospective dietary assessment methods are the reliance on people's memories and the risk of being given “socially desirable” answers,54 which might have resulted in a higher level of reported intake of ONS than actual intake. Self‐reported measures (interviews, questionnaires) of adherence to medicines also generally tend to produce overestimated rates.51 The MPR data with lower mean adherence rate and proportion of patients with 100% adherence supports the possibility of overestimated self‐reported intake data on ONS. However, medication refill measures such as MPR have also received criticism since they do not necessarily reflect the actual ingestion of a medicine.51 MPR does not take into account if the patient consumed all the ONS delivered or any potential adverse events, such as hospitalization of a patient. MPR can give overestimated or underestimated values for ONS intake. Other drawbacks of MPR in this study, in addition to the low number of cases, are the use of inconsistent observation times and, in some cases, only 1 refill interval, which is not an optimal approach.40 However, we find the use of 3 different adherence measures to be a strength of our study, since the use of a combination of measures of adherence has been endorsed when conducting adherence research.55 The nonexistent association between MPR and the 2 self‐reported measures of adherence might be explained by using different definitions of the prescribed amount, ie, documented prescription in the EMR or the amount delivered to the home. Another explanation might be the different time intervals covered by the different types of measures. We consider the adherence rate measured by the frequency question as most valid since a single 24‐h recall is not considered sufficient to determine the usual intake of a specific food.54
Conclusions
In contrast to results from other surveys on the use of ONS in clinical practice, adherence to ONS was very high in this population of hospital outpatients. The mean age of the patients was relatively low, with the majority being treated for malignancy or digestive system disease. The prescriptions were individually tailored by a dietitian and commonly contained 1–3 bottles of ONS per day in a variety of flavors. The majority of the patients liked the taste of the ONS and considered them to be good for their health. Influencing factors that might explain the high adherence rate are the hospital outpatient setting, a relatively low mean age, tailored prescriptions, positive experiences of ONS, and contact with the prescriber close in time to the point of data collection. Confirmation of these indications through intervention studies in which adherence to ONS is the primary outcome variable is warranted.
Acknowledgments
We thank all the dietitians at the university hospital for their help with the recruitment of patients to the study.
Statement of Authorship
E. Liljeberg, M. Nydahl, and A. Andersson contributed to the conception and design of the research; K. Blom Malmberg contributed to the design of the research; E. Liljeberg and K. Blom Malmberg contributed to the acquisition of the data; E. Liljeberg contributed to the analysis; all authors contributed to the interpretation of the data; E. Liljeberg drafted the manuscript. All authors critically revised the manuscript, agree to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
Consulted statistician: Inger Persson, PhD, Department of Statistics, Uppsala University.
Financial disclosure: This study was supported by SNF Swedish Nutrition Foundation. The PhD position of E. Liljeberg is partly funded by Stiftelsen Kronprinsessan Margarets Minnesfond.
Conflicts of interest: None declared.
References
- 1. Norman K, Pichard C, Lochs H, Pirlich M. Prognostic impact of disease‐related malnutrition. Clin Nutr. 2008;27(1):5‐15. [DOI] [PubMed] [Google Scholar]
- 2. Cawood AL, Elia M, Sharp SK, Stratton RJ. Malnutrition self‐screening by using MUST in hospital outpatients: validity, reliability, and ease of use. Am J Clin Nutr. 2012;96(5):1000‐1007. [DOI] [PubMed] [Google Scholar]
- 3. Lis CG, Gupta D, Lammersfeld CA, Markman M, Vashi PG. Role of nutritional status in predicting quality of life outcomes in cancer—a systematic review of the epidemiological literature. Nutr J. 2012;11:27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Norman K, Kirchner H, Lochs H, Pirlich M. Malnutrition affects quality of life in gastroenterology patients. World J Gastroenterol. 2006;12(21):3380‐3385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Correia MI, Waitzberg DL. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr. 2003;22(3):235‐239. [DOI] [PubMed] [Google Scholar]
- 6. Freijer K, Tan SS, Koopmanschap MA, Meijers JM, Halfens RJ, Nuijten MJ. The economic costs of disease related malnutrition. Clin Nutr. 2013;32(1):136‐141. [DOI] [PubMed] [Google Scholar]
- 7. National Institute for Health and Clinical Excellence (NICE) . Nutrition Support for Adults: Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition (Clinical guideline 32). London, United Kingdom: National Collaborating Centre for Acute Care; 2006. [PubMed] [Google Scholar]
- 8. Stratton RJ, Green CJ, Elia M. Disease‐Related Malnutrition: An Evidence‐Based Approach to Treatment. Cambridge, MA: Cabi Publishing; 2003. [Google Scholar]
- 9. Koretz RL, Avenell A, Lipman TO, Braunschweig CL, Milne AC. Does enteral nutrition affect clinical outcome? A systematic review of the randomized trials. Am J Gastroenterol. 2007;102(2):412‐429. [DOI] [PubMed] [Google Scholar]
- 10. Milne AC, Potter J, Vivanti A, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2009;2:CD003288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:CD000998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Baldwin C, Weekes CE. Dietary advice with or without oral nutritional supplements for disease‐related malnutrition in adults. Cochrane Database Syst Rev. 2011;9:CD002008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Volkert D, Beck AM, Cederholm T, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. [In Press]. Clin Nutr. 2018. 10.1016/j.clnu.2018.05.024 [DOI] [PubMed] [Google Scholar]
- 14. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11‐48. [DOI] [PubMed] [Google Scholar]
- 15. Isenring E, Zabel R, Bannister M, et al. Updated evidence‐based practice guidelines for the nutritional management of patients receiving radiation therapy and/or chemotherapy. Nutr Diet. 2013;70(4):312‐324. [Google Scholar]
- 16. Tappenden KA, Quatrara B, Parkhurst ML, Malone AM, Fanjiang G, Ziegler TR. Critical role of nutrition in improving quality of care: an interdisciplinary call to action to address adult hospital malnutrition. JPEN J Parenter Enteral Nutr. 2013;37(4):482‐497. [DOI] [PubMed] [Google Scholar]
- 17. WHO . Adherence to Long‐Term Therapies: Evidence for Action. Geneva, Switzerland: World Health Organization; 2003. [Google Scholar]
- 18. Hubbard GP, Elia M, Holdoway A, Stratton RJ. A systematic review of compliance to oral nutritional supplements. Clin Nutr. 2012;31(3):293‐312. [DOI] [PubMed] [Google Scholar]
- 19. Bauer J, Capra S, Battistutta D, Davidson W, Ash S; for Cancer Cachexia Study Group. Compliance with nutrition prescription improves outcomes in patients with unresectable pancreatic cancer. Clin Nutr. 2005;24(6):998‐1004. [DOI] [PubMed] [Google Scholar]
- 20. Wengstrom Y, Wahren LK, Grodzinsky E. Importance of dietary advice, nutritional supplements and compliance for maintaining body weight and body fat after hip fracture. J Nutr Health Aging. 2009;13(7):632‐638. [DOI] [PubMed] [Google Scholar]
- 21. Jobse I, Liao Y, Bartram M, et al. Compliance of nursing home residents with a nutrient‐ and energy‐dense oral nutritional supplement determines effects on nutritional status. J Nutr Health Aging. 2015;19(3):356‐364. [DOI] [PubMed] [Google Scholar]
- 22. Nieuwenhuizen WF, Weenen H, Rigby P, Hetherington MM. Older adults and patients in need of nutritional support: review of current treatment options and factors influencing nutritional intake. Clin Nutr. 2010;29(2):160‐169. [DOI] [PubMed] [Google Scholar]
- 23. Stratton RJ, Elia M. Encouraging appropriate, evidence‐based use of oral nutritional supplements. Proc Nutr Soc. 2010;69(4):477‐487. [DOI] [PubMed] [Google Scholar]
- 24. McMurdo ME, Price RJ, Shields M, Potter J, Stott DJ. Should oral nutritional supplementation be given to undernourished older people upon hospital discharge? A controlled trial. J Am Geriatr Soc. 2009;57(12):2239‐2245. [DOI] [PubMed] [Google Scholar]
- 25. Ginzburg Y, Shmilovitz I, Monastyrsky N, Endevelt R, Shahar DR. Barriers for nutritional care in the transition from hospital to the community among older patients. Clin Nutr ESPEN. 2018;25:56‐62. [DOI] [PubMed] [Google Scholar]
- 26. Gosney M. Are we wasting our money on food supplements in elder care wards? J Adv Nurs. 2003;43(3):275‐280. [DOI] [PubMed] [Google Scholar]
- 27. McCormick SE, Saquib G, Hameed Z, Glynn M, McCann D, Power DA. Compliance of acute and long stay geriatric patients with nutritional supplementation. Ir Med J. 2007;100(5):473‐475. [PubMed] [Google Scholar]
- 28. Kayser‐Jones J, Schell ES, Porter C, et al. A prospective study of the use of liquid oral dietary supplements in nursing homes. J Am Geriatr Soc. 1998;46(11):1378‐1386. [DOI] [PubMed] [Google Scholar]
- 29. Hubbard G, Buchan B, Sanders K, Brothers S, Stratton R. Improved compliance and increased intake of energy and protein with a high energy density, low volume multi‐nutrient supplement. Proc Nutr Soc. 2010;69(OCE2):E164. [Google Scholar]
- 30. Simmons SF, Patel AV. Nursing home staff delivery of oral liquid nutritional supplements to residents at risk for unintentional weight loss. J Am Geriatr Soc. 2006;54(9):1372‐1376. [DOI] [PubMed] [Google Scholar]
- 31. Akner G, Boström A‐M, Krachler B, et al. Kosttillägg för undernärda äldre: en systematisk litteraturöversikt. Stockholm, Sweden: SBU; 2014. [Google Scholar]
- 32. Kennelly S, Kennedy NP, Rughoobur GF, Slattery CG, Sugrue S. The use of oral nutritional supplements in an Irish community setting. J Hum Nutr Diet. 2009;22(6):511‐520. [DOI] [PubMed] [Google Scholar]
- 33. The National Board of Health and Welfare (Socialstyrelsen) . Näring för god vård och omsorg: en vägledning för att förebygga och behandla undernäring. Stockholm, Sweden: The National Board of Health and Welfare; 2011. [Google Scholar]
- 34. Gandy J. Manual of Dietetic Practice. 5th ed. Chichester, United Kingdom: John Wiley & Sons; 2014. [Google Scholar]
- 35. Bye A, Eklund A, Frick L, et al. Riktlinjer i Uppsala län fr.o.m . 2015‐01‐01 gällande livsmedel för särskilda näringsändamål. Uppsala kommun och Uppsala läns landsting; 2014. [Google Scholar]
- 36. Willis GB. Cognitive Interviewing: A Tool for Improving Questionnaire Design. Thousand Oaks, CA: Sage Publications; 2004. [Google Scholar]
- 37. Elia M. Screening for malnutrition: a multidisciplinary responsibility Development and Use of the Malnutrition Universal Screening Tool (‘MUST’) for Adults. Redditch, United Kingdom: Bristish Association for Parenteral and Enteral Nutrition (BAPEN); 2003. [Google Scholar]
- 38. Sattler EL, Lee JS, Perri M. Medication (re)fill adherence measures derived from pharmacy claims data in older Americans: a review of the literature. Drugs Aging. 2013;30(6):383‐399. [DOI] [PubMed] [Google Scholar]
- 39. Raper N, Perloff B, Ingwersen L, Steinfeldt L, Anand J. An overview of USDA's Dietary Intake Data System. J Food Compost Anal. 2004;17(3‐4):545‐555. [Google Scholar]
- 40. Andrade SE, Kahler KH, Frech F, Chan KA. Methods for evaluation of medication adherence and persistence using automated databases. Pharmacoepidemiol Drug Saf. 2006;15(8):565‐574. [DOI] [PubMed] [Google Scholar]
- 41. Bosworth HB. Enhancing Medication Adherence: The Public Health Dilemma. London, United Kingdom: Springer Healthcare Ltd; 2012. [Google Scholar]
- 42. Grass F, Bertrand PC, Schafer M, et al. Compliance with preoperative oral nutritional supplements in patients at nutritional risk horizontal line only a question of will? Eur J Clin Nutr. 2015;69(4):525‐529. [DOI] [PubMed] [Google Scholar]
- 43. Todorovic V. Evidence‐based strategies for the use of oral nutritional supplements. Br J Community Nurs. 2005;10(4):158, 160, 162‐154. [DOI] [PubMed] [Google Scholar]
- 44. Lad H, Gott M, Gariballa S. Elderly patients compliance and elderly patients and health professional's, views, and attitudes towards prescribed sip‐ feed supplements. J Nutr Health Aging. 2005;9(5):310‐314. [PubMed] [Google Scholar]
- 45. Paquay A, Baldwin C. A systematic review to identify the factors that affect compliance with oral nutritional supplements among older adults. J Hum Nutr Diet. 2010;23(3):327. [Google Scholar]
- 46. Liljeberg E, Andersson A, Lovestam E, Nydahl M. Incomplete descriptions of oral nutritional supplement interventions in reports of randomised controlled trials. Clin Nutr. 2018;37(1):61‐71. [DOI] [PubMed] [Google Scholar]
- 47. Hancock RE, Bonner G, Hollingdale R, Madden AM. ‘If you listen to me properly, I feel good’: a qualitative examination of patient experiences of dietetic consultations. J Hum Nutr Diet. 2012;25(3):275‐284. [DOI] [PubMed] [Google Scholar]
- 48. Makaryus AN, Friedman EA. Patients' understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005;80(8):991‐994. [DOI] [PubMed] [Google Scholar]
- 49. Cramer JA, Scheyer RD, Mattson RH. Compliance declines between clinic visits. Arch Intern Med. 1990;150(7):1509‐1510. [PubMed] [Google Scholar]
- 50. Feinstein AR. On white‐coat effects and the electronic monitoring of compliance. Arch Intern Med. 1990;150(7):1377‐1378. [PubMed] [Google Scholar]
- 51. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487‐497. [DOI] [PubMed] [Google Scholar]
- 52. Connor Gorber S, Tremblay M, Moher D, Gorber B. A comparison of direct vs. self‐report measures for assessing height, weight and body mass index: a systematic review. Obes Rev. 2007;8(4):307‐326. [DOI] [PubMed] [Google Scholar]
- 53. Sahyoun NR, Maynard LM, Zhang XL, Serdula MK. Factors associated with errors in self‐reported height and weight in older adults. J Nutr Health Aging. 2008;12(2):108‐115. [DOI] [PubMed] [Google Scholar]
- 54. Gibson RS. Principles of Nutritional Assessment. 2nd ed. New York, NY: Oxford University Press; 2005. [Google Scholar]
- 55. Turner BJ, Hecht FM. Improving on a coin toss to predict patient adherence to medications. Ann Intern Med. 2001;134(10):1004‐1006. [DOI] [PubMed] [Google Scholar]