

ABSTRACT
Sudden sensorineural hearing loss (SSNHL) after spinal-epidural anaesthesia is a very rare complication. The patient is a 25-year-old female who developed right-sided hearing loss, unbalance, a sensation of aural fullness and tinnitus 2 days post uncomplicated spinal-epidural anaesthesia for an emergency caesarean section. Initial management by her primary care physician for suspected eustachian tube dysfunction did not relieve symptoms, and 2 weeks subsequently, audiological assessment demonstrated right Sensorineural hearing loss (SNHL). Specialist consultation was sought, and the patient was commenced on systemic corticosteroids. Microscope otoscopy and posterior fossa magnetic resonance imaging were normal. High-resolution computed tomography scan demonstrated an enlarged right cochlear aqueduct. Repeat audiology after 2 weeks revealed unchanged hearing levels and improved speech discrimination scores in the right ear (from 53 to 90%). Repeat audiogram at 4 months and at 10 months showed no further improvement. Possible physiopathology of this complication, diagnostic dilemma and review of treatment options are discussed.
INTRODUCTION
Few cases of hearing loss following non-otological surgery have been reported, and the majority of these involve general anaesthesia and are associated with cardiopulmonary, laparoscopic, orthopaedic and urologic surgeries [1, 2]. Cases of hearing loss in association with spinal-epidural anaesthesia and lumbar puncture have been reported but are even more uncommon. The majority of patients’ hearing deficits are transient, often resolving without treatment within days; however, cases of permanent hearing loss have also been reported [3]. We present a case in which a patient developed sensorineural hearing loss (SNHL) post spinal-epidural anaesthesia for an emergency caesarean section.
CASE REPORT
A 26-year-old woman, primigravida and primipara, was admitted to the institution with spontaneous labour at full term. Emergency caesarean section was deemed necessary due to a prolonged latent phase of labour and foetal distress concerns as seen on cardiotocography. The patient was placed in an appropriate position for skin preparation with chlorhexidine, and then local infiltration was performed using 3 ml of 2% lidocaine. An 18-guage needle was used for the epidural catheter placement, and loss of resistance technique was used to identify the epidural space. The needle was inserted 5.5 cm cephalad into the epidural space at L3–4 by the midline approach. Then 12 ml of 0.2% ropivacaine and 16 micrograms of fentanyl was injected, followed by a ropivacaine and fentanyl infusion. Surgery was completed within 45 minutes, and no intraoperative complications transpired. Haemodynamic parameters remained normal throughout the perioperative period. The epidural catheter was removed within 12 hours postoperatively, with no complications. Day 1 postoperatively, the patient reported a sensation of light-headedness and dizziness but no headache. Day 2 postoperatively, she was discharged at home. No ototoxic medications were administered during admission or dispensed on discharge. On the same day, the patient noticed a constant right ear hearing loss, ongoing unbalance, a sensation of aural fullness and high-pitched non-pulsatile tinnitus. She attended her local primary care physician the same day and was treated with intranasal corticosteroids for possible eustachian tube dysfunction. Persistence of symptoms for 2 weeks prompted an audiological assessment which diagnosed a SNHL (Fig. 1). Urgent ENT specialist advice was sought over the phone, and the patient was commenced on systemic corticosteroids for 7 days (1 mg/kg of prednisone). The patient has no previous ear symptoms, no prior ear surgery, trauma or recent upper respiratory tract infection. A posterior fossa magnetic resonance imaging scan was performed but found no pathology. High-resolution temporal bone computed tomography (CT) scan demonstrated an enlarged right cochlear aqueduct (Fig. 2). Repeat audiological assessment in 2 weeks showed no pure tone audiometry change, but significant improvement in speech discrimination was present (53–90%). The patient was then seen in a specialist ENT clinic. Physical examination including microscopic otoscopy was unremarkable. Unilateral hearing loss management options were discussed with the patient, with conventional hearing amplification recommended. Repeat audiogram at 4 and 10 months’ time showed no further improvement but stabilised hearing. The patient has declined the use of amplification, and a recommendation to avoid further spinal-epidural anaesthesia was given.
Figure 1.
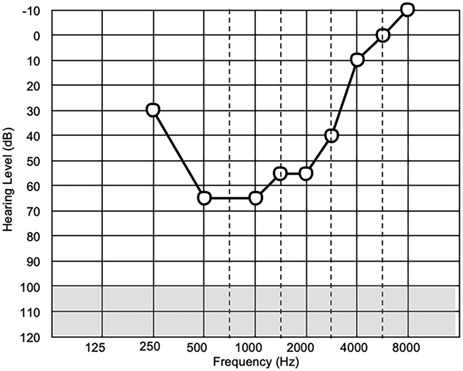
Patient’s audiological assessment 2 weeks after symptom onset.
Figure 2.
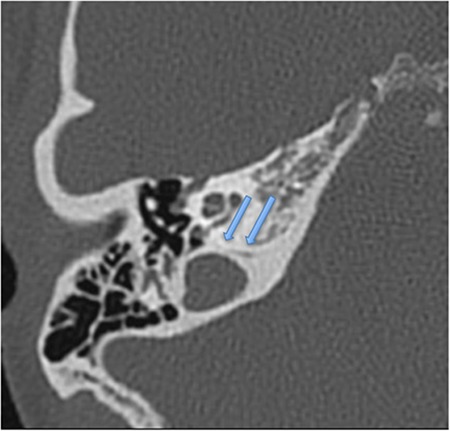
Patient’s CT scan showing an enlarged right cochlear aqueduct.
DISCUSSION
Hearing loss following non-cardiac surgery involving combined spinal-epidural anaesthesia has been reported before; however the incidence is estimated to be very low [4]. The majority of these cases involve temporary hearing loss, which typically returns to normal in 5–15 days. Hearing loss occurring primarily in lower frequency ranges (125–1000 Hz) [5]. Permanent hearing loss post spinal anaesthesia has been documented but is often combined with vertigo and tinnitus and is extremely rare [3]. The mechanism is theorised to result from disruption of the endolymph/perilymph balance caused by the decrease in cerebrospinal fluid (CSF) pressure due to CSF leakage from the epidural site. Decrease in perilymphatic pressure is transmitted via the cochlear aqueduct, fundus of the internal auditory canal, or the modiolus of the cochlea. This displaces hair cells in the basement membrane, resulting in low frequency hearing loss [6]. Our case describes a patient who underwent a combined spinal-epidural anaesthesia for an emergency caesarean section and subsequently suffered hearing loss which did not self-resolve in the usual time expected, was not associated with headache, and did not significantly improve post systemic corticosteroid administration. To the authors’ knowledge, there is only one similar report of SNHL following spinal-epidural anaesthesia without headache [7].
There have been previous controlled trials which after monitoring patients’ hearing by audiogram before and after spinal anaesthetic have concluded that patients under 40 [8] and obstetric patients are not at risk of hearing loss following spinal anaesthesia [9]. These studies also concluded that larger calibre needles would not induce enough CSG leakage to induce hearing effects. Our case illustrates that hearing loss can occur in young obstetric patients without headache following spinal-epidural anaesthesia.
Treatment of SNHL following spinal anaesthesia is controversial; however most patients recover spontaneously [10]. Treatment options for this complication are the same as with any other sudden SSNHL case and include observation, systemic corticosteroids (ideally delivered at onset of symptoms), hydration, cochlear vasodilators, betahistine, hyperbaric oxygen therapy, epidural blood patches, plasma expanders and carbogen inhalation. The results of all these treatment alternatives have been variable, and just like with sudden SSNHL, no standard treatment protocol is available at present [3, 5]. Nevertheless, it is the senior author’s preference to use initial systemic corticosteroids (prednisone 1 mg/kg daily, 7-day course), ideally within 72 hours of symptom onset, provided there are no contraindications for use of this medication. Trans-tympanic corticosteroid therapy may be considered as a salvage option in cases of failure with systemic corticosteroid therapy. In our case, systemic corticosteroid treatment was delayed by 2 weeks after the onset of symptoms, and this is likely to be a contributing factor in the limited hearing improvement experienced.
CONCLUSIONS
SNHL post spinal-epidural anaesthesia is a rare complication that is poorly understood. A high degree of suspicion is required for early diagnosis and treatment which may help prevent permanent hearing loss. It is not possible at this time to anticipate which patients are at higher risk of developing this complication post spinal-epidural anaesthesia; prompt attention and audiological assessment should be given to any patient who complains of hearing loss or tinnitus post epidural-spinal anaesthesia.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Funding
None.
REFERENCES
- 1. Ahmed MCM, Islam MS, Ahmmed S. Bilateral hearing loss after spinal anaesthesia. JAFMC Bangladesh 2009;5:3. [Google Scholar]
- 2. Vilhena D, Pereira L, Duarte D, Oliveira N. Sudden sensorineural hearing loss after orthopedic surgery under combined spinal and epidural anesthesia. Case Rep Otolaryngol 2016;2016:4295601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kilickan L, Gurkan Y, Ozkarakas H. Permanent sensorineural hearing loss following spinal anesthesia. Acta Anaesthesiol Scand 2002;46:1155–7. [DOI] [PubMed] [Google Scholar]
- 4. Sprung J, Bourke DL, Contreras MG, Warner ME, Findlay J. Perioperative hearing impairment. Anesthesiology 2003;98:241–57. [PubMed] [Google Scholar]
- 5. Yildiz TS, Solak M, Iseri M, Karaca B, Toker K. Hearing loss after spinal anesthesia: the effect of different infusion solutions. Otolaryngol Head Neck Surg 2007;137:79–82. [DOI] [PubMed] [Google Scholar]
- 6. Michel O, Brusis T. Hearing loss as a sequel of lumbar puncture. Ann Otol Rhinol Laryngol 1992;101:390–4. [DOI] [PubMed] [Google Scholar]
- 7. AG Benson RR. Unilateral sudden sensorineural hearing loss after spinal anesthesia for elective Cesarean section: a case report. J Anesth Clin Res. 2012;3. [Google Scholar]
- 8. Ok G, Tok D, Erbuyun K, Aslan A, Tekin I. Hearing loss does not occur in young patients undergoing spinal anesthesia. Reg Anesth Pain Med 2004;29:430–3. [DOI] [PubMed] [Google Scholar]
- 9. Finegold H, Mandell G, Vallejo M, Ramanathan S. Does spinal anesthesia cause hearing loss in the obstetric population? Anesth Analg 2002;95:198–203Table of contents. [DOI] [PubMed] [Google Scholar]
- 10. Gultekin S, Ozcan S. Does hearing loss after spinal anesthesia differ between young and elderly patients? Anesth Analg 2002;94:1318–20Table of contents. [DOI] [PubMed] [Google Scholar]