

Abstract
Background: Traumatic upper extremity amputation in a child can be a life-altering injury, yet little is known about the epidemiology or health care costs of these injuries. In this study, using the Healthcare Cost and Utilization Project (HCUP) Kids’ Inpatient Database (KID), we assess these trends to learn about the risk factors and health care costs of these injuries. Methods: Using the HCUP KID from 1997 to 2012, patients aged 20 years old or younger with upper extremity traumatic amputations were identified. National estimates of incidence, demographics, costs, hospital factors, patient factors, and mechanisms of injury were assessed. Results: Between 1997 and 2012, 6130 cases of traumatic upper extremity amputation occurred in children. This resulted in a $166 million cost to the health care system. Males are 3.4 times more likely to be affected by amputation than females. The most common age group to suffer amputation is in older children, aged 15 to 19 years old. The frequency of amputation has declined 41% from 1997 to 2012. The overwhelming majority of amputations (92.54%) involved digits. Conclusions: Pediatric traumatic amputations of the upper extremity are a significant contribution to health care spending. Interventions and educational campaigns can be targeted based on national trends to prevent these costly injuries.
Keywords: amputation, pediatric, upper extremity, trauma, adolescent, preventative, hand
Introduction
Traumatic amputations in children are relatively rare, ranging from 1.32 to 18.8 per 100 000 in varying reports.2,12-14 The costs from these injuries to the individual and to society can be great. The average cost of a traumatic pediatric amputation can be upward of $22 000 in hospital charges alone.32 In adult patients, the direct health care costs of traumatic lower extremity amputations during the first 2 years is more than $90 000, with lifetime costs surpassing $500 000, excluding indirect costs of lost wages from loss of function.29 In addition to functional limitations, patients with amputations are at higher risk for subsequent psychiatric disorders, and up to 30% of adult amputees have depression.17,20 In children, specifically, amputation injuries can severely limit psychosocial development, independence, and body image.19,31
Multiple case series exist about various mechanisms of upper extremity amputations. Most of these injuries are to fingers and are the result of a diverse array of causes including fireworks, slammed doors, exercise bicycles, farm equipment, and shop class.4-6,9,11,12,22,24,25,27,28 Replantation and revascularization can be successful in this patient population compared with adults as described in several case series.1,3,7,26,30,35 The incidence, temporal trends, and patient characteristics of upper extremity traumatic amputations in children are largely unknown. Given the severity of consequences and the lifetime impact of pediatric traumatic upper extremity amputation, it is essential to determine the incidence and predisposing risk factors of this injury to improve preventative strategies and treatment.
The purpose of this study is to assess the incidence, patient demographics, health system factors, and use of health care resources in traumatic upper extremity amputation in patients younger than 20 years old in the United States using a large nationwide inpatient database.
Patients and Methods
Data Source
Data were obtained from the Kids’ Inpatient Database (KID) from January 1, 1997, to December 31, 2012. The KID is a national, all-payer database of the Healthcare Cost and Utilization Project (HCUP) maintained by the Agency for Healthcare Research and Quality (AHRQ).21 The KID database is available every 3 years, with the most recent year including 44 states, for a total of more than 17 million unweighted hospital encounters in patients 20 years old and younger. These deidentified records are available from public, private, and academic hospitals and all regions of the country. These data include only inpatient records. The KID is derived from a state-level sampling of hospital discharges. Random sampling is used to select 80% of pediatric cases. The records are stratified based on region, hospital location and ownership, bed size, and teaching status to generate weighted data to allow researchers to investigate national trends.21,31 Due to the nature of deidentified data in the KID, neither ethical approval nor informed consent were required.
Study Population
Patients were identified using International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes. The ICD-9 codes used were 885.0, 885.1, 886.0, 886.1, and 887.0 to 887.7 denoting complete and partial traumatic amputations of the thumb, fingers, and arm below and above the elbow. Only cases where these codes are primary or secondary diagnoses were used in an effort to exclude cases with concomitant major nonamputation injuries that could confound results. Patients from 1997 were compared with those from 2012 to assess for temporal changes in these variables. Patients were then split into 4 cohorts based on level of amputation to determine the difference in patient and hospital characteristics and risk factors among these varying injuries. Next, patients were categorized by age group to determine factors affecting amputation trends by age. The ICD-9 external cause of injury codes (E codes) were used to analyze the mechanism of injury and assess temporal trends, and associations between age, sex, and level of amputation with mechanism of injury. These codes were not available prior to 2003; therefore, mechanism-of-injury data are reported from 2003 to 2012.
Statistical Analysis
The KID uses hospital-level sampling weights to account for error in random sampling methods and provide national estimates of hospitalizations.21 Categorical variables were assessed with a chi-square test, and continuous variables were assessed with a t test. Rates of hospitalizations per 100000 were generated using the US 2000 Census data.33 A P value of less than .05 was used as a threshold for significance.
Results
A total of 6130 weighted discharges for any traumatic upper extremity amputation were identified. The mean age of the amputation group was 12.11 ± 0.12 years old. The upper extremity amputation group was 77.33% male. Further demographic information is presented in Table 1. Average length of stay was 3.41 ± 0.08 days, resulting in mean hospital charges of $28 961.72 ± $945.36. In the period from 1997 to 2012, these injuries resulted in combined total hospital charges over $166 million. These patients were more likely to be treated at large, government, urban, or teaching hospitals (Table 1). In nearly half the patients affected by traumatic amputation, no mechanism of injury was specified. In those with a listed mechanism, machinery injuries, the extremity being caught between objects, and power tools were the most common causes of injury (Table 1). Rates of admission for amputation showed a significant increase in July and August (Figure 1), a trend which was driven largely by explosives, fireworks, and firearms injuries in males (P < .0001).
Table 1.
Demographic Information, Hospital Charges, Mechanism of Injury, and Hospital Characteristics for Pediatric Patients Suffering Traumatic Upper Extremity Amputation From 1997 to 2012.
| Variable | National estimate (n = 6130) | % |
|---|---|---|
| Age (mean), years (SD) | 12.11 (0.11) | |
| Mean charge, dollars (SD) | 28 961.72 (945.36) | |
| Median, dollars | 14 635.50 | |
| Estimated total charge, dollars | 166 161 910.54 | |
| Race | ||
| White | 2734 | 56.22 |
| Black | 609 | 12.53 |
| Hispanic | 1105 | 22.73 |
| Asian or Pacific Islander | 87 | 1.78 |
| Native American | 54 | 1.11 |
| Other | 273 | 5.62 |
| Sex (Female) | 1372 | 22.67 |
| Primary payment | ||
| Medicare | 9 | 0.15 |
| Medicaid | 1595 | 26.13 |
| Private, including health maintenance organization | 2809 | 46.04 |
| Self-pay | 621 | 10.18 |
| No charge | 28 | 0.45 |
| Other payment | 1040 | 17.05 |
| Mechanism of injury | ||
| Lawn mower/machinery | 729 | 11.89 |
| Caught between objects | 640 | 10.44 |
| Power tools/other cutting instruments | 557 | 9.08 |
| Motor vehicle accident | 294 | 4.79 |
| Explosives, fireworks, firearms | 142 | 2.32 |
| Struck accidentally by falling object | 109 | 1.78 |
| Striking against or struck accidentally by objects or persons | 99 | 1.61 |
| Bicycle | 46 | 0.75 |
| Other | 688 | 11.23 |
| Unspecified | 2826 | 46.11 |
| Bed size of hospital | ||
| Small | 377 | 7.73 |
| Medium | 972 | 19.94 |
| Large | 3523 | 72.33 |
| Ownership of hospital | ||
| Government/private collapsed category | 3326 | 79.55 |
| Government, nonfederal, public | 106 | 2.53 |
| Private, nonprofit, voluntary | 437 | 10.46 |
| Private, invest-own | 204 | 4.89 |
| Private, collapsed category | 107 | 2.57 |
| Hospital location setting | ||
| Rural | 303 | 7.25 |
| Urban | 3879 | 92.75 |
| Location/teaching status of hospital | ||
| Rural | 328 | 6.74 |
| Urban, nonteaching | 974 | 19.99 |
| Urban, teaching | 3569 | 73.27 |
| Region of hospital | ||
| Northeast | 898 | 18.13 |
| Midwest | 980 | 19.78 |
| South | 1799 | 36.33 |
| West | 1276 | 25.76 |
| Teaching status of hospital | ||
| Nonteaching | 1123 | 26.86 |
| Teaching | 3058 | 73.14 |
Figure 1.
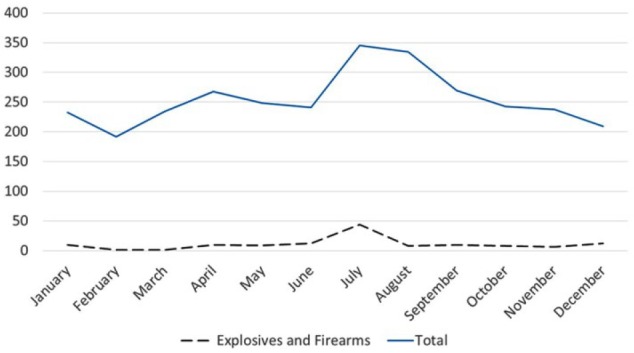
Admissions for upper extremity pediatric amputation per month, with contribution from firework and explosive injuries.
Traumatic amputation was most common in children aged 15 to 19 years old, followed by those who were 0 to 4 years old, a trend that has remained consistent in all years of the database (Figure 2). Mean length of stay increased with increasing age, from 2.55 ± 3.57 days to 3.76 ± 5.22 days (P < .0001), with a corresponding increase in hospital charge from $20 748.92 ± $37 416.99, for the youngest age group, to $33 758.54 ± $70 343.37 (P < .0001). The disparity in sex increased with older patient age, with females comprising 39.62% of patients affected by amputation in the 0 to 4 age group, but only 14.61% of the group aged 15 to 19 (P < .0001) (Table 2). Rates of alcohol abuse, drug abuse, depression, and psychoses in patients with traumatic upper extremity amputation were significantly increased in older patients (Table 2). In children aged 0 to 4 and 5 to 9, having the extremity caught between objects was the most common mechanism of injury, while in patients aged 15 to 19, lawn mowers and machinery were the most common cause of injury (Supplemental Figure 1). In patients aged 15 to 19 years old, alcohol abuse, depression, and psychoses significantly increased the odds of suffering above the elbow amputation (Table 3).
Figure 2.

Pediatric amputations by age group per year.
Table 2.
Demographic Information, Hospital Charges, and Comorbidities for Pediatric Patients Suffering Traumatic Upper Extremity Amputations per Age Group.
| Age 0-4 (n = 1003) |
Age 5-9 (n = 665) |
Age 10-14 (n = 797) |
Age 15-19 (n = 1973) |
P value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Length of stay (days) | 2.55 | 3.57 | 2.97 | 4.16 | 3.65 | 4.93 | 3.76 | 5.22 | <.0001 |
| Total charge (dollars) | 20 748.92 | 37 416.99 | 24 283.86 | 33 332.72 | 27 801.32 | 45 448.60 | 33 758.54 | 70 343.37 | <.0001 |
| Frequency | % | Frequency | % | Frequency | % | Frequency | % | ||
| Sex (Female) | 503 | 39.62 | 268 | 31.29 | 199 | 19.04 | 351 | 14.61 | <.0001 |
| Race | <.0001 | ||||||||
| White | 489 | 45.48 | 361 | 51.78 | 565 | 68.86 | 1139 | 59.56 | |
| Black | 177 | 16.43 | 138 | 19.74 | 99 | 12.05 | 156 | 8.14 | |
| Hispanic | 289 | 26.86 | 127 | 18.14 | 108 | 13.18 | 474 | 24.78 | |
| Asian or Pacific Islander | 37 | 3.47 | 16 | 2.31 | 3 | 0.35 | 26 | 1.35 | |
| Native American | 13 | 1.2 | 8 | 1.16 | 13 | 1.61 | 19 | 0.97 | |
| Other | 71 | 6.56 | 48 | 6.86 | 32 | 3.95 | 99 | 5.2 | |
| Comorbidities | |||||||||
| Alcohol abuse | 0 | 0 | 0 | 0 | 0 | 0 | 26 | 1.88 | <.0001 |
| Depression | 0 | 0 | 0 | 0 | 0 | 0 | 26 | 1.83 | <.0001 |
| Drug abuse | 0 | 0 | 0 | 0 | 0 | 0 | 15 | 1.09 | <.0001 |
| Psychoses | 0 | 0 | 0 | 0 | 5 | 0.78 | 17 | 1.23 | .032 |
| Mechanism | <.0001 | ||||||||
| Lawn mower/machinery | 72 | 7.14 | 58 | 8.79 | 98 | 12.26 | 390 | 19.76 | |
| Caught between objects | 242 | 24.11 | 152 | 22.81 | 108 | 13.54 | 112 | 5.68 | |
| Cutting instruments | 90 | 8.93 | 67 | 10.13 | 80 | 10.00 | 260 | 13.17 | |
| Motor vehicle accident | 58 | 5.79 | 35 | 5.26 | 34 | 4.27 | 126 | 6.37 | |
| Explosives and firearms | 3 | 0.29 | 4 | 0.67 | 51 | 6.42 | 68 | 3.46 | |
| Other | 189 | 18.81 | 130 | 19.49 | 156 | 19.57 | 340 | 17.21 | |
| Unspecified | 350 | 34.94 | 218 | 32.86 | 270 | 33.95 | 677 | 34.35 | |
Table 3.
Odds Ratio by Level of Amputation and Comorbidity in Children Aged 15 to 19 Years Old.
| Comorbidity | Finger amputation |
Thumb amputation |
Below-elbow amputation |
Above-elbow amputation |
||||
|---|---|---|---|---|---|---|---|---|
| Odds ratio | P value | Odds ratio | P value | Odds ratio | P value | Odds ratio | P value | |
| Alcohol abuse | 0.703 | .470 | 0.423 | .254 | 2.179 | .308 | 5.626 | .009 |
| Drug abuse | 0.296 | .061 | 5.265 | .011 | 1.000 | 1.000 | 1.000 | 1.000 |
| Depression | 0.638 | .366 | 0.451 | .294 | 2.327 | .271 | 6.035 | .007 |
| Psychoses | 0.899 | .864 | 1.000 | 1.000 | 1.562 | .672 | 9.441 | .001 |
Finger and thumb amputations comprised the vast majority of pediatric traumatic amputations, accounting for a total of 93.82% of total upper extremity amputation volume (Table 4), which was persistent through all collected time points (Supplemental Figure 2). Males made up an overwhelming majority for each level of amputation (Table 4). The mean age of patients with arm (14.20 ± 5.92 years) and forearm (14.64 ± 5.58 years) amputations was higher than those with thumb (13.53 ± 5.99 years) and finger (11.49 ± 6.64 years) amputations (Table 4). Length of stay was significantly longer for above-elbow amputations (14.02 ± 12.85 days) and below-elbow amputations (10.03 ± 10.02 days) compared with children with finger (2.51 ± 2.96 days) and thumb (3.86 ± 4.20 days) (P < .0001). Consequently, total charges followed a similar pattern with average above-elbow amputation costs that were 7-fold higher than finger amputation costs ($153 439.70 ± $202 184.50 vs $20 513.16 ± 25 280.97, P < .0001) (Table 4). Children with higher levels of amputation had increased loss of function, increased risk of mortality, and increased discharge to nursing or rehabilitation facilities (P < .0001) (Table 4). There was a higher rate of alcohol abuse, depression, drug abuse, and psychoses with increasingly proximal amputation levels (P < .02) (Table 4). Above-elbow amputations were most commonly caused by motor vehicle accidents, while digital amputations were most often associated with lawn mowers and machinery, being caught between objects, and cutting instruments (Supplemental Figure 3). Children with below-elbow and above-elbow amputations were more commonly treated at urban teaching hospitals than nonteaching or rural hospitals when compared with patients with digit amputations (P < .0001) (Table 4).
Table 4.
Demographic Information, Hospital Charges, Comorbidities, Hospital Characteristics, Patient Characteristics for Pediatric Patients Suffering Traumatic Upper Extremity Amputations per Level of Amputation.
| Finger (n = 4573) |
Thumb (n = 1178) |
Below elbow (n = 298) |
Above elbow (n = 142) |
P value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Age | 11.49 | 6.64 | 13.53 | 5.99 | 14.64 | 5.58 | 14.20 | 5.92 | <.0001 |
| Length of stay (days) | 2.51 | 2.96 | 3.86 | 4.20 | 10.03 | 10.02 | 14.02 | 12.85 | <.0001 |
| Total charge (dollars) | 20 513.16 | 25 280.97 | 28 591.09 | 32 034.40 | 94 510.32 | 131 560.20 | 153 439.70 | 202 184.50 | <.0001 |
| Frequency | Percentage | Frequency | Percentage | Frequency | Percentage | Frequency | Percentage | ||
| Sex (Female) | 1064 | 23.98 | 193 | 16.63 | 70 | 23.75 | 38 | 27 | .001 |
| Race | .05 | ||||||||
| White | 1968 | 54.93 | 539 | 58.86 | 148 | 63.98 | 71 | 60.14 | |
| Black | 480 | 13.41 | 101 | 11.07 | 21 | 9.19 | 5 | 4.09 | |
| Hispanic | 843 | 23.53 | 200 | 21.84 | 27 | 11.6 | 30 | 25.58 | |
| Asian or Pacific Islander | 63 | 1.75 | 11 | 1.24 | 8 | 3.57 | 5 | 3.8 | |
| Native American | 29 | 0.82 | 15 | 1.62 | 7 | 3.05 | 3 | 2.45 | |
| Other | 200 | 5.57 | 49 | 5.36 | 20 | 8.61 | 5 | 3.95 | |
| Comorbidities | |||||||||
| Alcohol abuse | 19 | 0.74 | 4 | 0.65 | 4 | 2.48 | 6 | 6.39 | <.0001 |
| Depression | 16 | 0.59 | 3 | 0.44 | 6 | 3.24 | 4 | 4.8 | <.0001 |
| Drug abuse | 13 | 0.5 | 10 | 1.55 | 7 | 3.75 | 1 | 1.59 | .014 |
| Psychoses | 16 | 0.61 | 3 | 0.43 | 3 | 1.64 | 4 | 4.57 | .004 |
| Severity of illness | <.0001 | ||||||||
| No class specified | |||||||||
| Minor loss of function | 1609 | 61.22 | 367 | 54.26 | 43 | 24.99 | 0 | 0 | |
| Moderate loss of function | 883 | 33.61 | 252 | 37.25 | 70 | 40.17 | 18 | 20.68 | |
| Major loss of function | 130 | 4.96 | 56 | 8.25 | 37 | 21.14 | 35 | 39.66 | |
| Extreme loss of function | 6 | 0.21 | 2 | 0.24 | 24 | 13.7 | 35 | 39.67 | |
| Risk of mortality | <.0001 | ||||||||
| Minor likelihood of dying | 2604 | 99.09 | 670 | 99.08 | 147 | 84.82 | 42 | 47.32 | |
| Moderate likelihood of dying | 15 | 0.57 | 6 | 0.92 | 14 | 8.27 | 12 | 13.05 | |
| Major likelihood of dying | 5 | 0.17 | 0 | 0 | 9 | 5.12 | 21 | 23.49 | |
| Extreme likelihood of dying | 4 | 0.17 | 0 | 0 | 3 | 1.79 | 14 | 16.14 | |
| Primary payment | .02 | ||||||||
| Medicare | 6 | 0.14 | 3 | 0.26 | 0 | 0 | 0 | 0 | |
| Medicaid | 1207 | 26.91 | 274 | 23.48 | 73 | 24.83 | 37 | 26.69 | |
| Private, including health maintenance organization | 2060 | 45.95 | 509 | 43.69 | 140 | 47.63 | 90 | 64.31 | |
| Self-pay | 448 | 10 | 134 | 11.51 | 31 | 10.45 | 3 | 2.11 | |
| No charge | 18 | 0.39 | 7 | 0.6 | 1 | 0.45 | 2 | 1.25 | |
| Other payment | 745 | 16.61 | 238 | 20.46 | 49 | 16.64 | 8 | 5.64 | |
| Disposition of patient | <.0001 | ||||||||
| Routine | 3506 | 96.24 | 892 | 95.98 | 188 | 79.5 | 74 | 59.11 | |
| Transfer to short-term hospital | 36 | 0.98 | 9 | 0.97 | 6 | 2.68 | 6 | 4.91 | |
| Other transfers (nursing, intermediate) | 10 | 0.26 | 1 | 0.15 | 9 | 3.86 | 27 | 21.85 | |
| Home health care | 82 | 2.25 | 26 | 2.75 | 33 | 13.96 | 13 | 10.4 | |
| Against medical advice | 7 | 0.19 | 1 | 0.15 | 0 | 0 | 0 | 0 | |
| Died in hospital | 3 | 0.08 | 0 | 0 | 0 | 0 | 5 | 3.73 | |
| Frequency | Percentage | Frequency | Percentage | Frequency | Percentage | Frequency | Percentage | ||
| Hospital location setting | .018 | ||||||||
| Rural | 258 | 8.43 | 35 | 4.34 | 9 | 4.25 | 2 | 1.76 | |
| Urban | 2801 | 91.57 | 766 | 95.66 | 192 | 95.75 | 105 | 98.24 | |
| Location/teaching status of hospital | <.0001 | ||||||||
| Rural | 279 | 7.76 | 39 | 4.3 | 9 | 3.66 | 2 | 1.58 | |
| Urban, nonteaching | 783 | 21.8 | 152 | 16.68 | 27 | 11.56 | 9 | 7.34 | |
| Urban, teaching | 2530 | 70.44 | 721 | 79.02 | 198 | 84.77 | 108 | 91.08 | |
| Region of hospital | .022 | ||||||||
| Northeast | 709 | 19.45 | 131 | 14.12 | 38 | 16.31 | 16 | 12.88 | |
| Midwest | 710 | 19.48 | 178 | 19.12 | 64 | 27.13 | 28 | 22.63 | |
| South | 1301 | 35.71 | 345 | 37.16 | 86 | 36.66 | 53 | 42.31 | |
| West | 924 | 25.36 | 275 | 29.6 | 47 | 19.9 | 28 | 22.17 | |
| Teaching status of hospital | <.0001 | ||||||||
| Nonteaching | 905 | 29.59 | 173 | 21.62 | 33 | 16.31 | 9 | 8.69 | |
| Teaching | 2153 | 70.41 | 628 | 78.38 | 168 | 83.69 | 97 | 91.31 | |
The overall incidence of traumatic upper extremity amputation in children has declined 41.4% in the period from 1997 to 2012 (Figure 3), and length of stay between 1997 and 2012 has decreased 28.4% (P = .02). Despite decreased length of stay, mean costs increased from $14 913.39 ± $21 326.09 in 1997 to $46 544.26 ± $76 573.81 in 2012 (P < .001). When accounting for inflation, mean costs more than doubled from 2003 to 2012 (P < .001).34 The average age of patients affected by traumatic amputation increased from 10.62 ± 6.03 years in 1997 to 11.09 ± 6.83 years in 2012 (P = .02). The distribution of mechanisms of injury causing amputation varied significantly from 2003 to 2012. Injuries from the extremity being caught between objects, lawn mowers, and machinery decreased significantly (P < .001, P = .001, P = .017, respectively), while motor vehicle accidents as a cause of traumatic upper extremity amputation nearly tripled (P < .001). Rates of injury from power tools, bicycles, explosives, and firearms did not significantly change over this time period (Supplemental Figure 4).
Figure 3.
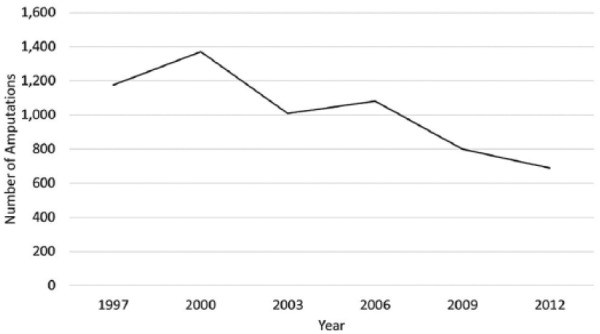
Temporal trend in incidence of traumatic upper extremity amputation in children.
Discussion
From 1997 to 2012, there were an estimated 6130 traumatic upper extremity amputations in pediatric patients in the United States. These injuries place a $21 million annual financial burden on the health care system.13 In our study, traumatic upper extremity amputations occurred at rate of 0.85 to 1.70 per 100 000 persons below 20 years old.33 Our rate is lower than some published rates in the literature that are upward of 10 per 100 000.12,18 However, our study only accounts for patients treated in the inpatient setting, as the KID excludes patients treated solely in the emergency department. When compared with other studies that use the KID, this incidence is consistent.13,31
Pediatric patients suffering from amputations of the upper extremity were most commonly teenagers, aged 15 to 19 years old, with the second most common age group being 0 to 4 years old, consistent with previously published studies.12,18,27 Machinery and power tools were the most common mechanisms of injury in children aged 15 to 19 years. This is in contrast with younger children aged 0 to 4 and 5 to 9, for whom amputations were most frequently caused by the extremity being caught between objects. The former was likely due to teenagers participating in shop class, beginning occupations that may require power tool use, or simply using a power tool without proper supervision or education.4,22
Young children are highly inquisitive and less fearful, potentially leading to their increased rate of injury. Males were far more likely to suffer from a traumatic amputation requiring hospital admission than females, especially with increasing age, a trend seen in most publications describing amputation in both children and adults.8,12,13,18,27,31 Rates of admission for amputation were much higher in July and August when children have summer vacations, due to the increased rate of explosive injuries during these months. Prevention measures addressing machinery safety and firework regulation may potentially significantly decrease the rate of these injuries in children and adolescents.
In upper extremity amputation, the overwhelming majority affected fingers and thumbs while a small minority was of the forearm or above the elbow, consistent with previously published reports.18 Motor vehicle accidents caused the majority of above-elbow amputations, while digital amputations were most frequently caused by digits being caught between objects, cutting instruments, or lawn mowers and machinery. The rate of amputation has been declining, and by 2012, there were 41.4% fewer amputations than in 1997. Fewer amputations were caused by lawn mower injuries, machinery, and being caught between objects, potentially due to automatic protections on power tools, more widely available safeguards to childproof doors, and increased awareness.15,16 However, motor vehicle accidents became an increasingly common cause for amputation. It is unclear in this database whether children in motor vehicle accidents were passengers or adolescent drivers, and the cause for this increase is unknown. Given the severity and functional deficits of amputation at more proximal levels because of motor vehicle accidents, prevention strategies aimed at improving the safety of teenage drivers may decrease the incidence of this devastating injury.
Depression, substance abuse, and psychoses were prominent comorbidities associated with amputation, especially with increasing age and more proximal levels of amputation. This database does not account for self-inflicted mechanisms of injury or if patients were intoxicated at the time of injury. Addressing mental health and substance abuse, especially in adolescents, may be vital in decreasing the rate of injury particularly at more proximal levels.23
Hospital costs related to traumatic upper extremity amputations were very high, and in the 6 years analyzed, total charges exceeded $166 million. Hospital charges were 62% higher for patients aged 15 to 19 than for patients aged 0 to 4, while length of stay was 47% higher for older patients. More proximal levels of amputation increased hospital costs, with above-elbow amputations costing 7.4 times more than finger amputations, and length of stay was 5.5 times longer in above-elbow amputations than finger amputations. This is likely because more complex surgeries and more intensive rehabilitation were required. Through the study period, the average costs nearly doubled despite accounting for inflation, while general US inflation-adjusted health care spending rose by approximately 5.4% annually.10
This study has several limitations inherent to a database study. This is a retrospective observational review of a national database searched by ICD-9 codes and is subject to inaccuracies in coding and incomplete data, most notably for mechanism of injury. The KID only includes inpatients, so any revision amputation performed in an emergency setting is not captured. Outcome data are limited and there is no follow-up data to determine clinical results. Finally, this database study allows us to draw only correlative associations and we cannot conclude the reasons behind trends in patterns. However, this study does provide valuable information regarding national trends in pediatric upper extremity amputations and can provide insight in prevention. This is the largest cohort of pediatric patients assessed using the KID which allows for evaluation of previously underpowered trends.
In conclusion, though pediatric upper extremity amputations are decreasing in incidence, they are still a sizable cause of morbidity in children. Males were affected nearly 3 times more often than females, and very young children and adolescents were disproportionately affected by traumatic amputation. These injuries were more common during the summer months, though this increase was solely due to explosive and firework use. In very young children, fingers caught between objects was the most common mechanism of injury and may be addressed with improved child safety devices. Children should avoid heavy machinery and lawn mowers, while teenagers using such equipment should be carefully instructed and closely monitored. To prevent proximal amputation levels related to car accidents, children should be safely secured with a seat belt and car seat if necessary, with hands kept in the vehicle. If mental health concerns or substance abuse is suspected, treatment should be sought expeditiously to mitigate the risk of life-altering injuries.
Supplementary Material
Supplemental Material, DS_10.1177_1558944718777865 for Trends in Pediatric Traumatic Upper Extremity Amputations by Venus Vakhshori, Gabriel J. Bouz, Cory K. Mayfield, Ram K. Alluri, Milan Stevanovic and Alidad Ghiassi in HAND
Footnotes
Supplemental material is available in the online version of the article.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval: This study was approved by our institutional review board.
Statement of Human and Animal Rights: This article does not contain any studies with human or animal subjects.
Statement of Informed Consent: Deidentified database records were used, and therefore informed consent was not required.
ORCID iDs: V Vakhshori  https://orcid.org/0000-0002-8509-7619
https://orcid.org/0000-0002-8509-7619
CK Mayfield
https://orcid.org/0000-0001-5268-3817
References
- 1. Abzug JM, Kozin SH. Pediatric replantation. J Hand Surg. 2014;39(1):143-145. doi: 10.1016/j.jhsa.2013.09.002. [DOI] [PubMed] [Google Scholar]
- 2. Atroshi I, Rosberg HE. Epidemiology of amputations and severe injuries of the hand. Hand Clin. 2001;17(3):343-350, vii. [PubMed] [Google Scholar]
- 3. Baker GL, Kleinert JM. Digit replantation in infants and young children: determinants of survival. Plast Reconstr Surg. 1994;94(1):139-145. [DOI] [PubMed] [Google Scholar]
- 4. Beavis RC, Classen DA. Hand trauma in shop class. J Pediatr Orthop. 2006;26(1):36-38. doi: 10.1097/01.bpo.0000188997.13803.25. [DOI] [PubMed] [Google Scholar]
- 5. Benson LS, Waters PM, Meier SW, et al. Pediatric hand injuries due to home exercycles. J Pediatr Orthop. 2000;20(1):34-39. [PubMed] [Google Scholar]
- 6. Berger LR, Kalishman S, Rivara FP. Injuries from fireworks. Pediatrics. 1985;75(5):877-882. [PubMed] [Google Scholar]
- 7. Beris AE, Soucacos PN, Malizos KN, et al. Major limb replantation in children. Microsurgery. 1994;15(7):474-478. [DOI] [PubMed] [Google Scholar]
- 8. Borne A, Porter A, Recicar J, et al. Pediatric traumatic amputations in the United States: A 5-year review. J Pediatr Orthop. 2017;37(2):e104-e107. doi: 10.1097/BPO.0000000000000693. [DOI] [PubMed] [Google Scholar]
- 9. Bull MJ, Agran P, Gardner HG, et al. Lawn mower-related injuries to children. Pediatrics. 2001;107(6):1480-1481. [DOI] [PubMed] [Google Scholar]
- 10. Catlin AC, Cowan CA. History of health spending in the United States, 1960-2013. Center for Medicare and Medicaid Services website. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/HistoricalNHEPaper.pdf. November 19, 2015.
- 11. Claudet I, Toubal K, Carnet C, et al. [When doors slam, fingers jam!]. Arch Pediatr Organe Off Soc Francaise Pediatr. 2007;14(8):958-963. doi: 10.1016/j.arcped.2007.03.019. [DOI] [PubMed] [Google Scholar]
- 12. Conn JM, Annest JL, Ryan GW, et al. Non-work-related finger amputations in the United States, 2001-2002. Ann Emerg Med. 2005;45(6):630-635. doi: 10.1016/j.annemergmed.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 13. Conner KA, McKenzie LB, Xiang H, et al. Pediatric traumatic amputations and hospital resource utilization in the United States, 2003. J Trauma. 2010;68(1):131-137. doi: 10.1097/TA.0b013e3181a5f2ec. [DOI] [PubMed] [Google Scholar]
- 14. Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the United States. South Med J. 2002;95(8):875-883. [DOI] [PubMed] [Google Scholar]
- 15. Doraiswamy NV. Childhood finger injuries and safeguards. Inj Prev J Int Soc Child Adolesc Inj Prev. 1999;5(4):298-300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Graham JD, Chang J. Reducing the risk of injury from table saw use: the potential benefits and costs of automatic protection. Risk Anal Off Publ Soc Risk Anal. 2015. February;35(2):307-317. doi: 10.1111/risa.12258. [DOI] [PubMed] [Google Scholar]
- 17. Grob M, Papadopulos NA, Zimmermann A, et al. The psychological impact of severe hand injury. J Hand Surg Eur. 2008;33(3):358-362. doi: 10.1177/1753193407087026. [DOI] [PubMed] [Google Scholar]
- 18. Hostetler SG, Schwartz L, Shields BJ, et al. Characteristics of pediatric traumatic amputations treated in hospital emergency departments: United States, 1990-2002. Pediatrics. 2005;116(5):e667-e674. doi: 10.1542/peds.2004-2143. [DOI] [PubMed] [Google Scholar]
- 19. Jaeger SH, Tsai TM, Kleinert HE. Upper extremity replantation in children. Orthop Clin North Am. 1981;12(4):897-907. [PubMed] [Google Scholar]
- 20. Kashani JH, Frank RG, Kashani SR, et al. Depression among amputees. J Clin Psychiatry. 1983;44(7):256-258. [PubMed] [Google Scholar]
- 21. KID Database Documentation. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality; 2017. [PubMed] [Google Scholar]
- 22. Knight S, Junkins EP, Lightfoot AC, et al. Injuries sustained by students in shop class. Pediatrics. 2000;106(1, pt 1):10-13. [DOI] [PubMed] [Google Scholar]
- 23. Large M, Babidge N, Andrews D, et al. Major self-mutilation in the first episode of psychosis. Schizophr Bull. 2009;35(5):1012-1021. doi: 10.1093/schbul/sbn040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lehrer MS, Bozentka DJ, Partington MT, et al. Pediatric hand injuries due to exercise bicycles. J Trauma. 1997;43(1):100-102. [DOI] [PubMed] [Google Scholar]
- 25. Letton RW, Chwals WJ. Patterns of power mower injuries in children compared with adults and the elderly. J Trauma. 1994;37(2):182-186. [DOI] [PubMed] [Google Scholar]
- 26. Linnaus ME, Langlais CS, Kirkilas M, et al. Outcomes of digital artery revascularization in pediatric trauma. J Pediatr Surg. 2016;51(9):1543-1547. doi: 10.1016/j.jpedsurg.2016.04.011. [DOI] [PubMed] [Google Scholar]
- 27. Lubicky JP, Feinberg JR. Fractures and amputations in children and adolescents requiring hospitalization after farm equipment injuries. J Pediatr Orthop. 2009;29(5):435-438. doi: 10.1097/BPO.0b013e3181aa21ab. [DOI] [PubMed] [Google Scholar]
- 28. MacKenzie DN, Green JA, Viglione W. Firecracker injuries to the hand. Med J Aust. 2001;174(5):231-232. [DOI] [PubMed] [Google Scholar]
- 29. MacKenzie EJ, Jones AS, Bosse MJ, et al. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007;89(8):1685-1692. doi: 10.2106/JBJS.F.01350. [DOI] [PubMed] [Google Scholar]
- 30. Shi D, Qi J, Li D, et al. Fingertip replantation at or beyond the nail base in children. Microsurgery. 2010;30(5):380-385. doi: 10.1002/micr.20743. [DOI] [PubMed] [Google Scholar]
- 31. Squitieri L, Reichert H, Kim HM, et al. Patterns of surgical care and health disparities of treating pediatric finger amputation injuries in the United States. J Am Coll Surg. 2011;213(4):475-485. doi: 10.1016/j.jamcollsurg.2011.07.017 [DOI] [PubMed] [Google Scholar]
- 32. Trautwein LC, Smith DG, Rivara FP. Pediatric amputation injuries: etiology, cost, and outcome. J Trauma. 1996;41(5):831-338. [DOI] [PubMed] [Google Scholar]
- 33. US Census Bureau PIO. Census 2000 data for the United States. https://www.census.gov/census2000/states/us.html.
- 34. US Inflation Rate. US Inflation. 2013. http://usinflation.org/us-inflation-rate/.
- 35. Van Beek AL, Wavak PW, Zook EG. Microvascular surgery in young children. Plast Reconstr Surg. 1979;63(4):457-462. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Material, DS_10.1177_1558944718777865 for Trends in Pediatric Traumatic Upper Extremity Amputations by Venus Vakhshori, Gabriel J. Bouz, Cory K. Mayfield, Ram K. Alluri, Milan Stevanovic and Alidad Ghiassi in HAND