

ABSTRACT
The viral infection during influenza includes several complications like primary pneumonitis, ARDS, bacterial pneumonia, otitis media along with severe increase in the ongoing chronic conditions. Fulminant myocarditis as a primary manifestation of H1N1 is rare. We are reporting four cases that developed fulminant viral myocarditis caused by the H1N1 strain of influenza. These four cases were reported between October 2018 and November 2018, during the post-flood time in Kerala.
How to cite this article
Thomas TP, Kumar S, Anand A, Kiran R, Sabu V, Gaffoor A. A Rare Presentation of Fulminant Viral Myocarditis Associated with H1N1: A Series of Four Cases. IJCCM 2019;23(11): 538–541.
Keywords: Fulminant myocarditis, H1N1 myocarditis, Viral myocarditis
INTRODUCTION
The viral infection during influenza includes several complications like primary viral pneumonia, ARDS, bacterial pneumonia, otitis media along with severe increase in the ongoing chronic conditions. Illness tends to be most severe in the elderly, infants and young children, as well as immunocompromised hosts.1 Fulminant myocarditis is an unusual complication and is generally detected along with circulatory collapse or at autopsy in patients with influenza-associated fatal outcomes. In literature, few case reports and case series of fulminant myocarditis have been reported.2 There are rare cases of influenza-induced cardiogenic shock, and large number of cases were caused by A/H1N1 flu-associated fulminant myocarditis during the 2009 pandemic. A total of 184 cases of patients suffering from influenza myocarditis are reported in the literature (2009–2017/2018), including 65 cases since the 2009 pandemic.3 We report four cases that developed fulminant viral myocarditis triggered by the H1N1 strain of influenza.
CASE DESCRIPTION
Case 1
A 23-year-old female who presented with complaints of fever, cough, and fatigue for 2–3 days was treated in a primary care center and was subsequently referred to our institution in view of worsening of fever, breathlessness, and cough. She had no known comorbidities. On arrival, she was febrile with tachycardia, hypotensive and tachypneic. The initial echocardiography revealed hypercontractile left ventricle (LV) with good LV systolic function without evidence of pericardial effusion. Initial trop I was negative. Her hypotension worsened and she was started on ionotropes—noradrenaline and adrenaline. She was intubated in view of her worsening general condition. Repeat echocardiography was done within 4 hours of admission that showed global LV dysfunction and pericardial effusion. ECG was suggestive of myopericarditis (Fig. 1). Chest X-ray findings were suggestive of pulmonary congestion. She was treated with negative pressure isolation, oseltamivir 150 mg twice daily dose, and other supportive measures. Piperacillin-tazobactum and azithromycin were started empirically suspecting the possibility of bacterial pneumonia. Her general condition further deteriorated and she developed refractory hypotension. Despite intensive therapy, she developed cardiac arrest within 24 hours of admission from which she was not revivable. Nasopharyngeal and throat swabs for H1N1 RT-PCR were positive.
Fig. 1.

ECG of Case 1
Case 2
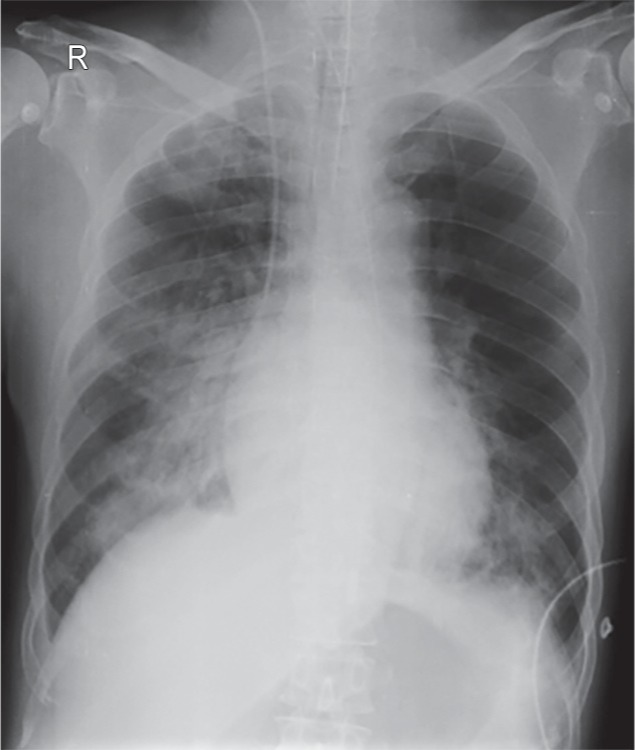
A 27-year-old female presented with complaints of fever, abdominal discomfort of 1-day duration, and one episode of loose stools that was treated in a primary care center and was referred to our institution in view of worsening hypotension and tachypnea. She had no known comorbidities. On arrival, she was febrile with tachycardia, hypotensive and tachypneic. Bedside echocardiography revealed severe LV dysfunction. Initial trop I was positive. ECG was suggestive of myocarditis (Fig. 2). Chest X-ray findings were suggestive of pulmonary congestion (Fig. 3). She was intubated in view of her worsening general condition. She was treated with oseltamivir 150 mg twice daily dose, negative pressure isolation and other supportive measures. Piperacillin-tazobactum and azithromycin were started empirically suspecting the possibility of bacterial pneumonia. She further developed hypotension for which noradrenaline and adrenaline were started. Despite intensive therapy, she developed cardiac arrest within 24 hours of admission from which she was not revivable. Nasopharyngeal and throat swabs for H1N1 RT-PCR were positive.
Fig. 2.

ECG of Case 2
Fig. 3.
Chest X-ray of Case 2
Case 3
A 61-year-old male with complaints of fever of 1-day duration followed by dyspnea was treated in a primary care center and was referred to our institution in view of worsening desaturation and tachypnea. He had a history of coronary artery disease, post-percutaneous transluminal coronary angioplasty (PTCA), diabetes mellitus, and hypertension. On arrival, he was febrile and had accelerated hypertension and pulmonary edema. Bedside echocardiography revealed severe LV dysfunction. Initial trop I was positive. He was treated as a case of acute left ventricular failure (LVF) precipitated by sepsis/myocarditis. He was treated with meropenem, levofloxacin, oseltamivir 150 mg twice daily dose, and other supportive measures. His general condition further deteriorated and he developed multiple organ dysfunction syndrome (MODS). Despite the intensive therapy, he developed cardiac arrest. Nasopharyngeal and throat swabs for H1N1 RT-PCR were positive.
Case 4
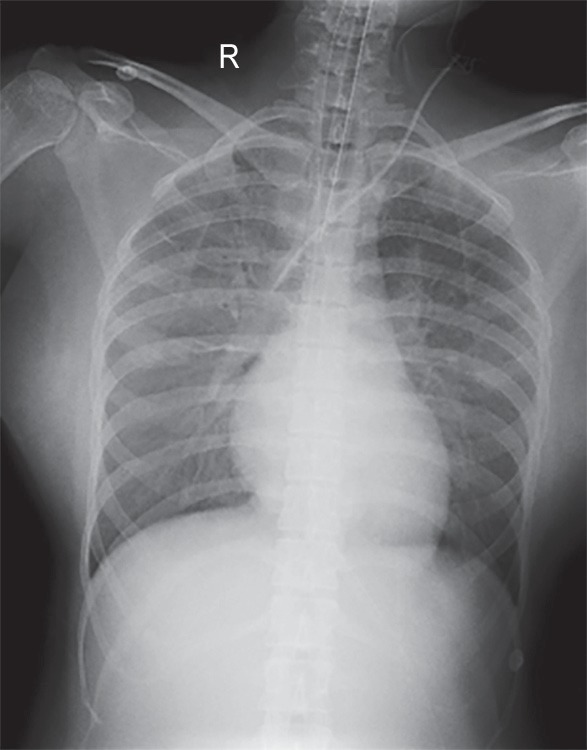
A 24-year-old female, with no comorbidities, presented with complaints of fever, cough, and fatigue for 2–3 days, was treated in a primary care center and was subsequently referred to our institution in view of worsening of fever, breathlessness, and cough. On arrival, she was febrile with a heart rate of 146/minute, hypotensive and tachypneic (with the respiratory rate of 36/minute) (Fig. 4). Bedside echocardiography revealed severe LV dysfunction. Initial trop I was positive. Her hypotension worsened and she was started on dobutamine, noradrenaline, and adrenaline. She was intubated in view of her worsening general condition. Considering the possibility of sepsis with hypotension, she was started on meropenem, azithromycin, and oseltamivir 150 mg twice daily. ECG was suggestive of myocardial injury, most likely due to myopericarditis. Despite intensive therapy, she developed cardiac arrest within 24 hours of admission from which she was not revivable. Nasopharyngeal and throat swabs for H1N1 RT-PCR were positive.
Fig. 4.
Chest X-ray of Case 3
DISCUSSION
The viral infection during influenza includes several complications like primary viral pneumonia, ARDS, bacterial pneumonia, otitis media along with severe increase in the ongoing chronic conditions. Illness tends to be most severe in the elderly, infants and young children, as well as immunocompromised hosts. The characteristics of influenza A (H1N1) include high activity during summer season in north, high mortality rates among healthy young adults, and high incidence of viral pneumonia.1 Acute myocarditis is a well-known, though rare, manifestation of numerous viral infections having wide range of symptoms and clinical features. Fulminant myocarditis is an unusual complication and is generally detected along with circulatory collapse or at autopsy in patients with influenza-associated fatal outcome. In literature, few case reports and case series of fulminant myocarditis have been reported.2 The occurrence of myocardial association in influenza infection ranges from 0% to 12%.4 Fulminant myocarditis may present with fatal arrhythmias, atrioventricular block, and/or varying degrees of cardiogenic shock.5 Influenza-induced cardiac shock occurs very rarely and most of the cases were initiated by A/H1N1 flu-associated fulminant myocarditis during the 2009 pandemic. The number of cases in which patients suffer from influenza myocarditis are 184 (2009–2017/2018), including 65 cases since the 2009 pandemic: 144 related to A/H1N1 virus, 5 to A/H3N2 virus, 25 to A virus (serotype not reported), and 10 to B virus. Fifty-one percent of the cases were reported in women followed by their mean ± SD age of 33 ± 17 years. Cardiogenic shock, new-onset heart failure, chest pain-inducing acute coronary syndrome, cardiac tamponade, electric storm, atrioventricular block, and sudden death are some of the main clinical presentations.3 Pathophysiology of influenza virus-associated myocarditis is unclear and might include a direct impact of influenza viral infection, proinflammatory cytokines, and endothelial cell dysfunction.6 Supportive care remains the mainstay of the treatment. Mild cases rarely require vasopressor support, whereas fulminant myocarditis may necessitate supportive actions like intra-aortic balloon pump and extracorporeal membrane oxygenation therapy to attain hemodynamic stability.7 There have been reports of the use of high-dose intravenous immunoglobulin and immunosuppressive therapy as treatment in acute viral myocarditis in pediatric population. But there is no consensus in the literature.8 In the first two and the fourth cases, fever was followed by an acute onset of cardiac dysfunction, abnormal cardiac biomarkers, and ECG changes suggesting diffuse myocardial injury in healthy young adult, which is suggestive of myocarditis. In the third case, the patient developed sepsis-related myocardial injury due to H1N1. The prodromal symptoms coupled with positive laboratory findings highly suggest the H1N1 influenza as the primary cause for both the cases. Our documented four cases of H1N1 developed myocarditis within a 60-day period, compared with our previous experience that raised the possibility of more atypical presentation. A high index of suspicion of myocarditis is warranted in such scenarios. Personal protection, proper hygiene, and adequate preventive care measures (like personal protection equipment, chemoprophylaxis, proper isolation, and vaccination) should be taken by the healthcare providers.
CONCLUSION
In our four cases of fulminant myocarditis, the prodromal symptoms were minimal and the duration of fever was very short. The presentation of four such cases in a span of 60 days is also a matter of concern. A high index of suspicion of myocarditis is warranted in such scenarios. A proper surveillance system is also necessary. Personal protection and proper hygiene and adequate preventive care measures (like personal protection equipment, chemoprophylaxis, proper isolation, and vaccination) should be taken by healthcare providers. Early referral of such cases to the tertiary center should be done.
Footnotes
Source of support: Nil
Conflict of interest: None
REFERENCES
- 1.Seasonal influenza and influenza A (H1N1), http://www.who.int/ith/diseases/si_iAh1n1/en/ http://www.who.int/ith/diseases/si_iAh1n1/en/
- 2.Bratincsák A, El-Said HG, Bradley JS, Shayan K, Grossfeld PD, Cannavino CR. Fulminant myocarditis associated with pandemic H1N1 influenza A virus in children. J Am Coll Cardiol. 2010;55(9):928–929. doi: 10.1016/j.jacc.2010.01.004. DOI: [DOI] [PubMed] [Google Scholar]
- 3.Hékimian G, Jovanovic T, Bréchot N, Lebreton G, Leprince P, Trouillet JL, et al. When the heart gets the flu: fulminant influenza B myocarditis: a case-series report and review of the literature. J Crit Care. 2018;47:61–64. doi: 10.1016/j.jcrc.2018.06.001. DOI: [DOI] [PubMed] [Google Scholar]
- 4.Mamas MA, Fraser D, Neyses L. Cardiovascular manifestations associated with influenza virus infection. Int J Cardiol. 2008;130(3):304–309. doi: 10.1016/j.ijcard.2008.04.044. DOI: [DOI] [PubMed] [Google Scholar]
- 5.Cooper LT., Jr Myocarditis. N Engl J Med. 2009;360(15):1526–1538. doi: 10.1056/NEJMra0800028. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ukimura A, Satomi H, Ooi Y, Kanzaki Y. Myocarditis associated with influenza a H1N1pdm2009. Influenza Res Treat. 2012;2012:351979. doi: 10.1155/2012/351979. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kato S, Morimoto S, Hiramitsu S, Nomura M, Ito T, Hishida H. Use of percutaneous cardiopulmonary support of patients with fulminant myocarditis and cardiogenic shock for improving prognosis. Am J Cardiol. 1999;83(4):623–625. doi: 10.1016/s0002-9149(98)00931-x. DOI: [DOI] [PubMed] [Google Scholar]
- 8.Lobo ML, Taguchi Â, Gaspar HA, Ferranti JF, de Carvalho WB, Delgado AF. Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review. Rev Bras Ter Intensiva. 2014;26(3):321–326. doi: 10.5935/0103-507X.20140046. [DOI] [PMC free article] [PubMed] [Google Scholar]