

Abstract
BACKGROUND:
Knee and hip joints endoprosthetics are the main surgical method of arthrosis treatment. The epidemiological incidence rate of the disease is growing steadily every year, affecting younger and younger people. Despite the proven tactics of joint endoprosthetics, an important issue is quality planning of surgery.
AIM:
The aim of this research is to develop a device and a method that would contribute to solving the existing challenges of pre-surgery planning of hip endoprosthetics in patients with related pathologies, which have caused compensatory deformation, and making long vertebrarium-pelvis-lower limbs scout images with the patient lying on his back with an axial load in a computer tomography.
METHODS:
Analog X-ray photographs of the pelvis made on film, digital DICOM images, and special planning programs are used for planning. However, according to numerous studies, the disease of the hip joint is not an independently isolated pathology. In most cases, this pathology is accompanied by changes in the lumbar spine. Often, patients prepared for endoprosthetics have a congenital deformity of tarsus or hip segment, which, during the knee, joint endoprosthetics surgery causes difficulties with the installation of an intramedullary guide.
RESULTS:
The results after total knee arthroplasty according to the method modified at the Department showed a reduction of the WOMAC index slightly more than twice down to 37.26 ± 7.92. The number of revision surgeries after endoprosthetics decreased from 5 (5.7%) to 1 (1.1%) for the hip joint, and from 7 (4.3%) to 2 (1.3%) for the knee joint, respectively.
CONCLUSION:
To form a proper guide entry point, it is necessary to assess the segment at the stage of surgery planning and examination of patients, which can be done using the proposed method. To remove the complications during the pre-surgery planning of hip joint endoprosthetics in patients with related pathologies, a device and methods have been developed for obtaining long topograms of the vertebrarium-pelvis-lower limbs complex with the patient lying on his back with the axial load in computer tomography.
Keywords: Arthroplasty, Hip joint Limb shortening, Computer tomography, Load, Hip-spine syndrome, Contracture, Axial load, Functional study
Introduction
Depending on the duration of the disease, compensatory deformations in every patient are expressed to varying degrees due to limb shortening on the side of the affected joint [1]. All these changes together affect the vertebrarium-pelvis-lower limbs anatomic complex [2], [3], [4]. Especially in case of marked changes after joint endoprosthetics with the observation of all rules of components installation, patients are troubled by pain both in the early and the late post-surgery periods, which is not associated with the prosthesis [2], [5], [6], [7]. Many papers have been published that are focused on studying this problem, and various authors propose methods of components installation concerning the characteristics of each patient [8], [9], [10], [11], [12]. It should be noted that there are various methods of visualisation and assessing the adjacent hip joint structures [13], [14] (Figure 1).
Figure 1.
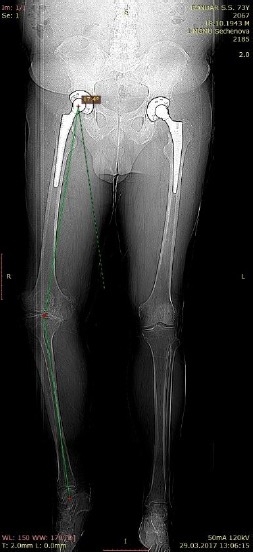
Long digital X-ray image
An example is X-ray imaging of the entire lower extremity and the pelvis. However, this examination is often performed in the lying position on the back with the use of several films (Figure 2) [15], and, in case of analog X-ray photography, without the possibility of assessing the vertebrarium-pelvis-lower limbs anatomical complex with the baseload [16], [17], [18] (Figure 3).
Figure 2.

A patient with posttraumatic arthrosis of the knee joint. Planning by the method of bonding films
Figure 3.

The use of several films for a rough estimation of the vertebrarium-pelvis-lower limbs anatomical complex
The aim of this research is to develop a device and a method that would contribute to solving the existing challenges of pre-surgery planning of hip endoprosthetics in patients with related pathologies, which have caused compensatory deformation, and making long vertebrarium-pelvis-lower limbs scout images with the patient lying on his back with an axial load in a computer tomography.
Material and Methods
To test the method, the authors conducted 247 studies along with the routine planning procedures to assess the efficiency of the method. The study was performed both in the standard conditions and with the use of the device developed at the Department of Traumatology, Orthopedics and Disaster Surgery of the Sechenov University (Figure 4).
Figure 4.

The use of the device developed at the Department of Traumatology, Orthopedics and Disaster Surgery
The device is a vest that is put on the patient. The vest is connected to a rigid platform under the patient’s feet with rods. The rods are fitted with force meters connected to the monitor that displays the pressure on the platform.
Thus, the device allows creating an axial load on the vertebrarium, hip joints, knee joints, ankle joints and feet with the patient lying on his back. The monitor continuously records the force applied to force meters and displays the axial load in kilograms.
A CT scanner Toshiba Aquilion ONE 640 was used for the study. The analysis was performed by standard X-ray imaging of the pelvis and knee joints followed by CT scanning of the same patients with the use of the method developed at the Department of Traumatology, Orthopedics and Disaster Surgery of the Sechenov University.
The results of the research with the use of the new method were assessed with the help of building axes and angles before (Figure 5) and after surgery (Figure 6).
Figure 5.
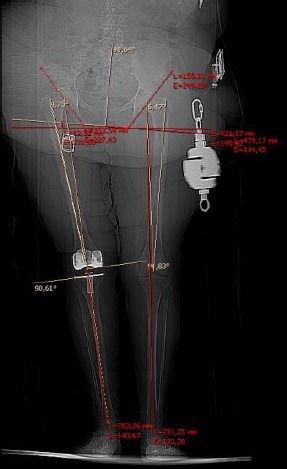
Planning endoprosthetics of the knee joint
Figure 6.
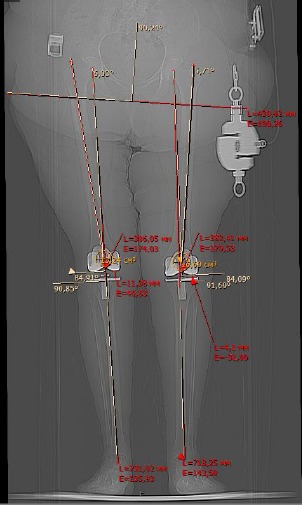
After knee joint endoprosthetics
The data were statistically processed with the use of Statistica 8.0 software suite. The quantitative variables were described using standard methods of variation statistics, for which the arithmetic mean was (M), and the standard deviation was (δ). The mean values were presented as M + δ. Qualitative variables were characterised as absolute and relative frequency ratios. The differences were considered veracious with p < 0.05. For assessing the results, the following methods of statistical analysis were used: Student’s t-test; nonparametric tests for variable samples that were incompatible with the law of normal distribution (Mann–Whitney U test, Wilcoxon test).
All studies were approved by the appropriate Ethics Committee and were therefore performed by the ethical standards laid down in the 1964 Helsinki Declaration. All persons gave their informed consent before being involved in the research.
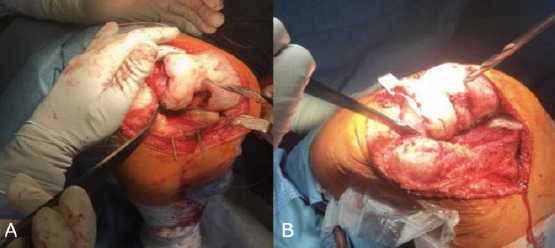
To determine the tactics of knee joint treatment, the authors assessed the anatomical axis of the limb, the mechanical axis of the limb, the Q-angle, and evaluated positioning of the components in the post-surgery period. During pre-surgery planning, the method made it possible to identify predominant lesion of the medial sections of the knee joint under axial load, which changed the tactics of the planned surgery – making unicondylar endoprosthetics instead of total knee arthroplasty. In planning the hip joint endoprosthetics with concomitant pathology of the vertebrarium, the authors managed to estimate the degree of pelvic bones displacement, the degree of scoliotic vertebral deformity, lower limb shortening (Figure 7A and 7B). This allowed more precise pre-surgery planning and monitoring the positioning of endoprosthesis components after surgery.
Figure 7.
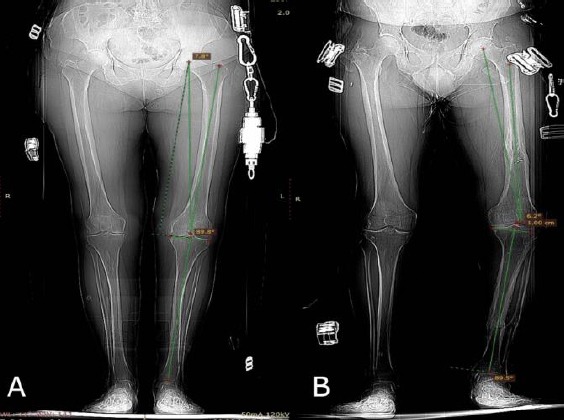
A) Pre-surgery planning with the normal anatomical axis of the lower limb; B) Pre-surgery planning with varus deformity of the lower limb
In the framework of pre-surgery planning before total hip arthroplasty, the authors evaluated the anatomical and mechanical axes of the limbs, and the degree of pelvic bones displacement during a CT examination with the help of devices that simulated the axial load, and without it. An important role for proper pre-surgery planning and for determining further tactics of treatment, in the opinion of the authors, was also played by studying the lumbar spine for identifying the vertebral column deformities, pathologies of the sacroiliac joint, and the degenerative-dystrophic changes in the spinal motion segment.
To monitor the efficiency of the method, CT scanning was performed by standard methods with pre-surgery planning, after which an examination with the use of the new method was performed with subsequent planning for further analysis and identifying the differences in the tactics of the surgical treatment.
The study was performed with 247 patients, of which 87 (35.3%) had hip joint endoprosthetics, and 160 (64.7%) had knee joint endoprosthetics. From the second group, 37 (23.1% of patients with knee endoprosthetics) had total endoprostheses installed in both knee joints.
Out of 247 patients, in 54 (21.9%) post-traumatic arthrosis was diagnosed, 163 patients (66%) had degenerative arthrosis, and the remaining 30 patients (12.1%) had dysplastic arthrosis.
As a result, information was obtained about changes in the plan of surgical intervention with fairly pronounced differences during the pre-surgery planning in the position of the components of the endoprosthesis after using the standard and the modified methods of examination, respectively. In planning hip joint endoprosthetics, surgeons most often changed the angles of acetabular components; the second frequent pattern was the difference in selecting the length of the prosthesis head. In planning knee joint endoprosthetics, surgeons most often changed the positioning of the tibial component and calculated the entry point for the intramedullary guide (Figure 8A and 8B).
Figure 8.
A) Determination of the entry point for the femoral intramedullary guide with the normal axis; B) Determination of the entry point of the femoral intramedullary guide with varus deformity of the lower limb
Results
For comparison of long-term results of prosthetics with the use of the new method, the authors chose for reference 247 case reports of patients with similar models of pathology, which had undergone endoprosthetics with the use of the standard planning methods. The data of assessment scales, the amount of movement and survival of the prosthesis were obtained (Table 1; Figure 9). The WOMAC (Western Ontario McMaster Universities OA Index) estimation scale, which allows assessing the intensity of the pain syndrome in the osteoarthritis of the hip or knee joints in course of five activities in the standing position – walking, climbing stairs, at rest, and at night [15], [19], [20], was mainly used. The clinical characteristic of the patients was the following: most patients were female: 156 patients (63.2%), the average age was 63.16 ± 12.41. The duration of the disease ranged from 1 to 12 years; the average duration of aggravation was 6.0 ± 1.5 weeks. In most patients, radiographic osteoarthritis stage III was found (by Kellgren – Lawrence) – in 180 patients (72.9%), stage II – in 25 patients (10.1%), and stage IV – in the remaining 42 patients (17 %). In most patients (92%), a limited range of movement was noted, mostly in the degree of affected knee joints bending.
Table 1.
The data of assessment scales, the amount of movement and survival of the prosthesis
| WOMAC | The number of revision interventions | |||
|---|---|---|---|---|
| Standard method | Modified method | Standard method | Modified method | |
| Total hip arthroplasty (THA) | 32.81 ± 9.63 | 31.32 ± 8.13 | 5 | 1 |
| Total knee arthroplasty (TKA) | 84.14 ± 8.74 | 37.26 ± 7.92 | 7 | 2 |
Figure 9.
Adjustment of the acetabular component inclination in surgical treatment planning (before and after making scout images with axial load)
Pain syndrome intensity during movement ranged from 0 to 93 (82.43 ± 4.76) by the visual analogue scale. The functional state of the joints by the WOMAC index before surgery was 68.26 ± 7.51 mm. After a surgical intervention with the use of the standard method for the hip joint, the WOMAC index was 32.81 ± 9.63, and after total hip arthroplasty according to the modified method with pre-surgery planning with the use of the developed device, the index reached 31.32 ± 8.13. For the knee joint, the differences between the two groups were much more significant. WOMAC for the standard methodology was 84.14 ± 8.74. The results after total knee arthroplasty according to the method modified at the Department showed a reduction of the WOMAC index slightly more than twice down to 37.26 ± 7.92. The number of revision surgeries after endoprosthetics decreased from 5 (5.7%) to 1 (1.1%) for the hip joint, and from 7 (4.3%) to 2 (1.3%) for the knee joint, respectively.
Discussion
In many countries, the importance of pre-surgery planning is acknowledged, and they try improving it to achieve the most optimal result. In Japan, during pre-surgery planning of hip joint endoprosthetics, they are guided by the pelvis inclination angle [21], [22]. German surgeons during pre-surgery planning use a 3D modelling application, magnetic resonance imaging, and fluoroscopy without axial load [23], [24]. In the United States, the importance of using digital templates in surgical practice is noted [25], [26]. In the studies in German authors, digital calibrated X-ray photographs are made, while in North America, they use individual tools prepared before the surgery [5], [27]. The work of specialists from Delft, the Netherlands is quite interesting; they note the correlation between the patient’s shoe size and the size of implants used for primary knee joint endoprosthetics [28], [29].
The obtained results of our study show attractiveness of the pre-surgery planning method developed at the Department of Traumatology, Orthopedics and Disaster Surgery of the First MSMU n.a. I. M. Sechenov (Sechenov University). Modern literature describes many various techniques of improving pre-surgery planning of endoprosthetics of large joints of the lower extremities [11], [12].
The authors’ method involves the use of a standard horizontal tomographic scanner, which makes it unique in terms of the scope of application, unlike the methods that involve the presence of a vertical tomographic scanner. The examination in the tomographic scanner takes a short time, usually less than one minute; there is a possibility of making additional slices to facilitate surgical planning. In medical literature, the use of the above device in combination with a horizontal computer tomograph, has not been described. In Russia, this method of pre-surgery planning for the patients with combined pathology of the hip and knee joints and lumbar spine has been granted a patent for invention No. 2651056 dated April 18, 2018 [30]. As a result, this method has a distinct advantage in minimising the duration of examination and radiation exposure. With that, the informative value of the data obtained exceeds the standard methods of patient examination.
In conclusion, the use of the new method of pre-surgery planning for knee and hip joint endoprosthetics with concomitant spinal pathology allows to reduce the duration and improve the quality of pre-surgery planning to avoid repeated CT studies with low informative value of scout images, to reduce the time of surgery on the average by 17 minutes, and to improve treatment results and survival rate of the endoprostheses. For the examination, one can use a tomographic scanner with any number of spirals from various manufacturers. There is no need to use special planning software. The use of this method will significantly improve the quality of arthroplasty and reduce the time and costs for preparing a surgery.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Phan D, Bederman SS, Schwarzkopf R. The influence of sagittal spinal deformity on anteversion of the acetabular component in total hip arthroplasty. Bone Joint J. 2015;97-B(8):1017–1023. doi: 10.1302/0301-620X.97B8.35700. https://doi.org/10.1302/0301-620X.97B8.35700 PMid:26224815. [DOI] [PubMed] [Google Scholar]
- 2.Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004;419:280–284. doi: 10.1097/00003086-200402000-00044. https://doi.org/10.1097/00003086-200402000-00044 PMid:15021166. [DOI] [PubMed] [Google Scholar]
- 3.Rajnish RK, Kumar P, Aggarwal S. Letter to the Editor concerning “The effect of total hip arthroplasty on sagittal spinal-pelvic-leg alignment and low back pain in patients with severe hiposteoarthritis“ by W. Weng et al. Eur Spine J. (2016); 25(11):3608-3614. Eur Spine J. 2017;26(8):2211. doi: 10.1007/s00586-017-5137-0. https://doi.org/10.1007/s00586-017-5137-0 PMid:28516229. [DOI] [PubMed] [Google Scholar]
- 4.Tang WM, Chiu KY. Primary total hip arthroplasty in patients with ankylosing spondylitis. J Arthroplasty. 2000;15(1):52–58. doi: 10.1016/s0883-5403(00)91155-0. https://doi.org/10.1016/S0883-5403(00)91155-0. [DOI] [PubMed] [Google Scholar]
- 5.Weng W, Wu H, Wu M, Zhu Y, Qiu Y, Wang W. The effect of total hip arthroplasty on sagittal spinal-pelvic-leg alignment and low back pain in patients with severe hip osteoarthritis. Eur Spine J. 2016;25(11):3608–3614. doi: 10.1007/s00586-016-4444-1. https://doi.org/10.1007/s00586-016-4444-1 PMid:26883265. [DOI] [PubMed] [Google Scholar]
- 6.Wong TK, Lee RY. Effects of low back pain on the relationship between the movements of the lumbar spine and hip. Hum Mov Sci. 2004;23(1):21–34. doi: 10.1016/j.humov.2004.03.004. https://doi.org/10.1016/j.humov.2004.03.004 PMid:15201039. [DOI] [PubMed] [Google Scholar]
- 7.Denisov AO. Pain syndrome after hip joint endoprosthetics: abstract of diss. Saint Peterburg. 2010 [Google Scholar]
- 8.Berge C. Heterochronic processes in human evolution: an ontogenetic analysis of the hominid pelvis. Am J Phys Anthropol. 1998;105(4):441–459. doi: 10.1002/(SICI)1096-8644(199804)105:4<441::AID-AJPA4>3.0.CO;2-R. https://doi.org/10.1002/(SICI)1096-8644(199804)105:4<441::AID-AJPA4>3.0.CO;2-R. [DOI] [PubMed] [Google Scholar]
- 9.Legaye J, Duval-Beaupere G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for threedimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7(2):99–103. doi: 10.1007/s005860050038. https://doi.org/10.1007/s005860050038 PMid:9629932 PMCid:PMC3611230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Oonishi H, Ohashi H, Kawahara I. Total Hip Arthroplasty around the Inception of the Interface Bioactive Bone Cement Technique. Clin Orthop Surg. 2016;8(3):237–242. doi: 10.4055/cios.2016.8.3.237. https://doi.org/10.4055/cios.2016.8.3.237 PMid:27583104 PMCid:PMC4987305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Raphael IJ, Rasouli MR, Kepler CK, Restrepo S, Albert TJ, Radcliff KE. Pelvic incidence in patients with hip osteoarthritis. Arch Bone Jt Surg. 2016;4(2):132–136. [PMC free article] [PubMed] [Google Scholar]
- 12.Stagnara P, De Mauroy JC, Dran G, Gonon GP, Costanzo G, Dimnet J. Reciprocal angulation of vertebral bodies in a sagittal plane: approach to references for the evaluation of kyphosis and lordosis. Spine. 1982;7(4):335–342. doi: 10.1097/00007632-198207000-00003. https://doi.org/10.1097/00007632-198207000-00003 PMid:7135066. [DOI] [PubMed] [Google Scholar]
- 13.Merchant AC, Mercer RL, Jacobsen RH, Cool CR. Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am. 1974;56:1391–1396. https://doi.org/10.2106/00004623-197456070-00007 PMid:4433362. [PubMed] [Google Scholar]
- 14.Michelitsch C, Nguyen-Kim TD, Jentzsch T, Simmen HP, Werner CM. Computed tomography-based three-dimensional visualization of bone corridors and trajectories for screws in open reduction and internal fixation of symphysis diastasis: a retrospective radiological study. Arch Orthop Trauma Surg. 2016;136(12):1673–1681. doi: 10.1007/s00402-016-2568-8. https://doi.org/10.1007/s00402-016-2568-8 PMid:27628459. [DOI] [PubMed] [Google Scholar]
- 15.Hawker GA, Davis AM. Chapter 176-Assessment of the patient with osteoarthritis and measurement of outcomes. In: Hochberg, Silman, Smolen, Weinblatt, Weisman, editors. Rheumatology. 5th edition. Roseville: Mosby Elsevier; 2010. [Google Scholar]
- 16.Lazennec JY, Rousseau MA, Rangel A, Gorin M, Belicourt C, Brusson A. Pelvis and total hip arthroplasty acetabular component orientations in sitting and standing positions: measurements reproductibility with EOS imaging system versus conventional radiographies. Orthop Traumatol Surg Res. 2011;97(4):373–380. doi: 10.1016/j.otsr.2011.02.006. https://doi.org/10.1016/j.otsr.2011.02.006 PMid:21570378. [DOI] [PubMed] [Google Scholar]
- 17.Le Huec J, Aunoble S, Philippe L, Nicolas P. Pelvic parameters: origin and significance. Eur Spine J. 2011;20(Suppl 5):564–571. doi: 10.1007/s00586-011-1940-1. https://doi.org/10.1007/s00586-011-1940-1 PMid:21830079 PMCid:PMC3175921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wan Z, Malik A, Jaramaz B, Chao L, Dorr LD. Imaging and navigation measurement of acetabular component position in THA. Clin Orthop Relat Res. 2009;467(1):32–42. doi: 10.1007/s11999-008-0597-5. https://doi.org/10.1007/s11999-008-0597-5 PMid:18979147 PMCid:PMC2600979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vaz G, Roussouly P, Berthonnaud E, Dimnet J. Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J. 2002;11(1):80–87. doi: 10.1007/s005860000224. https://doi.org/10.1007/s005860000224 PMid:11931071 PMCid:PMC3610486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yoshimura N, Muraki S, Oka H, Mabuchi A, En-Yo Y, Yoshida M. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. J Bone Miner Metab. 2009;27(5):620–628. doi: 10.1007/s00774-009-0080-8. https://doi.org/10.1007/s00774-009-0080-8 PMid:19568689. [DOI] [PubMed] [Google Scholar]
- 21.Hube R, Birke A, Hein W, Klima S. CT-based and fluoroscopy-based navigation for cup implantation in total hip arthroplasty (THA) Surg Technol Int. 2003;11:275–280. [PubMed] [Google Scholar]
- 22.Inaba Y. Pre-surgery planning for implant placement with consideration of pelvic tilt in total hip arthroplasty: postoperative efficacy evaluation. BMC Musculoskelet Disord. 2016;17:280. doi: 10.1186/s12891-016-1120-x. https://doi.org/10.1186/s12891-016-1120-x PMid:27412447 PMCid:PMC4944317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bugbee WD, Mizu-Uchi H, Patil S, D'Lima D. Accuracy of implant placement utilizing customized patient instrumentation in total knee arthroplasty. Adv Orthop 2013. 2013:891210. doi: 10.1155/2013/891210. https://doi.org/10.1155/2013/891210 PMid:24151556 PMCid:PMC3787656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chepelev L, Wake N, Ryan J, Althobaity W, Gupta A, Arribas E, Santiago L, Ballard DH, Wang KC, Weadock W, Ionita CN, Mitsouras D, Morris J, Matsumoto J, Christensen A, Liacouras P, Rybicki FJ, Sheikh A. Radiological Society of North America (RSNA) 3D printing Special Interest Group (SIG): guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print Med. 2018;4(1):11. doi: 10.1186/s41205-018-0030-y. https://doi.org/10.1186/s41205-018-0030-y PMid:30649688 PMCid:PMC6251945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.DeCrane SK, Stark LD, Johnston B, Lim E, Hicks MK, Ding Q. Pain, opioids, and confusion after arthroplasty in older adults. Orthop Nurs. 2014;33(4):226–232. doi: 10.1097/NOR.0000000000000066. https://doi.org/10.1097/NOR.0000000000000066 PMid:25058729. [DOI] [PubMed] [Google Scholar]
- 26.Pullen WM, Whiddon DR. Accuracy and reliability of digital templating in primary total hip arthroplasty. J Surg Orthop Adv. 2013;22:148–151. doi: 10.3113/jsoa.2013.0148. https://doi.org/10.3113/JSOA.2013.0148. [DOI] [PubMed] [Google Scholar]
- 27.Gonzarez Della Valle A, Slullitel G, Piccaluga F, Salvati EA. The precision and usefulness of pre-surgery planning for cemented and hybrid primary total hip arthroplasty. Journal of Arthroplasty. 2005;20(1):51–58. doi: 10.1016/j.arth.2004.04.016. https://doi.org/10.1016/j.arth.2004.04.016 PMid:15660060. [DOI] [PubMed] [Google Scholar]
- 28.Van Egmond JC, Verburg H, Hesseling B, Mathijssen NMC. The Correlation of Shoe Size and Component Size of Primary Total Knee Arthroplasty. Journal of Knee Surgery. 2019 doi: 10.1055/s-0039-1677841. [DOI] [PubMed] [Google Scholar]
- 29.Vanin N, Kenaway M, Panzica M, Jagodzinski M, Meller R, Krettek C, Hankemeier S. Accuracy of digital pre-surgery planning for total knee arthroplasty. Technol Health Care. 2010;18:335–340. doi: 10.3233/THC-2010-0598. https://doi.org/10.3233/THC-2010-0598 PMid:21209482. [DOI] [PubMed] [Google Scholar]
- 30.RF patent No. RU 2651056, 18.04.2018. The Method of Presurgery Planning in patients with combined pathology of the hip and knee joint and lumbar spine; applicant and patentee - FSAEI First Moscow State Medical University named after I. M. Sechenov of the Ministry of Health (Sechenov University) - application No. 2017114403 [Google Scholar]