

Abstract
Background
Primary delusional infestation (DI) is a primary psychiatric disorder characterised by delusions and abnormal tactile sensations. The pathophysiology is undecided and treatment includes both pharmacological and non‐pharmacological options. There is currently no Cochrane Review of the treatments used. Primary DI is a diagnosis often encountered by both dermatologists and psychiatrists, with a large associated disease burden.
Objectives
To evaluate the effectiveness of different treatments in primary delusional infestation (DI).
Search methods
On 24 December 2014 and 19 March 2019, we searched the Cochrane Schizophrenia Group’s Study‐Based Register of Trials including registries of clinical trials.
Selection criteria
Randomised controlled trials involving the treatment of adults with primary DI.
Data collection and analysis
Two review authors independently screened and assessed studies for inclusion using pre‐specified inclusion criteria.
Main results
We did not identify any studies for inclusion.
Authors' conclusions
Currently there is no evidence from RCTs available to compare treatment of primary DI with placebo. We cannot, therefore, make any conclusions regarding the effects of treatments (pharmacological or non‐pharmacological) for primary DI. This lack of evidence for treatment of primary DI has implications for research and practice. Robust randomised trials are indicated.
Plain language summary
Treatments for primary delusional infestation
People with delusional infestation (DI) believe themselves to be infested with an unknown pathogen (may be described as worms, mites or insects), manifesting as itch or crawling sensations. Through repeated self‐examination, cleansing routines, or attempts to capture the agent, patients will cause skin lesions, perpetuating the belief of ongoing infestation. People with DI will seek the advice of general practitioners or specialist physicians (e.g. dermatologists and microbiologists) but tend to avoid seeking psychiatric advice. DI has two main forms: primary (a disorder characterised by delusions and abnormal tactile sensations); and secondary (symptoms caused by another defined organic or pre‐existing psychiatric disorder, or substance abuse). This review is concerned with primary DI. There is no definite cause of primary DI and no current licensed treatment options. Treatments that have been reported in the literature include pharmacological (e.g. antipsychotic medication) and non‐pharmacological (e.g. talking therapy) options. The aim of this review was to evaluate the effectiveness of treatments for primary DI compared with placebo. In March 2019 we ran a search of Cochrane Schizophrenia's register of trials for relevant studies, but found none. The review authors could not, therefore, comment about the effects of current treatments for primary DI. The authors call for more well‐conducted randomised trials in this area.
Summary of findings
for the main comparison.
| Treatments for primary delusional infestation | ||||||
|
Patient or population: people with primary delusional infestation Settings: inpatient or outpatient Intervention: any relevant treatment intervention Comparison: any relevant comparison | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Any treatment | Placebo | |||||
| Global state: clinically important change in global state | See comments | Not estimated | 0 | See comments | No data are available for any of these important outcomes. | |
| Global state: relapse | ||||||
| Mental state: clinically important change in mental state | ||||||
| Behaviour: clinically important change in general behaviour | ||||||
| Behaviour: occurrence of violent incidents (to self, others, or property) | ||||||
| Adverse events: any adverse events requiring hospitalisation | ||||||
| Quality of life: clinically important change in quality/satisfaction of life | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
CI ‐ Confidence Interval
GRADE ‐ Grading of Recommendations Assessment, Development and Evaluation
Background
Description of the condition
Delusional infestation (DI) is the persistent belief that there is pathogenic infestation of the skin or body, without objective medical evidence (Freudenmann 2009). DI was previously known as delusional parasitosis or Ekbom's syndrome. The term 'delusional infestation' much more comprehensively covers the pathogens which patients report as infesting their skin (Bewley 2010). Another term used is 'unexplained dermopathy', which usually refers to a specific subset of patients, or may be used to avoid offending patients. The infestation manifests as itch or crawling sensations and resultant skin lesions. Patients will seek the advice of general practitioners or specialist physicians (e.g. dermatologists and microbiologists) but tend to avoid seeking psychiatric advice (Freudenmann 2009).
DI has two main forms: primary (a monosymptomatic disorder characterised by delusions and abnormal tactile sensations); and secondary (symptoms caused by another defined organic or pre‐existing psychiatric disorder or by substance abuse) (Berrios 1985; Trabert 1995). Patients believe themselves to be infested with an unknown pathogen (may be described as worms, mites or insects) and through repeated self‐examination, rigorous cleansing routines or attempts to capture the agent, patients will cause skin lesions, perpetuating the belief of ongoing infestation. Diagnostic criteria are limited, and classically patients with primary DI will be middle‐aged to elderly, with a female predominance, and little social, medical or psychiatric background (Freudenmann 2009). Patients tend to be socially isolated (Trabert 1993). There is functional magnetic resonance imaging (fMRI) evidence that brain changes are identifiable in patients with primary DI (Eccles 2013). Disordered reasoning and judgement have also been described in patients with primary DI, which makes treatment particularly difficult, especially when patients are difficult to engage and averse to the possibility of a non‐skin disorder (Zomer 1998). There is, however, increasing evidence that engagement, adherence to treatment and prognosis may be better than previously thought, especially when patients are seen in a dedicated psycho‐dermatology clinic (Ahmed 2013; Wong 2011).
Although largely considered a rare or infrequent disorder, there is a lack of objective data to describe the true incidence of primary DI. The disorder is likely under‐reported, and over 1400 cases have been described in the existing literature (Freudenmann 2009). A previous study estimated the incidence of primary DI as 0.845 per 100,000 persons (Trabert 1993). More recently, however, a population‐based study of the incidence of primary DI reports an overall age and sex‐adjusted incidence of 1.9 per 100,000 person years (Bailey 2014). This supports previous suggestions that primary DI is under‐reported, with a lack of accurate epidemiological information (Freudenmann 2009). The duration of the illness has been reported as lasting between days to 35 years, with an average duration of 3.13 years (this includes all forms of DI) (Trabert 1991). The pathophysiology of primary DI is multifactorial, and a number of factors have been suggested, including genetics, premorbid traits, acute triggers and social vulnerability (Freudenmann 2009).
Description of the intervention
The review considered any interventions used in the treatment of primary DI. This involves both pharmacological and non‐pharmacological options. Pharmacological options are prescribed according to the type of DI experienced by the patient (primary or secondary). Primary DI is treated most commonly with antipsychotics, including risperidone, amisulpride, quetiapine, olanzapine and historically, pimozide (Elmer 2000; Freudenmann 2009). Second generation (or atypical) antipsychotics are the preferred treatment option mainly because of the more favourable side‐effect profile. Controlled clinical trials of antipsychotics are difficult and there are consequently very few such trials. Evidence for use of one medication over another is largely based on case series evidence. Antidepressants have been used in the treatment of secondary DI, but also in primary DI with symptoms of antipsychotic‐induced depression or for associated co‐morbid affective disease (Cipriani 2009; Freudenmann 2009). Non‐pharmacological options have included psychotherapy (useful in 10% of patients studied) (Zanol 1998), neurosurgery (prefrontal leucotomy was successful for remission of DI in a single patient) (Partridge 1950), transcutaneous electric stimulation (used for peripheral tactile symptoms) (Yamashita 1986), and electroconvulsive therapy (most efficacious in treatment‐resistant secondary DI and elderly patients) (Srinivasan 1994). However, despite there being some evidence of remission of primary DI using non‐pharmacological options, the effect is limited.
Most clinicians working with patients with primary DI emphasise the importance of treating the skin symptoms and signs at the same time as treating the patients' psychological or psychiatric disease. Cutaneous treatments are tailored to the clinical picture and may include treatment with emollients, topical anti‐inflammatories, topical or systemic antibiotics and phototherapy. Management of underlying organic or psychiatric disease is also important.
How the intervention might work
The pathophysiology of primary DI is undecided. The most popular theory is via dopaminergic neurotransmission, and this is the mechanism behind the use of antipsychotics for the treatment of primary DI. The mechanisms of action of antipsychotic treatment include dopaminergic antagonism, specifically blockade of the post‐synaptic D2 receptors, although other neurotransmitter pathways are implicated (e.g. serotonergic pathways, which supports the use of antidepressant agents for relevant symptoms) (Freudenmann 2009). Pimozide, a typical antipsychotic, is a potent dopamine receptor blocker, with additional 5‐HT2 and opiate receptor blockade, as well as anti‐pruritic properties (Freudenmann 2009). It has shown to be effective in patients with primary DI, but is now used less frequently due to its side‐effect profile (including extrapyramidal symptoms and an increased risk of sudden death due to prolongation of the QT interval) (Freudenmann 2009). Risperidone, an atypical antipsychotic, acts on serotonergic 5‐HT2 and dopaminergic D2 receptors, and has a more favoured safety profile than traditional antipsychotic medications (Friedmann 2006). Other atypical antipsychotics used in the treatment of primary DI include olanzapine, amisulpride, quetiapine and aripiprazole. The success reported in cases of primary DI responding to antipsychotic medication make this unlikely to be a placebo effect. The mechanisms involved in the non‐pharmacological treatment of primary DI are, as yet, unclear, and may involve neural pathways (Freudenmann 2009).
The mechanism of a non‐pharmacological intervention depends entirely on the intervention used. Zanol 1998 demonstrated that patients with DI who have 'shakable beliefs' (i.e. could imagine that they are not infested) may respond well to suggestion therapy (i.e. the suggestion by a health professional that they are not infected and their symptoms are explainable). These patients, once identified, could be reassured and offered alternative treatment (Zanol 1998). Prefrontal leucotomy was performed by Partridge 1950, and induced remission of symptoms in the index case. This type of psychosurgery was performed as psychoses were thought to be secondary to brain pathology, that was theoretically removed during the procedure. Transcutaneous electric stimulation was used to reduce peripheral tactile symptoms experienced by patients with DI (Yamashita 1986). The mechanism likely involves symptom control via peripheral receptor blockade (Yamashita 1986). Electroconvulsive therapy for elderly patients with refractory DI, secondary to depression, or contraindications to antipsychotic agents, has shown to be useful (Srinivasan 1994). Although the mechanism of electroconvulsive therapy is unknown, it is thought to alter brain metabolism and chemistry through seizure induction.
Why it is important to do this review
There is currently no review of the treatments used for primary DI. This is largely due to the lack of randomised controlled trials in this area. Primary DI is a diagnosis not infrequently encountered by both dermatologists and psychiatrists, it can severely disable a patient's quality of life as well as that of their friends, families or care‐givers yet no high quality evidence base regarding effectiveness of interventions currently used for people with primary DI is available.
Objectives
To evaluate the effectiveness of different treatments in primary delusional infestation (DI) (see Differences between protocol and review).
Methods
Criteria for considering studies for this review
Types of studies
All relevant randomised controlled trials. We planned to include trials described as 'double blind', but whose randomisation was implied, in a sensitivity analysis (see Sensitivity analysis). If their inclusion did not result in a substantive difference, they were to remain in the analyses. If their inclusion did result in important clinically significant but not necessarily statistically significant differences, we were not going to add the data from these lower quality studies to the results of the better trials, but would have presented such data within a subcategory. We also decided to exclude quasi‐randomised studies, such as those allocating by alternate days of the week. Where people were given additional treatments within antipsychotics, antidepressants, psychotherapy, neurosurgery, transcutaneous electric stimulation or electroconvulsive therapy, we planned to include data if the adjunct treatment was evenly distributed between groups and it was only the antipsychotics, antidepressants, psychotherapy, neurosurgery, transcutaneous electric stimulation or electroconvulsive therapy that was randomised.
Types of participants
Adults, however defined, with primary DI by any means of diagnosis. We were interested in making sure that information was as relevant to the current care of people with primary DI as possible so intended to clearly highlight the current clinical state (acute, early post‐acute, partial remission, remission), as well as the stage (prodromal, first episode, early illness, persistent), and whether the studies primarily focused on people with particular problems (for example, treatment‐resistant illnesses).
Types of interventions
1. Pharmacological treatment
1.1 Antipsychotics: any dose and any mode or pattern of administration. This includes first‐ or second‐generation antipsychotic medications 1.2 Antidepressants: any dose and any mode or pattern of administration. This includes antidepressant medications of any class
2. Non‐pharmacological treatment
2.1 Psychotherapy: any form of psychotherapy. This includes individual or group therapy 2.2 Neurosurgery 2.3 Transcutaneous electric stimulation 2.4 Electroconvulsive therapy
3. Any other treatment (pharmacological and non‐pharmacological)
4. No treatment, standard care or placebo
Types of outcome measures
We intended, where possible, to divide outcomes into short term (less than six months), medium term (six to 12 months) and long term (over one year).
We intended to report binary outcomes recording clear and clinically meaningful degrees of change (e.g. global impression of much improved, or more than 50% improvement on a rating scale as defined within the trials) before any others. Thereafter we planned to list other binary outcomes and then those that are continuous.
For outcomes such as 'clinically important change', 'any change', and 'relapse', we planned to employ the definition used by each of the trials.
For valid scales please see (Data extraction and management).
Primary outcomes
1. Global state
1.1 Clinically important change in global state 1.2 Relapse
2. Mental state
2.1 Clinically important change in overall mental state
3. Leaving the study
3.1 For any reason
Secondary outcomes
1. Global state
1.1 Any change in global state 1.2 Average endpoint or change score on global state scale
2. Mental state
2.1 Clinically important change in mental state 2.2 Average endpoint or change score on mental state scale
3. Behaviour
3.1. General
3.1.1 Clinically important change in general behaviour 3.1.2 Any change in general behaviour 3.1.2 Average endpoint or change score on behaviour scale
3.2 Specific
3.2.1 Employment status during trial (employed/unemployed) 3.2.2 Occurrence of violent incidents (to self, others, or property) 3.2.3 Substance abuse
4. Functioning
4.1 Clinically important change in functioning (including social) 4.2 Any change in functioning 4.3 Average endpoint or change score on functioning scale
5. Adverse effect/events
5.1 General
5.1.1 Adverse event requiring hospitalisation 5.1.2 At least one serious adverse effect/event 5.1.3 Average endpoint or change score on adverse effect scale
5.2 Specific ‒ incidence
5.2.1 Allergic reactions 5.2.2 Blood dyscrasia such as agranulocytosis 5.2.3 Central nervous system (ataxia, nystagmus, drowsiness, fits, diplopia, tremor) 5.2.4 Death (suicide and non‐suicide deaths) 5.2.5 Endocrinological dysfunction (hyperprolactinaemia) 5.2.6 Movement disorders (extrapyramidal side effects) 5.2.7 Weight change
6. Quality/satisfaction of life
6.1. Clinically important change in quality/satisfaction of life ‒ as defined by each of the studies 6.2 Any change in quality/satisfaction of life ‒ as defined by each of the studies 6.3. Average endpoint or change score on quality/satisfaction of life scale
7. Service use
7.1. Hospital admission 7.2. Days in hospital 7.3. Change in hospital status
8. Economic 8.1 Direct cost of care 8.2 Indirect cost of care
'Summary of findings' table
We planned to use the GRADE approach to interpret findings (Schünemann 2017); and use GRADE profiler to import data from Review Manager 5 (RevMan 5) to create a 'Summary of findings' table (GRADEpro GDT; Review Manager 2014). These tables provide outcome‐specific information concerning the overall quality of evidence from each included study in the comparison, the magnitude of effect of the interventions examined, and the sum of available data on all outcomes we rated as important to patient care and decision making. We selected the following main outcomes as important for inclusion in a 'Summary of findings' table.
Global state: clinically important change in global state
Global state: relapse
Mental state: clinically important change in mental state
Behaviour: clinically important change in general behaviour
Behaviour: occurrence of violent incidents (to self, others, or property)
Adverse events: any adverse events requiring hospitalisation
Quality of life: clinically important change in quality/satisfaction of life
In future versions of this review, if data are not available for these pre‐specified outcomes but are available for ones that are similar, we will present the closest outcome to the pre‐specified one in the table but take this into account when grading the finding; (see Differences between protocol and review).
Search methods for identification of studies
Electronic searches
Cochrane Schizophrenia Group's Study‐Based Register of Trials
On 19 March 2019, the information specialist searched the register using the following search strategy.
*Delusional Infestation* in Healthcare Condition of STUDY
In such study‐based registers, searching the major concept retrieves all the synonyms and relevant studies because all the studies have already been organised based on their interventions and linked to the relevant topics (Shokraneh 2017).
This register is compiled by systematic searches of major resources (AMED, BIOSIS, CENTRAL, CINAHL, ClinicalTrials.Gov, Embase, ISRCTN, MEDLINE, PsycINFO, PubMed, WHO ICTRP) and their monthly updates, ProQuest Dissertations and Theses A&I and its quarterly update, Chinese databases (CBM, CNKI, and Wanfang) and their annual updates, handsearches, grey literature, and conference proceedings (see Group's website). There is no language, date, document type, or publication status limitations for inclusion of records into the register.
For previous searches, please see Appendix 1.
Searching other resources
1. Reference searching
We would have inspected references of all included studies for further relevant studies.
2. Personal contact
We also planned to contact the first author of each included study for information regarding unpublished trials.
Data collection and analysis
Selection of studies
Review authors IA and AA independently inspected citations from the searches to identify relevant abstracts. A random 20% sample was independently re‐inspected by RA to ensure reliability. Where disputes arose, we would have acquired the full report for more detailed scrutiny. We would have obtained full reports of the abstracts meeting the review criteria, which AB and RT would have inspected. Again, RA would have re‐inspected a random 20% of reports, in order to ensure reliable selection. Where it was not possible to resolve disagreement by discussion, we would have attempted to contact the authors of the study for clarification.
Data extraction and management
We did not find any studies that fulfilled our inclusions criteria and therefore we did not carry out any data extraction or management for this version of the review. In future versions we intend to use the methods outlined below. These methods are updated from our protocol methods (see Differences between protocol and review).
1. Extraction
Review authors IA and AA will extract data from all included studies. In addition, to ensure reliability, AB and RH will independently extract data from a random sample of these studies, comprising 10% of the total. We will attempt to extract data presented only in graphs and figures whenever possible, but will include only if two reviewers independently obtain the same result. If studies are multi‐centre, then where possible we will extract data relevant to each. We will discuss any disagreement and document our decisions. If necessary, we will attempt to contact authors through an open‐ended request in order to obtain missing information or for clarification. RT will help clarify issues regarding any remaining problems and we will document these final decisions.
2. Management
2.1 Forms
We will extract data onto standard, pre‐designed, simple forms.
2.2 Scale‐derived data
We will include continuous data from rating scales only if:
a) the psychometric properties of the measuring instrument have been described in a peer‐reviewed journal (Marshall 2000); b) the measuring instrument has not been written or modified by one of the trialists for that particular trial; and c) the instrument is a global assessment of an area of functioning and not sub‐scores which are not, in themselves, validated or shown to be reliable. There are, however, exceptions: we will include sub‐scores from mental state scales measuring positive and negative symptoms of schizophrenia.
Ideally the measuring instrument should either be i. a self‐report or ii. completed by an independent rater or relative (not the therapist). We realise that this is not often reported clearly: in 'Description of studies' we will note if this is the case or not.
2.3 Endpoint versus change data
There are advantages of both endpoint and change data: change data can remove a component of between‐person variability from the analysis; however, calculation of change needs two assessments (baseline and endpoint) that can be difficult to obtain in unstable and difficult‐to‐measure conditions such as schizophrenia. We have decided primarily to use endpoint data, and only use change data if the former are not available. If necessary, we will combine endpoint and change data in the analysis, as we prefer to use mean differences (MDs) rather than standardised mean differences (SMDs) throughout (Deeks 2011).
2.4 Skewed data
Continuous data on clinical and social outcomes are often not normally distributed. To avoid the pitfall of applying parametric tests to non‐parametric data, we will apply the following standards to relevant continuous data before inclusion.
For endpoint data from studies including fewer than 200 participants:
a) when a scale starts from the finite number zero, we will subtract the lowest possible value from the mean, and divide this by the standard deviation. If this value is lower than one, it strongly suggests that the data are skewed and we will exclude these data. If this ratio is higher than one but less than two, there is a suggestion that the data are skewed: we will enter these data and test whether their inclusion or exclusion would change the results substantially. If such data change results we will enter as 'other data'. Finally, if the ratio is larger than two we will include these data, because it is less likely that they are skewed (Altman 1996).
b) if a scale starts from a positive value (such as the Positive and Negative Syndrome Scale (PANSS), which can have values from 30 to 210 (Kay 1986)), we will modify the calculation described above to take the scale starting point into account. In these cases skewed data are present if 2 SD > (S − S min), where S is the mean score and 'S min' is the minimum score.
Please note: we will enter all relevant data from studies of more than 200 participants in the analysis irrespective of the above rules, because skewed data pose less of a problem in large studies. We will also enter all relevant change data, as when continuous data are presented on a scale that includes a possibility of negative values (such as change data), it is difficult to tell whether or not data are skewed.
2.5 Common measurement
To facilitate comparison between trials we aim, where relevant, to convert variables that can be reported in different metrics, such as days in hospital (mean days per year, per week or per month) to a common metric (e.g. mean days per month).
2.6 Conversion of continuous to binary
Where possible, we will make efforts to convert outcome measures to dichotomous data. This can be done by identifying cut‐off points on rating scales and dividing participants accordingly into 'clinically improved' or 'not clinically improved'. It is generally assumed that if there is a 50% reduction in a scale‐derived score such as the Brief Psychiatric Rating Scale (BPRS) (Overall 1962), or the PANSS (Kay 1986), this could be considered as a clinically significant response (Leucht 2005a; Leucht 2005b). If data based on these thresholds are not available, we will use the primary cut‐off presented by the original authors.
2.7 Direction of graphs
Where possible, we will enter data in such a way that the area to the left of the line of no effect indicates a favourable outcome for the treatment intervention. Where keeping to this makes it impossible to avoid outcome titles with clumsy double‐negatives (e.g. 'not un‐improved') we will report data where the left of the line indicates an unfavourable outcome and note this in the relevant graphs.
Assessment of risk of bias in included studies
Review authors IA and AA will work independently to assess risk of bias by using criteria described in the Cochrane Handbook for Systematic Reviews of Interventions to assess trial quality (Higgins 2017). This set of criteria is based on evidence of associations between potential overestimation of effect and the level of risk of bias of the article that may be due to aspects of sequence generation, allocation concealment, blinding, incomplete outcome data and selective reporting, or the way in which these 'domains' are reported.
If the raters disagree, we will make the final rating by consensus. Where inadequate details of randomisation and other characteristics of trials are provided, we will attempt to contact authors of the studies in order to obtain further information. We will report non‐concurrence in quality assessment, but if disputes arise regarding the category to which a trial is to be allocated, we will resolve this by discussion.
We will note the level of risk of bias in both the text of the review, Figure 1, Figure 2, and the Table 1
1.
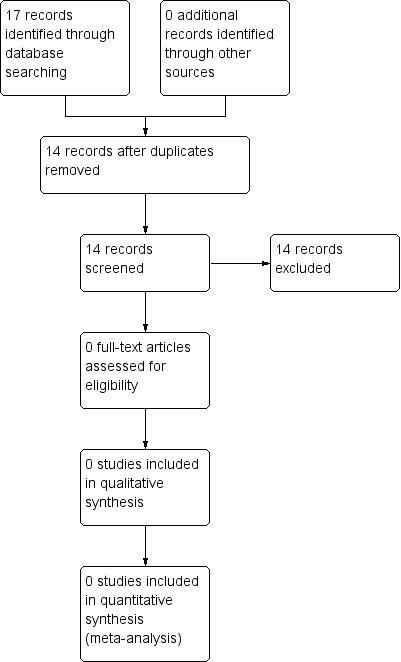
Study flow diagram.
Measures of treatment effect
1. Binary data
For binary outcomes we will calculate a standard estimation of the risk ratio (RR) and its 95% confidence interval (CI), as it has been shown that RR is more intuitive than odds ratios (Boissel 1999); and that odds ratios tend to be interpreted as RR by clinicians (Deeks 2000). Although the number needed to treat for an additional beneficial outcome (NNTB) and the number needed to treat for an additional harmful outcome (NNTH), with their CIs, are intuitively attractive to clinicians, they are problematic to calculate and interpret in meta‐analyses (Hutton 2009). For binary data presented in the 'Summary of findings' table/s we will, where possible, calculate illustrative comparative risks.
2. Continuous data
For continuous outcomes we will estimate MD between groups. We prefer not to calculate effect size measures (SMD). However if scales of very considerable similarity are used, we will presume there is a small difference in measurement, and we will calculate effect size and transform the effect back to the units of one or more of the specific instruments.
Unit of analysis issues
1. Cluster trials
Studies increasingly employ 'cluster randomisation' (such as randomisation by clinician or practice), but analysis and pooling of clustered data poses problems. Authors often fail to account for intra‐class correlation in clustered studies, leading to a unit‐of‐analysis error whereby P values are spuriously low, CIs unduly narrow and statistical significance overestimated (Divine 1992). This causes type I errors (Bland 1997; Gulliford 1999).
Where clustering has been incorporated into the analysis of primary studies, we will present these data as if from a non‐cluster randomised study, but adjust for the clustering effect.
Where clustering is not accounted for in primary studies, we will present data in a table, with a (*) symbol to indicate the presence of a probable unit‐of‐analysis error. We will seek to contact first authors of studies to obtain intra‐class correlation coefficients for their clustered data and to adjust for this by using accepted methods (Gulliford 1999).
We have sought statistical advice and have been advised that the binary data from cluster trials presented in a report should be divided by a 'design effect'. This is calculated using the mean number of participants per cluster (m) and the intra‐class correlation coefficient (ICC): thus design effect = 1 + (m − 1) * ICC (Donner 2002). If the ICC is not reported we will assume it to be 0.1 (Ukoumunne 1999).
If cluster studies have been appropriately analysed and have taken intra‐class correlation coefficients and relevant data documented in the report into account, synthesis with other studies will be possible using the generic inverse variance technique.
2. Cross‐over trials
A major concern of cross‐over trials is the carry‐over effect. This occurs if an effect (e.g. pharmacological, physiological or psychological) of the treatment in the first phase is carried over to the second phase. As a consequence, participants can differ significantly from their initial state at entry to the second phase, despite a wash‐out phase. For the same reason cross‐over trials are not appropriate if the condition of interest is unstable (Elbourne 2002). As both carry‐over and unstable conditions are very likely in severe mental illness, we will only use data from the first phase of cross‐over studies.
3. Studies with multiple treatment groups
Where a study involves more than two treatment arms we will (if relevant) present the additional treatment arms in comparisons. If data are binary we will simply add these and combine within the two‐by‐two table. If data are continuous we will combine data following the formula in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Where additional treatment arms are not relevant, we will not reproduce these data.
Dealing with missing data
1. Overall loss of credibility
At some degree of loss to follow‐up, data must lose credibility (Xia 2009). We choose that, for any particular outcome, should more than 50% of data be unaccounted for we will not reproduce these data or use them within analyses. If, however, more than 50% of those in one arm of a study are lost, but the total loss is less than 50%, we will address this within the 'Summary of findings' table/s by down‐rating quality. Finally, we will also downgrade quality within the 'Summary of findings' table/s should the loss be 25% to 50% in total.
2. Binary
In the case where attrition for a binary outcome is between 0% and 50% and where these data are not clearly described, we will present data on a 'once‐randomised‐always‐analyse' basis (an intention‐to‐treat analysis (ITT)). Those leaving the study early are all assumed to have the same rates of negative outcome as those who completed. We will use the rate of those who stay in the study — in that particular arm of the trial — and apply this also to those who did not. We will undertake a sensitivity analysis testing how prone the primary outcomes are to change when data only from people who complete the study to that point are compared to the intention‐to‐treat analysis using the above assumptions.
3. Continuous
3.1 Attrition
We will use data where attrition for a continuous outcome is between 0% and 50%, and data only from people who complete the study to that point are reported.
3.2 Standard deviations
If standard deviations (SDs) are not reported, we will try to obtain the missing values from the authors. If these are not available, where there are missing measures of variance for continuous data, but an exact standard error (SE) and CIs available for group means, and either P value or t value available for differences in mean, we can calculate SDs according to the rules described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). When only the SE is reported, SDs are calculated by the formula SD = SE * √(n). The Cochrane Handbook for Systematic Reviews of Interventions presents detailed formulae for estimating SDs from P, t or F values, CIs, ranges or other statistics (Higgins 2011). If these formulae do not apply, we will calculate the SDs according to a validated imputation method which is based on the SDs of the other included studies (Furukawa 2006). Although some of these imputation strategies can introduce error, the alternative would be to exclude a given study’s outcome and thus to lose information. We will nevertheless examine the validity of the imputations in a sensitivity analysis that excludes imputed values.
3.3 Assumptions about participants who left the trials early or were lost to follow‐up
Various methods are available to account for participants who left the trials early or were lost to follow‐up. Some trials just present the results of study completers; others use the method of last observation carried forward (LOCF); while more recently, methods such as multiple imputation or mixed‐effects models for repeated measurements (MMRM) have become more of a standard. While the latter methods seem to be somewhat better than LOCF (Leon 2006), we feel that the high percentage of participants leaving the studies early and differences between groups in their reasons for doing so is often the core problem in randomised schizophrenia trials. We will therefore not exclude studies based on the statistical approach used. However, by preference we will use the more sophisticated approaches, i.e. we will prefer to use MMRM or multiple‐imputation to LOCF, and we will only present completer analyses if some kind of ITT data are not available at all. Moreover, we will address this issue in the item 'Incomplete outcome data' of the 'Risk of bias' tool.
Assessment of heterogeneity
1. Clinical heterogeneity
We will consider all included studies initially, without seeing comparison data, to judge clinical heterogeneity. We will simply inspect all studies for participants who are clearly outliers or situations that we had not predicted would arise and, where found, discuss such situations or participant groups.
2. Methodological heterogeneity
We will consider all included studies initially, without seeing comparison data, to judge methodological heterogeneity. We will simply inspect all studies for clearly outlying methods which we had not predicted would arise and discuss any such methodological outliers.
3. Statistical heterogeneity
3.1 Visual inspection
We will inspect graphs visually to investigate the possibility of statistical heterogeneity.
3.2 Employing the I² statistic
We will investigate heterogeneity between studies by considering the I² statistic alongside the Chi² P value. The I² statistic provides an estimate of the percentage of inconsistency thought to be due to chance (Higgins 2003). The importance of the observed value of I² depends on the magnitude and direction of effects as well as the strength of evidence for heterogeneity (e.g. P value from Chi² test, or a confidence interval for I²). We will interpret an I² estimate greater than or equal to 50% and accompanied by a statistically significant Chi² statistic as evidence of substantial heterogeneity (Chapter 9; Cochrane Handbook for Systematic Reviews of Interventions) (Deeks 2011). When substantial levels of heterogeneity are found in the primary outcome, we will explore reasons for heterogeneity (Subgroup analysis and investigation of heterogeneity
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings is influenced by the nature and direction of results (Egger 1997). These are described in section 10.1 of the Cochrane Handbook for Systematic Reviews of Interventions (Sterne 2011).
1. Protocol versus full study
We will try to locate protocols of included randomised trials. If the protocol is available, we will compare outcomes in the protocol and in the published report. If the protocol is not available, we will compare outcomes listed in the Methods section of the trial report with actually reported results.
2. Funnel plot
We are aware that funnel plots may be useful in investigating reporting biases but are of limited power to detect small‐study effects. We will not use funnel plots for outcomes where there are less than 10, or where all studies are of similar size. In cases where funnel plots are possible, we will seek statistical advice in their interpretation.
Data synthesis
We understand that there is no closed argument for preference for use of fixed‐effect or random‐effects models. The random‐effects method incorporates an assumption that the different studies are estimating different, yet related, intervention effects. This often seems to be true to us and the random‐effects model takes into account differences between studies, even if there is no statistically significant heterogeneity. There is, however, a disadvantage to the random‐effects model: it puts added weight onto small studies, which often are the most biased ones. Depending on the direction of effect, these studies can either inflate or deflate the effect size. We choose to use a random‐effects model for analyses.
Subgroup analysis and investigation of heterogeneity
1. Subgroup analyses
1.1 Primary outcomes
We do not anticipate sub‐group analysis.
2. Investigation of heterogeneity
We will report if inconsistency is high. Firstly, we will investigate whether data have been entered correctly. Secondly, if data are correct we will inspect the graph visually and remove outlying studies successively to see if homogeneity is restored. For this review we have decided that should this occur with data contributing to the summary finding no more than 10% of the total weighting, we will present data. If not, we will not pool these data and will discuss any issues. We know of no supporting research for this 10% cut‐off but are investigating use of prediction intervals as an alternative to this unsatisfactory state.
When unanticipated clinical or methodological heterogeneity is obvious we will simply state hypotheses regarding these for future reviews or versions of this review. We do not anticipate undertaking analyses relating to these.
Sensitivity analysis
We will carry out sensitivity analyses for primary outcomes only. If there are substantial differences in the direction or precision of effect estimates in any of the sensitivity analyses listed below, we will not add data from the lower‐quality studies to the results of the higher‐quality trials, but will present these data within a subcategory. If their inclusion does not result in a substantive difference, they will remain in the analyses.
1. Implication of randomisation
If trials are described in some way as to imply randomisation, we will compare data from the implied trials with trials that are randomised.
2. Assumptions for lost binary data
Where we have to make assumptions regarding people lost to follow‐up (see Dealing with missing data) we will compare the findings when we use our assumption compared with completer data only. If there is a substantial difference, we will report results and discuss them but continue to employ our assumption.
3. Assumptions for lost continuous data
Where we have to make assumptions regarding missing SDs (see Dealing with missing data), we will compare the findings when we use our assumption compared with data that are not imputed. If there is a substantial difference, we will report results and discuss them but continue to employ our assumption.
4. Risk of bias
We will analyse the effects of excluding trials that are at high risk of bias across one or more of the domains (see Assessment of risk of bias in included studies).
5. Imputed values
We will also undertake a sensitivity analysis to assess the effects of including data from trials where we use imputed values for ICC in calculating the design effect in cluster randomised trials.
6. Fixed‐ and random‐effects
We will synthesise data using a random‐effects model; however, we will also synthesise data for the primary outcome using a fixed‐effect model to evaluate whether this alters the significance of the results. If there is a difference, we will note this in the text.
Results
Description of studies
We did not find any studies that fulfilled the inclusion criteria.
Results of the search
We found 17 records through electronic searching; these were from 14 studies (Figure 1).
Included studies
There are no included studies in this review.
Excluded studies
There are no excluded studies in this review.
Risk of bias in included studies
No studies could be included in this review; hence we are unable to assess risk of bias.
Allocation
There are no included studies in this review.
Blinding
There are no included studies in this review.
Incomplete outcome data
There are no included studies in this review.
Selective reporting
There are no included studies in this review.
Other potential sources of bias
There are no included studies in this review.
Effects of interventions
See: Table 1
We had hoped to gather information on the effects of pharmacological treatment (including antipsychotic and antidepressant medications), non‐pharmacological treatment (including any form of psychotherapy, neurosurgery, transcutaneous electric stimulation and electroconvulsive therapy), and any other treatment or no treatment on clinical response, behaviour, any adverse events, satisfaction of life, service utilisation and cost of care. Such data are not available from randomised trials of care.
Discussion
Summary of main results
We did not find any study which compared different treatments in primary delusional infestation (DI) to placebo.
Overall completeness and applicability of evidence
There were no RCTs examining treatments for this condition. A general search of the literature for this condition reveals clinical anecdotal evidence in the form of case reports, retrospective case series, audits and literature reviews. None of this approached the criteria required for this review.
Quality of the evidence
The review identified no evidence from randomised controlled trials.
Potential biases in the review process
The authors were interested in any evidence examining treatment efficacy in delusional infestation. The authors can see limited potential for bias because the electronic search followed Cochrane methodology and used a wide range of terminology encompassing this disorder. No search limitations were placed on document type, publication date, language or publication status.
Agreements and disagreements with other studies or reviews
We have been unable to find any trials for inclusion in this Cochrane Review. Review of the literature in this area produces treatment studies which are either case reports or case series or other literature reviews summarising these. Lepping 2007 reviewed evidence for efficacy of first and second generation antipsychotics in primary and other delusional infestation. They found no randomised controlled trials with adequate samples. Since their search in 2005, this current Cochrane Review has found no change in this situation and there is still no evidence from randomised controlled trials available. For many years from the 1980s pimozide was regarded as the treatment of choice with some evidence base. This evidence came from two very small trials: (i) Hamann 1982 performed a double‐blind cross‐over trial with a 4‐week washout period comparing pimozide and placebo in 11 patients with mixed DI; (ii) Ungvári 1986 performed a second placebo controlled trial in 10 patients with primary and secondary delusional infestation using an on‐off‐on design. Both trials produced evidence suggesting the efficacy of pimozide but both had major limitations: neither used random allocation, samples were small and there was a mixture of primary and secondary DI. In both, treatment periods were short (6 weeks, and 2 or 3 weeks). Despite these limitations this was the best available evidence and for many years pimozide was widely used, until more recent concerns about its safety have led to it no longer being recommended (Freudenmann 2009). A huge range of typical antipsychotics have been used for treating people with delusional infestation but the only evidence concerning effectiveness comes from two open trials (Paholpak 1990; Srinivasan 1994), or case reports (Freudenmann 2009). These trials and reports indicate that there is nothing specific in the effect of pimozide, and reduction of symptoms in DI could be achieved with many other antidopaminergic agents. There is only one open study of the use of depot antipsychotics in delusional infestation: it showed a good response but is very limited as the sample was small, and it was not controlled (Frithz 1979). The evidence is even slimmer when considering atypical antipsychotics. The most comprehensive review is again by Freudenmann and Lepping who, as in this Cochrane Review, found no randomised controlled trials, and even a lack of open or prospective trials (Freudenmann 2008). They summarise the case reports in this area and helpfully try to summarise these quantitatively in order to provide some guidance on choice of antipsychotic. This would still seem to be the best evidence available although, as they themselves acknowledge, this evidence is low level and needs confirmation by more rigorous trials.
Authors' conclusions
Implications for practice.
1. For people with primary delusional infestation
People with primary delusional infestation continue to struggle with engagement and compliance. The lack of evidence for pharmacological and non‐pharmacological treatment makes it more difficult to convince people with primary delusional infestation to take part in the management plan.
2. For clinicians
There is currently a lack of evidence to support any specific intervention to treat people with primary delusional infestation.
3. For policy makers
We could not find any trial comparing pharmacological or non‐pharmacological treatment to placebo. Any available evidence is therefore not of high quality and is not generalisable to the population of people with primary delusional infestation.
Implications for research.
1. General
This review highlights the need for quality‐controlled clinical trials. Where trials are conducted, strict adherence to CONSORT standards would aid clarity and result in high‐quality reporting. Data should be made available so that further research can be undertaken (AllTrials). Where only P values are presented, it is difficult to obtain data of value. Numerical data should be clearly presented to aid extraction and statistical analysis. Information regarding the number of participants, standard deviations and means is beneficial to obtaining data of sufficient quality for inclusion. Studies with attrition should make it clear where 'last observation carried forward' (LOCF) or intention‐to‐treat analysis has been used, as otherwise randomisation is broken.
2. Specific
It is clear that no RCTs have been conducted in delusional parasitosis. Several of the authors of this review attempted to set up a randomised controlled trial of the use of risperidone in a specialist London psychodermatology clinic. The obstacles proved insurmountable so the trial never went ahead. The problems encountered are likely to arise in any attempt to set up such a trial which probably explains the dearth of RCT evidence. From the authors' experience the main obstacle to conducting any RCTs in the patient group is likely to be negotiating the ethics of a trial in a disorder where many patients' illness explanation differs from their doctors' view of the disorder. In the case of antipsychotic trials, the use of antipsychotics in delusional infestation is an off‐license use and as such ethics committees require stringent criteria to be fulfilled. Patients with primary delusional infestation are relatively rare in dermatology clinics though common in specialist psychodermatology clinics. We believe the only way an adequately powered RCT could be run would be using a multicentre design and there are then huge issues with co‐ordination of ethics approval and NHS research office approval across different sites. We hope that co‐ordination of specialists with an interest in this disorder and committed to designing and running a multicentre trial will provide the RCT evidence base currently lacking. We suggest a design of a future trial in Table 2.
1. Future trial design.
| Methods | Allocation: randomised, fully explicit description of methods of randomisation and allocation concealment. Every precaution is taken to minimise the effect of biases by using blinded or independent raters. Intention‐to‐treat analysis: clear description from which groups the withdrawals happened, the reason for the withdrawal and their outcome. Setting: community psychodermatology clinic or psychiatric outpatient clinic. Duration: 6 months minimum, and then follow‐up to at least 6 months. |
| Participants | Diagnosis: people with primary delusional infestation N = 300.* Age: adults (18+). Sex: both. |
| Interventions | 1. Treatment as usual + randomised to intervention (e.g. 2nd generation antipsychotic medication, at low dose). N = 150. 2. Standard treatment as usual + placebo. N = 150. The above trial could be amended to address non‐pharmacological therapy as an intervention and patients could be accordingly randomised to this in addition to treatment as usual, compared to placebo. |
| Outcomes | General: global improvement, use of scales such as CGI. Quality of life. Compliance with treatment Mental state: BPRS and PANSS. Service outcomes: frequency of clinic appointments. Functioning: including employment. Loss to follow‐up. Serious events: any, list. Satisfaction. Economic outcomes. |
| Notes | * Size of study with sufficient power to highlight ˜20% difference between groups for primary outcome |
Acknowledgements
The Cochrane Schizophrenia Group Editorial Base in Nottingham produces and maintains standard text for use in the Methods section of their reviews. We have used this text as the basis of what appears here and adapted it as required.
The search terms were developed by Farhad Shokraneh, the Trial Search Co‐ordinator of the Cochrane Schizophrenia Group; and by Iyas Assalman, lead review author.
Appendices
Appendix 1. Previous electronic searches
Search in 2014
1. Cochrane Schizophrenia Group’s Trials Register
On 24 December 2014, the Trials Search Co‐ordinator (TSC) searched the Cochrane Schizophrenia Group’s Register of Trials using the following phrase:
(Delusion* or (Ekbom* NEXT Syndrome*) or (Unexplained NEXT Dermopath*) or Morgellon* or Parasitophobi*) in Title or Abstract Fields of REFERENCE or (Delusion* or (Ekbom* NEXT Syndrome*) or (Unexplained NEXT Dermopath*) or Morgellon* or Parasitophobi*) in Health Care Condition Field of STUDY
The Cochrane Schizophrenia Group’s Registry of Trials is compiled by systematic searches of major resources (including AMED, BIOSIS, CINAHL, Embase, MEDLINE, PsycINFO, PubMed, and registries of Clinical Trials) and their monthly updates, handsearches, grey literature, and conference proceedings (see Group Module). There is no language, date, document type, or publication status limitations of inclusion of records in the register.
Differences between protocol and review
We have updated the Methods section since protocol publication to reflect latest changes to the Methods template employed by Cochrane Schizophrenia. These are modifications and improvements or clarifications to previous methods and not major changes in methodology.
We have clarified and corrected our objectives to indicate that the aim of the review is to assess effectiveness of treatments for primary delusional infestation compared with any other relevant comparison and not just placebo, as per our 'Types of interventions' published in the protocol.
We have renamed some of the outcomes to follow latest terminology and layout used by Cochrane Schizophrenia: for example 'clinical response' is now 'global state'; 'significant response' is now 'clinically important change'. These are not changes to the type of outcomes considered for inclusion.
We have clarified outcomes that the 'Summary of findings' table should ideally report for clinically important change, and clarified what type of adverse effect and specific behaviour we feel is important to report, as well as added in a mental state outcome.
Contributions of authors
Iyas Assalman ‒ trial selection, write‐up of the review.
Anthony P Bewley ‒ write‐up of the review.
Randa Alhajjar ‒ trial selection, write‐up of the review.
Alia Ahmed ‒ trial selection, write‐up of the review.
Ruth Taylor ‒ write‐up of the review.
Sources of support
Internal sources
-
East London NHS Foundation Trust, UK.
Lead author is employed by this institution
External sources
None, Other.
Declarations of interest
Iyas Assalman: no conflicts of interest directly related to this review. He has attended conferences organised and funded by pharmaceutical companies: (i) Changing Faces, 30 & 31 January 2012 organised by Lundbeck; and (ii) IMPACT Paris: "Laying the Foundation for Recovery in Mental Illness", 19‒21 March 2010 organised by Otsuka Pharmaceuticals.
Anthony P Bewley: none
Randa Alhajjar: none
Alia Ahmed: none
Ruth Taylor: none
New
References
Additional references
Ahmed 2013
- Ahmed A, Bewley A. Delusional infestation and patient adherence to treatment: an observational study. British Journal of Dermatology 2013;169(3):607‐10. [DOI] [PubMed] [Google Scholar]
Altman 1996
- Altman DG, Bland JM. Detecting skewness from summary information. BMJ 1996;313(7066):1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bailey 2014
- Bailey CH, Andersen LK, Lowe GC, Pittelkow MR, Bostwick JM, Davis MDP. A population‐based study of the incidenceof delusional infestation in Olmsted County, Minnesota, 1976‐2010. British Journal of Dermatology 2014;170(5):1130‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Berrios 1985
- Berrios GE. Delusional parasitosis and physical disease. Comprehensive Psychiatry 1985;26(5):395‐403. [DOI] [PubMed] [Google Scholar]
Bewley 2010
- Bewley AP, Lepping P, Freudenmann RW, Taylor R. Delusional parasitosis: time to call it delusional infestation. British Journal of Dermatology 2010;163(1):1‐2. [DOI] [PubMed] [Google Scholar]
Bland 1997
- Bland JM. Statistics notes. Trials randomised in clusters. BMJ 1997;315(7108):600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Boissel 1999
- Boissel JP, Cucherat M, Li W, Chatellier G, Gueyffier F, Buyse M, et al. The problem of therapeutic efficacy indices. 3. Comparison of the indices and their use [Aperçu sur la problématique des indices d'efficacité thérapeutique, 3: comparaison des indices et utilisation. Groupe d'Etude des Indices D'efficacite]. Therapie 1999;54(4):405‐11. [PUBMED: 10667106] [PubMed] [Google Scholar]
Cipriani 2009
- Cipriani A, Furukawa TA, Salanti G, Geddes JR, Higgins JP, Churchill R, et al. Comparative efficacy and acceptability of 12 new‐generation antidepressants: a multiple‐treatments meta‐analysis. Lancet 2009;373(9665):746‐58. [DOI] [PubMed] [Google Scholar]
Deeks 2000
- Deeks J. Issues in the selection for meta‐analyses of binary data. Proceedings of the 8th International Cochrane Colloquium; 2000 Oct 25‐28; Cape Town. Cape Town: The Cochrane Collaboration, 2000.
Deeks 2011
- Deeks JJ, Higgins JP, Altman DG. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JP, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Divine 1992
- Divine GW, Brown JT, Frazier LM. The unit of analysis error in studies about physicians' patient care behavior. Journal of General Internal Medicine 1992;7(6):623‐9. [DOI] [PubMed] [Google Scholar]
Donner 2002
- Donner A, Klar N. Issues in the meta‐analysis of cluster randomized trials. Statistics in Medicine 2002;21(19):2971‐80. [DOI] [PubMed] [Google Scholar]
Eccles 2013
- Eccles JA, Garfinkel SN, Taylor RE, Bewley AP, Critchley HD. Imaging abnormal skin sensations: a novel functional MRI study. Lancet 2013;381:S38. [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315(7109):629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne D, Altman DG, Higgins JP, Curtina F, Worthingtond HV, Vaile A. Meta‐analyses involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [DOI] [PubMed] [Google Scholar]
Elmer 2000
- Elmer KB, George RM, Peterson K. Therapeutic update: use of risperidone for the treatment of monosymptomatic hypochondriacal psychosis. Journal of the American Academy of Dermatology 2000;43:683‐6. [DOI] [PubMed] [Google Scholar]
Freudenmann 2008
- Freudenmann RW, Lepping P. Second‐Generation Antipsychotics in Primary and Secondary Delusional Parasitosis: Outcome and efficacy. Journal of Clinical Psychopharmacology 2008;28:500‐8. [DOI] [PubMed] [Google Scholar]
Freudenmann 2009
- Freudenmann RW, Lepping P. Delusional infestation. Clinical Microbiology Reviews 2009;22(4):690‐732. [DOI] [PMC free article] [PubMed] [Google Scholar]
Friedmann 2006
- Friedmann AC, Ekeowa‐Anderson A, Taylor R, Bewley A. Delusional parasitosis presenting as folie à trois: successful treatment with risperidone. British Journal of Dermatology 2006;155:841‐2. [DOI] [PubMed] [Google Scholar]
Frithz 1979
- Frithz A. Delusions of infestation: treatment by depot injections of neuroleptics. Clinical and Experimental Dermatology 1979;4(4):485‐8. [DOI] [PubMed] [Google Scholar]
Furukawa 2006
- Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta‐analyses can provide accurate results. Journal of Clinical Epidemiology 2006;59(1):7‐10. [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 6 August 2016. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Gulliford 1999
- Gulliford MC. Components of variance and intraclass correlations for the design of community‐based surveys and intervention studies: data from the Health Survey for England 1994. American Journal of Epidemiology 1999;149(9):876‐83. [DOI] [PubMed] [Google Scholar]
Hamann 1982
- Hamann K, Avnstorp C. Delusions of infestation treated by pimozide: a double‐blind crossover clinical study. Acta Dermato‐venereologica 1982;62(1):55‐8. [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Green S. Chapter 7: Selecting studies and collecting data. In: Higgins JP, Green S editor(s), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2017
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Hutton 2009
- Hutton JL. Number needed to treat and number needed to harm are not the best way to report and assess the results of randomised clinical trials. British Journal of Haematology 2009;146(1):27‐30. [PUBMED: 19438480] [DOI] [PubMed] [Google Scholar]
Kay 1986
- Kay SR, Opler LA, Fiszbein A. Positive and Negative Syndrome Scale (PANSS) Manual. North Tonawanda, NY: Multi‐Health Systems, 1986. [Google Scholar]
Leon 2006
- Leon AC, Mallinckrodt CH, Chuang‐Stein C, Archibald DG, Archer GE, Chartier K. Attrition in randomized controlled clinical trials: methodological issues in psychopharmacology. Biological Psychiatry 2006;59(11):1001‐5. [PUBMED: 16905632] [DOI] [PubMed] [Google Scholar]
Lepping 2007
- Lepping P, Russell I, Freudenmann RW. Antipsychotic treatment of delusional parasitosis: systematic review. British Journal of Psychiatry 2007;191:198‐205. [DOI] [PubMed] [Google Scholar]
Leucht 2005a
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel RR. What does the PANSS mean?. Schizophrenia Research 2005;79(2‐3):231‐8. [PUBMED: 15982856] [DOI] [PubMed] [Google Scholar]
Leucht 2005b
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. Clinical implications of brief psychiatric rating scale scores. British Journal of Psychiatry 2005;187:366‐71. [PUBMED: 16199797] [DOI] [PubMed] [Google Scholar]
Marshall 2000
- Marshall M, Lockwood A, Bradley C, Adams C, Joy C, Fenton M. Unpublished rating scales: a major source of bias in randomised controlled trials of treatments for schizophrenia. British Journal of Psychiatry 2000;176:249‐52. [DOI] [PubMed] [Google Scholar]
Overall 1962
- Overall JE, Gorham DR. The Brief Psychiatric Rating Scale. Psychological Reports 1962;10:799‐812. [Google Scholar]
Paholpak 1990
- Paholpak S. Delusion of parasitosis: a report of ten cases at Srinagarind Hospital. Journal of the Medical Association of Thailand 1990;73(2):111‐4. [PubMed] [Google Scholar]
Partridge 1950
- Partridge M. One operation cures three people. Effect of prefrontal leucotomy on a case of folie a deux et demi. Archives of Neurology and Psychiatry 1950;64:792‐6. [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schünemann 2017
- Schünemann HJ, Oxman AD, Higgins JP, Vist GE, Glasziou P, Akl E, et al. Chapter 11: Completing ‘Summary of findings’ tables and grading the confidence in or quality of the evidence. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Shokraneh 2017
- Shokraneh F, Adams CE. Study‐based registers of randomized controlled trials: Starting a systematic review with data extraction or meta‐analysis. BioImpacts 2017;7(4):209‐217. [DOI: 10.15171/bi.2017.25] [DOI] [PMC free article] [PubMed] [Google Scholar]
Srinivasan 1994
- Srinivasan TN, Suresh TR, Jayaram V, Fernandez MP. Nature and treatment of delusional parasitosis: a different experience in India. International Journal of Dermatology 1994;33:851‐5. [DOI] [PubMed] [Google Scholar]
Sterne 2011
- Sterne JA, Egger M, Moher D. Chapter 10: Addressing reporting biases. In: Higgins JP, Green S editor(s). Cochrane Handbook for Systematic Reviews of Intervention. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Trabert 1991
- Trabert W. Epidemiology of ectoparasitic infestation. Nervenarzt 1991;62(3):165‐9. [PubMed] [Google Scholar]
Trabert 1993
- Trabert W. Delusional parasitosis. Studies on frequency, classification and prognosis. Dissertation. Universitat des Sarlaandes, Homberg/Saar, Germany 1993.
Trabert 1995
- Trabert W. 100 years of delusional parasitosis. Meta‐analysis of 1,223 case reports. Psychopathology 1995;28(5):238‐46. [DOI] [PubMed] [Google Scholar]
Ukoumunne 1999
- Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ. Methods for evaluating area‐wide and organistation‐based intervention in health and health care: a systematic review. Health Technology Assessment 1999;3(5):iii‐92. [PubMed] [Google Scholar]
Ungvári 1986
- Ungvári G, Vladár K. Pimozide treatment for delusion of infestation. Activitas Nervosa Superior 1986;28(2):103‐7. [PubMed] [Google Scholar]
Wong 2011
- Wong S, Bewley A. Patients with delusional infestation (delusional parasitosis) often require prolonged treatment as recurrence of symptoms after cessation of treatment is common: an observational study. British Journal of Dermatology 2011;165(4):893‐6. [DOI] [PubMed] [Google Scholar]
Xia 2009
- Xia J, Adams CE, Bhagat N, Bhagat V, Bhoopathi P, El‐Sayeh H, et al. Loss to outcomes stakeholder survey: the LOSS study. Psychiatric Bulletin 2009;33(7):254‐7. [Google Scholar]
Yamashita 1986
- Yamashita T. Treatment of delusions of parasitosis: efficacy of transcutaneous electrical stimulation. Seishin Shinkeigaku Zasshi 1986;88:1‐13. [PubMed] [Google Scholar]
Zanol 1998
- Zanol K, Slaughter J, Hall R. An approach to the treatment of psychogenic parasitosis. International Journal of Dermatology 1998;37(1):56‐63. [DOI] [PubMed] [Google Scholar]
Zomer 1998
- Zomer SF, Wit RF, Bronswijk JE, Nabarro G, Vloten WA. Delusions of parasitosis. A psychiatric disorder to be treated by dermatologists? An analysis of 33 patients. British Journal of Dermatology 1998;138(6):1030‐2. [DOI] [PubMed] [Google Scholar]