

Abstract
Rationale for review
The increasing mobility of populations allows pathogens to move rapidly and far, making endemic or epidemic regions more connected to the rest of the world than at any time in history. However, the ability to measure and monitor human mobility, health risk and their changing patterns across spatial and temporal scales using traditional data sources has been limited. To facilitate a better understanding of the use of emerging mobile phone technology and data in travel medicine, we reviewed relevant work aiming at measuring human mobility, disease connectivity and health risk in travellers using mobile geopositioning data.
Key findings
Despite some inherent biases of mobile phone data, analysing anonymized positions from mobile users could precisely quantify the dynamical processes associated with contemporary human movements and connectivity of infectious diseases at multiple temporal and spatial scales. Moreover, recent progress in mobile health (mHealth) technology and applications, integrating with mobile positioning data, shows great potential for innovation in travel medicine to monitor and assess real-time health risk for individuals during travel.
Conclusions
Mobile phones and mHealth have become a novel and tremendously powerful source of information on measuring human movements and origin–destination-specific risks of infectious and non-infectious health issues. The high penetration rate of mobile phones across the globe provides an unprecedented opportunity to quantify human mobility and accurately estimate the health risks in travellers. Continued efforts are needed to establish the most promising uses of these data and technologies for travel health.
Keywords: Mobile phone, mHealth, population movement, connectivity, epidemiology, risk assessment, travel medicine
Introduction
Human populations are highly mobile in this modern world. The volume of worldwide population travel has expanded at an exceptional rate over the last few decades, with international tourist arrivals increasing from 674 million in 2000 to 1.3 billion in 2017 and expected to reach 1.8 billion by 2030.1,2 The increasing mobility of populations allows pathogens to move rapidly and far, making endemic or epidemic regions more connected to the rest of the world than at any time in history. The pathogens introduced by travellers may lead to secondary transmission and local outbreaks, as has been observed in severe acute respiratory syndrome, influenza, Ebola, Zika, yellow fever and measles, among others, or to the appearance of diseases such as malaria in non-endemic areas following migration for work or travel to visit friends and relatives.3–13 The spread of infectious diseases and their potential health risk in travellers has resulted in substantial concerns and challenges to global health systems and economies,14–17 with a need to place more emphasis on understanding population mobility, infectious disease connectivity and the individual health risk of travellers.
Human movements vary from short, periodically recurring travel to work or school, to rare international migration, but the ability to measure and monitor human mobility and its changing patterns across temporal (hour, day, week, month or year) and spatial (individual, house, community, city or nation) scales using traditional data sources has been limited. In resource-poor settings, demographic data collected via traditional censuses and surveys at subnational scales can often be lacking or outdated.18 However, many recent studies have highlighted how our understanding of human mobility across contexts can be significantly improved through quantitative analyses of positioning data from the huge population of mobile phone users.19,20 In 2017, there were already over 5 billion unique mobile subscribers globally, with a penetration rate of 66% of the global population, and the total number of mobile cellular subscriptions exceeds the world population at 7.79 billion.21,22 Moreover, mobile phone penetration is constantly rising and is predicted to nearly reach 6 billion users by 2025 with 5 billion connecting to internet.21,23 Even in the most resource-poor regions, such as Sub-Saharan Africa, the penetration rate of mobile cellular subscriptions has reached 75% of the population in 2017 (Figure 1), which is estimated to steadily increase to 85% by 2025.21,22 As mobile phones are now an integral part of modern life, mobile positioning data have become a novel and tremendously powerful sources of information on measuring human movements and pathogen spread.12,19,20,24–35
Figure 1.
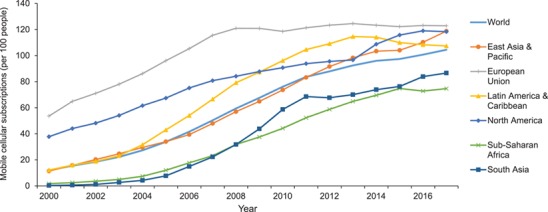
The penetration rate of mobile cellular subscriptions by region, 2000–2017 (Data source: The World Bank 22).
Quantifying how people move throughout their daily activities within the context of spatial risks enables a better understanding of environmental drivers of infectious disease, as well as chronic disease and other issues that involve long-term differences in exposure and mobility during travel.36–39 Recent advances in mobile health (mHealth) technology, together with the increasing penetration of smartphones and the internet, have facilitated the monitoring of traveller health behaviour and assessment of environmental risks, e.g. air pollution, and offer more reliable and more frequently updated ‘apps’ that consolidate travel health information from multiple sources in travel medicine research and practice.36,37,40–45
To facilitate a better understanding of the use of mobile phone data in travel health, here we review the research work aimed at measuring human movements, disease connectivity and health risk in travellers using mobile geopositioning data and mHealth technology. We searched PubMed for all related studies, published up until 5 March 2019 and in English, by the queries ‘(mobile phone OR cell phone OR smartphones OR call detail records OR mHealth OR eHealth) and (travel OR mobility OR movement OR connectivity) AND (disease OR health OR risk OR illness)’ in the title and abstract fields. The number of relevant publications resulting from these searches has grown rapidly over the last decade (Figure 2). We also searched the relevant reports and reviews published by the World Health Organization , and relevant references cited in publications were also reviewed. In this paper, first, we outline traditional and novel data sources for measuring population movements, highlighting the potential of mobile positioning data. Then, we sketch out approaches using human mobility data as a proxy for infectious disease connectivity. Further, the progress of mHealth for individual health risk monitoring and assessment in travel medicine research and public health practice is also summarized. Finally, we discuss the challenges of using mobile phone data and future directions for research in this area.
Figure 2.

The number of relevant publications searched in the PubMed as of 5 March 2019.
Measuring human mobility using mobile phone data
Traditionally, approaches to measuring human mobility rely on data from population and housing censuses, travel history surveys or cross-border and traffic surveys (Table 1).35,46,47 With technological advancements, however, increasing numbers of novel data sources have been used to measure human movements. Data from small-scale studies using personal Global Positioning System (GPS) trackers provide information on short-distance, circulatory movement and can directly inform activity spaces, the local areas within which people move or travel during the course of their daily activities.35,48,49 The trajectories of bank notes were traced to model human mobility over a long time period.50 Data of global air traffic and itineraries have also been analysed to measure internal and international connectivity and its impact on the spread of pathogens and vectors at city or airport level.3–8 Infrastructure data have also been used to define the connectivity between regions with the travel time as a proxy of human mobility and health accessibility.51,52 Moreover, earth observation data, such as satellite imagery of night-time lights can help inform on the changing densities of populations within cities over the course of a year.35,53 Mobile phone data are particularly promising for analysing travel-related phenomena on a scale previously impossible, providing a ‘big data’ approach to understanding human mobility and its changes.16–30 Two types of mobile-based positioning data that have so far been increasingly explored in travel-related studies are call detail records (CDRs) and mobile location history.
Table 1.
Traditional and innovative data sources for measuring human movements
| Data type | Description | Strengths | Challenges |
|---|---|---|---|
| Traditional data source | |||
| Population and housing census | Assembly of population and housing census data on place of residence 1–5 years ago. | Primary source for migration statistics; Global extent, consistent measure for complete population; Shows strong correlations to shorter scale domestic and international movements; Of value for global, continental, regional connectivity assessments. |
Long-term movements and permanent migrations only; Coarse spatial scale, bias to longer spatial scales; Lack of census data in countries affected by conflicts; Normally collected once every decade. |
| Travel history surveys | Travel log collected at health facilities, or through active surveillance/surveys. | Valuable data on relevant population pathogen movements; High value for measuring temporal trends in domestic and international travel; Important data for refining and validating models. |
Not collected in many settings; Sample a small proportion of population; Selection and recall biases; Difficult to access, inconsistent coverage/quality. |
| Cross-border and traffic surveys | Counting the number of cars and people that are crossing a border. | Cross-border movements; Measuring seasonal patterns by multiple cross-sectional surveys |
Difficult to obtain the origins and destination locations of travel; Difficult to capture the whole picture of movements in where there are porous borders. |
| Novel data source—mobile phone | |||
| CDRs | Individual-level records routinely collected by mobile phone operators for billing purposes, located to cell towers. | Cover large population of mobile users, potential to track hard-to-reach populations; Rich spatiotemporal data on individual, fine-scale movements; Capture long time series and seasonality with timely information; Of value for national-scale analyses, assessing population distributions, disease connectivity, and the parameterization of mobility models. |
Difficult to access and share; Ownership biases; Privacy issues and loss of information due to anonymization; Difficult to capture international movements. |
| Smartphone-based internet/social media location histories | Geolocated data on use of internet/social-media-connected devices, integrating online media content. | Timely, spatially precise positioning data on users’ locations; Long time series to capture seasonal domestic and international travel of users; Rapidly increasing penetration, potential to track hard-to-reach populations; Richness of information to understanding social connections and behaviours. |
Ownership and selection biases, changing sample over time; Data availability and loss of information due to anonymization; Privacy and ethical issues; Additional logistical, technical issues for analysis. |
| mHealth apps data | Individual travel history and health risk monitoring data collected by the mobile applications for mHealth. | Timely information on users’ location; High value in real-time individual travel patterns, environmental exposure monitoring and health risk assessment during travel; Improving healthcare access for travel medicine and public health interventions; Of value for the individual-level quantitative research on travel-related risk exposure and health outcome. |
Reliability of self-reported information; Selection bias and small sample size; Indicators for measuring the risk and exposure; Privacy and ethical issues. |
| Novel data source—other | |||
| Air travel data | Route aggregated statistics of flight passengers and air transportation network data. | Includes the origins, stops and destinations at airport or city level; Captures seasonality in long time series; High value in route-scale analyses, assessing international connectivity and modelling the risk of pathogen spread. |
Incomplete picture of population movements; Difficult to access travel itinerary data, and lacks demographic data; Coarse spatial scale and difficult to capture the origins and destinations beyond airports. |
| Infrastructure | Georeferenced data on transport links that form the basis of regional mobility. | Global coverage, consistent data; Useful proxy indicative of mobility, connectivity and healthcare accessibility. |
Based on an assumption that those travel times influence how population’s move; no measure of actual movements; Few time series; Validation. |
| Earth observation data | Data collected via remote-sensing technologies to monitor and assess the status of and changes in environments, e.g. satellite nightlight imagery | Proxy measures of population movements; Global coverage and high spatial resolution; High comparability and timely information. |
No actual movements with unknown origins and destinations; Methodological and technical issues; Continuity and validation. |
CDRs
CDRs are routinely collected by mobile phone operators for billing purposes.20,31 Each CDR contains an entry for each call or text made or received by any user with the subscriber identification module (SIM) card, together with the date and time of each communication and the tower that the communication was routed through within mobile phone networks.23,24 Every time an individual makes a call or sends a text via a short messaging service, it normally will be routed through the closest tower in the network. If these data are available in conjunction with geographic coordinates of relevant towers, then the tower-level location of each communication can be identified, and from this, the movement of individual mobile users between different calls can be derived. When mobile penetration rate is high in the population, or mobile users’ movements could be taken to represent the mobility pattern of the general population, spatially and temporarily explicit estimations of human mobility and densities at national scales can be derived from anonymized CDRs. Previous studies for Namibia, Bangladesh, Portugal and France have shown that estimates derived from CDRs can accurately replicate population counts and migration patterns from censuses.19,30,54–57 In these studies, each individual user was assigned a primary daily location based on either the most frequently used mobile phone tower or the most recently used mobile phone tower if a communication was not placed on the day. However, as the data on very infrequent mobile phone users may introduce noise in defining locations and population mobility, infrequent mobile phone users, e.g. a subscriber with 30 days or less worth of data for each year, could be filtered out to obtain more accurate estimates of population movements.58
Furthermore, these passive positioning data derived from CDRs can also be used to measure seasonal changes in subnational population numbers and produce density maps of human distribution changes over multiple timescales, providing more precise denominators for health metrics than static measures from censuses.20 However, CDRs cannot measure spatial movements finer than tower-level spatial resolution, and estimates are limited to domestic movements, as it is more difficult to obtain CDRs from operators in different countries to get estimates of international traveller flows. Nevertheless, mobile phone location history data are promising for measuring cross-border movements, as outlined below.
Mobile location history
When smartphones are connecting to the internet, various applications record user check-in locations with high spatial precision where various services are used.34,35,59,60 Location history data can be extracted from populations using mobile-based social media, e.g. Tweets, Facebook and WeChat, search engines, e.g. Google and Baidu, and other applications such as mHealth apps.34,35,56,57 These data are associated with a consolidated user account, allowing for recording of geographic coordinates that are passively recorded across all mobile devices that an individual has owned. Because location is identified using a combination of the phone’s internal GPS and connected WiFi devices and cell towers, these data are as spatially refined as GPS tracker data and can span years. Moreover, the passively collected nature of these data avoids many known biases from compliance issues in studies that use GPS trackers and avoids recall bias found in self-reported travel history data.35 However, the biases may still exist, as the smartphone penetration is still very low in low-income countries. The opt-out nature makes them sensitive and careful controls and ethics clearance need to be in place before accessing these data.
The high resolution of mobile-based location history data, however, means they are one of few viable sources of information for better understanding and mapping these differences towards mapping activity spaces and travel routes across long periods and countries. For instance, studies using Google location history and Twitter geotag data, being collected in an opt-out, passive fashion for users, demonstrated that mobile location history can be a reliable source to capture rich features of mobility movements within and between cities and even between countries.35,59 Further, based on CDRs and social media location history data from different nations, a variety of individual and collective mobility patterns can be accurately predicted by using a universal model at diverse spatial scales.34 Therefore, mobile phone data provide an unprecedented opportunity to understand global and seasonal dynamics associated with contemporary human mobility.
Mobile-derived human movements and disease connectivity
Based on the enormously detailed travel itineraries that mobile phone data can produce, patterns of pathogen spread through space and time can be simulated and measured using individual human movement trajectories combined with existing knowledge on pathogens. Though some pathogens are transmitted via vectors or animal hosts, most infectious diseases rely on human movement for wide-scale spread, and even for those spread by vectors, human movement plays a substantial role in transmission dynamics.61,62 To measure the risk of infectious disease spread via travellers by various modes of transportation, a variety of individual or metapopulation-based statistical and mathematical models have been used to estimate the time, origins, destinations, probability and magnitude of pathogen importation and onward transmission from epidemic or endemic areas (Table S1 available as Supplementary data at JTM online). To date, mobile-derived human mobility, especially using CDRs, have been used to explore the transmission of malaria,12,31,55 dengue,29 cholera,63 measles,64 rubella,28 Ebola,65,66 and HIV infection.67
Taking malaria as an example, we illustrate how spatiotemporally explicit mobility derived from mobile positioning data has been used to define malaria connectivity and inform interventions. Although malaria is a mosquito-borne disease, human travel-mediated transmission on spatial scales that exceed the limits of mosquito dispersal has been undermining the success of malaria control and elimination programmes that have been implemented in many countries.10–12,68 The early detection and treatment of imported parasites due to human travel become high priorities for informing malaria elimination policy. A variety of models, integrating CDR-derived human mobility and malaria epidemiological and entomological data, have investigated the dynamics of human carriers to identify importation routes and locate transmission foci that contribute to malaria epidemiology for endemic countries in sub-Saharan Africa, Mesoamerica and South-East Asia.12,26,31,46,55,56,69,70 In these studies, spatial clusters of primary sinks and sources of parasite importation and their seasonal changes were disentangled, with the estimates of net export and import of travellers and infection risks by region. Using near real-time mobile-derived mobility data, this evidence can be rapidly updated and used to identify where active surveillance for both local and imported cases should be increased, which regions would benefit from coordinating efforts and how spatially progressive elimination plans can be designed.55 To achieve local or national malaria control or elimination goals, even global malaria eradication, these approaches and findings have significant implications for targeting interventions at source locations to maximally reduce the number of cases exported to other regions, as well as providing health advice and healthcare for the travellers visiting to or returning from source regions.31,55,56
It is noteworthy that models parametrized by various mobility data sources and spatiotemporal resolutions can generate divergent outcomes.32 Based on a spatially structured reaction–diffusion metapopulation model where the whole population is divided into sub-populations connected by mobility fluxes, a previous study found that the adequacy of mobile phone data for infectious disease models becomes higher when epidemics spread between highly connected and heavily populated locations, such as large urban areas.32 Furthermore, seasonal and geographic spread of pathogens depends on connectivity fluctuations through the year, because seasonal travel and directional asymmetries could be across a spectrum from rural nomadic populations to highly urbanized communities, with combined effects of school terms and holidays.33 These variations in travel impact how fast communities are likely to be reached by an introduced pathogen. In addition to measuring the risk of pathogen spread, mobile-derived population movement data also play an important role in understanding the relationship between geographic isolation and health disparities by measuring the accessibility of health resources,71 identifying vulnerable and high-risk populations in vaccination campaigns28,64 and evaluating interventions, e.g. screen/travel restrictions for epidemic containment.66
mHealth applications and risk assessment in travellers
Because mobile positioning data are opt-out and are passively collected as users carry their smartphones, the recent rise of mHealth methodology, e.g. smartphone applications, offers new opportunities to capture the full range of health risks during travel in real time, from travel location, physical activity, health symptoms and sleep to environmental hazards such as extreme weather conditions and air pollution.42 For instance, mHealth has been used for dynamic assessment of exposure to air pollution during travel.36,37
Research on travellers using mHealth applications offers many advantages in improving risk assessment over prior methodologies such as pre- and post-travel risk questionnaires. Using mHealth applications to assess risk in travellers daily during their trips minimizes the risk of recall bias that is an inherent problem in administering health questionnaires weeks or months after the event actually occurred during the trip. In addition, novel publicly available data sources (e.g. weather patterns, social media data, traffic patterns) can be integrated with daily self-reported data on symptoms and risk behaviours in order to create a complex picture of how environmental factors, health behaviours and personal risk factors interact during travel to create health outcomes. The ability to create a real-time map of traveller health events such as traffic accidents or infectious disease transmission has the potential to improve medical advice given prior to travel and enable a faster public health response to major events. Finally, prior research suggests that participants may be more likely to share sensitive or socially unacceptable information on an online form, improving understanding of rates of risky behaviours during travel.72
Farnham et al.42–45 used mHealth technology to identify the range of health outcomes during travel using real-time monitoring and daily reporting of health behaviours and outcomes and identify traveller subgroups who may benefit from more targeted advice before and during travel. In this mHealth-based study, non-infectious disease-related health issues were commonly found in travellers, despite being largely unaddressed in traditional travel medicine research; in addition, clear patterns of traveller behaviour and health outcomes emerged, suggesting that subgroups of travellers exist for whom specialized medical advice is needed. These results suggest a substantial potential for improving evidence-based travel medicine advice. Rodriguez-Valero et al. developed an mHealth application that tracked incidence of disease among travellers in real time and provide telemedicine care to ill travellers.73 This study suggests the potential of mHealth for detecting and responding to traveller health issues in real time, providing a two-way monitoring and response application. These studies also show that the use of a smartphone app to collect health information is technically feasible and acceptable among a traveller population, allowing researchers to minimize recall bias, greatly increases the quality and quantity of data collected during travel and even respond to emergent health issues. Therefore, inferences from data monitored by mHealth apps can yield important insights for health risk assessment that were previously impossible in travel medicine. Moreover, mHealth data from a smartphone application integrated with streaming data sources have supported healthcare delivery, laboratory diagnostic tests and data collection and allowed for the operation of a national-level disease reporting and health surveillance with fine geolocated data at a low cost.74–79
Discussion
It has long been appreciated that population movements drive the transmission patterns and intensity of many infectious diseases. Understanding the changing patterns of human travel over time is critical for tailoring and updating evidence-driven surveillance and strategies to address travel-related health issues.80 In this study, although a systematic literature review approach was not performed by using a comprehensive search strategy to collate all relevant empirical evidence, we still found the highly detailed mobile positioning data undoubtedly provide one of the most powerful, scalable and real-time data sets on human mobility available, yielding insight into individual’s movement trajectories across various time and space scales. The advantages of using this innovative data source for travel-related aspects are linked to its potential to overcome many limitations of traditional data sources and other approaches. Moreover, the recent advance of mHealth technology, together with mobile positioning data, shows great potential for innovation in travel medicine to monitor and assess real-time health risks for individuals during travel.32,42 However, there are a number of challenges that must be met to ensure the success of using mobile-derived human movement data.
First, there are always confidentiality and ethical issues in using mobile positioning data automatically generated by individuals. This makes the location data held by individual, private or state actors logistically difficult to be accessed, as it is limited by the telecom, internet and data-protection regulations in many countries.23,81 To facilitate data sharing and avoid privacy and commercial concerns, appropriate safeguards should be in place to ensure data security, with data anonymization and aggregation taking place on separate servers hosted by operators behind operators’ firewall before sharing.82 As the public health usefulness of these data continues to be demonstrated, mobile phone operators and technology companies are becoming more receptive to providing these anonymous data for research and public health purposes. Currently, however, access to these data has primarily been through negotiated agreements between operators and research groups. To make outputs from CDRs more accessible, the initiatives like the Open Algorithms project and the FlowKit, a CDR analytics toolset developed by the Flowminder Foundation and the WorldPop research group at the University of Southampton, aim to unlock the potential of private data for public good in a privacy-conscientious, scalable, socially and economically sustainable manner.83,84 Moreover, it is necessary to create adequate legislative and regulatory frameworks to safeguard confidentiality of the information and ensure the ethical use of data for development projects.81
Second, as mobile phone or social media users only represent a proportion of the whole population, the interpretation of mobility estimates must account for biases introduced by heterogeneous use of mobile phones, social media platforms and the internet.81 It is often assumed that mobile phones are sufficiently widespread that users represent a true random sample of a population. However, mobile users are not necessarily representative of the population at large, as the differences in the use of mobile devices, social media platforms and internet are still significant by level of socioeconomic development, sex, age and urban/rural areas. In many low-resource settings, for instance, the users are commonly disproportionately male, educated and from larger households, compared with the general population.20,85,86 Moreover, the behaviours of using mobile phones and social media as well as the possibility that individuals own multiple SIM cards or mobiles affect the ability to produce accurate and representative estimates of population mobility.20,23,25 Though these potential biases are decreasing as mobile phone ownership rises,20 a prerequisite for these studies is still to understand the demographic features of mobile phone owners or users of social media and mHealth apps. For instance, household surveys such as the Demographic and Health Surveys programme can provide information on mobile phone usage and ownership patterns and allow assessment of spatial differences that could bias results.20
Third, given the increasing volume of these huge, complex and ‘noisy’ mobile data as well as the spatiotemporal heterogeneity of disease transmission,81 another major challenge is the methodological difficulties of measuring transmission risk of infectious diseases at appropriate spatial and temporal spatial scales. Regarding the diverse biological aspects of pathogens, population immunity and entomology and ecology of vectors, the complexity can be very different in the inference of the arrivals and spread risk of different pathogens. For instance, for pathogens with sufficiently high transmissibility, higher transmissibility could result in more rapid spatial spread. However, for pathogens with weak transmission, both seasonal patterns and the impact of distance might be obscured, and many locations might not be affected.28,29,33 Moreover, modelling results are also sensitive to the choices in the parametrization of population movements, considering the variety of individual travel activities and data sources.23,32 Understanding how modelling results are affected by limitations inherent to the mobile phone data will help to increase the predictive capacity of models based on such novel data sources and facilitate the interpretation in uncertainties of travel-mediate epidemic modelling and the sensible use of big data for decision-making.23,81,87,88
Despite inherent biases in mobile phone data, the progress of analytic tools for adjusting estimates and increasing penetration rate of mobile devices and internet-based platforms in populations may diminish the impact of these biases on measures of human movements.71,85,86 More research is needed to establish the most promising uses of these data for travel health, and the combination of information extracted from traditional and innovative data sources are beginning to be produced and yield a proof of concept and road map for future studies on individual’s risk assessment in travel medicine.43–45 For instance, phylogeographic analyses can relate travel and epidemiological dynamics by integrating mobile data with expanding genetic data.
However, given the mobile location data being collected every second across the world, as well as the upcoming 5G networks and advances of artificial intelligence technology, these digital records provide an unprecedented opportunity to quantify human mobility and accurately estimate the health risks through the sheer numbers of individuals reflected in the data streams.23,81
Author contributions
Shengjie Lai, PhD: conception and study design, literature search and writing
Andrea Farnham, PhD: literature search, technical editing and critical revision and writing
Nick W Ruktanonchai, PhD: technical editing, critical revision and writing
Andrew J Tatem, PhD: conception and study design, technical editing and critical revision and writing
Funding
S.L. is supported by the grants from the National Natural Science Fund (81773498), the Ministry of Science and Technology of China (2016ZX10004222-009) and the Program of Shanghai Academic/Technology Research Leader (18XD1400300). A.J.T. is supported by funding from the Bill & Melinda Gates Foundation (OPP1106427, 1032350, OPP1134076, OPP1094793), the Clinton Health Access Initiative, the UK Department for International Development (DFID) and the Wellcome Trust (106866/Z/15/Z, 204613/Z/16/Z). The study sponsors had no role in study design or the collection, analysis and interpretation of data and the writing of the article and the decision to submit it for publication.
Conflict of interest: None declared.
Supplementary Material
Reference
- 1. World Tourism Organization UNWTO Tourism Highlights (2018 Edition). https://www.e-unwto.org/doi/pdf/10.18111/9789284419876(17 January 2019, date last accessed).
- 2. Glaesser D, Kester J, Paulose H et al. Global travel patterns: an overview. J Travel Med 2017; 24:tax007. [DOI] [PubMed] [Google Scholar]
- 3. Bogoch II, Brady OJ, Kraemer MUG et al. Potential for Zika virus introduction and transmission in resource-limited countries in Africa and the Asia-Pacific region: a modelling study. Lancet Infect Dis 2016; 16:1237–1245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bogoch II, Creatore MI, Cetron MS et al. Assessment of the potential for international dissemination of Ebola virus via commercial air travel during the 2014 west African outbreak. Lancet 2015; 385:29–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Brockmann D, Helbing D. The hidden geometry of complex, network-driven contagion phenomena. Science 2013; 342:1337–1342. [DOI] [PubMed] [Google Scholar]
- 6. Lai S, Johansson MA, Yin W et al. Seasonal and interannual risks of dengue introduction from South-East Asia into China, 2005-2015. PLoS Negl Trop Dis 2018; 12:e0006743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Tatem AJ, Hay SI, Rogers DJ. Global traffic and disease vector dispersal. Proc Natl Acad Sci U S A 2006; 103:6242–6247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wang L, Wu JT. Characterizing the dynamics underlying global spread of epidemics. Nat Commun 2018; 9:218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kraemer MUG, Faria NR, Reiner RC Jr et al. Spread of yellow fever virus outbreak in Angola and the Democratic Republic of the Congo 2015-16: a modelling study. Lancet Infect Dis 2017; 17:330–338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Lai S, Li Z, Wardrop NA et al. Malaria in China, 2011-2015: an observational study. Bull World Health Organ 2017; 95:564–573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Tatem AJ, Jia P, Ordanovich D et al. The geography of imported malaria to non-endemic countries: a meta-analysis of nationally reported statistics. Lancet Infect Dis 2017; 17:98–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ihantamalala FA, Herbreteau V, Rakotoarimanana FMJ et al. Estimating sources and sinks of malaria parasites in Madagascar. Nat Commun 2018; 9:3897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Fang LQ, Sun Y, Zhao GP et al. Travel-related infections in mainland China, 2014-16: an active surveillance study. Lancet Public Health 2018; 3:e385–e394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Gulland A. Zika virus is a global public health emergency, declares WHO. BMJ 2016; 352:i657. [DOI] [PubMed] [Google Scholar]
- 15. Sands P, El Turabi A, Saynisch PA et al. Assessment of economic vulnerability to infectious disease crises. Lancet 2016; 388:2443–2448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Soghaier MA, Saeed KMI, Zaman KK. Public Health Emergency of International Concern (PHEIC) has declared twice in 2014; polio and Ebola at the top. AIMS Public Health 2015; 2:218–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Abubakar I, Aldridge RW, Devakumar D et al. The UCL-Lancet Commission on Migration and Health: the health of a world on the move. Lancet 2018; 392:2606–2654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Wardrop NA, Jochem WC, Bird TJ et al. Spatially disaggregated population estimates in the absence of national population and housing census data. Proc Natl Acad Sci U S A 2018; 115:3529–3537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Deville P, Linard C, Martin S et al. Dynamic population mapping using mobile phone data. Proc Natl Acad Sci U S A 2014; 111:15888–15893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Zu Erbach-Schoenberg E, Alegana VA, Sorichetta A et al. Dynamic denominators: the impact of seasonally varying population numbers on disease incidence estimates. Popul Health Metr 2016; 14:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. The GSM Association The Mobile Economy 2018 https://www.gsma.com/mobileeconomy/ (30 July 2018, date last accessed).
- 22. World Bank Mobile cellular subscriptions (per 100 people) https://data.worldbank.org/indicator/IT.CEL.SETS.P2 (17 January 2019, date last accessed).
- 23. Wesolowski A, Buckee CO, Engo-Monsen K et al. Connecting mobility to infectious diseases: the promise and limits of mobile phone data. J Infect Dis 2016; 214:S414–S420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Tatem AJ, Qiu Y, Smith DL et al. The use of mobile phone data for the estimation of the travel patterns and imported Plasmodium falciparum rates among Zanzibar residents. Malar J 2009; 8:287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Lu X, Bengtsson L, Holme P. Predictability of population displacement after the 2010 Haiti earthquake. Proc Natl Acad Sci U S A 2012; 109:11576–11581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Wesolowski A, Eagle N, Tatem AJ et al. Quantifying the impact of human mobility on malaria. Science 2012; 338:267–270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Bengtsson L, Gaudart J, Lu X et al. Using mobile phone data to predict the spatial spread of cholera. Sci Rep 2015; 5:8923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Wesolowski A, Metcalf CJE, Eagle N et al. Quantifying seasonal population fluxes driving rubella transmission dynamics using mobile phone data. Proc Natl Acad Sci U S A 2015; 112:11114–11119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Wesolowski A, Qureshi T, Boni MF et al. Impact of human mobility on the emergence of dengue epidemics in Pakistan. Proc Natl Acad Sci U S A 2015; 112:11887–11892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Lu X, Wrathall DJ, Sundsoy PR et al. Unveiling hidden migration and mobility patterns in climate stressed regions: a longitudinal study of six million anonymous mobile phone users in Bangladesh. Glob Environ Chang 2016; 38:1–7. [Google Scholar]
- 31. Ruktanonchai NW, DeLeenheer P, Tatem AJ et al. Identifying malaria transmission foci for elimination using human mobility data. PLoS Comput Biol 2016; 12:e1004846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Panigutti C, Tizzoni M, Bajardi P et al. Assessing the use of mobile phone data to describe recurrent mobility patterns in spatial epidemic models. R Soc Open Sci 2017; 4:160950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Wesolowski A, Zu Erbach-Schoenberg E, Tatem AJ et al. Multinational patterns of seasonal asymmetry in human movement influence infectious disease dynamics. Nat Commun 2017; 8:2069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Yan XY, Wang WX, Gao ZY et al. Universal model of individual and population mobility on diverse spatial scales. Nat Commun 2017; 8:1639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Ruktanonchai NW, Ruktanonchai CW, Floyd JR et al. Using Google Location History data to quantify fine-scale human mobility. Int J Health Geogr 2018; 17:28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Gately CK, Hutyra LR, Peterson S et al. Urban emissions hotspots: quantifying vehicle congestion and air pollution using mobile phone GPS data. Environ Pollut 2017; 229:496–504. [DOI] [PubMed] [Google Scholar]
- 37. Dewulf B, Neutens T, Lefebvre W et al. Dynamic assessment of exposure to air pollution using mobile phone data. Int J Health Geogr 2016; 15:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Nyhan MM, Kloog I, Britter R et al. Quantifying population exposure to air pollution using individual mobility patterns inferred from mobile phone data. J Expo Sci Environ Epidemiol 2019; 29:238–247. [DOI] [PubMed] [Google Scholar]
- 39. Nyhan M, Grauwin S, Britter R et al. “Exposure track”—the impact of mobile-device-based mobility patterns on quantifying population exposure to air pollution. Environ Sci Technol 2016; 50:9671–9681. [DOI] [PubMed] [Google Scholar]
- 40. Flaherty GT. Research on the move: the potential applications of mobile health technology in travel medicine. J Travel Med 2016; 23:taw061. [DOI] [PubMed] [Google Scholar]
- 41. Seed SM, Khov SL, Binguad FS et al. Identification and review of mobile applications for travel medicine practitioners and patients. J Travel Med 2016; 23:taw034. [DOI] [PubMed] [Google Scholar]
- 42. Farnham A, Blanke U, Stone E et al. Travel medicine and mHealth technology: a study using smartphones to collect health data during travel. J Travel Med 2016; 23:taw056. [DOI] [PubMed] [Google Scholar]
- 43. Farnham A, Furrer R, Blanke U et al. The quantified self during travel: mapping health in a prospective cohort of travellers. J Travel Med 2017; 24:tax050. [DOI] [PubMed] [Google Scholar]
- 44. Farnham A, Roosli M, Blanke U et al. Streaming data from a smartphone application: a new approach to mapping health during travel. Travel Med Infect Dis 2018; 21:36–42. [DOI] [PubMed] [Google Scholar]
- 45. Farnham A, Ziegler S, Blanke U et al. Does the DOSPERT scale predict risk-taking behaviour during travel? A study using smartphones. J Travel Med 2018; 25:tay064. [DOI] [PubMed] [Google Scholar]
- 46. Buckee CO, Wesolowski A, Eagle NN et al. Mobile phones and malaria: modeling human and parasite travel. Travel Med Infect Dis 2013; 11:15–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Brucker DL, Rollins NG. Trips to medical care among persons with disabilities: evidence from the 2009 National Household Travel Survey. Disabil Health J 2016; 9:539–543. [DOI] [PubMed] [Google Scholar]
- 48. Paz-Soldan VA, Reiner RC Jr, Morrison AC et al. Strengths and weaknesses of Global Positioning System (GPS) data-loggers and semi-structured interviews for capturing fine-scale human mobility: findings from Iquitos, Peru. PLoS Negl Trop Dis 2014; 8:e2888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Vazquez-Prokopec GM, Bisanzio D, Stoddard ST et al. Using GPS technology to quantify human mobility, dynamic contacts and infectious disease dynamics in a resource-poor urban environment. PLoS One 2013; 8:e58802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Brockmann D, Hufnagel L, Geisel T. The scaling laws of human travel. Nature 2006; 439:462–465. [DOI] [PubMed] [Google Scholar]
- 51. Alegana VA, Maina J, Ouma PO et al. National and sub-national variation in patterns of febrile case management in sub-Saharan Africa. Nat Commun 2018; 9:4994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Strano E, Viana MP, Sorichetta A et al. Mapping road network communities for guiding disease surveillance and control strategies. Sci Rep 2018; 8:4744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Bharti N, Lu X, Bengtsson L et al. Remotely measuring populations during a crisis by overlaying two data sources. Int Health 2015; 7:90–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Tatem AJ. Mapping the denominator: spatial demography in the measurement of progress. Int Health 2014; 6:153–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Tatem AJ, Huang Z, Narib C et al. Integrating rapid risk mapping and mobile phone call record data for strategic malaria elimination planning. Malar J 2014; 13:52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Ruktanonchai NW, Bhavnani D, Sorichetta A et al. Census-derived migration data as a tool for informing malaria elimination policy. Malar J 2016; 15:273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Wesolows ki A, Buckee CO, Pindolia DK et al. The use of census migration data to approximate human movement patterns across temporal scales. PLoS One 2013; 8:e52971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Lai S, Zu Erbach-Schoenberg E, Pezzulo C et al. Exploring the use of mobile phone data for national migration statistics. Palgrave Communications 2019; 5. doi: 10.1057/s41599-019-0242-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Jurdak R, Zhao K, Liu J et al. Understanding human mobility from twitter. PLoS One 2015; 10:e0131469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Burton SH, Tanner KW, Giraud-Carrier CG et al. "Right time, right place" health communication on Twitter: value and accuracy of location information. J Med Internet Res 2012; 14:e156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Tatem AJ, Rogers DJ, Hay SI. Global transport networks and infectious disease spread. Adv Parasitol 2006; 62:293–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Mier YT-RL, Tatem AJ, Johansson MA. Mosquitoes on a plane: disinsection will not stop the spread of vector-borne pathogens, a simulation study. PLoS Negl Trop Dis 2017; 11:e0005683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Finger F, Genolet T, Mari L et al. Mobile phone data highlights the role of mass gatherings in the spreading of cholera outbreaks. Proc Natl Acad Sci U S A 2016; 113:6421–6426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Wesolowski A, Winter A, Tatem AJ et al. Measles outbreak risk in Pakistan: exploring the potential of combining vaccination coverage and incidence data with novel data-streams to strengthen control. Epidemiol Infect 2018; 146:1575–1583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Wesolowski A, Buckee CO, Bengtsson L et al. Commentary: containing the ebola outbreak—the potential and challenge of mobile network data. PLoS Curr 2014; 6:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Peak CM, Wesolowski A, Zu Erbach-Schoenberg E et al. Population mobility reductions associated with travel restrictions during the Ebola epidemic in Sierra Leone: use of mobile phone data. Int J Epidemiol 2018; 47:1562–1570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Isdory A, Mureithi EW, Sumpter DJ. The impact of human mobility on HIV transmission in Kenya. PLoS One 2015; 10:e0142805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. World Health Organization World Malaria Report 2018 https://www.who.int/malaria/publications/world-malaria-report-2018/report/en/(25 November 2018, date last accessed).
- 69. Sorichetta A, Bird TJ, Ruktanonchai NW et al. Mapping internal connectivity through human migration in malaria endemic countries. Sci Data 2016; 3:160066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Tompkins AM, McCreesh N. Migration statistics relevant for malaria transmission in Senegal derived from mobile phone data and used in an agent-based migration model. Geospat Health 2016; 11:408. [DOI] [PubMed] [Google Scholar]
- 71. Wesolowski A, O'Meara WP, Tatem AJ et al. Quantifying the impact of accessibility on preventive healthcare in sub-Saharan Africa using mobile phone data. Epidemiology 2015; 26:223–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Burkill S, Copas A, Couper MP et al. Using the web to collect data on sensitive behaviours: a study looking at mode effects on the British National Survey of sexual attitudes and lifestyles. PLoS One 2016; 11:e0147983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Rodriguez-Valero N, Carbayo MJL, Sanchez DC et al. Real-time incidence of travel-related symptoms through a smartphone-based app remote monitoring system: a pilot study. J Travel Med 2018; 25:tay034. [DOI] [PubMed] [Google Scholar]
- 74. Wang LJ, Naude N, Demissie M et al. Analytical validation of an ultra low-cost mobile phone microplate reader for infectious disease testing. Clin Chim Acta 2018; 482:21–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Arie S. Can mobile phones transform healthcare in low and middle income countries? BMJ 2015; 350:h1975. [DOI] [PubMed] [Google Scholar]
- 76. Hotez PJ, Biritwum NK, Fenwick A et al. Ghana: accelerating neglected tropical disease control in a setting of economic development. PLoS Negl Trop Dis 2019; 13:e0007005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Hurt K, Walker RJ, Campbell JA et al. mHealth interventions in low and middle-income countries: a systematic review. Glob J Health Sci 2016; 8:54429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Zaidi SM, Labrique AB, Khowaja S et al. Geographic variation in access to dog-bite care in Pakistan and risk of dog-bite exposure in Karachi: prospective surveillance using a low-cost mobile phone system. PLoS Negl Trop Dis 2013; 7:e2574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Brinkel J, Kramer A, Krumkamp R et al. Mobile phone-based mHealth approaches for public health surveillance in sub-Saharan Africa: a systematic review. Int J Environ Res Public Health 2014; 11:11559–11582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Freedman DO, Chen LH, Kozarsky PE. Medical considerations before international travel. N Engl J Med 2016; 375:247–260. [DOI] [PubMed] [Google Scholar]
- 81. IOM’s Global Migration Data Analysis Centre (GMDAC) Big data, migration and human mobility https://migrationdataportal.org/themes/big-data (16 January 2019, date last accessed).
- 82. The GSM Association GSMA guidelines on the protection of privacy in the use of mobile phone data for responding to the Ebola outbreak 2014. https://www.gsma.com/mobilefordevelopment/wp-content/uploads/2014/11/GSMA-Guidelines-on-protecting-privacy-in-the-use-of-mobile-phone-data-for-responding-to-the-Ebola-outbreak-_October-2014.pdf(9 January 2019, date last accessed).
- 83. de Montjoye YA, Gambs S, Blondel V et al. On the privacy-conscientious use of mobile phone data. Sci Data 2018; 5:180286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Flowminder Foundation Flowminder and the Digital Impact Alliance announce FlowKit: a free and open analytics toolkit for Call Details Records 2018. http://www.flowminder.org/news/flowminder-and-the-digital-impact-alliance-announce-flowkit-a-free-and-open-analytics-toolkit-for-call-details-records (10 January 2019, date last accessed).
- 85. Wesolowski A, Eagle N, Noor AM et al. Heterogeneous mobile phone ownership and usage patterns in Kenya. PLoS One 2012; 7:e35319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Wesolowski A, Eagle N, Noor AM et al. The impact of biases in mobile phone ownership on estimates of human mobility. J R Soc Interface 2013; 10:20120986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. International Organization for Migration Data Bulletin—Big data and migration. 2018https://publications.iom.int/system/files/pdf/issue_5_big_data_and_migration.pdf(23 June 2018, date last accessed).
- 88. Tizzoni M, Bajardi P, Decuyper A et al. On the use of human mobility proxies for modeling epidemics. PLoS Comput Biol 2014; 10:e1003716. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.