

Abstract
Background
Halitosis or bad breath is a symptom in which a noticeably unpleasant breath odour is present due to an underlying oral or systemic disease. 50% to 60% of the world population has experienced this problem which can lead to social stigma and loss of self‐confidence. Multiple interventions have been tried to control halitosis ranging from mouthwashes and toothpastes to lasers. This new Cochrane Review incorporates Cochrane Reviews previously published on tongue scraping and mouthrinses for halitosis.
Objectives
The objectives of this review were to assess the effects of various interventions used to control halitosis due to oral diseases only. We excluded studies including patients with halitosis secondary to systemic disease and halitosis‐masking interventions.
Search methods
Cochrane Oral Health's Information Specialist searched the following databases: Cochrane Oral Health's Trials Register (to 8 April 2019), the Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 3) in the Cochrane Library (searched 8 April 2019), MEDLINE Ovid (1946 to 8 April 2019), and Embase Ovid (1980 to 8 April 2019). We also searched LILACS BIREME (1982 to 19 April 2019), the National Database of Indian Medical Journals (1985 to 19 April 2019), OpenGrey (1992 to 19 April 2019), and CINAHL EBSCO (1937 to 19 April 2019). The US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (8 April 2019), the World Health Organization International Clinical Trials Registry Platform (8 April 2019), the ISRCTN Registry (19 April 2019), the Clinical Trials Registry ‐ India (19 April 2019), were searched for ongoing trials. We also searched the cross‐references of included studies and systematic reviews published on the topic. No restrictions were placed on the language or date of publication when searching the electronic databases.
Selection criteria
We included randomised controlled trials (RCTs) which involved adults over the age of 16, and any intervention for managing halitosis compared to another or placebo, or no intervention. The active interventions or controls were administered over a minimum of one week and with no upper time limit. We excluded quasi‐randomised trials, trials comparing the results for less than one week follow‐up, and studies including advanced periodontitis.
Data collection and analysis
Two pairs of review authors independently selected trials, extracted data, and assessed risk of bias. We estimated mean differences (MDs) for continuous data, with 95% confidence intervals (CIs). We assessed the certainty of the evidence using the GRADE approach.
Main results
We included 44 trials in the review with 1809 participants comparing an intervention with a placebo or a control. The age of participants ranged from 17 to 77 years. Most of the trials reported on short‐term follow‐up (ranging from one week to four weeks). Only one trial reported long‐term follow‐up (three months).
Three studies were at low overall risk of bias, 16 at high overall risk of bias, and the remaining 25 at unclear overall risk of bias.
We compared different types of interventions which were categorised as mechanical debridement, chewing gums, systemic deodorising agents, topical agents, toothpastes, mouthrinse/mouthwash, tablets, and combination methods.
Mechanical debridement: for mechanical tongue cleaning versus no tongue cleaning, the evidence was very uncertain for the outcome dentist‐reported organoleptic test (OLT) scores (MD ‐0.20, 95% CI ‐0.34 to ‐0.07; 2 trials, 46 participants; very low‐certainty evidence). No data were reported for patient‐reported OLT score or adverse events.
Chewing gums: for 0.6% eucalyptus chewing gum versus placebo chewing gum, the evidence was very uncertain for the outcome dentist‐reported OLT scores (MD ‐0.10, 95% CI ‐0.31 to 0.11; 1 trial, 65 participants; very low‐certainty evidence). No data were reported for patient‐reported OLT score or adverse events.
Systemic deodorising agents: for 1000 mg champignon versus placebo, the evidence was very uncertain for the outcome patient‐reported visual analogue scale (VAS) scores (MD ‐1.07, 95% CI ‐14.51 to 12.37; 1 trial, 40 participants; very low‐certainty evidence). No data were reported for dentist‐reported OLT score or adverse events.
Topical agents: for hinokitiol gel versus placebo gel, the evidence was very uncertain for the outcome dentist‐reported OLT scores (MD ‐0.27, 95% CI ‐1.26 to 0.72; 1 trial, 18 participants; very low‐certainty evidence). No data were reported for patient‐reported OLT score or adverse events.
Toothpastes: for 0.3% triclosan toothpaste versus control toothpaste, the evidence was very uncertain for the outcome dentist‐reported OLT scores (MD ‐3.48, 95% CI ‐3.77 to ‐3.19; 1 trial, 81 participants; very low‐certainty evidence). No data were reported for patient‐reported OLT score or adverse events.
Mouthrinse/mouthwash: for mouthwash containing chlorhexidine and zinc acetate versus placebo mouthwash, the evidence was very uncertain for the outcome dentist‐reported OLT scores (MD ‐0.20, 95% CI ‐0.58 to 0.18; 1 trial, 44 participants; very low‐certainty evidence). No data were reported for patient‐reported OLT score or adverse events.
Tablets: no data were reported on key outcomes for this comparison.
Combination methods: for brushing plus cetylpyridium mouthwash versus brushing, the evidence was uncertain for the outcome dentist‐reported OLT scores (MD ‐0.48, 95% CI ‐0.72 to ‐0.24; 1 trial, 70 participants; low‐certainty evidence). No data were reported for patient‐reported OLT score or adverse events.
Authors' conclusions
We found low‐ to very low‐certainty evidence to support the effectiveness of interventions for managing halitosis compared to placebo or control for the OLT and patient‐reported outcomes tested. We were unable to draw any conclusions regarding the superiority of any intervention or concentration. Well‐planned RCTs need to be conducted by standardising the interventions and concentrations.
Keywords: Adolescent, Adult, Aged, Female, Humans, Male, Middle Aged, Young Adult, Chewing Gum, Chlorhexidine, Chlorhexidine/therapeutic use, Dental Scaling, Halitosis, Halitosis/therapy, Mouthwashes, Mouthwashes/therapeutic use, Oral Health, Oral Hygiene, Oral Hygiene/methods, Randomized Controlled Trials as Topic, Tongue, Tongue/microbiology, Toothbrushing, Toothbrushing/methods, Toothpastes
Plain language summary
Interventions for managing bad breath
Review question
With this Cochrane Review we tried to find out the best way to control bad breath, also called halitosis, due to a disease within the mouth in adults.
Background
Bad breath or halitosis is caused by too much bacteria or small food parts left inside the mouth, most commonly at the back of the tongue. It can be a sign of a disease within the mouth or other body diseases. People with bad breath can have low self‐esteem and feel embarrassed. It can affect their personal relationships and work. In this review, we looked at treatments for bad breath due to a disease within the mouth and at treatments that aim to control not just mask bad breath.
Study characteristics
This review is up‐to‐date as of 8 April 2019. The review includes 44 studies involving 1809 people who were 17 to 77 years old. The review compared an intervention with another intervention, a placebo or a control. It looked at eight different ways to control bad breath: mechanical cleaning (e.g. tongue cleaners and toothbrushes), chewing gums, systemic deodorising agents (e.g. mushroom extract that you eat), topical agents (e.g. gel that you apply), toothpastes, mouthrinse/mouthwash, tablets, and combination of different treatments.
Key results
The evidence was very uncertain for mechanical tongue cleaning versus no tongue cleaning, 0.6% eucalyptus chewing gum versus placebo chewing gum, 1000 mg mushroom extract versus placebo, hinokitiol gel versus placebo gel, 0.3% triclosan toothpaste versus control toothpaste, mouthwash containing chlorhexidine and zinc acetate versus placebo mouthwash, and brushing plus cetylpyridium mouthwash versus brushing.
Harmful effects of the different interventions were not reported or were not important.
Certainty of the evidence
The level of certainty we have in these findings is low to very low. This was due mainly to risk of bias and the small number of people studied in the included trials.
Conclusion
We do not have enough evidence to say which intervention works better to control bad breath.
Summary of findings
Summary of findings for the main comparison. Mechanical tongue cleaning compared to no tongue cleaning for managing halitosis.
| Mechanical tongue cleaning compared to no tongue cleaning for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: mechanical tongue cleaning Comparison: no tongue cleaning | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with no tongue cleaning | Risk with mechanical tongue cleaning | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 2 weeks | The mean dentist‐reported OLT score was 1.804 units | MD 0.20 units lower (0.34 lower to 0.07 lower) | ‐ | 46 (2 RCTs)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
Summary of findings 2. 0.6% eucalyptus chewing gum compared to placebo chewing gum for managing halitosis.
| 0.6% eucalyptus chewing gum compared to placebo chewing gum for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: University hospital Intervention: 0.6% eucalyptus chewing gum Comparison: placebo chewing gum | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo chewing gum | Risk with 0.6% eucalyptus chewing gum | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 4 weeks | The mean dentist‐reported organoleptic score was 1.60 units | MD 0.10 units lower (0.31 lower to 0.11 higher) | ‐ | 65 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
|
*The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aTanaka 2010. bDowngraded for risk of bias ‐ unclear risk of bias due to lack of allocation concealment. cDowngraded for imprecision ‐ wide confidence intervals, low sample size and event rate.
Summary of findings 3. 1000 mg champignon compared to placebo for managing halitosis.
| 1000 mg champignon compared to placebo for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: 1000 mg champignon Comparison: placebo | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo | Risk with 1000 mg champignon | |||||
| Dentist‐reported OLT score assessed with dentist's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Patient‐reported VAS assessed with patient's perception Scale from: 0 to 100 Follow‐up: mean 2 weeks | The mean patient‐reported VAS was 63.47 units | MD 1.07 units lower (14.51 lower to 12.37 higher) | ‐ | 40 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aNishihira 2017. bDowngraded for risk of bias ‐ unclear risk of performance and detection bias and high risk of bias in reporting bias. cDowngraded for imprecision ‐ wide confidence interval crossing the line of no effect, low sample size and event rate.
Summary of findings 4. Hinokitiol gel compared to placebo gel for managing halitosis.
| Hinokitiol gel compared to placebo gel for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: hinokitiol gel Comparison: placebo gel | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo gel | Risk with hinokitiol gel | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 4 weeks | The mean dentist‐reported OLT score was 2.10 units | MD 0.27 units lower (1.26 lower to 0.72 higher) | ‐ | 18 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aIha 2013. bDowngraded for risk of bias ‐ high risk of performance and detection bias. cDowngraded for imprecision ‐ wide confidence interval, low sample size and event rate.
Summary of findings 5. 0.3% triclosan toothpaste compared to control toothpaste for managing halitosis.
| 0.3% triclosan toothpaste compared to control toothpaste for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: 0.3% triclosan toothpaste Comparison: control toothpaste | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with control toothpaste | Risk with 0.3% triclosan toothpaste | |||||
| Dentist‐reported breath odour score assessed with dentist's perception Scale from: 1 to 9 Follow‐up: mean 1 week | The mean dentist‐reported breath odour score was 7.14 units | MD 3.48 units lower (3.77 lower to 3.19 lower) | ‐ | 81 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aHu 2005. bDowngraded for risk of bias ‐ unclear risk of bias due to improper selection, lack of allocation concealment, performance, detection and reporting. cDowngraded for imprecision ‐ low sample size and event rate.
Summary of findings 6. Mouthwash containing chlorhexidine and zinc acetate compared to placebo mouthwash for managing halitosis.
| Mouthwash containing chlorhexidine and zinc acetate compared to placebo mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: mouthwash containing chlorhexidine and zinc acetate Comparison: placebo mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo mouthwash | Risk with mouthwash containing chlorhexidine and zinc acetate | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 3 months | The mean dentist‐reported OLT score was 2.30 units | MD 0.20 units lower (0.58 lower to 0.18 higher) | ‐ | 44 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aAdemovski 2017. bDowngraded for risk of bias ‐ unclear risk of selection bias, detection bias and other bias. cDowngraded for imprecision ‐ wide confidence intervals, low sample size and event rate.
Summary of findings 7. Brushing + cetylpyridium mouthwash compared to brushing for managing halitosis.
| Brushing + cetylpyridium mouthwash compared to brushing for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: brushing + cetylpyridium mouthwash Comparison: brushing | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with brushing | Risk with brushing + cetylpyridium mouthwash | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 3 weeks | The mean dentist‐reported OLT score was 1.37 units | MD 0.48 units lower (0.72 lower to 0.24 lower) | ‐ | 70 (1 RCT)a | ⊕⊕⊝⊝ LOWb | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aFeres 2015. bDowngraded for imprecision ‐ low sample size and event rate.
Background
The term halitosis is a general term used to describe any disagreeable odour of expired air, regardless of its origin. It is derived from the Latin word halitus meaning 'breath' or halare 'to breath' with a suffix from the Greek based noun osis (Harper 2016) which means pathologic alteration (Wu 2019). The lay term, bad breath, is the generally accepted term for foul smells emanating from the mouth but the term oral malodour is reserved for halitosis originating from the oral cavity (Tangerman 2002). Mouthwashes and tongue scrapers are popular ways of dealing with oral malodour.
Description of the condition
Prevalence and aetiology
The reliability of relevant epidemiological data has been questioned, but the prevalence of halitosis has been reported to be as high as 50% to 65% of the world's population (Mookem 2014; Yaegaki 2000). Severe halitosis may involve less than 5% of the population (Rosing 2011). In a study in Japan, 24% of patients complained of oral malodour (Miyazaki 1995) while in France it was reported that between 50% and 60% of the population suffer from chronic halitosis (Meningaud 1999). In Belgium, a study evaluated the characteristics of 2000 patients who visited a halitosis clinic, and reported that 76% of the patients had a possible oral cause e.g. tongue coating 43%, gingivitis/periodontitis 11%, or a combination of the two 18% (Quirynen 2009). A review of the literature reported a wide variation in the prevalence of halitosis around the world, with a rate ranging from 22% to 50% of the population (Akaji 2014). A systematic review and meta‐regression analysis done by Silva 2018 reported the prevalence of halitosis to be 31.8% (95% confidence interval (CI) 24.6% to 39.0%).
Multiple factors contribute to the aetiology of halitosis, and these may be the combination of drugs, food, local, systemic and psychological causes (Singh 2015; Thoppay 2018). It is now fairly widely accepted that halitosis originates from the oral cavity (Ayers 1998; Delanghe 1997; De Geest 2016). Accumulation of bacteria and food residues at the posterior part and in the furrows of the tongue (Seeman 2014; van Steenberghe 1997) is considered to be the major cause (Scully 1997; Thoppay 2018). Interdental plaque and gingivitis may also play a contributory role, and although periodontal pockets may produce putrid odours, their contribution to oral malodour is still unclear (De Geest 2016; Morita 2001).
3% to 10% of halitosis cases are caused by ear, nose and throat related problems like tonsillitis, sinusitis and postnasal drip which are commonly known as extraoral or non‐oral halitosis or throat halitosis (Bollen 2012). Interventions for such halitosis are not covered under the scope of this review.
Halitosis‐causing bacteria are the primary sources of volatile sulphur compounds (VSC); the chief components of which are hydrogen sulphide and methyl mercaptans (Kleinberg 1990; Tonzetich 1977). VSC and other additional odours such as indole, skatole, putrescine and cadaverine (Kleinberg 1995) are produced through the bacterial metabolic degradation of food debris, desquamated cells, saliva proteins, dental plaque and microbial putrefaction (Ratcliff 1999). The periodontal pocket also provides an ideal environment for VSC production thus explaining why patients with periodontal disease often complain of oral malodour (Morita 2001). The intensity of clinical bad breath has been shown to be significantly associated with the intraoral VSC level and to be correlated directly with periodontal health status (Bosy 1994; Replogle 1996; Stamou 2005).
Classification of halitosis
Halitosis has been defined as an unpleasant odour exhaled through the mouth and upper airways, caused by biofilm accumulation on the dorsum of the tongue, the interdental spaces or due to periodontal disease, although the condition is multifactorial and may involve both oral and non‐oral conditions (Oliveira‐Neto 2013; van den Broek 2007).
Although this classification has not been universally accepted by all experts in the field there is general agreement that halitosis can be categorised as genuine halitosis, pseudo‐halitosis and halitophobia (Yaegaki 2000). Genuine halitosis has been further subclassified as physiological halitosis in which there is no readily apparent disease or pathological condition, or pathological halitosis which occurs as a result of an infective process of the oral tissues. Pseudo‐halitosis is a condition in which there is absence of halitosis but patients believe that they have oral malodour. Halitophobia can occur when there is no physical or social evidence to suggest that halitosis is present and which can persist after treatment for either genuine halitosis or as pseudo‐halitosis.
Organoleptic test (OLT) measurement by trained breath judges is considered to be the gold standard and the most reliable way of evaluating malodour (Rosenberg 1992; Rosenberg 1995), but this has been contested by studies showing that measurements with the halimeter appear to be more reproducible albeit possibly less reliable than OLT methods (Silwood 2001). Methods of assessment of levels of malodour include those which are very simple, highly subjective and others which are complex, time consuming and involve the use of sophisticated equipment:
OLT score (Rosenberg 1992): 0: no detectable odour; 1: hardly detectable odour; 2: light odour; 3: moderate odour; 4: strong odour; and 5: extremely strong odour
portable VSC monitor, the halimeter (Rosenberg 1991): normal: 80 to 160 parts per billion (ppb); weak: 160 to 250 ppb; and strong: > 250 ppb (Baharvand 2008)
gas chromatography coupled with flame‐photometric detection (Solis‐Gaffar 1975)
culture of plaque and periodontal pocket exudates (Loesche 1995) and
multisensor approach, BIONOTE (Marchetti 2015).
Measurement of VSC levels can be carried out by a variety of methods: OLT which are considered subjective by some investigators but are the ones most relevant to patients (Tsunoda 1981), and the more complex gas chromatography techniques (Solis‐Gaffar 1975). Portable computerized VSC monitors or halimeters are available, they are compact, easy to use and relatively inexpensive (Pedrazzi 2004) but have their limitations in that they have a high sensitivity for hydrogen sulphide, but low sensitivity for one of the other sources of malodour, methyl mercaptan (Rosenberg 1991). Silwood 2001 have shown good reproducibility of VSCs in their study.
A correlation rate has been reported between the self‐estimation of bad breath and the presence of oral malodour as determined by OLT examination by odour‐judge assessment in patients with slight or moderate oral halitosis (Romano 2010).
Description of the intervention
At present there are no standard and accepted protocols for the treatment of oral malodour (Morita 2001) which could be because of its multiple aetiology. Halitosis, by itself, is not a disease, but a sign/symptom of a disease. Patients who are conscious that they have halitosis may attempt to mask it through compulsive brushing or with a range of over‐the‐counter methods such as chewing gum, mints, scented liquid drops, and the use of mouthrinses (Borden 2002). Most of these merely provide a competing and temporary smell that is capable of masking the unfavourable malodour. Some mouthrinses contain certain components that can neutralise the malodour or the bacteria which produce it. The most common of these include alcohol, zinc, phenol, chlorhexidine and folic acid. Reduction of the causative bacteria can also be accomplished through improving oral hygiene (Tonzetich 1978) in addition to cleaning of the tongue (Rosenberg 1996). This can be achieved by brushing or scraping the dorsum of the tongue to dislodge trapped food, cells, and bacteria from between the filiform papillae. Methods for treating or masking halitosis include:
mechanical methods: tongue cleaners which are more commonly made of plastic, resin, rubber or metal. These may contain nylon bristles and grooves or corrugations but they must be smooth. Toothbrushes can be used but these normally have soft bristles (or extra soft bristles) only (Pedrazzi 2004)
chemical methods: these include a range of mouthwashes containing antimicrobials such as chlorhexidine (0.2% to 0.12%), cetylpyridinium chloride (0.05% to 0.07%), hydrogen peroxide and essential oils to combat proteolytic odoriferous bacteria, producing VSCs, and those that mask odours, without interfering with microbial viability (zinc chloride or lactate, chlorine dioxide – 0.3%). Combinations of antimicrobial agents in one mouthwash, such as zinc salts and essential oils, or zinc salts and chlorhexidine or cetylpyridinium chloride are also available (van den Broek 2008).
Some combinations of mechanical and chemical methods have also been explored, with the combination of brushes and toothpastes containing zinc salts or even toothbrushes and chlorhexidine or other antimicrobial agents (Slot 2015; Slots 2012).
How the intervention might work
A range of mechanical and chemical hygiene (mouthrinses or mouthwashes) methods have been advocated (Oliveira‐Neto 2013), however the effectiveness of any intervention may be influenced by the nature of the mouthrinse formulation (Fedorowicz 2008), or by the type of mechanical device (dental floss, toothbrush, toothpaste) used to reduce VSCs (Oliveira‐Neto 2013).
The intervention needs to be able to reduce, eliminate or mask the production of VSCs, i.e. actions aimed at minimising the food available for odoriferous bacteria, reduce the total number exists of these bacteria, or make any environment where VSC‐producing bacteria live, less hospitable. The success of any halitosis intervention appears to hinge on the reduction of VSC levels and other foul volatiles and consequently the majority focus on mechanical and chemical options. Mechanical interventions (i.e. brushing, flossing and tongue scraping) aim to reduce the numbers of VSC‐producing bacteria, residual food matter and cellular debris from the gingivae and tongue. In an earlier version of a systematic review of the effectiveness of tongue scraping for treating halitosis, the review authors found that mechanical tongue cleaning with tongue scrapers appeared to have very limited and short acting benefits in controlling halitosis (Outhouse 2006). The limitations of mechanical methods to effectively reach and remove VSC‐producing bacteria from all oral ecological sites are acknowledged. The possibility that mouthrinses may be more effective in reaching the less accessible parts of the oral cavity, their greater social acceptance and ease of use has led to the development of a large number and range of over‐the‐counter mouthrinses (Ayers 1998; Richter 1996).
A number of mouthrinses contain antibacterial agents in addition to flavouring agents and these have been generally categorised into those that neutralise and those that mask the odour. Components which neutralise can further be divided into those that affect the bacteria directly or the chemical compounds they produce, and include chlorhexidine, phenol, triclosan, chlorine dioxide, alcohol and metal ions, the most common of which is zinc (Carvalho 2004; Farrell 2006). Some of the odour‐masking agents, consist of essential oils, which can also provide a competing and purely temporary smell that is capable of disguising the unfavourable malodour.
Tongue cleaning has been claimed to reduce oral malodour by decreasing VSC concentration by 20% to 70% (Tonzetich 1977). Oliveira‐Neto 2013 compared both mechanical and mouthrinses for treatment of morning breath and concluded that chlorhexidine and mechanical oral hygiene reduced bad breath for longer periods than tongue cleaning alone.
Continuous usage of mouthrinses can lead to adverse effects such as oral mucosa and dental‐crown staining, mucosal lesions, taste modifications, or abnormal oral sensation (Tartaglia 2019).
Why it is important to do this review
Halitosis can be serious enough to cause personal embarrassment, reduce self‐esteem and adversely affect personal relationships. It may also be a barrier to certain types of employment. There is existing uncertainty as to which is the most effective method of oral malodour control. The most popular method used involves mouthwashes containing chemicals which destroy odour‐forming bacteria and include other odour‐masking constituent which can disguise the smell. The simplicity in use and social acceptance of mouthrinses appear to support their popularity over mechanical means.
This new Cochrane Review incorporates the previous Cochrane Reviews on tongue scraping (Outhouse 2006) and mouthrinses (Fedorowicz 2008) for halitosis and aims to assess the effects of interventions used to control halitosis due to oral diseases.
Objectives
The objectives of this review were to assess the effects of various interventions used to control halitosis due to oral diseases only. We excluded studies including patients with halitosis secondary to systemic disease and halitosis‐masking interventions.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials only.
Types of participants
We included studies that recruited adolescents and adult participants over the age of 16 who presented with a clinical or self‐assessed diagnosis of halitosis, with no significant comorbidity or health condition that might lead to increased halitosis (e.g. diabetes). We excluded studies which had been conducted on participants with induced halitosis either by stopping or altering the oral hygiene habits, physiological halitosis such as morning breath, non‐oral halitosis, refractory and severe chronic periodontal diseases. Subjects with clinical attachment level (CAL) ≥ 5 mm were considered to have severe chronic periodontitis (Kinane 2015).
Types of interventions
Any intervention for the management of halitosis compared to another or placebo, or no intervention. The active interventions or controls were administered over a minimum of one week and with no upper time limit.
Studies which included single use mouthwashes were not considered for this review as the aim was to evaluate therapeutic effect rather than masking effect (Dadamio 2013).
Types of outcome measures
We did not consider these prespecified outcomes as criteria for including studies in this review, but they are a representative list of the outcomes of interest within whichever studies were included. See Section 5.1.2 in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Primary outcomes
For the primary outcomes in this review we considered self‐expressed (perceived) (Greenman 2004) and organoleptic test (OLT) (human nose) assessments of halitosis using any validated malodour intensity scale.
Secondary outcomes
Quality of life.
Assessment of halitosis as measured by any of the validated methods (halimeter, portable sulphide monitor or gas chromatography coupled with flame‐photometric detection).
Peak and steady‐state volatile sulphur compound levels using a sulphide monitor, prior to and at several time points after any intervention.
Adverse events.
Search methods for identification of studies
Electronic searches
Cochrane Oral Health's Information Specialist conducted systematic searches in the following databases for randomised controlled trials and controlled clinical trials without language or publication status restrictions:
Cochrane Oral Health's Trials Register (searched 8 April 2019) (Appendix 1);
Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 3) in the Cochrane Library (searched 8 April 2019) (Appendix 2);
MEDLINE Ovid (1946 to 8 April 2019) (Appendix 3);
Embase Ovid (1 November 2016 to 8 April 2019) (Appendix 4).
Subject strategies were modelled on the search strategy designed for MEDLINE Ovid. Where appropriate, they were combined with subject strategy adaptations of the highly sensitive search strategy designed by Cochrane for identifying randomised controlled trials and controlled clinical trials as described in the Cochrane Handbook for Systematic Reviews of Interventions Chapter 6 (Lefebvre 2011).
Due to the Cochrane Centralised Search Project to identify all clinical trials in the database and add them to CENTRAL, only the most recent months of the Embase database were searched. See the searching page on the Cochrane Oral Health website for more information. No other restrictions were placed on the date of publication when searching the electronic databases.
We also conducted additional searches in the following databases:
LILACS BIREME Virtual Health Library (Latin American and Caribbean Health Science Information database; from 1982 to 19 April 2019) (Appendix 5);
CINAHL EBSCO (Cumulative Index to Nursing and Allied Health Literature; 1937 to 19 April 2019) (Appendix 6);
the National Database of Indian Medical Journals (IndMed, indmed.nic.in/) (1985 to 19 April 2019) (Appendix 7);
OpenGrey (1992 to 19 April 2019) (Appendix 8).
Searching other resources
Cochrane Oral Health's Information Specialist searched the following trials registers/databases for ongoing trials on 8 April 2019:
the US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (Appendix 9);
the World Health Organization International Clinical Trials Registry Platform (www.who.int/trialsearch) (Appendix 10).
We also conducted additional searches in the following trials registries on 19 April 2019:
ISRCTN registry (www.isrctn.com) (Appendix 11);
Clinical Trials Registry ‐ India (ctri.nic.in/Clinicaltrials/login.php)(Appendix 12).
Prashanti Eachempati (PE) examined the bibliographies of the included and excluded studies and systematic reviews published in the year 2019 and 2018 for further references to potentially eligible randomised controlled trials based on the assumption that these reviews could have included previously published trials.
Sumanth Kumbargere Nagraj (SKN), Vijendra Pal Singh (VPS) and Eswara Uma (EU) contacted trial investigators and asked them to provide missing data or clarify study details.
We did not conduct a separate search for adverse effects of interventions for halitosis. However, we examined data on adverse effects from the included studies that were identified.
We checked that none of the included studies in this review were retracted due to error or fraud.
Data collection and analysis
Selection of studies
Two pairs of review authors (PE and VPS; EU and Eby Varghese (EV); Noorliza Mastura Ismail (NMI) and SKN) independently assessed the abstracts of studies resulting from the searches. The search was designed to be sensitive and include controlled clinical trials, these were filtered out early in the selection process if they were not randomised. We obtained full copies of all relevant and potentially relevant studies, those appearing to have met the inclusion criteria, or for which there was insufficient information in the title and abstract to make a clear decision on eligibility. We assessed the full‐text papers independently and resolved any disagreement on the eligibility of included studies through discussion and consensus. We excluded those records that did not meet the inclusion criteria, and we noted the reasons for their exclusion in the 'Characteristics of excluded studies' section of the review.
Data extraction and management
Two pairs of review authors (PE and VPS; EU and SKN; NMI and EV) independently collected study details and outcome data using a predetermined form designed for this purpose. We entered study details into the 'Characteristics of included studies' table in Review Manager (RevMan) (Review Manager 2014). The authors included data if there was an independently reached consensus.
We extracted the following details from the eligible trials.
Trial methods: method of sequence generation and concealment of allocation sequence; masking of participants, trialists and outcome assessors; exclusion of participants after randomisation; proportion of and reasons for losses to follow‐up.
Participants: country and study setting; sample size; age; ethnicity; inclusion and exclusion criteria.
Intervention: type; concentration, dose, and frequency; route of administration; duration of intervention and follow‐up.
Control: type; duration of intervention and follow‐up.
Outcomes: primary and secondary outcomes as specified in the 'Types of outcome measures' section.
If available, we collected data on sources of funding of the included studies, country, set‐up and number of centres.
Assessment of risk of bias in included studies
Two review authors (SKN and PE) assessed the risk of bias of the selected studies independently using Cochrane's tool for assessing risk of bias as described in Chapter 8, Section 8.5, in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We compared the evaluations and discussed and resolved any inconsistencies between the review authors.
We assessed the following domains as at 'low', 'unclear', or 'high' risk of bias:
sequence generation;
allocation concealment;
blinding of participants and personnel;
blinding of outcomes assessment;
incomplete outcome data;
selective outcome reporting; and
other bias.
We reported these assessments for each individual study in the 'Risk of bias' tables.
We categorised and reported the overall risk of bias of each of the included studies according to the following:
low risk of bias (plausible bias unlikely to seriously alter the results) if all criteria were met;
unclear risk of bias (plausible bias that raises some doubt about the results) if one or more criteria were assessed as unclear; or
high risk of bias (plausible bias that seriously weakens confidence in the results) if one or more criteria were not met.
Measures of treatment effect
We presented continuous outcomes on the original scale as reported in each individual study. If similar outcomes were reported using different scales, we intended to convert these to standardised mean differences (SMD). However, we did not find any studies using different scales to use SMD. We presented measures of treatment effect as mean differences (MD) with their 95% confidence intervals (CIs).
We intended to present the dichotomous outcomes as risk ratios (RR) and 95% CIs, if found significant, we intended to convert them to either: the number of patients needed to treat to find one additional beneficial outcome (NNTB); or the number needed to treat to find one additional harmful outcome (NNTH). However, none of the review outcomes were reported as dichotomous outcomes.
Unit of analysis issues
Cross‐over trials
Unit of analysis issues can arise in studies where participants have been randomised to multiple treatments in multiple periods or where there has been an inadequate wash‐out period. We analysed these data based on the advice provided in Section 16.4.4 in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We intended to assess the carry‐over and period effects descriptively, and if there was evidence of minimal impact and there were adequate data, we planned to carry out a paired analysis. However, we did not carry out paired analysis.
Studies with multiple treatment groups
Studies that are reported with multiple treatment groups have the potential for participant data to contribute to multiple comparisons. We planned to assess the treatments and determine which were relevant to our review then allocate the non‐intervention participants as the 'shared' group. We intended to split the 'shared' group equally into the number of comparisons made, as discussed in Section 16.5.4 in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). However, we did not encounter such studies in this review.
Dealing with missing data
If we encountered data missing from trials that are less than 10 years old, we would have tried wherever possible to contact the investigators or sponsors of these studies. We planned to re‐analyse data according to the intention‐to‐treat (ITT) principle whenever possible. However, we did not encounter such studies in the review.
Assessment of heterogeneity
We assessed clinical heterogeneity by examining the characteristics of the studies and the similarity between the types of participants and the interventions. We assessed the degree of heterogeneity between the studies using the I2 statistic. We reported heterogeneity as important and at least moderate to substantial if the I2 statistic > 60% (Higgins 2011). If this was explained by clinical reasoning and a coherent argument could be made for combining the studies, we entered these into a meta‐analysis. In cases where the heterogeneity could not be adequately explained, we intended to pool the data but would account for any heterogeneity and downgrade the certainty of the body of evidence according to GRADE methods. However, we did not find such cases in the review.
Assessment of reporting biases
We planned to follow reporting bias assessment as recommended by Egger 1997, through testing for funnel plot asymmetry as described in Section 10.4.3.1 in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We intended to perform these for primary and secondary outcomes for meta‐analysis if we included a minimum number of studies, to allow a reasonable estimate of the effect of intervention (nominally nine studies). However, none of our analyses included nine or more studies and hence we did not assess reporting bias as planned.
Data synthesis
Two review authors (SKN and PE) analysed the data in RevMan (Review Manager 2014) and reported them in accordance with the advice in Chapter 9 in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We carried out a random‐effects meta‐analysis and planned to report data that exhibited not more than moderate heterogeneity (Treadwell 2006). However, the majority of the analyses included not more than two studies and none of the analyses showed heterogeneity.
Subgroup analysis and investigation of heterogeneity
We planned to conduct the following subgroup analyses subject to availability of a reasonable number of studies (n ≥ 3) reporting data:
OLT level of halitosis ≥ 3 at baseline;
evaluation method: OLT or halimeter;
duration of treatment and the time of assessments.
However, because of a less number of studies in the analyses, we did not conduct any subgroup analysis.
Sensitivity analysis
We planned to carry out sensitivity analyses to assess the robustness of the results of this review. This intended to include repeating the analyses with the following adjustment: exclusion of studies at high risk of bias and reporting of any comparative difference between the results of these analyses. However, we did not have multiple similar studies included to carry out sensitivity analysis.
Presentation of main results
We produced 'Summary of findings' tables using GRADEpro GDT 2015 for the most important comparisons and the following outcomes:
dentist‐reported OLT change from baseline in halitosis;
patient‐reported OLT change from baseline in halitosis; and
adverse events.
We assessed the level of certainty in the findings with reference to the risk of bias assessments, the directness of the evidence, the inconsistency of the results, the precision of the estimates, and the risk of publication bias. The level of certainty for each of the comparisons was categorised as high, moderate, low, or very low.
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification and Characteristics of ongoing studies.
Results of the search
We included 44 trials (55 reports) in the review. (If the same study (one population) was separated into multiple reports we included the primary study and considered the rest as reports as per Higgins 2011.) See Figure 1 for the selection process of search results.
1.

Study flow diagram.
Included studies
Characteristics of trial settings and investigators
Publication status
Out of 44 reports, 43 were published and one was an unpublished report (NCT02628938).
Language
We had five studies in foreign languages. Two in Mandarin (An 2011; Wang 2017), one in Portuguese (Garcia 2014), one in Spanish (López Jornet 2003), and one in Arabic (Talebian 2009). The other 39 trials were in the English language.
Countries of origin
Two were from Sweden (Ademovski 2012; Ademovski 2017), three were from China (An 2011; Hu 2018; Wang 2017), four were from India (Asokan 2011; Lomax 2017; Mamgain 2016; Patil 2017), one from Myanmar (Aung 2015), six from USA (Barak 2012; Borden 2002; Hu 2005; Lee 2018; Niles 1999; Wirthlin 2011), three from Turkey (Acar 2019; Caygur 2017; Kara 2008), one from Belgium (Dadamio 2013), three from Brazil (Feres 2015; Garcia 2014; Nogueira‐Filho 2002), eight from Japan (Iha 2013; Iwamura 2016; Nakano 2017; Nishihira 2017; Nohno 2012; Suzuki 2014; Tanaka 2010; Watanabe 2018), one from Israel (Kozlovsky 1996), one from Spain (López Jornet 2003), one from Italy (Marchetti 2015), one from UK (Payne 2011), three from Thailand (Rassameemasmaung 2007; Rassameemasmaung 2012; Satthanakul 2014), one from Iran (Talebian 2009), two from Germany (Wigger‐Alberti 2010; Wilhelm 2012), one from Saudi Arabia (NCT02628938), and one from the Netherlands (Winkel 2003). One study was conducted in two centres (India and Shanghai) (Navada 2008).
Funding
Six trials were government funded (An 2011; Garcia 2014; Iwamura 2016; Kozlovsky 1996; Tanaka 2010; Watanabe 2018), seven trials were university funded (Acar 2019; NCT02628938; Nishihira 2017; Rassameemasmaung 2007; Rassameemasmaung 2012; Talebian 2009; Wirthlin 2011), 16 trials were funded by private agencies (Ademovski 2012; Ademovski 2017; Barak 2012; Borden 2002; Dadamio 2013; Hu 2018; Lomax 2017; Marchetti 2015; Nakano 2017; Navada 2008; Patil 2017; Payne 2011; Satthanakul 2014; Wigger‐Alberti 2010; Wilhelm 2012; Winkel 2003), two were funded by both government and private agencies (Iha 2013; Suzuki 2014), and the other 13 trials did not mention any funding details (Asokan 2011; Aung 2015; Caygur 2017; Feres 2015; Hu 2005; Kara 2008; Lee 2018; López Jornet 2003; Mamgain 2016; Niles 1999; Nogueira‐Filho 2002; Nohno 2012; Wang 2017).
Trial design
36 trials had a parallel‐arm design (Acar 2019; Ademovski 2017; An 2011; Asokan 2011; Aung 2015; Barak 2012; Borden 2002; Caygur 2017; Dadamio 2013; Feres 2015; Garcia 2014; Hu 2005; Hu 2018; Iha 2013; Iwamura 2016; Kara 2008; Kozlovsky 1996; Lee 2018; Lomax 2017; López Jornet 2003; Mamgain 2016; Marchetti 2015; NCT02628938; Nakano 2017; Navada 2008; Nishihira 2017; Patil 2017; Rassameemasmaung 2007; Rassameemasmaung 2012; Satthanakul 2014; Tanaka 2010; Wang 2017; Watanabe 2018; Wigger‐Alberti 2010; Winkel 2003; Wirthlin 2011), and eight were cross‐over trials (Ademovski 2012; Niles 1999; Nogueira‐Filho 2002; Nohno 2012; Payne 2011; Suzuki 2014; Talebian 2009; Wilhelm 2012).
Trial arms
31 trials had two arms (Acar 2019; Ademovski 2017; An 2011; Asokan 2011; Aung 2015; Caygur 2017; Feres 2015; Garcia 2014; Hu 2005; Hu 2018; Iha 2013; Kozlovsky 1996; Lee 2018; Lomax 2017; Mamgain 2016; Marchetti 2015; Nakano 2017; Navada 2008; Niles 1999; Nohno 2012; Patil 2017; Payne 2011; Rassameemasmaung 2007; Rassameemasmaung 2012; Satthanakul 2014; Suzuki 2014; Talebian 2009; Wang 2017; Watanabe 2018; Winkel 2003; Wirthlin 2011), five trials had three arms (Iwamura 2016; Kara 2008; NCT02628938; Tanaka 2010; Wilhelm 2012), five trials had four arms (Ademovski 2012; Borden 2002; López Jornet 2003; Nishihira 2017; Wigger‐Alberti 2010), and three trials had five arms (Barak 2012; Dadamio 2013; Nogueira‐Filho 2002).
Sample size
The minimum sample size was seven (Talebian 2009) and the maximum sample size was 190 (Navada 2008).
Characteristics of participants
Age
The minimum age of the participants in the included trials was 17 years (Asokan 2011; Patil 2017; Rassameemasmaung 2007) and the maximum age was 77 years (Ademovski 2017).
Gender
32 trials included both the genders (Acar 2019; Ademovski 2012; Ademovski 2017; An 2011; Barak 2012; Borden 2002; Dadamio 2013; Feres 2015; Hu 2005; Hu 2018; Iha 2013; Kara 2008; Kozlovsky 1996; Lee 2018; Lomax 2017; López Jornet 2003; Marchetti 2015; Nakano 2017; Nishihira 2017; Nogueira‐Filho 2002; Patil 2017; Payne 2011; Rassameemasmaung 2007; Rassameemasmaung 2012; Satthanakul 2014; Suzuki 2014; Tanaka 2010; Wang 2017; Watanabe 2018; Wigger‐Alberti 2010; Wilhelm 2012; Winkel 2003). Four trials included only males (Aung 2015; Iwamura 2016; Nohno 2012; Talebian 2009), one trial included only females (NCT02628938), and the other seven trials did not mention the gender details of the participants (Asokan 2011; Caygur 2017; Garcia 2014; Mamgain 2016; Navada 2008; Niles 1999; Wirthlin 2011).
Characteristics of interventions
1. Mechanical debridement
We included four studies and the following comparisons were identified.
1a. Scaling and root planing (SRP) with air polishing versus SRP: we included one study (Caygur 2017) in this comparison. This study had two arms, comparing SRP plus glycerine powder air polishing with SRP alone in patients with halitosis with follow‐ups after 7, 14 and 30 days. The outcome measure used was volatile sulphur compound (VSC) measured using a halimeter. In this review, we have used data after 30 days follow‐up only.
1b. SRP + laser versus SRP: we included one study (Kara 2008) for this comparison. The study had three arms, SRP (group I), subgingival laser irradiation combined with povidone‐iodine application (group II), and SRP and subgingival laser irradiation (group III). They followed‐up for one week and four weeks after the intervention. The outcome measures they used were organoleptic test (OLT) score and VSC. However, we have used the data from group I and II only for the one week follow‐up period for both the outcome measures.
1c. Mechanical tongue cleaning versus no tongue cleaning: we included two studies (Acar 2019; Wang 2017) in this comparison. Acar 2019 did a two parallel‐arm study. After scaling and polishing, tongue cleaning by using a tongue scraper was compared to no tongue cleaning in 36 patients. The outcome measures were dentist‐reported OLT scores and VSC with a follow‐up of seven days. Wang 2017, a two parallel arm study, compared toothbrushing and mechanical tongue cleaning with toothbrushing and have followed‐up for a period of one, two, four and eight weeks. The outcomes measured were OLT scores and VSC. However, we have used the data for VSC scores after one week follow‐up only (standard deviation (SD) could not be calculated for OLT).
2. Chewing gum/lozenges
We included two studies using chewing gum, one study using candy and one study using lozenges under this category.
2a. 0.6% eucalyptus chewing gum versus 0.4% eucalyptus chewing gum and placebo: one study (Tanaka 2010) is included in this comparison which was a three parallel‐arm study comparing high and low concentration eucalyptus chewing gum and a placebo chewing gum, five minutes, five times per day for a period of 12 weeks. The outcome measures used in the study were OLT and VSC scores evaluated by the dentist and were assessed at the end of 4, 8, 12 and 14 weeks. We have used the data for both scores after four weeks follow‐up only and have analysed the outcomes between 0.4% and 0.6% eucalyptus chewing gums and 0.6% eucalyptus chewing gum and placebo groups.
2b. Pycnogenol chewing gum versus placebo chewing gum: one study (Watanabe 2018) compared these two chewing gums, 2.5 mg for 15 minutes, six times daily for a period of four weeks. The outcome measures used were VSC scores of three volatile gases. We have used the data at the end of two weeks.
2c. Abrasive candy; abrasive candy with propolis and abrasive candy with zinc gluconate versus abrasive candy with propolis and zinc:Barak 2012 in their 5‐arms parallel‐group randomised controlled trial (RCT), compared the reduction of halitosis in the subjects using abrasive candy (Breezy candy); abrasive candy with 2% propolis and abrasive candy with 0.5% zinc gluconate versus abrasive candy with 1% propolis and 0.25% zinc. The outcome measured was VSC score using a halimeter. We could not use the results of this study in the meta‐analysis because of the missing SD and P value in the report.
2d. Lactobacillus brevis CD2 lozenges versus placebo lozenges: in a two‐arm parallel‐group RCT conducted by Marchetti 2015, reduction in halitosis was compared between groups consuming Lactobacillus brevis CD2 lozenges and placebo lozenges. The outcome measures were OLT, VSC and breath print scores measured using Rosenberg scale, OralChroma and Bionote. The study did not report any usable data and hence could not be included in the meta‐analysis.
3. Systemic deodorising agent
We have only one comparison of systemic agents under this section.
3a. Champignon extract versus placebo: we included one study (Nishihira 2017) in this comparison. This is a four parallel‐arm study which compared 50 mg/day, 500 mg/day and 1000 mg/day champignon (champignon extract, an extract boiled from the mushroom Agaricus bisporus) with placebo tablets. The follow‐up period was four weeks and the outcome measures were visual analogue scale (VAS) score (0 to 100) which was reported by the study participants and relative of the participant. We have used the data after two weeks follow‐up for 50 mg, 1000 mg, and placebo groups only.
4. Topical agents
We have two comparisons reported by two trials.
4a. Hinokitiol gel versus placebo gel: this comparison was seen in only one study (Iha 2013) which is a two‐arm parallel‐group study comparing hinokitiol gel (hinokitiol C10H12O2 (b‐thujaplicin), a component of the essential oils isolated from Cupressaceae) with placebo gel. The outcome measures were OLT scores, VSC scores for methyl mercaptan and hydrogen sulphide after a follow‐up of 28 days, as reported by the dentist.
4b. Topical G32 versus chlorhexidine gel:Patil 2017 compared topical G32 (ayurvedic preparation consisting of extracts of Mimusops elengi, Acacia catechu, Myrtus caryophyllus, Barleria prionitis) with chlorhexidine digluconate 1% gel in a single‐blind parallel‐designed trial. The study participants crushed 2 to 3 G32 tablets and massaged it on their gums twice a day for five minutes. The outcome measures were VSC and OLT scores reported by the dentist after one week follow‐up. However, we have used the data for VSC only as the OLT score data were not available.
5. Toothpaste
We have seven comparisons reported by seven trials.
5a. Triclosan + polyvinyl methyl ether/maleic acid (PVM/MA) toothpaste versus sodium fluoride toothpaste:Hu 2005 compared the effectiveness of a dentifrice containing 0.3% triclosan, 2% PVM/MA copolymer, 0.243% sodium fluoride (TCF) to a commercially available dentifrice containing 0.243% sodium fluoride (control) for the management of oral malodour in a three‐week, randomised double‐blind, longitudinal clinical trial. The outcome measure was OLT score which was done using a nine‐point hedonic scale (1: most pleasant, 5: neutral, and 9: most unpleasant).
5b. Zinc toothpaste versus placebo toothpaste: two randomised, two‐cell parallel, double‐blind, placebo‐controlled clinical trials were done by Navada 2008. Both the studies compared the efficacy of toothpaste containing 0.2% zinc sulphate to toothpaste without zinc. In the first study, VSC was measured by halimeter and in second, breath freshness was assessed by four odour judges using OLT scores (0: no odour present and 5: extremely foul odour).
5c. Sodium bicarbonate toothpaste versus control toothpaste: a single‐centre, single examiner‐blind, randomised, controlled, two‐treatment, parallel‐group study, with a six‐week intervention period was conducted by Lomax 2017. Toothpaste containing sodium bicarbonate was compared to control toothpaste which did not have sodium bicarbonate. The outcome measure for halitosis was VSC using gas chromatography with flame photometric detection.
5d. Dual zinc + arginine dentifrice versus control toothpaste: in a double‐blind, clinical study done by Hu 2018 a dual zinc plus arginine dentifrice containing zinc oxide and zinc citrate 0.96%, 1.5% arginine and 1450 parts per million (ppm) fluoride (F) as sodium fluoride in a silica base was compared to a regular fluoride dentifrice containing 1450 ppm F as sodium fluoride in a silica base to control halitosis. The outcome measure for halitosis was OLT hedonic scale (1: most pleasant to 9: most unpleasant).
5e. Zinc chloride (ZnCl) + sodium fluoride (NaF) dentifrice versus control dentifrice containing NaF:Payne 2011, in his cross‐over randomised trial, compared the reduction of halitosis in subjects brushing using dentifrice containing ZnCl + NaF with control dentifrice containing NaF. The outcome measure was VSC score using gas chromatography with flame photometric detection. The trial reported the adjusted mean VSC scores in the graph and hence we could not use the data in the meta‐analysis.
5f. Triclosan + PVM/MA copolymer + NaF in a silica base toothpaste versus placebo toothpaste: In a cross‐over trial done by Niles 1999, reduction in halitosis was compared in subjects using 0.3% triclosan + 2.0% PVM/MA copolymer + 0.243% NaF in a silica base toothpaste with a placebo toothpaste. The outcome measure was VSC score using a 565 Tracor gas chromatograph with a flame photometric detector. We could not use the results of this study in the meta‐analysis as there was no correlation coefficient reported and we could not find similar intervention trial to impute the SD of differences.
5g. Crest Complete A dentifrice; Signal Global A dentifrice; Colgate Total A dentifrice and experimental formulation versus negative control: In a five‐arm parallel‐group trial by Nogueira‐Filho 2002, three commercial dentifrices with 0.3% triclosan (Crest Complete A, Signal Global A and Colgate Total A) were compared with similar experimental formulation (0.3% triclosanπ2% PVM/MA 0.75% Zn 4% tetrapotassium pyrophosphate (PPi)) and a negative control dentifrice for reduction of halitosis. The outcome measure was VSC score measured using a halimeter. We could not use the results of this study in the meta‐analysis as there was no correlation coefficient reported and we could not find similar intervention trial to impute the SD of differences.
6. Mouthrinse or mouthwash
Mouthwashes are antiseptic solutions used after brushing. Whereas, a mouthrinse is used before brushing to freshen the breath (Sumanth 2019). However, we are not sure if the study authors have used it synonymously or followed the above described definition. Hence we have used the same terminology as used by the trial authors. We have 17 comparisons reported by 17 trials under this section.
6a. Halita mouthwash versus placebo:Winkel 2003 compared a newly developed mouthrinse (chlorhexidine (0.05%), cetylpyridinium chloride (0.05%) and zinc lactate (0.14%)) to placebo mouthrinse in the treatment of oral halitosis in patients without periodontitis in their dual centre, double‐blind, parallel‐arm, randomised controlled trial. The outcomes were measured after 14 days using VSC (halimeter) and OLT scores (0: no halitosis and 5: offensive halitosis).
6b. Chlorhexidine + zinc acetate mouthwash versus placebo: a randomised, double‐blind, placebo‐controlled, parallel‐group, 6‐month trial, was conducted by Ademovski 2017 comparing chlorhexidine plus zinc acetate mouthwash to placebo mouthwash in patients with halitosis. The outcome measures were OLT score (0: no odour and 5: extremely strong odour), total VSC (halimeter) and hydrogen sulphide (H2S) and methyl mercaptan (MM) concentration using portable gas chromatograph at the duration of three and six months.
6c. Cetylperidinium chloride mouthwash versus placebo; essential oil mouthwash versus placebo and chlorine dioxide + zinc mouthwash versus placebo:Borden 2002 conducted a randomised, double‐blind, longitudinal clinical trial comparing four different mouthrinses (essential oil, chlorine dioxide + zinc, cetylpyridinium and placebo) for four weeks. The outcome measures for oral halitosis were OLT score (0: no odour and 5: extremely foul odour) and VSC scores (halimeter).
6d. Chlorine dioxide mouthwash versus placebo:Lee 2018 did a cross‐over, double‐blind randomised controlled trial comparing a mouthwash containing 0.1% stabilized chlorine dioxide or a placebo twice daily for a period of eight weeks. The outcome measure was OLT score (0: no odour and 5: extremely strong odour).
6e. Herbal mouthwash versus placebo:Rassameemasmaung 2007 compared the effect of a herbal mouthwash to placebo mouthwash in their double‐blind, randomised, placebo‐controlled trial for two weeks. The outcome measure was VSC score.
6f. Benzethonium chloride mouthwash versus placebo:Iwamura 2016 conducted a randomised, double‐blind pilot study comparing benzethonium chloride mouthwash to placebo mouthwash and no mouthwash. The outcome measures were OLT score (0: absence of odour and 5: extreme malodour) and VSC (OralChroma) for all three components separately.
6g. Green tea mouthwash versus placebo: in a double‐blind, placebo‐controlled trial done by Rassameemasmaung 2012, the effects of a green tea mouthwash were compared to placebo mouthwash for a period of four weeks. The outcome measure was VSC (halimeter).
6h. Lemongrass mouthwash versus placebo:Satthanakul 2014 did a randomised double‐blind clinical study to compare the effects of lemongrass oil mouthwash to placebo mouthwash for eight days. The outcome measure was VSC (halimeter).
6i. Halita mouthrinse versus Perio‐plus mouthrinse:Dadamio 2013 conducted a single‐centre, double‐blind, randomised, parallel‐group clinical trial comparing the efficacy of halita and meridol with and without zinc lactate versus negative and positive control. The outcome measures were OLT score (0 to 5) and VSC determined by a portable gas chromatograph.
6j. Oil water two‐phase mouthwash versus control mouthwash: In a six‐week randomised clinical trial done by Kozlovsky 1996, oil water two‐phase mouthwash containing cetylpyridinium chloride (CPC) was compared to control mouthwash. The outcome measures were OLT score (0: no appreciable odour and 5: extremely foul odour) and VSC (sulphide monitor). However, the report does not give any details of OLT score and hence we have used only VSC score in the meta‐analysis.
6k. Triphala and Ela decoction versus mouthwash:Mamgain 2016 conducted a randomised controlled trial comparing mouthwash containing decoction of Triphala and Ela with chlorhexidine mouthwash for 21 days. The outcome measure was OLT score.
6l. Miswak mouthwash versus chlorhexidine mouthwash: an unpublished clinical trial (NCT02628938) compared miswak (Salvadora persica) mouthwash with chlorhexidine mouthwash twice a day, among female students who had halitosis. The outcome measures were OLT score (0: no appreciable odour and 5: extremely foul odour), VSC (Tanita FitScan HC‐212SF Breath Checker; 0: no odour and 5: intense odour) and patient self‐assessment score (10 cm VAS that is marked as 'no odour' on the 0 cm end, and as 'extremely foul odour' on the 10 cm end) after seven days.
6m. Chlorine dioxide mouthwash versus chlorhexidine mouthwash:Wirthlin 2011, in their double‐blind, randomised, parallel‐group clinical trial, compared tongue scraping + chlorine dioxide mouthwash to tongue scraping + chlorhexidine mouthwash for one week. The outcome measures were VSC (OralChroma) and OLT score (0 to 5). However, we could not include the OLT scores in the analysis as the group‐wise data were not given.
6n. Triclosan + NaF + ZnCl + alcohol mouthwash; triclosan + NaF + ZnCl mouthwash; zinc lactate + chlorhexidine gluconate + cetylpyridine chloride mouthwash versus placebo mouthwash:López Jornet 2003 conducted a randomised, four‐arm parallel‐group clinical trial comparing triclosan mouthwash with and without alcohol, mouthwash containing zinc lactate 0.14%, chlorhexidine gluconate 0.005% and cetylpyridine chloride 0.05% with placebo mouthwash. The outcome measures were VSC scores obtained from halimeter and OLT score. We could not include the results of this trial in the meta‐analysis because of the missing SD and P value in the results.
6o. Essential oil mouthwash versus placebo mouthwash: in a two‐arm parallel‐group RCT done by Garcia 2014, the group using essential oil mouthwash was compared to the group using placebo mouthwash. The outcome measure was VSC score measured using halimeter. We could not include the results of this trial in the meta‐analysis because of the missing SD and P value in the results.
6p. Cinnamon herbal mouthwash with alcohol; Nanosil mouthwash with hydrogen peroxide; Irsha mouthwash with alcohol versus water (negative control) and zinc solution (positive control):Talebian 2009 did a double‐blind, placebo‐controlled, randomised cross‐over study. The subjects were tested with cinnamon herbal mouthwash with alcohol, Nanosil mouthwash with hydrogen peroxide, Irsha mouthwash with alcohol and compared with a negative control ‐ water and a positive control ‐ zinc solution. The outcome measure was VSC score measured by halimeter. We could not include the results of this trial in the meta‐analysis as the report did not mention any data that could be used.
6q. Sesame oil versus chlorhexidine mouthwash: in a two‐arm, parallel‐group trial done by Asokan 2011, the efficacy of sesame oil was compared with the efficacy of chlorhexidine 0.2% mouthwash in the reduction of halitosis measured with OLT and BANA test. We could not include the results of this trial in the meta‐analysis because they did not report post‐intervention OLT score and P value.
7. Tablets
We have three comparisons using tablets reported by three trials.
7a. Protease cysteine + actinidine tablets versus placebo tablets: in a double‐blind, randomised cross‐over trial done by Nohno 2012, protease cysteine + actinidine tablets were compared to placebo tablets for seven days to reduce the tongue coating and thus the halitosis. The outcome measure was VSC (OralChroma).
7b. Lactobacillus β lactoperoxidase (LPO) tablets versus placebo tablets: in a two‐arm parallel‐group trial conducted by Nakano 2017, halitosis reduction was compared between groups consuming Lactobacillus ß LPO tablets and placebo tablets. The outcome measure was VSC score using OralChroma. The trial did not report any data that could be used in the meta‐analysis and hence could not be included in the analysis.
7c. Lactobacillus salivarius WB21 tablets versus placebo tablets: in a randomised, double‐blind, cross‐over, placebo‐controlled clinical trial with two arms conducted by Suzuki 2014, the reduction in halitosis was compared between subjects consuming Lactobacillus salivarius WB21 tablets versus placebo tablets. The outcome measures were OLT scores and VSC scores (gas chromatography). The trial did not give data that could be used in the meta‐analysis and there was no colour difference in the graph and hence we could not extract the data from the graph.
8. Combination methods
We have seven comparisons reported by seven trials under this section.
8a. Miswak stick versus chlorhexidine mouthwash: an unpublished clinical trial (NCT02628938) compared miswak (Salvadora persica) stick with chlorhexidine mouthwash twice a day, among female students who had halitosis. The outcome measures were OLT score (0: no appreciable odour and 5: extremely foul odour), VSC (Tanita FitScan HC‐212SF Breath Checker; 0: no odour and 5: intense odour) and patient self‐assessment score (10 cm VAS that is marked as 'no odour' on the 0 cm end, and as 'extremely foul odour' on the 10 cm end) after seven days.
8b. Brushing + mouthwash versus brushing + tongue cleaning:Aung 2015 conducted a single‐blind, parallel‐design, randomised controlled trial comparing three oral hygiene regimens for oral malodour reduction. Toothbrushing and mouthwashing with chlorine dioxide mouthwash was compared to toothbrushing and tongue cleaning after four weeks. The outcome measure was VSC using Breathron portable sulphide monitoring device. After four weeks, both the groups used toothbrushing plus mouthwashing with chlorine dioxide plus tongue cleaning and VSC was tested at the end of the fifth week. However, in our review, we have used the data at the end of four weeks only.
8c. Toothbrushing + rinsing with a 0.075% CPC mouthwash versus toothbrushing:Feres 2015 compared the efficacy of toothbrushing with fluoride toothpaste and CPC mouthwash to toothbrushing with fluoride toothpaste in their trial. The outcomes were measured using halimeter and OLT scores (0: no odour present and 5: extremely foul odour) after 21 days.
8d. Brushing + Turkish gall oral rinse versus brushing: a single‐blinded, randomised controlled trial was conducted by An 2011 to compare the effects of toothbrushing and oral rinsing with Turkish gall (traditional Chinese medicine) to toothbrushing alone. The outcome measures used were VSC (halimeter) and OLT scores (0 to 5) reported by the investigator.
8e. Laser with povidone iodine application versus SRP: one study (Kara 2008) was included for this comparison. The study had three arms, SRP (group I), subgingival laser irradiation combined with povidone‐iodine application (group II), and SRP and subgingival laser irradiation (group III). They have followed‐up for one week and four weeks after the intervention. The outcome measures used were OLT score and VSC. However, we have used the data from group I and II only for the one week follow‐up period only for both the outcome measures.
8f. Active rinse and active rinse + tongue scraping versus negative control rinse or negative control rinse + tongue scraping: in a four‐arm, cross‐over trial done by Ademovski 2012, reduction of halitosis was compared in subjects using an active rinse (water, glycerin, sorbitol, alcohol (1.8%), zinc acetate (0.3%), chlorhexidine diacetate (0.025%), sodium fluoride (0.05%), hydrogenated Castro oil, citric acid, acesulphame potassium, menthol and Mentha piperita), active rinse plus tongue scraping with a negative control rinse or negative control rinse plus tongue scraping. The outcome measures were OLT and VSC scores (OralChroma and halimeter). The authors did not report the correlation coefficient and we could not find a similar intervention trial to impute the SD of differences, thus excluding this trial from meta‐analysis.
8g. Toothbrushing with a reference toothpaste, toothbrushing with reference toothpaste + tongue cleaning, and toothbrushing + tongue cleaning with a tooth‐and‐tongue gel:Wilhelm 2012 conducted a single‐centre, examiner‐blind, randomised cross‐over trial in which the participants received each of the three interventions (toothbrushing with a reference toothpaste (1400 ppm F from sodium monofluorophosphate), toothbrushing with reference toothpaste and tongue cleaning, and toothbrushing and tongue cleaning with a tooth‐and‐tongue gel (Meridol halitosis tooth and tongue gel; 1400 ppm F ‐ from amine fluoride/stannous fluoride (ASF), 0.5% zinc lactate, oral malodour counter‐actives (OMCs)). The outcome measures were OLT, VSC (OralChroma CHM‐1, Abilit), and patient satisfaction scores. The authors did not report the correlation coefficient and we could not find a similar intervention trial to impute the SD of differences and thus we could not include this trial results in our meta‐analysis.
Outcome measuring methods
Fifteen trials measured the VSC levels as outcome (Aung 2015; Barak 2012; Caygur 2017; Garcia 2014; Lomax 2017; Nakano 2017; Niles 1999; Nogueira‐Filho 2002; Nohno 2012; Patil 2017; Payne 2011; Rassameemasmaung 2007; Rassameemasmaung 2012; Talebian 2009; Watanabe 2018). Three trials measured OLT scores as the outcome (Hu 2005; Lee 2018; Mamgain 2016). Twenty‐one trials measured both OLT scores as well as VSC levels as outcomes (Acar 2019; Ademovski 2012; Ademovski 2017; An 2011; Borden 2002; Dadamio 2013; Feres 2015; Iha 2013; Iwamura 2016; Kara 2008; Kozlovsky 1996; López Jornet 2003; NCT02628938; Navada 2008; Suzuki 2014; Tanaka 2010; Wang 2017; Wigger‐Alberti 2010; Wilhelm 2012; Winkel 2003; Wirthlin 2011). One study (Hu 2018) used OLT hedonic scores to measure the halitosis and another study (Asokan 2011) measured OLT score as well as self‐assessment of breath by the participants. One study measured VSC level along with self‐assessment as outcomes (Satthanakul 2014). Self‐assessment using VAS was used only in one trial (Nishihira 2017). Three outcome measurements, namely, OLT scores, VSC and breath print analysis were done in one trial (Marchetti 2015). Four studies (Iha 2013; Iwamura 2016; Watanabe 2018; Wirthlin 2011) reported VSC scores of different volatile gases (hydrogen sulphide, methyl mercaptan and methyl sulphide) rather than a compiled VSC score.
Quality of life
None of the included studies reported data on the outcome quality of life.
Adverse events
Seven trials reported adverse events (Borden 2002; Dadamio 2013; Lomax 2017; Patil 2017; Payne 2011; Winkel 2003; Wirthlin 2011). Other studies have either not given the details of adverse events or no adverse events were reported. Adverse events reported by Borden 2002 and Lomax 2017 were not related to the interventions. Dadamio 2013 reported unpleasant feeling and teeth staining in their trial. Patil 2017 trial reported burning mucosa and drying of mouth in few subjects using the control drug (chlorhexidine) and no adverse effects were reported in the intervention group (G32 tablets). Payne 2011 reported 19 non‐oral and 12 oral adverse effects. The oral effects were tingling sensation in lips, dry mouth or sore gums. Winkel 2003 reported discolouration of teeth and Wirthlin 2011 reported altered taste sensation as the adverse effect.
Studies awaiting classification
Eight trials are awaiting classification. Full texts were not available in the British Library for six trials (Cuihua 2009; Dongling 2017; Niles 2003; Rostoka 2012; Shimei 2014; Vazquez 2003), one trial (Gupta 2016) has not mentioned the inclusion criteria for healthy volunteers and we are waiting for translation of one report (Liang 2013).
Among these eight trials, three are in English (Gupta 2016; Niles 2003; Vazquez 2003), one in Russian (Rostoka 2012), and four in Chinese (Cuihua 2009; Dongling 2017; Liang 2013; Shimei 2014). Two are from the USA (Niles 2003; Vazquez 2003), one from India (Gupta 2016), one from Russia (Rostoka 2012), and four from China (Cuihua 2009; Dongling 2017; Liang 2013; Shimei 2014).
Ongoing studies
There are 18 ongoing studies (CTRI/2014/04/004519; CTRI/2018/05/014049; CTRI/2018/06/014686; DRKS00010618; IRCT201105136466N1; IRCT2014121520314N1; IRCT2015030921395N1; IRCT2016012026122N1; ISRCTN67671859; ISRCTN74655176; ISRCTN75902618; NCT02794766; NCT03031756; NCT03053882; NCT03160573; NCT03468595; TCTR20151109001; UMIN000023832).
Excluded studies
We have excluded 99 studies (104 reports): 52 studies were excluded because of short duration of intervention, either single dose or dose for less than a week duration, or outcomes were measured immediately after the intervention (Ademovski 2016; Alqumber 2014; Badanjak 2016; Bordas 2008; Boulware 1984; Carvalho 2004; Chen 2010; DRKS00005334; Farrell 2006; Farrell 2007; Frascella 1998; Frascella 2000; Farrell 2008; Feng 2010; Gerlach 1998; Greenstein 1997; Haas 2007; Leal 2019; Lodhia 2008; Nakano 2016; NCT00250289; NCT03346460; NCT03656419; NCT00655772; NCT00875927; Newby 2008; Pitts 1981; Porciani 2012; Reingewirtz 1999; Roldán 2004; Rolla 2002; Rosenberg 1992; Rosing 2009; Saad 2011; Saad 2016; Schmidt 1978; Seemann 2001; Sharma 1999; Sharma 2007; Shin 2011; Shinada 2008; Sterer 2008; Sterer 2013; Thrane 2010; Tian 2013; Uchida 1973; UMIN000002713; Wild 2001; Wilhelm 2010; Wilhelm 2013; Yaegaki 1992; Yoshimatsu 2007). 16 studies included participants with physiological malodour and thus were excluded (Faveri 2006; Keller 2012; Mendes 2016; NCT00748943; NL3100 (NTR3240); Peruzzo 2007; Peruzzo 2008; Quirynen 2002; Shinada 2010; Soares 2015; Steenberghe 2001; Tolentino 2011; Troccaz 2011; UMIN000002145; Van der Sluijs 2018; Wåler 1997). One study included pregnant women (Sheikh 2016). Six trials checked the outcomes related to the bacterial count (Fine 2005; NCT02194621; Quirynen 2004; Sreenivasan 2003; Sreenivasan 2004; Thaweboon 2011). Nine studies were excluded as the participants had advanced periodontitis (Betsy 2014; Moreno 2005; NCT02789436; Penala 2016; Silveira 2014; Silveria 2017; Soares 2015a; Quirynen 2005; Wang 2015). Six studies induced halitosis by requesting the participants to refrain from brushing (Brunette 1998; Codipilly 2004; Pedrazzi 2004; Seemann 2001a; Tamaki 2007; Yoshimatsu 2006). Five studies included patients with secondary halitosis (post‐surgical) or systemic disease and were excluded (Conceição 2008; EUCTR 2007‐003756‐11; Katsinelos 2007; NCT03591484; Polat 2008). Three studies were not related to halitosis outcome (Hu 2013; Malhotra 2011a; Wessel 2017), and one was an abstract publication (Mousquer 2017).
Risk of bias in included studies
We assessed three studies as at low risk of bias overall (Feres 2015; Lee 2018; Marchetti 2015). 16 studies had high risk of bias (An 2011; Asokan 2011; Aung 2015; Caygur 2017; Dadamio 2013; Iha 2013; Iwamura 2016; Mamgain 2016; NCT02628938; Nishihira 2017; Nohno 2012; Patil 2017; Payne 2011; Satthanakul 2014; Wang 2017; Wilhelm 2012) and the remaining 25 studies had unclear risk of bias (Figure 2).
2.
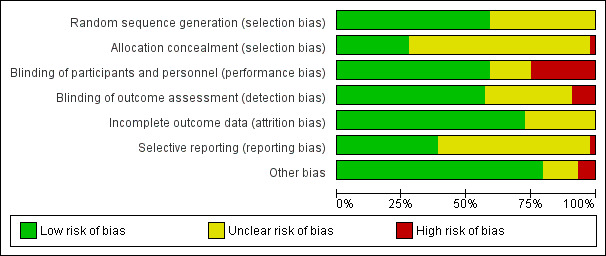
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
32 studies had unclear risk of bias either in random sequence generation or allocation concealment processes (Acar 2019; Ademovski 2012; Ademovski 2017; Asokan 2011; Borden 2002; Caygur 2017; Garcia 2014; Hu 2005; Hu 2018; Iwamura 2016; Kara 2008; Kozlovsky 1996; Lomax 2017; López Jornet 2003; Mamgain 2016; Nakano 2017; Navada 2008; NCT02628938; Niles 1999; Nogueira‐Filho 2002; Nohno 2012; Rassameemasmaung 2007; Rassameemasmaung 2012; Satthanakul 2014; Suzuki 2014; Talebian 2009; Tanaka 2010; Wang 2017; Watanabe 2018; Wigger‐Alberti 2010; Wilhelm 2012; Winkel 2003). One study (Payne 2011) had high risk of selection bias and 11 studies had low risk of selection bias (Figure 3).
3.
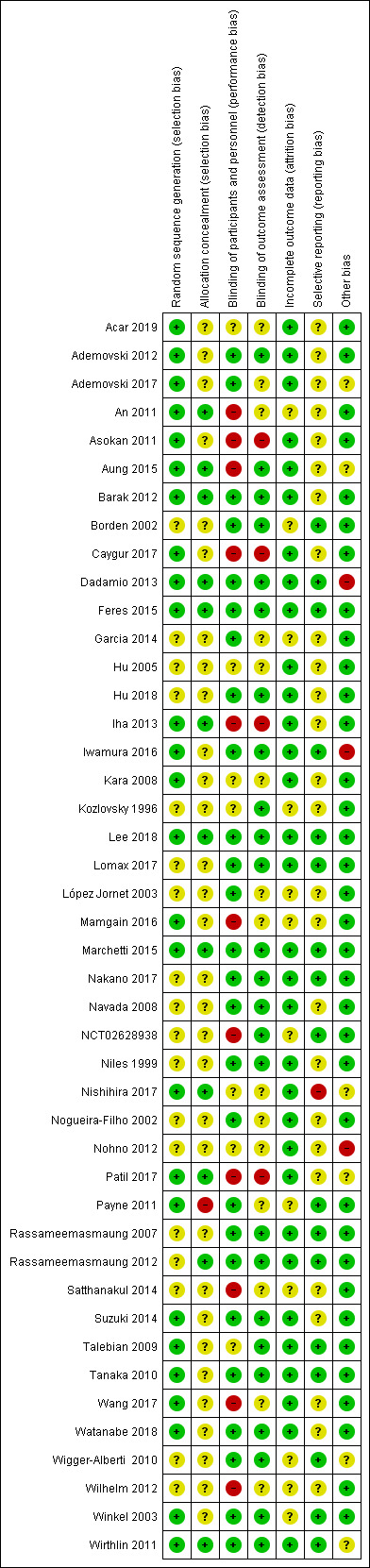
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Blinding
12 studies had either unclear risk of performance bias or unclear risk of detection bias (Acar 2019; Ademovski 2017; Garcia 2014; Hu 2005; Kara 2008; Kozlovsky 1996; López Jornet 2003; Nishihira 2017; Nogueira‐Filho 2002; Nohno 2012; Payne 2011; Talebian 2009). 11 studies had high risk of performance or detection bias (An 2011; Asokan 2011; Aung 2015; Caygur 2017; Iha 2013; Mamgain 2016; NCT02628938; Patil 2017; Satthanakul 2014; Wang 2017; Wilhelm 2012), and the remaining 21 studies had low risk of bias in blinding (Figure 3)
Incomplete outcome data
12 studies had unclear risk of attrition bias (An 2011; Borden 2002; Garcia 2014; Kozlovsky 1996; López Jornet 2003; Mamgain 2016; NCT02628938; Payne 2011; Satthanakul 2014; Wigger‐Alberti 2010; Wilhelm 2012; Winkel 2003). None of the studies had high risk of attrition bias and the remaining 32 studies had low risk of attrition bias (Figure 3).
Selective reporting
26 studies had unclear risk of reporting bias (Acar 2019; Ademovski 2012; Ademovski 2017; An 2011; Asokan 2011; Aung 2015; Barak 2012; Caygur 2017; Garcia 2014; Hu 2005; Hu 2018; Iha 2013; Kara 2008; Kozlovsky 1996; López Jornet 2003; Mamgain 2016; Navada 2008; Niles 1999; Nogueira‐Filho 2002; Nohno 2012; Patil 2017; Satthanakul 2014; Suzuki 2014; Wang 2017; Watanabe 2018; Wilhelm 2012), and one study had high risk of reporting bias (Nishihira 2017). The remaining 17 studies had low risk of reporting bias (Figure 3).
Other potential sources of bias
Six studies had unclear risk of other biases (Ademovski 2017; Aung 2015; Nishihira 2017; Patil 2017; Wigger‐Alberti 2010; Wirthlin 2011). Three studies had high risk of other biases (Dadamio 2013; Iwamura 2016; Nohno 2012), and the remaining 35 studies had low risk of other biases (Figure 3).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7
Out of 44 included studies, we could analyse results from only 30 studies (38 reports). We could not use the data from the other 14 studies (17 reports): we could not analyse data from Barak 2012; Garcia 2014 and López Jornet 2003 because of the missing SD and P values. Three studies (Marchetti 2015; Nakano 2017; Talebian 2009) did not give any data that could be used in the meta‐analysis. Asokan 2011 did not give post‐intervention OLT score and P value and hence could not be included in the meta‐analysis. Suzuki 2014 did not give data that could be used in the meta‐analysis and there was no colour difference in the graph and hence we could not extract the data from the graph. Payne 2011 gave the adjusted mean VSC scores in a graph and hence we could not use the data in the meta‐analysis. We could not calculate mean difference and impute correlation coefficient for Ademovski 2012; Niles 1999; Nogueira‐Filho 2002 and Wilhelm 2012 as there was no correlation coefficient reported. We could not find a similar intervention trial to impute the SD of differences. We calculated the data from the graph (Additional Table 8), however, we did not include the data from Wigger‐Alberti 2010 as the report did not give details of sample size per group.
1. Wigger‐Alberti 2010 data.
| Mouthwash used | Median | Q1 | Q2 | Mean (calculated) |
| ASF | 2.419 | 0.835 | 3.568 | 3.69 |
| CHX + CPC + Zn | 2.046 | 0.714 | 3.994 | 4.43 |
| CHX | 2.143 | 0.281 | 4.275 | 5.39 |
| Tap water | 2.695 | 1.147 | 4.719 | 4.39 |
Median, Q1, Q3 for 7 days follow‐up calculated from the graph using PlotDigitizer software. ASF = amine fluoride/stannous fluoride; CHX = chlorhexidine; CPC = cetylpyridinium chloride; Zn = zinc.
We categorised the interventions found in the included studies under eight broad types and have explained the results based on the type of intervention as follows.
Mechanical debridement.
Chewing gum.
Systemic deodorising agent.
Topical agents.
Toothpaste.
Mouthrinse/mouthwash.
Tablets.
Combination methods.
We could not combine the interventions because the majority of the included trials had heterogenous interventions or control. As most of the trials reported data at multiple time points, the clinically relevant follow‐up time was considered in the meta‐analysis as described by the Cochrane Handbook for Systematic Reviews of Interventions Section 9.3.4 (Higgins 2011). We analysed data from cross‐over trials and parallel‐arm trials separately (Section 16.4.7, Higgins 2011). We did 'Summary of findings' tables for the most commonly used interventions with clinical outcomes. We discussed all the outcomes separately in the individual comparisons for ease of understanding. None of the included studies reported data on the outcome quality of life. Seven studies reported adverse events, other studies have either not given the details of adverse events or no adverse events were reported.
1. Mechanical debridement
1a. SRP + air polishing versus SRP: under this comparison, we had one trial (Caygur 2017) in which VSC was the outcome assessed. In this trial, SRP along with glycine powder air polishing was compared with SRP alone to see the effect on the VSC in halitosis patients. Using glycine powder air polishing adjunctively with SRP had no beneficial effects on halitosis when compared to SRP alone (mean difference (MD) ‐3.87; 95% confidence interval (CI) ‐17.93 to 10.19; 1 trial; 60 participants; 30 days follow‐up; Analysis 1.1).
1.1. Analysis.
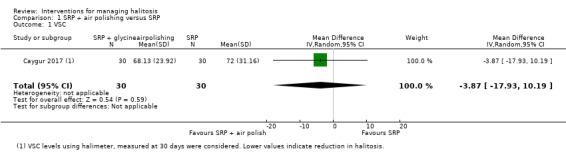
Comparison 1 SRP + air polishing versus SRP, Outcome 1 VSC.
1b. SRP + laser versus SRP: one trial (Kara 2008) assessed VSC under this comparison as outcome. The effect estimate for this outcome showed improvement in SRP + laser group compared to SRP group. However, the confidence interval crossed the line of no effect (MD ‐3.30; 95% CI ‐9.38 to 2.78; 1 trial; 40 participants; 4 weeks follow‐up; Analysis 2.1).
2.1. Analysis.

Comparison 2 SRP + laser versus SRP, Outcome 1 VSC.
1c. Mechanical tongue cleaning versus no tongue cleaning: we have three trials under this comparison with two outcomes, VSC and OLT score. Acar 2019 and Wang 2017 were parallel‐arm trials and were analysed together.
VSC scores showed improvement in the intervention group with wider confidence intervals crossing the line of no effect (MD ‐7.69; 95% CI ‐47.08 to 31.69; 2 trials; 46 participants; 1 week follow‐up; Analysis 3.1).
3.1. Analysis.
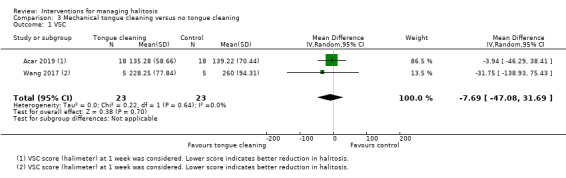
Comparison 3 Mechanical tongue cleaning versus no tongue cleaning, Outcome 1 VSC.
OLT scores in parallel‐arm and cross‐over trials showed improvement in the intervention group (MD ‐0.20; 95% CI ‐0.34 to ‐0.07; 2 trials; 46 participants; 1 week follow‐up; Analysis 3.2).
3.2. Analysis.
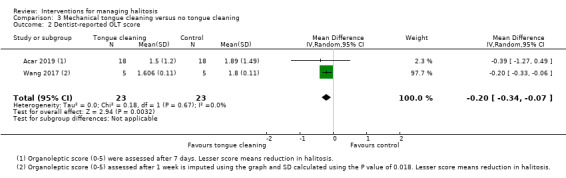
Comparison 3 Mechanical tongue cleaning versus no tongue cleaning, Outcome 2 Dentist‐reported OLT score.
2. Chewing gum
2a. 0.6% eucalyptus chewing gum versus 0.4% eucalyptus chewing gum: one trial (Tanaka 2010) under this comparison reported two outcomes, VSC and OLT score. The effect estimate for OLT scores showed marginal improvement with wide confidence intervals crossing the line of no effect, in the 0.6% chewing gum group compared to 0.4% chewing gum group (MD ‐0.10; 95% CI ‐0.37 to 0.17; 1 trial; 64 participants; 4 weeks follow‐up; Analysis 4.1). However, the effect estimate for VSC did not show any improvement in the 0.6% chewing gum group (MD 0.00; 95% CI ‐0.21 to 0.21; 1 trial; 64 participants; 4 weeks follow‐up; Analysis 4.2).
4.1. Analysis.
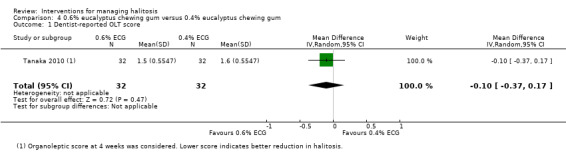
Comparison 4 0.6% eucalyptus chewing gum versus 0.4% eucalyptus chewing gum, Outcome 1 Dentist‐reported OLT score.
4.2. Analysis.
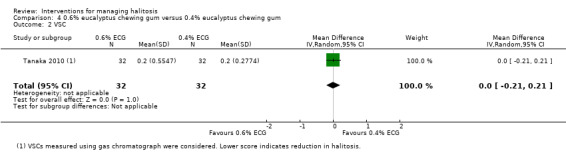
Comparison 4 0.6% eucalyptus chewing gum versus 0.4% eucalyptus chewing gum, Outcome 2 VSC.
2b. 0.6% eucalyptus chewing gum versus placebo chewing gum: one trial (Tanaka 2010) under this comparison reported two outcomes, VSC and OLT score. The effect estimate for OLT scores showed marginal improvement with wide confidence intervals crossing the line of no effect, in the 0.6% chewing gum group compared to placebo chewing gum group (MD ‐0.10; 95% CI ‐0.31 to 0.11; 1 trial; 65 participants; 4 weeks follow‐up; Analysis 5.1). However, the effect estimate for VSC did not show any improvement in the 0.6% chewing gum group (MD 0.00; 95% CI ‐0.21 to 0.21; 1 trial; 65 participants; 4 weeks follow‐up; Analysis 5.2).
5.1. Analysis.
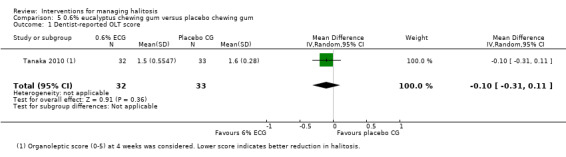
Comparison 5 0.6% eucalyptus chewing gum versus placebo chewing gum, Outcome 1 Dentist‐reported OLT score.
5.2. Analysis.
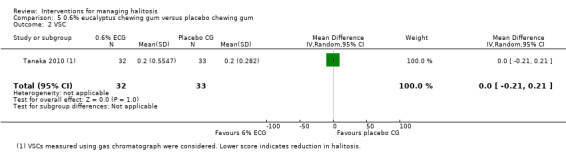
Comparison 5 0.6% eucalyptus chewing gum versus placebo chewing gum, Outcome 2 VSC.
2c. Pycnogenol chewing gum versus placebo chewing gum: one trial (Watanabe 2018) reported each component of VSC as the outcome under this comparison. The effect estimates are given for hydrogen sulphide, methyl mercaptan and methyl sulphide separately. All three components of VSC decreased in the intervention group compared to the placebo group. In the hydrogen sulphide outcome, the confidence intervals were wide and did not cross the line of no effect (MD ‐114.90; 95% CI ‐206.59 to ‐23.21; 1 trial; 21 participants; 4 weeks follow‐up; Analysis 6.1). However, in methyl mercaptan and methyl sulphide outcomes, the effect estimates showed wider confidence intervals crossing the line of no effect (MD ‐8.40; 95% CI ‐24.95 to 8.15; 1 trial; 21 participants; 4 weeks follow‐up; Analysis 6.2 and MD ‐4.70; 95% CI ‐27.01 to 17.61; 1 trial; 21 participants; 4 weeks follow‐up; Analysis 6.3 respectively).
6.1. Analysis.
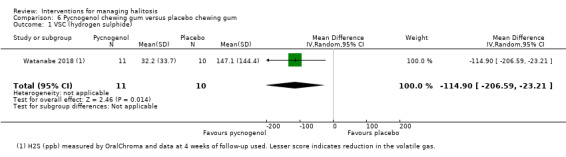
Comparison 6 Pycnogenol chewing gum versus placebo chewing gum, Outcome 1 VSC (hydrogen sulphide).
6.2. Analysis.

Comparison 6 Pycnogenol chewing gum versus placebo chewing gum, Outcome 2 VSC (methyl mercaptan).
6.3. Analysis.
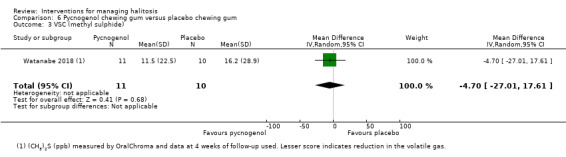
Comparison 6 Pycnogenol chewing gum versus placebo chewing gum, Outcome 3 VSC (methyl sulphide).
3. Systemic deodorising agent
3a. 1000 mg champignon extract versus placebo: one trial (Nishihira 2017) reported patient score and patient's family member score in VAS. The effect estimates for both the outcomes showed marginal decrease of halitosis in the intervention group with wide confidence intervals crossing the line of no effect (MD ‐1.07; 95% CI ‐14.51 to 12.37; 1 trial; 40 participants; 2 weeks follow‐up; Analysis 7.1 and MD ‐1.74; 95% CI ‐15.52 to 12.04; 1 trial; 40 participants; 2 weeks follow‐up; Analysis 7.2 respectively).
7.1. Analysis.
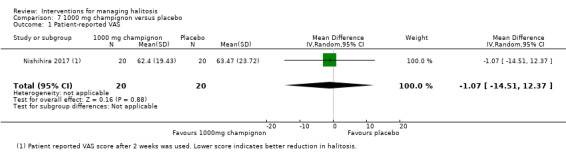
Comparison 7 1000 mg champignon versus placebo, Outcome 1 Patient‐reported VAS.
7.2. Analysis.
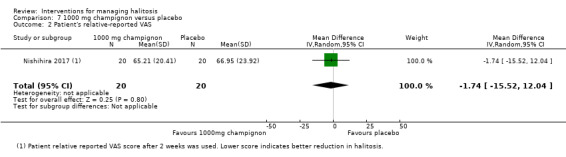
Comparison 7 1000 mg champignon versus placebo, Outcome 2 Patient's relative‐reported VAS.
3b. 1000 mg champignon versus 50 mg champignon extract: one trial (Nishihira 2017) reported patient score and patient's family member score in VAS. The effect estimates for both the outcomes showed marginal decrease of halitosis in the intervention group with wide confidence intervals crossing the line of no effect (MD ‐5.32; 95% CI ‐18.14 to 7.50; 1 trial; 40 participants; 2 weeks follow‐up; Analysis 8.1 and MD ‐0.61; 95% CI ‐15.58 to 14.36; 1 trial; 40 participants; 2 weeks follow‐up; Analysis 8.2 respectively).
8.1. Analysis.
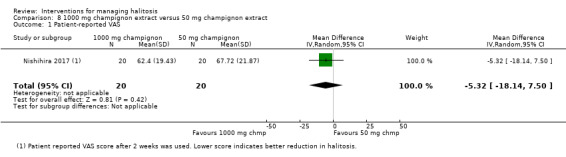
Comparison 8 1000 mg champignon extract versus 50 mg champignon extract, Outcome 1 Patient‐reported VAS.
8.2. Analysis.
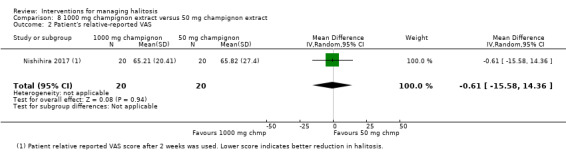
Comparison 8 1000 mg champignon extract versus 50 mg champignon extract, Outcome 2 Patient's relative‐reported VAS.
4. Topical agents
4a. Hinokitiol gel versus placebo gel: one trial (Iha 2013) reported OLT scores and scores of two components of VSC (hydrogen sulphide and methyl mercaptan) for this comparison. The effect estimates for all three outcomes showed marginal decrease of halitosis in the hinokitiol gel group compared to placebo group with wide confidence intervals crossing the line of no effect (MD ‐0.27; 95% CI ‐1.26 to 0.72; 1 trial; 18 participants; 28 days follow‐up; Analysis 9.1, MD ‐2.13; 95% CI ‐5.33 to 1.08; 1 trial; 18 participants; 28 days follow‐up; Analysis 9.2 and MD ‐1.64; 95% CI ‐5.77 to 2.49; 1 trial; 18 participants; 28 days follow‐up; Analysis 9.3 respectively).
9.1. Analysis.
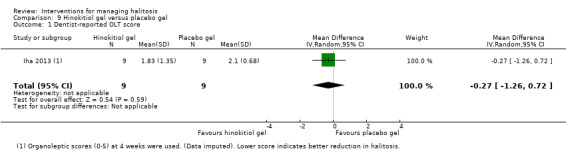
Comparison 9 Hinokitiol gel versus placebo gel, Outcome 1 Dentist‐reported OLT score.
9.2. Analysis.
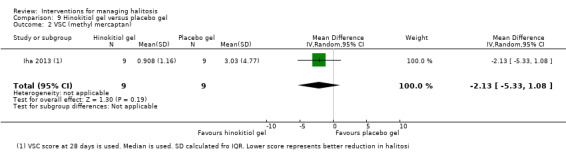
Comparison 9 Hinokitiol gel versus placebo gel, Outcome 2 VSC (methyl mercaptan).
9.3. Analysis.
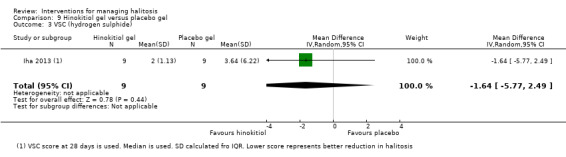
Comparison 9 Hinokitiol gel versus placebo gel, Outcome 3 VSC (hydrogen sulphide).
4b. G32 versus chlorhexidine gel: one trial (Patil 2017) reported VSC score as the outcome under this comparison. The effect estimate for this outcome showed marginal improvement in control (chlorhexidine gel) group compared to the intervention (G32 tablets) group (MD 0.05; 95%CI ‐0.28 to 0.38; 1 trial; 40 participants; 1 week follow‐up; Analysis 10.1). Regarding adverse events, Patil 2017 reported burning mucosa and drying of mouth in a few subjects using the control drug (chlorhexidine) and no adverse effects were reported in the intervention group (G32 tablets).
10.1. Analysis.
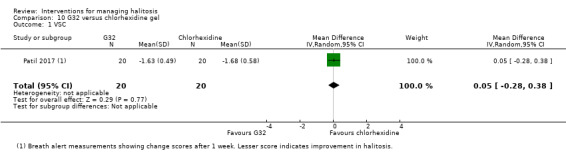
Comparison 10 G32 versus chlorhexidine gel, Outcome 1 VSC.
5. Toothpaste
5a. Triclosan + PVM/MA toothpaste versus control toothpaste: one trial (Hu 2005) reported OLT scores as reported by odour judges. The effect estimate for this outcome showed improvement in the intervention group compared to control group (MD ‐3.48; 95% CI ‐3.77 to ‐3.19; 1 trial; 81 participants; 1 week follow‐up; Analysis 11.1).
11.1. Analysis.
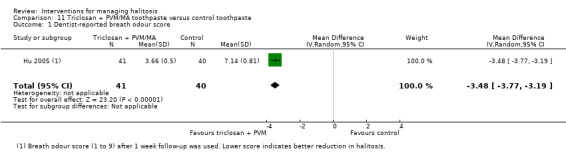
Comparison 11 Triclosan + PVM/MA toothpaste versus control toothpaste, Outcome 1 Dentist‐reported breath odour score.
5b. Zinc toothpaste versus placebo toothpaste: one trial (Navada 2008) reported OLT score and VSC score for this comparison. The effect estimates for OLT and VSC outcomes showed improvement in the intervention group compared to the control group (MD ‐1.31; 95% CI ‐1.39 to ‐1.23; 1 trial; 187 participants; 4 weeks follow‐up; Analysis 12.1 and MD ‐11.30; 95% CI ‐20.45 to ‐2.15; 1 trial; 188 participants; 4 weeks follow‐up; Analysis 12.2 respectively).
12.1. Analysis.
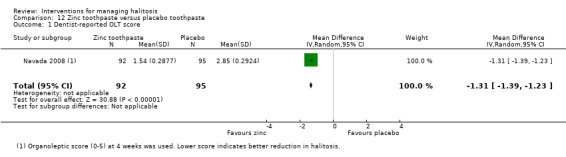
Comparison 12 Zinc toothpaste versus placebo toothpaste, Outcome 1 Dentist‐reported OLT score.
12.2. Analysis.
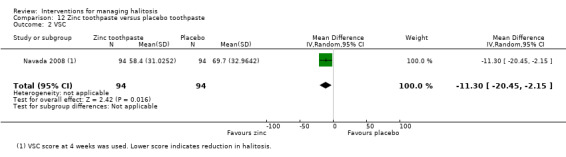
Comparison 12 Zinc toothpaste versus placebo toothpaste, Outcome 2 VSC.
5c. Sodium bicarbonate toothpaste versus control toothpaste: one trial (Lomax 2017) reported VSC score for this comparison. The effect estimate showed improvement in the placebo group compared to the intervention group with wide confidence interval crossing the line of no effect (MD 105.80; 95% CI ‐16.20 to 227.80; 1 trial; 148 participants; 6 weeks follow‐up; Analysis 13.1). Adverse events reported by Lomax 2017 were not related to the interventions.
13.1. Analysis.
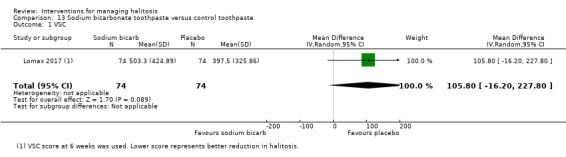
Comparison 13 Sodium bicarbonate toothpaste versus control toothpaste, Outcome 1 VSC.
5d. Dual zinc + arginine dentifrice versus control dentifrice: one trial (Hu 2018) reported OLT hedonic ratings. The effect estimate showed improvement in the intervention group compared to the control group (MD ‐2.00; 95% CI ‐2.19 to ‐1.81; 1 trial; 80 participants; 3 weeks follow‐up; Analysis 14.1).
14.1. Analysis.
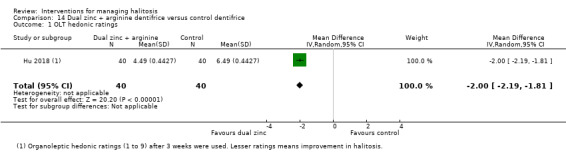
Comparison 14 Dual zinc + arginine dentifrice versus control dentifrice, Outcome 1 OLT hedonic ratings.
6. Mouthrinse/mouthwash
Intervention mouthwash versus placebo mouthwash
6a. Halita versus placebo mouthwash: one trial (Winkel 2003) reported OLT score and VSC score as outcomes for this comparison. Both the effect estimates showed improvement in the intervention group compared to placebo group (MD ‐1.00; 95% CI ‐1.65 to ‐0.35; 1 trial; 40 participants; 2 weeks follow‐up; Analysis 15.1 and MD ‐188.00; 95% CI ‐308.29 to ‐67.71; 1 trial; 40 participants; 2 weeks follow‐up; Analysis 15.2 respectively). Regarding adverse events, Winkel 2003 reported tongue staining was seen in patients who gargled, rather than rinsed in the halita mouthwash group.
15.1. Analysis.
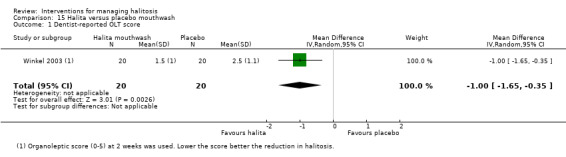
Comparison 15 Halita versus placebo mouthwash, Outcome 1 Dentist‐reported OLT score.
15.2. Analysis.
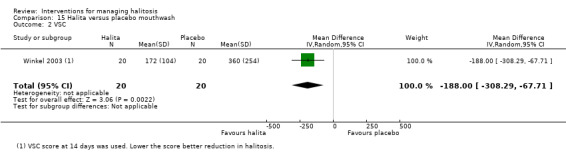
Comparison 15 Halita versus placebo mouthwash, Outcome 2 VSC.
6b. Chlorhexidine + zinc acetate mouthwash versus placebo mouthwash: one trial (Ademovski 2017) reported OLT score as outcome for this comparison. The effect estimate showed improvement in the intervention group compared to placebo group, however the confidence intervals crossed the line of no effect (MD ‐0.20; 95% CI ‐0.58 to 0.18; 1 trial; 44 participants; 3 months follow‐up; Analysis 16.1).
16.1. Analysis.
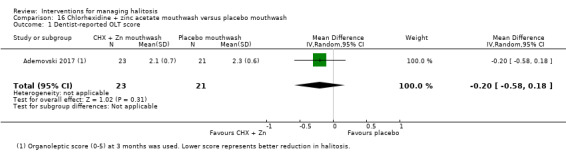
Comparison 16 Chlorhexidine + zinc acetate mouthwash versus placebo mouthwash, Outcome 1 Dentist‐reported OLT score.
6c. Cetylperidinium chloride mouthwash versus placebo mouthwash: one trial (Borden 2002) reported OLT and VSC scores as outcomes for this comparison. The effect estimates showed improvement in the intervention group compared to placebo group (MD ‐0.50; 95% CI ‐0.83 to ‐0.17; 1 trial; 47 participants; 2 weeks follow‐up; Analysis 17.1 and MD ‐20.04; 95% CI ‐37.71 to ‐2.37; 1 trial; 47 participants; 2 weeks follow‐up; Analysis 17.2 respectively). Adverse events reported by Borden 2002 were not related to the interventions.
17.1. Analysis.
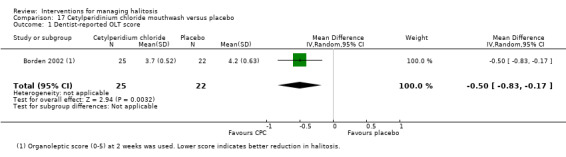
Comparison 17 Cetylperidinium chloride mouthwash versus placebo, Outcome 1 Dentist‐reported OLT score.
17.2. Analysis.
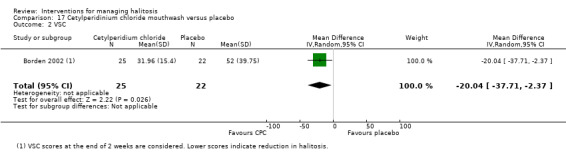
Comparison 17 Cetylperidinium chloride mouthwash versus placebo, Outcome 2 VSC.
6d. Essential oil mouthwash versus placebo mouthwash: one trial (Borden 2002) reported OLT and VSC scores as outcomes for this comparison. The effect estimates showed improvement in the intervention group compared to placebo group, however the confidence intervals crossed the line of no effect (MD ‐0.09; 95% CI ‐0.47 to 0.29; 1 trial; 45 participants; 2 weeks follow‐up; Analysis 18.1 and MD ‐5.13; 95% CI ‐32.94 to 22.68; 1 trial; 45 participants; 2 weeks follow‐up; Analysis 18.2 respectively). Adverse events reported by Borden 2002 were not related to the interventions.
18.1. Analysis.
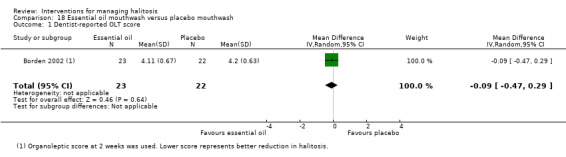
Comparison 18 Essential oil mouthwash versus placebo mouthwash, Outcome 1 Dentist‐reported OLT score.
18.2. Analysis.
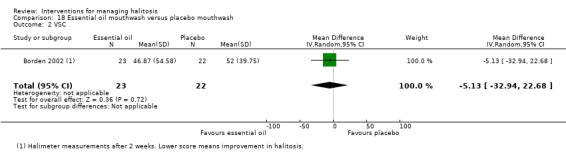
Comparison 18 Essential oil mouthwash versus placebo mouthwash, Outcome 2 VSC.
6e. Chlorine dioxide + zinc mouthwash versus placebo mouthwash: one trial (Borden 2002) reported both OLT and VSC scores as outcomes for this comparison. In this trial, both outcomes (OLT and VSC) showed improvement in the intervention group, however the confidence interval was crossing the line of no control in OLT outcome (MD ‐0.17; 95% CI ‐0.59 to 0.25; 1 trial; 41 participants; 2 weeks follow‐up; Analysis 19.1 and MD ‐20.53; 95% CI ‐38.52 to ‐2.54; 1 trial; 41 participants; 2 weeks follow‐up; Analysis 19.2 respectively). Adverse events reported by Borden 2002 were not related to the interventions.
19.1. Analysis.
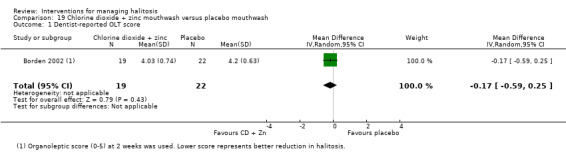
Comparison 19 Chlorine dioxide + zinc mouthwash versus placebo mouthwash, Outcome 1 Dentist‐reported OLT score.
19.2. Analysis.
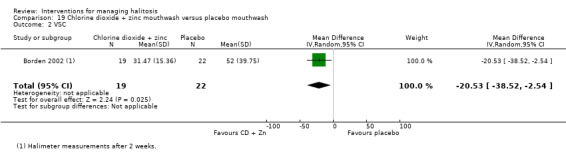
Comparison 19 Chlorine dioxide + zinc mouthwash versus placebo mouthwash, Outcome 2 VSC.
6f. Chlorine dioxide mouthwash versus placebo mouthwash: one trial (Lee 2018) reported OLT score as outcome for this comparison. The effect estimates showed improvement in the intervention group compared to placebo group (MD ‐0.61; 95% CI ‐0.73 to ‐0.49; 1 trial; 47 participants; 3 weeks follow‐up; Analysis 20.1). However, when week 6 data were used, the effect estimate favoured the intervention group with 95% CI crossing the line of no effect.
20.1. Analysis.

Comparison 20 Chlorine dioxide mouthwash versus placebo, Outcome 1 Dentist‐reported OLT score.
6g. Herbal mouthwash versus placebo mouthwash: one trial (Rassameemasmaung 2007) reported VSC score as outcome for this comparison. The effect estimates showed improvement in the intervention group compared to placebo group (MD ‐70.29; 95% CI ‐121.01 to ‐19.57; 1 trial; 60 participants; 15 days follow‐up; Analysis 21.1).
21.1. Analysis.
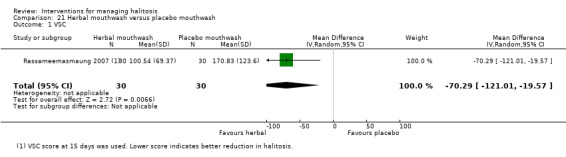
Comparison 21 Herbal mouthwash versus placebo mouthwash, Outcome 1 VSC.
6h. Benzethonium chloride mouthwash versus placebo mouthwash: one trial (Iwamura 2016) reported VSC scores of individual gases as outcomes for this comparison. The effect estimate showed no improvement in the intervention group compared to placebo group for the VSC score of methyl mercaptan (MD 7.20; 95% CI ‐24.92 to 39.32; 1 trial; 20 participants; 9 days follow‐up; Analysis 22.1). The effect estimates showed improvement in the intervention group compared to placebo group for the VSC scores of hydrogen sulphide and dimethyl sulphide and the confidence intervals crossed the line of no effect for both the outcomes (MD ‐125.10; 95% CI ‐286.32 to 36.12; 1 trial; 20 participants; 9 days follow‐up; Analysis 22.2 and MD ‐0.03; 95% CI ‐0.63 to 0.57; 1 trial; 20 participants; 9 days follow‐up; Analysis 22.3 respectively).
22.1. Analysis.
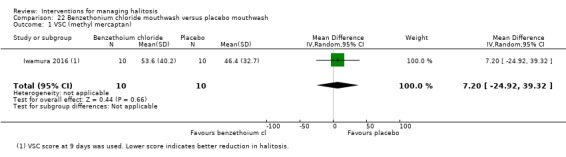
Comparison 22 Benzethonium chloride mouthwash versus placebo mouthwash, Outcome 1 VSC (methyl mercaptan).
22.2. Analysis.
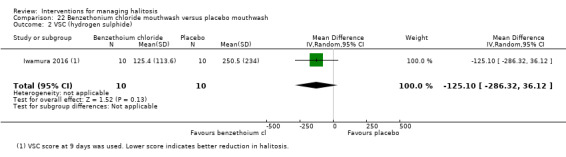
Comparison 22 Benzethonium chloride mouthwash versus placebo mouthwash, Outcome 2 VSC (hydrogen sulphide).
22.3. Analysis.
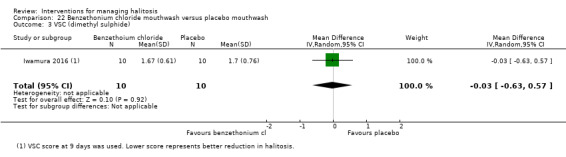
Comparison 22 Benzethonium chloride mouthwash versus placebo mouthwash, Outcome 3 VSC (dimethyl sulphide).
6i. Green tea mouthwash versus placebo mouthwash: one trial (Rassameemasmaung 2012) reported VSC score as the outcome for this comparison. The effect estimates showed improvement in the intervention group compared to placebo group, however the confidence intervals crossed the line of no effect (MD ‐57.39; 95% CI ‐184.63 to 69.85; 1 trial; 60 participants; 28 days follow‐up; Analysis 23.1).
23.1. Analysis.
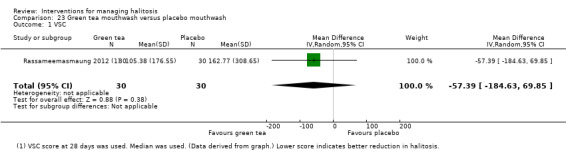
Comparison 23 Green tea mouthwash versus placebo mouthwash, Outcome 1 VSC.
6j. Lemongrass mouthwash versus placebo mouthwash: one trial (Satthanakul 2014) reported VSC score as the outcome for this comparison. The effect estimates showed improvement in the intervention group compared to placebo group (MD ‐26.66; 95% CI ‐43.39 to ‐9.93; 1 trial; 20 participants; 8 days follow‐up; Analysis 24.1).
24.1. Analysis.
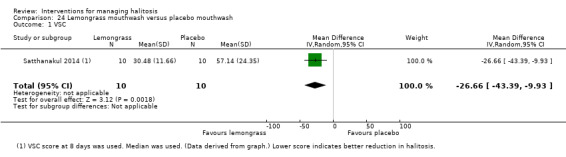
Comparison 24 Lemongrass mouthwash versus placebo mouthwash, Outcome 1 VSC.
Intervention mouthwash versus control mouthwash
6k. Cetylpyridinium chloride mouthwash versus chlorhexidine + zinc mouthwash: one trial (Borden 2002) reported OLT and VSC scores as the outcomes for this comparison. The OLT effect estimate showed improvement in the cetylpyridinium chloride group compared to chlorhexidine + zinc group and the VSC score showed no improvement in the intervention group compared to control group. However, the confidence intervals in both the outcomes crossed the line of no effect (MD ‐0.33; 95% CI ‐0.72 to 0.06; 1 trial; 44 participants; 2 weeks follow‐up; Analysis 25.1 and MD 0.49; 95% CI ‐8.68 to 9.66; 1 trial; 44 participants; 2 weeks follow‐up; Analysis 25.2 respectively). Adverse events reported by Borden 2002 were not related to the interventions.
25.1. Analysis.
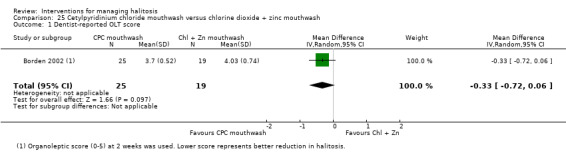
Comparison 25 Cetylpyridinium chloride mouthwash versus chlorine dioxide + zinc mouthwash, Outcome 1 Dentist‐reported OLT score.
25.2. Analysis.
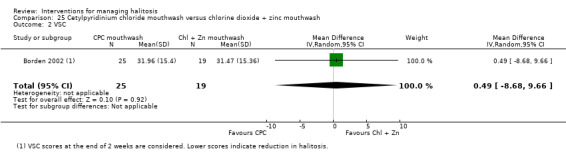
Comparison 25 Cetylpyridinium chloride mouthwash versus chlorine dioxide + zinc mouthwash, Outcome 2 VSC.
6l. Halita mouthrinse versus Perio‐plus mouthrinse: one trial (Dadamio 2013) reported OLT and VSC scores as the outcomes for this comparison. The effect estimates for both the outcomes showed improvement in the halita group compared to Perio‐plus mouthrinse, however the confidence intervals crossed the line of no effect (MD ‐0.20; 95% CI ‐0.86 to 0.46; 1 trial; 36 participants; 8 days follow‐up; Analysis 26.1 and MD ‐25.00; 95% CI ‐64.21 to 14.21; 1 trial; 36 participants; 8 days follow‐up; Analysis 26.2 respectively). Regarding adverse events, one patient from each group reported unpleasant feeling after the use of the product and one patient from the halita mouthrinse group reported tooth staining. There were no severe adverse events reported.
26.1. Analysis.
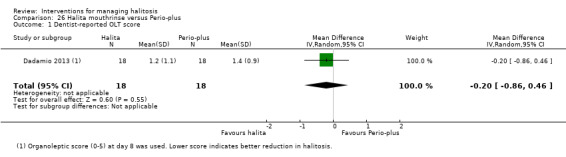
Comparison 26 Halita mouthrinse versus Perio‐plus, Outcome 1 Dentist‐reported OLT score.
26.2. Analysis.
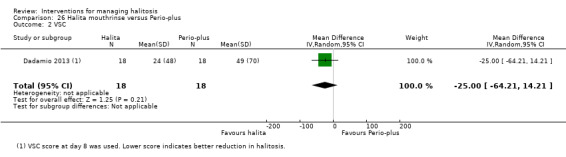
Comparison 26 Halita mouthrinse versus Perio‐plus, Outcome 2 VSC.
6m. Oil water two‐phase mouthwash versus control mouthwash: one trial (Kozlovsky 1996) reported VSC score as the outcome for this comparison. The effect estimates showed improvement in the oil water two‐phase mouthwash group compared to control group, however the confidence intervals crossed the line of no effect (MD ‐11.00; 95% CI ‐25.26 to 3.26; 1 trial; 50 participants; 1 week follow‐up; Analysis 27.1).
27.1. Analysis.
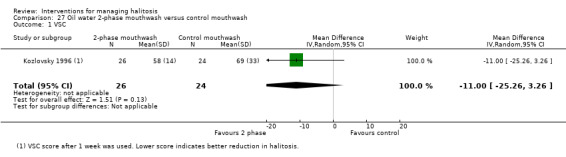
Comparison 27 Oil water 2‐phase mouthwash versus control mouthwash, Outcome 1 VSC.
6n. Triphala and Ela decoction versus chlorhexidine mouthwash: one trial (Mamgain 2016) reported OLT score as the outcome for this comparison. The effect estimates showed no improvement in the Triphala and Ela decoction group compared to chlorhexidine group (MD 0.20; 95% CI 0.09 to 0.31; 1 trial; 60 participants; 14 days follow‐up; Analysis 28.1).
28.1. Analysis.
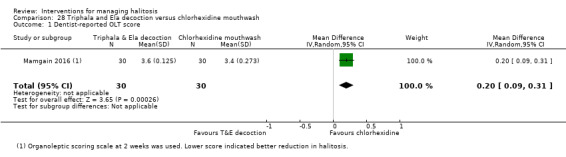
Comparison 28 Triphala and Ela decoction versus chlorhexidine mouthwash, Outcome 1 Dentist‐reported OLT score.
6o. Miswak mouthwash versus chlorhexidine mouthwash: one unpublished trial (NCT02628938) reported OLT and VSC scores and patient self‐assessment scores as the outcomes for this comparison. The effect estimate of the OLT outcome showed marginal improvement and effect estimates of the other two outcomes showed no improvement for the miswak mouthwash compared to chlorhexidine mouthwash (MD 0.01; 95% CI ‐0.95 to 0.97; 1 trial; 21 participants; 1 week follow‐up; Analysis 29.1, MD ‐0.20; 95% CI ‐1.03 to 0.63; 1 trial; 21 participants; 1 week follow‐up; Analysis 29.2 and MD ‐0.18; 95% CI ‐1.59 to 1.23; 1 trial; 21 participants; 1 week follow‐up; Analysis 29.3 respectively).
29.1. Analysis.
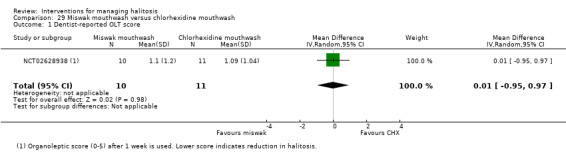
Comparison 29 Miswak mouthwash versus chlorhexidine mouthwash, Outcome 1 Dentist‐reported OLT score.
29.2. Analysis.
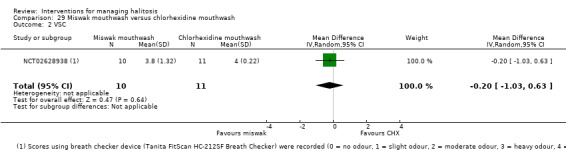
Comparison 29 Miswak mouthwash versus chlorhexidine mouthwash, Outcome 2 VSC.
29.3. Analysis.
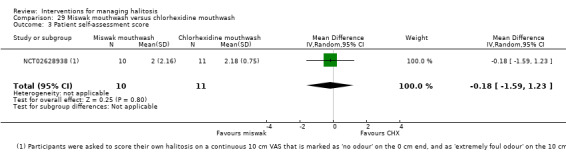
Comparison 29 Miswak mouthwash versus chlorhexidine mouthwash, Outcome 3 Patient self‐assessment score.
6p. Chlorine dioxide mouthrinse versus chlorhexidine mouthwash: one trial (Wirthlin 2011) reported VSC scores of individual gases as outcomes for this comparison. The effect estimate showed improvement in the chlorine dioxide group compared to chlorhexidine group for the VSC score of hydrogen sulphide and no improvement for the other two components of VSC (MD ‐11.00; 95% CI ‐31.61 to 9.61; 1 trial; 22 participants; 1 week follow‐up; Analysis 30.1, MD 7.63; 95% CI ‐1.70 to 16.96; 1 trial; 22 participants; 1 week follow‐up; Analysis 30.2 and MD 22.80; 95% CI ‐33.18 to 78.78; 1 trial; 22 participants; 1 week follow‐up; Analysis 30.3 respectively).Wirthlin 2011 reported altered taste sensation as the adverse event.
30.1. Analysis.
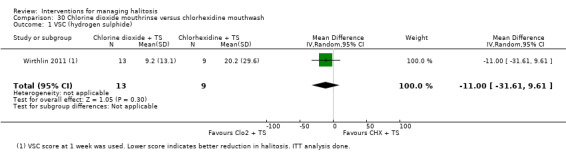
Comparison 30 Chlorine dioxide mouthrinse versus chlorhexidine mouthwash, Outcome 1 VSC (hydrogen sulphide).
30.2. Analysis.
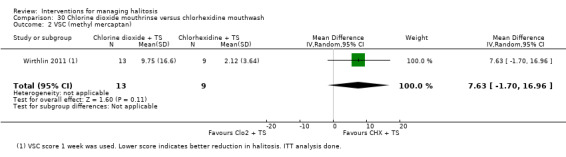
Comparison 30 Chlorine dioxide mouthrinse versus chlorhexidine mouthwash, Outcome 2 VSC (methyl mercaptan).
30.3. Analysis.
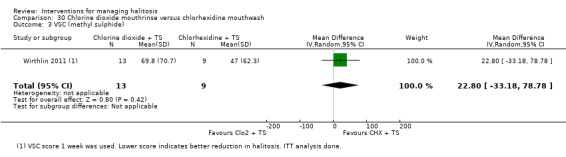
Comparison 30 Chlorine dioxide mouthrinse versus chlorhexidine mouthwash, Outcome 3 VSC (methyl sulphide).
7. Tablets
7a. Protease cysteine + actinidine versus placebo tablets: one trial (Nohno 2012) reported VSC score as the outcome for this comparison. The effect estimates showed improvement in the intervention tablets group compared to placebo group however, the confidence intervals crossed the line of no effect (MD ‐45.80; 95% CI ‐258.38 to 166.78; 1 trial; 14 participants; 1 week follow‐up; Analysis 31.1).
31.1. Analysis.
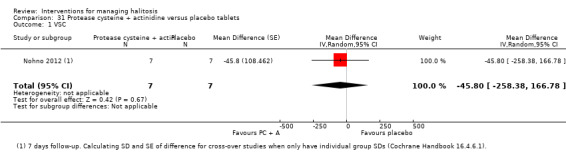
Comparison 31 Protease cysteine + actinidine versus placebo tablets, Outcome 1 VSC.
8. Combination methods
8a. Miswak stick versus chlorhexidine mouthwash: one unpublished trial (NCT02628938) reported OLT and VSC scores and patient self‐assessment scores as the outcomes for this comparison. The effect estimate of all three outcomes showed improvement in the miswak mouthwash compared to chlorhexidine mouthwash. However, the confidence intervals crossed the line of no effect in OLT and patient self‐assessment scores (MD ‐0.55; 95% CI ‐1.33 to 0.23; 1 trial; 24 participants; 1 week follow‐up; Analysis 32.1, MD ‐0.77; 95% CI ‐1.19 to ‐0.35; 1 trial; 24 participants; 1 week follow‐up; Analysis 32.2 and MD ‐0.26; 95% CI ‐1.16 to 0.64; 1 trial; 24 participants; 1 week follow‐up; Analysis 32.3 respectively).
32.1. Analysis.
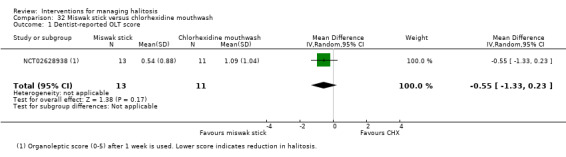
Comparison 32 Miswak stick versus chlorhexidine mouthwash, Outcome 1 Dentist‐reported OLT score.
32.2. Analysis.
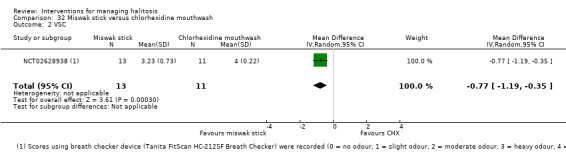
Comparison 32 Miswak stick versus chlorhexidine mouthwash, Outcome 2 VSC.
32.3. Analysis.
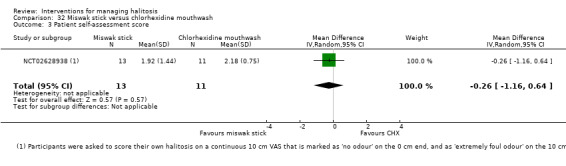
Comparison 32 Miswak stick versus chlorhexidine mouthwash, Outcome 3 Patient self‐assessment score.
8b. Brushing + mouthwash versus brushing + tongue cleaning: one trial (Aung 2015) reported VSC score as the outcome for this comparison. The effect estimates showed improvement in the brushing plus mouthwash group compared to brushing plus tongue cleaning group (MD ‐81.87; 95% CI ‐140.12 to ‐23.62; 1 trial; 30 participants; 4 weeks follow‐up; Analysis 33.1).
33.1. Analysis.
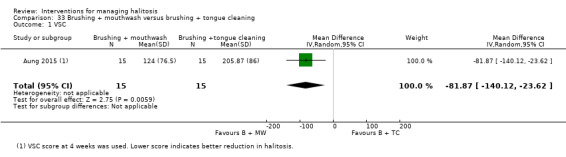
Comparison 33 Brushing + mouthwash versus brushing + tongue cleaning, Outcome 1 VSC.
8c. Brushing + cetylpyridium mouthwash versus brushing: one trial (Feres 2015) reported OLT and VSC score as the outcomes for this comparison. The effect estimates showed improvement in the brushing plus cetylpyridium mouthwash group compared to brushing group (MD ‐0.48; 95% CI ‐0.72 to ‐0.24; 1 trial; 70 participants; 3 weeks follow‐up; Analysis 34.1 and MD ‐8.04; 95% CI ‐15.87 to ‐0.21; 1 trial; 70 participants; 3 weeks follow‐up; Analysis 34.2 respectively).
34.1. Analysis.
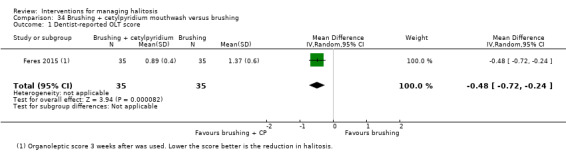
Comparison 34 Brushing + cetylpyridium mouthwash versus brushing, Outcome 1 Dentist‐reported OLT score.
34.2. Analysis.
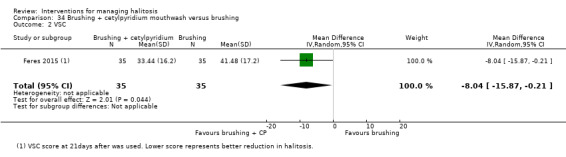
Comparison 34 Brushing + cetylpyridium mouthwash versus brushing, Outcome 2 VSC.
8d. Turkish gall oral rinse versus brushing: one trial (An 2011) reported OLT and VSC score as the outcomes for this comparison. The effect estimates showed improvement in the Turkish gall oral rinse group compared to brushing group. However, the confidence intervals crossed the line of no effect (MD ‐0.10; 95% CI ‐0.50 to 0.30; 1 trial; 66 participants; 2 weeks follow‐up; Analysis 35.1 and MD ‐211.47; 95% CI ‐503.58 to 80.64; 1 trial; 66 participants; 2 weeks follow‐up; Analysis 35.2 respectively).
35.1. Analysis.
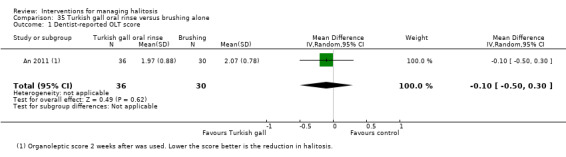
Comparison 35 Turkish gall oral rinse versus brushing alone, Outcome 1 Dentist‐reported OLT score.
35.2. Analysis.
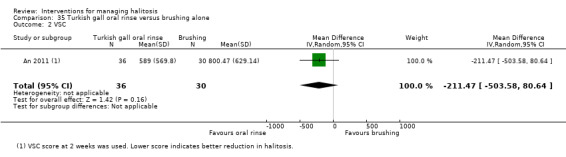
Comparison 35 Turkish gall oral rinse versus brushing alone, Outcome 2 VSC.
8e. Laser + povidone iodine versus SRP: one trial (Kara 2008) compared subgingival Nd:YAG laser irradiation combined with povidone‐iodine application with SRP. Both the effect estimates for OLT scores and VSC showed lesser improvement in laser group compared to SRP group (MD 0.49; 95% CI 0.30 to 0.68; 1 trial; 40 participants; 4 weeks follow‐up; Analysis 36.1 and MD 70.00; 95% CI 63.88 to 76.12; 1 trial; 40 participants; 4 weeks follow‐up; Analysis 36.2 respectively).
36.1. Analysis.
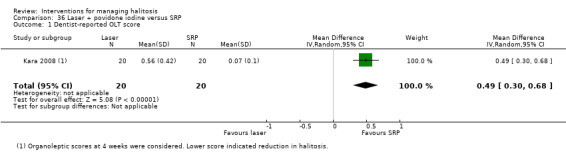
Comparison 36 Laser + povidone iodine versus SRP, Outcome 1 Dentist‐reported OLT score.
36.2. Analysis.

Comparison 36 Laser + povidone iodine versus SRP, Outcome 2 VSC.
Discussion
Summary of main results
We found 36 comparisons in this Cochrane Review which were grouped for ease of understanding as comparisons related to eight broad interventions: mechanical debridement, chewing gum, systemic deodorising agent, topical agents, toothpaste, mouthrinse/mouthwash, tablets, and combination of methods.
The majority of the included trials presented the results for reduction in halitosis as self‐perceived or dentist‐perceived outcome or both in terms of organoleptic test (OLT) or visual analogue scale (VAS). Some studies used other methods like halimeter and breath print analysis. Adverse events were reported only in seven trials. Other included trials either not mentioned the adverse events or there were no adverse events. None of the trials reported quality of life as an outcome. These outcomes were reported for a minimum follow‐up period of seven days to a maximum follow‐up period of three months, with one to two weeks as the most commonly reported duration.
We produced 'Summary of findings' tables for the most commonly used interventions with findings also summarized for the rest of important comparisons and included under Additional tables. We considered only the clinical outcomes of commonly used interventions for the summary of main results. We could not find any COMET 2019 recommendations for the most important outcome measures. Hence, in this review, we considered OLT score reported by odour judges as the gold standard outcome measure (Quirynen 2018) followed by patient self‐assessment scores as the most important clinical outcomes. Certainty of the evidence was assessed for only these outcome measures and adverse events when reported. We found low‐ to very low‐certainty evidence for all the interventions included in this review and therefore we cannot draw any conclusions regarding the superiority of any of the interventions.
See Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7 and Additional Table 9; Table 10; Table 11; Table 12; Table 13; Table 14; Table 15; Table 16; Table 17; Table 18; Table 19; Table 20; Table 21; Table 22; Table 23.
2. 0.6% eucalyptus chewing gum compared to 0.4% eucalyptus chewing gum for managing halitosis.
| 0.6% eucalyptus chewing gum compared to 0.4% eucalyptus chewing gum for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: 0.6% eucalyptus chewing gum Comparison: 0.4% eucalyptus chewing gum | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with 0.4% eucalyptus chewing gum | Risk with 0.6% eucalyptus chewing gum | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 4 weeks | The mean dentist‐reported OLT score was 1.60 units | MD 0.10 units lower (0.37 lower to 0.17 higher) | ‐ | 64 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aTanaka 2010. bDowngraded for risk of bias ‐ unclear risk of bias due to lack of allocation concealment. cDowngraded for imprecision ‐ wide confidence intervals, low sample size and event rate.
3. 1000 mg champignon compared to 50 mg champignon for managing halitosis.
| 1000 mg champignon compared to 50 mg champignon for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: 1000 mg champignon Comparison: 50 mg champignon | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with 50 mg champignon | Risk with 1000 mg champignon | |||||
| Dentist‐reported OLT score assessed with dentist's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Patient‐reported VAS assessed with patient's perception Scale from: 0 to 100 Follow‐up: mean 2 weeks | The mean patient‐reported VAS was 67.72 units | MD 5.32 units lower (18.14 lower to 7.50 higher) | ‐ | 40 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aNishihira 2017. bDowngraded for risk of bias ‐ unclear risk of performance and detection bias and high risk of reporting bias. cDowngraded for imprecision ‐ wide confidence interval crossing the line of no effect, low sample size and event rate.
4. Toothpaste with 0.2% zinc sulphate compared to placebo toothpaste for managing halitosis.
| Toothpaste with 0.2% zinc sulphate compared to placebo toothpaste for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: toothpaste with 0.2% zinc sulphate Comparison: placebo toothpaste | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo toothpaste | Risk with toothpaste with 0.2% zinc sulphate | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 4 weeks | The mean dentist‐reported OLT scores was 2.85 units | MD 1.31 units lower (1.39 lower to 1.23 lower) | ‐ | 187 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aNavada 2008. bDowngraded for risk of bias ‐ unclear risk of selection bias in random sequence generation and allocation concealment. cDowngraded for imprecision ‐ low sample size and event rate.
5. Dual zinc + arginine dentifrice compared to control dentifrice for managing halitosis.
| Dual zinc + arginine dentifrice compared to control dentifrice for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: dual zinc+ arginine dentifrice Comparison: control dentifrice | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with control dentifrice | Risk with dual zinc + arginine dentifrice | |||||
| Dentist‐reported OLT hedonic ratings assessed with dentist's perception Scale from: 1 to 9 Follow‐up: mean 3 weeks | The mean dentist‐reported OLT hedonic rating was 6.49 units | MD 2.00 units lower (2.19 lower to 1.81 lower) | ‐ | 80 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aHu 2018. bDowngraded for risk of bias ‐ unclear risk of bias in random sequence generation and lack of allocation concealment details. cDowngraded for imprecision ‐ low sample size and event rate.
6. Halita mouthwash compared to placebo mouthwash for managing halitosis.
| Halita mouthwash compared to placebo mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: halita mouthwash Comparison: placebo mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo mouthwash | Risk with halita mouthwash | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 2 weeks | The mean dentist‐reported OLT score was 2.50 units | MD 1.00 units lower (1.65 lower to 0.35 lower) | ‐ | 40 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | None reported | Tongue staining was seen in patients who gargled, rather than rinsed | ‐ | 40 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aWinkel 2003. bDowngraded for risk of bias ‐ unclear risk of bias due to lack of allocation concealment and attrition bias. cDowngraded for imprecision ‐ low sample size and event rate.
7. Cetylperidium chloride mouthwash compared to placebo mouthwash for managing halitosis.
| Cetylperidium chloride mouthwash compared to placebo mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: cetylperidium chloride mouthwash Comparison: placebo mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo mouthwash | Risk with cetylperidium chloride mouthwash | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 2 weeks | The mean dentist‐reported OLT score was 4.20 units | MD 0.50 units lower (0.83 lower to 0.17 lower) | ‐ | 47 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aBorden 2002. bDowngraded for risk of bias ‐ unclear risk of bias due to random sequence generation, lack of allocation concealment, and attrition bias. cDowngraded for imprecision ‐ low sample size and event rate.
8. Mouthwash containing essential oil compared to placebo mouthwash for managing halitosis.
| Mouthwash containing essential oil compared to placebo mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: mouthwash containing essential oil Comparison: placebo mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo mouthwash | Risk with mouthwash containing essential oil | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 2 weeks | The mean dentist‐reported OLT score was 4.20 units | MD 0.09 units lower (0.47 lower to 0.29 higher) | ‐ | 45 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aBorden 2002. bDowngraded for risk of bias ‐ unclear risk of bias due to random sequence generation, lack of allocation concealment and attrition bias. cDowngraded for imprecision ‐ wide confidence interval, low sample size and event rate
9. Mouthwash containing chlorine dioxide and zinc compared to placebo mouthwash for managing halitosis.
| Mouthwash containing chlorine dioxide and zinc compared to placebo mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: mouthwash containing chlorine dioxide and zinc Comparison: placebo mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo mouthwash | Risk with mouthwash containing chlorine dioxide and zinc | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 2 weeks | The mean dentist‐reported OLT score was 4.20 units | MD 0.17 units lower (0.59 lower to 0.25 higher) | ‐ | 41 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aBorden 2002. bDowngraded for risk of bias ‐ unclear risk of bias in random sequence generation, lack of allocation concealment and attrition bias. cDowngraded for imprecision ‐ wide confidence interval, low sample size and event rate.
10. Chlorine dioxide mouthwash compared to placebo mouthwash for managing halitosis.
| Chlorine dioxide mouthwash compared to placebo mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: chlorine dioxide mouthwash Comparison: placebo mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo mouthwash | Risk with chlorine dioxide mouthwash | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 3 weeks | The mean dentist‐reported OLT score was 3.19 units | MD 0.61 units lower (0.73 lower to 0.49 lower) | ‐ | 47 (1 RCT)a | ⊕⊕⊝⊝ LOWb | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
|
*The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aLee 2018. bDowngraded for imprecision ‐ low sample size and event rate. However, when week 6 data were used, the effect estimate favoured placebo group with 95% CI crossing the line of no effect.
11. Cetylpyridinium mouthwash compared to mouthwash containing chlorhexidine and zinc for managing halitosis.
| Cetylpyridinium mouthwash compared to mouthwash containing chlorhexidine and zinc for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: cetylpyridinium mouthwash Comparison: mouthwash containing chlorhexidine and zinc | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with mouthwash containing chlorhexidine and zinc | Risk with cetylpyridinium mouthwash | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 2 weeks | The mean dentist‐reported OLT score was 4.03 units | MD 0.33 units lower (0.72 lower to 0.06 higher) | ‐ | 44 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aBorden 2002. bDowngraded for risk of bias ‐ unclear risk of bias in random sequence generation, lack of allocation concealment and attrition bias. cDowngraded for imprecision ‐ wide confidence interval, low sample size and event rate.
12. Halita mouthrinse compared to Perio‐plus mouthrinse for managing halitosis.
| Halita mouthrinse compared to Perio‐plus mouthrinse for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: halita mouthrinse Comparison: Perio‐plus mouthrinse | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with Perio‐plus mouthrinse | Risk with halita mouthrinse | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 8 days | The mean dentist‐reported OLT score was 1.40 units | MD 0.20 units lower (0.86 lower to 0.46 higher) | ‐ | 36 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | 1 patient reported unpleasant feeling after the use of the product. There were no severe adverse events reported | 1 patient reported unpleasant feeling after the use of the product and 1 involving tooth staining. There were no severe adverse events reported | ‐ | 36 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aDadamio 2013. bDowngraded for risk of bias ‐ high risk of other bias. cDowngraded for imprecision ‐ wide confidence interval, low sample size and event rate.
13. Mouthwash containing Triphala and Ela decoction compared to chlorhexidine mouthwash for managing halitosis.
| Mouthwash containing Triphala and Ela decoction compared to chlorhexidine mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: mouthwash containing Triphala and Ela decoction Comparison: chlorhexidine mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with chlorhexidine mouthwash | Risk with mouthwash containing Triphala and Ela decoction | |||||
| Dentist‐reported OLT score assessed with dentist's perception
Scale from: 0 to 5 Follow‐up: mean 2 weeks |
The mean dentist‐reported OLT score was 3.40 units | MD 0.20 units higher (0.09 higher to 0.31 higher) | ‐ | 60 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aMamgain 2016. bDowngraded for risk of bias ‐ unclear risk of bias due to lack of allocation concealment, detection and attrition bias and high risk of performance bias. cDowngraded for imprecision ‐ low sample size and event rate.
14. Miswak mouthwash compared to chlorhexidine mouthwash for managing halitosis.
| Miswak mouthwash compared to chlorhexidine mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: miswak mouthwash Comparison: chlorhexidine mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with chlorhexidine mouthwash | Risk with miswak mouthwash | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 1 week | The mean dentist‐reported OLT score was 1.09 units | MD 0.01 units higher (0.95 lower to 0.97 higher) | ‐ | 21 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported VAS assessed with patient's perception Scale from: 0 to 10 Follow‐up: mean 1 week |
The mean patient‐reported VAS was 2.18 units | MD 0.18 units lower (1.59 lower to 1.23 higher) | ‐ | 21 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aNCT02628938. bDowngraded for risk of bias ‐ unclear risk of selection and attrition bias and high risk of performance bias. cDowngraded for imprecision ‐ low sample size and event rate; wide confidence intervals crossing the line of no effect.
15. Miswak stick compared to chlorhexidine mouthwash for managing halitosis.
| Miswak stick compared to chlorhexidine mouthwash for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: miswak stick Comparison: chlorhexidine mouthwash | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with chlorhexidine mouthwash | Risk with miswak stick | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 1 week | The mean dentist‐reported OLT score was 1.09 units | MD 0.55 units lower (1.33 lower to 0.23 higher) | ‐ | 24 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported VAS assessed with patient's perception Scale from: 0 to 10 Follow‐up: mean 1 week | The mean patient‐reported VAS was 2.18 units | MD 0.26 units lower (1.16 lower to 0.64 higher) | ‐ | 24 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aNCT02628938. bDowngraded for risk of bias ‐ unclear risk of selection and attrition bias and high risk of performance bias. cDowngraded for imprecision ‐ low sample size and event rate; wide confidence intervals crossing the line of no effect.
16. Laser + povidone iodine compared to SRP alone for managing halitosis.
| Laser + povidone iodine compared to SRP alone for managing halitosis | ||||||
| Patient or population: patients reporting halitosis Setting: university hospital Intervention: laser + povidone iodine Comparison: SRP alone | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with SRP alone | Risk with laser + povidone iodine | |||||
| Dentist‐reported OLT score assessed with dentist's perception Scale from: 0 to 5 Follow‐up: mean 4 weeks | The mean dentist‐reported OLT score was 0.07 units | MD 0.49 units higher (0.30 higher to 0.68 higher) | ‐ | 40 (1 RCT)a | ⊕⊝⊝⊝ VERY LOWb,c | ‐ |
| Patient‐reported OLT score assessed with patient's perception | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OLT: organoleptic test; RCT: randomised controlled trial; SRP: scaling and root planing | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aKara 2008. bDowngraded for risk of bias ‐ unclear risk of bias due to lack of allocation concealment, performance and detection bias. cDowngraded for imprecision ‐ low sample size and event rate.
Overall completeness and applicability of evidence
We systematically searched for trials according to the methodology written in the protocol. We checked all cross references of included articles and other systematic reviews on the management of halitosis to be sure that we did not miss any article. Two pairs of review authors did data extraction in duplicate. Trials which were not included in the meta‐analysis were explained qualitatively. We selected trials with adult participants treated for halitosis and included all types of interventions and concentrations. We included comparisons with placebo and control. All clinically relevant outcomes of interest were analysed. We also included trials in which herbal and alternative medicines were tested.
We did not exclude any trial due to missing data. For trials reporting data in graphs, we derived the data using PlotDigitizer software. When mean and standard error (SE) were given, we calculated the standard deviation (SD) as given in the Cochrane Handbook for Systematic Reviews of Interventions Section 7.7.3.3 (Higgins 2011). In cross‐over trials, mean difference (MD) and SE were calculated using the MD, imputing correlation coefficient (Corr) method as described in the Cochrane Handbook for Systematic Reviews of Interventions Section 16.4.6.3 (Higgins 2011). When mean and P value were given, SD was calculated according to the methods described in the Cochrane Handbook for Systematic Reviews of Interventions Section 7.7.3.3 (Higgins 2011). When median and interquartile range were given, we used the data to calculate mean and SD according to the methods described in the Cochrane Handbook for Systematic Reviews of Interventions Section 7.7.3.5 (Higgins 2011).
We have used data from the clinically relevant time points as the therapeutic effect could be at different durations. For scaling and root planing (SRP), we considered 4 weeks as time point as this is the time taken for epithelial and initial connective tissue healing. For antiseptic mouthwashes, we considered the therapeutic effect to happen at a minimum of seven days and this time point was considered in this review. We considered the reported minimal time point for other interventions (champignon, G32, sesame oil, protease cysteine + actinidine tablets, miswak, Turkish gall) for which we were not sure of the therapeutic effect time period.
In cross‐over trials, we used the data before and after cross‐over to see the consistency in the results. If the results were not consistent, we mentioned the same in the footnotes of the meta‐analysis.
In case of completed and unpublished trials, we cross‐checked the trial registry for any updated results and used it in the meta‐analysis.
We could not use the data from 14 trials (17 reports) due to improper reporting and missing details. 12 trials out of these 14 were published after the publication of the CONSORT Statement (Moher 2001). It is surprising to note that the reporting of trials is still an issue and not standardised.
Although we had 44 trials (55 reports) included in this review, most of the comparisons were single trials and could not be combined in meta‐analyses due to varying methods of intervention and concentrations. The evidence generated was also of very low to low quality for most of the comparisons testing an intervention versus placebo or control, and hence the results cannot be considered with certainty.
Most of the trials reported on short‐term improvement of halitosis (ranging from one to four weeks). Long‐term follow‐up (three months) was reported in one trial only (Ademovski 2017). The results cannot reflect the retention period for the improvement in halitosis as the oral hygiene maintenance issues would determine the long‐term success. However, the review encourages further high‐quality randomised controlled trials (RCTs) to be conducted by standardising methods of interventions, concentrations, and dosage.
Quality of the evidence
The certainty of the evidence for all comparisons was low to very low for the considered outcomes. We downgraded the trials mainly for two reasons: risk of bias and imprecision. Most of the trials were downgraded by one level for unclear risk of bias, by two levels for high risk of bias, and downgraded by two levels for imprecision as most were single trials with limited number of participants and low event rates.
Potential biases in the review process
We have taken steps to minimise bias in every step of the review. We searched all the above mentioned databases, conference proceedings, and trial registries to include all relevant reports. We included reports not in the English language in our review. We contacted trial authors for missing data through emails, peer‐contacts,Google search and university/hospital websites where they were previously affiliated. Nevertheless, there could be unpublished data which we could not trace with the above methods. We checked all cross‐references in the included articles and other systematic reviews conducted on interventions for halitosis and found articles which were missed in the search. Two review authors independently reviewed data extraction forms obtained from translators and cross‐checked doubtful areas using Google translator.
Agreements and disagreements with other studies or reviews
We found six systematic reviews published in the last two years. All these six reviews were limited to any one particular type of intervention. We could not find a review which covered all types of interventions.
Kellesarian 2017 conducted a systematic review to assess the efficacy of laser therapy and antimicrobial photodynamic therapy as an adjunct to mechanical debridement to manage halitosis. The review included six RCTs and concluded that the efficacy of laser therapy and antimicrobial photodynamic therapy to manage halitosis is unclear due to moderate to high risk of bias in the included trials. This review included advanced periodontitis cases and adolescents unlike the present Cochrane Review in which these two were excluded.
Muniz 2017 did a systematic review to analyse the impact of chewing gum on halitosis parameters. They concluded that chewing gums containing probiotics Lactobacillus, zinc acetate and magnolia bark extract, eucalyptus extract and allylisothiocyanate (AITC) with zinc lactate may be suitable for halitosis management. However, there is lack of evidence in applying these findings clinically due to high heterogeneity and low number of included studies. Unlike this Cochrane Review, Muniz 2017 included single‐dose interventions and follow‐ups of few hours.
Deutscher 2018 published a systematic review to give the best available evidence on the impact of professional tooth cleaning and SRP on oral halitosis in patients with periodontal diseases. They concluded that the professional tooth cleaning and SRP in combination with oral hygiene instructions reduced volatile sulphur compound (VSC) values in patients with oral halitosis or periodontal diseases or both, independent of tongue cleaning and the use of mouthrinses. Only controlled clinical trials (CCTs) were included in this review, unlike the present Cochrane Review, which included RCTs only. The difference in conclusions could be due to the patient‐related outcomes evaluated in the present Cochrane Review.
Wu 2018 reported a systematic review and meta‐analysis which evaluated the effective rate of Chinese medicine and combined Chinese and Western medicine on halitosis. It included 17 RCTs (10 intraoral halitosis and 7 extraoral halitosis) and concluded that both Chinese medicine and the combined Chinese and Western medicines have significantly better effect on halitosis than Western medicine alone. The authors included intraoral and extraoral halitosis, searched the Chinese biomedical databases CNKI, Wanfang and CBM, and had different exclusion criteria. The differences in the conclusion between Wu 2018 and our review could be because of these reasons.
Tahani 2018 did a systematic review to evaluate the clinical effect of green tea on halitosis. The search was limited to English language publications and included RCTs and quasi‐RCTs. The review included two RCTs out of which, one evaluated the short‐term effects and the other the long‐term effects of green tea. Due to the small number of included studies, this review was inconclusive.
Yoo 2019 published a systematic review and meta‐analysis of RCTs to summarize the evidence on the effect of probiotics on halitosis. The review concluded that the Lactobacillus strain given for an average of two weeks has a moderate effect on the OLT outcome and did not confirm the effect on the reduction of VSC. However, the authors included trials testing morning breath and patients with advanced periodontitis, unlike this Cochrane Review.
Authors' conclusions
Implications for practice.
We found low‐ to very low‐certainty evidence to support the effectiveness of interventions for managing halitosis compared to placebo or control for the outcomes tested over short‐time periods. We were unable to draw any conclusions regarding the superiority of any intervention or concentration.
Implications for research.
Further research should be undertaken to determine the most effective methods for managing halitosis by conducting well‐planned randomised controlled trials (RCTs) with more clarity and uniformity in the variables. In designing such clinical trials, the following should be considered.
Evidence: the present evidence was insufficient to conclude that any of the comparisons are effective to manage halitosis. Trials should focus on testing similar concentrations with similar methods of intervention. Trials should focus on both short‐term and long‐term benefits of treatment. Studies should also focus on patient‐related outcomes and cost effectiveness. Furthermore, reports on clinical trials would be improved by following CONSORT 2010 recommendations. Cross‐over trials should clearly mention the wash‐out period and use statistical tests to rule out any carry‐over effect.
Population: inclusion criteria for clinical trials should be well defined and grade of gingivitis or periodontitis should be clearly mentioned. Trials should include both genders in equal distribution.
Intervention: intervention should focus on similar methods and concentrations used in earlier studies and with a longer follow‐up. This will add on to the existing evidence pool allowing us to make robust conclusions.
Comparison: various comparisons have been reported, but we found only single trials in most of the comparisons due to which the certainty of evidence is very low. Hence, RCTs need to be conducted keeping in mind already published studies so that the number of trials for a particular comparison increase.
Outcome: patient‐reported outcomes were not considered in most of the trials. Most important outcome measures should be standardised by the COMET initiative. Cost effectiveness also needs to be added in the RCTs, which is of most interest to consumers. In trials using mouthwashes or toothpastes, remnant/bad taste and decrease in the taste perception should be considered as adverse effects and reported.
Acknowledgements
We are extremely thankful to Cochrane Oral Health: Anne Littlewood, Information Specialist; Luisa M Fernandez Mauleffinch, Managing Editor and Copy Editor; Philip Riley, Editor; and Professor Helen Worthington, Co‐ordinating Editor. We thank Professor Datuk Dr Abdul Razzak, Pro Vice Chancellor, Manipal Academy of Higher Education (MAHE), Melaka campus, for his constant encouragement to undertake Cochrane Reviews; Professor Dr Jaspal Singh Sahota, Chief Executive, Melaka‐Manipal Medical College, Melaka campus for his support; Professor Dr Adinegara Lutfi Abas, Dean, Faculty of Medicine and Professor Dr Abdul Rashid Hj Ismail, Dean, Faculty of Dentistry, Melaka‐Manipal Medical College for constant support during the review preparation. The review authors would like to thank the authors (Fedorowicz Z, Aljufairi H, Nasser M, Outhouse TL, Pedrazzi V, Al‐Alawi R, Keenan JV) of the two previous Cochrane Reviews (Fedorowicz 2008; Outhouse 2006) which have been consolidated into this single review. We are thankful to our translators: Anette Bluemle (German); Malgorzata Bala and Professor Maria Chomyszyn‐Gajewska (Polish); Eishu Nango, Rina Nango and Keika Hoshi (Japanese); Szabolcs Szatmári (Romanian); Fang Hua, Yanxiaoxue Liu, Wong Ming Yin and Choo Mei Yee (Chinese); Gemma Villanueva (Spanish); Alireza Talebian and Sepideh Banava (Persian); Myonghwa Park (Korean); and Maira Parra and Paulo Jorge Pereira Alves (Portuguese). We thank Anirudha Agnihotry who has contributed in the protocol preparation and Professor Dr Rajesh Hosadurga for his valuable suggestions and inputs during the review preparation. We are indebted to C Albert Yeung, Consultant in Dental Public Health, NHS, Lanarkshire, UK for the valuable comments and suggestions.
Appendices
Appendix 1. Cochrane Oral Health's Trials Register search strategy
Cochrane Oral Health's Trials Register is available via the Cochrane Register of Studies. For information on how the register is compiled, see oralhealth.cochrane.org/trials.
1 (halitosis or halitose*):ti,ab 2 ("oral malodour*" or "oral malodor*"):ti,ab 3 ((breath and odor*) or (breath and odour*) or "bad breath" or (breath and smell*) or (breath and offensive) or (mouth and odor*) or (mouth and odour*) or (mouth and malodor*) or (mouth and malodour*) or "morning breath"):ti,ab 4 ("volatile sulphur compound*" or "volatile sulphur compound*"):ti,ab 5 ("fetor oris" or "foetor oris" or "fetor ex ore" or "foetor ex ore" or "foul breath" or "fetid breath" or "putrid breath"):ti,ab 6 (#1 or #2 or #3 or #4 or #5) AND (INREGISTER)
Appendix 2. Cochrane Central Register of Controlled Trials (CENTRAL) search strategy
#1 [mh halitosis] #2 (halitosis or halitose*) #3 ("oral malodour*" or "oral malodor*") #4 ((breath near/4 odor*) or ("bad breath") or (breath near/4 odour*) or (breath near/4 smell*) or (breath near/4 offensive) or (mouth near/4 odour*) or (mouth near/4 odor*) or (mouth near/4 malodour*) or (mouth near/4 malodor*) or "morning breath") #5 ("volatile sulphur compound*" or "volatile sulphur compound*") #6 ("fetor oris" or "foetor oris" or "fetor ex ore" or "foetor ex ore" or "foul breath" or "fetid breath" or "putrid breath") #7 {or #1‐#6}
Appendix 3. MEDLINE Ovid search strategy
1. Halitosis/ 2. (halitosis or halitose$).mp. 3. ((oral adj malodour$) or (oral adj malodor$)).mp. 4. ((breath adj4 odor$) or (bad adj breath) or (breath adj4 odour$) or (breath adj4 smell$) or (breath adj4 offensive) or (mouth adj4 odour$) or (mouth adj4 odor$) or (mouth adj4 malodour$) or (mouth adj4 malodor$) or "morning breath").mp. 5. ("volatile sulphur compound$" or "volatile sulphur compound$").mp. 6. ("fetor oris" or "foetor oris" or "fetor ex ore" or "foetor ex ore" or "foul breath" or "fetid breath" or "putrid breath").mp. 7. or/1‐6
This subject search was linked to the Cochrane Highly Sensitive Search Strategy (CHSSS) for identifying randomised trials (RCTs) in MEDLINE: sensitivity‐maximising version (2008 revision) as referenced in Chapter 6.4.11.1 and detailed in Box 6.4.c of theCochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 (updated March 2011) (Lefebvre 2011).
1. randomized controlled trial.pt. 2. controlled clinical trial.pt. 3. randomized.ab. 4. placebo.ab. 5. drug therapy.fs. 6. randomly.ab. 7. trial.ab. 8. groups.ab. 9. or/1‐8 10. exp animals/ not humans.sh. 11. 9 not 10
Appendix 4. Embase Ovid search strategy
1. Halitosis/ 2. (halitosis or halitose$).mp. 3. ((oral adj malodour$) or (oral adj malodor$)).mp. 4. ((breath adj4 odor$) or (bad adj breath) or (breath adj4 odour$) or(breathadj4 smell$) or (breath adj4 offensive) or (mouth adj4 odour$) or (mouth adj4 odor$) or (mouth adj4 malodour$) or (mouth adj4 malodor$)or “morning breath”).mp. 5. ("volatile sulphur compound$" or "volatile sulphur compound$").mp. 6. ("fetor oris" or "foetor oris" or "fetor ex ore" or "foetor ex ore" or "foulbreath" or "fetid breath" or "putrid breath").mp. 7. or/1‐6
The above subject search was linked to adapted version of the Cochrane Embase Project filter for identifying RCTs in Embase Ovid see www.cochranelibrary.com/help/central‐creation‐details.html for information). 1. Randomized controlled trial/ 2. Controlled clinical study/ 3. Random$.ti,ab. 4. randomization/ 5. intermethod comparison/ 6. placebo.ti,ab. 7. (compare or compared or comparison).ti. 8. ((evaluated or evaluate or evaluating or assessed or assess) and (compareor compared or comparing or comparison)).ab. 9. (open adj label).ti,ab. 10. ((double or single or doubly or singly) adj (blind or blinded or blindly)).ti,ab. 11. double blind procedure/ 12. parallel group$1.ti,ab. 13. (crossover or cross over).ti,ab. 14. ((assign$ or match or matched or allocation) adj5 (alternate or group$1 or intervention$1 or patient$1 or subject$1 or participant$1)).ti,ab. 15. (assigned or allocated).ti,ab. 16. (controlled adj7 (study or design or trial)).ti,ab. 17. (volunteer or volunteers).ti,ab. 18. trial.ti. 19. or/1‐18 20. (exp animal/ or animal.hw. or nonhuman/) not (exp human/ or humancell/ or (human or humans).ti.) 21. 19 not 20
Appendix 5. LILACS BIREME search strategy
1. Halitosis 2. Controlled clinical trial (filter)
Appendix 6. CINAHL EBSCO search strategy
1. 'halitosis OR bad breath OR fetid odor OR malodor' 2. 'randomized controlled trials or rtc or randomised control trials or randomized clinical trial or randomized controlled study'
Appendix 7. The National Database of Indian Medical Journals (IndMed) search strategy
1. Halitosis
Appendix 8. OpenGrey search strategy
1. Halitosis 2. Bad breath 3. Fetid odor 4. Malodor
Appendix 9. US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) search strategy
halitosis
Appendix 10. World Health Organization International Clinical Trials Registry Platform search strategy
1.Halitosis
Appendix 11. ISRCTN registry search strategy
1. Halitosis
Appendix 12. Clinical Trials Registry ‐ India search strategy
1. Halitosis 2. Bad breath
Data and analyses
Comparison 1. SRP + air polishing versus SRP.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 60 | Mean Difference (IV, Random, 95% CI) | ‐3.87 [‐17.93, 10.19] |
Comparison 2. SRP + laser versus SRP.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 40 | Mean Difference (IV, Random, 95% CI) | ‐3.30 [‐9.38, 2.78] |
Comparison 3. Mechanical tongue cleaning versus no tongue cleaning.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 2 | 46 | Mean Difference (IV, Random, 95% CI) | ‐7.69 [‐47.08, 31.69] |
| 2 Dentist‐reported OLT score | 2 | 46 | Mean Difference (IV, Random, 95% CI) | ‐0.20 [‐0.34, ‐0.07] |
Comparison 4. 0.6% eucalyptus chewing gum versus 0.4% eucalyptus chewing gum.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 64 | Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.37, 0.17] |
| 2 VSC | 1 | 64 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.21, 0.21] |
Comparison 5. 0.6% eucalyptus chewing gum versus placebo chewing gum.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 65 | Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.31, 0.11] |
| 2 VSC | 1 | 65 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.21, 0.21] |
Comparison 6. Pycnogenol chewing gum versus placebo chewing gum.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC (hydrogen sulphide) | 1 | 21 | Mean Difference (IV, Random, 95% CI) | ‐114.90 [‐206.59, ‐23.21] |
| 2 VSC (methyl mercaptan) | 1 | 21 | Mean Difference (IV, Random, 95% CI) | ‐8.4 [‐24.95, 8.15] |
| 3 VSC (methyl sulphide) | 1 | 21 | Mean Difference (IV, Random, 95% CI) | ‐4.70 [‐27.01, 17.61] |
Comparison 7. 1000 mg champignon versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Patient‐reported VAS | 1 | 40 | Mean Difference (IV, Random, 95% CI) | ‐1.07 [‐14.51, 12.37] |
| 2 Patient's relative‐reported VAS | 1 | 40 | Mean Difference (IV, Random, 95% CI) | ‐1.74 [‐15.52, 12.04] |
Comparison 8. 1000 mg champignon extract versus 50 mg champignon extract.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Patient‐reported VAS | 1 | 40 | Mean Difference (IV, Random, 95% CI) | ‐5.32 [‐18.14, 7.50] |
| 2 Patient's relative‐reported VAS | 1 | 40 | Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐15.58, 14.36] |
Comparison 9. Hinokitiol gel versus placebo gel.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 18 | Mean Difference (IV, Random, 95% CI) | ‐0.27 [‐1.26, 0.72] |
| 2 VSC (methyl mercaptan) | 1 | 18 | Mean Difference (IV, Random, 95% CI) | ‐2.13 [‐5.33, 1.08] |
| 3 VSC (hydrogen sulphide) | 1 | 18 | Mean Difference (IV, Random, 95% CI) | ‐1.64 [‐5.77, 2.49] |
Comparison 10. G32 versus chlorhexidine gel.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 40 | Mean Difference (IV, Random, 95% CI) | 0.05 [‐0.28, 0.38] |
Comparison 11. Triclosan + PVM/MA toothpaste versus control toothpaste.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported breath odour score | 1 | 81 | Mean Difference (IV, Random, 95% CI) | ‐3.48 [‐3.77, ‐3.19] |
Comparison 12. Zinc toothpaste versus placebo toothpaste.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 187 | Mean Difference (IV, Random, 95% CI) | ‐1.31 [‐1.39, ‐1.23] |
| 2 VSC | 1 | 188 | Mean Difference (IV, Random, 95% CI) | ‐11.30 [‐20.45, ‐2.15] |
Comparison 13. Sodium bicarbonate toothpaste versus control toothpaste.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 148 | Mean Difference (IV, Random, 95% CI) | 105.80 [‐16.20, 227.80] |
Comparison 14. Dual zinc + arginine dentifrice versus control dentifrice.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 OLT hedonic ratings | 1 | 80 | Mean Difference (IV, Random, 95% CI) | ‐2.0 [‐2.19, ‐1.81] |
Comparison 15. Halita versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 40 | Mean Difference (IV, Random, 95% CI) | ‐1.0 [‐1.65, ‐0.35] |
| 2 VSC | 1 | 40 | Mean Difference (IV, Random, 95% CI) | ‐188.0 [‐308.29, ‐67.71] |
Comparison 16. Chlorhexidine + zinc acetate mouthwash versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 44 | Mean Difference (IV, Random, 95% CI) | ‐0.20 [‐0.58, 0.18] |
Comparison 17. Cetylperidinium chloride mouthwash versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 47 | Mean Difference (IV, Random, 95% CI) | ‐0.5 [‐0.83, ‐0.17] |
| 2 VSC | 1 | 47 | Mean Difference (IV, Random, 95% CI) | ‐20.04 [‐37.71, ‐2.37] |
Comparison 18. Essential oil mouthwash versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 45 | Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.47, 0.29] |
| 2 VSC | 1 | 45 | Mean Difference (IV, Random, 95% CI) | ‐5.13 [‐32.94, 22.68] |
Comparison 19. Chlorine dioxide + zinc mouthwash versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 41 | Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.59, 0.25] |
| 2 VSC | 1 | 41 | Mean Difference (IV, Random, 95% CI) | ‐20.53 [‐38.52, ‐2.54] |
Comparison 20. Chlorine dioxide mouthwash versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 47 | Mean Difference (Random, 95% CI) | ‐0.61 [‐0.73, ‐0.49] |
Comparison 21. Herbal mouthwash versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 60 | Mean Difference (IV, Random, 95% CI) | ‐70.29 [‐121.01, ‐19.57] |
Comparison 22. Benzethonium chloride mouthwash versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC (methyl mercaptan) | 1 | 20 | Mean Difference (IV, Random, 95% CI) | 7.20 [‐24.92, 39.32] |
| 2 VSC (hydrogen sulphide) | 1 | 20 | Mean Difference (IV, Random, 95% CI) | ‐125.10 [‐286.32, 36.12] |
| 3 VSC (dimethyl sulphide) | 1 | 20 | Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.63, 0.57] |
Comparison 23. Green tea mouthwash versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 60 | Mean Difference (IV, Random, 95% CI) | ‐57.39 [‐184.63, 69.85] |
Comparison 24. Lemongrass mouthwash versus placebo mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 20 | Mean Difference (IV, Random, 95% CI) | ‐26.66 [‐43.39, ‐9.93] |
Comparison 25. Cetylpyridinium chloride mouthwash versus chlorine dioxide + zinc mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 44 | Mean Difference (IV, Random, 95% CI) | ‐0.33 [‐0.72, 0.06] |
| 2 VSC | 1 | 44 | Mean Difference (IV, Random, 95% CI) | 0.49 [‐8.68, 9.66] |
Comparison 26. Halita mouthrinse versus Perio‐plus.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 36 | Mean Difference (IV, Random, 95% CI) | ‐0.20 [‐0.86, 0.46] |
| 2 VSC | 1 | 36 | Mean Difference (IV, Random, 95% CI) | ‐25.0 [‐64.21, 14.21] |
Comparison 27. Oil water 2‐phase mouthwash versus control mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 50 | Mean Difference (IV, Random, 95% CI) | ‐11.0 [‐25.26, 3.26] |
Comparison 28. Triphala and Ela decoction versus chlorhexidine mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 60 | Mean Difference (IV, Random, 95% CI) | 0.20 [0.09, 0.31] |
Comparison 29. Miswak mouthwash versus chlorhexidine mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 21 | Mean Difference (IV, Random, 95% CI) | 0.01 [‐0.95, 0.97] |
| 2 VSC | 1 | 21 | Mean Difference (IV, Random, 95% CI) | ‐0.20 [‐1.03, 0.63] |
| 3 Patient self‐assessment score | 1 | 21 | Mean Difference (IV, Random, 95% CI) | ‐0.18 [‐1.59, 1.23] |
Comparison 30. Chlorine dioxide mouthrinse versus chlorhexidine mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC (hydrogen sulphide) | 1 | 22 | Mean Difference (IV, Random, 95% CI) | ‐11.0 [‐31.61, 9.61] |
| 2 VSC (methyl mercaptan) | 1 | 22 | Mean Difference (IV, Random, 95% CI) | 7.63 [‐1.70, 16.96] |
| 3 VSC (methyl sulphide) | 1 | 22 | Mean Difference (IV, Random, 95% CI) | 22.80 [‐33.18, 78.78] |
Comparison 31. Protease cysteine + actinidine versus placebo tablets.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 14 | Mean Difference (Random, 95% CI) | ‐45.8 [‐258.38, 166.78] |
Comparison 32. Miswak stick versus chlorhexidine mouthwash.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 24 | Mean Difference (IV, Random, 95% CI) | ‐0.55 [‐1.33, 0.23] |
| 2 VSC | 1 | 24 | Mean Difference (IV, Random, 95% CI) | ‐0.77 [‐1.19, ‐0.35] |
| 3 Patient self‐assessment score | 1 | 24 | Mean Difference (IV, Random, 95% CI) | ‐0.26 [‐1.16, 0.64] |
Comparison 33. Brushing + mouthwash versus brushing + tongue cleaning.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 VSC | 1 | 30 | Mean Difference (IV, Random, 95% CI) | ‐81.87 [‐140.12, ‐23.62] |
Comparison 34. Brushing + cetylpyridium mouthwash versus brushing.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 70 | Mean Difference (IV, Random, 95% CI) | ‐0.48 [‐0.72, ‐0.24] |
| 2 VSC | 1 | 70 | Mean Difference (IV, Random, 95% CI) | ‐8.04 [‐15.87, ‐0.21] |
Comparison 35. Turkish gall oral rinse versus brushing alone.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 66 | Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.50, 0.30] |
| 2 VSC | 1 | 66 | Mean Difference (IV, Random, 95% CI) | ‐211.47 [‐503.58, 80.64] |
Comparison 36. Laser + povidone iodine versus SRP.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dentist‐reported OLT score | 1 | 40 | Mean Difference (IV, Random, 95% CI) | 0.49 [0.30, 0.68] |
| 2 VSC | 1 | 40 | Mean Difference (IV, Random, 95% CI) | 70.0 [63.88, 76.12] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Acar 2019.
| Methods | Location/setting: Periodontology Department, Dental Faculty of Hacettepe University, Ankara, Turkey Number of centres: 1 Recruitment period (duration): 1 week Trial design (including number of arms): RCT, 2 parallel arms Trial registration number: not mentioned Funding source (or sponsored drugs/materials): funded by the Hacettepe University Scientific Research Project, Turkey (grant number THD‐2015‐5523) | |
| Participants | Total number before randomisation: 80 Inclusion criteria: probing depths were ≤ 3 mm at all sites, the value of gingival index > 0.1, lack of clinical attachment loss, and had not received any periodontal treatment or tongue cleaning instruction within the last 6 months Exclusion criteria: the presence of any systemic disease or medical conditions causing halitosis such as respiratory tract diseases, gastrointestinal system, kidney or liver disorders, neurologic or metabolic diseases (diabetes mellitus); using medicines or having salivary gland diseases that cause xerostomia; the intake of antibiotics or non‐steroidal anti‐inflammatory drugs within 3 months prior to the study; pregnancy or lactation; the use of a removable denture; ongoing orthodontic treatment; use of alcohol or cigarettes; having a tongue cleaning routine; subjects with tongue abnormalities; or the use of mouthrinses Age (SD) at baseline for each arm: aged 18 to 56 years, mean age: 30 ± 10.8 years Gender (% of males): 23 females, 13 males Sample size (per group): 18 Number randomised: 36 Method of assessing the outcome (calibration, name/company of the instrument/scale): gingival index (GI), plaque index (PI), bleeding on probing (BoP), and probing depth (PD) were performed for all participants with a periodontal probe. Tongue coating index, OLT score, and VSC levels were determined and GCF samples were collected at baseline Number evaluated (mention ITT or per protocol, if any): 36 Dropouts and reasons: 0 | |
| Interventions | Intervention: Group 1 (G1) received oral hygiene instructions including the use of tongue scraper (once per day for 15 seconds on the dorsum of the tongue) Comparison: Control: Group 2 (G2) received oral hygiene instructions alone without tongue cleaning Duration of treatment: 1 week Duration of follow‐up: baseline and after 1 week |
|
| Outcomes | OLT score ‐ Rosenberg scale ranging from 0 to 5 VSC levels ‐ portable sulphur monitor (halimeter) used to detect the total concentration of VSC in the breath (Halimeter®, Interscan Corp, Chatsworth, CA, USA) Any adverse events reported: not mentioned | |
| Notes | Sample size calculation: not mentioned
Key conclusions of the study authors: "Oral prophylaxis including tongue scraping might be considered as an effective method for improving intra‐oral halitosis and local cytokine response in gingivitis patients" Contact: Buket Acar, Department of Periodontology, Faculty of Dentistry, Hacettepe University, 06100 Ankara, Turkey; buket.acar@hacettepe.edu.tr |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Coin toss method |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All 36 participants evaluated. No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Ademovski 2012.
| Methods | Location/setting: Dental Clinic University of Kristianstad, Sweden Number of centres: 1 Recruitment period (duration): 2008 to 2009 Trial design (including number of arms): 4 arms, cross‐over trial, with wash‐out period of 1 week Trial registration number: not mentioned Funding source (or sponsored drugs/materials): The Research Foundation at Kristianstad University, Kristianstad, Sweden and from Antula Healthcare AB, Stockholm, Sweden | |
| Participants | Total number before randomisation: 53 Inclusion criteria: halitosis of intraoral origin, OLS > 2, T‐VSC > 160 ppb, as determined with a halimeter Exclusion criteria: untreated periodontitis defined as the presence of more than 1 periodontal pocket with a probing pocket depth > 6 mm, open caries lesions, pregnancy, systemic medications known to cause hyposalivation, systemic antibiotic therapy within the preceding 3 months prior to the study, current smoker, medical history with a disease known to be associated with extraoral halitosis Age (SD) at baseline for each arm: 45.7 ± 13.3 years Gender (% of males): 52.4% males Sample size (per group): 21 Number randomised: 21 Method of assessing the outcome (calibration, name/company of the instrument/scale): halimeter (Interscan Corporation, Chatsworth, CA, USA) was used to assess total VSC in breath air; OralChroma (ABIMEDICAL Corporation, Kawasaki City, Japan) was used to assess H2S, MM and DMS Number evaluated (mention ITT or per protocol, if any): none Dropouts and reasons: 0 | |
| Interventions | Intervention: 4 parallel arms, procedure sequence:
Comparison: 4 interventions Dosage: 10 ml of the provided solution during 1 minute twice daily and then to spit out the rinse solution. Active mouthrinse included water, glycerin, sorbitol, alcohol (1.8%), zinc acetate (0.3%), chlorhexidine diacetate (0.025%), sodium fluoride (0.05%), hydrogenated Castro oil, citric acid, acesulphame potassium, menthol and mentha piperita (SB12, Antula Healthcare AB, Stockholm, Sweden). Composition of the inactive mouthrinse contained the same ingredients except that the inactive mouthrinse did not include zinc acetate, chlorhexidine diacetate or sodium fluoride Total number of intervention groups: 4 Duration of treatment: 14 days Duration of follow‐up: 4 time points |
|
| Outcomes | OLT assessment scores ‐ subjective assessments of intraoral halitosis performed using an arbitrary 0 = no halitosis to 5 = offensive halitosis H2S, MM and DMS assessment at 4 time points after any intervention using OralChroma and halimeter Any adverse events reported: not mentioned | |
| Notes | Sample size calculation: estimated based on the assumption that the negative control rinse would provide limited to no effects on VSCs, whereas the active rinse should reduce VSCs by 40%. Thus, a sample size of 20 subjects should provide statistical power (85%) Key conclusions of the study authors: "The use of a tongue scraper did not provide additional benefits to the active mouthrinse, but reduced OLS and tongue coating index" Contact: Professor Stefan Renvert, Department of Oral Health Sciences, Section for Health and Society, Kristianstad University, 291 88 Kristianstad, Sweden; stefan.renvert@hkr.se |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Subjects were randomly assigned to protocol sequence order (Latin square) using a computer‐based randomisation software program IBM/SPSS 18.0 (IBM, Corporation Somers, NY)" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Study subjects and examiner (SEA) were unaware of sequence assignment" Comment: however, it is not clear which method was employed to conceal the allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Study subjects, but not the examiner (SEA), knew, of course, if they, during the specific study sequence, had used the tongue scraper or not" Quote: "The rinse products were, however, bottled in the same type of bottles and labelled such that the subjects and the investigator were unaware if the subjects had been using the active or negative control rinse solutions during the dedicated study sequence" Comment: however, the outcome measurements (OLT and Halimeter readings) were done by investigator which would have not been influenced by the absence of patient blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "One and the same investigator (SEA) performed all registrations" Quote: "The rinse products were, however, bottled in the same type of bottles and labelled such that the subjects and the investigator were unaware if the subjects had been using the active or negative control rinse solutions during the dedicated study sequence" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | Baseline data assessments at the beginning of each intervention sequence were comparable and indicate that the 1 week wash‐out period was sufficient to control for any carry‐over effect. Cross‐over study design is appropriate for such stable and chronic conditions where the interventions have a temporary effect |
Ademovski 2017.
| Methods | Location/setting: Department of Oral Health Science, University of Kristianstad, Sweden Number of centres: 4 Recruitment period (duration): December 2011 to August 2013 Trial design (including number of arms): double‐blind placebo‐controlled RCT Trial registration number: not mentioned Funding source (or sponsored drugs/materials): Research Foundation Krsitianstad University Sweden & Research Grant Antula Health Care AB, Stockholm, Sweden (now acquired by Meda OTC AB) |
|
| Participants | Total number before randomisation: 70 Inclusion criteria: healthy individuals required to have: more than or equal to 20 teeth, bleeding on probing (BOP) more than or equal to 20%, halitosis of intraoral origin, an OLS more than or equal to 2, and a T‐VSC concentration > 160 ppb prior to the first dose of study treatment; to avoid selecting individuals with morning halitosis, the study screenings were not performed in the morning Exclusion criteria: open carious lesions, periodontal pockets with probing depths more than or equal to 6 mm, pregnant or had used either systemic medication resulting in hyposalivation, systemic antibiotic therapy within the preceding month of the study Age (SD) at baseline for each arm: intervention group 51.04 years (range 22 to 71); placebo group 46.55 (range 24 to 77) Gender (% of males): intervention 33.3% males; placebo 54.5% males Sample size (per group): intervention 24; placebo 22 Number randomised: 46 Method of assessing the outcome (calibration, name/company of the instrument/scale): OLS, measurement of T‐VSC, H2S, MM, DMS using halimeter and portable gas chromatograph (OralChroma Model CHM‐1, software OralChroma data manager version 3.04, Hyogo, Japan) Number evaluated (mention ITT or per protocol, if any): 46 (ITT analysis was done) Dropouts and reasons: 2 from intervention and 1 from control group could not complete the 6‐months follow‐up. However, reasons for dropouts were not given |
|
| Interventions | Intervention: rinsing 10 ml in the mouth for 1 minute, twice daily. Morning rinsing was done after toothbrushing, post‐breakfast, and evening rinsing was done before bedtime. During the study period of 6 months, no additional periodontal treatment was performed Comparison: control group: mouthrinse contained the same ingredients except for the active substances (0.3% zinc and 0.025% CHX) Dosage: test rinse contained 0.3% zinc and 0.025% CHX, aqua, glycerin, hydrogenated starch hydrolysate, alcohol, sodium fluoride, PEG‐40, hydrogenated castor oil, potassium acesulphame, citric acid and aroma (CB12, Meda OTC AB, Solna Sweden) Total number of intervention groups: 1 Duration of treatment: 1 minute twice daily Duration of follow‐up: 3 and 6 months |
|
| Outcomes | OLS, and measurement of T‐VSC, H2S and MM in exhaled air The intensity of bad breath was assessed by a trained odour judge (SEA) using the 0 to 5 OLT scale by Rosenberg: 0 = no odour; 1 = barely noticeable odour; 2 = slightly but clearly noticeable odour; 3 = moderate odour; 4 = strong odour; 5 = extremely strong odour close to saturation The total concentration of oral VSCs was assessed using measurement of total VSCs in breath air using a sulphide monitor. H2S and MM concentrations in mouth air were measured by a portable gas chromatograph. All assessments including OLS scores and VSC values were registered at baseline, 3 months and 6 months Any adverse events reported: not mentioned |
|
| Notes | Sample size calculation: based on the previous study by the authors (Ademvoski 2016) sample size was calculated to be 20 subjects per group (α‐level = 95%) Key conclusions of the study authors: "Rinsing with a Zn/CHX mouthrinse provides statistically significant improvement in subjectively assessed intra‐oral halitosis, as well as a significant reduction in volatile sulphur compounds in exhaled air compared to placebo mouthrinse at both 3 and 6 months. With regular use, the Zn/CHX effect is sustained for 6 months" Contact: School for Health and Society, Kristianstad University, 29188, Kristianstad, Sweden; seida.erovic_ademovski@hkr.se |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A computer‐based randomisation program IBM SPSS 22.0 (IBM, Corp., Armonk, NY, USA) was used to randomise the participants into two groups – intervention and placebo" |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Both the examiner and study participants were unaware of mouthrinse used. The non‐active mouthrinse had a similar flavour as the active treatment rinse but without any of the active ingredients. All bottles with mouthrinses were distributed in coded non‐transparent bottles but otherwise with the same appearance" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Clinical examination was performed by one trained investigator (SEA)" Comment: however, it is not clear if the examiner was blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 from intervention and 1 from control group could not complete the 6‐months follow‐up and reasons were not given. ITT analysis was followed in the report. However, the sample size calculated for 95% power is 20 per group which was not affected by the dropouts |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Unclear risk | Quote: "Another limitation of the study is the lack of compliance control" Comment: we are not sure how this could have affected the overall results |
An 2011.
| Methods | Location/setting: Department of Periodontology, Peking University School and Hospital of Stomatology, China Number of centres: 1 Recruitment period (duration): October 2008 to September 2009 (11 months) Trial design (including number of arms): 2‐arm parallel group Trial registration number: not reported Funding source (or sponsored drugs/materials): National Key Project of Scientific and Technological Supporting Programs of China (2007BAZ18B02) | |
| Participants | Total number before randomisation: 70
Inclusion criteria: candidates selected according to 1999 periodontal disease classification of gingival disease with no attachment loss (AL), probing depth (PD) ≥ 4 mm, at least 1 bleeding on probing (BOP)
mild to moderate chronic periodontitis AL ≥ 4 mm, at least 1 BOP +, x‐ray showing neighbouring alveolar bone resorption not more than half of root length; C/O halitosis and confirmed halitosis cases; non‐smoker; no systemic disease especially respiratory disease and tonsillitis, etc.; no history of periodontitis in the past half year; with at least 20 teeth in the oral cavity; no obvious food impaction and wisdom tooth that is hard to clean properly; absence of faulty prostheses; no ongoing treatment of dental disease; absence of salivary gland and mucosal disease; no ongoing orthodontic treatment; absence of history of taking antibiotics and mouthwash for the past 1 month; and female candidate selected should be not be on her menstrual period or pregnant or in her nursing period
Exclusion criteria: chronic severe periodontitis and aggressive periodontitis
Age (SD): intervention: mean 32.8 ± 9.2 years; control: mean 36.5 ± 10.2 years
Gender (% of males): intervention: 19 male and 18 female; control: 22 male and 11 female
Sample size (per group): intervention 37; control 33
Number randomised: 70 (intervention: 37, control: 33)
Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT method, halimeter test (RH‐17, Interscan, USA) Number evaluated (mention ITT or per protocol, if any): 66 (intervention: 36, control: 30) Dropouts and reasons: no dropouts, but 4 participants (1 in treatment group, 3 in control group) were further excluded because their OS remained ≥ 2, which indicates that their halitosis was not from their oral cavity |
|
| Interventions | Intervention: Turkish gall rinse. Both groups were given the same soft toothbrushes and sodium fluoride toothpaste, underwent same oral hygiene instructions and proper brushing techniques were taught
Comparison: control group Dosage: rinse for 2 weeks, thrice a day, each rinse using 5 ml for 2 minutes Total number of intervention groups: 1 Duration of treatment: 2 weeks Duration of follow‐up: 2 weeks |
|
| Outcomes | The outcomes were assessed before and after the trial (at the beginning and 2 weeks) OLT assessment scores: a trained odour panellist assessed OLT score (OS) as 6 levels according to Rosenberg's grading standards VSC: assessed by halimeter (RH‐17, Interscan, USA). The average of 3 consecutive measurements was recorded Any adverse events reported: not given |
|
| Notes | Sample size calculation: not reported Key conclusions: "oral rinse of Turkish gall displayed significant inhibition of dental plaque without staining, while no predominated effect on halitosis when compared to correct conventional plaque control methods" Contact: He Lu; Department of Periodontology, Peking University School and Hospital of Stomatology, Beijing 100081, China; helubj@tom.com |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The random number table was kept by a pharmacist" |
| Allocation concealment (selection bias) | Low risk | Quote: "The random number table was kept by a pharmacist ...the pharmacist allocated the included patients into the treatment group and control group according to the random number table" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Single blinded study. Dentist was blinded for the grouping of patients, however, patients were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Single blinded study" Quote: "Doctors do not know participants' grouping situation" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No dropouts. Though 4 participants (1 in treatment group, 3 in control group) were further excluded because they were found to be ineligible, there was less than 10% attrition |
| Selective reporting (reporting bias) | Unclear risk | Adverse effects not mentioned |
| Other bias | Low risk | No other source of bias identified |
Asokan 2011.
| Methods | Location/setting: Department of Periodontic Dentistry, Meenakshi Ammal Dental College, Chennai, India Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): 2 parallel arms Trial registration number: not available Funding source (or sponsored drugs/materials): unclear | |
| Participants | Total number before randomisation: 20 Inclusion criteria: 20 age‐matched healthy adolescents, should have at least 24 permanent teeth with gingival probing depth < 3 mm, gingival and plaque index score = 1 in more than 10% of the sites Exclusion criteria: history of antibiotics for past 3 to 4 weeks, wear orthodontic appliances or prosthesis, smokers and participants with deep‐fissured tongue Age (SD) at baseline for each arm: 17 to 19 years but no mention of SD Gender (% of males): not mentioned Sample size (per group): 10 Number randomised: 20 Method of assessing the outcome (calibration, name/company of the instrument/scale): modified gingival index (MGI), plaque index (PI), and probing depth (PD); OLT breath assessment (ORG1) by a blinded and calibrated examiner (examiner A); self‐assessment of breath (ORG2) by participants themselves; BANA test from tongue coating samples (Examiner B) on days 0 and 14 of the experimental period Number evaluated (mention ITT or per protocol, if any): 20 Dropouts and reasons: none | |
| Interventions | Intervention: study group was subjected to oil pulling with sesame oil (Idhayam Oil, VVV Sons India) for 10 to 15 minutes every day in the morning before brushing. The participants of both groups were allowed to brush their teeth once daily as per their daily home oral hygiene schedule Comparison: control: was given 0.2% CHX mouthwash (Hexidine, ICPA Health Products Ltd, India) for 1 minute every day in the morning for 14 days Dosage: not mentioned Total number of intervention groups: 2 Duration of treatment: oil pulling 10 to 15 minutes every day and CHX 1 minute every day for 14 days Duration of follow‐up: 14 days |
|
| Outcomes | OLT assessment: participants were asked to keep their mouths completely closed for 3 minutes, breathing only through the nose. After the time had elapsed they were instructed to release the air slowly through the mouth from a distance of 10 cm from the examiner's nose. Asking the participant to lick his wrist and smell it after it has dried constituted the self‐assessment part. The intensity ratings of 0 to 5 score, as proposed by Rosenberg and McCulloh was used (0 = no odour present, 1 = barely noticeable odour, 2 = slight but clearly noticeable odour, 3 = moderate odour, 4 = strong offensive odour, 5 = extremely foul odour) BANA test Any adverse events reported: not mentioned | |
| Notes | Contact: Dr Sharath Asokan, Department of Paediatric Dentistry, Meenakshi Ammal Dental College, Alapakkam Main Road, Tamil Nadu, Chennai ‐ 600 095, India; asokansharath@yahoo.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Simple random number table" |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote:"Blinded and calibrated examiner (examiner A)" Comment: patients were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote:"Blinded and calibrated examiner (examiner A)" Quote: "Self‐assessment of breath (ORG2) by participant themselves" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events are not mentioned |
| Other bias | Low risk | None |
Aung 2015.
| Methods | Location/setting: Yangon, Myanmar but unclear of setting Number of centres: 1 Recruitment period (duration): September to October 2013 Trial design (including number of arms): 2 parallel arms Trial registration number: NCT02113137 Funding source (or sponsored drugs/materials): not mentioned | |
| Participants | Total number before randomisation: 48 Inclusion criteria: no systemic disease, no current use of antibiotics, no severe dental caries, no periodontal pocket > 3 mm, no history of allergy to any mouthwash, no smoking and betel nut chewing Exclusion criteria: not mentioned Age (SD) at baseline for each arm: 20.18 +2.8 years Gender (% of males): 100% males Sample size (per group): 15 Number randomised: 30 Method of assessing the outcome (calibration, name/company of the instrument/scale): total VSC by portable sulphide monitoring device (Breathtron® Yoshida, Tokyo, Japan); bleeding on probing by periodontal probe (University of North Carolina, UNC‐15, USA); tongue coating using WTCI Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: none | |
| Interventions | Intervention: Group A: toothbrushing and mouthwashing 1st to 4th week (4th to 5th week all 3 methods)
Comparison: Group B: toothbrushing and tongue cleaning 1st to 4th week (4th to 5th week all 3 methods) Dosage: toothpaste usage depended on the subject's choice. For the next 3 weeks, both groups continued toothbrushing; Group A used 12 mL of chlorine dioxide (ClO2) Fresh® mouthwash (Bio‐Cide International, Inc, Oklahoma, USA and Pine Medical Co, Tokyo, Japan) for 30 seconds twice daily, and Group B performed tongue cleaning twice daily with a small toothbrush Total number of intervention groups: 2 Duration of treatment: 5 weeks Duration of follow‐up: weekly |
|
| Outcomes | Debris Index score of the OHI: 0 = no debris or stain present; 1 = soft debris covering not more than a third of the tooth surface being examined, or the presence of extrinsic stains without debris, regardless of surface area covered; 2 = soft debris covering more than a third but not more than 2 thirds of the exposed tooth surface; 3 = soft debris covering more than 2 thirds of the exposed tooth surface. The highest score for each tooth was recorded
Tongue coating: evaluated by a modified Winkel tongue‐coating index. The tongue dorsum was divided into 9 areas and tongue coating was evaluated for all 9 areas with a score of 0 = no coating, 1 = a light coating (a thin tongue coating with clearly visible papillae), and 2 = a thick coating (a dense coating totally covered the papillae and they were not visible). The tongue coating score was calculated by adding the scores of all 9 areas, resulting in a possible range from 0 to 18
Saliva measurement: subjects were requested to spit out all saliva into a collecting paper cup for 5 minutes. The flow rate of saliva (mL/min) was calculated, and the saliva pH level was measured with a bromothymol blue test paper Changes in malodour: reductions in VSC (ppb) weekly Any adverse events reported: not mentioned |
|
| Notes | Contact: Department of Oral Health Promotion, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, 1‐5‐45 Yushima, Bunkyo‐ku, Tokyo 113‐8549, Japan; ueno.ohp@tmd.ac.jp | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation system |
| Allocation concealment (selection bias) | Low risk | Subjects were allocated to each group using random sequences by a person not related with the current study |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Single‐blind study. Participants were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Total VSCs, debris index (DI) score, bleeding on probing (BOP), and tongue coating were examined at the baseline and weekly during the 5 weeks by a principal investigator who was blinded to the examined subject's group" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Unclear risk | Though baseline characteristics are similar, type of toothpaste used varied between individuals in both the groups and it is not clear if they changed their toothpaste during the study period |
Barak 2012.
| Methods | Location/setting: Department of Oral Diagnostic Sciences, University of Florida College of Dentistry, USA Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): RCT 5 arms Trial registration number: not mentioned Funding source (or sponsored drugs/materials): Breeze LTD Israel | |
| Participants | Total number before randomisation: 75 Inclusion criteria: healthy, suffer from halitosis, subjects were asked to refrain from food, or using mouthwash or toothbrushing for 10 hours prior the first visit Exclusion criteria: subjects who suffer from diabetes, renal disease, on chemotherapy, medications, smokers, had oral diseases for the last 3 months, pregnant or using dentures Age (SD) at baseline for each arm: 38 ±14 years Gender (% of males): 64% males Sample size (per group): 15 Number randomised: 75 Method of assessing the outcome (calibration, name/company of the instrument/scale): the subject was instructed to close his/her mouth and keep his/her lips sealed in preparation for sampling mouth air. Halimeter measurements were taken by a trained nurse 3 times for each visit, and mean values of each visit were used for the analysis Number evaluated (mention ITT or per protocol, if any): none Dropouts and reasons: none | |
| Interventions | Intervention: patients were randomly divided into 5 groups
Comparison: control group: treated by commercial lollipop Candy, without the abrasive capabilities and without any additional antibacterial substances Dosage: not mentioned Total number of intervention groups: 4 Duration of treatment: 4 weeks Duration of follow‐up: 1 week interval |
|
| Outcomes | Assessment by using halimeter per cent change till 4 visits at 1 week interval Any adverse events reported: not mentioned | |
| Notes | Contact: Joseph Katz, Department of Oral Diagnostic Sciences, University of Florida College of Dentistry, PO Box 100414, Gainesville FL 32606, USA; jkatz@dental.ufl.edu | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Each envelop was marked by a number randomly distributed according to a computerized random permutation system" |
| Allocation concealment (selection bias) | Low risk | Quote: "Each enrolled subject was given a sealed envelope containing the randomly chosen candy (one of 5 options). All documentation in the CRF relating to the treatment were designated by the envelope's number only. Coding was not broken during the entire study" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Both the participating subject and the investigator were blinded to the type of the candy chosen to the treatment" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Both the participating subject and the investigator were blinded to the type of the candy chosen to the treatment" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events are not mentioned |
| Other bias | Low risk | None |
Borden 2002.
| Methods | Location/setting: Hill Top Research Inc, Cincinnati, Ohio, USA Number of centres: 1 Recruitment period (duration): 4 weeks Trial design (including number of arms): randomised, double‐blind, longitudinal clinical trial with 4 arms Trial registration number: not mentioned Funding source (or sponsored drugs/materials): Discus Dental, Inc, Culver City, California |
|
| Participants | Total number before randomisation: 138 Inclusion criteria: good general health, male or female, 18 to 65 years of age, signed informed consent, 2‐judge average intensity score of ≥ 4, minimum 16 natural teeth with at least 4 molars, availability to complete 4‐week study Exclusion criteria: gross oral pathoses, orthodontic devices, partial or complete dentures, systemic diseases, irritation or sensitivity to oral products, pregnant or lactating women, periodontal disease pocket depth > 4 mm and/or bleeding on probing on > 6 non‐adjacent sites, gross neglect of oral hygiene, smokers, prophylactic antibiotic coverage for RCT, systemic antibiotics or prescription mouthwash 21 days before the study, current participation in other dental or investigational trials, concomitant drug therapy, alcohol abuse, recent history of bronchitis, tonsillitis or sinusitis, if received emergency dental treatment during study, loss of teeth during study if more than minimum requirement, course of antibiotic or antibacterial agent during study Age (SD) at baseline for each arm: 19 to 65 years Gender (% of males): 30.5% Sample size (per group): Group 1: 25, Group 2: 25, Group 3: 23, Group 4: 22 Number randomised: 95 Method of assessing the outcome (calibration, name/company of the instrument/scale): 2 OLT judges, halimeter (Interscan Corporation, Chatsworth, CA 91313‐2231) Number evaluated (mention ITT or per protocol, if any): 89 Dropouts and reasons: 5 (3: low OLT score, 1: withdrew consent after 1st visit, 1: cellulitis) |
|
| Interventions | Intervention: Group 1: Listerine antiseptic rinse (essential oil); Group 2: BreathRx mouthrinse (CPC), Group 4: Oxygene mouthwash (CD/Zn) Comparison: Group 3 ‐ placebo rinse Dosage: twice daily according to supplied instructions Total number of intervention groups: 3 Duration of treatment: 4 weeks Duration of follow‐up: baseline, 15 minutes, 2 hours and 4 hours at 0, 2 and 4 weeks |
|
| Outcomes | OLT assessment scores: 0 = no odour present, 1 = barely noticeable odour, 2 = slight but clearly noticeable odour, 3 = moderate odour, 4 = strong offensive odour, 5 = extremely foul odour (Rosenberg) Assessment by using halimeter (Interscan Corporation, Chatsworth, CA 91313‐2231, Model RH‐17K) Any adverse events reported: 13, lip blisters, localized gingival aedema, canker sores, all were later determined as unrelated to product use |
|
| Notes | Contact: Gary M Hollar, Director of Regulatory Affairs, Discuss Dental, Inc, Culver city, California, USA | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind (subjects and examiners) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind (subjects and examiners) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropouts before or after randomisation were not clearly mentioned |
| Selective reporting (reporting bias) | Low risk | All objectives are reported adequately |
| Other bias | Low risk | None evident |
Caygur 2017.
| Methods | Location/setting: Department of Periodontology, Faculty of Dentistry, Turkey Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): 2 parallel arms Trial registration number: not mentioned Funding source (or sponsored drugs/materials): none | |
| Participants | Total number before randomisation: 60 Inclusion criteria: those who had at least 3 teeth with 4 to 6 mm periodontal pockets undergoing periodontal treatment Exclusion criteria: acute infectious oral lesions, furcation defects, use of antibiotics for any reason within the last 4 weeks, periodontal treatment within the last 6 months, pregnancy, lactation Age (SD) at baseline for each arm: 28 to 68 years Gender (% of males): not mentioned Sample size (per group): not mentioned Number randomised: 60 Method of assessing the outcome: Perio‐Flow device (Electro Medical Systems, Nyon, Switzerland); using periodontal probe at 6 sites on all teeth to measure: Plaque Index (PI), Gingival Index (GI), clinical attachment level (CAL), pocket depth, position of the gingival margin, and bleeding on probing (BOP), VSC levels using portable sulphide monitor (halimeter) Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: not mentioned | |
| Interventions | Intervention: SRP with ultrasonic and hand instrumentation, GPAP (Air‐Flow PerioPowder Electro Medical Systems) was performed for 10 seconds per periodontal pocket using a Perio‐Flow device (Air‐Flow Master, Electro Medical Systems)
Comparison: control group: SRP was performed using an ultrasonic scaler (Piezon Master 700; Electro Medical Systems, Nyon, Switzerland) and hand instrumentation. Dosage: none Total number of intervention groups: 2 Duration of treatment: 30 days Duration of follow‐up: none |
|
| Outcomes | VSC prior to and at several time points after intervention using halimeter Changes in outcome parameters using periodontal probe Any adverse events reported: not mentioned | |
| Notes | Contact: Hasan Guney Yilmaz, Department of Periodontology, Faculty of Dentistry, Near East University, Mersin, 33000, Turkey; guneyyilmaz@hotmail.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computer‐randomised" |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "This was a computer‐randomised, single blind, controlled clinical study" Quote: "Measured at baseline and 1 month after treatment by a single calibrated examiner who was not aware of the type of treatment applied" |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "This was a computer‐randomised, single blind, controlled clinical study" Quote: "Measured at baseline and 1 month after treatment by a single calibrated examiner who was not aware of the type of treatment applied" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events are not mentioned |
| Other bias | Low risk | None |
Dadamio 2013.
| Methods | Location/setting: University Hospital of the Catholic University of Leuven, Belgium Number of centres: 1 Recruitment period (duration): April 2007 and July 2011 Trial design (including number of arms): double‐blind, randomised, parallel‐group clinical trial Trial registration number: not mentioned Funding source (or sponsored drugs/materials): supported by GABA International AG, Grabetsmattweg, 4106 Therwil, Switzerland | |
| Participants | Total number before randomisation: 739 Inclusion criteria: age between 18 and 70 years, OLT scores > 2, halimeter readings of at least 150 ppb, intraoral cause of bad breath, non‐smoker Exclusion criteria: an ongoing dental or medical treatment, allergy to previously used oral hygiene products/any known allergy to any of the ingredients of the study products, pathological change of the oral mucosa, use of prohibited treatments or therapies and/or abuse of drugs or alcohol, pregnancy or breastfeeding, participation in a clinical study within the previous 30 days, active caries, acute sinusitis, medication which can cause malodour, reduced salivary flow due to pathological reasons (e.g. Sjogren syndrome), conditions not compatible with the study according to the investigator's opinion (e.g. patients eating very spicy food, persons under homeopathic therapy, patients who used antibiotics during the 2 months before the study, patients frequently using chewing gum, patients under corticosteroids or other serious medications, non‐Caucasians, patients unwilling to abstain from additional oral hygiene, particularly mouthrinses, chewing gums, breath strips Age (SD) at baseline for each arm: mean age 48.2 years Gender (% of males): 62.2% males Sample size (per group): 18 Number randomised: 98 Method of assessing the outcome (calibration, name/company of the instrument/scale): smell identification test (Sensonics Inc, Haddon Heights, NJ, USA) score 0 to 5; initial screening with the halimeter, a portable gas chromatograph (OralChroma™, Abilit Corporation, Kanagawa, Japan) was used to measure the concentration of H2S, CH3; SH and (CH3)2S separately Number evaluated (mention ITT or per protocol, if any): 90 Dropouts and reasons: 4 dropouts and 4 other volunteers were withdrawn from the study by the principal investigator after notification of antibiotic intake during the study period or participation in parallel in another trial. All of them were replaced with new volunteers to maintain 90 | |
| Interventions | Intervention: 5 groups: 3 formulations (halita TM (H), meridol (M) and meridol formulation with the addition of zinc lactate (M + Zn)) Comparison: fluoride rinse considered negative control (NC) and 0.12% CHX‐based rinse positive control (PC) Dosage: 15 ml twice/day Total number of intervention groups: 5 Duration of treatment: 7 days Duration of follow‐up: 15 minutes after first rinse at day 1, 12 hours after latest rinse at day 8 |
|
| Outcomes | OLT evaluation through Smell Identification Test (0 to 5) VSC reading portable gas chromatograph: initial screening with the halimeter, a portable gas chromatograph was used to measure the concentration of H2S, CH3SH and (CH3)2S separately Microbiological samples: saliva and tongue coating samples were taken during both visits for the analysis of the microbiota Any adverse events reported: 4 adverse events were reported during the study; 3 regarding unpleasant feelings after the use of the product (1 each for NC, PC and H) and 1 other involving tooth staining (H). There were no severe adverse events | |
| Notes | Contact: Marc Quirynen, Catholic University Leuven,, Department of Periodontology, Kapucijnenvoer, 33, 3000 Leuven, Belgium; marc.quirynen@med.kuleuven.be | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation schedule was generated for a parallel group trial design with 23 blocks of 5 subjects using software employing a pseudo‐random number generator according to Algorithm AS 183 (Wichmann & Hill 1982)" |
| Allocation concealment (selection bias) | Low risk | Quote: "Random allocation sequence was generated by the GMP manager of the sponsor" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Patients, odour judge and investigator were blinded regarding the product allocation" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Patients, odour judge and investigator were blinded regarding the product allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "4 dropouts and 4 other volunteers were withdrawn from the study by the principle investigation after notification of antibiotic intake during the study period or participation in parallel in another trial. All of them were replaced with new volunteers to maintain 90" |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported adequately |
| Other bias | High risk | Quote: "4 dropouts and 4 other volunteers were withdrawn from the study by the principle investigation after notification of antibiotic intake during the study period or participation in parallel in another trial. All of them were replaced with new volunteers to maintain 90" Comment: if these 8 new volunteers are included after randomisation, there is a risk of breaching the random sequence and the entire randomisation process becomes questionable |
Feres 2015.
| Methods | Location/setting: Dental Clinic of Guarulhos University, Guarulhos, SP, Brazil Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): parallel 2 arms Trial registration number: not mentioned Funding source (or sponsored drugs/materials): not mentioned | |
| Participants | Total number before randomisation: 300 Inclusion criteria: availability for the duration of the study, at least 20 natural teeth with minimal restorations, good general health or health well controlled under a physician's care, age ≥18 years Exclusion criteria: medical condition that requires premedication before dental visits/procedures, use of any medication that may interfere with salivary flux, xerostomia, no carious lesions, no sites with probing depth 3 mm, more than 10% of sites presenting bleeding on probing or gingival bleeding, orthodontic appliances, use of antibiotics within last 6 months before or during the study, use of any OTC medications that would interfere with results, other than analgesics (i.e. aspirin, ibuprofen, acetaminophen or naproxen) at the time of informed consent, pregnant or breastfeeding mothers, immunocompromised individuals, history of allergies to oral care/personal‐care consumer products or their ingredients, history of alcohol, smoking or drug abuse Age (SD) at baseline: 24.3 (8.5) years Gender: 30 males and 40 females Sample size (per group): 35 Number randomised: 70 Method of assessing outcome (calibration, name of the instrument/scale): portable gas chromatograph (OralChromaTM ‐ Abilit Corporation, Osaka City, Japan) Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: none | |
| Interventions | Intervention: CPC group: brushing with regular fluoride toothpaste for 2 minutes, twice a day (morning and evening), followed by 30 seconds rinsing with 20 mL 0.075% CPC mouthwash (Colgate‐Palmolive Company, NY, USA) Comparison: control group: brushing with same toothpaste for 2 minutes, twice a day (morning and evening) Total number of intervention groups: 2 Duration of treatment: 21 days Duration of follow‐up: 21 days + 4 hours | |
| Outcomes | Odour rating on the following 6‐point scale: 0 = no odour (below smell threshold); 1 = barely noticeable odour; 2 = slight odour; 3 = moderate odour; 4 = strong odour; 5 = extremely strong odour VSC levels using a portable gas chromatograph (OralChromaTM) that measures the concentration of H2S, CH3SH and (CH3)2S displaying concentrations of gases in either ng/10 mL or ppb (nmol/mol) Any adverse events reported: none reported by the subjects | |
| Notes | Contact: Magda Feres, Centro de Posgraduacao e Pesquisa (CEPPE),Universidade Guarulhos, Praca Tereza Cristina, 229 – Centro –CEP 07023‐070, Guarulhos, SP, Brazil; mferes@ung.br | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Computer‐generated table" |
| Allocation concealment (selection bias) | Low risk | Quote: "Allocation concealment was achieved through the use of numbered, opaque, sealed envelopes by the study coordinator" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "The study coordinator, not involved in the clinical evaluations, distributed the oral hygiene products to the participants" Quote: "All products were stored in a sealed bag to remove any differences in product aesthetics and packaging between the study groups" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Judges measuring intra‐oral halitosis of subjects were blinded regarding one another's scores and their own previous scores for the OLT assessment" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Low risk | All outcomes were adequately reported |
| Other bias | Low risk | None |
Garcia 2014.
| Methods | Location/setting: not reported: participants received 1 session of ultrasonic professional scraping (does not say where), but the rest of the treatment, the use of mouthwash was conducted at participants' homes Number of centres: not reported Recruitment period (duration): not reported Trial design (including number of arms): RCT with 2 parallel arms, test and placebo Trial registration number: not reported Funding source (or sponsored drugs/materials): Fapesp (São Paulo Research Foundation) research support 2010/20424‐1 and scientific initiation scholarship PIBIC (Institutional Program of Scholarships for Scientific Initiation funded by the Brazilian Government) ODO063/2013 | |
| Participants | Total number before randomisation: 60 Inclusion criteria: individuals with gingivitis showing at least 30% of sites with bleeding (Lopez et al 2002), without radiographic evidence of alveolar bone reabsorption, of both genders, presenting a minimum of 20 teeth, good systemic health and normal salivary flow (1.5 ml to 2ml/min) and the absence of clinically evident lingual sores Exclusion criteria: not reported Age (SD) at baseline for each arm: not reported Gender (% of males): not reported Sample size (per group): in the abstract, the author reported that the test group had 27 participants and the placebo had 25. Then, on the first line of the results section, the author states "Each one of the two groups was composed by 20 adults systemically healthy and with gingivitis" Number randomised: 60 Method of assessing the outcome (calibration, name/company of the instrument/scale): determination of VSC using halimeter Number evaluated (mention ITT or per protocol, if any): 27 in the test and 25 in the placebo group finished the study (available in the abstract). In the results section, it states that 20 individuals composed each of the groups. It does not mention analysis per protocol or ITT. It is unclear how many participants per group were considered for analysis and the sample size Dropouts and reasons: not reported (not clear) | |
| Interventions | Intervention: essential oils (20 ml twice a day) Comparison: placebo solution (20 ml twice a day) Dosage: 20 ml Duration of treatment: 3 months Duration of follow‐up: 3 months (measurements were before and after treatment) |
|
| Outcomes | Determination of VSC: halitometry was conducted by a trained and calibrated examiner introducing a disposable straw connected to the reading device about 4 cm inside the oral cavity. The participant was instructed to stay with lips parted, not breathing for 15 seconds and the maximum peak was registered indicating the VSC oral concentration. The VSC results were interpreted as follows: 80: without perceptible odour; 80 to 100: perceptible odour; 100 to 120: moderated halitosis; 120 to 150: pronounced halitosis and > 150: severe halitosis. This measurement was repeated 3 consecutive times, creating a mean VSC Adverse events: not mentioned |
|
| Notes | Sample size calculation: not mentioned Key conclusions of the study authors: "Besides the reduction of the clinical GI parameter frequently observed in the literature, the professional treatment complemented by the daily use of solution containing essential oils was accompanied of superior reductions in the total subgingival bacterial load and VSC levels" Contact: Maíra Terra Garcia, Rua Expedicionário Ernesto Pereira, 110 – Centro, 12020‐330 Taubaté, SP Brazil; maa.terra@hotmail.com |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It mentions that a trained and calibrated examiner assessed the outcomes, but it does not inform if he/she was blinded to groups |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Discrepancy in the number of participants reported in the abstract and results section. Unclear what was the real number of losses/withdraws |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | No other source of bias identified |
Hu 2005.
| Methods | Location/setting: not mentioned Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): randomised, double‐blind, stratified, 2‐treatment design Trial registration number: not mentioned Funding source (or sponsored drugs/materials): not mentioned | |
| Participants | Total number before randomisation: 81 Inclusion criteria: not mentioned Exclusion criteria: not mentioned Age (SD) at baseline for each arm: test: 45.12 years; control: 44.33 years Gender (% of males): 53% males Sample size (per group): 41 test; 40 control Number randomised: 81 adults Method of assessing the outcome (calibration, name/company of the instrument/scale): hedonic scale Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: not mentioned | |
| Interventions | Intervention: 0.3% triclosan, 2% copolymer and 0.243% sodium fluoride in a silica base Comparison: control: 0.243% sodium fluoride in a silica base Duration of treatment: 3 weeks Duration of follow‐up: 3 weeks | |
| Outcomes | Oral odour rating was done using a 9‐point hedonic scale (1 = most pleasant, 5 = neutral and 9 = most unpleasant) at time points 1.5 hours, 4 hours, 12 hours, 1 week, 2 weeks and 3 weeks Determination of peak and steady‐state VSC levels using a sulphide monitor, prior to and at several time points after any intervention: none Any adverse events reported: not mentioned | |
| Notes | Contact: Dr Yun Po Zhang, Colgate‐Palmolive Technology Center, 909 River Road, Piscataway, NJ 08854‐1343, USA; yunpo_zhang@colpal.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not given |
| Allocation concealment (selection bias) | Unclear risk | Not given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "The study employed a double‐blind, stratified, two treatment design" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "The study employed a double‐blind, stratified, two treatment design" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Hu 2018.
| Methods | Location/setting: West China College of Stomatology, Sichuan University Chengdu, Sichuan, People's Republic of China Number of centres: 1 Recruitment period (duration): not given Trial design (including number of arms): 2 arms Trial registration number: not given Funding source (or sponsored drugs/materials): sponsored by the Colgate‐Palmolive Company | |
| Participants | Total number before randomisation: not given Inclusion criteria: aged between 18 and 70 (inclusive); in good general health; in good oral health based on self‐assessment; possess a minimum of 20 natural uncrowned teeth (excluding 3rd molars); and were available for the 3‐week duration of the study for all time point assessments, and signed an informed consent form Exclusion criteria: full or partial (upper or lower) dentures; immunocompromised (HIV, AIDS, immune suppressive drug therapy), medical conditions prohibiting them from not eating or drinking for the post‐use treatment evaluation time points (6 hours + overnight), pregnant or breastfeeding; use of tobacco and phenolic flavoured products such as mint flavoured candies or chewing gum, the morning of the study or during the sampling periods; history of allergies to personal care/consumer products or their ingredients or to common mouthwash ingredients; participating in any other clinical study during the duration of this study Age (SD) at baseline for each arm: intervention arm: 43.13 ±11.26 years; control arm: 43.23 ±10.62 years Gender (% of males): intervention arm: 23 males; control arm: 18 males Sample size (per group): 40 per group Number randomised: 80 Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT hedonic odour ratings (1: most pleasant and 9: most unpleasant). Following individual judge scoring, an overall score was determined for each subject by averaging the scores assigned by the 4 judges Number evaluated (mention ITT or per protocol, if any): 80 Dropouts and reasons: none | |
| Interventions | Intervention: a dual zinc + arginine dentifrice containing zinc (zinc oxide, zinc citrate) 0.96%, 1.5% arginine, and 1450 ppm F as NaF in a silica base (Colgate‐Palmolive Co, New York, NY, USA) Comparison: a regular fluoride dentifrice containing 1450 ppm fluoride as NaF in a silica base (Colgate‐Palmolive Co, New York, NY, USA) Dosage: brush twice/day for 1 minute with approximately 1.5 g of toothpaste for 3 weeks Total number of intervention groups: 1 Duration of treatment: 3 weeks Duration of follow‐up: 3 weeks |
|
| Outcomes | OLT assessment scores: 1 to 9 Any adverse events reported: not mentioned | |
| Notes | Sample size calculation: not mentioned Key conclusions of the study authors: "The overall results of this double‐blind clinical study support the conclusion that a new Dual Zinc + Arginine dentifrice containing zinc provides significantly greater reduction in oral malodour as compared to a regular fluoride dentifrice 12‐hours post‐brushing (overnight) after 3 weeks of product use" Contact: Dr Yun Po Zhang, Colgate‐Palmolive Company, Piscataway, NJ, USA; yunpo_zhang@colpal.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not given |
| Allocation concealment (selection bias) | Unclear risk | Not given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Qualifying subjects and all clinical study site personnel were blinded to product assignment. All dentifrices were covered with white over wrapping in order to conceal product identity" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Qualifying subjects and all clinical study site personnel were blinded to product assignment" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Iha 2013.
| Methods | Location/setting: Oral Malodour Clinic of Fukuoka Dental College Medical and Dental Hospital, Japan Number of centres: 1 Recruitment period (duration): December 2011 and November 2012 Trial design (including number of arms): open‐label RCT Trial registration number: not mentioned Funding source (or sponsored drugs/materials): Grant‐in‐Aid for Young Scientists (no. 23792532); Grant‐in‐Aid for Scientific Research (no. 23593078); Grant‐in‐Aid for Advanced Science Research from the Ministry of Education, Culture, Sports, Science and Technology, Japan, and by the MEXT‐Supported Program for the Strategic Research Foundation at Private Universities, 2012‐2016 | |
| Participants | Total number before randomisation: 18 Inclusion criteria: oral malodour scores above questionable levels (OLT > 1.5), not halitophobic, no acute symptoms requiring immediate oral cavity treatment or no antibiotic use within the previous month, did not smoke or consume alcohol above recommended levels (≤ 20 g/day), not on any medications, and no previous treatment for oral malodour Exclusion criteria: not mentioned Age (SD) at baseline for each arm: test group: 52.2 (11.4) years; control group: 57.2 (8.6) years Gender (% of males): test group: 33.3%, control group: 11.1% Sample size (per group): 9 Number randomised: 18 adults Method of assessing the outcome (calibration, name/company of the instrument/scale): oral malodour ‐ determined using an OLT test and gas chromatography (model GC2014; Shimadzu Works, Kyoto, Japan) Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: not mentioned | |
| Interventions | Intervention: oral care gel including hinokitiol as an active ingredient (REFRECARE H; EN Otsuka Pharmaceutical Co. Ltd, Iwate, Japan) Comparison: 0.01% CPC‐containing control gel that did not include hinokitiol Dosage: not given Duration of treatment: thrice a day for 4 weeks Duration of follow‐up: 4 weeks |
|
| Outcomes | Oral malodour: scale of 0 to 5 (0 = absence of odour; 1 = questionable odour; 2 = slight malodour; 3 = moderate malodour; 4 = strong malodour; 5 = severe malodour) VSC by gas chromatography Sites of bleeding on probing and average probing pocket depth measured at 6 points around each tooth in all subjects Plaque Index by Silness and Löe Plaque Index Tongue coating score (TCS) using a scale of 0 to 4 (0 = no tongue coating; 1 = thin tongue coating covering less than 1/3 of the tongue dorsum; 2 = thick tongue coating covering approximately 1/3 of tongue dorsum or thin tongue coating covering 1/3 to 2/3 of the tongue dorsum; 3 = thick tongue coating covering 1/3 of tongue dorsum or thin tongue coating covering more than 2/3 of tongue dorsum; 4 = thick tongue coating covering more than 2/3 of the tongue dorsum) Any adverse events reported: not mentioned |
|
| Notes | Contact: Dr Nao Suzuki, Section of General Dentistry, Department of General Dentistry, Fukuoka Dental College, 2‐15‐1 Tamura, Sawara‐ku, Fukuoka 801‐0193, Japan; naojsz@college.fdcnet.ac.jp | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The subjects were randomly assigned to 1 of 2 groups by simple randomisation using computer‐generated random numbers" |
| Allocation concealment (selection bias) | Low risk | Quote: "After being allocated randomly by a third party, the subjects and the examiner knew the kind of gel that each was using" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open label trial Quote: "After being allocated randomly by a third party, the subjects and the examiner knew the kind of gel that each was using" |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open label trial Quote: "After being allocated randomly by a third party, the subjects and the examiner knew the kind of gel that each was using" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Iwamura 2016.
| Methods | Location/setting: Aichi Gakuin University, Nagoya, Japan Number of centres: 1 Recruitment period (duration): October 2013 to September 2014 Trial design (including number of arms): parallel group, 3 arms, randomised, double‐blind pilot study Trial registration number: ISRCTN67671859 (retrospectively registered) Funding source (or sponsored drugs/materials): Grant‐in‐Aid from the Strategic Research AGU‐Platform formation (2008‐2012) and Grants‐in‐Aid for Scientific Research (C) 24593135 (JH) and 24593136 (MF) fro the Ministry of Education, Culture, Sports, Science and Technology, Tokyo, Japan |
|
| Participants | Total number before randomisation: 228 Inclusion criteria: to have visited the Aichi Gakuin University Dental Hospital and claiming oral malodour Exclusion criteria: history of antibiotic use within the past 3 months, history of otolaryngology consultation due to sinusitis, tonsillitis or tonsilloliths within past 3 months, use of gargling solution on the day of screening, periodontitis, O'Leary's Plaque Control Record score > 30%, OLT score of 0 and CH3SH in mouth air < 26 ppb Age (SD) at baseline for each arm: test: 60.7 (16.9) years; placebo: 57.9 (17.6) years; control: 64.6 (12.3) years Gender (males): test: 3; placebo: 2; control: 2 Sample size (per group): test: 10; placebo: 10; control: 9 Number randomised: 29 Method of assessing the outcome (calibration, name/company of the instrument/scale): OralChroma (Abimedical, Kawasaki, Japan) was used to measure the concentrations of VSCs (H2S, CH3SH, CH3SCH3) in mouth air Number evaluated (mention ITT or per protocol, if any): 29 Dropouts and reasons: none |
|
| Interventions | Intervention: test group: professional mechanical tooth cleaning (PMTC) + gargling with benzethonium chloride mouthwash Comparison: placebo group: PMTC + gargling with placebo mouthwash (sterile distilled water with artificial colorants) and control group: PMTC without any gargling Dosage: 10 mL of 0.004% benzethonium chloride mouthwash for 1 minute, 4 times per day (after meals and before sleeping) for 9 days Total number of intervention groups: 1 Duration of treatment: 9 days Duration of follow‐up: baseline and at day 9 |
|
| Outcomes | OLT assessment scores: recorded by 3 calibrated (Kappa 0.882) examiners using a 0 to 5 scale and if different, a mean score was used Assessment by using any equipment: OralChroma to measure VSC in mouth air and judges rated malodour on a 0 to 5 scale where 0 = absence of odour; 1 = barely noticeable odour; 2 = slight malodour; 3 = moderate malodour; 4 = strong malodour and 5 = severe malodour Any adverse events reported: none |
|
| Notes | Contact: Dr Jun‐Ichiro Hayashi, Department of Periodontology, School of Dentistry, Aichi Gakuin University, 2‐11 Suemoridori, Chikusa‐ku, Nagoya, Aichi 464‐8651, Japan; jun1row@dpc.agu.ac.jp | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated randomised numbers used |
| Allocation concealment (selection bias) | Unclear risk | Not given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded Quote: "Mouthwash prescriptions were provided and PMTC was undertaken by a single dentist who was different from those who carried out the clinical assessments" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinded Quote: "Mouthwash prescriptions were provided and PMTC was undertaken by a single dentist who was different from those who carried out the clinical assessments" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes mentioned in the trial registry were reported |
| Other bias | High risk | Baseline imbalance was statistically significant for CH3SH Pocket rate more than 4 mm was included in the trial whereas periodontitis was part of exclusion criteria |
Kara 2008.
| Methods | Location/setting: Department of Periodontology, Ataturk University, Erzurum, Turkey Number of centres: 1 Recruitment period (duration): June 2006 to March 2007 Trial design (including number of arms): 3‐arm parallel design RCT Trial registration number: not mentioned Funding source (or sponsored drugs/materials): not mentioned | |
| Participants | Total number before randomisation: not given Inclusion criteria: chronic periodontitis with 5 to 7 mm pocket depth, radiographic evidence of bone loss, complain of oral malodour Exclusion criteria: antibiotic treatment within the previous 3 months, evidence of systemic disease that may influence oral malodour, OLT rating 0 to 1, no detectable VSC, pseudo‐halitosis, halitophobia, < 3 mm probing depth, fewer than 20 natural teeth Age (SD) at baseline for each arm: Group I: 41.9 (5.09) years; Group II: 40.08 (3.91) years; Group III: 43.83 (5.27) years Gender: 37 males out of 60 Sample size (per group): 20 Number randomised: 60 Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT method; VSC using halimeter (Interscan, Chatsworth, CA, USA) Number evaluated (mention ITT or per protocol, if any): 60 Dropouts and reasons: none | |
| Interventions | Intervention: subgingival Nd:YAG laser irradiation with and without povidone‐iodine application
Comparison: SRP Dosage: 20 Hz, 100 mJ, 2 W power output Total number of intervention groups: 2. Group II: subgingival laser + povidone iodine and Group III: SRP + subgingival laser Duration of treatment: 90 seconds Duration of follow‐up: baseline, 1 week and 4 weeks for plaque, gingival indices, probing depth and clinical attachment levels. Oral malodour was measured at 3 hours, 24 hours, 1 week and 4 weeks |
|
| Outcomes | Plaque Index Gingival Index Periodontal probing depth Clinical attachment levels OLT assessment scores (0 = no appreciable malodour; 1 = barely noticeable malodour; 2 = slight but clearly noticeable malodour; 3 = moderate malodour; 4 = strong malodour and 5 = extremely strong malodour Assessment by using any equipment (halimeter, portable sulphide monitor etc.): halimeter measurements were repeated 3 times and the peak ppb values were recorded for each trial Any adverse events reported: not mentioned | |
| Notes | Contact: Dr Cankat Kara, Atatürk Üniversitesi, Diş Hekimliği Fakültesi Periodontoloji Anabilim Dalı 25240, Erzurum, Turkey; mcankat@hotmail.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers table |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Treatment allocation was carried out by the periodontist (CK) using a randomising table comprising the patient numbers (1‐60). The therapy methods were randomly allocated to one of the patients from the table" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Kozlovsky 1996.
| Methods | Location/setting: Authority for Applied Research and Development Tel Aviv University, Israel Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): RCT Trial registration number: not mentioned Funding source (or sponsored drugs/materials): grant from Ramot‐Tel Aviv AuthorityFor Applied Research and Development, Israel | |
| Participants | Total number before randomisation: 50 Inclusion criteria: not mentioned Exclusion criteria: smokers and partial denture wearers Age (SD) at baseline for each arm: 24 years Gender (% of males): 26% males Sample size (per group): intervention: 26, control: 24 Number randomised: 50 Method of assessing the outcome (calibration, name/company of the instrument/scale): sulphide monitor Model 1170, InterScan Corp, Chatsworth, and OLT measurement with 2 odour judges Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: not mentioned | |
| Interventions | Intervention: 2‐phase oil:water mouthrinse Comparison: control mouthrinse Dosage: 30 seconds, twice/day for 6 weeks Total number of intervention groups: 2 Duration of treatment: 6 weeks Duration of follow‐up: 6 weeks |
|
| Outcomes | Measurement days were day 1 (baseline prior to rinsing), and 1, 3, and 6 weeks OLT oral malodour rated on a semi‐integer scale of 0 to 5 (0 = no appreciable odour; 1 = barely noticeable odour; 2 = slight, but clearly noticeable odour; 3 = moderate odour; 4 = strong odour; 5 = extremely foul odour) VSC Oral microbial levels Any adverse events reported: not mentioned | |
| Notes | Contact: A Kozlovsky, The Maurice and Gabriela Goldschleger School of Dental Medicine, Sackler Faculty of Medicine, Tel‐Aviv University, Ramat‐Aviv, Israel | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Following randomised distribution into one of the two mouthrinse group" |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Both judges were blinded to one another's scores, as well as to the mouthrinse used by each volunteer" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropout details and reasons not mentioned |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Lee 2018.
| Methods | Location/setting: Loma Linda University, School of Dentistry, Chan Shun Pavilion CA‐92350, USA Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): RCT, 2 arms Trial registration number: not reported Funding source (or sponsored drugs/materials): not reported | |
| Participants | Total number before randomisation: 50 Inclusion criteria: informed consent, good general health, average organoleptic score of more than 2.6 but less than 4.5 on an intensity scale of 0 to 5 following 12 hours without performing oral hygiene care Exclusion criteria: xerostomia, oral piercing, oral appliances, excessive gingival recession, advanced periodontal disease, heavy deposits of calculus, fixed or removable oral appliances, mucosal inflammation, visible oral disease, unwillingness or abstain from other oral hygiene product during the study Age (SD) at baseline for each arm: placebo: 45.7 (13.9) years; test: 45.6 (13.5) years Gender (% of males): 18 male, 30 female Number randomised: 48 Method of assessing the outcome (calibration, name/company of the instrument/scale): organoleptic score (0 to 5) Number evaluated (mention ITT or per protocol, if any): 47 Dropouts and reasons: 3 dropouts. 1 of the 3 members of the test group did not complete the study |
|
| Interventions | Intervention: oral rinse containing 0.1% stabilized chlorine dioxide Comparison: placebo Dosage: twice a day with 15 ml of mouthwash for 30 seconds Total number of intervention groups: 1 Duration of treatment: 8 weeks Duration of follow‐up: weekly follow‐up for 8 weeks |
|
| Outcomes | OLT score (0 to 5) Adverse events: no adverse events were reported in both groups |
|
| Notes | Sample size calculation: not mentioned Key conclusions of the study authors: "Placebo oral rinse failed to provide statistically significant oral malodour reduction from baseline" and "Buffered stabilized chlorine dioxide counting unflavoured oral rinse provide statistically significant oral malodour reduction" Contact: Dr Sean Lee, Center for Dental Research, Loma Linda University, USA; seanlee@llu.edu | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Low risk | A study co‐ordinator who was not involved with the clinical assessment or as an odour judge, allocated the subjects to the treatment groups |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Identical bottle packaging was used for dispensing mouthwashes and the appearance and taste of intervention and placebo mouthwashes closely matched. These mouthwashes were identified using the numerical codes and concealed through out the study Quote: "The assignment of each subject to a group was not known to subjects principal investigator, and odour judges" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The assignment of each subject to a group was not known to subjects principal investigator, and odour judges" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 dropouts which was not because of the adverse events |
| Selective reporting (reporting bias) | Low risk | Conclusions matched the results |
| Other bias | Low risk | Adequate wash‐out period |
Lomax 2017.
| Methods | Location/setting: specialized research centre, Delhi, India Number of centres: 1 Recruitment period (duration): November 2013 to January 2014 Trial design (including number of arms): 2 Trial registration number: not reported Funding source (or sponsored drugs/materials): GSK Consumer Healthcare |
|
| Participants | Total number before randomisation: 198 Inclusion criteria: at least 18 years of age and had a total score of at least 7 on a 'Subject's level of understanding' questionnaire, in good general and mental health, with no clinically significant or relevant abnormalities, with at least 20 gradable teeth, with mild‐to‐moderate gingivitis, a positive response to bleeding on brushing (at screening) and at least 20 bleeding sites (at baseline) Exclusion criteria: intolerance or hypersensitivity to the study materials or stated ingredients, currently active dental caries, more than 3 pockets with 5 mm or over, excessive calculus, other severe oral/gingival conditions, medical conditions which may influence gingival bleeding, restorations in a poor state of repair or orthodontic appliances Age (SD) at baseline for each arm: test: 27.7 (7.69) years; control 28.6 (10.34) years Gender (% of males): test: 27 (36.5 %); control: 37 (50%) Sample size (per group): 74 Number randomised: 148 Method of assessing the outcome: gas chromatography with flame photometric detection (FPD) Number evaluated: 66 + 69 Dropouts and reasons: 13. Test: 7 (lost to follow‐up) + 1 discontinued intervention (did not meet study criteria); control: 5 (lost to follow‐up) |
|
| Interventions | Intervention: parodontax Comparison: experimental non‐sodium bicarbonate, silica sodium fluoride toothpaste, not commercially available (control group) Dosage: twice daily for 6 weeks Total number of intervention groups: 1 Duration of treatment: 6 weeks Duration of follow‐up: not reported |
|
| Outcomes | Outcomes assessed using gas chromatography with flame photometric detection (FPD) Any adverse events reported: "A total of four subjects, two from each treatment group, reported four treatment‐emergent adverse events. One of the four AEs was an oral AE (pharyngitis, in the test group); the other three AEs were non‐oral (headache, one in the test group and two in the control group). None of the four treatment‐emergent AEs were treatment related" |
|
| Notes | Contact: Shiva Patel, GSK Consumer Healthcare, St Georges Avenue, Weybridge, Surrey KT13 0DE, UK; Shiva.8.patel@gsk.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation was achieved using randomisation numbers assigned in ascending numerical order according to a schedule provided by the study sponsor |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "supplied in commercial packaging with a study label affixed to the tube (described hereafter as 'test group'), or an experimental non‐sodium bicarbonate, silica sodium fluoride toothpaste, not commercially available (control group)" Quote: "The study statistician, data management staff and other employees of the sponsor were blinded to treatment, as was the examiner" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The study statistician, data management staff and other employees of the sponsor were blinded to treatment, as was the examiner" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts were due to loss of follow‐up and 1 participant from intervention group was excluded due to the discontinuation of the intervention |
| Selective reporting (reporting bias) | Low risk | None |
| Other bias | Low risk | None |
López Jornet 2003.
| Methods | Location/setting: Dental Clinic at Murcia University, Spain Number of centres: 1 Recruitment period (duration): not reported Trial design (including number of arms): RCT, 4 arms Trial registration number: not reported Funding source (or sponsored drugs/materials): not reported | |
| Participants | Total number before randomisation: 40 participants Inclusion criteria: age ≥18 years; having clinical halitosis and having signed informed consent Exclusion criteria: people treated with antibiotics 1 month before the study; people who had used mouthwash Age (SD) at baseline for each arm: not reported; total cohort: mean age 33.70 years, SD 11.0, age range 21 to 55 years Gender (% of males): total cohort: 48.6% males; 51.4% females Sample size (per group): 10 Number randomised: 40 Method of assessing the outcome (calibration, name/company of the instrument/scale): halimeter and OLT method Number evaluated (mention ITT or per protocol, if any): not reported Dropouts and reasons: 3 people did not complete the study – no group or reasons reported | |
| Interventions | Intervention: 4 groups
Comparison: each other Dosage: 10 ml of mouthwash/ 2 times per day. In addition, all participants were instructed not to use other oral hygiene products or tongue scrapers Total number of intervention groups: 4 Duration of treatment: 3 weeks Duration of follow‐up: 4 weeks |
|
| Outcomes | Halimeter OLT method Any adverse events reported: not mentioned |
|
| Notes | Contact: P López Jornet, Clínica Odontológica Universitaria, Medicina Bucal, Hospital Morales Meseguer, Avd Marques de los Velez s/n, Murcia 3008, Spain; majornet@um.es | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The mouthwash was coded by a person external to the investigation team, using identical bottles. Both the participants and the researchers were blinded to the condition (page 277, "productos evaluados" section) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Results not available for 3 participants. Unclear which group. Reasons not reported |
| Selective reporting (reporting bias) | Unclear risk | Halitosis was measured in 2 ways.1st, using an Halimeter® (results reported in Fig 2 and extracted in this form). 2nd, using clinician's judgement using a 0 to 10 scale. These results are not reported in the paper. Unclear if this would have shown different results (probably this is a more subjective measure). Data reported in a graph, with no SD. Differences between groups reported with P value only. Adverse events not mentioned |
| Other bias | Low risk | None |
Mamgain 2016.
| Methods | Location/setting: Department of Ayurveda, Himalayan Institute of Medical Sciences, Swami Rama Himayalan University, Dehradun, Uttarakhand, India Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): 2 Trial registration number: not reported Funding source (or sponsored drugs/materials): nil |
|
| Participants | Total number before randomisation: 60 Inclusion criteria: age >18 years, systemically healthy, plaque‐induced gingivitis, halitosis Exclusion criteria: mouthwash use in past 3 months, antibiotic therapy in past 3 months, orthodontic and prosthetic appliances use, systemic disorders like diabetes mellitus, renal failure, and so on, pregnancy, smoking Age (SD) at baseline for each arm: not reported Gender (% of males): not reported Sample size (per group): 30 Number randomised: 60 Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT scoring scale Number evaluated (mention ITT or per protocol, if any): 60 Dropouts and reasons: not reported |
|
| Interventions | Intervention: Ela churna was mixed in 100 mL of Triphala Comparison: chlorhexidine mouthwash for 21 days twice daily after cleaning the oral cavity with water Dosage: not reported Duration of treatment: 21 days Duration of follow‐up: not reported |
|
| Outcomes | OLT scores Any adverse events reported: not mentioned |
|
| Notes | Contact: Abhishek Kandwal, MDS(Periodontology), 262, Bank Colony, Ajabpurkalan, Dehradun 248001, Uttarakhand, India; way2drabhi@gmail.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote:"2 groups of 30 each by random computer allocation" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding, though not reported, the taste of the intervention mouthwash will be different from that of the control mouthwash and can be affecting the blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropout details not mentioned |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Marchetti 2015.
| Methods | Location/setting: Research Centre for the Diagnosis and Treatment of Halitosis, University of L'Aquila, L'Aquila, Italy Number of centres: 1 Recruitment period (duration): January 2014 to June 2014 Trial design (including number of arms): 2 arms Trial registration number: not reported Funding source (or sponsored drugs/materials): company CD Investment provided the supply of products for tests, and Vito Trinchieri |
|
| Participants | Total number before randomisation: 32 Inclusion criteria: adult age (> 18 years of age); halitosis in active phase; informed consent by the patient Exclusion criteria: need to take antibiotics for the presence of signs and/or symptoms of infection; use of non‐steroidal anti‐inflammatory drugs during the 30 days prior to the beginning of the study; use of steroid medications during the 30 days prior to the beginning of the study; dental care in progress; current gingivitis and periodontitis; systemic diseases such as: chronic liver disease, chronic renal failure, gastro‐oesophageal reflux; alcoholism and/or drug addiction Age (SD) at baseline for each arm: test: 33 (9) years; placebo: 36 (7) years Gender: 12 + 11(no other details given) Sample size (per group): 10 Number randomised: 20 Method of assessing the outcome (calibration, name/company of the instrument/scale): Rosenberg OLT score and WTCI (tongue coating anterior and posterior); OralChroma™ gas chromatography; BIONOTE® (test analysis) (breath print) Number evaluated (mention ITT or per protocol, if any): 20 Dropouts and reasons: none |
|
| Interventions | Intervention: Lactobacillus brevis CD2‐containing lozenges Comparison: matching placebo Dosage: 4 tablets/day for 14 days Total number of intervention groups: 2 Duration of treatment: 14 days Duration of follow‐up: not reported |
|
| Outcomes | OLT assessment scores: the Rosenberg score, the scale includes the following values: 0 = no odour; 1 = doubtful presence of halitosis; 2 = slight odour but clearly notifiable; 3 = moderate halitosis; 4 = strong halitosis; 5 = very intense halitosis VSC levels: OralChroma gas chromatography, the levels (measured in ppm) are reported in a diagram from low to high level, a cognitive threshold is individuated and levels are individuated as 'more than' or 'less than' the cognitive threshold; BIONOTE, individual breath print (BP) of a patient is represented with a radar plot, equiangular radii shape each radar plot, where each radius represents one of the 28 sensor responses. The radius length gives magnitude of each sensor response (expressed in Hz, because relative to a resonant frequency shoft of the quartz slice). The radar plot 'profile' consists of a line drawn connecting the data values for each radius Adverse effects: no adverse effects were registered |
|
| Notes | Contact: enrico.marchetti@cc.univaq.it | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computerized random numbers were used" |
| Allocation concealment (selection bias) | Low risk | Quote: "The allocation of treatment or placebo group was undertaken by a person not directly involved in the research project" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Lactobacillus brevis (CD2)–containing lozenges and matched placebo were in lozenge form and had identical appearance. They were pre‐packed in boxes, each containing 20 tablets, with the same look and the same weight, so it was impossible to distinguish them a priori. The packages were consecutively numbered according to the randomisation schedule" Quote: "The operator assessing outcomes and data collectors were blinded to the allocation of subjects" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The operator assessing outcomes and data collectors were blinded to the allocation of subjects" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Low risk | None |
| Other bias | Low risk | None |
Nakano 2017.
| Methods | Location/setting: Department of Special Needs Dentistry, Division of Hygiene and Oral Health, Showa University School of Dentistry, Tokyo, Japan Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): RCT, 2 arms Trial registration number: UMIN clinical trial registration system (ID: UMIN000015706) Funding source (or sponsored drugs/materials): research grants from Morinaga Milk Industry | |
| Participants | Total number before randomisation: 47 Inclusion criteria: adults aged 65 years and older with tongue coating Exclusion criteria: eating pureed and finely‐chopped meals; receiving parenteral nutrition; receiving treatment for dental disease (except adjustment of dentures, oral hygiene instructions); history of allergy to milk; received antibiotic treatment in the past 1 month, or expected to receive it in the near future; use of oral care products for prevention of oral malodour or improvement of oral hygiene; regular consumption of LF or LPO‐containing food or oral care products; and presence of exacerbating diseases of the liver, kidney, heart, lung, gastro‐intestine, blood, endocrine system, and metabolic system Age (SD) at baseline for each arm: placebo: 85.9 (6.7) years; test: 80.4 (6.4) years Gender (% of males): 12/37 Sample size (per group): 22 (placebo) and 24 (test) Number randomised: 46 Method of assessing the outcome (calibration, name/company of the instrument/scale): concentrations of VSCs in oral air were analysed with a portable gas chromatography device (OralChroma; FIS, Itami, Japan) according to the manufacturer's instructions Number evaluated (mention ITT or per protocol, if any): 37 Dropouts and reasons: 1 of the members of the test group did not complete the study; 5 participants in the placebo group and 3 in the test group failed to comply with the suggested intake rate | |
| Interventions | Type of intervention: Lactobacillus β LPO tablets
Comparison: placebo Dosage: test tablets contained 80 mg of LFβ LPO powder (Orabarrier; Morinaga Milk Industry, Tokyo, Japan) including the active ingredients of 20 mg of LF, 2.6 mg of LPO and 2.6 mg of glucose oxidase Total number of intervention groups: 1 Duration of treatment: 8 weeks Duration of follow‐up: not mentioned |
|
| Outcomes | VSC using portable gas chromatography device (OralChroma) Adverse events: no adverse events were reported in both groups |
|
| Notes | Sample size calculation: not mentioned Key conclusions of the study authors: "Results suggest that LF and LPO‐containing tablets promote a shift from a highly diverse and gram‐negative‐dominated to a gram‐positive‐dominated community in the microbiota of supragingival plaque and tongue coating. This microbial shift may contribute to improvements in oral health, including oral malodour and state of the gingiva" Contact: authors contacted on 25 April requesting the results for the halitosis outcome. Awaiting reply. Manabu Nakano, Food Ingredients & Technology Institute, Morinaga Milk Industry, 5‐1‐83 Higashihara, Zama, Kanagawa 252‐8583, Japan; m‐nakano@morinagamilk.co.jp | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind, all involved were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding details not given. However, the method of outcome assessment was objective (OralChroma) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 dropout from intervention group 5 from placebo group and 3 from intervention group were not included in the analysis as they failed to comply with the suggested intake of medications. Per‐protocol analysis was done |
| Selective reporting (reporting bias) | Low risk | All outcomes are reported adequately and the conclusions match the results |
| Other bias | Low risk | None |
Navada 2008.
| Methods | Location/setting: Unilever Oral Care, Mumbai, India and Unilever Shanghai, Shanghai, China Number of centres: 2 Recruitment period (duration): 4 weeks Trial design (including number of arms): randomised, 2‐cell parallel, double‐blind, placebo‐controlled Trial registration number: not mentioned Funding source (or sponsored drugs/materials): Unilever Oral Care |
|
| Participants | Total number before randomisation: 190 Inclusion criteria: halimeter study: males and females, 18 to 45 years, VSC between 120 and 250 ppb, a minimum of 24 teeth, at least 20 teeth free from caries or periodontal disease; OLT study: males and females, 18 to 45 years, OLT score of 3 or greater, a minimum of 24 teeth, at least 20 teeth free from caries or periodontal disease Exclusion criteria: not mentioned Age (SD) at baseline for each arm: 18 to 45 years Gender (% of males): not mentioned Sample size (per group): halimeter: 95 per group, OLT group: 95 per group Number randomised: 190 Method of assessing the outcome (calibration, name/company of the instrument/scale): Interscan Halimeter Model RH‐17K (Interscan Corp, Chatsworth, CA, USA) – average of 3 readings; OLT score – average score of calibrated judges Number evaluated (mention ITT or per protocol, if any): halimeter: 94, OLT: 92 Dropouts and reasons: halimeter: 2 dropouts with reasons unconnected to the use of toothpaste; OLT: 3 dropouts with reasons unconnected to the use of toothpaste |
|
| Interventions | Intervention: silica gel toothpaste with 1000 ppm fluoride and 0.2% zinc sulphate Comparison: placebo: silica gel toothpaste with 1000 ppm fluoride without zinc Dosage: 1 brush length to be used to brush for 2 minutes Total number of intervention groups: 2 – assessed by different methods but using same intervention Duration of treatment: 4 weeks Duration of follow‐up: baseline, 2 hours after brushing on day 1 and at end of 4 weeks |
|
| Outcomes | OLT assessment scores: 0 = no odour present, 5 = extremely foul odour low score is better Assessment by Interscan Halimeter Model RH‐17K (Interscan Corp, Chatsworth, CA, USA) – average of 3 readings Any adverse events reported: not mentioned |
|
| Notes | Contact: Rekha Navada; Rekha.Navada@Unilever.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinding done |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinding done Halimeter – average of 3 readings, OLT ‐ average reading of all judges |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 to 3 dropouts in a group of 95 |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
NCT02628938.
| Methods | Location/setting: Riyadh Colleges of Dentistry and Pharmacy, Riyadh, Saudi Arabia Number of centres: 1 Recruitment period (duration): March 2014 to December 2014 Trial design (including number of arms): 3 Other trial registration number: FUGRP/2013/114 Funding source (or sponsored drugs/materials): Riyadh Colleges of Dentistry and Pharmacy |
|
| Participants | Number before randomisation: 212 Inclusion criteria: participants should report that they suffered from bad oral malodour, OLT score of 2 or above Exclusion criteria: smoking, current systemic diseases or medical treatment, active caries or any faulty restorations, acute sinusitis or oropharyngeal infection, chronic periodontitis, pregnancy, breastfeeding, eating very spicy food, use of antibiotic during the last 2 months before the start of the study Age (SD) at baseline for each arm: 18 to 35 years Gender (% of males): only females Sample size (per group): 15 per group Number randomised: 45 Number evaluated (mention ITT or per protocol, if any): per‐protocol evaluation done Dropouts and reasons: 11 dropouts (5 from miswak mouthwash group, 2 from miswak stick group and 4 from chlorhexidine group) |
|
| Interventions | Intervention:
Comparison: 5 ml of 0.2% chlorhexidine gluconate mouthwash Oraxine® twice a day for 7 days Total number of intervention groups: 2 Duration of treatment: 7 days Duration of follow‐up: after the 1st use of the prescribed method by 15 minutes, and after 7 days of use |
|
| Outcomes | OLT scores (0 to 5 scores): 0 = no odour present, 1 = barely noticeable odour, 2 = slight but clearly noticeable odour, 3 = moderate odour, 4 = strong offensive odour and 5 = extremely foul odour VSC scores using breath checker device (Tanita FitScan HC‐212SF Breath Checker): 0 = no odour, 1 = slight odour, 2 = moderate odour, 3 = heavy odour, 4 = strong odour, 5 = intense odour Change from baseline self‐assessment of mouth odour after 7 days of use: scores were collected twice, before the use of the prescribed method (baseline scores) and after 7 days of use Participants were asked to score their own halitosis on a continuous 10 cm VAS that is marked as no odour on the 0 cm end, and as extremely foul odour on the 10 cm end Adverse events: not mentioned |
|
| Notes | Contact: Mohammad Ramadan Rayyan, Riyadh Colleges of Dentistry and Pharmacy | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Single‐blind (outcome assessor) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Substantial number of participants dropped out which could have affected the overall results |
| Selective reporting (reporting bias) | Low risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Niles 1999.
| Methods | Location/setting: Colgate‐Palmolive Technology Center, Piscataway, New Jersey, USA Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): double‐blind, stratified, 2‐treatment cross‐over design with 2 arms Trial registration number: not mentioned Funding source (or sponsored drugs/materials): not mentioned |
|
| Participants | Total number before randomisation: not given Inclusion criteria: 21 to 55 years, good general health, no history of allergy or idiosyncrasies to dentifrice ingredients, available for duration of study, sign informed consent form, unpleasant breath at pre‐treatment evaluation (high levels of VSC in morning mouth air – 10 ng/ml or higher) Exclusion criteria: orthodontic appliances, tumours of hard and soft oral tissues, moderate or advanced periodontal disease, 5 or more carious lesions, use of tobacco in any form, partial or full upper or lower dentures, received antibiotic or antihistamine therapy during the 2 weeks prior to entry into study Age (SD) at baseline for each arm: 21 to 55 years Gender (% of males): not mentioned Sample size (per group): not mentioned, cross‐over design Number randomised: 20 Method of assessing the outcome (calibration, name/company of the instrument/scale): 565 Tracor gas chromatograph with a flame photometric detector. 4'6" Teflon (FEP) BHT‐100 Supelco column was used to specifically separate the primary sulphur components. Standard methyl mercaptan gas permeation tube was used to convert resulting measurements into nanograms per millilitre (ng/ml) Number evaluated (mention ITT or per protocol, if any): 19 overnight, 20 7 hours after intervention Dropouts and reasons: overnight measurements – 19 due to scheduling difficulty |
|
| Interventions | Intervention: dentifrice containing 0.3% triclosan and 2.0% PVM/MA polyvinyl methyl ether/maleic acid copolymer in a 0.243% sodium fluoride/silica base (Colgate Total Toothpaste) Comparison: placebo dentifrice containing 0.243% sodium fluoride in a silica base Dosage: not mentioned Total number of intervention groups: 20 subjects cross‐over design Duration of treatment: intervention: 1 to 7 days; wash‐out: 7 days; placebo: 7 days Duration of follow‐up: overnight measurement on 8th day, 7 hours post‐intervention |
|
| Outcomes | Assessment by using 565 Tracor gas chromatograph with a flame photometric detector Any adverse events reported: not mentioned |
|
| Notes | Contact: Ms Hollandra P Niles, Colgate Palmolive Technology Center, Piscataway, NJ, USA; Holly_Niles@Colpal.com | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind Quote: "Dentifrices were packaged in tubes with plain white over wrapping" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind 565 Tracor gas chromatograph used ‐ objective measurement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Only 1 subject's overnight reading not measured |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | No evidence of any other bias |
Nishihira 2017.
| Methods | Location/setting: Department of Medical Management and Informatics, Hokkaido Information University, Hokkaido, Japan Number of centres: 1 Recruitment period (duration): 23 June 2014 to 14 August 2014 Trial design (including number of arms): 4 Trial registration number: UMIN Clinical Trial Registration System (certificate number UMIN000014256) Funding source (or sponsored drugs/materials): COSMO BIO Co Ltd, Japan and Hokkaido Information University |
|
| Participants | Total number before randomisation: 80 Inclusion criteria: subjects who are aged between 50 to 80 years and are worried about fecal odour, body odour or oral odour, a subject with an observer, for objectively evaluating above odours Exclusion criteria: subjects who are suffering from serious cerebrovascular disease, heart disease, liver disease, renal disease, gastrointestinal disease or any infectious disease which needs immediate reporting; with a clinical history of gastrointestinal cancer or are currently under its medical treatment; having a clinical history of gastrectomy, gastrointestinal suture, bowel resection or any major surgery in the digestive system.; having a gastrointestinal disorder, irritable bowel syndrome, inflammatory bowel syndrome, etc.; under the medication for bowel movements (such as antibiotics, laxatives, medicine for constipation) or using functional foods and supplements (containing lactic acid bacteria, Bifidobacterium, oligosaccharides, dietary fibre, etc.); subjects who will undergo dental treatment during this study period; with frequent complaints of post‐menopausal symptoms; with unusually high and/or low blood pressure, or with abnormal haematological data; with serious anaemia; with a history of allergy to medicine and food (especially mushroom); who have defecation frequency less than 4 times per week or those who suffer from diarrhoea; heavy smokers or alcoholics, or exhibit irregular pattern in their lifestyles such as meals or sleep, etc.; who has donated 400 ml whole blood within past 12 weeks or 200 ml within past 4 weeks or who has donated plasma or platelets within past 2 weeks prior to this study; pregnant or under lactation, or who expect to get pregnant during this study period; who has participated in other clinical trials within past month or currently undergoing any clinical trial; judged ineligible by our physician Age (Std Dev) at baseline for each arm: not given Gender (% of males): placebo: 9 males; 50 mg: 9 males; 500 mg: 11 males; 1000 mg: 9 males Sample size (per group): placebo 19; 50 mg 18; 500 mg 20; 1000 mg 20 Number randomised: 80 Method of assessing the outcome (calibration, name/company of the instrument/scale): VAS Number evaluated (mention ITT or per protocol, if any): 77 Dropouts and reasons: 3 (personal reason) before the trial started |
|
| Interventions | Intervention: 50 mg/day, 500 mg/day and 1000 mg/day champignon extract Comparison: placebo tablets: 2 grams of powder containing dextrin, ingested daily over a period of 4 weeks Dosage: 2 grams of powder containing 50, 500 and 1000 mg of champignon ingested daily for 4 weeks Total number of intervention groups: 3 Duration of treatment: 4 weeks Duration of follow‐up: 2 and 4 weeks |
|
| Outcomes | Self‐assessment scores: for VAS questionnaire, 100 mm lines were prepared for each item with the left and right edges indicating worst and best states, respectively Any adverse events reported: no severe adverse events or side effects were noted during the study period |
|
| Notes | Contact: Jun Nishihira, Hokkaido Information University, Department of Medical Management and Informatics, 59‐2, Nishi‐nopporo, Ebetsu, 069‐8585, Hokkaido, Japan; nishihira@do‐johodai.ac.jp | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "....equally divided the subjects via stratified randomisation into four groups considering age composition, male‐to‐female ratio, and odour questionnaire scores" |
| Allocation concealment (selection bias) | Low risk | Quote: "The allocation manager carefully stored the allocation‐related documents containing personal information of the subjects in a locked cabinet. Subjects were then notified of the date, time, and place for the clinical trial" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double‐blind method was used, however no details available |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Double‐blind method was used, however no details available |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 dropouts before the trial started |
| Selective reporting (reporting bias) | High risk | Trial registration (UMIN000014256) shows 1 arm with 200 mg of champignon which is not reported in the report. It is not clear if this arm was initiated or not as the trial registry shows the number randomised as 80 only |
| Other bias | Unclear risk | This is a pragmatic trial and the participants did not fulfil the exclusion criteria. We are not sure if this could have influenced the study results |
Nogueira‐Filho 2002.
| Methods | Location/setting: Faculty of Dentistry of Piracicaba, University of Campinas, Piracicaba, Sao Paulo, Brazil Number of centres: 1 Recruitment period (duration): not reported Trial design (including number of arms): 5 arms, cross‐over trial Trial registration number: not reported Funding source (or sponsored drugs/materials): no details given |
|
| Participants | Total number before randomisation: 19 Inclusion criteria: all subjects had at least 20 natural teeth and 4 experimental posterior teeth in the lower left quadrant Exclusion criteria: subjects with medical disorders, periodontal disease, undergoing antibiotic or other antimicrobial therapy, smokers, pregnant women, and those presenting, on pre‐study clinical screening, a probing depth of > 3 mm associated with any of the 4 experimental mandibular teeth Age (SD) at baseline for each arm: aged 19 to 28 years Gender (% of males): 5 Sample size (per group): 19 Number randomised: 19 (cross‐over) Method of assessing the outcome (calibration, name/company of the instrument/scale): portable industrial sulphide monitor (Halimeter A, Interscan Corp, Chatsworth, California, USA) Number evaluated (mention ITT or per protocol, if any): 19 in each group Dropouts and reasons: none |
|
| Interventions | Intervention: 3 commercial dentifrices containing triclosan:
Comparison: as a negative control, a dentifrice without antiplaque agents (SorrisoA) was used Total number of intervention groups: 5 Duration of treatment: "comparison of five crossover groups performed in five experimental periods of 21days each" Duration of follow‐up: "Each period was followed by a 30‐day washout interval" |
|
| Outcomes | VSC levels Adverse effects: not mentioned |
|
| Notes | Contact: Jaime . Cury, Faculty of Dentistry of Piracicaba, UNICAMP, Av. Limeira 901, 13414–903 Piracicaba, SP, Brazil; jcury/fop.unicamp.br | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details of randomisation given |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "repackaged in plain white tubes to ensure double blindness of the study" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details of assessor blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Nohno 2012.
| Methods | Location/setting: Division of Preventive Dentistry, Graduate School of Medical and Dental Sciences, Niigata University, 2‐5274, Gakko‐Cho, Cho‐ku, Niigata City, Niigata, Japan Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): double‐blind, randomised, cross‐over trial Trial registration number: not reported Funding source (or sponsored drugs/materials): not mentioned |
|
| Participants | Total number before randomisation: 14 Inclusion criteria: whom over the threshold VSC concentration had been detected from their mouth air at baseline; they were aged 23 to 54 years Exclusion criteria: antibiotics 3 weeks before the study initiation or were of poor periodontal health were excluded from the study Age (SD) at baseline for each arm: aged 23 to 54 years Gender (% of males): 14 (100%) Sample size (per group): 14 Number randomised: 14 Method of assessing the outcome (calibration, name/company of the instrument/scale): portable gas chromatograph (OralChroma, Abimedical, Japan) Number evaluated (mention ITT or per protocol, if any): 14 Dropouts and reasons: none |
|
| Interventions | Intervention: actinidine tablet Comparison: placebo Dosage: test or placebo tablets (2.0 g) 3 times (at 11:00, 17:00 and 23:00) a day until the 6th day after starting Total number of intervention groups: 1 Duration of treatment: 7 days Duration of follow‐up: 7 (intervention ‐ test) + 14 (wash‐out) + 7 (intervention ‐ placebo) |
|
| Outcomes | Level of VSC Adverse effects: no details given |
|
| Notes | Sample size calculation: not mentioned Key conclusions of the study authors: "Tablets containing actinidine had an accumulative effect in reducing VSC in mouth air with long‐term use" Contact: K Nohno, Division of Preventive Dentistry, Graduate School of Medical and Dental Sciences, Niigata University, 2‐5274, Gakko‐Cho, Cho‐ku, Niigata City, Niigata, Japan; no2@dent.niigata‐u.ac.jp |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | High risk | Quote: "although we might have adopted a wrong protocol for deciding the time of the measurements" |
Patil 2017.
| Methods | Location/setting: MCODS, Manipal, India Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): randomised, parallel‐group trial Trial registration number: CTRI/2012/05/002695 Funding source (or sponsored drugs/materials): Alarsin Pharmaceuticals, Alarsin House, A/32 Street no 3 MIDC Andheri 400093, India | |
| Participants | Total number before randomisation: 40 Inclusion criteria: periodontal pockets ≤ 4 mm, subjects with VSC and hydrocarbon gas levels more than 3 Exclusion criteria: smokers, undergoing antibiotic or other antimicrobial therapy, medically compromised conditions contraindicating the oral examination, active periodontitis and multiple carious lesions, systemic disease pertaining to renal system Age (SD) at baseline for each arm: 17 to 35 years Gender (% of males): 50% males Sample size (per group): 20 Number randomised: 40 Method of assessing the outcome (calibration, name/company of the instrument/scale): Breath Alert (Tanita®) Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: no losses to follow‐up observed during the study period | |
| Interventions | Intervention: G32 experimental drug (commercially available ayurvedic formulation)
Comparison: chlorhexidine – digluconate 1% (Hexigel, ICPA company; gold standard for treating halitosis) Dosage: subjects of G32 group were advised to crush 2 to 3 tablets and massage it on the gums and surrounding areas twice a day for 5 minutes, once in the morning and once before going to bed at night followed by rinsing the mouth with water. Subjects of CHX group (control group) were advised to use the gel twice daily and massage the gums and surrounding areas for 5 minutes, once in the morning and once before going to bed at night followed by rinsing the mouth with water Total number of intervention groups: 2 Duration of treatment: 1 week Duration of follow‐up: 1 week |
|
| Outcomes | Oral malodour using Breath Alert (1 = no odour, 2 = mild odour, 3 = moderate odour, 4 = strong odour) Reduction of the gingival and plaque scores using Löe H and Silness J index (1963) and plaque with Silness J and Löe H index (1964) Tongue coating was measured using Winkel tongue coating index Any adverse events reported: burning mucosa and drying of mouth in chlorhexidine group were reported by few subjects and none in G32 group | |
| Notes | Contact: Snehal Patil, Dental Section, Dr TMA Pai Hospital, Opposite Taluk office, Udupi, Karnataka, India; snehal_2086@yahoo.com Mail sent to study authors on 27 June 2019 for missing data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "the participants were provided at random (coin flip method) with G32" |
| Allocation concealment (selection bias) | Low risk | Quote: "Sequentially numbered, sealed, opaque envelopes, allocation of subjects to either of the groups was done by a person not related to the researchers or subjects" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote from published trial: "Single blind randomised controlled trial" Quote from the trial registry: "Participant and Investigator Blinded" |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Single blind randomised controlled trial" Quote from trial registry: "Participant and Investigator Blinded" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "No loss to follow up observed during the study period" |
| Selective reporting (reporting bias) | Unclear risk | Missing data |
| Other bias | Unclear risk | Retrospective trial registration |
Payne 2011.
| Methods | Location/setting: Intertek 4‐Front Research, Ellesmere Port, UK Number of centres: 1 Recruitment period (duration): August to November 2010 Trial design (including number of arms): randomised, cross‐over clinical trial Trial registration number: not reported Funding source (or sponsored drugs/materials): funded by Glaxo Smith Kline Consumer Healthcare |
|
| Participants | Total number before randomisation: 89 Inclusion criteria: at least 18 years old and in good general health, good oral health with at least 20 natural uncrowned teeth, with a reproducible level of hydrogen sulphide (> 300 ppb by GC analysis) on at least 3 separate occasions Exclusion criteria: pregnant or breastfeeding; had diabetes mellitus, evidence or recent history of bronchitis, tonsillitis or sinusitis, a significant autoimmune or infectious disease, such as hepatitis, tuberculosis, HIV positive or AIDS, any infectious disease, respiratory infection, oesophageal reflux, colds, flu, sore throat or any condition which could be transmitted in saliva or salivary aerosols, or severe xerostomia; had known or suspected intolerance or hypersensitivity to oral care products, orthodontic or prosthetic appliances, including dental implants; had undergone dental professional cleaning within 3 weeks prior to the screening visit; had used chlorhexidine containing mouthwashes, used ColgateTotal within 7 days prior to treatment, or had used antibiotics within 14 days prior to treatment Age (SD) at baseline for each arm: 46.3 (12.21) years for whole sample Gender (% of males): 18 (23.1%) Sample size (per group): 78 (cross‐over) Number randomised: 78 (cross‐over) Method of assessing the outcome (calibration, name/company of the instrument/scale): gas chromatography with flame photometric detection (FPD) Number evaluated (mention ITT or per protocol, if any): 78 (ITT analysis done) Dropouts and reasons: 10 of the randomised subjects did not complete the study; 1 was due to an adverse event, 1 to protocol violation and the remaining 8 for 'other' reasons |
|
| Interventions | Intervention: 0.1% w/w o‐cymen‐5‐ol / 0.6% w/w zinc chloride / sodium fluoride dentifrice Comparison: sodium fluoride control dentifrice Dosage: twice daily for 1 week Total number of intervention groups: 1 Duration of treatment: 1 week Duration of follow‐up: 1 week test intervention + 7 to 21 days wash‐out period + 1 week control |
|
| Outcomes | Gas chromatography with flame photometric detection (FPD) Any adverse events reported: "There were a total of 31 treatment‐emergent AEs reported for 26 subjects, 19 non‐oral and 12 oral. One oral AE (tingling of lips) was associated with the test dentifrice while two other oral AEs (dry mouth and sore gums) were associated with the reference dentifrice. All of the oral AEs were mild in nature. There were no serious adverse events" |
|
| Notes | Sample size calculation: a sample size of 70 subjects was calculated for 80% power. To allow for withdrawals from the study approximately 85 subjects were randomised Key conclusions of the study authors: "The results of the present clinical study demonstrated that the use of the 0.1% o‐cymen‐5‐ol /0.6% zinc chloride dentifrice over a one week period provided a statistically significant benefit in controlling oral malodour up to 12 hours post‐treatment compared to a sodium fluoride control dentifrice" Contact: Jenny J Gordon, GlaxoSmithKline Consumer Healthcare, St George's Avenue, Weybridge, Surrey, KT130DE, UK; Jenny.J.Gordon@gsk.com |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computerised randomisation generator was used" |
| Allocation concealment (selection bias) | High risk | Quote: "Randomisation numbers were assigned chronologically as subjects were randomised to treatment" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "The study treatments were both white dentifrices provided in plain white tubes with study label detailing the treatment codes and instructions for use to ensure the subject was blinded to the treatment identity" Quote: "The study staff who dispensed the treatment were provided with a randomisation schedule that did not contain the treatment identities" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Ten of the randomised subjects did not complete the study; one was due to an adverse event, one to protocol violation and the remaining eight for 'other' reasons" Comment: authors have not given an explanation for 'other reasons' |
| Selective reporting (reporting bias) | Low risk | None |
| Other bias | Low risk | None |
Rassameemasmaung 2007.
| Methods | Location/setting: Mahidol University, Thailand Number of centres: 1 Recruitment period (duration): 15 days + 4 weeks wash‐out + 15 days (recurrence after scaling) = 2 months Trial design (including number of arms): randomised, double‐blind, placebo‐controlled clinical trial, 2 arms Trial registration number: not mentioned Funding source (or sponsored drugs/materials): Mahidol University research grant (2002) |
|
| Participants | Total number before randomisation: 60 Inclusion criteria: at least 20 teeth, mild to moderate gingivitis, gingival index of each tooth 1 to 2 according to Loe and Silness, 80 ppb of VSC in morning breath Exclusion criteria: smokers, denture wearers, systemic complicating factors, oral pathology, antibiotic treatment within 1 month prior to study Age (SD) at baseline for each arm: 17 to 37 years (26.15 ± 6.25 years) Gender (% of males): 20% (48 females, 12 males) Sample size (per group): 30 Number randomised: 60 Method of assessing the outcome (calibration, name/company of the instrument/scale): sulphide monitor – halimeter model RH‐17 (Interscan Corp, Chatsworth, CA, USA) Number evaluated (mention ITT or per protocol, if any): 60 Dropouts and reasons: none |
|
| Interventions | Intervention:
Comparison: placebo mouthwash (details not given) Dosage: 15 ml to be swished for 1 minute, twice a day after toothbrushing Total number of intervention groups: 1 Duration of treatment: 15 days + 4 weeks + 15 days Duration of follow‐up: baseline at 8 am, 30 minutes and 3 hours on day 1 and day 15 of intervention |
|
| Outcomes | Assessment by using sulphide monitor – halimeter model RH‐17, Interscan Corp, Chatsworth, CA, USA Periodontally‐related parameters ‐ Plaque Index (PI) Silness and Loe, Papillary Bleeding Index (PBI) Any adverse events reported: none |
|
| Notes | Contact: Dr Supanee Rassameemasmaung, Department of Oral Medicine, Faculty of Dentistry, Mahidol University, 6 Yothi Road, Rachathewi, Bangkok 10400, Thailand; dlsrs@mahidol.ac.th | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind Objective measurements (halimeter) and average of 3 measurements taken |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Low risk | Outcomes all objectives reported |
| Other bias | Low risk | No other bias evident |
Rassameemasmaung 2012.
| Methods | Location/setting: Mahidol University, Thailand Number of centres: 1 Recruitment period (duration): 28 days Trial design (including number of arms): double‐blind, placebo‐controlled clinical trial Trial registration number: ClinialTrials.gov (NCT00932347) Funding source (or sponsored drugs/materials): Mahidol University |
|
| Participants | Total number before randomisation: 60 Inclusion criteria: at least 20 teeth present, more than 80 ppb of VSC Exclusion criteria: systemic complicating factors, oral mucosal lesions, smokers, denture wearers, took antibiotics 1 month prior to study Age (SD) at baseline for each arm: green tea: 18 to 55 years (27.2 ± 9.1 years); placebo: 19 to 42 years (25.8 ± 7.6 years) Gender (% of males): 10% in each group Sample size (per group): calculated as 25 + 5 expected dropouts Number randomised: 60 Method of assessing the outcome (calibration, name/company of the instrument/scale): VSC level measured by portable sulphide monitor (Halimeter RH 17, Interscan Corp, CA, USA), average of 3 readings Number evaluated (mention ITT or per protocol, if any): 60 Dropouts and reasons: none |
|
| Interventions | Intervention: green tea mouthwash (C sinensis extract) Comparison: placebo: hydroalcoholic brownie solution (same ingredients except green tea extract) Dosage: 15 ml to be swished for 1 minute Total number of intervention groups: 1 Duration of treatment: 28 days Duration of follow‐up: baseline, 30 minutes, 3 hours after intervention on day 1 and day 28 |
|
| Outcomes | VSC level measured by portable sulphide monitor (Halimeter RH 17, Interscan Corp, CA, USA), average of 3 readings Any adverse events reported: none |
|
| Notes | Contact: Dr Supanee Rassameemasmaung, dtsrs@mahidol.ac.th | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No mentioned |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes were used |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind Objective measurements used (VSC measured using Halimeter – average of 3 readings) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Low risk | Outcomes of all objectives reported adequately |
| Other bias | Low risk | No other bias evident |
Satthanakul 2014.
| Methods | Location/setting: university, Thailand Number of centres: 1 Recruitment period (duration): not clear Trial design (including number of arms): randomised, double‐blind, clinical study Trial registration number: not mentioned Funding source (or sponsored drugs/materials): materials purchased steam‐distillated LG, peppermint oil and anise oil were obtained from Thai China Flavours and Fragrances Industry Co (Bangkok, Thailand). Reference compounds (citral and geraniol, myrcene) were obtained from Fluka, Switzerland. Polyethylene glycol 4000 (PEG 4000), Tween 80 and menthol were purchased from S Tong Chemicals Bangkok, Thailand. Financially supported by the Faculty of Pharmaceutical Sciences and National Research University (NRU) Project, Khon Kaen University, Khon Kaen, Thailand |
|
| Participants | Total number before randomisation: not mentioned Inclusion criteria: "Qualified subjects in this study were in good health and did not have a history of serious medical conditions or diseases, allergy to EO, and were not pregnant or lactating. They had no clinical signs of oral disease based on a visual examination by a dentist" Exclusion criteria: not mentioned Age (SD) at baseline for each arm: test group: 32.0 ± 6.7 years; placebo group: 32.6 ± 5.3 years Gender (% of males): test group 0; placebo group 50% Sample size (per group): test group 10; placebo group 10 Number randomised: not mentioned Method of assessing the outcome (calibration, name/company of the instrument/scale): VSC, using halimeter; self‐rated hedonic scale Number evaluated (mention ITT or per protocol, if any): 20 Dropouts and reasons: not mentioned |
|
| Interventions | Intervention: test group: lemongrass mouthrinse; "LG mouthrinse contained 1% by volume of LG as an active ingredient, 10% by weight of PEG 4000 and 5% by weight of Tween 80 as a solvent system, 1% by weight of sodium chloride and 0.003% by weight of the flavour mixture containing menthol, peppermint oil, anise oil and vanilla in ethanol as flavouring agents and the mixture was adjusted to 100% with deionised water" Comparison: placebo; "the placebo contained all the same ingredients except for LG" Dosage: only day 0 dosage is mentioned – 15 ml; "On day 0, before and after rinsing with 15 ml sample for 1 min,each volunteer was measured for volatile sulphur compounds (VSCs) level to test the immediate effect of the mouthrinse. Then, they were asked to continue to use the mouthrinse twice a day in the morning and at night for 7 days" Total number of intervention groups: 1 Duration of treatment: 7 days Duration of follow‐up: not mentioned |
|
| Outcomes | Self‐assessment scores: 9‐point hedonic scores (1 = most pleasant; 9 = most unpleasant) Assessment by using halimeter: "The VSC values detected were equivalent to sulphide in parts per billion (ppb) and were recorded" Patient satisfaction scores: "On day 8 before brushing all volunteers rinsed their mouth with 15 ml of the given sample for 1 min. Then they rated overall satisfaction, odour, taste, spiciness and breath freshening" Determination of peak and steady‐state VSC levels using a sulphide monitor, prior to and at several time points after any intervention: "A series of three 30 s‐sampling sessions were performed. To study the possible effect of volatile oil on the VSC measurement, both LG and placebo mouthrinses were pre‐tested in 10 healthy volunteers per group to evaluate the changes of VSC level as time passed after rinsing. Each volunteer was asked to rinse with either LG or placebo" Any adverse events reported: not mentioned |
|
| Notes | Contact: Watcharee Khunkitti, Faculty of Pharmaceutical Sciences, Khon Kaen University, KhonKaen 40002, Thailand; watkhu@kku.ac.th Email was sent on 16 May 2018 ‐ yet to receive reply |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Each mouthrinse sample either LG or placebo was randomly labelled with a different 3‐digit number and randomly distributed to the subjects" Lemongrass oil gives a strong aroma which can be easily detected. Hence blinding will not be possible |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | No evidence of any other bias |
Suzuki 2014.
| Methods | Location/setting: university, Japan Number of centres: 1 Recruitment period (duration): June 2010 and September 2011 Trial design (including number of arms): randomised, double‐blind, cross‐over, placebo‐controlled clinical trial; 2 arms Trial registration number: ISRCTN74332440 Funding source (or sponsored drugs/materials): supported in part by a Grant‐in‐Aid for Young Scientists (no 23792532), Grants‐in‐Aid for Scientific Research (Nos 23593078, 25463278, 25463279) from the Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan, and the MEXT‐Supported Program for the Strategic Research Foundation at Private Universities, 2012‐2016. The tablets (Minna No Zendamakin WB21 Tablet; Wakamoto Pharmaceutical Co, Tokyo, Japan) contained 6.7 x 108 colony‐forming units of L salivarius WB21 |
|
| Participants | Total number before randomisation: 82 Inclusion criteria: having oral malodour above a questionable level (OLT score ≥ 1.5), not currently visiting a dentist for treatment, having no acute symptoms requiring immediate oral cavity treatment, having 1 or more 3 to 6 mm periodontal pockets that bleed on after probing, being non‐edentulous, not wearing prostheses, not using probiotic supplements, not using antibiotics within 3 months, having no daily smoking habit, having no systemic illness, and having no adverse reactions to lactose or fermented milk products Exclusion criteria: not mentioned Age (SD) at baseline for each arm: mean age 44.3 ± 11.6 years; age range 22 to 67 years. Mean age not mentioned for each arm Gender (% of males): 17.4% Sample size (per group): first phase – intervention group 20, placebo group 6; second phase – intervention group 6, placebo group 19 Number randomised: 26 Method of assessing the outcome (calibration, name/company of the instrument/scale): use of OLT test score and the total VSC concentration. Gas chromatography (model GC2014; Shimadzu Works, Kyoto, Japan) to measure the concentration of H2S, CH3SH, andCH3SCH3 in mouth air Number evaluated (mention ITT or per protocol, if any): 23 Dropouts and reasons: 1 patient did not return to clinic on the 2nd test day, and 2 patients used antibiotics |
|
| Interventions | Intervention:
Comparison: placebo Dosage: 1 tablet 3 times per day, taken orally after eating and mouth cleaning Total number of intervention groups: 1 Duration of treatment: 14 days Duration of follow‐up: cross‐over design after 2 weeks wash‐out period, group taking intervention took placebo tablets for 14 days |
|
| Outcomes | OLT assessment scores 0 to 5 (upper and lower limits not defined); means of findings from 2 observers were used Gas chromatography for VSC: total VSC was defined as the sum of the H2S, CH3SH, and CH3SCH3 Any adverse events reported: not mentioned |
|
| Notes | Contact: Nao Suzuki, Section of General Dentistry, Department of General Dentistry Fukuoka Dental College 2‐15‐1 Tamura, Sawara‐ku Fukuoka 814‐0193, Japan; naojsz@college.fdcnet.ac.jp | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Random numbers were computer‐generated" |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "The principal investigator, clinical examiner, and study staff responsible for patient contact and endpoint measurement were blinded to medication assignment until after enrolment and data collection were completed" Quote: "The test and placebo tablets were identical in taste, texture, appearance, and shape (round, 14 mm in diameter, and 4 mm in thickness)" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The principal investigator, clinical examiner, and study staff responsible for patient contact and endpoint measurement were blinded to medication assignment until after enrolment and data collection were completed" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "After starting the investigation, one patient did not return to our clinic on the second test day, and two patients used antibiotics; therefore, a comparative analysis was performed on 23 patients" |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Talebian 2009.
| Methods | Location/setting: Tehran University of Medical Sciences, Iran Number of centres: 1 Recruitment period (duration): conducted in 9 days with 7 days wash‐out, total duration was 63 days Trial design (including number of arms): double‐blind, placebo‐controlled, randomised, cross‐over study (water was negative control and zinc solution was positive control) Trial registration number: no Funding source (or sponsored drugs/materials): funded by Tehran University of Medical Sciences by the number of 2348 | |
| Participants | Total number before randomisation: 10 Inclusion criteria: healthy persons without oral or dental problems related with oral malodour such as decayed teeth, gum disease Exclusion criteria: persons not able to attend in all 9 days of the research, women also excluded to avoid any interference of the elevated oral malodour during period Age (SD) at baseline for each arm: 28 to 42 years Gender (% of males): all male Sample size (per group): 7 Number randomised: 7 Method of assessing the outcome (calibration, name/company of the instrument/scale): halimeter Number evaluated (mention ITT or per protocol, if any): 7 Dropouts and reasons: none | |
| Interventions | Intervention: cinnamon herbal mouthwash with alcohol, nanosil mouthwash with hydrogen peroxide, irsha mouthwash with alcohol
Comparison: distilled water (negative control) and zinc solution (positive control) Total number of intervention groups: 3 Duration of treatment: 3 hours each day for 9 days Duration of follow‐up: 20 minutes after the mouthwash for non‐alcoholic mouthwashes |
|
| Outcomes | Halimeter readings of VSC. According to the cysteine challenge test the basal induction was measured by Halimeter then each person gargle with the mouthwashes and negative solution (water) and positive solution (zinc solution). After 20 minutes the effect of the intervention was measured. This delay was due to alcohol content of 2 commercial mouthwashes. According to halimeter manufacturer alcohol may cause erroneous reading and may be harmful to the device. Mean percentile reduction of VSC was calculated Adverse effects: no details given |
|
| Notes | Report published in Persian and data extraction done by the corresponding author of the study. Authors contacted regarding missing details | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random tables were used (from personal communication) |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Patients were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessors were blinded and halimeter was used for outcome assessment which is an objective measurement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were adequately reported |
| Other bias | Low risk | None |
Tanaka 2010.
| Methods | Location/setting: university, Japan Number of centres: 1 Recruitment period (duration): February 2006 and June 2006 Trial design (including number of arms): double‐blind randomised trial Trial registration number: not mentioned Funding source (or sponsored drugs/materials): supported by commissioned research from Lotte Central Laboratory at Osaka University (J050801012) |
|
| Participants | Total number before randomisation: 149 Inclusion criteria: 20 to 50 years old Exclusion criteria: antibiotic treatment or periodontal treatment within the previous 3 months, a history of systemic disease, abnormal findings on blood tests and/or urinalysis (HbA1c > 5.8% and/or glucose uria positive and/or aspartate aminotransferase > 40 IU/L and/or alanine aminotransferase > 49IU/L and/or g‐glutamyl transpeptidase > 80 IU/Land/or urobilinogen uria positive), decreased number of teeth (< 24 teeth), absence of gingivitis (GI = 0), existence of deep periodontal probing depth (> 6 mm) at 1 site Age (SD) at baseline for each arm: high concentration group 33.7 (8.6) years; low concentration group 33.4 (8.7) years; placebo 34.7 (8.8) years Gender (% of males): high concentration group 50%; low concentration group 40.6%; placebo 57.6% Sample size (per group): high concentration group (n = 32); low concentration group (n = 32), placebo group (n = 33) Number randomised: 100 Method of assessing the outcome (calibration, name/company of the instrument/scale): measurement of VSCs with a gas chromatograph and an OLT score. Gas chromatograph (Shimadzu GC‐14B, Shimadzu, Kyoto, Japan). The glass column was packed with 25% ββ‐oxydipropionitrile on a 60‐ to 80‐mesh support system (Chromosorb W AW‐DMCS‐ST, Shimadzu). The concentration of each sulphur compound was determined with a standard sample of hydrogen sulphide, methylmercaptan, or dimethyl sulphide prepared with a permeater (PD‐1B, Gastec, Kanagawa, Japan) Number evaluated (mention ITT or per protocol, if any): 1 individual (in the high concentration group) was lost after the baseline examination; however, the data at baseline were included in the intention‐to‐treat analysis. All other subjects were followed to their final examination. As a result, 97 subjects were analysed (high concentration group, n = 32 (ITT); low concentration group, n = 32; and placebo group, n = 33) Dropouts and reasons: 2 from high concentration group, 1 from low concentration and placebo groups after baseline examination. Reasons not mentioned |
|
| Interventions | Intervention:
Comparison: placebo group (chewing gum without eucalyptus extract) Dosage: subjects chewed 2 chewing‐gum tablets for 5 minutes, 5 times per day. Subjects were instructed to chew the gum after 3 main meals and between meals (2 periods) Total number of intervention groups: 2 Duration of treatment: 12 weeks Duration of follow‐up: not mentioned |
|
| Outcomes | OLT assessment scores: estimated based on a scale of 0 to 5 (scale not mentioned) VSC levels with a gas chromatograph, equipped with a flame photometric detector system. The level of VSC was defined as ppm of the total concentrations of hydrogen sulphide, methylmercaptan, and dimethyl sulphide Any adverse events reported: no adverse effects were detected or reported by subjects |
|
| Notes | Contact: Dr Muneo Tanaka, Department of Preventive Dentistry, Osaka University Graduate School of Dentistry, 1‐8, Yamadaoka, Suita, Osaka 565‐0871, Japan; tanakam@dent.osaka‐u.ac.jp Email was sent on 16 May 2018 ‐ mail got bounced due to wrong email address |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation was performed according to the method of minimization" Comment: to keep the balance of the distribution of the confounder, the weight factor was set differently for the stratification factors (GI = 10, age = 8, and gender = 7) |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "For participants all chewing gums look alike. All investigators and study personnel were masked to the treatment assignment for the duration of the study" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "All investigators and study personnel were masked to the treatment assignment for the duration of the study" Comment: chewing gum, with and without eucalyptus extract, was used in this study. The components in sugarless chewing‐gum tablets, other than eucalyptus extract, were identical to those found in sugarless chewing‐gums. gum tablets currently on the market. The weight of each tablet was 1.5 g |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 individual (in the high concentration group) was lost after the baseline examination; however, the data at base‐line were included in the intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Low risk | All outcomes are reported adequately |
| Other bias | Low risk | None |
Wang 2017.
| Methods | Location/setting: Department of Periodontology, Peking University School and Hospital of Stomatology & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory Digital Stomatology, Beijing, China Number of centres: 1 Recruitment period (duration): October 2012 to October 2013 (1 year) Trial design (including number of arms): 2‐arm parallel group Trial registration number: not reported Funding source (or sponsored drugs/materials): not reported | |
| Participants | Total number before randomisation: 196 patients and 60 teenage volunteers
Inclusion criteria: OLT test, VSC value (halimeter)
Exclusion criteria: not reported
Age (SD) at baseline for each arm: 27.9 (4.2) years
Gender (% of males): both test and control group had 1 male and 4 females
Sample size (per group): 5
Number randomised: 10
Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT test by Oho and VSC by halimeter Number evaluated (mention ITT or per protocol, if any): all 10 evaluated Dropouts and reasons: none |
|
| Interventions | Intervention: test group was given proper guidance on how to clean tongue coating by using GUM tongue scraper (until no tongue coating can be scrapped off = clean) and OHI was given Comparison: no tongue scrapping and OHI was given Dosage: test candidates should do it once in the morning and once at night while control candidates did not practice tongue scrapping Total number of intervention groups: 1 Duration of treatment: 8 weeks Duration of follow‐up: 8 weeks (during 1st week, 2nd week, 4th week, 8th week – follow‐up timing was set at 08:30 to 10:00), after measuring all the values, patient given OHI after every follow‐up session |
|
| Outcomes | OLT assessment scores: a trained odour panellist assessed OLT test according to Oho's grading standards as: 0 = no halitosis; 1 = halitosis that cannot be easily perceived; 2 = slight but can be clearly noticed; 3 = severe halitosis VSCs assessed by halimeter: the average of 3 consecutive measurements was recorded Any adverse events reported: not reported |
|
| Notes | Sample size calculation: not mentioned Key conclusions of the study authors: "Mechanical self‐cleaning of tongue coating did not influence plaque index while it had tendency to reduce tongue coating area and thickness" Contact: He Lu, Department of Periodontology, Peking University School and Hospital of Stomatology, Beijing 100081, China; helubj@tom.com |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "10 patients were allocated into 2 groups by drawing of lots …" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participant blinding was not possible |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Adverse effects not reported |
| Other bias | Low risk | No other source of bias identified |
Watanabe 2018.
| Methods | Location/setting: Kanagawa Dental University, Japan Number of centres: 1 Recruitment period (duration): December 2011 to August 2012 Trial design (including number of arms): 2‐arm (experimental and placebo) study Trial registration number: UMIN000018305 Funding source (or sponsored drugs/materials): Grant‐in Aid for Scientific Research, Japan Society for Promotion of Science | |
| Participants | Total number before randomisation: 44
Inclusion criteria: healthy volunteers, no antibiotic therapy within last 30 days, probing depth not more than 5 mm
Exclusion criteria: cigarette smokers, systemic diseases Age (SD) at baseline for each arm: 40.1 (12.3) years Gender (% of males): 10 males (47.6%), 11 females (52.4%) Sample size (per group): experimental group: 11; placebo group: 10 Number randomised: 21 Method of assessing the outcome (calibration, name/company of the instrument/scale): oral malodour assessment using OralChroma portable gas chromatograph; tongue coating score using semi‐quantitative conventional scores; microbial study using salivary sample cultured, and antibacterial activity against oral bacteria Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: not mentioned |
|
| Interventions | Intervention: pycnogenol chewing gum Comparison: placebo chewing gum Dosage: 12 Pycnogenol® (PYC) tablet 0.42% PYC (2.52 mg per gum piece) per day (i.e. chewing 2 pieces 6 times daily) Total number of intervention groups: 1 Duration of treatment: 4 weeks Duration of follow‐up: 2 weeks and 4 weeks |
|
| Outcomes | Oral malodour using OralChromaTM portable gas chromatograph, same time of assessment for each subject of VSC in concentrations of ppb Any adverse events reported: not mentioned |
|
| Notes | Sample size calculation: met Key conclusions of the study authors: "Use of gum chewing containing PYC is effective in reducing oral malodour by decreasing the number of bacteria producing volatile sulphur compounds in saliva as well as the accumulation of tongue‐coating bacteria" Contact: Kiyoko Watanabe, Department of Oral Science, Kanagawa Dental University, 82 Inaoka‐cho, Yokosuka 238‐8580, Japan; watanabe@kdu.ac.jp | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The subjects were divided into the groups with a stratified randomisation method based on age and gender" |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | No details given in the report. However, the trial registration mentions it as "Double blind ‐ all involved are blinded" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding details not given. However, the method of outcome assessment is objective (OralChroma) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Wigger‐Alberti 2010.
| Methods | Location/setting: not mentioned Number of centres: 1 Recruitment period (duration): 21 days Trial design (including number of arms): randomised, double‐blind, placebo‐controlled, parallel‐group clinical trial Trial registration number: NCT01747226 Funding source (or sponsored drugs/materials): funded by GABA International AG |
|
| Participants | Total number before randomisation: not mentioned Inclusion criteria: Caucasian, age ≥ 18 years, OLT score of breath ≥ 2, VSC readings (sum of H2S and CH3SH by OralChroma) ≥ 120 ppb*, intraoral cause of bad breath, non‐smokers, willing to participate and able to give written informed consent Exclusion criteria: volunteers with obvious caries or periodontal disease were not included into the study; ongoing dental treatment or any other medical treatment of the oral cavity; any known allergy to previously used oral hygiene products or any known allergy to any of the ingredients of the study products, which are used during the study; any pathological change of the oral mucosa; use of prohibited treatments/therapies and/or abuse of drugs, alcohol, etc.; pregnancy or breastfeeding; active caries; acute sinusitis; severe oropharyngeal infections; on medications which can cause malodour; reduced salivary flow due to pathological reasons (e.g. Sjögren syndrome); situation considered not compatible with the study according to the investigator's opinion, the latter includes: patients eating very spicy food, persons under homeopathic therapy, patients who used antibiotics during the 2 months before the study, patients frequently using chewing gum, patients under corticosteroids or other serious medication; patients unwilling to abstain from additional oral hygiene (only toothbrushing allowed) particularly mouthrinse, chewing gums, breath strips etc. Age (SD) at baseline for each arm: age 43.1 ± 12.3 years (whether for each arm not clear) Gender (% of males): 18% Sample size (per group): not mentioned Number randomised: not mentioned Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT evaluation was performed by trained evaluators (sniffers) using a 6‐point scale (ranging from 0 = odour cannot be detected to 5 = very strong malodour); VSC levels, specifically H2S, were recorded with the OralChroma® instrument Number evaluated (mention ITT or per protocol, if any): 174 in total all groups. ITT is mentioned but protocol not specified for ITT Dropouts and reasons: not mentioned |
|
| Interventions | Intervention:
Comparison: chlorhexidine‐containing products, including a bench mark product (reference) and a positive control as well as water(negative control) Dosage: 15 ml for 1 minute twice daily Total number of intervention groups: 1 Duration of treatment: 21 days Duration of follow‐up: not mentioned |
|
| Outcomes | OLT assessment scores: 0 = odour cannot be detected, 1 = questionable malodour, barely detectable, 2 = slight malodour, exceeds the threshold of malodour recognition, 3 = malodour is definitely detected, 4 = strong malodour, and 5 = very strong malodour VSC reading of the OralChroma which shows the concentration values of hydrogen sulphide, methyl mercaptan and dimethyl sulphide in ppb and ng/ml Patients' opinion (time frame: after 3 weeks): opinion regarding product satisfaction was scored on a VAS line (0 to 10). The questionnaire included the following points: satisfaction, side effects, use, future use and effectiveness Any adverse events reported: no adverse events were documented during the study |
|
| Notes | Contact: K‐P Wilhelm, proDERM Institute for Applied Dermatological Research GmbH, Schenefeld, Germany; kpw@proderm.de Email sent on 15 December 2018 (no reply as on date) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Quadruple masking (Participant, Care Provider, Investigator, Outcomes assessor)" (obtained from trial registration) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Quadruple masking (Participant, Care Provider, Investigator, Outcomes assessor)" (obtained from trial registration) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ITT analysis was done, however, reasons for dropout were not mentioned |
| Selective reporting (reporting bias) | Low risk | All outcomes mentioned during the trial registration were reported |
| Other bias | Unclear risk | Discrepancy in the methodology mentioned during the trial registration and the publication |
Wilhelm 2012.
| Methods | Location/setting: research institute Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): single‐centre, examiner‐blind, clinical randomised cross‐over design Trial registration number: not mentioned Funding source (or sponsored drugs/materials): funded by GABA International |
|
| Participants | Total number before randomisation: not mentioned Inclusion criteria: non‐smokers Exclusion criteria: subjects with active caries or periodontal disease Age (SD) at baseline for each arm: not mentioned, only range 18 to 65 years Gender (% of males): 20% Sample size (per group): not mentioned Number randomised: not mentioned Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT rating; VSC levels were measured with a portable sulphide monitor (OralChroma CHM‐1, Abilit) Number evaluated (mention ITT or per protocol, if any): 50 to 54 Dropouts and reasons: not mentioned |
|
| Interventions | Intervention: tooth‐and‐tongue gel (meridol HALITOSIS tooth & tongue gel; 1400 ppm F‐ from amine fluoride/stannous fluoride (ASF), 0.5% zinc lactate, oral malodour counter‐actives (OMCs)); reference toothpaste – (1400 ppm F from sodium monofluorophosphate); tongue cleaner; toothbrush Comparison: intra group Dosage: subjects were instructed to brush their teeth with the provided toothpaste twice daily (morning and evening) for 2 minutes (stop‐watch provided) Total number of intervention groups: 3 Duration of treatment: 7 days Duration of follow‐up: not mentioned |
|
| Outcomes | OLT assessment scores: 6‐point scale, upper and lower limit not mentioned VSC levels using portable sulphide meter focusing on H2S and CH3SH, the sum of H2S and CH3SH, and total VSCs (H2S + CH3SH + (CH3)2S). Determination of peak and steady‐state levels, raw data and individual relative differences between baseline VSC readings and corresponding readings 5 and 60 minutes after the first application as well as after 7 days of treatment (overnight effect) were recorded, prior to and at several time points after any intervention Patient satisfaction scores: subjects completed a questionnaire regarding tolerability, efficacy, handling of the tongue cleaner, and coping with the combined use of gel and tongue cleaning (i.e., patient acceptance) Any adverse events reported: not mentioned |
|
| Notes | Contact: Dr Klaus‐Peter Wilhelm, proDERM Institute for Applied Dermatological Research, Kiebitzweg 2, 22869 Schenefeld, Germany; kpw@proderm.de Email was sent on 16 May 2018 ‐ yet to receive reply |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Single blinding "examiner‐blind clinical study" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | Adverse events not mentioned |
| Other bias | Low risk | None |
Winkel 2003.
| Methods | Location/setting: university Number of centres: 2 clinics for Periodontology Amsterdam or the University Complutense of Madrid Recruitment period (duration): not mentioned Trial design (including number of arms): parallel, dual‐centre, randomised, double‐blind, placebo‐controlled clinical trial Trial registration number: not mentioned Funding source (or sponsored drugs/materials): supported by a grant from Dentaid SL, Barcelona, Spain |
|
| Participants | Total number before randomisation: not mentioned Inclusion criteria: presenting halitosis of oral origin, an OLT score 41, using an arbitrary 0 to 5 scale (0 = no halitosis to 5 = offensive halitosis), a level of VSC 4170 ppb determined with a portable sulphur compounds detector (halimeters), a Winkel tongue coating index (WTCI) 44 and probing pocket depths not exceeding 4 mm with the possible exception of distal sites of 2nd molars and pockets at wisdom teeth if present Exclusion criteria: systemic diseases, pregnancy and systemic medication related to oral dryness and systemic antibiotic therapy 1 month prior to the study Age (SD) at baseline for each arm: mean age of the study population was 43.8 years (SD 15.8, range 21 to 84). Test group: 40.9 years (SD 14.1); placebo group: 46.8 years (SD 17.1) Gender (% of males): 52.5% Sample size (per group): 20 Number randomised: not mentioned Method of assessing the outcome (calibration, name/company of the instrument/scale): OLT scale; halimeter®, connected to a pen recorder Number evaluated (mention ITT or per protocol, if any): 20 each in both groups Dropouts and reasons: not mentioned |
|
| Interventions | Intervention: halitas, Dentaid SL,Spain ‐ contains chlorhexidine (0.05%), cetylpyridinium chloride (0.05%) and zinc lactate (0.14%) Comparison: placebo Dosage: gargle with 15 ml of the mouthwash for 1 minute and to avoid rinsing Total number of intervention groups: 1 Duration of treatment: 2 weeks Duration of follow‐up: not mentioned |
|
| Outcomes | OLT assessment scores: OLT measurements were taken, using an arbitrary 0 to 5 scale (0 = no halitosis to 5 = offensive halitosis) VSC levels: using halimeter, connected to a pen recorder. Peak VSC level was registered in ppb. 2 independent and consecutive measurements were taken. The mean of both scores represented the individual VSC score Any adverse events reported: more discolouration was present after therapy in the test group whereas no changes after therapy was present in the placebo group |
|
| Notes | Contact: Edwin G Winkel, Clinic for Periodontology Amsterdam, de Boelelaan 589, 1082 RM Amsterdam, The Netherlands; edwinwinkel@kliniekvoorparodontologie.com Email was sent on 16 May 2018 ‐ mail got bounced due to wrong address |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated list was used (information taken from Roldan 2003 trial) |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "participants ‐placebo mouthwash had a similar colour as the experimental product, a slightly bitter taste but lacked the active ingredients" Quote: "at the time of re‐evaluation, the clinical investigators were unaware of the treatment at any time point of the study" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The clinical investigators were unaware of the treatment at any time point of the study" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No attrition (information taken from Roldan 2003 trial) |
| Selective reporting (reporting bias) | Low risk | All outcomes were adequately reported |
| Other bias | Low risk | None |
Wirthlin 2011.
| Methods | Location/setting: University of California, San Francisco, California, USA Number of centres: 1 Recruitment period (duration): April 2008 to February 2009 Trial design (including number of arms): double‐blind, randomised, parallel‐group clinical trial Trial registration number: NCT00867035 Funding source (or sponsored drugs/materials): University of California, San Francisco |
|
| Participants | Total number before randomisation: 47 Inclusion criteria: adult with threshold score of 2 on OLT halitosis evaluation Exclusion Criteria: taking another experimental drug, or antibiotic Age (SD) at baseline for each arm: not available Gender (% of males): not available Sample size (per group): intervention 9; control 13 Number randomised: 22 Method of assessing the outcome (calibration, name/company of the instrument/scale): organoleptic and portable gas chromatography Number evaluated (mention ITT or per protocol, if any): 19; ITT analysis was done Dropouts and reasons: 3 dropouts (1 from intervention and 2 from control group due to unknown reasons and all 3 were women) |
|
| Interventions | Intervention: chlorhexidine gluconate and scraper (Peridex) Comparison: chlorine dioxide and scraper 20 ml of mouthwash used for 30 seconds as adjunct to tongue scraper twice a day; other name: "CloSYS" Dosage: 20 ml of 0.12% chlorhexidine gluconate mouthwash used for 30 seconds, twice a day, for 1 week Total number of intervention groups: 2 Duration of treatment: 1 week Duration of follow‐up: 1 week |
|
| Outcomes | The Rosenberg scale: scored 0 to 5 with 0 = no bad breath, 5 = worst bad breath. A score of 2 is the threshold at which bad breath is determined (time frame: baseline, 1 hour, 2 hours, 4 hours, 1 week) VSC assessment using portable gas chromatograph at time frame: baseline, 1 hour, 2 hours, 4 hours, 1 week) Any adverse events reported: 1 subject in the intervention group reported altered taste sensation which subsided after discontinuation of the mouthwash (Peridex) |
|
| Notes | Sample size calculation: not mentioned Key conclusions of the study authors: "This investigation has shown that both 0.12% chlorhexidine gluconate and 0.1% stabilized chlorine dioxide mouthrinse used as adjuncts to daily tongue scraping are effective in reducing unpleasant bad breath to a socially acceptable level" Contact: M Robert Wirthlin, Department of Orofacial sciences, University of California, San Francisco, California 94143, United States | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "subjects were assigned an identification number, in sequence, from a computer generated table of random numbers. The number was used to code their data sheets and allocate to a rinse" |
| Allocation concealment (selection bias) | Low risk | Quote: "the allocation scheme was decided by a third investigator not in contact with subjects, was an odd random identification number for 0.12% CHX and an even number for 0.1% ClO2" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quadruple blinding (participant, care provider, investigator, outcomes assessor) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quadruple blinding (participant, care provider, investigator, outcomes assessor) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 dropouts (1 from intervention and 2 from control group due to unknown reasons and all 3 were women). ITT analysis was done. However, in comparison, no values at any time point differed between groups |
| Selective reporting (reporting bias) | Low risk | All outcomes were adequately reported |
| Other bias | Unclear risk | The study investigators have changed the eligibility threshold of 75 ppb for H2S measure to OLT of 2 or more |
CHX = chlorhexidine; CPC = cetylpyridinium chloride; DMS = dimethylsulphide; F = fluoride; GCF = gingival crevicular fluid; H2S = hydrogen sulphide; ITT = intention‐to‐treat; LF = lactoferrin; LPO = lactoperoxidase; MM = methyl mercaptan; NaF = sodium fluoride; ppb = parts per billion; ppm = parts per million; OHI = oral hygiene instruction; OLS = organoleptic test scores; OLT = organoleptic test; RCT = randomised controlled trial; SD = standard deviation; SRP = scaling and root planing; VAS = visual analogue scale; VSC = volatile sulphur compounds; ZnCl = zinc chloride; w/w = weight for weight.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ademovski 2016 | Intervention given once and followed up for 12 hours. |
| Alqumber 2014 | Intervention given for 4 days only. |
| Badanjak 2016 | Mouthwash used twice (60 seconds and 30 seconds) only. |
| Betsy 2014 | Advanced periodontitis (pocket depth 4 mm to 6 mm) patients were included in the trial. |
| Bordas 2008 | Intervention given for 3 days only. |
| Boulware 1984 | Comparison of 4 different interventions but only for a day by single use. |
| Brunette 1998 | Patients without halitosis were included in the trial and intervention was used only once for a day. |
| Carvalho 2004 | Intervention given for 4 days only. |
| Chen 2010 | Iinterventions were used for a period less than 1 week (28 hours). |
| Codipilly 2004 | Participants were induced halitosis. |
| Conceição 2008 | Subjects who had halitosis secondary to caseous tonsillitis were included in the trial. |
| Dereci 2016 | Patients with pocket depth of 5 mm or more were included in the trial. |
| DRKS00005334 | Mouthwash administered for 30 seconds twice per week. |
| EUCTR 2007‐003756‐11 | Halitosis secondary to gut disease included. |
| Farrell 2006 | Duration of intervention is less than a week. |
| Farrell 2007 | Intervention used only for single day (2 brushings) and measurements taken at baseline and 24 hours after baseline were compared. |
| Farrell 2008 | Duration of intervention was 24 hours. |
| Faveri 2006 | Study was conducted on people with morning breath disorder which is part of our exclusion criteria. |
| Feng 2010 | Interventions used only for 2 days during each treatment period. Each group had 3 treatment periods using 2 different interventions. |
| Fine 2005 | Microbial study. |
| Frascella 1998 | Intervention period was 1 day with single use and measurements at 0.5, 1, 2 and 4 hours post‐rinsing. |
| Frascella 2000 | Single use intervention with measurements at 2, 4, 8, 24, 48, 72 and 92 hours. |
| Gerlach 1998 | Intervention period was less than 1 week (i.e. 1 day and 5 days with measurements at 3, 6 and 8 hours). |
| Greenstein 1997 | Intervention given for less than a week. |
| Haas 2007 | Intervention less than 1 week. |
| Hu 2013 | Study did not involve intervention for halitosis but evaluated if 2 dentifrices containing arginine would increase malodour due to increased ammonia production from breakdown of arginine. |
| Katsinelos 2007 | Subjects with halitosis had chronic systemic disease. |
| Keller 2012 | Subjects with morning breath were included. |
| Leal 2019 | Single use intervention for 1 minute was used. |
| Lodhia 2008 | Single dose chewing gum and follow‐up of 3 hours. |
| Malhotra 2011a | Halitosis was not an outcome in the trial. |
| Mendes 2016 | Trial participants were with morning malodour. |
| Moreno 2005 | Subjects diagnosed with aggressive periodontitis were included in the trial. |
| Mousquer 2017 | Abstract publication. |
| Nakano 2016 | Single tablet was used as intervention and VSC was tested at baseline, 10 minutes and 30 minutes after ingestion. |
| NCT00250289 | Single use oral sticker and assessment at every 7 minutes. |
| NCT00655772 | Outcome assessed up to 4 hours after intervention. |
| NCT00748943 | Trial participants were with morning malodour. |
| NCT00875927 | Trial outcome measured at 150 minutes. |
| NCT02194621 | Outcome assessed was oral bacteria causing malodour. |
| NCT02789436 | Advanced chronic periodontitis cases were included in the trial. |
| NCT03346460 | Single session of photodynamic therapy and tongue scraping was planned. |
| NCT03591484 | Patients with bronchiectasis were included. |
| NCT03656419 | Single session of photodynamic therapy and tongue scraping was planned. |
| Newby 2008 | Outcome assessment done up to 7 hours after intervention. |
| NL3100 (NTR3240) | Trial participants were with morning malodour. |
| Pedrazzi 2004 | Volunteers were induced halitosis by refraining them from cleaning their tongue. |
| Penala 2016 | Subjects with severe periodontitis were included in the trial. |
| Peruzzo 2007 | Trial participants were with morning malodour. |
| Peruzzo 2008 | Trial participants were with morning malodour. |
| Pitts 1981 | Single use of intervention and outcome measurement up to 120 minutes. |
| Polat 2008 | Halitosis secondary to wisdom tooth extraction was studied. |
| Porciani 2012 | Follow‐up was up to 2 hours only. |
| Quirynen 2002 | Trial participants were with morning malodour. |
| Quirynen 2004 | Outcome of the trial was microbial load and taste sensation. |
| Quirynen 2005 | Patients with more than 6 mm pocket depth included (severe periodontitis). |
| Reingewirtz 1999 | Single use intervention. |
| Roldán 2004 | Evaluation period is 1 to 5 hours. |
| Rolla 2002 | Outcome measured at 1, 2 and 3 hours. |
| Rosenberg 1992 | Outcomes assessed on second day. |
| Rosing 2009 | VSC was measured before and at 5, 15, 30, 45 and 60 minutes of chewing the test gums. In the second series, VSC production was monitored prior to and up to 30 minutes after a rinse with cysteine 6 mM alone or after a rinse followed by chewing the test gums. |
| Saad 2011 | Single use mouthwash and outcomes assessed at 30, 60, 90 and 180 minutes. |
| Saad 2016 | Single use of intervention. |
| Schmidt 1978 | Duration of follow‐up after use of mouthrinse was only 3 hours. |
| Seemann 2001 | All 3 interventions used once with a follow‐up of 35 minutes. |
| Seemann 2001a | Participants were healthy and without specific complaints of halitosis or chosen based on VSC levels. |
| Sharma 1999 | Single use of intervention with measurements done at baseline and 12 hours after intervention. |
| Sharma 2007 | Single use of intervention with measurements at baseline and 12 hours after treatment. |
| Sheikh 2016 | Pregnant patients were the study subjects. |
| Shin 2011 | The subjects ingested a test or placebo tablet twice in the morning at a 1‐hour interval and there was no follow‐up. |
| Shinada 2008 | Single use mouthwash. |
| Shinada 2010 | Subjects included were having morning malodour. |
| Silveira 2014 | Included patients had advanced chronic periodontitis. |
| Silveria 2017 | Included patients had advanced chronic periodontitis. |
| Soares 2015 | Subjects included were having morning malodour. |
| Soares 2015a | Patients with probing pocket depth (PPD) ≥ 5 mm in at least 6 sites were included in the trial. |
| Sreenivasan 2003 | Outcome measure for intervention was decrease in hydrogen sulfide‐producing odorigenic bacteria. |
| Sreenivasan 2004 | Outcome measure for intervention was decrease in range of microbial flora. |
| Steenberghe 2001 | Intervention was meant to evaluate morning breath. |
| Sterer 2008 | Intervention followed up for 120 minutes only. |
| Sterer 2013 | Intervention used only twice (night before and next morning) and was evaluated the same evening. |
| Tamaki 2007 | Halitosis was induced and interventions were tested. |
| Thaweboon 2011 | Evaluation of outcome was decrease in VSC producing bacteria. |
| Thrane 2010 | Study period was only 5 days. Single use of intervention on fourth day and measurements at baseline and after 12 hours on the fifth day. |
| Tian 2013 | Intervention followed up for 180 minutes only. |
| Tolentino 2011 | Subjects included were having morning malodour. |
| Troccaz 2011 | Subjects included were having morning malodour. |
| Uchida 1973 | Intervention given for 5 days and outcome assessment was done after 1 day follow‐up. |
| UMIN000002145 | Subjects with physiological halitosis included. |
| UMIN000002713 | Single use intervention. |
| Van der Sluijs 2018 | Subjects included were having morning malodour. |
| Wang 2015 | Patients with deep pockets were included. |
| Wessel 2017 | The study was not designed to treat halitosis. |
| Wild 2001 | Single use of intervention with measurements at baseline, 1, 2 and 3 hours after treatment. |
| Wilhelm 2010 | Single use mouthrinse. |
| Wilhelm 2013 | Single use of intervention and measurements at baseline and after 5 minutes and 60 minutes of treatment. |
| Wåler 1997 | Subjects included were having morning malodour. |
| Yaegaki 1992 | Single use of intervention and outcomes measured at the end of 3.5 hours. |
| Yoshimatsu 2006 | The authors have not mentioned about whether the participants (11 male adults) had breath odour or not in the paper. The purpose of this study was to investigate the effect of tablets containing the protease, actinidin on the reduction of human tongue coating. |
| Yoshimatsu 2007 | The duration of follow‐up was only 90 minutes after administration of tablets. |
CAL = clinical attachment level; RCT = randomised controlled trial; VSC = volatile sulphur compounds.
Characteristics of studies awaiting assessment [ordered by study ID]
Cuihua 2009.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Full‐text not available at British Library |
Dongling 2017.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Full‐text not available at British Library |
Gupta 2016.
| Methods | Location: Department of Oral Medicine and Radiology, Sharad Pawar Dental College and Hospital, Sawangi (Meghe), District – Wardha 442001, Maharashtra, India Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): 2 Trial registration number: not mentioned Funding source (or sponsored drugs/materials): not mentioned |
| Participants | Total number before randomisation: 50 Inclusion criteria: male and female subjects age 18 to 45 years, at least 20 natural uncrowned teeth excluding third molars, subjects suffering from gingivitis and periodontitis, have tooth stains, gingival index > 1 at more than 60% of sites examined, dental plaque index of 2 or more Exclusion criteria: subjects having pain and multiplicity or chronic inflammatory periodontal/gingival problems, relatively severe tetracycline stained teeth, gross oral pathology, known sensitivity or oral mucosal tissue reaction to toothpaste and systemic infections – respiratory, gastrointestinal, skin or urinary, any external dental treatment ‐ scaling, polishing, flossing, fluoride treatment in preceding 2 weeks, history of intake of antibiotics and anti‐inflammatory drugs in the past 3 to 4 weeks, pregnant and lactating females Age (SD) at baseline for each arm: not given Gender (% of males): Group 1: 20 females (21 to 50 years) and 10 males (25 to 42 years); Group 2: healthy volunteer 10 females and 10 males Sample size (per group): Group 1: 30, Group 2: 20 Number randomised: Group 1: 30 (n = 15 for Babool and n = 15 for placebo group); Group 2: 20 (n = 10 for Babool and n = 10 for placebo group) Method of randomisation: not mentioned Allocation concealment method: not mentioned Blinding: not mentioned Method of assessing the outcome (calibration, name/company of the instrument/scale): not mentioned Number evaluated (mention ITT or per protocol, if any): not mentioned Dropouts and reasons: not mentioned |
| Interventions | Type of intervention: Babool neem toothpaste Dosage: not mentioned Total number of intervention groups: 2 Comparison: placebo toothpaste Duration of treatment: Group 1: 12 weeks of use of study product and 1 week follow‐up; Group 2: 6 weeks of use of study product Duration of follow‐up: Group 1: followed up every 2 weeks interval from baseline up to 12 weeks (6 visits) and 1 follow‐up visit after study completion at 13th week (visit 7); Group 2: analysis was carried over 4 visits from baseline visit (visit 0) i.e., day 1 before brushing, visit 1 after brushing, visit 2 was 6 hours after visit 1 and visit 3, 12 hours after visit 1, the last visit (visit 4) was after 6 weeks from visit 0 |
| Outcomes |
|
| Notes | Need clarifications from authors regarding the inclusion criteria of the healthy volunteers and the comparisons given in table 2 Contact: Dr Arun Gupta, Dabur Research & Development Centre, arun.gupta@mail.dabur |
Liang 2013.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Waiting for translation |
Niles 2003.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Full‐text not available at British Library |
Rostoka 2012.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Full‐text not available at British Library. |
Shimei 2014.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Full‐text not available at British Library |
Vazquez 2003.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Full‐text not available at British Library |
ITT = intention‐to‐treat; OLT = organoleptic test; SD = standard deviation.
Characteristics of ongoing studies [ordered by study ID]
CTRI/2014/04/004519.
| Trial name or title | Effect of test chewing gums on bad breath and oral micro‐organisms |
| Methods | Location/setting: university and private practice Number of centres: 2 Recruitment period (duration): not mentioned Trial design (including number of arms): randomised, parallel‐group, placebo‐controlled trial Funding source (or sponsored drugs/materials):
|
| Participants | Inclusion criteria:
Exclusion criteria:
Sample size (per group): not mentioned Number randomised: 78 Method of randomisation: permuted block randomisation, fixed Allocation concealment method: not mentioned Blinding: participant, investigator, outcome assessor and data‐entry operator blinded |
| Interventions | Type of intervention:
Dosage: gums must be consumed thrice a day after meals for 15 days Total number of intervention groups: 3 groups Comparison: placebo chewing gum Duration of treatment: 15 days Duration of follow‐up: baseline, day 1, day 15 and day 21 |
| Outcomes |
|
| Starting date | 7 April 2014 |
| Contact information | Sushama R Galgali, VS Dental College & Hospital KR Road VV Puram, Bangalore, Karnataka, 560004, India shamagl@yahoo.co.in |
| Notes | Recruitment status: completed |
CTRI/2018/05/014049.
| Trial name or title | Effect of novel herbal dentifrice in control of plaque, gingivitis and halitosis ‐ randomised controlled trial |
| Methods | Location: Department of Public Health Dentistry, Manipal College of Dental Sciences, Manipal, Udupi, Karnataka 576104, India Number of centres: 1 Recruitment period (duration): from 15 June 2018 Trial design: randomised, parallel‐group, active controlled trial Funding source: Sriveda Sattva Pvt Ltd 21st KM, Udayapura Kanakapura Main Road, Bangalore, India |
| Participants | Total number before randomisation: not given Sample size: 110 Inclusion criteria: adults, both genders and subjects having plaque and gingivitis of more than score 2. Subjects willing to participate and those giving informed consent Exclusion criteria: subjects with history of use of antibiotics or anti‐inflammatory drugs in the last 1 week, allergy to any herbal products or rampant caries or subjects with more than 30% of the teeth missing or crowns or large restorations |
| Interventions | Intervention: Sudanta toothpaste Control: Colgate Total toothpaste Dose: twice daily brushing for 4 minutes with pea size amount of toothpaste |
| Outcomes | Primary outcome: plaque, gingivitis Secondary outcome: halitosis and saliva pH Outcome assessment: baseline and after 30 days Outcome assessment method: halitosis would be recorded at baseline and 1 month using handheld breath analyser (Tanita) as per the manufacturer instructions |
| Starting date | 15 June 2018 |
| Contact information | P Kalyana Chakravarthy, Room number 8, Department of Public Health Dentistry, Madhav Nagar Manipal Udupi, Karnataka, India drkalyan81@gmail.com |
| Notes | Results not available |
CTRI/2018/06/014686.
| Trial name or title | Effectiveness of a polyherbal formulation to treat gingivitis over a period of 3 months: a randomised trial |
| Methods | Location: Public Health Dentistry, Thai Moogambigai Dental College and Hospital, Chennai‐107, Tamil Nadu, India Number of centres: 1 Recruitment period: 3 months Trial design: randomised, parallel‐group, active controlled trial Funding source: Dr MGR Educational and Research Institute University |
| Participants | Inclusion criteria: aged 18 to 50 years, both genders; patients suffering from moderate to severe gingivitis and malodour of oral origin; those providing consent to participate and willing to be available for follow‐up for 3 months Exclusion criteria: systemic diseases, oral malodour from extraoral origin and those allergic to any constituents of toothpaste Number randomised: 30 Method of randomisation: computer generated randomisation Allocation concealment method: pre‐numbered or coded identical containers Blinding: participant and investigator blinded |
| Interventions | Intervention: polyherbal paste formulation (haritaki, vibhitaki, amalaki, yasthimadu, sonth, kalimirch, pippili, vat vriksha, babbula, sonf are pulverized and added in specific concentrations of 5 g/100 g of toothpaste) Control: Colgate toothpaste (triclosan) Dose: to be used twice daily (morning and night) for a period of 3 months |
| Outcomes | Primary outcome: reduction in gingivitis and halitosis over a period of 3 months Secondary outcome: reduction in plaque microbial load, total salivary bacterial load and total protein content Outcome assessment: 30, 60 and 90 days Outcome assessment method: not given |
| Starting date | 15 July 2018 |
| Contact information | Dr S Samuel Raj; Public Health Dentistry, Thai Moogambigai Dental College and Hospital , Chennai‐107, Tamil Nadu, India samuelrajsrinivasan@gmail.com |
| Notes | Results not available |
DRKS00010618.
| Trial name or title | Clinical evaluation of the efficacy of Shur Breath (Sylphar) in the reduction of bad breath |
| Methods | Location/setting: Medical Center Universitätszahnklinik Witten/Herdecke, Witten, Germany Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): 3 Funding source (or sponsored drugs/materials): Sylphar nv, Xavier De Cocklaan 42, 9531 Deurle, Belgium |
| Participants | Inclusion criteria:
Exclusion criteria: alcoholism, nicotine, pregnancy or lactation, participation in a clinical trial within the last 30 days, active caries, acute sinusitis, strong oropharyngeal infection, medicines that can cause halitosis, reduced salivation, subjects eat the food very sharp, volunteers receiving homeopathic treatment, taking antibiotics 2 months prior to study entry, eat frequent gum, subjects who do not comply with the study protocol, severe systemic disease, known hypersensitivity to a substance used in the study, serious oral diseases such as acute ulcerative gingivitis or acute gingivostomatitis, and orthodontic appliances. Sample size (per group): not given Number randomised: 54 Method of randomisation: not given Allocation concealment method: not given Blinding: investigator/therapist, assessor |
| Interventions | Type of intervention: Arm 1: Shur Breath twice daily (1st after brushing and 2nd after 6 hours) for 14 days; Arm 2: Fresh Breath halitosis meridol mouthrinse twice daily 15 ml after brushing for 14 days Dosage: Arm 1: twice daily; Arm 2: 15 ml twice daily Total number of intervention groups: 2 Comparison: Arm 3: tap water 15 ml twice daily after brushing for 14 days Duration of treatment: 2 weeks Duration of follow‐up: not given |
| Outcomes | The primary endpoint is before the reduction of VSC with halimeter (InterScan) |
| Starting date | 1 July 2016 (anticipated) |
| Contact information | Universität Witten/HerdeckeFakultät für Gesundheit (Department für Zahn‐,Mund‐ und Kieferheilkunde) Lehrstuhl für Zahnerhaltung und Präventive Zahnmedizin, Germany |
| Notes | Recruiting planned |
IRCT201105136466N1.
| Trial name or title | The effect of persica (herbal oral rinse) on halitosis in patient visiting Shiraz dental school ‐ 2011 |
| Methods | Location/setting: Shiraz Faculty of Dentistry, Iran Number of centres: 1 Recruitment period (duration): 15 July 2011 to 2 October 2011 Trial design (including number of arms): parallel Funding source (or sponsored drugs/materials): Research Deputy, Shiraz Dental School, Shiraz, Iran |
| Participants | Inclusion criteria: participants with OLT score > 2 and tongue coating score > 4 Exclusion criteria: smoking; being an alcoholic; systemic disease; consumption of medications that cause xerostomia; using antibiotics in previous month; pocket depth > 6 mm; eating spicy food or garlic or onion 48 hours ago and having prosthesis (fix or removable) or orthodontic appliance Sample size (per group): not given Number randomised: 100 Method of randomisation: not given Allocation concealment method: not given Blinding: double‐blind |
| Interventions | Type of intervention: persica herbal mouthwash that is available in pharmacies, as directed by company brochure (15 drops in 15 ml water) in the same glass (marked with X for making double blind) with a volume of 140 ml for use 7 days (14th round) was poured Dosage: 2 soup spoons, twice a day (morning after breakfast and before bed at night) to gargle for 40 seconds Total number of intervention groups: 1 Comparison: placebo (including water and alcohol and essential oil flavourings without active substance) in the same glass (marked O for making double blind) with a volume of 140 ml for use 7 days (14th round) was poured Duration of treatment: 7 days Duration of follow‐up: before and 7 days after intervention |
| Outcomes | •OLT assessment scores •Winkle tongue coating score |
| Starting date | 15 July 2011 |
| Contact information | Akram Nikpour, Shiraz Faculty of Dentistry, Iran nikpoura@sums.ac.ir |
| Notes | Expected recruitment end date: 2 October 2011 |
IRCT2014121520314N1.
| Trial name or title | Clinical trial of comparison of efficacy of halita mouthrinse with chlorhexidine mouthrinse in reducing oral malodour in patients with halitosis in 7‐day consumption |
| Methods | Location: Tabriz University of Medical Sciences, Daneshgah Street, Iran Number of centres: 1 Recruitment period (duration): 21st March 2014 to 23rd August 2014 Trial design (including number of arms): 2 Funding source (or sponsored drugs/materials): Rozhin Co, Tabriz, Iran and Vice Chancellor for Research, Faculty of Dentistry, Tabriz University of Medical Sciences |
| Participants | Total number before randomisation: not given Inclusion criteria: OLT score (OLS) of over 2; age: from 17 years to 26 years old; both genders Exclusion criteria: alcohol and tobacco use; systemic diseases; medications that cause dry mouth; consumption of antibiotics in the previous 2 weeks; pocket depth greater than 6 mm; eating spicy foods, onion, and garlic 48 hours prior to the examination; use of orthodontic appliances (fixed or removable) and removable dental prosthesis; allergy or any undesirable reactions to either of test mouthrinses Sample size (per group): 25 Number randomised: 50 Method of randomisation: not available Allocation concealment method: not available Blinding: triple‐blind |
| Interventions | Type of intervention: mouthwash Dosage: halita (containing 0.05% chlorhexidine, 0.05% cetylpyridinium chloride, and zinc) mouthrinse in 140 ml volume for 7‐day use (14 doses) 10 ml for 1 dose Total number of intervention groups: 1 Comparison: chlorhexidine mouthrinses (control) Duration of treatment: 7 days Duration of follow‐up: before intervention and after 7 days of intervention |
| Outcomes | OLT measurement |
| Starting date | 21 March 2014 |
| Contact information | Dr Zahra Jamali, Assistant Professor of Oral Medicine, Tabriz University of Medical Sciences, Iran Z.jamali55@gmail.com |
| Notes | Results: not available |
IRCT2015030921395N1.
| Trial name or title | Preparation and clinical trial of toothpaste containing Pistacia atlantica subsp mutica oleo‐gum resin, Punica granatum var pleniflora flowers and Eugenia caryophyllata buds for halitosis |
| Methods | Location: Shiraz University of Medical Sciences, Iran Number of centres: 1 Recruitment period (duration): 1 January 2016 to 1 January 2017 Trial design (including number of arms): double‐blind, stratified, 2‐treatment design Funding source (or sponsored drugs/materials): Shiraz University of Medical Sciences, Iran |
| Participants | Inclusion criteria: OLT score ≥ 2; tongue coating score ≥ 4; age (SD) at baseline for each arm: 18 and 65 years Exclusion criteria: smoking; alcohol; systemic disease; medicinal causing dry month; use of antibiotics in the past month; eating spicy foods, onions and garlic in the 48 hours prior to the examination; using orthodontic appliance (fixed and mobile) and mobile dentures; diabetes; metabolic disease; infections of the upper respiratory tract kidney and liver failure, chronic inflammatory diseases; surgery of the head and neck malignancies; anticoagulation therapy such as aspirin; heparin; warfarin Sample size (per group): not mentioned Number randomised: 80 adults Method of randomisation: not mentioned Allocation concealment method: not mentioned Blinding: double‐blind |
| Interventions | Intervention: toothpaste containing mastic resin, pomegranate and clove oil Dosage: 2 weeks Comparison: placebo toothpaste Time points: 2 weeks |
| Outcomes | Plaque index, bleeding index and halitosis checklist, microbial contamination of salivary and tongue coating |
| Starting date | 1 January 2016 |
| Contact information | Atefeh Arabzadeh, Shiraz University of Medical Sciences, Iran arabzade_a@sums.ac.ir |
| Notes | Registered while recruiting |
IRCT2016012026122N1.
| Trial name or title | Comparison of the effectiveness of mouthwashes containing green tea on the severity of halitosis in patients with halitosis |
| Methods | Location/setting: Isfahan University of Medical Sciences, Iran Number of centres: 1 Recruitment period (duration): 20th to 27th February 2016 Trial design (including number of arms): 2 Funding source (or sponsored drugs/materials): Vice Chancellor for Research, Isfahan University of Medical Sciences |
| Participants | Inclusion criteria: patients who complain of oral malodour; patients whose halitosis will be confirmed after clinical examination Exclusion criteria: patients who were not willing to participate in the study; female patients in their period of menstruation; smokers; those with systemic diseases Sample size (per group): 21 per group Number randomised: 42 Method of randomisation: table of random numbers Allocation concealment method: not available Blinding: double‐blind (scholars and patients) |
| Interventions | Type of intervention: mouthwash Dosage: green tea mouthwash for 1 week twice a day in intervention group Total number of intervention groups: 1 Comparison: placebo mouthwash Duration of treatment: 1 week Duration of follow‐up: before and after 1 week |
| Outcomes | OLT assessment scores: the patient will be asked to keep his/her mouth closed for 2 minutes and then exhale out the air. To determine the severity of the oral malodour, the researcher will measure the severity of the patient's halitosis from the distance of 10 cm and 50 cm, and then the severity of patient's halitosis is classified following 5 categories based on the OLT method: 0 = no smell of halitosis, 1 = low, 2 = moderate, 3 = severe, 4 = very intense smell |
| Starting date | 20 February 2016 |
| Contact information | Parichehr Behfarnia, Periodontist, Assistant Professor, Department of Periodontics, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran behfarniaa@dnt.mui.ac.ir; rnazeria@gmail.com |
| Notes | Results: not available |
ISRCTN67671859.
| Trial name or title | Assessment of oral malodour and tonsil bacteria after gargling of throat with an antiseptic |
| Methods | Location: Division of Periodontal Health Promotion, Aichi Gakuin University Dental Hospital, Japan Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): interventional and parallel Funding source (or sponsored drugs/materials): The Ministry of Education, Culture, Sports, Science and Technology, Japan |
| Participants | Inclusion criteria: those who visited Aichi Gakuin University Dental Hospital claiming oral malodour; no history of antibiotic use within the past 3 months; no history of otolaryngology consultation due to sinusitis, tonsillitis and tonsilloliths within the past 3 months Exclusion criteria: otolaryngological disease at baseline; periodontitis; to have used a gargle on the day of screening; a negative result for an OLT assessment (score 0); less than 26 ppb CH3SH in mouth air; score of more than 30% on the Plaque Control Record Sample size (per group): not mentioned Number randomised: not mentioned Method of randomisation: not mentioned Allocation concealment method: not mentioned Blinding: not mentioned |
| Interventions | Total number of intervention groups: 3 Comparison:
During the 9‐day test period, all of the participants underwent professional mechanical tooth cleaning (PMTC) every 3 days. VSC concentration in mouth air, OLT score and profile of tonsillar microbiota of halitosis patient were assessed before and after gargling with benzethonium chloride Intervention type: drug Duration of treatment: 9 days Duration of follow‐up: not mentioned |
| Outcomes | Outcomes measured at baseline and after 9 days:
|
| Starting date | 12 August 2015 |
| Contact information | Dr Mitsuo Fukuda, 2‐11 Suemori‐Dori Chikusa‐Ku, Nagoya, 464‐8651, Japan fukuda‐m@dpc.agu.ac.jp |
| Notes | Retrospectively registered |
ISRCTN74655176.
| Trial name or title | The safety and efficacy of an herbal chlorhexidine gel on bad breath caused by oral bacteria |
| Methods | Location: Periodontal Solutions (USA), 7600 S Red Rd Ste 216 Florida, South Miami, 33143, USA Number of centres: 1 Recruitment period (duration): 1 March 2018 to 28 April 2018 Trial design (including number of arms): interventional RCT Funding source (or sponsored drugs/materials): Rainforest Nutritionals Inc, 9201 Leesville Rd, Suite 120C, Raleigh, 27613 USA |
| Participants | Inclusion criteria:
Exclusion criteria:
Sample size (per group): not given Number randomised: 30 Method of randomisation: not given Allocation concealment method: not given Blinding: double‐blind |
| Interventions | Type of intervention: herbal‐chlorhexidine gel Dosage: not given Total number of intervention groups: 1 Comparison: placebo gel (flavoured gel) Duration of treatment: 7 days Duration of follow‐up: 7 days |
| Outcomes |
|
| Starting date | 1 March 2018 |
| Contact information | Paul Bobrowski, Rainforest Nutritionals Inc, 9201 Leesville Rd, Suite 120C, Raleigh 27613, USA |
| Notes | Results not available |
ISRCTN75902618.
| Trial name or title | Efficacy of 0.1% chlorine dioxide mouthwash in reducing oral malodour |
| Methods | Location: Faculty of Odonto‐Stomatology, University of Medicine and Pharmacy, Ho Chi Minh City, Vietnam Number of centres: 1 Recruitment period: February to April 2017 Study design: cross‐over, randomised, double‐blind clinical trial, wash‐out period: 4‐week wash‐out period between 2 2‐week stages Funding: University of Medicine and Pharmacy, Ho Chi Minh City, Vietnam |
| Participants | Participant inclusion criteria: 1st to 3rd year students at the University of Medicine and Pharmacy, Ho Chi Minh City who had halitosis as a chief complaint; an OLT score ≥ 2 based on the Rosenberg scale; a level of hydrogen sulphide (H2S) > 1.5 ng/10 mL or methyl mercaptan (CH3SH) > 0.5 ng/10 mL (1) determined by OralChromaTM
Target number of participants: During the study, 5 subjects were eliminated because they did not participate in the full protocol, so that the final sample was 39 participants. Participant exclusion criteria: gastrointestinal diseases or respiratory diseases; habit of smoking; wearing dentures or orthodontic appliances; undergoing any antibiotic treatment 1 month before and during the study course Sample size: 39 Number randomised: 44 Random sequence generation: not mentioned Allocation concealment: quote: "The subjects were randomised into two groups by a person who was outside the trial. This assignment was secured secretly in the patient records, and only revealed (if necessary) after the trial ended" Blinding: double‐blind |
| Interventions | Intervention: commercial mouthwash (TheraBreath® Mild Mint Oral Rinse) containing 0.1% chlorine dioxide Control: 0.9% sodium chloride solution with additional flavours to imitate the taste of the experimental oral rinse Dose: participants in both groups were instructed to use their mouthwash in the following way: rinse with 15 mL mouthwash for 30 seconds, then spit and continue to gargle with 15 mL mouthwash for 15 seconds After 4 weeks of wash‐out, in the 2nd stage, each group used the other mouthwash for 2 weeks |
| Outcomes | Primary outcome measures:
Secondary outcome measures:
|
| Starting date | 1 February 2017 |
| Contact information | Dr Thuy Pham AV, Department of Periodontology, Faculty of Odonto‐Stomatology, University of Medicine and Pharmacy, 652 Nguyen Trai St, Ward 11, District 5, Ho Chi Minh City, 700000, Vietnam |
| Notes | Trial registered retrospectively Results not yet published |
NCT02794766.
| Trial name or title | Inulin and Streptococcus salivarius reduce halitosis associated with tongue coating: a randomised clinical trial |
| Methods | Location/setting: Fernando Fornari, Universidade de Passo Fundo, Rio Grande do Sul, Brazil Number of centres: 1 Recruitment period (duration): March 2014 to May 2015 Trial design (including number of arms): 3 Funding source (or sponsored drugs/materials): Universidade de Passo Fundo, Brazil |
| Participants | Inclusion criteria:
Exclusion criteria:
Sample size (per group): 15 Number randomised: 45 Method of randomisation: not given Allocation concealment method: not given Blinding: double‐blind (participant, investigator) |
| Interventions | Intervention: inulin + Streptococcus salivarius: a gum of inulin 1 g + Streptococcus salivarius 1 billion CFU per oral; Streptococcus salivarius: a gum of Streptococcus salivarius 1 billion CFU per oral each 12 hours for 10 days Dosage: 12 hours for 10 days Total number of intervention groups: 2 Comparison: placebo: 1 gum each 12 hours for 10 days Duration of treatment: 10 days Duration of follow‐up: 10 to 14 days |
| Outcomes |
|
| Starting date | March 2014 |
| Contact information | Fernando Fornari, Universidade de Passo Fundo, Brazil |
| Notes | Results: not available |
NCT03031756.
| Trial name or title | Efficacy of glycine powder air polishing combined with scaling and root planing in the treatment of periodontitis and halitosis: a randomised clinical study |
| Methods | Location/setting: Near East University, Faculty of Dentistry, Turkey Number of centres: 1 Recruitment period (duration): January 2015 to July 2015 Trial design (including number of arms): 2 Funding source (or sponsored drugs/materials): Near East University, Turkey |
| Participants | Inclusion criteria: patients who had at least 3 teeth with 4 to 6 mm periodontal pockets; age (SD) at baseline for each arm: 28 to 68 years Exclusion criteria: acute infectious oral lesions, furcation defects, using antibiotics for any reason in the last 4 weeks, periodontal treatment in the last 6 months and pregnant or lactating patients Sample size (per group): not given Number randomised: 60 Method of randomisation: not reported Allocation concealment method: not reported Blinding: single‐blind (participant) |
| Interventions | Intervention: SRP performed using routine ultrasonic (Piezon Master 700; EMS, Nyon, Switzerland) and hand instrumentation, glycine powder air polishing (GPAP) performed for 10 seconds per surface after the instrumentation (Air‐Flows Perio Powder, EMS, Nyon, Switzerland) was applied using a Perio‐Flows hand‐piece connected to an airflow unit (Air‐Flow Masters, EMS) Dosage: not applicable Total number of intervention groups: 2 Comparison: SRP performed using routine ultrasonic (Piezon Master 700; EMS, Nyon, Switzerland) and hand instrumentation Duration of treatment: not reported Duration of follow‐up: 7, 14 and 30 days |
| Outcomes |
|
| Starting date | January 2015 |
| Contact information | Hasan Guney Yilmaz, Near East University, Turkey |
| Notes | Results: not available |
NCT03053882.
| Trial name or title | Comparative study of the effects of green tea and peppermint herbal mouthwash on halitosis |
| Methods | Location: Shahid Beheshti University of Medical Sciences, Tehran, Iran Number of centres: 1 Recruitment period (duration): January 2015 to January 2016 Trial design (including number of arms): 2 arms, cross‐over trial Funding source (or sponsored drugs/materials): Shahid Beheshti University of Medical Sciences, Iran |
| Participants | Inclusion criteria:
Exclusion criteria:
Sample size (per group): not given Number randomised: 88 Method of randomisation: not given Allocation concealment method: not given Blinding: single‐blind (investigator, outcomes assessor) |
| Interventions | Type of intervention: mouthwash containing herbal peppermint or green tea Dosage: no details given Total number of intervention groups: no details given Comparison: mouthwash containing herbal peppermint or green tea Duration of treatment: 21 days Duration of follow‐up: baseline, 7, 14 and 21 days |
| Outcomes |
|
| Starting date | January 2015 |
| Contact information | Mahin Bakhshi, Associate Professor of Oral Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran |
| Notes | Results: not available |
NCT03160573.
| Trial name or title | Efficacy of ClōSYS oral rinse products in human subjects in controlling oral malodour |
| Methods | Location/setting: University Health Resources Group, USA Number of centres: 1 Recruitment period (duration): November 2016 to February 2017 Trial design (including number of arms): in‐vivo, 8‐week, single‐centre, randomised, double‐blind (subject/investigator), cross‐over clinical study Funding source (or sponsored drugs/materials): Rowpar Pharmaceuticals, Inc |
| Participants | Inclusion criteria:
Exclusion criteria:
Sample size (per group): not given Number randomised: 100 Method of randomisation: not given Allocation concealment method: not given Blinding: double‐blind (participant, investigator) |
| Interventions | Intervention: drug: ClōSYS® unflavoured rinse; ClōSYS® flavoured rinse Dosage: 15 ml Total number of intervention groups: 2 Comparison: placebo Duration of treatment: 30 seconds, twice per day for 1 week and 2 weeks of wash‐out period Duration of follow‐up: weekly for 3 weeks |
| Outcomes | Reduction in malodour as measured by OLT score (time frame: weekly for 3 weeks) A 6‐level OLT score from 0 to 5 will be used (0 = malodour cannot be detected; 5 = very strong malodour) |
| Starting date | November 2016 |
| Contact information | Sushma Nachnani, University Health Resources Group, Inc, USA |
| Notes | Other study ID: UHRG‐RPR‐Malodour‐ADA‐2016 Results not yet published |
NCT03468595.
| Trial name or title | Clinical evaluation of some local antimicrobial agents' adjunctive effects on periodontal parameters and halitosis with subgingival ultrasonic instrumentation in periodontitis patients: a randomised clinical study |
| Methods | Location: Near East University, Turkey Number of centres: 1 Trial design: RCT Trial arms: 3 Recruitment period: March to September 2016 Funding: Near East University, Turkey |
| Participants | Inclusion criteria: 20 to 80 years old, both genders, who had periodontitis/patients undergoing periodontal treatment at the Department of Periodontology of Near East University Exclusion criteria: individuals who presented any systemic disorders which cause halitosis (diabetes mellitus, nephropathy, liver disease, gastrointestinal diseases, respiratory problems); pregnancy or lactation; individuals who had taken antibiotics over the last 6 months or permanently used any drugs; individuals who had any form of periodontal treatment within 6 months prior to the study Number randomised: 90 Sample per group: 30 Random sequence generation: not given Allocation concealment: not given Blinding: single‐blind (participant) |
| Interventions | Intervention:
Comparator: control |
| Outcomes |
|
| Starting date | March 2016 |
| Contact information | Hasan Guney Yilmaz, Near East University, Turkey |
| Notes | Other study ID number: EK‐2012‐9‐51 Results: not available |
TCTR20151109001.
| Trial name or title | Effectiveness of alcohol‐free fluoride and essential oils containing mouthrinse in controlling dental plaque, gingivitis and halitosis in pregnancy: RCT |
| Methods | Location/setting: Faculty of Dentistry, Prince of Songkla University, Thailand Number of centres: 1 Recruitment period (duration): 1 February 2016 to 1 February 2017 Trial design (including number of arms): 2 Funding source (or sponsored drugs/materials): Johnson & Johnson |
| Participants | Inclusion criteria:
Exclusion criteria:
Sample size (per group): not mentioned Number randomised: 150 Method of randomisation: not mentioned Allocation concealment method: not mentioned Blinding: single‐blind (masked roles: outcome assessor) |
| Interventions | Intervention: Arm 1: alcohol‐free fluoride and essential oils containing mouthrinse; Arm 2: alcohol‐free fluoride containing mouthrinse Dosage: rinse 10 to 15 ml of mouthrinse at bedtime for 30 seconds, no water rinse Comparison: active comparator Duration of treatment: 3 months Duration of follow‐up: 3 months |
| Outcomes | OralChroma CHM‐2 Follow‐up: baseline, 2 weeks and 3 months after baseline |
| Starting date | 1 February 2016 |
| Contact information | Jaranya Hunsrisakhun, Faculty of Dentistry, Prince of Songkla University, Hadyai, Songkhla State/Province, Thailand hjaranya@hotmail.com |
| Notes | Current status: enrolling by invitation ‐ last updated on 8 December 2016 Email sent on 16 May 2018 and study authors have replied data are in analysis stage |
UMIN000023832.
| Trial name or title | Cross‐over test for reducing oral malodour by the chewing gums containing Myrsine seguinii extracts |
| Methods | Location: Nippon Dental University School of Life Dentistry at Tokyo Department of Oral Health, Japan Number of centres: 1 Recruitment period (duration): not mentioned Trial design (including number of arms): randomised cross‐over trial Funding source (or sponsored drugs/materials): Lotte Co, Ltd, Japan |
| Participants | Inclusion criteria: normally eating 3 times daily; in the screening test, 1.5 ng or more than 1.5 ng of hydrogen sulphide in 10 mL mouth air by gas chromatography; no dental treatment now and at least 20 natural teeth; without the habit to brush the tongue during toothbrushing (it was allowed who quitted the tongue brushing during the test period); received the sufficient explanation about the purpose and the content of the study, had the consentability, volunteered to voluntarily participate in to fully understand, and agreed to the study participation in writing Exclusion criteria: smokers; suffering from diabetes mellitus, chronic nephritis, stomach disorders, lung diseases, malignant tumours, hepatitis, taking medicines; utilizing mouthwash or anti‐malodour products daily; currently participating or trying to participate in studies of other medicines or foods; at the screening test, being diagnosed with periodontitis or dental caries; wearing removable denture; taking antibiotics/antimicrobial within 1 month before the screening test; with food allergies, lactose intolerance or feeling of unwellness due to dairy products; pregnant or with the intention of pregnancy or while breastfeeding during the test; judged to be inappropriate to the test by the chief researcher because of other reasons than those mentioned Sample size (per group): not mentioned Number randomised: not mentioned Method of randomisation: not mentioned Allocation concealment method: quote: "No need to know" Blinding: not mentioned |
| Interventions |
Duration of treatment: not mentioned Duration of follow‐up: not mentioned |
| Outcomes | Concentration of VSC (hydrogen sulphide and methyl mercaptan) in the oral air, method of assessment not mentioned |
| Starting date | 31 December 2015 |
| Contact information | Ken Yaegaki, Nippon Dental University School of Life Dentistry at Tokyo, Department of Oral Health, Chiyoda‐ku, Tokyo, Japan Yaegaki‐k@tky.ndu.ac.jp |
| Notes | Unpublished as on 17 January 2018 |
CFU = colony‐forming unit; CPC = cetylpyridinium chloride; OLT = organoleptic test; ppb = parts per billion; RCT = randomised controlled trial; SD = standard deviation; SRP = scaling and root planing; T‐RFLP = terminal restriction fragment length polymorphism; VSC = volatile sulphur compounds.
Differences between protocol and review
We searched the following databases and trials registries in addition to those mentioned in the protocol:
LILACS (Latin American and Caribbean Health Science Information database);
CINAHL EBSCO (Cumulative Index to Nursing and Allied Health Literature);
the National Database of Indian Medical Journals (IndMed, indmed.nic.in/);
OpenGrey;
ISRCTN registry (www.isrctn.com);
Clinical Trials Registry ‐ India (ctri.nic.in/Clinicaltrials/login.php).
Contributions of authors
Sumanth Kumbargere Nagraj (SKN) is the contact person with the editorial base. Prashanti Eachempati (PE), Eswara Uma (EU), Vijendra Pal Singh (VPS), Noorliza Mastura Ismail (NMI) screened the titles and abstracts against the eligibility criteria. EU, SKN and PE obtained the full‐text articles of the selected titles. SKN obtained the data on ongoing and unpublished studies. SKN and NMI, EU and SKN, VPS and PE and SKN and Eby Varghese (EV) extracted the data in duplicate for the review and sought additional information about the papers. SKN and PE entered the data into Review Manager software. SKN and PE analysed and interpreted the data and would respond to the clinical comments of the peer reviewers. VPS drafted the clinical sections of the background and entered references. SKN co‐ordinated the contributions from the co‐authors and together with PE wrote the final draft of the review.
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research (NIHR), UK.
This project was supported by the NIHR, via Cochrane Infrastructure funding to Cochrane Oral Health. The views and opinions expressed are those of the authors and not necessarily those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health and Social Care.
-
Cochrane Oral Health's Global Alliance, Other.
The production of Cochrane Oral Health reviews has been supported financially by our Global Alliance since 2011 (oralhealth.cochrane.org/partnerships‐alliances). Contributors over the past year have been the American Association of Public Health Dentistry, USA; AS‐Akademie, Germany; the British Association for the Study of Community Dentistry, UK; the British Society of Paediatric Dentistry, UK; the Canadian Dental Hygienists Association, Canada; the Centre for Dental Education and Research at All India Institute of Medical Sciences, India; the National Center for Dental Hygiene Research & Practice, USA; New York University College of Dentistry, USA; NHS Education for Scotland, UK; and the Swiss Society for Endodontology, Switzerland.
Declarations of interest
There are no financial conflicts of interest and all the review authors (Sumanth Kumbargere Nagraj, Prashanti Eachempati, Eswara Uma, Vijendra Pal Singh, Noorliza Mastura Ismail, and Eby Varghese) declare that they do not have any associations with any parties who may have vested interests in the results of this Cochrane Review.
New
References
References to studies included in this review
Acar 2019 {published data only}
- Acar B, Berker E, Tan C, Ilarslan YD, Tekcicek M, Tezcan I. Effects of oral prophylaxis including tongue cleaning on halitosis and gingival inflammation in gingivitis patients ‐ a randomized controlled clinical trial. Clinical Oral Investigations 2019;23(4):1829‐36. [DOI] [PubMed] [Google Scholar]
Ademovski 2012 {published data only}
- Ademovski SE, Lingström P, Winkel E, Tangerman A, Persson GR, Renvert S. Comparison of different treatment modalities for oral halitosis. Acta Odontologica Scandinavica 2012;70(3):224‐33. [DOI] [PubMed] [Google Scholar]
- Ademovski SE, Persson GR, Winkel E, Tangerman A, Lingström P, Renvert S. The short‐term treatment effects on the microbiota at the dorsum of the tongue in intra‐oral halitosis patients ‐ a randomized clinical trial. Clinical Oral Investigations 2013;17(2):463‐73. [DOI] [PubMed] [Google Scholar]
Ademovski 2017 {published data only}
- Ademovski SE, Mårtensson C, Persson GR, Renvert S. The long‐term effect of a zinc acetate and chlorhexidine diacetate containing mouthrinse on intra‐oral halitosis ‐ a randomized clinical trial. Journal of Clinical Periodontology 2017;44(10):1010‐9. [DOI] [PubMed] [Google Scholar]
An 2011 {published data only}
- An Yb, He L, Meng Hx, Liu Tt, Yan Fh. Effect of oral rinse with Turkish gall on the clinical periodontal parameters and halitosis. Beijing Da Xue Xue Bao Yi Xue Ban [Journal of Peking University (Health Sciences)] 2011;43(1):22‐5. [PubMed] [Google Scholar]
Asokan 2011 {published data only}
- Asokan S, Kumar RS, Emmadi P, Raghuraman R, Sivakumar N. Effect of oil pulling on halitosis and microorganisms causing halitosis: a randomized controlled pilot trial. Journal of Indian Society of Pedodontics and Preventive Dentistry 2011;29(2):90‐4. [DOI] [PubMed] [Google Scholar]
Aung 2015 {published data only}
- Aung EE, Ueno M, Zaitsu T, Furukawa S, Kawaguchi Y. Effectiveness of three oral hygiene regimens on oral malodor reduction: a randomised clinical trial. Trials 2015;16:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02113137. Oral hygiene procedures on reduction of oral malodor [Effects of various oral hygiene procedures on the reduction of oral malodor in periodontally healthy patients]. clinicaltrials.gov/ct2/show/NCT02113137 (first received 14 April 2014).
Barak 2012 {published data only}
- Barak S, Katz J. The effect of Breezy candy on halitosis: a double‐blind,controlled, and randomized study. Quintessence International 2012;43(4):313‐7. [PubMed] [Google Scholar]
Borden 2002 {published data only}
- Borden LC, Chaves ES, Bowman JP, Fath BM, Hollar GL. The effect of four mouthrinses on oral malodor. Compendium of Continuing Education in Dentistry 2002;23(6):531‐6. [PubMed] [Google Scholar]
Caygur 2017 {published data only}
- Caygur A, Albaba MR, Berberoglu A, Yilmaz HG. Efficacy of glycine powder air‐polishing combined with scaling and root planing in the treatment of periodontitis and halitosis: a randomised clinical study. Journal of International Medical Research 2017;45(3):1168‐74. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dadamio 2013 {published data only}
- Dadamio J, Tournout M, Teughels W, Dekeyser C, Coucke W, Quirynen M. Efficacy of different mouthrinse formulations in reducing oral malodour: a randomized clinical trial. Journal of Clinical Periodontology 2013;40(5):505‐13. [DOI] [PubMed] [Google Scholar]
Feres 2015 {published data only}
- Feres M, Figueiredo LC, Faveri M, Guerra MC, Mateo LR, Stewart B, et al. The efficacy of two oral hygiene regimens in reducing oral malodour: a randomised clinical trial. International Dental Journal 2015;65(6):292‐302. [DOI] [PMC free article] [PubMed] [Google Scholar]
Garcia 2014 {published data only}
- Garcia MT, Silveira JO, Gargioni Filho A, Cortelli JR, Costa FO, Aquino DR, et al. Pre‐ and post‐treatment comparative levels of VSC, subgingival total bacterial load and gingival bleeding [Níveis comparativos pré‐ e pós‐tratamento de CSV, carga bacteriana total subgengival e sangramento gengival]. Periodontia 2014;24(1):24‐9. [Google Scholar]
Hu 2005 {published data only}
- Hu D, Zhang YP, Petrone M, Volpe AR, DeVizio W, Proskin HM. Clinical effectiveness of a triclosan/copolymer/sodium‐fluoride dentifrice in controlling oral malodour: a three‐week clinical trial. Compendium of Continuing Education in Dentistry 2003;24(9 Suppl):34‐41. [PubMed] [Google Scholar]
- Hu D, Zhang YP, Petrone M, Volpe AR, Devizio W, Giniger M. Clinical effectiveness of a triclosan/copolymer/sodium fluoride dentifrice in controlling oral malodor: a 3‐week clinical trial. Oral Disease 2005;11(Suppl 1):51‐3. [DOI] [PubMed] [Google Scholar]
Hu 2018 {published data only}
- Hu D, Zhang X, Zhong Y, Mateo LR, Dibart S, Delgado E. A clinical investigation of the efficacy of a dual zinc + arginine dentifrice for controlling oral malodor. Journal of Clinical Dentistry 2018;29(Spec No A):A41‐5. [PUBMED: 30620870] [PubMed] [Google Scholar]
Iha 2013 {published data only}
- Iha K, Suzuki N, Yoneda M, Takeshita T, Hirofuji T. Effect of mouth cleaning with hinokitiol‐containing gel on oral malodor: a randomized, open‐label pilot study. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2013;116(4):433‐9. [DOI] [PubMed] [Google Scholar]
Iwamura 2016 {published data only}
- ISRCTN67671859. Assessment of oral malodour and tonsil bacteria after gargling of throat with an antiseptic [Assessment of oral malodour and tonsillar microbiota after gargling in oropharynx with benzethonium chloride]. doi.org/10.1186/ISRCTN67671859 (first received 12 August 2015).
- Iwamura Y, Hayashi J, Sato T, Sato S, Murakami T, Fujimura T, et al. Assessment of oral malodor and tonsillar microbiota after gargling with benzethonium chloride. Journal of Oral Science 2016;58(1):83‐91. [DOI] [PubMed] [Google Scholar]
Kara 2008 {published data only}
- Kara C, Demir T, Orbak R, Tezel A. Effect of Nd: YAG laser irradiation on the treatment of oral malodour associated with chronic periodontitis. International Dental Journal 2008;58(3):151‐8. [DOI] [PubMed] [Google Scholar]
Kozlovsky 1996 {published data only}
- Kozlovsky A, Goldberg S, Natour I, Rogatky‐Gat A, Gelernter I, Rosenberg M. Efficacy of a 2‐phase oil: water mouthrinse in controlling oral malodor, gingivitis, and plaque. Journal of Periodontology 1996;67(6):577‐82. [DOI] [PubMed] [Google Scholar]
Lee 2018 {published data only}
- Lee S, Suprono M, Stephens J, Withers S, Li Y. Efficacy of stabilized chlorine dioxide‐based unflavored mouthwash in reducing oral malodor: an 8‐week randomized controlled study. American Journal of Dentistry 2018;31(6):309‐12. [PubMed] [Google Scholar]
Lomax 2017 {published data only}
- Lomax A, Patel S, Wang N, Kakar K, Kakar A, Bosma ML. A randomized controlled trial evaluating the efficacy of a 67% sodium bicarbonate toothpaste on gingivitis. International Journal of Dental Hygiene 2017;15(4):e35‐e41. [DOI] [PubMed] [Google Scholar]
López Jornet 2003 {published data only}
- López Jornet P, Henarejas Hernández JL, Saura Pérez M, Camacho Alonso F. Pilot study to assess effectiveness of different mouthwashes for the treatment of oral halitosis. [Efectos de los diferentes colutorios para el tratamiento de la halitosis oral]. Avances en Odontoestomatología 2003;19(6):275‐82. [Google Scholar]
Mamgain 2016 {published data only}
- Mamgain P, Kandwal A, Mamgain RK. Comparative evaluation of Triphala and Ela decoction with 0.2% chlorhexidine as mouthwash in the treatment of plaque‐induced gingivitis and halitosis: a randomised controlled clinical trial. Journal of Evidence‐Based Complementary and Alternative Medicine 2017;22(3):468‐72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Marchetti 2015 {published data only}
- Marchetti E, Tecco S, Santonico M, Vernile C, Ciciarelli D, Tarantino E, et al. Multi‐sensor approach for the monitoring of halitosis treatment via Lactobacillus brevis (CD2)‐containing lozenges ‐ a randomized, double‐blind placebo‐controlled clinical trial. Sensors (Basel, Switzerland) 2015;15(8):19583‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nakano 2017 {published data only}
- Nakano M, Wakabayashi H, Sugahara H, Odamaki T, Yamauchi K, Abe F, et al. Effects of lactoferrin and lactoperoxidase‐containing food on the oral microbiota of older individuals. Microbiology and Immunology 2017;61(10):416‐26. [PUBMED: 28881387] [DOI] [PubMed] [Google Scholar]
Navada 2008 {published data only}
- Navada R, Kumari H, Le S, Zhang J. Oral malodor reduction from a zinc‐containing toothpaste. Journal of Clinical Dentistry 2008;19(2):69‐73. [PubMed] [Google Scholar]
NCT02628938 {unpublished data only}
- NCT02628938. Effect of miswak and miswak extract on oral malodor. clinicaltrials.gov/ct2/show/NCT02628938 (first received 11 December 2015).
Niles 1999 {published data only}
- Niles HP, Vazquez J, Rustogi KN, Williams M, Gaffar A, Proskin HM. The clinical effectiveness of a dentifrice containing triclosan and a copolymer for providing long‐term control of breath odor measured chromatographically. Journal of Clinical Dentistry 1999;10(4):135‐8. [PubMed] [Google Scholar]
Nishihira 2017 {published data only}
- Nishihira J, Nishimura M, Tanaka A, Yamaguchi A, Taira T. Effects of 4‐week continuous ingestion of champignon extract on halitosis and body and fecal odor. Journal of Traditional and Complementary Medicine 2015;7(1):110‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nogueira‐Filho 2002 {published data only}
- Nogueira‐Filho GR, Duarte PM, Toledo S, Tabchoury CP, Cury JA. Effect of triclosan dentifrices on mouth volatile sulphur compounds and dental plaque trypsin‐like activity during experimental gingivitis development. Journal of Clinical Periodontology 2002;29(12):1059‐64. [DOI] [PubMed] [Google Scholar]
Nohno 2012 {published data only}
- Nohno K, Yamaga T, Kaneko N, Miyazaki H. Tablets containing a cysteine protease, actinidine, reduce oral malodor: a crossover study. Journal of Breath Research 2012;6(1):017107. [DOI] [PubMed] [Google Scholar]
Patil 2017 {published data only}
- CTRI/2012/05/002695. G32 (Ayurvedic drug) ‐ an affordable alternative to chlorhexidine in treating bad breath [Evaluation of the efficacy of G32 (commercially available Ayurvedic preparation) in reducing halitosis as compared to chlorhexidine]. ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=4667&EncHid=&userName=G32 (first received 25 May 2012).
- Patil S, Acharya S, Hathiwala S, Singhal DK, Srinivasan SR, Khatri S. Evaluation of the efficacy of G32 (commercially available Ayurvedic preparation) in reducing halitosis ‐ a randomized controlled trial. Journal of Clinical and Diagnostic Research 2017;11(9):ZC79‐ZC83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Payne 2011 {published data only}
- Payne D, Gordon JJ, Nisbet S, Karwal R, Bosma ML. A randomised clinical trial to assess control of oral malodour by a novel dentifrice containing 0.1% w/w o‐cymen‐5‐ol, 0.6% w/w zinc chloride. International Dental Journal 2011;61 Suppl 3:60‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rassameemasmaung 2007 {published data only}
- Rassameemasmaung S, Sirikulsathean A, Amornchat C, Hirunrat K, Rojanapanthu P, Gritsanapan W. Effects of herbal mouthwash containing the pericarp extract of Garcinia mangostana L on halitosis, plaque and papillary bleeding index. Journal of the International Academy of Periodontology 2007;9(1):19‐25. [PubMed] [Google Scholar]
Rassameemasmaung 2012 {published data only}
- NCT00932347. Effect of mouthwash containing camellia sinensis extracts on oral malodor [Effect of mouthwash containing camellia sinensis extracts on oral malodor, plaque and papillary bleeding indices in gingivitis patients]. clinicaltrials.gov/ct2/show/NCT00932347 (first received 3 July 2009).
- Rassameemasmaung S, Phusudsawang P, Sangalungkarn V. Effect of green tea mouthwash on oral malodor. ISRN Preventive Medicine 2012;2013:975148. [DOI: 10.5402/2013/975148] [DOI] [PMC free article] [PubMed] [Google Scholar]
Satthanakul 2014 {published data only}
- Satthanakul P, Taweechaisupapong S, Paphangkorakit J, Pesee M, Timabut P, Khunkitti W. Antimicrobial effect of lemongrass oil against oral malodour micro‐organisms and the pilot study of safety and efficacy of lemongrass mouthrinse on oral malodour. Journal of Applied Microbiology 2015;118(1):11‐7. [DOI] [PubMed] [Google Scholar]
Suzuki 2014 {published data only}
- Suzuki N, Yoneda M, Tanabe K, Fujimoto A, Iha K, Seno K, et al. Lactobacillus salivarius WB21‐containing tablets for the treatment of oral malodor: a double‐blind, randomized, placebo‐controlled crossover trial. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2014;117(4):462‐70. [DOI] [PubMed] [Google Scholar]
- Suzuki N, Yoneda M, Tanabe K, Fujimoto A, Iha K, Seno K, et al. Lactobacillus salivarius WB21‐containing tablets for the treatment of oral malodor: a double‐blind, randomized, placebo‐controlled crossover trial ‐ reply to letter. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2014;118(4):506. [DOI] [PubMed] [Google Scholar]
Talebian 2009 {published data only}
- Talebian A, Doosti M, Tazhibi M, Iranpoor R, Namazi G, Khonakdar A. Comparative effects of selected mouthwashes on halitosis using sulphide monitoring devise [sic]. Journal of Islamic Dental Association of Iran 2009;20(4):335‐42. [Google Scholar]
Tanaka 2010 {published data only}
- Tanaka M, Toe M, Nagata H, Ojima M, Kuboniwa M, Shimizu K, et al. Effect of eucalyptus‐extract chewing gum on oral malodor: a double‐masked, randomized trial. Journal of Periodontology 2010;81(11):1564‐71. [DOI] [PubMed] [Google Scholar]
Wang 2017 {published data only}
- Wang J, He L. Effect of mechanical self‐cleaning of tongue coating on malodor in halitosis patients originating from tongue coating. Beijing Da Xue Xue Bao YiXue Ban [Journal of Peking University (Health Sciences)] 2017;49(2):344‐8. [PubMed] [Google Scholar]
Watanabe 2018 {published data only}
- UMIN000018305. Effects of Pycnogenol chewing gum on oral malodor, gingivitis and plaque formation. upload.umin.ac.jp/cgi‐open‐bin/ctr_e/ctr_view.cgi?recptno=R000021186 (first received 14 July 2015).
- Watanabe Hiramine H, Toyama T, Hamada N. Effects of French pine bark extract chewing gum on oral malodor and salivary bacteria. Journal of Nutritional Science and Vitaminology 2018;64(3):185‐91. [DOI] [PubMed] [Google Scholar]
Wigger‐Alberti 2010 {published data only}
- NCT01747226. Effect of mouth rinses in oral malodor (MR2012) [Masking and therapeutic effect of different mouth rinses in patients with oral malodor]. clinicaltrials.gov/ct2/show/NCT01747226 (first received 11 December 2012).
- Wigger‐Alberti W, Gysen K, Axmann EM, Wilhelm KP. Efficacy of a new mouthrinse formulation on the reduction of oral malodour in vivo. A randomized, double‐blind, placebo‐controlled, 3 week clinical study. Journal of Breath Research 2010;4(1):017102. [DOI] [PubMed] [Google Scholar]
Wilhelm 2012 {published data only}
- Wilhelm D, Himmelmann A, Axmann EM, Wilhelm KP. Clinical efficacy of a new tooth and tongue gel applied with a tongue cleaner in reducing oral halitosis. Quintessence International 2012;43(8):709‐18. [PubMed] [Google Scholar]
Winkel 2003 {published data only}
- Roldán S, Winkel EG, Herrera D, Sanz M, Winkelhoff AJ. The effects of a new mouthrinse containing chlorhexidine, cetylpyridinium chloride and zinc lactate on the microflora of oral halitosis patients: a dual‐centre, double‐blind placebo‐controlled study. Journal of Clinical Periodontology 2003;30(5):427‐34. [DOI] [PubMed] [Google Scholar]
- Winkel EG, Roldán S, Winkelhoff AJ, Herrera D, Sanz M. Clinical effects of a new mouthrinse containing chlorhexidine, cetylpyridinium chloride and zinc‐lactate on oral halitosis. A dual‐center, double‐blind placebo‐controlled study. Journal of Clinical Periodontology 2003;30(4):300‐6. [DOI] [PubMed] [Google Scholar]
Wirthlin 2011 {published data only}
- NCT00867035. Bad breath response to tongue scraper and rinses [Bad breath response to tongue scraper and rinses, a double‐blind, randomized, parallel group clinical trial]. clinicaltrials.gov/ct2/show/NCT00867035 (first received 23 March 2009).
- Wirthlin MR, Im T, Ellis RR, Hoover CI. Effect of tongue scraper and rinses on bad breath, a double‐blind, randomized, parallel group clinical trial. Journal of the Western Society of Periodontology/Periodontal Abstracts 2011;59(3):67‐73. [PubMed] [Google Scholar]
References to studies excluded from this review
Ademovski 2016 {published data only}
- Erovic Ademovski S, Lingström P, Renvert S. The effect of different mouth rinse products on intra‐oral halitosis. International Journal of Dental Hygiene 2016;14(2):117‐23. [DOI] [PubMed] [Google Scholar]
Alqumber 2014 {published data only}
- Alqumber MA, Arafa KA. Site‐specific mouth rinsing can improve oral odor by altering bacterial counts. Blind crossover clinical study. Saudi Medical Journal 2014;35(11):1412‐6. [PMC free article] [PubMed] [Google Scholar]
Badanjak 2016 {published data only}
- Badanjak SM, Boyd LD, Perry KR, LaSpina LM, Rothman AT, Byrne L. Efficacy of sodium chlorite + zinc gluconate on volatile sulfur compound halitosis: a randomized, double‐blind, placebo‐controlled pilot study. Canadian Journal of Dental Hygiene 2016;50(3):116‐25. [Google Scholar]
Betsy 2014 {published data only}
- Betsy J, Prasanth CS, Baiju KV, Prasanthila J, Subhash N. Efficacy of antimicrobial photodynamic therapy in the management of chronic periodontitis: a randomized controlled clinical trial. Journal of Clinical Periodontology 2014;41(6):573‐81. [PUBMED: 24617449] [DOI] [PubMed] [Google Scholar]
- Betsy J, Prasanth CS, Baiju KV, Presanthila J, Subhash N. Patients' perceptions of antimicrobial photodynamic therapy in the management of chronic periodontitis. Photodiagnosis and Photodynamic Therapy 2016;14:84‐90. [DOI] [PubMed] [Google Scholar]
Bordas 2008 {published data only}
- Bordas A, McNab R, Staples AM, Bowman J, Kanapka J, Bosma MP. Impact of different tongue cleaning methods on the bacterial load of the tongue dorsum. Archives of Oral Biology 2008;53 Suppl 1:S13‐8. [DOI] [PubMed] [Google Scholar]
Boulware 1984 {published data only}
- Boulware RT, Southard GL. Sanguinarine in the control of volatile sulfur compounds in the mouth: a comparative study. Compendium of Continuing Education in Dentistry 1984;Suppl 5:S61‐4. [PubMed] [Google Scholar]
Brunette 1998 {published data only}
- Brunette DM, Proskin HM, Nelson BJ. The effects of dentifrice systems on oral malodor. Journal of Clinical Dentistry 1998;9(3):76‐82. [PubMed] [Google Scholar]
Carvalho 2004 {published data only}
- Carvalho MD, Tabchoury CM, Cury JA, Toledo S, Nogueira‐Filho GR. Impact of mouthrinses on morning bad breath in healthy subjects. Journal of Clinical Periodontology 2004;31(2):85‐90. [DOI] [PubMed] [Google Scholar]
Chen 2010 {published data only}
- Chen X, He T, Sun L, Zhang Y, Feng X. A randomized cross‐over clinical trial to evaluate the effect of a 0.454% stannous fluoride dentifrice on the reduction of oral malodor. American Journal of Dentistry 2010;23(3):175‐8. [PubMed] [Google Scholar]
Codipilly 2004 {published data only}
- Codipilly DP, Kaufman HW, Kleinberg I. Use of a novel group of oral malodor measurements to evaluate an anti‐oral malodor mouthrinse (TriOralTM) in humans. Journal of Clinical Dentistry 2004;15(4):98‐104. [PubMed] [Google Scholar]
Conceição 2008 {published data only}
- Conceição MD, Marocchio LS, Tárzia O. Evaluation of a new mouthwash on caseous formation. Revista Brasileira de Otorrinolaringologia [Brazilian Journal of Otorhinolaryngology] 2008;74(1):61‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dereci 2016 {published data only}
- Dereci Ö, Hatipoğlu M, Sindel A, Tozoğlu S, Üstün K. The efficacy of Er,Cr:YSGG laser supported periodontal therapy on the reduction of periodontal disease related oral malodor: a randomized clinical study. Head and Face Medicine 2016;12(1):20. [DOI] [PMC free article] [PubMed] [Google Scholar]
DRKS00005334 {published data only}
- DRKS00005334. Double‐blind, controlled, randomised, three‐fold cross‐over study to investigate the efficacy of two different mouthwashes in patients with intra‐oral halitosis. www.drks.de/DRKS00005334 (first received 17 October 2013).
EUCTR 2007‐003756‐11 {published data only}
- EUCTR 2007‐003756‐11. Treatment for GUT‐caused halitosis with with E. coli strain Nissle 1917. www.clinicaltrialsregister.eu/ctr‐search/trial/2007‐003756‐11/DE (first received 17 June 2008).
Farrell 2006 {published data only}
- Farrell S, Baker RA, Somogyi‐Mann M, Witt JJ, Gerlach RW. Oral malodor reduction by a combination of chemotherapeutical and mechanical treatments. Clinical Oral Investigations 2006;10(2):157‐63. [DOI] [PubMed] [Google Scholar]
Farrell 2007 {published data only}
- Farrell S, Barker ML, Gerlach RW. Overnight malodor effect with a 0.454% stabilized stannous fluoride sodium hexametaphosphate dentifrice. Compendium of Continuing Education in Dentistry 2007;28(12):658‐61. [PubMed] [Google Scholar]
Farrell 2008 {published data only}
- Farrell S, Barker ML, Walanski A, Gerlach RW. Short‐term effects of a combination product night‐time therapeutic regimen on breath malodor. Journal of Contemporary Dental Practice 2008;9(6):1‐8. [PubMed] [Google Scholar]
Faveri 2006 {published data only}
- Faveri M, Hayacibara MF, Pupio GC, Cury JA, Tsuzuki CO, Hayacibara RM. A cross‐over study on the effect of various therapeutic approaches to morning breath odour. Journal of Clinical Periodontology 2006;33(8):555‐60. [DOI] [PubMed] [Google Scholar]
Feng 2010 {published data only}
- Feng X, Chen X, Cheng R, Sun L, Zhang Y, He T. Breath malodor reduction with use of a stannous‐containing sodium fluoride dentifrice: a meta‐analysis of four randomized and controlled clinical trials. American Journal of Dentistry 2010;23 Spec No B:27B‐31B. [PubMed] [Google Scholar]
Fine 2005 {published data only}
- Fine DH, Furgang D, Sinatra K, Charles C, McGuire A, Kumar LD. In vivo antimicrobial effectiveness of an essential oil‐containing mouthrinse 12 h after a single use and 14 days' use. Journal of Clinical Periodontology 2005;32(4):335‐40. [DOI] [PubMed] [Google Scholar]
Frascella 1998 {published data only}
- Frascella J, Gilbert R, Fernandez P. Odor reduction potential of a chlorine dioxide mouthrinse. Journal of Clinical Dentistry 1998;9(2):39‐42. [PubMed] [Google Scholar]
Frascella 2000 {published data only}
- Frascella J, Gilbert RD, Fernandez P, Hendler J. Efficacy of a chlorine dioxide‐containing mouthrinse in oral malodor. Compendium of Continuing Education in Dentistry 2000;21(3):241‐4. [PubMed] [Google Scholar]
Gerlach 1998 {published data only}
- Gerlach RW, Hyde JD, Poore CL, Stevens DP, Witt JJ. Breath effects of three marketed dentifrices: a comparative study evaluating single and cumulative use. Journal of Clinical Dentistry 1998;9(4):83‐8. [PubMed] [Google Scholar]
Greenstein 1997 {published data only}
- Greenstein RB, Goldberg S, Marku‐Cohen S, Sterer N, Rosenberg M. Reduction of oral malodor by oxidizing lozenges. Journal of Periodontology 1997;68(12):1176‐81. [DOI] [PubMed] [Google Scholar]
Haas 2007 {published data only}
- Haas AN, Silveira EM, Rösing CK. Effect of tongue cleansing on morning oral malodour in periodontally healthy individuals. Oral Health & Preventive Dentistry 2007;5(2):89‐94. [PUBMED: 17722433] [PubMed] [Google Scholar]
Hu 2013 {published data only}
- Hu D, Li X, Yin W, DeVizio W, Mateo LR, Dibart S, et al. Clinical investigation of oral malodor during long‐term use of arginine‐containing dentifrices. American Journal of Dentistry 2013;26(6):329‐34. [PubMed] [Google Scholar]
Katsinelos 2007 {published data only}
- Katsinelos P, Tziomalos K, Chatzimavroudis G, Vasiliadis T, Katsinelos T, Pilpilidis I, et al. Eradication therapy in Helicobacter pylori‐positive patients with halitosis: long‐term outcome. Medical Principles and Practice 2007;16(2):119‐23. [DOI] [PubMed] [Google Scholar]
Keller 2012 {published data only}
- Keller MK, Bardow A, Jensdottir T, Lykkeaa J, Twetman S. Effect of chewing gums containing the probiotic bacterium Lactobacillus reuteri on oral malodour. Acta Odontologica Scandinavica 2012;70(3):246‐50. [DOI] [PubMed] [Google Scholar]
Leal 2019 {published data only}
- Leal MB, Goes JS, Dellovo AG, Sao Mateus CR, Macedo GO. Effect of polyethylene terephthalate tongue scraper on oral levels of volatile sulfur compounds: a randomized clinical trial. Brazilian Dental Science 2019;22(1):31‐8. [Google Scholar]
Lodhia 2008 {published data only}
- Lodhia P, Yaegaki K, Khakbaznejad A, Imai T, Sato T, Tanaka T, et al. Effect of green tea on volatile sulfur compounds in mouth air. Journal of Nutritional Science and Vitaminology 2008;54(1):89‐94. [PUBMED: 18388413] [DOI] [PubMed] [Google Scholar]
Malhotra 2011a {published data only}
- Malhotra R, Grover V, Kapoor A, Saxena D. Comparison of the effectiveness of a commercially available herbal mouthrinse with chlorhexidine gluconate at the clinical and patient level. Journal of Indian Society of Periodontology 2011;15(4):349‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mendes 2016 {published data only}
- Mendes L, Coimbra J, Pereira AL, Resende M, Pinto MG. Comparative effect of a new mouthrinse containing chlorhexidine, triclosan and zinc on volatile sulphur compounds: a randomized, crossover, double‐blind study. International Journal of Dental Hygiene 2016;14(3):202‐8. [DOI] [PubMed] [Google Scholar]
Moreno 2005 {published data only}
- Moreno T, Haas AN, Castro GD, Winter R, Oppermann RV, Rosing CK. Treatment of aggressive periodontitis and alterations on volatile sulfur compounds. Revista Odonto Ciência – Faculdade de Odontologia 2005;20(49):217‐21. [Google Scholar]
Mousquer 2017 {published data only}
- Mousquer CR, Thomé BB, Iserhard WB, Callegari‐Jacques SM, Bona AD, Venturini AP, et al. Inulin and Streptococcus salivarius reduce halitosis associated with tongue coating: a randomized clinical trial. Gastroenterology 2017;152(5 Suppl 1):S815. [Google Scholar]
Nakano 2016 {published data only}
- Nakano M, Shimizu E, Wakabayashi H, Yamauchi K, Abe F. A randomized, double‐blind, crossover, placebo‐controlled clinical trial to assess effects of the single ingestion of a tablet containing lactoferrin, lactoperoxidase, and glucose oxidase on oral malodor. BMC Oral Health 2016;16:37. [PUBMED: 27001471] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT00250289 {published data only}
- NCT00250289. Prevention of oral malodor with an oral sticker containing herbal formula [Invivo study of the efficacy of an innovative herbal formula and delivery system on oral malodor]. clinicaltrials.gov/show/NCT00250289 (first received 8 November 2005).
NCT00655772 {published data only}
- NCT00655772. A clinical trial to assess the effects of a mouthwash containing chlorine dioxide on oral malodor [A randomized, double blind, crossover, placebo‐controlled clinical trial to assess the effects of a mouthwash containing chlorine dioxide on oral malodor]. clinicaltrials.gov/show/NCT00655772 (first received 10 April 2008). [DOI] [PMC free article] [PubMed]
NCT00748943 {published data only}
- NCT00748943. Clinical and microbiological effects of a mouthwash containing chlorine dioxide [The clinical effects of a mouthwash containing chlorine dioxide on oral malodor and salivary periodontal and malodorous bacteria using for 7 days]. clinicaltrials.gov/show/NCT00748943 (first received 9 September 2008).
NCT00875927 {published data only}
- NCT00875927. Effects of Breezy candy on halitosis [Breezy candy halitosis study]. clinicaltrials.gov/show/NCT00875927 (first received 6 April 2009).
NCT02194621 {published data only}
- NCT02194621. Clinical investigation to examine toothpaste effect on oral bacteria [A randomized, single center, three cell, double blind and parallel groups clinical study conducted in Newark, NJ to evaluate the antibacterial effects of two toothpastes containing 0.3% Triclosan/2% copolymer/0.243% sodium fluoride in a silica base as compared to a control regular fluoride toothpaste on oral bacteria 12 hours after 13 days product use]. clinicaltrials.gov/show/NCT02194621 (first received 18 July 2014).
NCT02789436 {published data only}
- NCT02789436. Effect of probiotic lozenges on halitosis in patients with chronic periodontitis [Effect of probiotic Lactobacillus reuteri‐containing lozenges (Prodentis) on halitosis in patients with chronic periodontitis]. clinicaltrials.gov/ct2/show/NCT02789436 (first received 3 June 2016).
NCT03346460 {published data only}
- NCT03346460. Effect of photodymamic therapy with urucum and LED in the reduction of halitosis [Effect of photodymamic therapy with urucum and LED in the reduction of halitosis: a clinical and microbiological trial]. clinicaltrials.gov/ct2/show/NCT03346460 (first received 17 November 2017).
NCT03591484 {published data only}
- NCT03591484. Treatment of halitosis with photodynamic therapy in older patients [Treatment of halitosis with photodynamic therapy in older patients: protocol for a randomized, controlled trial]. clinicaltrials.gov/ct2/show/record/NCT03591484 (first received 19 July 2018).
NCT03656419 {published data only}
- NCT03656419. Photodynamic therapy with red leds in microorganisms related to halitosis [Action of antimicrobial photodynamic therapy with red leds in microorganisms related to halitose: clinical controlled and randomized trial]. clinicaltrials.gov/ct2/show/NCT03656419 (first received 3 September 2018).
Newby 2008 {published data only}
- Newby EE, Hickling JM, Hughes FJ, Proskin HM, Bosma MP. Control of oral malodour by dentifrices measured by gas chromatography. Archives of Oral Biology 2008;53 Suppl 1:S19‐25. [DOI] [PubMed] [Google Scholar]
NL3100 (NTR3240) {published data only}
- NL3100 (NTR3240). The effect of chemotherapeutic agents and mechanical tongue cleaning on morning bad breath. trialregister.nl/trial/3100 (first received 17 January 2012).
Pedrazzi 2004 {published data only}
- Pedrazzi V, Sato S, Mattos Mda G, Lara EH, Panzeri H. Tongue‐cleaning methods: a comparative clinical trial employing a toothbrush and a tongue scraper. Journal of Periodontology 2004;75(7):1009‐12. [DOI] [PubMed] [Google Scholar]
Penala 2016 {published data only}
- Penala S, Kalakonda B, Pathakota KR, Jayakumar A, Koppolu P, Bolla VL, et al. Efficacy of local use of probiotics as an adjunct to scaling and root planing in chronic periodontitis and halitosis: a randomized controlled trial. Journal of Research in Pharmacy Practice 2016;5(2):86‐93. [DOI] [PMC free article] [PubMed] [Google Scholar]
Peruzzo 2007 {published data only}
- Peruzzo DC, Jandiroba PF, Nogueira Filho Gda R. Use of 0.1% chlorine dioxide to inhibit the formation of morning volatile sulphur compounds (VSC). Brazilian Oral Research 2007;21(1):70‐4. [DOI] [PubMed] [Google Scholar]
Peruzzo 2008 {published data only}
- Peruzzo DC, Salvador SL, Sallum AW, Nogueira‐Filho Gda R. Flavoring agents present in a dentifrice can modify volatile sulphur compounds (VSCs) formation in morning bad breath. Brazilian Oral Research 2008;22(3):252‐7. [DOI] [PubMed] [Google Scholar]
Pitts 1981 {published data only}
- Pitts G, Pianotti R, Feary TW, McGuiness J, Masurat T. The in vivo effects of an antiseptic mouthwash on odor‐producing microorganisms. Journal of Dental Research 1981;60(11):1891‐6. [PUBMED: 6945328] [DOI] [PubMed] [Google Scholar]
Polat 2008 {published data only}
- Polat HB, Ozdemir H, Ay S. Effect of different mouthrinses on third molar surgery‐related oral malodor. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 2008;105(3):e1‐8. [DOI] [PubMed] [Google Scholar]
Porciani 2012 {published data only}
- Porciani PF, Franciosi G, Grandini S. Effect of zinc and magnolia tablets on oral VSC. IADR, 2013 Continental European Division Meeting (Florence, Italy): 583.
- Porciani PF, Grandini S. The effect of zinc acetate and magnolia bark extract added to chewing gum on volatile sulfur‐containing compounds in the oral cavity. Journal of Clinical Dentistry 2012;23(3):76‐9. [PUBMED: 23210417] [PubMed] [Google Scholar]
Quirynen 2002 {published data only}
- Quirynen M, Avontroodt P, Soers C, Zhao H, Pauwels M, Coucke W, et al. The efficacy of amine fluoride/stannous fluoride in the suppression of morning breath odour. Journal of Clinical Periodontology 2002;29(10):944‐54. [DOI] [PubMed] [Google Scholar]
Quirynen 2004 {published data only}
- Quirynen M, Avontroodt P, Soers C, Zhao H, Pauwels M, Steenberghe D. Impact of tongue cleansers on microbial load and taste. Journal of Clinical Periodontology 2004;31(7):506‐10. [DOI] [PubMed] [Google Scholar]
Quirynen 2005 {published data only}
- Quirynen M, Zhao H, Soers C, Dekeyser C, Pauwels M, Coucke W, et al. The impact of periodontal therapy and the adjunctive effect of antiseptics on breath odor‐related outcome variables: a double‐blind randomized study. Journal of Periodontology 2005;76(5):705‐12. [DOI] [PubMed] [Google Scholar]
Reingewirtz 1999 {published data only}
- Reingewirtz Y, Girault O, Reingewirtz N, Senger B, Tenenbaum H. Mechanical effects and volatile sulfur compound‐reducing effects of chewing gums: comparison between test and base gums and a control group. Quintessence International 1999;30(5):319‐23. [PubMed] [Google Scholar]
Roldán 2004 {published data only}
- Roldán S, Herrera D, Santa‐Cruz I, O'Connor A, González I, Sanz M. Comparative effects of different chlorhexidine mouth‐rinse formulations on volatile sulphur compounds and salivary bacterial counts. Journal of Clinical Periodontology 2004;31(12):1128–34. [DOI] [PubMed] [Google Scholar]
Rolla 2002 {published data only}
- Rolla G, Jonski G, Young A. The significance of the source of zinc and its anti‐VSC effect. International Dental Journal 2002;52 Suppl 3:233‐5. [DOI] [PubMed] [Google Scholar]
Rosenberg 1992 {published data only}
- Rosenberg M, Gelernter I, Barki M, Bar‐Ness R. Day‐long reduction of oral malodor by a two‐phase oil:water mouthrinse as compared to chlorhexidine and placebo rinses. Journal of Periodontology 1992;63(1):39‐43. [DOI] [PubMed] [Google Scholar]
Rosing 2009 {published data only}
- Rosing CK, Gomes SC, Bassani DG, Oppermann RV. Effect of chewing gums on the production of volatile sulfur compounds (VSC) in vivo. Acta Odontologica Latinoamericana 2009;22(1):11‐4. [PUBMED: 19601490] [PubMed] [Google Scholar]
Saad 2011 {published data only}
- Saad S, Greenman J, Shaw H. Comparative effects of various commercially available mouthrinse formulations on oral malodor. Oral Diseases 2011;17(2):180‐6. [DOI] [PubMed] [Google Scholar]
Saad 2016 {published data only}
- ISRCTN38199132. Breath freshening effects of mechanical removal of tongue biofilm [Clinical study on the breath freshening effects of mechanical removal of tongue biofilm used with oral formulations]. isrctn.com/ISRCTN38199132 (first received 14 December 2015).
- Saad S, Gomez‐Pereira P, Hewett K, Horstman P, Patel J, Greenman J. Daily reduction of oral malodor with the use of a sonic tongue brush combined with an antibacterial tongue spray in a randomized cross‐over clinical investigation. Journal of Breath Research 2016;10(1):016013. [PUBMED: 26869586] [DOI] [PubMed] [Google Scholar]
Schmidt 1978 {published data only}
- Schmidt NF, Tarbet WJ. The effect of oral rinses on organoleptic mouth odor ratings and levels of volatile sulfur compounds. Oral Surgery, Oral Medicine, and Oral Pathology 1978;45(6):876‐83. [DOI] [PubMed] [Google Scholar]
Seemann 2001 {published data only}
- Seemann R, Kison A, Bizhang M, Zimmer S. Effectiveness of mechanical tongue cleaning on oral levels of volatile sulfur compounds. Journal of the American Dental Association 2001;132(9):1263‐7. [DOI] [PubMed] [Google Scholar]
Seemann 2001a {published data only}
- Seemann R, Passek G, Zimmer S, Roulet JF. The effect of an oral hygiene program on oral levels of volatile sulfur compounds (VSC). Journal of Clinical Dentistry 2001;12(4):104‐7. [PubMed] [Google Scholar]
Sharma 1999 {published data only}
- Sharma NC, Galustians HJ, Qaquish J, Galustians A, Rustogi KN, Petrone ME, et al. The clinical effectiveness of a dentifrice containing triclosan and a copolymer for controlling breath odor measured organoleptically twelve hours after toothbrushing. Journal of Clinical Dentistry 1999;10(4):131‐4. [PubMed] [Google Scholar]
Sharma 2007 {published data only}
- Sharma NC, Galustians HJ, Qaqish J, Galustians A, Rustogi K, Petrone ME, et al. Clinical effectiveness of a dentifrice containing triclosan and a copolymer for controlling breath odor. American Journal of Dentistry 2007;20(2):79‐82. [PubMed] [Google Scholar]
Sheikh 2016 {published data only}
- Sheikh FS, Iyer RR. The effect of oil pulling with rice bran oil, sesame oil, and chlorhexidine mouth rinsing on halitosis among pregnant women: a comparative interventional study. Indian Journal of Dental Research 2016;27(5):508‐12. [DOI] [PubMed] [Google Scholar]
Shin 2011 {published data only}
- Shin K, Yaegaki K, Murata T, Ii H, Tanaka T, Aoyama I, et al. Effects of a composition containing lactoferrin and lactoperoxidase on oral malodor and salivary bacteria: a randomized, double‐blind, crossover, placebo‐controlled clinical trial. Clinical Oral Investigations 2011;15(4):485‐93. [DOI] [PubMed] [Google Scholar]
Shinada 2008 {published data only}
- Shinada K, Ueno M, Konishi C, Takehara S, Yokoyama S, Kawaguchi Y. A randomized double blind crossover placebo‐controlled clinical trial to assess the effects of a mouthwash containing chlorine dioxide on oral malodor. Trials 2008;9:71. [PUBMED: 19068114] [DOI] [PMC free article] [PubMed] [Google Scholar]
Shinada 2010 {published data only}
- Shinada K, Ueno M, Konishi C, Takehara S, Yokoyama S, Zaitsu T, et al. Effects of a mouthwash with chlorine dioxide on oral malodor and salivary bacteria: a randomized placebo‐controlled 7‐day trial. Trials 2010;11:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Silveira 2014 {published data only}
- Silveira JO. Effect of Full‐Mouth Disinfection and Quadrant Root Scraping and Smoothing Techniques on Halitosis in Individuals with Advanced Chronic Periodontitis: a Randomized Controlled Trial [Efeito das Técnicas de Full‐Mouth Disinfection e Raspagem e Alisamento Radicular por Quadrante na Halitose em Indivíduos com Periodontite Crônica Avançada: Ensaio Clínico Randomizado Controlado] [Masters thesis]. Minas Gerais (Brazil): Federal University of Minas Gerais, 2014. [Google Scholar]
Silveria 2017 {published data only}
- NCT02368678. Study of halitosis in patients with advanced chronic periodontitis (HACP) [Effect of full mouth disinfection and scaling root planing per quadrant in halitosis in patients with advanced chronic periodontitis: randomized clinical controlled trial]. clinicaltrials.gov/ct2/show/NCT02368678 (first received 23 February 2015).
- Silveira JO, Costa FO, Oliveira PAD, Dutra BC, Cortelli SC, Cortelli JR, et al. Effect of non‐surgical periodontal treatment by full‐mouth disinfection or scaling and root planing per quadrant in halitosis‐a randomized controlled clinical trial. Clinical Oral Investigations 2017;21(5):1545‐52. [DOI] [PubMed] [Google Scholar]
Soares 2015 {published data only}
- Soares LG, Jonski G, Tinoco EM, Young A. Short‐term effect of strontium‐ and zinc‐containing toothpastes and mouthrinses on volatile sulphur compounds in morning breath: a randomized, double‐blind, cross‐over clinical study. European Journal of Oral Sciences 2015;123(2):72‐9. [DOI] [PubMed] [Google Scholar]
Soares 2015a {published data only}
- G Soares L, Castagna L, C Weyne S, G Silva D, EV Falabella M, MB Tinoco E. Effectiveness of full‐ and partial‐mouth disinfection on halitosis in periodontal patients. Journal of Oral Science 2015;57(1):1‐6. [PUBMED: 25807902] [DOI] [PubMed] [Google Scholar]
Sreenivasan 2003 {published data only}
- Sreenivasan P. The effects of a triclosan/copolymer dentifrice on oral bacteria including those producing hydrogen sulfide. European Journal of Oral Sciences 2003;111(3):223‐7. [DOI] [PubMed] [Google Scholar]
Sreenivasan 2004 {published data only}
- Sreenivasan PK, Gittins E. The effects of a chlorhexidine mouthrinse on culturable microorganisms of the tongue and saliva. Microbiological Research 2004;159(4):365‐70. [DOI] [PubMed] [Google Scholar]
Steenberghe 2001 {published data only}
- Steenberghe D, Avontroodt P, Peeters W, Pauwels M, Coucke W, Lijnen A, et al. Effect of different mouthrinses on morning breath. Journal of Periodontology 2001;72(9):1183‐91. [DOI] [PubMed] [Google Scholar]
Sterer 2008 {published data only}
- Sterer N, Nuas S, Mizrahi B, Goldenberg C, Weiss EI, Domb A, et al. Oral malodor reduction by a palatal muco‐adhesive tablet containing herbal formulation. Journal of Dentistry 2008;36(7):535‐9. [DOI] [PubMed] [Google Scholar]
Sterer 2013 {published data only}
- Sterer N, Ovadia O, Weiss EI, Perez Davidi M. Day‐long reduction of oral malodor by a palatal muco‐adhesive tablet containing herbal formulation. Journal of Breath Research 2013;7(2):026004. [DOI] [PubMed] [Google Scholar]
Tamaki 2007 {published data only}
- Tamaki K, Tamaki T, Yamazaki T. Studies on the deodorization by mushroom (Agaricus bisporus) extract of garlic extract‐induced oral malodor. Journal of Nutritional Science and Vitaminology (Tokyo) 2007;53(3):277‐86. [DOI] [PubMed] [Google Scholar]
Thaweboon 2011 {published data only}
- Thaweboon S, Thaweboon B. Effect of an essential oil‐containing mouthrinse on VSC‐producing bacteria on the tongue. Southeast Asian Journal of Tropical Medicine and Public Health 2011;42(2):456‐62. [PubMed] [Google Scholar]
Thrane 2010 {published data only}
- Thrane P, Jonski G, Young A, Rolla G. Beating bad breath with zinc and chlorhexidine. Dental Practice 2010;48(11):14‐6. [Google Scholar]
Tian 2013 {published data only}
- Tian M, Hanley AB, Dodds MW, Yaegaki K. Chewing gum containing allyl isothiocyanate from mustard seed extract is effective in reducing volatile sulfur compounds responsible for oral malodor. American Journal of Dentistry 2013;26(4):180‐4. [PubMed] [Google Scholar]
Tolentino 2011 {published data only}
- Tolentino Ede S, Chinellato LE, Tarzia O. Saliva and tongue coating pH before and after use of mouthwashes and relationship with parameters of halitosis. Journal of Applied Oral Science 2011;19(2):90‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Troccaz 2011 {published data only}
- Troccaz M, Haefliger OP, Cayeux I, Beccucci S, Jeckelmann N, Barra J, et al. Effects of flavoured mouthrinses on morning breath odour: a sensory, analytical and microbial evaluation. Flavour and Fragrance Journal 2011;26(2):90‐7. [Google Scholar]
Uchida 1973 {published data only}
- Uchida Y, Ishii Y, Kusunoki M, Murai S, Kinoshita S, Yashima T, et al. Investigation on the effect of 'Flagyl' in fetor ex ore by means of the double blind test. Journal of Japanese Society of Oral and Maxillofacial Surgery 1973;19(3):309‐22. [DOI] [PubMed] [Google Scholar]
UMIN000002145 {published data only}
- UMIN000002145. Randomized controlled trial on an effect of preparation of botanical extract on physiological halitosis. upload.umin.ac.jp/cgi‐open‐bin/ctr_e/ctr_view.cgi?recptno=R000002623 (first received 1 August 2009).
UMIN000002713 {published data only}
- UMIN000002713. Randomized cross‐over trial on an effect of quercus salicina extract chewing gum on genuine halitosis. upload.umin.ac.jp/cgi‐open‐bin/ctr_e/ctr_view.cgi?recptno=R000003307 (first received 1 December 2009).
Van der Sluijs 2018 {published data only}
- Sluijs E, Weijden GA, Hennequin‐Hoenderdos NL, Slot DE. The effect of a tooth/tongue gel and mouthwash regimen on morning oral malodour: a 3‐week single‐blind randomized clinical trial. International Journal of Dental Hygiene 2018;16(1):92‐102. [DOI] [PubMed] [Google Scholar]
Wåler 1997 {published data only}
- Wåler SM. The effect of some metal ions on volatile sulfur‐containing compounds originating from the oral cavity. Acta Odontologica Scandinavica 1997;55(4):261‐4. [PubMed] [Google Scholar]
Wang 2015 {published data only}
- Wang SC. Thirty‐seven cases of bad breath due to periodontitis treated with therapy of integrated traditional Chinese and Western medicine. He Nan Zhong Yi [Henan Traditional Chinese Medicine] 2015;35(9):2251‐2. [Google Scholar]
Wessel 2017 {published data only}
- Wessel SW, Mei HC, Slomp AM, Belt‐Gritter B, Dodds MWJ, Busscher HJ. Self‐perceived mouth feel and physico‐chemical surface effects after chewing gums containing sorbitol and Magnolia bark extract. European Journal of Oral Sciences 2017;125(5):379‐84. [DOI] [PubMed] [Google Scholar]
Wild 2001 {published data only}
- Wild JE, Nelson BJ, Hubbard ME, Bowman JP. Oral malodor control afforded through the use of sodium bicarbonate‐containing chewing gum. Compendium of Continuing Education in Dentistry 2001;22(7A):43‐6. [PubMed] [Google Scholar]
Wilhelm 2010 {published data only}
- Wilhelm D, Gysen K, Himmelmann A, Krause C, Wilhelm KP. Short‐term effect of a new mouthrinse formulation on oral malodour after single use in vivo: a comparative, randomized, single‐blind, parallel‐group clinical study. Journal of Breath Research 2010;4(3):036002. [DOI] [PubMed] [Google Scholar]
Wilhelm 2013 {published data only}
- Wilhelm D, Himmelmann A, Krause C, Wilhelm KP. Short term clinical efficacy of new meridol HALITOSIS tooth & tongue gel in combination with a tongue cleaner to reduce oral malodor. Journal of Clinical Dentistry 2013;24(1):12‐9. [PubMed] [Google Scholar]
Yaegaki 1992 {published data only}
- Yaegaki K, Sanada K. Effects of a two‐phase oil‐water mouthwash on halitosis. Clinical Preventive Dentistry 1992;14(1):5‐9. [PubMed] [Google Scholar]
Yoshimatsu 2006 {published data only}
- Yoshimatsu D, Sugimura S, Ioka T, Kometani T, Yamaga T, Miyazaki H. Effect of protease tablet on reduction of tongue coating. Oral Diseases 2005;11(Suppl 1):112 (Abs No P20). [Google Scholar]
- Yoshimatsu D, Sugimura S, Ioka T, Shiraishi K, Kometani T, Yamaga T, et al. Effect of protease tablet on reduction of tongue coating. Journal of Dental Health 2006;56:37‐41. [Google Scholar]
Yoshimatsu 2007 {published data only}
- Yoshimatsu D, Sugimura S, Ioka T, Shiraishi K, Kometani T, Yamaga T. Reduction of volatile sulfur compounds in mouth air by protease tablet. Journal of Dental Health 2007;57:22‐7. [Google Scholar]
References to studies awaiting assessment
Cuihua 2009 {published data only}
- Cuihua X. Observation on the efficacy of integrated traditional Chinese and Western medicine in treating halitosis caused by periodontitis. Chinese Medical Innovation 2009;15:35. [Google Scholar]
Dongling 2017 {published data only}
- Dongling M. Clinical effect of integrated traditional Chinese and Western medicine on halitosis caused by periodontitis. Chinese Health Care Nutrition 2017;31:285‐6. [Google Scholar]
Gupta 2016 {published data only}
- Gupta A, Bhowate R, Srivastava R, Sunilkumar, Devasthale SV, Sastry JLN. Clinical evaluation of Babool neem toothpaste in oral hygiene and dental care. International Journal of Pharmaceutical Research 2016;8(2):57‐64. [Google Scholar]
Liang 2013 {published data only}
- Yulin L. Observation on the efficacy of combined treatment of traditional Chinese medicine and Western medicine for halitosis caused by periodontitis. Chinese Journal of Trauma and Disability Medicine 2013;5:247‐8. [Google Scholar]
Niles 2003 {published data only}
- Niles HP, Hunter CM, Vazquez J, Williams MI, Cummins D. Clinical comparison of Colgate Total Advanced Fresh vs a commercially available fluoride breath‐freshening toothpaste in reducing breath odor overnight: a multiple‐use study. Compendium of Continuing Education in Dentistry 2003;24(9):29‐33. [PubMed] [Google Scholar]
Rostoka 2012 {published data only}
- Rostoka D, Kroica J, Iriste V, Reinis A, Kuznetsova V, Teibe U. Treatment of halitosis with mouth rinsing agents containing essential oils. Stomatologiia 2012;91(3):27‐34. [PubMed] [Google Scholar]
Shimei 2014 {published data only}
- Shimei S. Clinical observation of Banxia Xiexin decoction in treating Helicobacter pylori related halitosis. Inner Mongolia Medical Journal 2014;33(31):33‐4. [Google Scholar]
Vazquez 2003 {published data only}
- Vazquez J, Pilch S, Williams MI, Cummins D. Clinical efficacy of Colgate Total Advanced Fresh and a commercially available breath‐freshening dentifrice in reducing mouth‐odor‐causing bacteria. Compendium of Continuing Education in Dentistry 2003;24(9):20‐4. [PubMed] [Google Scholar]
References to ongoing studies
CTRI/2014/04/004519 {published data only}
- CTRI/2014/04/004519. Effect of test chewing gums on bad breath and oral micro‐organisms [Effect of test chewing gums on oral malodour and oral pathogens]. ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=8809&EncHid=&userName=chewing%20gum (first received 2 April 2014).
CTRI/2018/05/014049 {published data only}
- CTRI/2018/05/014049. Effect of a new herbal toothpaste on gum disease, bad breath and debris on the tooth surfaces [Effect of novel herbal dentifrice in control of plaque, gingivitis and halitosis ‐ randomized controlled trial]. ctri.nic.in/Clinicaltrials/showallp.php?mid1=26212&EncHid=&userName=halitosis (first received 22 May 2018).
CTRI/2018/06/014686 {published data only}
- CTRI/2018/06/014686. Ability of a polyherbal formulation to treat gum imflammation and bad breath over a period of three months [Effectiveness of a polyherbal formulation to treat gingivitis over a period of three months: a randomized trial]. ctri.nic.in/Clinicaltrials/showallp.php?mid1=26374&EncHid=&userName=halitosis (first received 29 June 2018).
DRKS00010618 {published data only}
- DRKS00010618. Clinical evaluation of the efficacy of Shur breath (Sylphar) in the reduction of bad breath. www.drks.de/DRKS00010618 (first received 10 June 2016).
IRCT201105136466N1 {published data only}
- IRCT201105136466N1. The effect of persica (herbal oral rinse) on halitosis [The effect of persica (herbal oral rinse) on halitosis in patient visiting Shiraz dental school‐2011]. en.irct.ir/trial/6901 (first received 5 November 2011).
IRCT2014121520314N1 {published and unpublished data}
- IRCT2014121520314N1. Comparison of efficacy of Halita mouthrinse with chlorhexidine mouthrinse in reducing oral malodor in patients with oral malodor [Clinical trial of comparison of efficacy of Halita mouthrinse with chlorhexidine mouthrinse in reducing oral malodor in patients with halitosis in 7‐day consumption]. en.irct.ir/trial/18026 (first received 23 February 2015).
IRCT2015030921395N1 {published data only}
- IRCT2015030921395N1. Effect of Pistacia atlantica subsp. mutica oleo‐gum resin, Punica granatum var. pleniflora flowers and Eugenia on halitosis [Preparation and clinical trial of toothpaste contained Pistacia atlantica subsp. mutica oleo‐gum resin, Punica granatum var. pleniflora flowers and Eugenia caryophyllata buds for halitosis]. en.irct.ir/trial/18763 (first received 30 August 2016).
IRCT2016012026122N1 {published and unpublished data}
- IRCT2016012026122N1. Comparison of the effectiveness of mouthwashes containing green tea on the severity of halitosis in patients with halitosis. en.irct.ir/trial/21738 (first received 25 February 2016).
ISRCTN67671859 {published data only}
- ISRCTN67671859. Assessment of oral malodour and tonsil bacteria after gargling of throat with an antiseptic [Assessment of oral malodour and tonsillar microbiota after gargling in oropharynx with benzethonium chloride]. doi.org/10.1186/ISRCTN67671859 (first received 19 August 2015).
ISRCTN74655176 {published data only}
- ISRCTN74655176. The safety and efficacy of an herbal chlorhexidine gel on bad breath caused by oral bacteria [A double‐bind placebo controlled study to determine the effectiveness of a new oral gel for halitosis]. doi.org/10.1186/ISRCTN74655176 (first received 24 October 2017).
ISRCTN75902618 {published data only}
- ISRCTN75902618. Efficacy of 0.1% chlorine dioxide mouthwash in reducing oral malodour [Efficacy of 0.1% chlorine dioxide mouthwash in reducing oral malodour ‐ a 2‐week randomized double‐blind cross‐over study]. doi.org/10.1186/ISRCTN75902618 (first received 15 March 2018).
NCT02794766 {published data only}
- NCT02794766. Inulin and S salivarius reduce halitosis [Inulin and Streptococcus salivarius reduce halitosis associated with tongue coating: a randomized clinical trial]. clinicaltrials.gov/ct2/show/NCT02794766 (first received 9 June 2016).
NCT03031756 {published data only}
- NCT03031756. Efficacy of Glycine powder air‐polishing combined with scaling and root planing in the treatment of periodontitis and halitosis. clinicaltrials.gov/ct2/show/NCT03031756 (first received 26 January 2017). [DOI] [PMC free article] [PubMed]
NCT03053882 {published data only}
- NCT03053882. Efficacy of peppermint and green tea in malodor [Comparative study of the effects of green tea and peppermint herbal mouthwash on halitosis]. clinicaltrials.gov/ct2/show/NCT03053882 (first received 15 February 2017).
NCT03160573 {published data only}
- NCT03160560. Controlling oral malodor by ClōSYS® oral rinse [Efficacy of ClōSYS® oral rinse products in human subjects in controlling oral malodor]. clinicaltrials.gov/ct2/show/NCT03160560 (first received 19 May 2017).
- NCT03160573. Controlling oral malodor by ClōSYS oral rinse [Efficacy of ClōSYS oral rinse products in human subjects in controlling oral malodor]. clinicaltrials.gov/ct2/show/NCT03160573 (first received 19 May 2017).
NCT03468595 {published data only}
- NCT03468595. Clinical evaluation of some local antimicrobial agents' adjunctive effects on periodontal parameters and halitosis. clinicaltrials.gov/ct2/show/NCT03468595?view=record (first received 16 March 2018).
TCTR20151109001 {published data only}
- TCTR20151109001. Effectiveness of alcohol‐free fluoride and essential oils containing mouthrinse in controlling dental plaque, gingivitis and halitosis in pregnancy: RCT (Alcohol‐free EO mouthwash for controlling gingivitis and halitosis in pregnancy). clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=1593 (first received 8 November 2015).
UMIN000023832 {published data only}
- UMIN000023832. Crossover test for reducing oral malodor by the chewing gums containing Myrsine seguinii extracts. upload.umin.ac.jp/cgi‐open‐bin/ctr_e/ctr_view.cgi?recptno=R000027456 (first received 30 August 2016).
Additional references
Akaji 2014
- Akaji EA, Folaranmi N, Ashiwaju O. Halitosis: a review of the literature on its prevalence, impact and control. Oral Health & Preventive Dentistry 2014;12(4):297‐304. [DOI] [PubMed] [Google Scholar]
Ayers 1998
- Ayers KM, Colquhoun AN. Halitosis: causes, diagnosis, and treatment. New Zealand Dental Journal 1998;94(418):156‐60. [PubMed] [Google Scholar]
Baharvand 2008
- Baharvand M, Maleki Z, Mohammadi S, Alavi K, Moghaddam EJ. Assessment of oral malodor: a comparison of the organoleptic method with sulfide monitoring. Journal of Contemporary Dental Practice 2008;9(5):76‐83. [PubMed] [Google Scholar]
Bollen 2012
- Bollen CM, Beikler T. Halitosis: the multidisciplinary approach. International Journal of Oral Sciences 2012;4:55‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bosy 1994
- Bosy A, Kulkarni GV, Rosenberg M, McCulloch CA. Relationship of oral malodor to periodontitis: evidence of independence in discrete subpopulations. Journal of Periodontology 1994;65(1):37‐46. [DOI] [PubMed] [Google Scholar]
COMET 2019
- COMET. Core Outcome Measures in Effectiveness Trials. www.comet‐initiative.org/ (accessed 15 September 2019).
CONSORT 2010
- CONSORT Group. CONSORT Statement. www.consort‐statement.org/ (accessed 15 September 2019).
De Geest 2016
- Geest S, Laleman I, Teughels W, Dekeyser C, Quirynen M. Periodontal diseases as a source of halitosis: a review of the evidence and treatment approaches for dentists and dental hygienists. Periodontology 2000 2016;71(1):213‐7. [DOI] [PubMed] [Google Scholar]
Delanghe 1997
- Delanghe G, Ghyselen J, Steenberghe D, Feenstra L. Multidisciplinary breath‐odour clinic. Lancet 1997;350(9072):187. [DOI] [PubMed] [Google Scholar]
Deutscher 2018
- Deutscher H, Derman S, Barbe AG, Seemann R, Noack MJ. The effect of professional tooth cleaning or non‐surgical periodontal therapy on oral halitosis in patients with periodontal diseases. A systematic review. International Journal of Dental Hygiene 2018;16(1):36‐47. [PUBMED: 28836329] [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315(7109):629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fedorowicz 2008
- Fedorowicz Z, Aljufairi H, Nasser M, Outhouse TL, Pedrazzi V. Mouthrinses for the treatment of halitosis. Cochrane Database of Systematic Reviews 2008, Issue 8. [DOI: 10.1002/14651858.CD006701.pub2] [DOI] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 15 September 2019. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Greenman 2004
- Greenman J, Duffield J, Spencer P, Rosenberg M, Corry D, Saad S, et al. Study on the organoleptic intensity scale for measuring oral malodor. Journal of Dental Research 2004;83(1):81‐5. [DOI] [PubMed] [Google Scholar]
Harper 2016
- Douglas Harper H. Halitosis. dictionary.com/browse/halitosis (accessed 4 June 2016).
Higgins 2011
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Kellesarian 2017
- Kellesarian SV, Malignaggi VR, Al‐Kheraif AA, Al‐Askar M, Yunker M, Javed F. Effect of antimicrobial photodynamic therapy and laser alone as adjunct to mechanical debridement in the management of halitosis: a systematic review. Quintessence International 2017;48(7):575‐83. [PUBMED: 28512650] [DOI] [PubMed] [Google Scholar]
Kinane 2015
- Kinane DF, Lindhe J, Trombelli L. Chronic periodontitis. In: Lindhe J, Lang NP, Karring T editor(s). Clinical Periodontology and Implant Dentistry. 5th Edition. Vol. 1, Blackwell Munksgaard, Blackwell Publishing Ltd, 2015:420‐1. [ISBN: 978‐1‐4051‐6099‐5] [Google Scholar]
Kleinberg 1990
- Kleinberg I, Westbay G. Oral malodor. Critical Reviews in Oral Biology and Medicine 1990;1(4):247‐59. [DOI] [PubMed] [Google Scholar]
Kleinberg 1995
- Kleinberg I, Codipilly M. The biological basis of oral malodor formation. In: Rosenberg M editor(s). Bad Breath: Research Perspectives. Tel Aviv: Ramot Publishing, 1995:13‐40. [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration, 2011, Version 5.1.0 (updated March 2011). [Google Scholar]
Loesche 1995
- Loesche WJ, Boever EH. Strategies to identify the main microbial contributors to oral malodor. In: Rosenberg M editor(s). Bad Breath: Research Perspectives. Tel Aviv: Ramot Publishing, 1995:41‐69. [Google Scholar]
Meningaud 1999
- Meningaud JP, Bado F, Favre E, Bertrand JC, Guilbert F. Halitosis in 1999. Revue de Stomatologie et de Chirurgie Maxillo‐Faciale 1999;100(5):240‐4. [PubMed] [Google Scholar]
Miyazaki 1995
- Miyazaki H, Sakao S, Katoh Y, Takehara T. Oral malodor in the general population of Japan. In: Rosenberg M editor(s). Bad Breath: Research Perspectives. Tel Aviv: Ramot Publishing, 1995:119‐36. [Google Scholar]
Moher 2001
- Moher D, Schulz KF, Altman DG. The CONSORT Statement: revised recommendations for improving the quality of reports of parallel‐group randomised trials. Lancet 2001;357:1191‐4. [PubMed] [Google Scholar]
Mookem 2014
- Mokeem SA. Halitosis: a review of the etiologic factors and association with systemic conditions and its management. Journal of Contemporary Dental Practice 2014;15(6):806‐11. [DOI] [PubMed] [Google Scholar]
Morita 2001
- Morita M, Wang HL. Association between oral malodor and adult periodontitis: a review. Journal of Clinical Periodontology 2001;28(9):813‐9. [DOI] [PubMed] [Google Scholar]
Muniz 2017
- Muniz FW, Friedrich SA, Silveira CF, Rosing CK. The impact of chewing gum on halitosis parameters: a systematic review. Journal of Breath Research 2017;11(1):014001. [PUBMED: 28212110] [DOI] [PubMed] [Google Scholar]
Oliveira‐Neto 2013
- Oliveira‑Neto J, Sato S, Pedrazzi V. How to deal with morning bad breath: a randomized, crossover clinical trial. Journal of Indian Society of Periodontology 2013;17(6):757‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Outhouse 2006
- Outhouse TL, Al‐Alawi R, Fedorowicz Z, Keenan JV. Tongue scraping for treating halitosis. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD005519.pub2] [DOI] [PubMed] [Google Scholar]
Quirynen 2009
- Quirynen M, Dadamio J, Velde S, Smit M, Dekeyser C, Tornout M, et al. Characteristics of 2000 patients who visited a halitosis clinic. Journal of Clinical Periodontology 2009;36(11):970‐5. [DOI] [PubMed] [Google Scholar]
Quirynen 2018
- Quirynen M, Lalemen I, Geest SD, Hous C, Dekeyser C, Teughels W. Breath malodour. In: Newman M, Klokkevold HTP, Carranza F editor(s). Newman and Carranza's Clinical Periodontology. 13th Edition. Philadelphia: Saunders, 2018:2756. [Google Scholar]
Ratcliff 1999
- Ratcliff PA, Johnson PW. The relationship between oral malodor, gingivitis, and periodontitis. Journal of Periodontology 1999;70(5):485‐9. [DOI] [PubMed] [Google Scholar]
Replogle 1996
- Replogle WH, Beebe DK. Halitosis. American Family Physician 1996;53(4):1215‐8, 1223. [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Richter 1996
- Richter JL. Diagnosis and treatment of halitosis. Compendium of Continuing Education in Dentistry 1996;17(4):370‐2, 374‐6 passim. [PubMed] [Google Scholar]
Romano 2010
- Romano F, Pigella E, Guzzi N, Aimetti M. Patients' self‐assessment of oral malodour and its relationship with organoleptic scores and oral conditions. International Journal of Dental Hygiene 2010;8(1):41‐6. [DOI] [PubMed] [Google Scholar]
Rosenberg 1991
- Rosenberg M, Septon I, Eli I, Bar‐Ness R, Gelernter I, Brenner S, et al. Halitosis measurement by an industrial sulphide monitor. Journal of Periodontology 1991;62(8):487‐94. [DOI] [PubMed] [Google Scholar]
Rosenberg 1995
- Rosenberg M. Introduction. In: Rosenberg M editor(s). Bad Breath: Research Perspectives. Tel Aviv: Ramot Publishing, 1995:1‐12. [Google Scholar]
Rosenberg 1996
- Rosenberg M. Clinical assessment of bad breath: current concepts. Journal of the American Dental Association 1996;127(4):475‐82. [DOI] [PubMed] [Google Scholar]
Rosing 2011
- Rosing CK, Loesche W. Halitosis: an overview of epidemiology, etiology and clinical management. Brazilian Oral Research 2011;25(5):466‐71. [DOI] [PubMed] [Google Scholar]
Scully 1997
- Scully C, el‐Maaytah M, Porter SR, Greenman J. Breath odor: etiopathogenesis, assessment and management. European Journal of Oral Sciences 1997;105(4):287‐93. [DOI] [PubMed] [Google Scholar]
Seeman 2014
- Seemann R, Duarte da Conceicao M, Filippi A, Greenman J, Lenton P, Nachnani S, et al. Halitosis management by the general dental practitioner‐ results of an International Consensus Workshop. Swiss Dental Journal 2014;124(11):1205‐11. [DOI] [PubMed] [Google Scholar]
Silva 2018
- Silva MF, Leite FRM, Ferreira LB, Pola NM, Scannapieco FA, Demarco FF, et al. Estimated prevalence of halitosis: a systematic review and meta‐regression analysis. Clinical Oral Investigations 2018;22(1):47‐55. [PUBMED: 28676903] [DOI] [PubMed] [Google Scholar]
Silwood 2001
- Silwood CJL, Grootveld MC, Lynch E. A multifactorial investigation of the ability of oral health care products (OHCPs) to alleviate oral malodour. Journal of Clinical Periodontology 2001;28:634–41. [DOI] [PubMed] [Google Scholar]
Singh 2015
- Singh VP, Malhotra N, Apratim A, Verma M. Assessment and management of halitosis. Dental Update 2015;42(4):346‐8; 351‐3. [DOI] [PubMed] [Google Scholar]
Slot 2015
- Slot DE, Geest S, Weijden FA, Quirynen M. Treatment of oral malodour. Medium‐term efficacy of mechanical and/or chemical agents: a systematic review. Journal of Clinical Periodontology 2015;42 Suppl 16:S303‐16. [DOI: 10.1111/jcpe.12378] [DOI] [PubMed] [Google Scholar]
Slots 2012
- Slots J. Low‐cost periodontal therapy. Periodontology 2000 2012;60(1):110‐37. [DOI] [PubMed] [Google Scholar]
Solis‐Gaffar 1975
- Solis‐Gaffar MC, Niles HP, Rainieri WC, Kestenbaum RC. Instrumental evaluation of mouth odor in a human clinical study. Journal of Dental Research 1975;54(2):351‐7. [PubMed] [Google Scholar]
Stamou 2005
- Stamou E, Kozlovsky A, Rosenberg M. Association between oral malodour and periodontal disease‐related parameters in a population of 71 Israelis. Oral Diseases 2005;11 Suppl 1:72‐4. [DOI] [PubMed] [Google Scholar]
Sumanth 2019
- Sumanth KN. Dental therapeutics. In: Karemore T editor(s). Text Book of Oral Medicine and Radiology. 1st Edition. New Delhi: CBS Publishers, 2019. [Google Scholar]
Tahani 2018
- Tahani B, Sabzian R. Effect of Camellia sinensis plant on decreasing the level of halitosis: a systematic review. Dental Research Journal 2018;15(6):379‐84. [PUBMED: 30534164] [PMC free article] [PubMed] [Google Scholar]
Tangerman 2002
- Tangerman A. Halitosis in medicine: a review. International Dental Journal 2002;52(Suppl 3):201‐6. [DOI] [PubMed] [Google Scholar]
Tartaglia 2019
- Tartaglia GM, Tadakamadla SK, Connelly ST, Sforza C, Martin C. Adverse events associated with home use of mouthrinses: a systematic review. Therapeutic Advances in Drug Safety 2019;10:2042098619854881. [PUBMED: 31579502] [DOI] [PMC free article] [PubMed] [Google Scholar]
Thoppay 2018
- Thoppay JR, Filippi A, Ciarrocca K, Greenman J, Rossi SS. Halitosis. In: Farah C, Balasubramaniam R, McCullough M editor(s). Contemporary Oral Medicine. Cham: Springer, 2018. [Google Scholar]
Tonzetich 1977
- Tonzetich J. Production and origin of oral malodor: a review of mechanisms and methods of analysis. Journal of Periodontology 1977;48(1):13‐20. [DOI] [PubMed] [Google Scholar]
Tonzetich 1978
- Tonzetich J. Oral malodour: an indicator of health status and oral cleanliness. International Dental Journal 1978;28(3):309‐19. [PubMed] [Google Scholar]
Treadwell 2006
- Treadwell JR, Tregear SJ, Reston JT, Turkelson CM. A system for rating the stability and strength of medical evidence. BMC Medical Research Methodology 2006;19(6):52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tsunoda 1981
- Tsunoda M, Sato H, Ohkushi T. [The experimental study for the effect of sodium copper chlorophyllin in halitosis (author's transl)]. Nippon Shishubyo Gakkai Kaishi [Journal of the Japanese Association of Periodontology] 1981;23(3):490‐8. [DOI] [PubMed] [Google Scholar]
van den Broek 2007
- Broek AM, Feenstra L, Baat C. A review of the current literature on aetiology and measurement methods of halitosis. Journal of Dentistry 2007;35(8):627‐35. [DOI] [PubMed] [Google Scholar]
van den Broek 2008
- Broek AM, Feenstra L, Baat C. A review of the current literature on management of halitosis. Oral Diseases 2008;14(1):30‐9. [DOI] [PubMed] [Google Scholar]
van Steenberghe 1997
- Steenberghe D. Breath malodor. Current Opinion in Periodontology 1997;4:137‐43. [PubMed] [Google Scholar]
Wu 2018
- Wu X, Zhang J, Zhou Y, He Z, Cai Q, Nie M. Whether Chinese medicine have effect on halitosis: a systematic review and meta‐analysis. Evidence‐Based Complementary and Alternative Medicine: eCAM 2018;2018:4347378. [PUBMED: 30598685] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wu 2019
Yaegaki 2000
- Yaegaki K, Coil JM. Examination, classification, and treatment of halitosis; clinical perspectives. Journal of the Canadian Dental Association 2000;66(5):257‐61. [PubMed] [Google Scholar]
Yoo 2019
- Yoo JI, Shin IS, Jeon JG, Yang YM, Kim JG, Lee DW. The effect of probiotics on halitosis: a systematic review and meta‐analysis. Probiotics and Antimicrobial Proteins 2019;11(1):150‐7. [PUBMED: 29168154] [DOI] [PubMed] [Google Scholar]