

Abstract
Objective:
To determine whether resistance training is similarly effective in reducing skeletal muscle efficiency and increasing strength in weight-reduced and maximal weight subjects.
Methods:
We examined the effects of supervised resistance exercise on skeletal muscle in 14 overweight and obese individuals sustaining a 10% or greater weight loss for over 6 months, and a phenotypically similar group of 15 subjects who were nonweight-reduced and weight stable at their maximal lifetime body weight. We assessed skeletal muscle work efficiency and fuel utilization (bicycle ergometry), strength (dynamometry), body composition (dual energy x-ray absorptiometry), and resting energy expenditure (indirect calorimetry) before and after 12 weeks of thrice weekly resistance training.
Results:
Non-weight-reduced subjects were significantly (10–20%) stronger before and after the intervention than reduced weight subjects and gained significantly more fat-free mass with a greater decline in % body fat than weight-reduced subjects. Resistance training resulted in similar significant decreases (~10 %) in skeletal muscle work efficiency at low level exercise and ~10–20% increases in leg strength in both weight-reduced and non-weight-reduced subjects.
Conclusion:
Resistance training similarly increases muscle strength and decreases efficiency regardless of weight loss history. Increased resistance training could be an effective adjunct to reduced-weight maintenance therapy.
Keywords: skeletal muscle, exercise intervention, weight loss, weight regain
INTRODUCTION
Most individuals find that it is harder to sustain weight loss than to lose weight. Maintenance of a 10% or greater dietary-induced weight loss is accompanied by decreases in energy expenditure to levels significantly (approximately 300–400 kcal/day) below those predicted solely on the basis of changes in weight and body composition as well as increased hunger and delayed satiety (1). This decline in energy expenditure does not abate over time, and individuals who are successful at keeping weight off for prolonged periods of time report that to do so they must decrease their energy intake and substantially increase their energy expenditure via exercise (usually aerobic for 200–300 more minutes per week) compared to individuals at the same weight who have never lost weight (2, 3). Increased physical activity is clearly associated with less weight regain after otherwise successful weight loss (4, 5). However, an important question is whether the benefits of increased exercise in sustaining weight loss are dependent only the type of exercise performed as well as the number of calories expended.
Skeletal muscle is the primary effector organ for the disproportionate decline in energy expenditure following 10% or greater weight loss (6). Molecular changes in skeletal muscle following dietary weight loss result in an approximate 20% increase in muscle work efficiency at low levels of power output, which is significantly correlated with the degree of disproportionate decline in energy expenditure that occurs following weight loss (6). Decreasing skeletal muscle work efficiency would therefore be advantageous in sustaining weight loss, especially if the decrease in efficiency, and therefore increased caloric expenditure per unit of work, occurred at levels of physical activity commensurate with those of daily living. Energy expended during exercise at the level described above is similar that expended during activities of daily living outside of voluntary exercise which is defined as non-exercise activity thermogenesis (NEAT) (7). This decline in efficiency would essentially “reverse” some of the changes in muscle metabolism that occurred as a result of dietary weight loss. Muscle resistance training is a potential means to achieve this goal (8, 9).
In individuals stable at their usual weight, resistance training is associated with increased strength (10) and decreased skeletal muscle contractile efficiency (8, 9). In contrast, aerobic training results in increased skeletal muscle efficiency at without the increase in strength noted during resistance training (11).
The aim of the present study was to compare the effects of muscle resistance training on skeletal muscle work efficiency in weight-reduced individuals versus a control group of non-weight-reduced individuals at their maximal lifetime weights. We hypothesized that resistance training would similarly decrease skeletal muscle work efficiency and increase muscle strength in both groups. The alternative hypothesis was that restoration of body energy stores (fat) following weight loss was so vital to reproductive integrity and biological survival that the weight-reduced individual would be less responsive to the effects of resistance training on muscle.
MATERIALS AND METHODS
Subjects
Twenty-nine overweight (30 kg/m2 > BMI > 25 kg/m2) or obese (BMI > 30 kg/m2) subjects (7 M, 22 F, age range 29–47 years) were recruited by on-line and newspaper advertisement and via physicians specializing in bariatric surgery and/or the treatment of obesity in New York City. Fourteen subjects (11F, 3M; BMI range 25.8–41.2 kg/m2) were weight-reduced through dietary restriction (i.e., did not reported increased physical activity to lose weight) and had sustained a 10% or greater weight loss for at least 6 months following laparoscopic banding (n=6) or dietary weight loss (n=8). Fifteen subjects (11F, 4M; BMI range 26.2–40.6 kg/m2) were at their maximal lifetime weights. Inclusion criteria included documentation of weight stability (within 3%) for at least 6 months, good health - without diabetes or hypertension - and capacity to engage in vigorous exercise but not currently participating in any type of regular physical training. Exclusion criteria included smoking, hypertension, diabetes, asthma, medication affecting the autonomic nervous system (e.g., beta-blockers), thyroid disease or medication, asthma requiring regular bronchodilator or steroid therapy, psychotropic medication, and any immunocompromising condition that would increase the risk of infection at biopsy sites. Subjects met with staff (MKH, SMW, or APS) on at least 4 occasions before enrollment to ascertain their ability to comply with the program and to attend regular exercise sessions. All subjects were prescreened by an MD (LJA or MR) with a physical examination, electrocardiogram, thyroid profile, complete blood count, liver function studies, and HIV testing. Studies were approved by the Institutional Review Board of The New York Presbyterian Medical Center and are consistent with guiding principles for research involving humans (12). Written informed consent was obtained from all subjects. Subject characteristics are presented in Table 1.
Table 1.
Mean (SD) subject demographics, body composition, resting energy expenditure and resting RQ. There were no significant differences between groups at baseline but there were significant group x time effects in the intervention such that non-weight-reduced individuals gained more FFM and had a higher reduction in weight, FM, and % body fat than individuals who were weight-reduced. Significant P values are in bold.
| Table 1. Subjects |
Non-weight-reduced Subjects | Weight-Reduced Subjects | All Subjects | P values | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre- training |
Post- training |
Delta | Pre- training |
Post- training |
Delta | Pre- training |
Post- training |
Delta | Group | Time | Group × Time |
|
| Gender | 5M, 10F | 4M, 10F | 9M, 20F | - | - | |||||||
| Age | 40.1 (8.2) |
36.7 (6.6) | 38.5 (6.0) |
0.45 | - | |||||||
| Height (cm) | 167 (9) | 168 (6) | 167 (8) | 0.78 | - | - | ||||||
| Weight (kg) | 91.8 (16.3) |
93.3 (17.6) |
1.5 (2.9) | 94.4 (16.8) |
94.7 (16.9) |
0.3 (2.6) | 93.0 (16.3) |
93.9 (17.0) |
0.61 | 0.07 | 0.33 | |
| BMI (kg/m2) | 32.5 (4.2) |
33.1 (4.7) | 0.6 (1.0) | 34.0 (5.9) | 34.0 (6.1) |
0.0 (1.1) | 33.2 (5.0) |
33.5 (5.4) | 0.3 (1.1) | 0.40 | 0.14 | 0.18 |
| FFM (kg) | 56.4 (10.9) |
58.2 (10.7) |
1.8 (4.8) | 60.9 (10.6) |
58.3 (8.9) |
−1.5 (4.4) | 58.6 (10.8) |
58.3 (9.7) | 0.3 (5.0) | 0.17 | 0.77 | 0.014 |
| FM (kg) | 35.3 (11.8) |
35.0 (11.7) |
−0.7 (3.4) | 33.5 (12.2) |
36.3 (12.1) |
2.8 (5.3) | 34.5 (11.1) |
35.7 (10.7) |
1.2 (4.9) | 0.10 | 0.18 | 0.042 |
| % Fat | 38.2 (6.9) |
36.5 (6.2) | −1.0 (3.7) | 34.9 (9.1) | 38.0 (8.2) |
2.8 (4.9) | 36.6 (8.1) |
37.2 (7.2) | 0.9 (4.7) | 0.18 | 0.53 | 0.026 |
| REE (kcal/kg FFM/day) |
26.7 (2.9) |
27.3 (3.3) | 0.6 (1.0) | 25.7 (4.9) | 27.3 (3.7) |
1.6 (1.0) | 26.2 (4.0) |
27.3 (3.4) | 1.0 (5.6) | 0.51 | 0.20 | 0.63 |
| Resting RQ | 0.85 (0.05) |
0.84 (0.08) |
−0.01 (0.07) |
0.82 (0.06) |
0.83 (0.07) |
−0.01 (0.09) |
0.84 (0.06) |
0.83 (0.08) |
0.0 (0.08) | 0.72 | 0.56 | 0.90 |
Study Design:
Prior to beginning the exercise intervention, subjects underwent the following testing:
Energy Expenditure:
Resting Energy Expenditure by indirect calorimetry using a Viasys 2 hood calorimeter was measured at 9AM in the post-absorptive state and following a 30 minute accommodation period (13).
Body Composition:
Fat mass (FM) and fat-free mass (FFM) were determined by dual energy x-ray absorptiometry (DXA) (13). DXA measurements were standardized. All subjects were studied following an overnight fast and height and weight were measured just prior to scanning for entry into the DXA software. All subjects must fit entirely within the DXA scan field-of-view, with arms placed at side of body (no overlapping). Subjects wear a hospital gown ensuring no metal in clothing or on body.
Skeletal muscle ergometry:
Skeletal muscle work efficiency and fuel utilization were assessed by graded bicycle ergometry (13) as described previously. Briefly, after a 10min period of accommodation, the subjects pedaled at 60 rpm against graded resistance to generate 10 W, 25 W, and 50W of power in successive 4-min intervals using a Lode Corival electromagnetically braked bicycle and ergometer with electrical braking. Oxygen uptake (VO2), carbon dioxide production (VCO2), and the respiratory exchange ratio were measured continuously using a Sensormedics VMAX 29 metabolic cart (14). Steady-state values were recorded at 0 W (rest), 10 W, 25 W, 50 W, and 75W with expectation that 50W of power is below the anaerobic threshold for even the most sedentary subjects. Steady-state VO2 and VCO2 are easily attained within 2–3 min of cycling (15).
31P-NMR spectroscopy of the medial and lateral gastrocnemius muscles at rest was performed in a 1.5T Philips Intera MRI scanner. Basal concentrations of inorganic phosphate (Pi), and phosphocreatinine (PCr) were measured in the medial and lateral gastrocnemius muscles as previously described (6). Pi at rest reflects the potential for muscle to oxidize free fatty acids (FFA) vs. carbohydrate and the ratio of Pi to PCr reflects the rate of energy flux (ATP consumption) through muscle and is a measure of resting muscle efficiency. Subjects exercised in the magnet by depressing a pedal against varying levels of resistance to allow calculation of the recovery constant for PCr (kPCr) which is a commonly utilized index of mitochondrial capacity (16).
Muscle strength:
Strength assessment was made using a Cybex Norm Dynamometer. Subjects were positioned in an adjustable chair and strapped in across the trunk, hip, and thigh and then instructed to push as hard as they could against a shin pad at the distal tibia for obtain maximal power and torque, muscle fatigability (decline over 25 repetitions) (17, 18).
Exercise Intervention:
Following completion of the initial assessments described above, subjects began a 12-week resistance training circuit consisting of 45–60 minute sessions on Mondays, Wednesdays, and Fridays. This circuit was based on studies of the effects of different types of exercise in subjects with type 2 diabetes, the majority of whom were overweight or obese (19). Baseline resistance loads for each subject were determined at the first session using a 10 resistance maximum (10RM) protocol. Subjects acclimated to the circuit during the first 2–3 sessions. The intensity of the resistance training was subsequently increased as tolerated based upon subjects’ ratings of perceived exertion and under the supervision of a trainer (MKH).
Subjects began each session with a 5–10 minute warmup that consisted of basic mobility movements such as knee lifts and shoulder circles and back flexion and extension exercises. This was followed by the exercise intervention which consisted of two sets of upper body exercises, and three sets of lower body exercises. The exercises consisted of 10 repetitions at a maximum tolerated intensity (weight) with a 1 minute rest between each set. Each subject was asked to give a rating of perceived exertion (RPE) (20) for the last repetition of each set which was used to evaluate whether an increase in the resistance load was warranted for the next session. Specifically, the resistance load was increased in increments of 5 pounds if subjects expressed an RPE below 7 on a 10-point scale. Exercises are listed below:
Shoulder Press (pushing handles directly upwards while seated)
Latissimus Pull (pulling a bar directly down while seated)
Seated Row (pulling handles towards chest while seated)
Chest press (pushing a bar away from the chest while seated)
Leg Press (using legs to push a plate while seated)
Leg Extension (extending at the knees while seated)
Leg Curl (flexing at the knees while seated)
Calf extension (extending the ankles against resistance while seated)
Selectorized resistance machines were chosen instead of free weights so that biomechanically-correct movement patterns could be more easily maintained, allowing subjects to focus on muscle force production rather than balance, control and additional aspects of proper technique that arise when using free weights. Exercises were selected to directly involve the muscles relevant to the ergometric and dynamometer studies. The NMR involves muscles used in the calf extension and the dynamometer involves muscles used in the leg press. All lower extremity exercise were directly relevant to bicycle ergometric studies. Upper body exercises were selected to provide participants with a ‘total body’ workout and aid in recruitment and adherence to completion of the intervention. Exercises were consistent with recommendations from the American College of Sports Medicine (21).
Calculations and statistics:
Skeletal muscle work efficiency during ergometry was calculated as Delta Mechanical Efficiency (DME) which is the slope of the line relating energy expended advancing from 10W-25W, 25–50W, and 50–75W of power generation. The three steps were analyzed individually. Delta mechanical efficiency was chosen to avoid any skewing of the data due to training-induced changes in resting energy expenditure or the degree of inefficiency due to fidgeting etc., on the bicycle (15, 22) (against the possibility that subjects were better accommodated to the bicycle at the post-training session and could pedal more efficiently). The steady state respiratory exchange ratio (RER) was used to calculate relative fuel utilization of carbohydrates versus fatty acids at each work level (23).
Data are presented as mean (SD). Statistical significance was prospectively defined as Pα<0.05. Between-group comparisons at baseline were made by ANOVA. Within-group comparisons were made by ANOVA with repeated measures. Comparisons of changes between groups (group x time interactions) were made by ANOVA comparing the deltas in each measures (post-training minus pre-training) between groups. Analyses were performed using the Statisica version 10 statistical package (24).
RESULTS
Subjects:
Protocol adherence was excellent and 28 out of 29 subjects attended all 36 exercise sessions and one subject missed only the last session. There were no significant differences between groups in subject demographics or body composition at baseline (see Table 1). Subjects in the non-weight-reduced group had significantly greater lower leg strength based on peak torque during flexion both before (63.4 (18.2) N·M in nonweight reduced vs. 45.6 (15.3) N·M in weight-reduced, P=0.009) and after training (88.2 (16.9) N·M in non-weight reduced vs.75.0 (15.9) N·M in weight-reduced, P=0.045) (see Figure 1). Though baseline muscle work efficiency in weight-reduced subjects at 10–25W of power tended to be more efficient [ratio of energy expended to work performed from 10–25W was 3.44 (0.98) in weight-reduced subjects vs 3.73 (0.88) in non-weight-reduced subjects] these between-group differences were not significant (see Figure 2). No significant differences in any variables were noted between subjects who had lost weight by diet vs. gastric banding.
Figure 1.
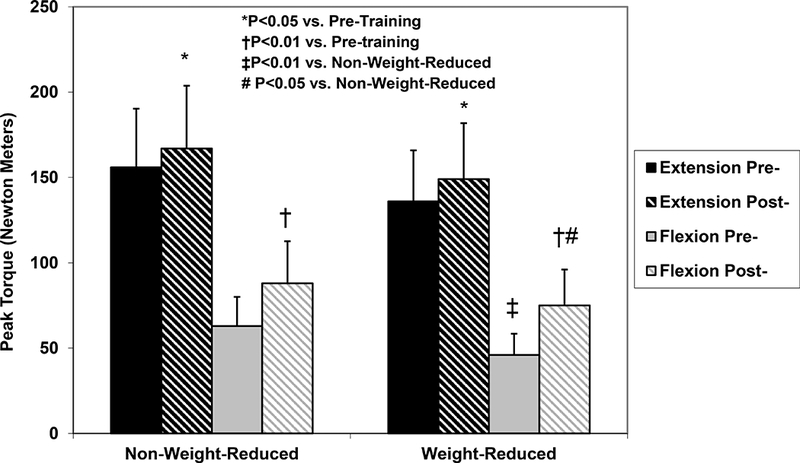
Strength training: Data are Mean (SD) lower leg extension and flexion strength. Lower leg flexion strength was significantly greater in the non-weight-reduced group compared to the weight-reduced group. Resistance training for 3 months resulted in significant increases in both extension and flexion strength in both groups. There were no significant differences in the absolute or proportional magnitudes of the treatment effects.
Figure 2.
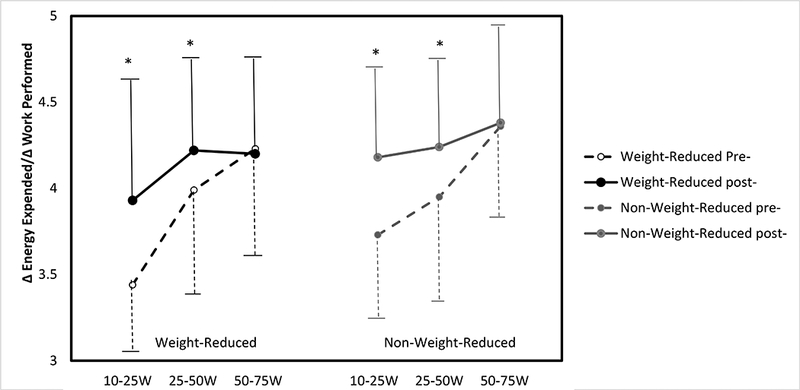
Muscle efficiency: Data are Mean (SD) delta efficiency (defined as the slope of the line relating energy expenditure to power generated at different workloads) by graded bicycle ergometry. In all groups, resistance training resulted in a significant decline in skeletal muscle work Efficiency over the power generation ranges: 10–25W and 25–50W. There were no significant between group differences in the absolute or proportional magnitudes of the treatment effects.
Resistance Training:
There were no significant changes in weight or body composition in either group during the period of resistance training but group x time interactions in measures of body composition were significan (see Table 1). Specifically, non-weight-reduced subjects tended to gain FFM and lose FM while weight-reduced subjects tended to lose FFM and gain FM and % fat were significant. There was no significant effect of resistance training on resting energy expenditure or resting RQ in either group.
Strength in both flexion and extension of the lower extremity were significantly increased by resistance training in both groups; the magnitude of the increase was not significantly different between groups (group x time interaction p = 0.70 for peak torque during extension and p=0.36 for peak torque during flexion, see Figure 1).
Resistance training caused significant declines in muscle work efficiency during bicycle ergometry as reflected in delta contractile efficiency (changes in energy expended/changes in work performed) in both groups at low levels of exercise, i.e., levels of exercise similar to those of activities of daily living. Specifically, the significant decline in work efficiency was evident when bicycling to generate increments between 10W to 25W of power [mean (95% CI) change in the ratio of energy expended/work performed as a result of resistance training in weight-reduced subjects = 0.49 (−0.01 – 0.82) and 0.46 (−0.36 – 1.27) in non-weight reduced subjects), and 25W to 50W of power [mean (95% CI) change in the ratio of energy expended/work performed as a result of resistance training in weight-reduced subjects = 0.17 (−0.10 – 0.44) and 0.22 (0.03 – 0.48) in non-weight reduced subjects), but was not detected between 50W to 75W of power [mean (95% CI) change in the ratio of energy expended/work performed as a result of resistance training in weight-reduced subjects = −0.07 (−0.60 – 0.45) and 0.03 (−0.25 – 0.30) in non-weight reduced subjects). The range in which significant decreases in muscle after resistance is is similar that within which muscle efficiency increase after weight loss (6, 13). There were no significant between-group differences in the magnitude of the decline in efficiency (group x time interaction p values = 0.90 from 10–25 W of power generated, 0.79 from 25–50 W of power generated, and 0.90 from 50–75 W of power generated; see Figure 2).
Resistance training resulted in a significant decline in RER and increase the the percentage of kcal derived from fatty acid oxidation during exercise to generate 25W of power only. No other significant training effects on fuel utilization were noted and there were no significant between group differences at any degree of exercise. Group x time interaction p values were also not significant (see Figure 3). NMR data (Table 2) did not show the significant decrease in the resting Pi/PCr ratio, which would reflect resting muscle ATP consumption, following resistance training that has been reported elsewhere (25) and response of Pi, PCr, Pi/PCr or kPCR to training were not significant in either group.
Figure 3.
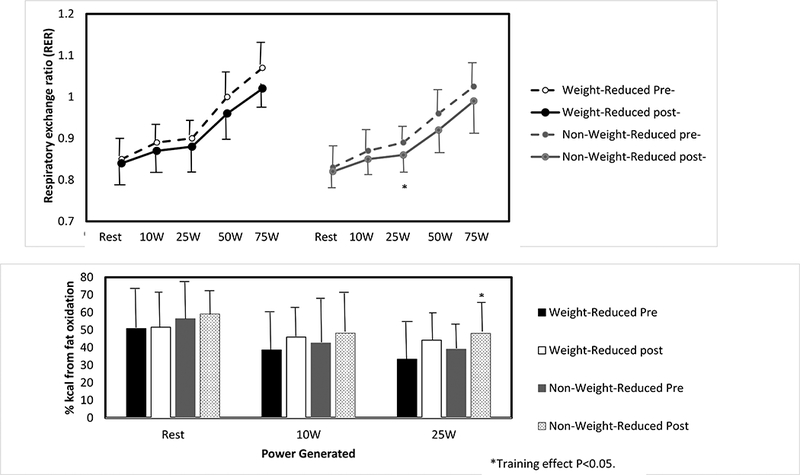
Fuel utilization. Data are Mean (SD) Respiratory Exchange Ratio (RER) at rest and during bicycle ergometry to perform 10W to 75W of power generated. These data are also expressed as the percentage of calories utilized that come from the oxidation of FFA which could not be assessed at 50W or 75W of power generate because some of the RER values were > 1.0 (45). There were no significant groupx x time differences in the absolute or proportional magnitudes of the treatment effects, though there was a significant treatment-associated decrease in RER and increase in the % of kcal derived from the oxidation of FFA at 25W of power generated in the nonweight-reduced subjects only.
Table 2.
31P-NMR data showed no differences between groups in propensity to oxidize FFA vs. glucose (Pi), resting muscle ATP consumption (Pi/PCr), or glycolytic potential (kPCr) at rest or in response to the exercise intervention. No significant effects of the exercise intervention were noted.
| Table 2. NMR Data |
Non-weight-reduced Subjects | Weight-Reduced Subjects | All Subjects | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-training | Post-training | P Value |
Pre-training | Post-training | P value |
Pre-training | Post-training | P value |
|
| Pi at rest (mmol/kg) |
4.27 (0.91) | 4.09 (0.92) | 0.61 | 4.27 (0.74) | 4.11 (0.62) | 0.60 | 4.27 (0.88) | 4.09 (0.92) | 0.46 |
| PCr at rest (mmol/kg) |
38.2 (0.90) | 38.4 (0.92) | 0.61 | 38.2 (0.74) | 38.4 (0.61) | 0.60 | 38.2 (0.88) | 38.4 (0.93) | 0.46 |
| Pi/PCr at rest |
0.11 (0.03) | 0.11 (0.03) | 0.65 | 0.11 (0.02) | 0.11 (0.02) | 0.60 | 0.11 (0.03) | 0.11 (0.03) | 0.45 |
| kPCr | 0.025 (0.012) | 0.026 (0.021) | 0.84 | 0.023 (0.11) | 0.018 (0.18) | 0.39 | 0.024 (0.012) | 0.022 (0.019) | 0.67 |
DISCUSSION
The major finding of this study is that that 12 weeks of resistance training causes similar increases in strength and decreases in muscle work efficiency in both weight-reduced and non-weight-reduced subjects of similar levels of adiposity that are of sufficient magnitude to significantly “reverse” some of the increased muscle efficiency that occurs as a result of weight loss. The lack of between-group differences in response to resistance training is significant in that it does not support the alternative hypothesis that the ability to affect skeletal muscle by resistance training is altered as a result of weight reduction.These findings suggest that resistance training following weight loss reverses some of the increased skeletal muscle work efficiency induced by weight loss and therefore might be a useful adjunctive therapy to help sustain weight reduction.
Attempts to sustain a 10% or greater dietary weight loss are opposed by changes in energy expenditure (about 300–400 kcal/day below predicted based on body composition), autonomic function (decreased sympathetic and increased parasympathetic nervous system tone), neuroendocrine function (decreased circulating concentrations of leptin and bioactive thyroid hormones), and energy intake (increased food reward and hunger, decreased food restraint and satiation) (1). These changes do not appear to abate over time (2, 26, 27, 28) and the likelihood of losing and sustaining a 10% or greater weight reduction is only about 15% (29). The primary effector organ of adaptive thermogenesis is skeletal muscle, the efficiency of which increases by approximately 20% following dietary weight loss work (6).
The American College of Sports Medicine recommends 150 min/wk of moderately vigorous physical activity to sustain good health and 200 min/wk which has been shown to lessen the likelihood of weight regain following weight loss (3, 30, 31). In previous studies (6) we have found that the rate of energy expenditure above resting while exercising to generate 25 W of power was 3.38 (0.50) kcal/min. In the present study, the efficiency of muscle in this same exercise range decreased by 14.9 (0.3)% in the nonweight reduced group and 8.4 (0.3)% in the non-weight reduced group following resistance training (group x time interaction p= 0.58). Extrapolating from these data resistance training would increase energy expenditure by 30 kcal/hr during exercise at this level. The average residual (difference between measured energy expenditure and predicted changes in energy expenditure based on changes in weight and body composition) for non-resting energy expenditure (NREE) is 201 kcal/day in subjects with obesity studied before and after a 10% and 20% weight loss (32, 33). Therefore, one would need to be engaging in physical activity comparable to pedaling a bicycle to generate 10–25W of power (~200 kcal/hr or 2–3 METS for an 80–100 kg adult which is consistent with activities of daily living (34, 35)) for approximately 7 hours/day to “reverse” the adaptive thermogenesis associated with weight loss. Large population surveys (36) report that the average adult spends approximately 8 hours per day in physical activity (predominantly in occupation-related and household-related activities) with large variation between individuals depending upon occupation and exercise habits and with the caveat that exercise efficiency studies reported here only reflect one type of activity.
Non-weight-reduced subjects were significantly stronger (see Figure 1), and tended to have lower muscle efficiency during low levels of work (10–25W, not statistically significant) at baseline (see Figure 1). These findings are consistent with our previous observations that weight loss results in a significant increase in skeletal muscle work efficiency during low level exercise (1, 6). Subjects for the weight-reduced group were recruited based on a documented history of weight loss and sustained maintenance of reduced body weight. Given the high level of variability between individuals in energy expenditure, muscle strength, muscle efficiency, etc., it was not expected that a between groups analysis at baseline would reveal significant inter-group differences, i.e., that weight-reduced subjects would have significantly greater skeletal muscle work efficiency than non-weight-reduced subjects prior to any intervention. The hypothesis related to whether or not there were significant inter-group differences in the within-subjects analyses of response to resistance training.
We have previously shown that the respiratory exchange ratio (RQ) during low level exercise decreases following weight loss, reflecting a greater propensity to oxidize FFA (6). The reasons for the lack of a resistance training effect to increase the respiratory exchange ratio despite the decline in muscle efficiency are not clear but may reflect an overall fitness improvement in subjects which has been associated with a decline in the respiratory exchange ratio (37) as a result of both resistance and aerobic training.
Weight-reduced subjects gained fat and lost FFM (both not statistically significant) over the course of the intervention with significant group x time interactions in these variables. The significant group differences in body composition changes may reflect more intense exercising in the non-weight-reduced group by virtue of the fact that they were initially stronger, differences in tissue hydration, dietary intake or compliance with the request to not alter usual exercise activities outside of the training intervention between groups interacting with primary differences in energy partitioning between groups.
The strengths of this study are in the close phenotypic matching of the study groups and the uniformity of the training. Important weaknesses include inability to control exercise activity and diet outside of the training regime and the lack of between group differences in skeletal muscle efficiency at baseline. The issue of energy intake is of particular importance in evaluating the potential efficacy of increased resistance training on longterm maintenance of reduced body weight of the molecular physiology of muscle under these circumstances are ongoing.
Based on the present study, we would predict that resistance-trained subjects, compared to non-exercising or aerobic exercising subjects, would display sustained relative increases in energy expenditure for comparable levels of physical activity and perhaps find it easier to sustain weight loss. Hunter et al (38) reported that resistance or aerobic training blunted the declines in TEE and non-exercise activity thermogenesis (NEAT) during weight loss. Drenowatz et al (39) found that men enrolled in a 16 week aerobic or resistance training regimen who were in the resistance training group experienced were more likely to maintain moderate vigorous physical activity levels beyond the exercise regimen while in the program.
A key question in the potential efficacy of resistance training in sustaining weight loss is the extent to which this increased expenditure would be compensated by increased food intake In 1956, Mayer et al (40) noted that energy intake in Bengalese jute work Ers increased in rough proportion to any increase in expenditure, but also noted that it increased -in the context of an extreme sedentary lifestyle. A recent review by Blundell et al (41) noted that appetite is affected acutely and chronically by diet composition, body composition, energy expenditure, energy balance, and numerous neuroendocrine and entero-endocrine signals all of which are influenced by the type and amount of exercise in a highly individualized manner. Some studies comparing the effects of the type of exercise on energy intake have reported that aerobic exercise, especially at high intensities, results in greater satiation and less hunger after exercise (42) than resistance training in non-weight-reduced subjects.
It should be emphasized that the level of resistance training was relatively low compared to maximal resistance training and high intensity interval training both of which have been reported to increase muscle efficiency (43, 44), and that the main outcome variable of this study was muscle efficiency at low levels of exercise. Other studies describe different types of training (e.g., high intensity interval cycling) and measure efficiency over a wider range of exercise and in ranges not examined in this study.
In summary, these data suggest that resistance training may “reverse” the increase in skeletal muscle contractile efficiency following dietary weight loss, thereby resulting in increased energy expenditure per unit of muscle power generation both during low level exercise and during activities of daily living (1). The implications for future studies are clear. Longer term studies are needed to determine whether isocaloric resistance training versus aerobic training will result in less regain of fat mass by virtue of differential effects on muscle contractile efficiency and energy intake after weight reduction. Our data suggest that exercise prescriptions to assist in sustaining weight loss should be modified to include a greater emphasis on resistance training.
What is already known about this subject?
During reduced weight maintenance following diet-induced weight loss there is an increased skeletal muscle work efficiency that promotes adaptive thermogenesis and weight regain.
Resistance training in non-weight-reduced individuals promotes increased skeletal muscle strength but decreased efficiency.
Resistance training after weight loss might have similar effects on muscle or these changes may not occur in order to promote adaptive thermogenesis in defense of maintenance of fat mass and reproductive integrity.
What does this study add?
Individuals maintaining a reduced weight and individuals who are not weightreduced respond similarly to resistance training (increased muscle strength and decreased efficiency).
Increased resistance training could be an effective adjunct to reduced weight maintenance therapy by “reversing” changes in skeletal muscle that promote adaptive thermogenesis.
ACKNOWLEDGEMENTS
First the authors would like to thank all our subjects for their participation in this study. The authors gratefully acknowledge the assistance of Dr. Fernando Arias-Mendoza who supervised collection of NMR data. Ms. Suzanne Wright recruited patients and conducted pre-screening and screening visits at Cornell. Ms. Victoria Billero, Ms. Madeline Gantz, Ms. Wanda Truong, William Buniak and Ms. Lindsay Williams worked on this study as part of their Masters Theses at the Columbia Institute for Human Nutrition and were invaluable in working with subjects during exercise training. Dr. Wahida Karmally and members of the bionutrition unit at the Irving Center for Clinical and Translational Research provided nutritional support for subjects on testing days.
Support: These studies were supported by generous grants from William Taubman, Diane & Darryl Mallah, David Shaw, Andrea Kantor and Donna Hamann, and NIH grants RR00645, 2K24 AR 052665, UL 1 TR000040, P30-DK63068, P30-DK26687, and R01 AG045761.
Footnotes
Disclosures: These studies were supported, in part, by Equinox Fitness (New York, NY) whose generosity in allowing use of their facilities and to work with their trainer Mr. Frank Maggi was essential to this project. The authors have no other relevant disclosures.
References
- 1.Leibel R, Rosenbaum M. Metabolic response to weight perturbation In: Clément K (ed). Novel Insights into Adipose Cell Functions, Research and Perspectives in Endocrine Interactions. Springer-Verlag: Heidelberg, 2010, pp 121–133. [Google Scholar]
- 2.Rosenbaum M, Hirsch J, Gallagher D, Leibel R. Long-term persistence of adaptive thermogenesis in subjects who have maintained a reduced body weight. Amer J Clin Nutr 2008;88: 906–912. [DOI] [PubMed] [Google Scholar]
- 3.Wing R, Phelan S. Long-term weight maintenance. Amer J Clin Nutr 2005;82: 222S–225S. [DOI] [PubMed] [Google Scholar]
- 4.Kerns J, Guo J, Fothergill E, Howard L, Knuth N, Brychta R, et al. Increased physical activity associated with less weight regain six years after “The Biggest Loser” competition. Obes 2017;25: 1838–1843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Thomson D, Ivanescu A, Martin C, Heymsfield S, Marshall K, Bodrato V, et al. Predicting successful long-term weight loss from short-term weight-loss outcomes: new insights from a dynamic energy balance model (the POUNDS Lost study). Amer J Clin Nutr 2015;101: 449–454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rosenbaum M, Vandenborne K, Goldsmith R, Simoneau J, Heymsfield S, Joanisse D, et al. Effects of experimental weight perturbation on skeletal muscle work efficiency in human subjects. Am J Physiol Endocrinol Metab 2003;285: R183–192. [DOI] [PubMed] [Google Scholar]
- 7.von Loeffeholz C The role of non-exercise activity thermogenesis in human obesity In: De Groot LJ, Chrousos G, Dungan Feingold KR, Grossman A, Hershman JM, et al. (eds). Endotext. MDText.com, Inc: South Dartmouth (MA), 2014. [Google Scholar]
- 8.Green H, Goreham C, Ouyang J, Ball-Burnett M, Ranney D. Regulation of fiber size, oxidative potential, and capillarization in human muscle by resistance exercise. Am J Physiol 1999;276: R591–596. [DOI] [PubMed] [Google Scholar]
- 9.Raue U, Trappe T, Estrem S, Qian H, Helvering L, Smith R, et al. Transcriptome signature of resistance exercise adaptations: mixed muscle and fiber type specific profiles in young and old adults. J Appl Physiol 2012;112: 1625–1636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Simoneau J Adaptation of human skeletal muscle to exercise-training. Int J Obes 1995;4: S9–S13. [PubMed] [Google Scholar]
- 11.Short K, Vittone J, Bigelow M, Proctor D, Coenen-Schimke J, Rys P, et al. Changes in myosin heavy chain mrRNA and protein expression in human skeletal muscle with age and endurance exercise training. J Appl Physiol 2005;99: 95–102. [DOI] [PubMed] [Google Scholar]
- 12.American Physiological Society. Guiding principles for research involving animals and human beings. Am J Physiol Regul Integr Comp Physiol 2002;283: R281–R283. [DOI] [PubMed] [Google Scholar]
- 13.Goldsmith R, Joanisse D, Gallagher D, Pavlovich K, Shamoon E, Leibel R, et al. Effects of experimental weight perturbation on skeletal muscle work efficiency, fuel utilization, and biochemistry in human subjects. Am J Physiol 2010;298: R79–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sensormedics. VMax Reference Manual Yorba Linda, CA, 1998. [Google Scholar]
- 15.Wasserman K, Hansen J, Sue D, Casaburi R, Whipp B. Principles of Exercise Testing and Interpretation. Lippincott Williams & Wilkins: Baltimore, MD, 1999, p 36. [Google Scholar]
- 16.Kemp G, Ahmad R, Nicolay K, Prompers J. Quantification of skeletal muscle mitochondrial function by 31P magnetic resonance spectroscopy techniques: a quantitative review. Acta Physiol 2015;213: 107–144. [DOI] [PubMed] [Google Scholar]
- 17.Impellizzeri F, Bizzini M, Rampinini E, Cereda F, Maffiuletti N. Reliability of isokinetic strength imbalance ratios measured using the Cybex NORM dynamometer. Clin Physiol Funct Imaging 2008;28: 113–119. [DOI] [PubMed] [Google Scholar]
- 18.Schulze P, Linke A, Schoene N, Winkler S, Adams V, Conradi S, et al. Functional and morphological skeletal muscle abnormalities correlate with reduced electromyographic activity in chronic heart failure. Eur J Cardiovasc Prev Rehabil 2004;11: 155–161. [DOI] [PubMed] [Google Scholar]
- 19.Church T, Blair S, Cochreham S, Johannsen N, Johnson W, Karmer K, et al. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: a randomized controlled trial. JAMA 2010;304: 2253–2262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Egan A, Winchester J, Foster C, McGuigan M. Using session RPE to monitor different methods of resistance exercise. J Sports Sci Med 2006;5: 289–295. [PMC free article] [PubMed] [Google Scholar]
- 21.Garber C, Blissmer B, Deschenes M, Franklin B, Lamonte M, Lee I, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, muscloskeletal and neuromotor fitness in apparently health adults: Guidance for prescribing exercise. Med Sci Sports Exerc 2011;43: 1334–1359. [DOI] [PubMed] [Google Scholar]
- 22.Gaesser GA, Brooks GA. Muscular efficiency during steady-rate exercise: effects of speed and work rate. J Appl Physiol 1975;38: 1132–1139. [DOI] [PubMed] [Google Scholar]
- 23.McArdle W, Katch F, Katch V. Exercise Physiology. Williams & Wilkins: Baltimore, MD, 1996, pp 145–147. [Google Scholar]
- 24.Statsoft I Statistica, Release 10, 2011 Edition. Statsoft: Tulsa, OK, 2011. [Google Scholar]
- 25.Walker P, Brunotte F, Rouhier-Marcer I, Cottin Y, Casillas J, Gras P, et al. Nuclear magnetic resonance of different muscular adaptations after resistance training. Arch Phys Med Rehabil 1998;79: 1391–1398. [DOI] [PubMed] [Google Scholar]
- 26.Le D, Pannacciulli N, Chen K, Salbe A, DelParigi A, Hill J, et al. Less activation in the left dorsolateral prefrontal cortex in the reanalysis of the response to a meal in obese than in lean women and its association with successful weight loss Am J Clin Nutr 2007;86: 573–579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McCaffery J, Haley A, Sweet L, Phelan S, Raynor H, Parigi AD, et al. Differential functional magnetic resonance imaging response to food pictures in successful weight-loss maintainers relative to normal-weight and obese controls. Am J Clin Nutr 2009;90: 928–934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wing R, Hill J. Successful weight loss maintenance. Annu Rev Nutr 2001;21: 323–341. [DOI] [PubMed] [Google Scholar]
- 29.Phelan S, Wing R. Prevalance of successful weight loss. Arch Int Med 2005;165: 2430. [DOI] [PubMed] [Google Scholar]
- 30.Swift D, Johannsen N, Lavie C, Earnest C, Church T. The role of exercise and physical activity in weight loss and maintenance. Prog Cardiovasc Dis 2014;56: 441–447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Jakicic J, Otto A. Treatment and prevention of obesity: what is the role of exercise. Nutr Rev 2006;64: S57–61. [DOI] [PubMed] [Google Scholar]
- 32.Leibel R, Rosenbaum M, Hirsch J. Changes in energy expenditure resulting from altered body weight. N Eng J Med 1995;332: 621–628. [DOI] [PubMed] [Google Scholar]
- 33.Rosenbaum M, Leibel RL. Models of energy homeostasis in response to maintenance of reduced body weight. Obesity (In Press) 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ainsworth B, Haskell W, Whitt M, Irwin M, Swartz A, Strath S, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 2000;32: S498–516. [DOI] [PubMed] [Google Scholar]
- 35.Lante K, Reece J, Walkley J. Energy expended by adults with and without intellectual disabilities during activities of daily living. Res Develop Disabilities 2010;31: 1380–1389. [DOI] [PubMed] [Google Scholar]
- 36.Csizmadi I, Lo Siou G, Friedenreich C, Owen N, Robson P. Hours spent and energy expended in physical activity domains: Results from The Tomorrow Projectcohort in Alberta, Canada. Int J Behav Nutr Phys Act 2011;8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Vilcaxa Alves J, Saavedra F, Simao R, Novaes J, Rhea M, Green D, et al. Does aerobic and strength exercise sequence in the same session affect the oxygen uptake during and postexercise? J Strength Cond Res 2012;26: 1872–1878. [DOI] [PubMed] [Google Scholar]
- 38.Hunter G, Fisher G, Neumeier W, Carter S, Plaisance E. Exercise training and energy expenditure following weight loss. Med Sci Sports Exerc 2015;47: 1950–1957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Drenowatz C, Grieve G, DeMello M. Changes in energy expenditure and physical activity in response to aerobic and resistance exercise programs. Springerplus 2015;798: doi: 10.1186/s40064-40015-41594-40062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mayer J, Roy P, Mitra K. Relation between caloric intake, body weight, and physical work: studies in an industrial male population in West Bengal. Amer J Clin Nutr 1956;4: 169–175. [DOI] [PubMed] [Google Scholar]
- 41.Blundell J, Gibbons C, Caudwell P, Finlayson G, Hopkins M. Appetite control and energy balance: Impact of exercise. Obes 2015;16 (Suppl 1): 67–76. [DOI] [PubMed] [Google Scholar]
- 42.Laan D, Leidy H, Lim E, Campbell W. Effects and reproducibility of aerobic and resistance exercise on appetite and energy intake in young, physically active adults. Appl Physiol Nutr Metab 2010;35: 842–847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Jabbour G, Ianchu H, Mauriege P, Joanisse D, Martin L. High intensity interval training improve performance in young and older indivudals by increasing mechanical efficiency. Physiol Rep 2017;5: e13232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Wang E, Nyberg S, Hoff J, Zhao J, Leivseth G, Torhaug T, et al. Impact of maximal strength training on work efficiency and muscle fiber type in the elderly: Implications for physical function and fall prevention. Exp Gerontol 2017;81: 64–71. [DOI] [PubMed] [Google Scholar]
- 45.Jequier E, Acheson K, Schutz Y. Assessment of energy expenditure and fuel utilization in man. Ann Rev Nutr 1987;7: 187–208. [DOI] [PubMed] [Google Scholar]