

In 2002, Lleras-Muney published a landmark working paper using changes in Compulsory Schooling Laws (CSLs) in US states as quasi-experiments to estimate the effects of education on mortality (Lleras-Muney, 2002). This paper, although it faced several technical challenges, solved a critical problem for research on the social determinants of health: by using CSLs as instrumental variables, Lleras-Muney’s approach established causal direction, ruling out the possibility that the association between education and health reflected the influence of health (or correlates) on education. This work sparked an outpouring of studies using a similar design to evaluate educational effects on numerous health and behavioral outcomes. In this issue of Social Science and Medicine, Hamad et al present an important review of this literature (Hamad, Elser, Tran, Rehkopf, & Goodman, 2018), based on 89 manuscripts presenting over 600 effect estimates. In this commentary, we discuss why the uptake of quasi-experimental approaches in social determinants of health research is a critical advance, highlight insights to be gained from Hamad’s findings, and suggest priorities for future work.
Why are quasi-experimental approaches important for social epidemiology?
Social epidemiology aims to provide evidence on interventions to improve population health. Most epidemiologic research on social determinants of health is observational and rests on glorified versions of correlations between measures of the exposure (such as educational attainment) and health outcomes. Only if we have managed to identify, measure, and appropriately control for every common cause of education and the health outcome would we expect the effect estimates from such observational studies to correspond with effects of interventions on schooling. For example, although dozens of cohort studies provide robust evidence that individuals with more education have lower risk of dementia (Beydoun, Beydoun, Gamaldo, Teel, Zonderman, & Wang, 2014; Sharp & Gatz, 2011), these studies can rarely account for a long list of plausible confounders, such as personality, adverse childhood experiences, childhood intelligence, or childhood health. Regional CSL changes provide quasi-experiments that influence education but arguably could not otherwise influence dementia and are not plausibly influenced by the individual-level confounders of education and dementia.
Because CSL studies are vulnerable to confounding by state- or regional-level differences that may influence both CSLs and the health of residents, CSL analyses routinely control for state fixed effects (indicator variables for each state) and temporal trends. Thus, analyses identify effects based on the timing of a CSL change within a state, comparing children attending school in the state before the change in CSL to their counterparts in the same state who attended school after the change in CSLs. Although this approach does not rule out all possible state-level confounders, it narrows the list substantially and essentially rules out individual-level confounders (Glymour, Kawachi, Jencks, & Berkman, 2008; Glymour, Walter, & Tchetgen Tchetgen, 2017).
Insights from CSL research on the causal relationship between education and health
Hamad undertook meta-analyses of four health outcomes and reported significant evidence of education benefits for three of these (mortality, obesity, and smoking). However, Hamad and a related recent review (Galama, Lleras-Muney, & van Kippersluis, 2018) show that findings from quasi-experimental CSL studies are mixed, with some reporting beneficial effects and others showing no effects or adverse effects. This is in marked contrast to observational studies, which show very consistent associations. Why are findings mixed in quasi-experiments? The inconsistent results may well be due to chance. Studies using CSLs have limited statistical power because CSLs typically increase average education by only a small amount within a small range (e.g., increasing the chances a child completes 10 instead of 9 years of schooling, a 1 year difference). An observational study instead might contrast people with more than high-school to those with less than high-school. A typical person who completes more than high-school attends several extra years of education beyond that completed by a typical person with less than high-school, so the observational effect estimate corresponds with several years of extra education. It is therefore not surprising that most of the individual study effect estimates presented by Hamad et al., were imprecisely estimated, with confidence intervals consistent with either large benefits of education or no benefits.
More worrisome explanations for the mixed findings across CSL studies call for a re-examination of theorized links between education and health. Incremental changes in education induced by CSLs may not benefit all people. The use of CSLs as an instrument for education delivers an estimate applicable to those children who would have left school earlier were it not for the CSL. This estimate does not refer to the effects for children who would have attended more school even if the law was not in place or for children who dropped out of school despite the mandate. Indeed there is some evidence of heterogeneity of treatment effects across these groups (Avendano, de Coulon, & Nafilyan, 2017; Meghir & Palme, 2005). In general, mandated education may not help children from racially, culturally, socioeconomically, or linguistically marginalized communities if the laws are not enforced in those communities, if schools are hostile environments, or if students are blocked from translating additional education into labor market or income gains (Kaplan, Ranjit, & Sarah, 2008). One can even imagine adverse psychological, behavioral, and health implications for people whose educational attainment increased due to CSLs but who are forced into menial jobs due to lack of opportunity or discrimination. Consistent with this hypothesis, health returns to educational attainment among blacks have generally been lower than whites (Braveman, Cubbin, Egerter, Williams, & Pamuk, 2010; Farmer & Ferraro, 2005; Kimbro, Bzostek, Goldman, & Rodríguez, 2008), perhaps due to occupational discrimination.
Another possibility is that education is beneficial, but duration of schooling is not the aspect of educational experience that drives health outcomes. Several studies suggest that educational quality, measured in various indirect ways, improves earnings and related outcomes (Card & Krueger, 1992; Chetty, Friedman, & Rockoff, 2014; Johnson, 2011). Countless dimensions of education may be relevant to health, including quality of instruction, prestige of the educational institution, and social advantages of classmates (Ross & Mirowsky, 1999). Theoretically, the health benefits of schooling could be attributed to numerous plausible mechanisms, including resources made available within the school setting, provision of knowledge and skills, impacts on social network, and opportunities for economic and occupational advancement (Figure 1)(Cohen & Syme, 2013; Link & Phelan, 1995; Ross & Wu, 1995). Health research rarely formally evaluates these characteristics of schooling, in either the observational or quasi-experimental literature. Numerous beneficial features of schooling are correlated with duration of education because children who attend prestigious schools with high quality teachers will also likely remain in school for a longer duration. As a result, conventional observational approaches to evaluating health effects of educational attainment would misleadingly attribute any effects of school quality to effects of school duration. However, CSL estimates would show no effects because policy-mandated increases in years of school would not affect any of these characteristics of schooling.
Figure 1. Education and Health: Mechanisms Potentially Triggered by Increased Duration or Quality of Schooling.
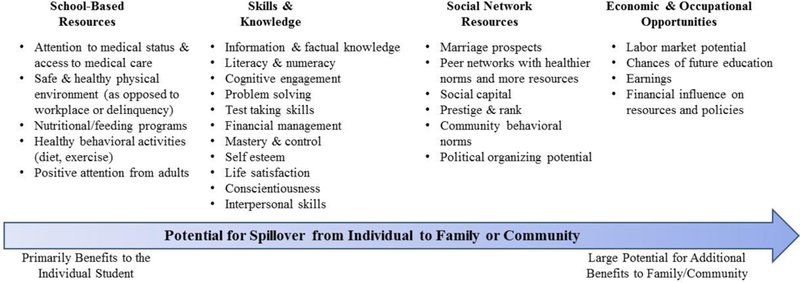
Although some benefits of schooling accrue directly to the child and have little relevance for the child’s family or community (e.g., school lunch and other feeding programs), other benefits may have spillover effects that are relevant for the health of the child’s extended network and community (e.g., earnings shared with family members).
Spillover effects may also bias the effects of education when estimated with state fixed effects (as is typical in the US based CSL literature) or within a single location (as is common in European CSL studies). Children’s receipt of additional education may pay off for the whole community, e.g., through generalized economic growth, by establishing healthier behavioral norms, or because the resources gained from education (money, knowledge) are shared with the student’s spouse, extended family, and social network (Figure 1). By including state fixed effects, we remove such spillover benefits from the estimate of CSLs on health outcomes. Prior evidence supports spillover effects from education and income to family or community members (Barrientos & Sabates-Wheeler, 2011; Case, 2004; Torssander, 2013). Spillovers between spouses seem very likely if earnings are a major mechanism via which education influences health. If so, CSL-based analyses will underestimate the effects of education, because married couples are not usually in the same birth cohort(Presser, 1975). Women in the first cohorts born under a recently increased CSL will typically marry older men, who would have been born under the previous, shorter CSL, and estimated benefits of education will be blunted in these cohorts. Acemoglu and Angrist tried to disentangle the individual from social benefits of education, by contrasting instrumental variable estimates using month of birth (which varies at the individual level) to those using state CSLs (which vary at the state level) (Acemoglu & Angrist, 2000). Although month of birth may violate the assumptions for a valid instrumental variable, identifying community health benefits of educational interventions is an important challenge.
Additionally, the spillover effects of increasing mandatory education are not necessarily beneficial. Enforced CSL increases could result in enrolling many additional children in school, differentially children from low socioeconomic status backgrounds. Unless accompanied by new instructional and classroom resources, this may lead to a deterioration in the quality of schooling, though some evidence suggests that CSLs did not negatively impact school quality in the US (Sansani, 2015).
Future directions: is it important to rigorously evaluate the health effects?
Exploring the possibility of heterogeneous effects of education on health for different groups of children, particularly by socioeconomic background, sex/gender, race/ethnicity, geographic region, and intersectional categories is critical for progress. Given statistical power limitations in quasi-experimental studies, this will most likely need to be pursued in both observational and quasi-experimental settings. If increases in educational attainment are not translating to health benefits for everyone, or for anyone, health equity considerations demand that we research this and understand why. The mixed results to date suggest that structural discrimination may differentially undermine the health benefits of education for black men. We need to study such phenomena to guide efforts to improve the health of black men and to carefully target limited resources to improve health of vulnerable populations by improved understanding of the mechanisms of education effects on health; which aspects of schooling convey health benefits; which health outcomes are most impacted; and the ways in which structural discrimination may limit health benefits. Future research in this area should prioritize larger sample sizes with enough power to evaluate interactions between instrumental variables and race/ethnicity, sex/gender, and geographic region. Ideally, follow-up of birth cohort and school-based studies that directly collected information during childhood or adolescence could be used to refine estimates of the differential contribution of individual ability from educational policy (Conti, Heckman, & Urzua, 2010). As for-profit and other non-traditional educational venues become increasingly common (Gelbgiser, 2018), we also urgently need more comprehensive evaluations of how quality, peer-group, type, and level of school modify the health benefits of education.
In conclusion, we hope the challenges Hamad identifies in her manuscript are taken up by researchers evaluating social determinants of health. The findings to date suggest that the causal effects of length of schooling are not necessarily as unequivocally and overwhelmingly positive as would be suggested by the observational literature. The next generation of research in this area needs to pursue mechanisms and mediators, with a more focused effort to build theoretical understanding of which aspects of education are beneficial and how those effects differ between individuals and across social contexts.
Acknowledgments:
The authors gratefully acknowledge contributions of Audrey Murchland to this manuscript and funding from the National Institute on Aging RF1 AG056164.
References
- Acemoglu D, & Angrist J. (2000). How large are human-capital externalities? Evidence from compulsory schooling laws. NBER macroeconomics annual, 15, 9–59. [Google Scholar]
- Avendano M, de Coulon A, & Nafilyan V. (2017). Does more education always improve mental health? Evidence from a British compulsory schooling reform: HEDG, c/o Department of Economics, University of York. [Google Scholar]
- Barrientos A, & Sabates-Wheeler R. (2011). Strategic complementarities and social transfers: how do PROGRESA payments impact nonbeneficiaries? Applied Economics, 43(23), 3175–3185. [Google Scholar]
- Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, & Wang Y. (2014). Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC public health, 14(1), 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braveman PA, Cubbin C, Egerter S, Williams DR, & Pamuk E. (2010). Socioeconomic disparities in health in the United States: what the patterns tell us. American journal of public health, 100(S1), S186–S196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Card D, & Krueger AB (1992). Does school quality matter? Returns to education and the characteristics of public schools in the United States. Journal of political Economy, 100(1), 1–40. [Google Scholar]
- Case A. (2004). Evidence from South African Pensions. Perspectives on the Economics of Aging, 287. [Google Scholar]
- Chetty R, Friedman JN, & Rockoff JE (2014). Measuring the impacts of teachers II: Teacher value-added and student outcomes in adulthood. American Economic Review, 104(9), 2633–2679. [Google Scholar]
- Cohen AK, & Syme SL (2013). Education: a missed opportunity for public health intervention. American journal of public health, 103(6), 997–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conti G, Heckman J, & Urzua S. (2010). The education-health gradient. American Economic Review, 100(2), 234–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farmer MM, & Ferraro KF (2005). Are racial disparities in health conditional on socioeconomic status? Social science & medicine, 60(1), 191–204. [DOI] [PubMed] [Google Scholar]
- Galama TJ, Lleras-Muney A, & van Kippersluis H. (2018). The Effect of Education on Health and Mortality: A Review of Experimental and Quasi-Experimental Evidence: National Bureau of Economic Research. [Google Scholar]
- Gelbgiser D (2018). College for all, degrees for few: for-profit colleges and socioeconomic differences in degree attainment. Social Forces, 96(4), 1785–1824. [Google Scholar]
- Glymour MM, Kawachi I, Jencks CS, & Berkman LF (2008). Does childhood schooling affect old age memory or mental status? Using state schooling laws as natural experiments. Journal of Epidemiology and Community Health, 62(6), 532–537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glymour MM, Walter S, & Tchetgen Tchetgen EJ (2017). Natural Experiments and Instrumental Variables Analyses in Social Epidemiology In Oakes J, & Kaufman J. (Eds.), Methods in Social Epidemiology (pp. 493–537). San Francisco, CA: Jossey-Bass. [Google Scholar]
- Hamad R, Elser H, Tran DC, Rehkopf DH, & Goodman SN. (2018). How and why studies disagree about the effects of education on health: A systematic review and meta-analysis of studies of compulsory schooling laws. Social Science & Medicine, 212, 168–178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson RC (2011). Long-run impacts of school desegregation & school quality on adult attainments: National Bureau of Economic Research. [Google Scholar]
- Kaplan G, Ranjit N, & Sarah B. (2008). Lifting Gates—Lengthening Lives: Did Civil Rights Policies Improve the Health of African-American Women in the 1960s and 1970s? In Schoeni R,House J,Kaplan G, & Pollack H. (Eds.), Making Americans Healthier: Social and Economic Policy As Health Policy (pp. 145–170). New York: Russell Sage Foundation. [Google Scholar]
- Kimbro RT, Bzostek S, Goldman N, & Rodríguez G. (2008). Race, ethnicity, and the education gradient in health. Health Affairs, 27(2), 361–372. [DOI] [PubMed] [Google Scholar]
- Link BG, & Phelan J. (1995). Social conditions as fundamental causes of disease. Journal of Health & Social Behavior., Spec, 80–94. [PubMed] [Google Scholar]
- Lleras-Muney A. (2002). The Relationship Between Education and Adult Mortality in the United States: National Bureau of Economic Research. [Google Scholar]
- Meghir C, & Palme M. (2005). Educational reform, ability, and family background. American Economic Review, 95(1), 414–424. [Google Scholar]
- Presser HB (1975). Age Differences Between Spouses: Trends, Patterns, and Social Implications. American Behavioral Scientist, 19(2), 190. [Google Scholar]
- Ross CE, & Wu C. l. (1995). The links between education and health. American sociological review, 719–745. [Google Scholar]
- Ross CE, & Mirowsky J. (1999). Refining the association between education and health: The effects of quantity, credential, and selectivity. Demography, 36(4), 445–460. [PubMed] [Google Scholar]
- Sansani S. (2015). The differential impact of compulsory schooling laws on school quality in the United States segregated South. Economics of Education Review, 45, 64–75. [Google Scholar]
- Sharp ES, & Gatz M. (2011). The relationship between education and dementia an updated systematic review. Alzheimer disease and associated disorders, 25(4), 289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torssander J. (2013). From child to parent? The significance of children’s education for their parents’ longevity. Demography, 50(2), 637–659. [DOI] [PubMed] [Google Scholar]