

History
Identifying spinal instability plays a vital role in the management of patients with metastatic spinal disease. To appropriately triage and treat patients who would benefit from surgical intervention, an accurate assessment of neoplastic spinal instability is imperative. Until recently, there was no consensus about how best to classify spinal instability in patients with neoplastic disease of the spine [14].
In the absence of robust evidence on this topic, knowledge about degenerative or traumatic instability has been applied to metastatic disease of the spine. However, such interpretations are problematic because pathologic fractures do not follow the usual patterns seen in patients with trauma and osteoporosis [5]. As opposed to traumatic conditions, ligaments and discs are less commonly affected by tumors, and the ability of the spine to heal is compromised [5]. Thus, classifications of spinal instability based on trauma may not be applicable to tumors.
With a lack of guidelines, physicians have relied on clinical experience to determine whether instability is present in patients with spinal neoplasia [6]. For the non-surgeon, difficulty diagnosing spinal instability can lead to inappropriate referrals of patients without instability or undertreatment of patients with instability. This highlights the need for a classification system to facilitate communication and to help identify which lesions are unstable and may benefit from evaluation by a spine surgeon. In 2010, the Spinal Oncology Study Group introduced the Spinal Instability Neoplastic score (SINS) to standardize the diagnosis of spinal instability in patients with neoplastic disease [6]. The Spinal Oncology Study Group, an international group of 30 spine oncology experts, developed the SINS using an evidence-based medicine process incorporating the best available studies and expert-opinion consensus.
Purpose
The spine is the most common site of malignant skeletal metastasis [3]; therefore, metastatic disease of the spine is a prevalent problem. In North America, approximately 18,000 patients are diagnosed with metastatic disease of the spine each year [16]. The incidence is increasing as detection methods improve and treatments of primary cancers allow patients with active disease to have a longer life expectancy [6]. Treatment advancements include improvement in adjuvant therapy, namely radiotherapy and chemotherapy. Although advancements in adjunct therapies have offered more treatment options, instability because of spinal metastasis remains an important indication for surgical intervention [5]. However, before the SINS was developed, no reliable criteria to assess instability risk in these patients had been established [2].
Spinal instability is the loss of spinal integrity because of a neoplastic process associated with movement-related pain, symptomatic or progressive deformity, and/or neural compromise under physiological loads [6]. Despite this definition, diagnosing spinal stability was difficult because of the lack of consensus guidelines rating the relevance and validity of specific clinical and imaging findings [8]. The assessment of tumor-related spinal instability is challenging for spine surgeons and is even more demanding for other non-surgical members of the multidisciplinary team [7]. Therefore, SINS was developed to help physicians assess and categorize spinal instability; facilitate communication and appropriate referrals between oncologists, radiologists, and spine surgeons; and ensure that prompt and appropriate treatment plans can be developed.
Description
The SINS is a scoring system based on one clinical factor (pain) and five radiographic parameters (location, bone lesion quality, spinal alignment, vertebral body collapse and involvement of posterolateral spinal elements) [4] (Fig. 1). Each component is assigned a score reflecting its contribution to overall instability of the spinal segment. The six individual scores of each component are added for a cumulative score ranging from 0 to 18. A higher the total score signals more severe instability. If multiple segments are involved, the total score applies separately to each lesion [5]. If there are multiple lesions in the spine, a separate SINS is calculated for each lesion. As described by Fisher et al. [6], the six components that make up the SINS are as follows:
Fig. 1.
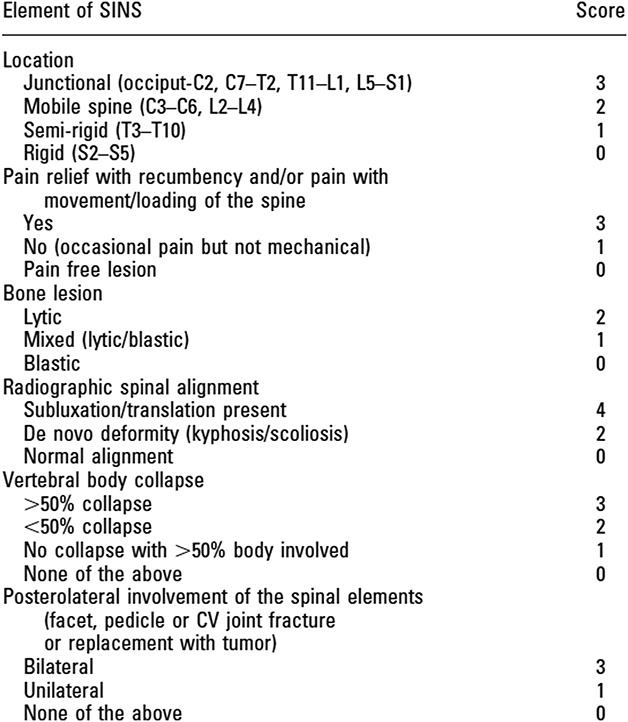
This figure shows the SINS scoring system. CV joint = costovertebral joint. Reprinted with permission from Wolters Kluwer Health Inc: Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fourney DR. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine. 2010;35:E1221-1229. Available at: https://journals.lww.com/spinejournal/Abstract/2010/10150/A_Novel_Classification_System_for_Spinal.19.aspx.
Location
This component reflects inherent stability based on the location of the lesion on the spine. A tumor at a junctional level (C0 to C2, C7 to T2, T11 to L1, and L5 to S1) is assigned the highest possible score of 3. Tumors located in mobile segments (C3 to C6 and L2 to L4) receive a score of 2, whereas lesions located in somewhat rigid segments (T3 to T10) receive a score of 1. Tumors in the most rigid sacral spine (S2 to S5) receive a score of 0.
Mechanical Pain
This component is the only clinical parameter of the six total factors. It considers the presence of mechanical pain associated with the tumor. Pain present with movement, upright posture, or loading of the spine but relieved by recumbence (mechanical pain) indicates instability. These tumors receive a high score of 3. Painful lesions without mechanical characteristics are assigned a score of 1 and painless lesions receive a score of 0. In describing spinal instability due to spinal metastases, many authors have used the presence of mechanical back pain, defined as pain aggravated by movement and relieved by recumbency, as the critical symptom for the presence of spinal instability [26].
Bone Lesion Quality
The bone quality of the lesion is considered to affect spinal instability. Compared with blastic or mixed tumors, lytic tumors are unstable and are thus assigned a high score of 2. Mixed blastic and lytic lesions receive a score of 1, while blastic lesions do not add any value (scored as zero) to the total score.
Spinal Alignment
This component is assessed via serial radiographs or by comparing supine and upright radiographs. Lesions associated with subluxation or translation receive a score of 4, denoting the highest possible contribution to instability in this subsection and throughout the entire cumulative score. A de novo deformity (kyphosis or scoliosis) without subluxation or translation receives a score of 2, and normal alignment receives a score of 0 [6].
Vertebral Body Collapse
This component considers the extent of vertebral body involvement and collapse. The greater the involvement and collapse, the greater the instability and hence a higher score. Tumors with greater than 50% collapse receive 3 points, those with less than 50% collapse receive 2 points, those with no collapse but greater than 50% vertebral body involvement receive a score of 1, and those with no collapse and less than 50% vertebral body involvement receive a score of 0 [15].
Posterolateral Involvement of Spinal Elements
Lesions involving the posterior elements of the spine adversely affect stability, underscoring the importance of these elements. Bilateral involvement of the pedicles, facets, and/or costovertebral joints indicates higher instability; thus, such lesions receive a score of 3. Tumors with unilateral posterior involvement receive a score of 1, whereas no tumor involvement in the posterior elements is assigned a score of 0.
The total SINS is generated by adding the six individual component scores. The total score stratifies patients into three categories of stability: stable (0 to 6 points), potentially unstable (7 to 12 points), and unstable (13 to 18 points). In addition, the SINS can also be analyzed as a binary indicator of surgical referral status: patients with a score from 0 to 6 points have a stable spine and do not generally need to be referred for evaluation of spinal stability, whereas those with scores from 7 to 18 points warrant referral for evaluation of potential instability [4]. Although the SINS does not provide treatment recommendations, surgical consultation is recommended for patients with a score of at least 7 [6].
Validation
Seven studies have assessed the reproducibility of the SINS [1, 2, 7-10, 23] (Table 1). These studies assessed agreement using either the intraclass correlation coefficient (ICC) [1, 2, 7, 9, 10] or the kappa (κ) coefficient [8, 23]. The ICC and κ values are used to assess the level of agreement between observers that is beyond what would occur by chance alone. Values range from 0 to 1; 0 indicates any agreement because of chance while 1 represents perfect agreement [12]. The criteria for determining the level of agreement were described by Landis and Koch [18]: (1) κ > 0.80, almost perfect; (2) κ = 0.61 to 0.80, substantial; (3) κ = 0.41 to 0.60, moderate; (4) κ = 0.21 to 0.40, fair; (5) κ = 0.00 to 0.20, slight.
Table 1.
Reproducibility of the SINS

Kappa statistics are used to compare categorical variables [20, 22]. With respect to the SINS, these categories are stable, potentially unstable, and unstable. The ICC is used to assess agreement on a continuous scale [20, 22], which is the total SINS score from 0 to 18. The level of agreement based on ICC can be evaluated as follows [17]: (1) κ > 0.90, excellent; (2) κ = 0.76 to 0.89, good; (3) κ = 0.5 to 0.75, moderate; (4) κ = 0.5, poor.
Reliability studies evaluating the SINS have had heterogenous reporting methods. In five studies that assessed the SINS using the ICC [1, 2, 7, 9, 10], the interrater reliability was good to near perfect (ICC = 0.55 to 0.99). Intraobserver reproducibility was good to excellent (ICC = 0.77 to 0.96) [1, 2, 7, 9, 10]. Studies that reported using the κ statistic [8, 23] found only fair-to-moderate interrater agreement (κ = 0.38 to 0.53). One study did not report intraobserver reproducibility [23]; one that did showed substantial reproducibility (κ = 0.69) [8].
Studies that have assessed reliability have used raters from various medical specialties and skill levels including members of the Spine Oncology Study Group [9], radiologists [8], radiation oncologists [7], multidisciplinary teams including fellowship-trained spine surgeons, medical oncologists, radiation oncologists and radiologists [1, 2, 23] and orthopaedic residents, neurosurgery residents, and spine fellows [10]. Teixeira et al. [23] showed increased interrater reliability with increasing experience when spine surgeons were compared with non-spine surgeons. However, other studies have shown that differing specialties [1, 2] and experience [1] did not affect interrater reproducibility.
The SINS has not been prospectively validated; however, several studies have attempted to validate the scoring system indirectly. In one study, 98.7% of patients who were assessed to have unstable or potentially unstable spines (SINS of at least 7) would have been identified by radiologists when a consensus among spine surgeons was used as a reference [8]. In a similar study, radiation oncologists would have identified and referred 97% of patients with unstable or potentially unstable spines using the same reference standard [7]. In patients who have undergone surgical stabilization, those with unstable and potentially unstable spines according to the SINS have also been shown to have higher levels of preoperative pain and functional limitations. This would be expected as pain is a component of the SINS. However, after subsequent surgical stabilization, these patients demonstrated an improvement in both pain and functional status postoperatively [14]. Furthermore, a lower SINS has been associated with a better response of pain to palliative radiotherapy, indicating that the SINS may be effective in identifying mechanical spinal instability [24].
Since its publication, the SINS has been adopted in several clinical practice guidelines and decision frameworks for patients with spinal metastases. It has been incorporated into an evaluation criteria for patients with spinal metastases; which includes four critical assessments: neurologic (N), oncologic (O), mechanical stability (M) and systemic disease (S) which together form the NOMS clinical decision framework [19]. Furthermore, the American College of Radiology incorporated SINS in their practice guideline for metastatic spinal cord compression and recurrent metastatic disease [26]. The American Academy of Orthopedic Surgeons incorporated SINS as classification for spinal instability in an institutional lecture on the management of patients with bone metastases for general practitioners [26]. However, the impact of using the SINS on clinical practice (such as referrals to spine surgeons and surgical decision making) needs further assessment via additional studies.
Limitations
The SINS is meant to be only one component of the evaluation process when the physician considers surgical referral or planning [4, 6]. Clinical situations and individual patient factors, such as the presence of neurologic deficits or high-grade spinal cord compression, may supersede the SINS. These factors may lead to surgical intervention regardless of the SINS. Various factors that are not accounted for in the SINS system, such as multilevel (contiguous) spinal disease, previous laminectomies, other surgical procedures, previous radiation therapy (including radiosurgery), the extent of diffuse bony involvement of metastatic disease, and poor bone quality, might contribute to spinal instability [6]. Other issues including patient body weight and activity level may also influence spinal loading and impending instability. All factors must be considered when assessing global spinal stability in patients with neoplastic disease. There are limitations to using the SINS for patients with widespread or multilevel spinal disease. These factors are a unique challenge because each tumor dictates its own SINS by virtue of its location and radiographic characteristics [14].
The SINS was primarily developed to serve as a referral tool for spine surgeons and its prognostic value is controversial. Studies have investigated the prognostic value of the SINS; however, the quality of evidence in these studies has been rated low and the results or conclusions drawn from them have been mixed [26].
Many authors agree that in the setting of metastatic spinal disease, a higher SINS indeed correlates with greater instability; however, the SINS may be limited in how it reflects this concept. In its current form, the total SINS is calculated by the sum of the individual components, some of which quantify the risk of instability (location, lesion quality), whereas others quantify the degree of instability (mechanical pain, deformity). However, this ignores the fact that some combination of components with the same final score are more unstable than others. We may therefore argue that certain components should have a greater weight toward the final score as they more closely correlate with spinal instability [26].
Teixeira et al. [23] showed that the experience or background of the physician may affect the degree of agreement between the total SINS and different components of the SINS. In their study, highly experienced spine surgeons had a higher level of agreement than less-experienced spine surgeons. This indicates that less-experienced physicians may need some training. However, other studies have shown that specialty and experience have little impact on the degree of agreement [1, 2]. Since primary care physicians and medical oncologists are initially assessing these patients, further studies are necessary to assess whether the level of agreement on the SINS is affected when considering these two specific non-spine specialties.
Furthermore, an increased SINS is associated with a worse prognosis that may complicate surgical intervention. De Oliviera et al. [4] assessed the association between the SINS and the Tokuhashi Scoring System and found an inverse relationship between these scoring systems. The Tokuhashi Scoring System is a widely used tool to determine prognosis in patients with metastatic spinal disease. In this study, patients with an unstable spine had a mean Tokuhashi Scoring System score of 6.28, indicating a life expectancy of less than 6 months [4]. In these situations, treatment decisions must be evaluated individually by considering the predicted longevity for each patient among other factors.
The SINS has yet to be validated in prospective studies. Some investigators have attempted to validate the SINS indirectly by comparing consensus to a reference standard [7, 8] or evaluating outcomes after treatment [14, 24]. The prospective application of SINS in different patient populations is needed to determine the validity and application of this tool for therapeutic decision making.
Conclusions
The SINS scoring system is a reproducible tool across multiple medical specialties that can be used to indicate the stability of a spinal metastatic lesion. It has filled a void, serving as a standard reference to evaluate the degree of spinal instability. It improves communication between specialties and facilitates appropriate referrals among spine oncology specialists. As a result, using SINS in patients with metastatic spinal disease standardizes the diagnosis of spinal instability and may result in earlier appropriate referrals for surgical intervention [25]. An increasing number of studies have supported additional clinical uses of the SINS. It may guide the selection and identification of patients who may benefit the most from radiotherapy [11, 13, 21] and may even be useful in predicting the survival of patients with metastatic spinal disease [21]. Although the relatively high reproducibility of the SINS among multiple medical specialties is encouraging, additional studies are needed to determine the validity of the SINS in prospective studies.
Footnotes
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his institution waived approval for the reporting of this investigation and that all investigations were conducted in conformity with ethical principles of research.
References
- 1.Arana E, Kovacs FM, Royuela A, Asenjo B, Perez-Ramirez U, Zamora J. Spine Instability Neoplastic score: agreement across different medical and surgical specialties. Spine J. 2016;16:591-599. [DOI] [PubMed] [Google Scholar]
- 2.Campos M, Urrutia J, Zamora T, Roman J, Canessa V, Borghero Y, Palma A, Molina M. The Spine Instability Neoplastic Score: an independent reliability and reproducibility analysis. Spine J. 2014;14:1466-1469. [DOI] [PubMed] [Google Scholar]
- 3.Chang SY, Ha JH, Seo SG, Chang BS, Lee CK, Kim H. Prognosis of single spinal metastatic tumors: predictive value of the Spinal Instability Neoplastic Score system for spinal adverse events. Asian Spine J. 2018;12:919-926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.de Oliveria M, Rotta J, Botelho R. Is there a relationship between spinal instability in disease and Tokuhashi scoring system? Neurosurg Rev. 2016;39:519-524. [DOI] [PubMed] [Google Scholar]
- 5.Filis AK, Aghayev KV, Doulgeris JJ, Gonzalez-Blohm SA, Vrionis FD. Spinal neoplastic instability: biomechanics and current management options. Cancer Control. 2014;21:144-150. [DOI] [PubMed] [Google Scholar]
- 6.Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan KT, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fourney DR. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine. 2010;35:E1221-1229. [DOI] [PubMed] [Google Scholar]
- 7.Fisher CG, Schouten R, Versteeg AL, Boriani S, Varge PP, Rhines LD, Kawahara N., Fourney D., Weir L, Reynolds JJ, Sahgal A, Fehlings MG, Gokaslan ZL. Reliability of the Spinal Instability Neoplastic Score (SINS) among radiation oncologists: an assessment of instability secondary to spinal metastases. Radiat Oncol. 2014;9:69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fisher CG, Schouten R, Versteeg AL, Boriani S, Varge PP, Rhines LD, Kawahara N., Fourney D., Weir L, Reynolds JJ, Sahgal A, Fehlings MG, Gokaslan ZL. Reliability of the spinal instability neoplastic scale among radiologists: an assessment of instability secondary to spinal metastases. AJR Am J Roentgenology. 2014;203:869-874. [DOI] [PubMed] [Google Scholar]
- 9.Fourney DR, Frangou EM, Ryken TC, Dipaola CP, Shaffrey CI, Berven SH, Bilsky MH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutosi MG, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NG, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fisher CG. Spinal Instability Neoplastic score: an analysis of reliability and validity from the spine oncology study group. J Clin Oncol. 2011;29:3072-3077. [DOI] [PubMed] [Google Scholar]
- 10.Fox S, Spiess M, Hnenny L, Fourney DR. Spinal Instability Neoplastic Score (SINS): Reliability among spine fellows and resident physicians in orthopedic surgery and neurosurgery. Global Spine J. 2017;7:744-748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gallizia E, Apicella G, Cena T, Di Genesio Pagliuca M, Deantonio L, Krengli M. The Spine Instability Neoplastic score (SINS) in the assessment of response to radiotherapy for bone metastases. Clin Transl Oncol. 2017;19:1382-1387. [DOI] [PubMed] [Google Scholar]
- 12.Garbuz DS, Masri BA, Esdaile J, Duncan CP. Classification systems in orthopaedics. J Am Acad Orthop Surg. 2002;10:290-297. [DOI] [PubMed] [Google Scholar]
- 13.Huisman M, van der Velden JM, van Vulpen M, van den Bosch MA, Chow E, Oner FC, Yee A, Verkooijen HM, Verlaan JJ. Spinal instability as defined by the Spinal Instability Neoplastic score is associated with radiotherapy failure in metastatic spinal disease. Spine J. 2014;14:2835-2840. [DOI] [PubMed] [Google Scholar]
- 14.Hussain I, Barzilai O, Reiner AS, DiStefano N, McLaughlin L, Ogilvie S, Bilsky M, Laufer I. Patient-reported outcomes after surgical stabilization of spinal tumors: symptom-based validation of the Spinal Instability Neoplastic score (SINS) and surgery. Spine J. 2018;18:261-267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ivanishvili Z, Fourney DR. Incorporating the Spine Instability Neoplastic score into a treatment strategy for spinal metastasis: LMNOP. Global Spine J. 2014;4:129-136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kaloostian PE, Yurter A, Zadnik PL, Sciubba DM, Gokaslan ZL. Current paradigms for metastatic spinal disease: an evidence-based review. Ann Surg Oncol. 2014;21:248-262. [DOI] [PubMed] [Google Scholar]
- 17.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr. 2016;15:155-163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159-174. [PubMed] [Google Scholar]
- 19.Laufer I, Rubin DG, Lis E, Cox BW, Subblefield MD, Yamada Y, Bilsky MH. The NOMS framework: approach to the treatment of spinal metastatic tumors. Oncologist. 2013;18:744-751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mandrekar JN. Measures of interrater agreement. J Thoracic Oncol. 2011;6:6-7. [DOI] [PubMed] [Google Scholar]
- 21.Masuda K, Ebata K, Yasuhara Y, Enomoto A, Saito T. Outcomes and prognosis of neurological decompression and stabilization for spinal metastasis: Is assessment with the Spinal Instability Neoplastic score useful for predicting surgical results? Asian Spine J. 2018;12:846-853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ranganathan P, Pramesh CS, Aggarwal R. Common pitfalls in statistical analysis: Measures of agreement. Perspect Clin Res. 2017;8:187-191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Teixeira WG, Coutinho PR, Marchese LD, Narazaki DK, Cristante AF, Teixeira MJ, de Barros Filho TEP, de Camargo OP. Interobserver agreement for the spine instability neoplastic score varies according to the experience of the evaluator. Clinics (Sao Paulo). 2013;68:213-218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.van der Velden JM, Versteeg AL, Verkooijen HM, Fisher CG, Chow E, Oner FC, van Vulpen M, Weir L, Verlaan JJ. Prospective evaluation of the relationship between mechanical stability and response to palliative radiotherapy for symptomatic spinal metastases. Oncologist. 2017;22:972-978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Versteeg AL, van der Velden JM, Verkooijen HM, van Vulpen, Oner FC, Fisher CG, Verlaan JJ. The effect of introducing the Spinal Instability Neoplastic score in routine clinical practice for patients with spinal metastases. Oncologist. 2016;21:95-101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Versteeg AL, Verlaan JJ, Sahgal A, Mendel E, Quraishi NA, Fourney DR, Fisher CG. The Spinal Instability Neoplastic score: Impact on oncologic decision-making. Spine. 2016;41(Suppl 20):S231-s237. [DOI] [PubMed] [Google Scholar]