

Abstract
BACKGROUND:
Cutaneous B-cell lymphomas represent about 25% of all cutaneous lymphomas. Peripheral diffuse large B-cell lymphoma of the leg type is the most aggressive subtype seen mainly in elderly patients. Treatment is not standardised.
CASE REPORT:
An 87-year-old female patient was presented in May 2018 because of the development of painless subcutaneous nodules on the legs since late 2017. On examination, we observed up to 5 cm large erythematous nodules on the legs and a smaller plaque in the left submammary fold. The histology of a skin demonstrated tumour infiltrate that was separated from the overlying epidermis by a grenz zone. It consisted of densely packed, blastoid lymphocytic cells with numerous, and some atypical mitoses. The cells were positive for CD20, CD79A and CD5. Almost 100% of the cells were labelled with Ki67. The diagnosis of a diffuse large B-cell lymphoma (PCLBCL-LT) of the leg was confirmed. Histologic analysis of a bone marrow biopsy demonstrated a hypercellular bone marrow without malignant lymphatic infiltrates. Diagnostic ultrasound of cervical nodes and computerised tomography (CT) scans (native and with contrast medium) of head, neck and trunk excluded an extracutaneous manifestation of the PCLBCL-LT. Treatment with rituximab plus bendamustibe was initiated, but tumour progress was noted after the second course. Suggested palliative therapy with radiation and rituximab was refused. The patient died 7 months after diagnosis.
CONCLUSIONS:
Although some trials suggested a beneficial effect of immuno-chemotherapy, the prognosis of (PCLBCL-LT) remains poor. Standardised treatment is missing due to the relative rarity of this malignancy.
Keywords: Cutaneous lymphomas, Peripheral diffuse large B-cell lymphoma of the leg-type, Immunochemotherapy, Rituximab, Bedamustine, Histopathology
Introduction
Among all primary cutaneous lymphomas, B-cell lymphomas (CBCL) represent the minority with 25% of all cases. Their diagnosis is based on histopathology, immunohistochemistry, and staging evaluation. There are 3 types of primary (CBCL): primary cutaneous marginal zone lymphoma, primary cutaneous follicle centre lymphoma, and primary cutaneous diffuse large B-cell lymphoma, leg-type and NOS-type (not otherwise specified) [1]. Since these malignancies have the same morphology as their systemic counterparts, the diagnosis is one of exclusion of extracutaneous manifestation.
Cutaneous large B-cell lymphomas that contain a majority (≥ 80%) of large-cells and a proliferative rate ≥ 40% need further subtyping into diagnosis between leg type peripheral B-cell lymphoma (PCLBCL-LT) or primary cutaneous follicle centre lymphoma with large cell morphology (PCFCL-LC), and unclassified lymphomas (PCLBCL/NOS). Both CD10 and MUM1 are characteristic for the leg-type [2]. Patients with PCLBCLs-LT are on average older than those with (PCLBCL/NOS) and express more Bcl-2. Negative prognostic markers are Bcl-2, MYC rearrangements, and female gender, while proliferation rate (Ki67) is not of prognostic significance. Overall survival (OS) is poorer for PCLBCL-LT than PCFCL-LC or PCLBCL/NOS [2], [3], [4].
Case Report
An 87-year-old female patient presented in May 2018 because of the development of painless subcutaneous nodules on the legs since late 2017. Past medical history was positive for a basal cell carcinoma of the nose which had been surgically removed in 2016, bilateral knee replacement and a large goitre.
On examination, we observed up to 5 cm large erythematous nodules on the legs and a smaller plaque in the left submammary fold (Figure 1).
Figure 1.
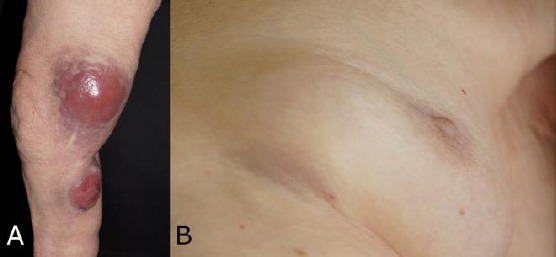
Primary cutaneous diffuse large B-cell lymphoma, leg-type; A) Large tumour nodules of the legs; B) Tumor plaque of the left submammary fold
A skin biopsy was performed. The tumour infiltrates separated from the overlying epidermis by a grenz zone. It consisted of densely packed, blastoid lymphocytic cells with numerous, and some atypical mitoses (Figure 2).
Figure 2.
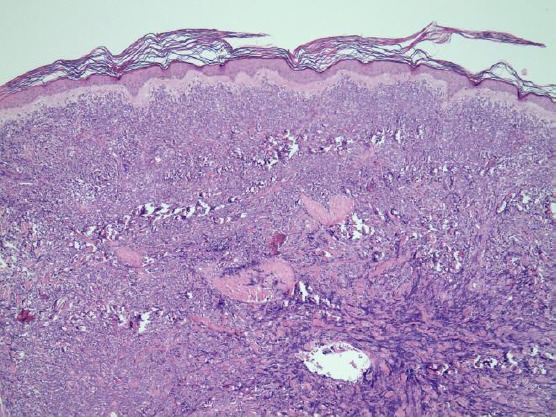
Histopathology of primary cutaneous diffuse large B-cell lymphoma, leg-type, with a grenz zone and blastoid lymphocytic cells of the dermis (Hematoxylin-eosin x 2)
The cells were positive for CD20, CD79A and CD5. Almost 100% of the cells were labelled with Ki67 (Figure 3). There was no reactivity with antibodies against CD10, CD30, Bcl-2, Bcl-6, cylin D1 and SOX11. The diagnosis of a diffuse large B-cell lymphoma (PCLBCL-LT) of the leg was confirmed.
Figure 3.
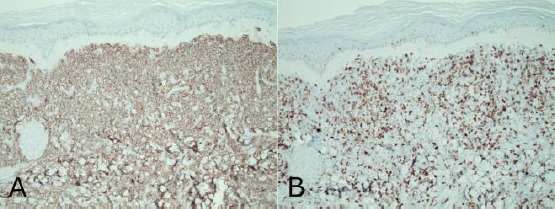
Immunohistology of primary cutaneous diffuse large B-cell lymphoma, leg-type, peroxidase stain; A) CD20 (x 10); B) Ki67 (x 10)
Histologic analysis of a bone marrow biopsy demonstrated a hypercellular bone marrow without malignant lymphatic infiltrates. Diagnostic ultrasound of cervical nodes and computerised tomography (CT) scans (native and with contrast medium) of head, neck and trunk demonstrated the giant goitre but no hints of an extracutaneous manifestation of the PCLBCL-LT were found. Laboratory investigations: Initially, we observed a leucopenia of 3.29 Gpt/L (Normal range: 3.8-11.0), increased lactate dehydrogenase of 5.33 µkat/L (2.25-3.55), beta-2-microglobulin 3.3 mg/L (0.8-2.4), and strongly increased soluble interleukin-2 receptor of 1,188 U/mL (223-710). In the differential blood count, there was a lymphopenia of 8%.
She was presented to the interdisciplinary tumour board. Combination of rituximab / bendamustin therapy was initiated, and adjuvant neutropenia prophylaxis with granulocyte-colony stimulation factor (Neupogen®) was administered. Infection prophylaxis with trimethoprim – sulfamethoxazole, and substitution with folic acid and vitamin B12 completed the medical treatment. She has undergone two cycles but experienced progress of the disease after an initial partial response. Therefore, palliative radiotherapy, in combination with rituximab once a week was planned. Tumour nodules increased by size and by number, the larger ones exulcerated. The patients rejected the suggested palliative treatment. She died 7 months after confirmation of the diagnosis.
Discussion
PCLBCL-LT is clinically more aggressive than other primary cutaneous B-cell lymphomas. This malignancy usually affects elderly females (mean age 76 years) and presents with rapidly progressive tumour nodules of the lower legs. The treatment is more challenging since PCLBCL-LT usually require multi-agent chemotherapy (cyclophosphamide, doxorubicin or epirubicin, vincristine, prednisone) and anti-CD20 monoclonal antibodies as their systemic counterparts [5], [6]. Most patients present with disease confined to the leg(s). Although only a few reports are available, the use of R-CHOP (with anti-CD20 monoclonal antibody rituximab) in these patients is associated with disease-free survival rates comparing to those of patients with high-risk systemic diffuse large B-cell lymphomas. Field radiation therapy is another option. The overall 5-year disease-specific survival rate has been estimated as 41%-50%. Location on the leg and multiple skin lesions were predictive of death in multivariate analysis [7], [8]. In another trial, disease-specific survival at 5 years was 100% for those receiving rituximab versus 67% for no rituximab [9]. Rituximab plus bendamustine is effective in a variety of lymphomas, including relapsed or refractory diffuse large B cell lymphoma [10], [11], [12]. One study in aggressive diffuse B-cell lymphoma achieved an objective response rate of 45.8 % (complete response, 15.3%; partial response, 30.5%). The median duration of response was 17.3 months, and the median progression-free survival lasted 3.6 months [11].
PCLBCL-LT is an aggressive variant of primary cutaneous B-cell lymphomas. Our patient belonged to the typical age group. Negative prognostic markers are female gender, Bcl-2 expression, and MYC rearrangements [2], [3], [4]. We did not perform an MYC rearrangement analysis. Her lymphoma did not express Bcl-2. Weekly immuno-chemotherapy with rituximab and alkylating agent bendamustine was initiated. After an initial partial response, the situation worsened in our patient. Therefore, the combination was stopped after the second cycle. Recently, Bruton’s tyrosine kinase inhibitor ibrutinib combined with chemotherapy-induced a durable remission in PCLBCL-LT with mutant MYD88 and wild type CD79 [13]. A single-arm phase II trial with the thalidomide derivate lenalidomide in relapsing or refractory PCLBCL-LT achieved a response rate of 26.3% with 4 complete responses. The median overall survival was 19.4 months [14].
Although another palliative approach had been suggested, the patient rejected any further therapy and died seven months after confirmation of the diagnosis. More effective treatment options that are tolerable in elderly patients are needed to improve prognosis.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Goyal A, LeBlanc RE, Carter JB. Cutaneous B-Cell Lymphoma. Hematol Oncol Clin North Am. 2019;33(1):149–161. doi: 10.1016/j.hoc.2018.08.006. https://doi.org/10.1016/j.hoc.2018.08.006. PMid:30497672. [DOI] [PubMed] [Google Scholar]
- 2.Menguy S, Beylot-Barry M, Marie P, Pham Ledard A, Frison E, Comoz F, Battistella M, Szablewski V, Balme B, Croue A, Franck F, Ortonne N, Tournier E, Lamant L, Carlotti A, De Muret A, Le Gall F, Lorton MH, Merlio JP, Vergier B. Primary Cutaneous Large B-Cell Lymphomas:relevance of the 2017 WHO Classification. Histopathology. 2019 doi: 10.1111/his.13832. [DOI] [PubMed] [Google Scholar]
- 3.Felcht M, Klemke CD, Nicolay JP, Weiss C, Assaf C, Wobser M, Schlaak M, Hillen U, Moritz R, Tantcheva-Poor I, Nashan D, Beyer M, Dippel E, Müller CSL, Sachse MM, Meiss F, Géraud C, Marx A, Goerdt S, Geissinger E, Kempf W. Primary cutaneous diffuse large B-cell lymphoma, NOS and leg type:Clinical, morphologic and prognostic differences. J Dtsch Dermatol Ges. 2019;17(3):275–285. doi: 10.1111/ddg.13773. https://doi.org/10.1111/ddg.13773. [DOI] [PubMed] [Google Scholar]
- 4.Schrader AMR, Jansen PM, Vermeer MH, Kleiverda JK, Vermaat JSP, Willemze R. High Incidence and Clinical Significance of MYC Rearrangements in Primary Cutaneous Diffuse Large B-Cell Lymphoma, Leg Type. Am J Surg Pathol. 2018;42(11):1488–1494. doi: 10.1097/PAS.0000000000001132. https://doi.org/10.1097/PAS.0000000000001132. PMid:30113335. [DOI] [PubMed] [Google Scholar]
- 5.Paulli M, Lucioni M, Maffi A, Croci GA, Nicola M, Berti E. Primary cutaneous diffuse large B-cell lymphoma (PCDLBCL), leg-type and other:an update on morphology and treatment. G Ital Dermatol Venereol. 2012;147(6):589–602. [PubMed] [Google Scholar]
- 6.Wilcox RA. Cutaneous B-cell lymphomas:2015 update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90(1):73–6. doi: 10.1002/ajh.23863. https://doi.org/10.1002/ajh.23863. PMid:25535037. [DOI] [PubMed] [Google Scholar]
- 7.Grange F, Beylot-Barry M, Courville P, Maubec E, Bagot M, Vergier B, Souteyrand P, Machet L, Dalac S, Esteve E, Templier I, Delaporte E, Avril MF, Robert C, Dalle S, Laroche L, Delaunay M, Joly P, Wechsler J, Petrella T. Primary cutaneous diffuse large B-cell lymphoma, leg type:clinicopathologic features and prognostic analysis in 60 cases. Arch Dermatol. 2007;143(9):1144–50. doi: 10.1001/archderm.143.9.1144. https://doi.org/10.1001/archderm.143.9.1144. PMid:17875875. [DOI] [PubMed] [Google Scholar]
- 8.Senff NJ, Hoefnagel JJ, Jansen PM, Vermeer MH, van Baarlen J, Blokx WA, Canninga-van Dijk MR, Geerts ML, Hebeda KM, Kluin PM, Lam KH, Meijer CJ, Willemze R. Reclassification of 300 primary cutaneous B-Cell lymphomas according to the new WHO-EORTC classification for cutaneous lymphomas:comparison with previous classifications and identification of prognostic markers. J Clin Oncol. 2007;25(12):1581–7. doi: 10.1200/JCO.2006.09.6396. https://doi.org/10.1200/JCO.2006.09.6396. PMid:17353548. [DOI] [PubMed] [Google Scholar]
- 9.Hamilton SN, Wai ES, Tan K, Alexander C, Gascoyne RD, Connors JM. Treatment and outcomes in patients with primary cutaneous B-cell lymphoma:the BC Cancer Agency experience. Int J Radiat Oncol Biol Phys. 2013;87(4):719–25. doi: 10.1016/j.ijrobp.2013.07.019. https://doi.org/10.1016/j.ijrobp.2013.07.019. PMid:24001373. [DOI] [PubMed] [Google Scholar]
- 10.Rummel MJ, Al-Batran SE, Kim SZ, Welslau M, Hecker R, Kofahl-Krause D, Josten KM, Dürk H, Rost A, Neise M, von Grünhagen U, Chow KU, Hansmann ML, Hoelzer D, Mitrou PS. Bendamustine plus rituximab is effective and has a favorable toxicity profile in the treatment of mantle cell and low-grade non-Hodgkin's lymphoma. J Clin Oncol. 2005;23(15):3383–9. doi: 10.1200/JCO.2005.08.100. https://doi.org/10.1200/JCO.2005.08.100. PMid15908650. [DOI] [PubMed] [Google Scholar]
- 11.Vacirca JL, Acs PI, Tabbara IA, Rosen PJ, Lee P, Lynam E. Bendamustine combined with rituximab for patients with relapsed or refractory diffuse large B cell lymphoma. Ann Hematol. 2014;93(3):403–9. doi: 10.1007/s00277-013-1879-x. https://doi.org/10.1007/s00277-013-1879-x. PMid:23955074 PMCid:PMC3918114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rigacci L, Puccini B, Cortelazzo S, Gaidano G, Piccin A, D'Arco A, Freilone R, Storti S, Orciuolo E, Zinzani PL, Zaja F, Bongarzoni V, Balzarotti M, Rota-Scalabrini D, Patti C, Gobbi M, Carpaneto A, Liberati AM, Bosi A, Iannitto E. Bendamustine with or without rituximab for the treatment of heavily pretreated non-Hodgkin's lymphoma patients:A multicenter retrospective study on behalf of the Italian Lymphoma Foundation (FIL) Ann Hematol. 2012;91(7):1013–22. doi: 10.1007/s00277-012-1422-5. https://doi.org/10.1007/s00277-012-1422-5. PMid:22349722. [DOI] [PubMed] [Google Scholar]
- 13.Deng AL, Kim YR, Lichtenstein EA, O'Connor OA, Deng C. Combination of ibrutinib and chemotherapy produced a durable remission in multiply relapsed diffuse large B-cell lymphoma leg type with mutant MYD88 and wildtype CD79. Haematologica. 2017;102(7):e275–e277. doi: 10.3324/haematol.2016.161893. https://doi.org/10.3324/haematol.2016.161893. PMid:28341730 PMCid:PMC5566054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Beylot-Barry M, Mermin D, Maillard A, Bouabdallah R, Bonnet N, Duval-Modeste AB, Mortier L, Ingen-Housz-Oro S, Ram-Wolff C, Barete S, Dalle S, Maubec E, Quereux G, Templier I, Bagot M, Grange F, Joly P, Vergier B, Vially PJ, Gros A, Pham-Ledard A, Frison E, Merlio JP. A Single-Arm Phase II Trial of Lenalidomide in Relapsing or Refractory Primary Cutaneous Large B-Cell Lymphoma, Leg Type. J Invest Dermatol. 2018;138(9):1982–1989. doi: 10.1016/j.jid.2018.03.1516. https://doi.org/10.1016/j.jid.2018.03.1516. PMid:29596904. [DOI] [PubMed] [Google Scholar]