

Abstract
Purpose
Muscle weakness and difficulty descending stairs are common after unilateral total knee arthroplasty (TKA), but the relationship between each is unclear. The purpose of this study was to compare lower extremity muscle strength, lower extremity support moments during step descent, and assess relationships between each.
Methods
The study included 40 subjects (20 post-TKA, 20 control). Knee extensor, hip abductor, and hip external rotator strength were measured and biomechanical analyses of step descent performed. Patients with TKA were assessed 3 and 6 months post-surgery.
Results
At 3 and 6 months post-TKA, operated limb hip external rotator and knee extensor strength were impaired compared to the non-operated limb (p < 0.01); however, no between-limb differences were observed during step descent. Compared to the control group, hip external rotator and knee extensor strength, total lower extremity support moment, and knee support moment during step descent were impaired post-TKA (p < 0.05). At 6 months post-TKA, knee extensor and hip external rotator strength correlated with total support moment during step descent (rs = 0.40, 0.41, p < 0.02). Hip abductor and external rotator strength negatively correlated with knee support moment during step descent (rs = −0.35, −0.39, p < 0.03).
Conclusions
Persistent operative limb knee extensor and hip external rotator muscle weakness is noted following unilateral TKA. Despite unilateral weakness, bilateral alterations in step descent strategy occur following TKA. Patients with TKA utilize hip musculature to reduce knee muscle demand during step descent, possibly contributing to limitations in long-term step descent performance.
Keywords: total knee arthroplasty, stair descent, total support moment, hip strength, quadriceps strength
INTRODUCTION
After total knee arthroplasty (TKA), patients commonly report improvement in knee pain from osteoarthritis. [24] Despite reduced pain, more than half of patients report persistent difficulty with step descent [25], the activity most tied to patient satisfaction after TKA. [22] Previous studies identified asymmetrical movement patterns that may contribute to difficulty with step descent, however, little is known of the potential relationships between hip and knee muscle strength and step descent performance [3, 20, 30]. Further, limited studies have assessed step down performance during the first six months following TKA, a window of time in which patients typically access rehabilitation to improve muscle strength and function. [9, 13, 23]
Total support moment is a biomechanical measure used to describe multi-joint compensatory strategies during weight-bearing activities and is defined by the summation of individual ankle, knee, and hip joint moments. [29, 35] Previous studies of total support moment identified patients 6 months after TKA having greater hip muscle contribution to the total support moment than from the knee musculature. [5, 29] Furthermore, one study found a positive relationship between greater peak knee extensor muscle strength and greater knee contribution to total support moment. [29] This result suggests that improving knee extensor strength may facilitate the restoration of movement patterns to those observed in control subjects. In addition, improving hip abduction strength may improve physical function in individuals after TKA. [1, 18, 28] Exploring hip muscle strength contributions to step descent performance would provide further insight into the development of compensatory movement strategies after TKA.
Persistent movement compensations are associated with long-term limitations in functional mobility and development of contralateral limb osteoarthritis.[6, 37] As such, understanding the development of and contributing factors to movement compensations after TKA is necessary in order develop improved intervention strategies. Thus, the primary purpose of this study was to compare peak knee extension, hip abduction, and hip external rotation muscle strength and total support moment characteristics during step descent in patients 3 and 6 months post-TKA and matched control participants. The secondary purpose was to assess relationships between peak muscle strength and total support moment characteristics during step descent. The primary hypothesis was that muscle strength and total support moment characteristics would be impaired in the operated limb of the TKA group compared to the non-operated limb and control group. Additionally, it was hypothesized that there would be a positive relationship between muscle strength and the corresponding muscle group’s contribution to the total support moment.
MATERIALS AND METHODS
Participants with initial TKA for degenerative (primary) osteoarthritis were recruited consecutively from eligible patients at the University’s orthopedic clinic from 2015 –2017 based on the following criteria: 1) between the ages of 40–90 years old, 2) undergone unilateral TKA within the past 3 months, 3) no prior surgery to the contralateral knee, low back, or either hip, ankle, or foot, 4) no neurological or balance disorder that requires use of an assistive device for mobility, 5) able to walk at least 10 minutes without an assistive device, and 6) self-reported contralateral knee pain <3/10. All control participants were taken from a sample of convenience from the community using recruitment flyers, digital displays, research participant registries, and word of mouth. All were required to be free of previous surgery and current injury or pain in the lower back and lower extremity joints, and match a TKA participant in the following characteristics: sex, age (±3 years), body mass index (same classification level), and physical activity level as measured by the Physical Activity Scale for the Elderly (±100 points). At 3 and 6 months post-TKA, participants completed muscle strength testing and three-dimensional biomechanical analysis of the step descent task. Control participants performed all testing procedures in a single session. Participants in the TKA group completed standard rehabilitation in community outpatient clinics with the total number of visits, visit frequency, and rehabilitation activities decided at the discretion of the surgeon and treating clinician. The primary goals of rehabilitation were 1) restoration of knee range of motion, 2) improving quadriceps activation, and 3) lower extremity muscle strengthening and neuromuscular training to return to walking and daily activity without an assistive device.
A total of 40 participants (20 TKA, 20 control) completed the study protocol (Fig 1). One hundred nineteen patients with TKA were screened with 24 patients enrolled. Four participants were unable to complete the step descent task independently at 3 months post-TKA and were excluded from this analysis. The most common reasons for pre-enrollment exclusion were: planned contralateral TKA (18), use of assistive device for balance (9), and history of prior joint surgery (8). The matching process was successful as no significant differences were observed between groups in sex, age, body mass index, height, mass, or physical activity level (Table 1). All participants with TKA had completed postoperative rehabilitation prior to the 3-month assessment.
Figure 1:
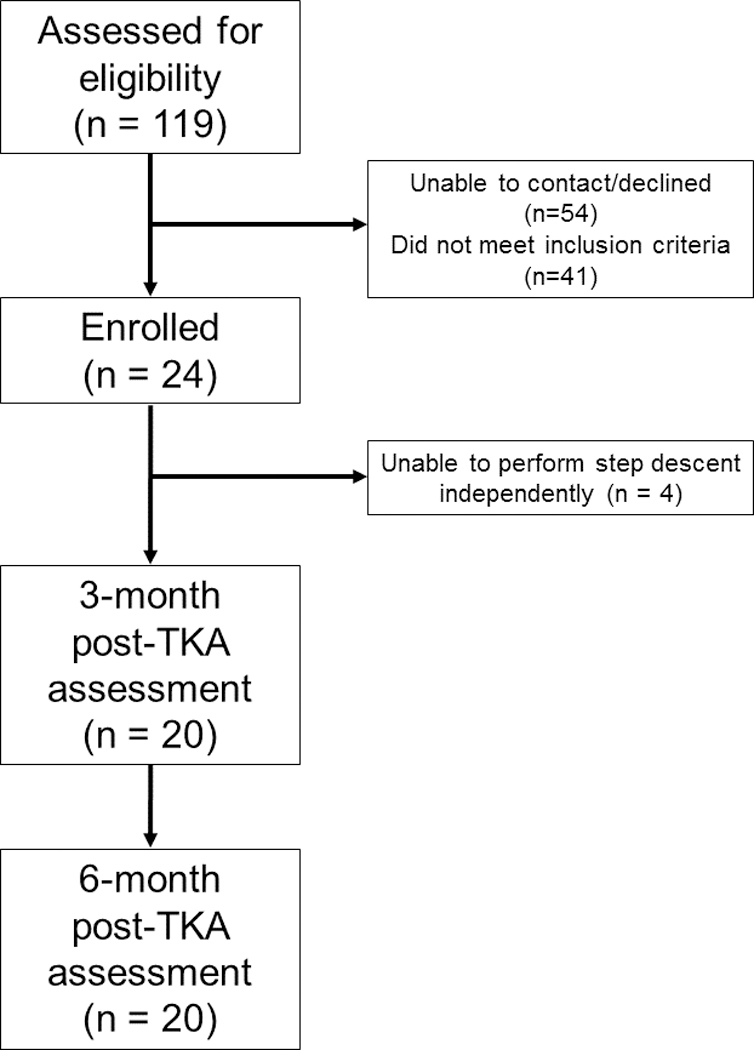
Flow Diagram of TKA Participant Recruitment and Assessment
Table 1.
Participant Demographics. Median (Range)
| Variable | TKA | Control | P-value |
|---|---|---|---|
| Sex (Male/Female) | 6/14 | 6/14 | - |
| Age (years) | 62 (47 – 74) | 58.5 (47 – 76) | n.s. |
| Body Mass Index (kg/m2) | 30.3 (20.6 – 44.7) | 29.3 (20.9 – 40.8) | n.s. |
| Height (m) | 1.69 (1.54 – 1.78) | 1.68 (1.51 – 1.83) | n.s. |
| Mass (kg) | 89 (57 – 129) | 83 (54 – 129) | n.s. |
| PASE | 155 (30 – 411) | 157 (43 – 319) | n.s. |
PASE: Physical Activity Scale for the Elderly
TKA: Total knee arthroplasty group
Control: Control group
Assessments
Muscle Strength
Participants completed isometric strength testing of hip abduction, hip external rotation, and knee extension using a Biodex System 4 (Biodex Systems, Shirley, NY, USA) with data sampled at 100 Hz. The Biodex dynamometer is a highly reliable and valid instrument for assessing torque production and is accurate to within ±1%. [8, 11] Hip abduction was assessed with the hip joint in neutral alignment and the participant in sidelying. The dynamometer arm was secured 5 cm proximal to the lateral tibiofemoral joint. Hip external rotation and knee extension were each assessed with the hip flexed to 85°, knee flexed to 90°, and hip in 0° rotation while the participant was seated. The dynamometer arm was secured 5 cm proximal the medial malleolus with a cushioned pad. During hip external rotation, participants were instructed to rotate their leg as if they were looking at the bottom of their shoe. For the knee extension strength assessment, participants were given verbal instruction to extend their knee as if to kick forward. One practice and three experimental trials, all with maximal effort, were performed for each muscle group bilaterally.[15] Visual and verbal encouragement was provided during all muscle performance testing with patients asked to provide maximal effort and perform each task with as much force as possible. A minimum of 30 seconds rest were allowed between trials to minimize the influence of fatigue.[15] All strength testing was conducted by a single investigator.
Biomechanical Analysis
All participants also underwent three-dimensional motion analysis while descending a 20.3 cm step using a previously established marker set. [17] Thigh and shank rigid clusters and pelvis markers were attached to underwraps to minimize soft tissue artifact.[19] Participants began on top of the step and were instructed to descend the step in a controlled manner and continue walking forward. At least two familiarization trials were allowed to ensure the participant was safe to perform the stair descent without supervision or the use of a handrail. Following familiarization, five complete trials were recorded with each limb acting as the stance limb during the descent. In order for a trial to be considered complete, the participant was required to control the descent, land with the entire landing limb on the force plate, and continue walking forward at least 2 steps. For the purposes of this analysis, only the stance limb was utilized and was defined as the limb remaining on the step during the lowering phase of the task. During the step descent task, marker trajectories were recorded using a 10-camera motion analysis system (Motion Analysis Corp, Santa Ana, CA, USA) with sampling rate of 200 Hz. Force-plate data were simultaneously recorded at 1200 Hz from an instrumented Bertec force plate (Bertec, Columbus, OH, USA). A single investigator was responsible for marker placement and data capture for all biomechanical analyses.
Data Analysis
Peak muscle strength was determined for each individual trial and averaged for each muscle group for use in statistical analyses. All values were normalized to body mass. Custom MATLAB code (MathWorks Inc, Natick, MA, USA) was used to identify peak torque from individual strength trials. For the step descent analysis, Visual 3D software (C-Motion, Inc, Germantown, MD, USA) was used to filter the data and perform inverse dynamics to determine joint moments. Marker position and force data were filtered at 8 and 35 Hz, respectively, using a fourth-order, low-pass, zero-lag Butterworth filter. Moments were calculated using Cardan XYZ angles referencing the distal segment to the proximal and were normalized to body mass and height. This data collection and processing methodology is highly reliable, valid, and accurate for tracking marker position (±0.38mm), sagittal plane joint kinematics (±3.9°), and sagittal plane joint kinetics (±0.1%).[2, 4, 10, 12, 27, 32] Custom MATLAB code was used to extract sagittal plane hip, knee, and ankle joint moments during the final 750 ms of lowering phase prior to the landing limb contacting the floor. This time range was selected due to peak knee flexion angle occurring during this period, which is the most mechanically demanding position for the knee. [16] Joint moments were averaged across the five single step descents resulting in a single result for hip, knee, and ankle kinetics for each limb. Total support moment was calculated by absolute summation of the sagittal plane hip, knee, and ankle net joint moments and the highest total support moment value during the period of interest used for subsequent data analysis.[35] Knee and hip joint contributions to the total support moment were calculated as a percentage of the total support moment. [29, 36]
Study Approvals
All participants read and signed an informed consent form prior to participation. The protocol for this prospective observational case-control study was approved by the University Institutional Review Board (14–0753-F2L). All study activities were performed at the University of Kentucky, Lexington, KY, USA.
Statistical Analysis
Continuous variables were first described using median and range. Categorical variables (e.g. implant type) were tabulated with absolute frequency. Normality was assessed using the Shapiro-Wilk test. Due to non-normally distributed outcomes, non-parametric statistical tests were used. Wilcoxon signed-rank tests were utilized to assess between-limb and 3 to 6 month comparisons of the operated and non-operated limbs of the TKA group. Mann-Whitney U-tests were used to compare the TKA group to the control group. Lastly, Spearman rank correlations were used to assess relationships between muscle performance measures and total support moment characteristics. All statistical tests were performed using SPPS Statistics 24 (IBM, Armonk, NY, USA) with statistical significance defined as P≤ 0.05 for all tests. An a-priori sample size calculation assuming an effect size of 0.5, α = 0.05, and 80% power to detect difference between participants with TKA and controls recommended a total sample of 36 participants. A total of 40 participants (20 per group) were collected to account for potential loss of data during data acquisition.
RESULTS
Between-Limb Comparisons
At both 3 and 6 months post-TKA, hip external rotation peak strength (3 month: p = 0.001, 6 month p < 0.001) and knee extension peak strength (3 month: p < 0.001, 6 month: p = 0.001) were significantly impaired in the operated limb compared to the non-operated limb in the TKA group (Table 2). No between-limb differences were observed at either time point in hip abduction peak strength, total support moment, knee or hip joint contribution to total support moment. See Table 2 for complete between-limb comparisons.
Table 2.
TKA Group: Between-Limb and 3 to 6 Month Comparisons
| 3 month | 6 month | |||||
|---|---|---|---|---|---|---|
| Variable | TKA | NON | P-value | TKA | NON | P-value |
| Hip Abduction Peak Strength (Nm/kg) | 0.7 (0.2 – 1.1) |
0.7 (0.2 – 1.4) |
n.s. | 0.7 (0.3 – 1.3) |
0.7 (0.2 – 1.7) |
n.s. |
| Hip External Rotation Peak Strength (Nm/kg) | 0.3 (0.2 – 0.5) |
0.35 (0.2 – 0.7) |
0.001* | 0.3 (0.2 – 0.5) |
0.4 (0.2 – 0.8) |
<0.001* |
| Knee Extension Peak Strength (Nm/kg) | 0.85 (0.5 – 1.7) |
1.35 (0.7 – 2.3) |
<0.001* | 0.9 (0.5 – 2.2) |
1.15 (0.6 – 2.6) |
0.001* |
| Total Support Moment (N/kg) | 1.26 (0.76 – 1.69) |
1.28 (0.97 – 1.72) |
n.s. | 1.31 (0.93 – 1.76) |
1.28 (0.96 – 1.67) |
n.s. |
| Knee contribution to Total Support Moment (%) | 52 (38 – 72) |
52 (36 – 72) |
n.s. | 55.5 (39 – 71) |
55.5 (41 – 66) |
n.s. |
| Hip contribution to Total Support Moment (%) | 21 (7 – 41) |
18 (5 – 42) |
n.s. | 17.5 (3 – 32) |
11.5 (4 – 38) |
n.s. |
Data presented as median (range)
TKA: operated limb
NON: non-operated limb
TKA vs Control Participants
Compared to the control group, hip external rotation peak strength was impaired in the operated limb at 3 months (p = 0.009). Additionally, knee extension peak strength (3 month: p < 0.001, 6 month: p < 0.001), peak total support moment (3 month: p = 0.002, 6 month: p = 0.012), and knee joint contribution to total support moment (3 month: p = 0.014, 6 month: p = 0.049) of the operated limb were each impaired at both 3 and 6 months post-TKA. The non-operated limb was impaired in peak total support moment (3 month: p = 0.002, 6 month: p = 0.002), and knee joint contribution to total support moment (3 month: p = 0.007, 6 month: p = 0.013) compared to controls at both time points. No muscle strength deficits were observed in the non-operated limb compared to the control group at either time point. See Table 3 for complete results.
Table 3.
A) Operated Limb vs Control and B) Non-operated Limb vs Control
| Variable | 3 month TKA | 6 month TKA | Control | 3 month P-value | 6 month P-value |
|---|---|---|---|---|---|
| Hip Abduction Peak Strength (Nm/kg) | 0.7 (0.2 – 1.1) |
0.7 (0.3 – 1.3) |
0.75 (0.3 – 1.0) |
n.s. | n.s. |
| Hip External Rotation Peak Strength Nm/kg) | 0.3 (0.2 – 0.5) |
0.3 (0.2 – 0.5) |
0.4 (0.2 – 0.6) |
0.009* | n.s. |
| Knee Extension Peak Strength (Nm/kg) | 0.85 (0.5 – 1.7) |
0.9 (0.5 – 2.2) |
1.65 (0.8 – 3.1) |
<0.001* | <0.001* |
| Total Support Moment (N/kg) | 1.26 (0.76 – 1.69) |
1.31 (0.93 – 1.76) |
1.47 (1.15 – 1.81) |
0.002* | 0.012* |
| Knee contribution to Total Support Moment (%) | 52 (38 – 72) |
55.5 (39 – 71) |
59.5 (48 – 69) |
0.014* | 0.049* |
| Hip contribution to Total Support Moment (%) | 21 (7 – 41) |
17.5 (3 – 32) |
18 (7 – 35) |
n.s. | n.s. |
| Variable | 3 month NON | 6 month NON | Control | 3 month P-value | 6 month P-value |
| Hip Abduction Peak Strength (Nm/kg) | 0.7 (0.2 – 1.4) |
0.7 (0.2 – 1.7) |
0.75 (0.3 – 1.0) |
n.s. | n.s. |
| Hip External Rotation Peak Strength (Nm/kg) | 0.35 (0.2 – 0.7) |
0.4 (0.2 – 0.8) |
0.4 (0.2 – 0.6) |
n.s. | n.s. |
| Knee Extension Peak Strength (Nm/kg) | 1.35 (0.7 – 2.3) |
1.15 (0.6 – 2.6) |
1.65 (0.8 – 3.1) |
n.s. | n.s. |
| Total Support Moment (N/kg) | 1.28 (0.97 – 1.72) |
1.28 (0.96 – 1.67) |
1.47 (1.15 – 1.81) |
0.002* | 0.002* |
| Knee contribution to Total Support Moment (%) | 52 (36 – 72) |
55.5 (41 – 66) |
59.5 (48 – 69) |
0.007* | 0.013* |
| Hip contribution to Total Support Moment (%) | 18 (5 – 42) |
11.5 (4 – 38) |
18 (7 – 35) |
n.s. | n.s. |
Data presented as median (range)
TKA: operated limb
NON: non-operated limb
Correlations
At 3 months post-TKA, peak knee extension strength (rs = 0.63, p < 0.01), peak hip external rotation strength (rs = 0.60, p < 0.01), and peak hip abduction strength (rs = 0.42, p < 0.01) were all significantly positively correlated with peak total support moment. Peak hip abduction strength was negatively correlated with the knee joint contribution to total support moment (rs = −0.37, p = 0.02). At 6 months post-TKA, peak knee extension strength (rs = 0.41, p = 0.008) and peak hip external rotation strength (rs = 0.40, p = 0.01) were correlated with peak total support moment. Hip abduction (rs = −0.39, p = 0.014) and peak hip external rotation strength (rs = −0.35, p = 0.026) were negatively correlated with knee joint contribution to total support moment. See Table 4 for complete results.
Table 4.
A) 3-month and B) 6-month correlations
| A) 3 month |
| Total Support Moment |
Knee contribution |
Hip contribution |
|
|---|---|---|---|
| Hip Abduction Peak Strength |
0.425 (0.007)* |
−0.366 (0.022)* |
0.069 (n.s.) |
| Hip External Rotation Peak Strength |
0.633 (<0.001)* |
−0.185 (n.s.) |
0.105 (n.s.) |
| Knee Extension Peak Strength |
0.597 (<0.001)* |
0.052 (n.s.) |
−0.059 (n.s.) |
| B) 6 month |
| Total Support Moment |
Knee contribution |
Hip contribution |
|
|---|---|---|---|
| Hip Abduction Peak Strength | 0.225 (n.s.) |
−0.390 (0.014)* |
−0.045 (n.s.) |
| Hip External Rotation Peak Strength |
0.400 (0.010)* |
−0.352 (0.026)* |
0.128 (n.s.) |
| Knee Extension Peak Strength |
0.411 (0.008)* |
−0.178 (n.s.) |
0.021 (n.s.) |
Data presented as rs (p-value)
Knee contribution: knee joint contribution to total support moment
Hip contribution: hip joint contribution to total support moment
DISCUSSION
The most important finding of this study is that the current standard of care postoperative rehabilitation does not adequately address deficits in knee extensor and hip external rotation strength and these deficits persist 6 months after TKA. Furthermore, these strength deficits are associated with impaired ability to navigate stairs: the task most associated with postoperative patient satisfaction. [22] Despite between-limb differences in muscle strength at both 3 and 6 months, the total support moment and knee joint contribution to total support moment during step descent were similar between-limbs but altered bilaterally compared to matched controls.
Impairment in knee extensor strength of the operated limb has been extensively reported following TKA. [33] Fewer investigations of hip muscle strength have been reported, but each observed deficits in hip abduction strength compared to control participants with conflicting findings between operated and non-operated limbs. [1, 18, 28] To date, no study has evaluated the role of hip external rotation strength. Deficits in peak hip external rotation strength, both between-limb and compared to matched control participants, suggests gluteus maximus muscle weakness persists during the first 6 months following TKA. [7] Interestingly, no significant differences were observed in peak hip abduction strength either between-limb or compared to the control group. This finding is contrary to a previous study, which identified between-limb differences prior to TKA, at 1-month post-TKA, and 3-months post-TKA in peak hip abduction strength in operated and non-operated limbs. [18]
Despite between-limb deficits in muscle strength, there were no differences between the operated and non-operated limbs in total support moment characteristics. However, bilateral differences were observed compared to matched controls, suggesting that the TKA group adapts a different step descent loading strategy than the controls in both limbs. The disparate findings in between-limb muscle performance and step descent loading characteristics indicate the participants with TKA have adopted an altered neuromuscular control strategy for step descent compared to matched controls. This hypothesis is supported by previous studies in patients with knee osteoarthritis and TKA which identified muscular demand shifting from the knee to the hip and ankle in the involved limb. [5, 29, 36] Alternatively, individuals could adapt the non-operated limb in an attempt to perform the task symmetrically. Additionally, step descent is a higher demand task than walking and may require lower extremity support beyond the capability of both the operated and non-operated limbs. [14] In support of this, bilateral deficits in total support moment and the knee joint contribution to total support moment suggests that individuals with TKA adapt a bilateral strategy to reduce total muscular demand during step descent.
The relationships between muscle performance measures to total support moment characteristics shed light on possible muscle contributions to the observed impairments in total limb mechanical strategy. At 3 months post-surgery, peak muscle strength of the knee extensors, hip abductors, and hip external rotators were positively correlated with peak total support moment. These relationships suggest that those patients with greater muscle strength after surgery and subsequent rehabilitation were more capable of controlling load during step descent. At 6 months, we observed similar relationships in knee extension and hip external rotation peak strength. Importantly, greater hip external rotation and hip abduction peak strength were associated with decreased knee joint contribution to total support moment (Table 4). Based on these relationships, those individuals with stronger hip musculature may utilize these muscle groups as a compensatory mechanism to shift demand from the knee to the hip. This finding confirms results of previous modeling studies of muscle force contribution during stair tasks after TKA, which demonstrate increased hip muscle contribution to compensate for reductions in knee extensor force production. [14, 31] Additional studies are needed to further explore the concept of altered neuromuscular patterns, the potential efficacy of hip and knee muscle strengthening on improving step descent mechanics, and the long-term consequences of hip compensatory strategies on knee extensor muscle strength.
There are limitations to this study. First, only individuals following TKA able to safely perform the step descent task without use of a handrail or assistive device were included in this study. For this reason, the findings of this study may not be applicable to individuals who are unable to descend a step without assistance. Additionally, both males and females were included and have been shown to recover from TKA at different rates. [21, 26, 34] However, use of a matched control group partially overcomes this limitation. Furthermore, preoperative measures including muscle strength, functional performance, pain level, duration of symptoms, and physical activity level were not assessed. Lastly, postoperative rehabilitation was not controlled nor monitored. Variability in preoperative measures and dosage, duration, mode, intensity, and patient compliance during rehabilitation may have influenced the observed outcomes.
CONCLUSION
Current standard of care postoperative rehabilitation does not adequately address deficits in knee extension and hip external rotation muscle strength with these deficits noted following completion of rehabilitation and persisting 6 months after TKA. Following TKA, patients present with bilateral alterations in step descent limb mechanics compared to matched control subjects. As a compensatory strategy for knee extensor weakness, patients with TKA utilize proximal hip musculature to shift muscular demand from the knee to the hip.
Acknowledegements/External Support
Research reported in the publication was supported by the National Center for Advancing Translational Sciences, National Institutes of Health [grant number TL1TR000115]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
LIST OF ABBREVIATIONS
- TKA
total knee arthroplasty
REFERENCES
- 1.Alnahdi AH, Zeni JA, Snyder-Mackler L (2014) Hip abductor strength reliability and association with physical function after unilateral total knee arthroplasty: a cross-sectional study. Phys Ther 94:1154–1162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Benedetti MG, Merlo A, Leardini A (2013) Inter-laboratory consistency of gait analysis measurements. Gait Posture 38:934–939 [DOI] [PubMed] [Google Scholar]
- 3.Bjerke J, Ohberg F, Nilsson KG, Foss OA, Stensdotter AK (2014) Peak knee flexion angles during stair descent in TKA patients. J Arthroplasty 29:707–711 [DOI] [PubMed] [Google Scholar]
- 4.Camomilla V, Cereatti A, Cutti AG, Fantozzi S, Stagni R, Vannozzi G (2017) Methodological factors affecting joint moments estimation in clinical gait analysis: a systematic review. Biomed Eng Online 16:106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Christensen JC, LaStayo PC, Mizner RL, Marcus RL, Pelt CE, Stoddard GJ, et al. (2017) Joint mechanical asymmetries during low- and high-demand mobility tasks: Comparison between total knee arthroplasty and healthy-matched peers. Gait Posture 60:104–110 [DOI] [PubMed] [Google Scholar]
- 6.Christiansen CL, Bade MJ, Judd DL, Stevens-Lapsley JE (2011) Weight-bearing asymmetry during sit-stand transitions related to impairment and functional mobility after total knee arthroplasty. Arch Phys Med Rehabil 92:1624–1629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Claiborne TL, Timmons MK, Pincivero DM (2009) Test-retest reliability of cardinal plane isokinetic hip torque and EMG. J Electromyogr Kinesiol 19:e345–352 [DOI] [PubMed] [Google Scholar]
- 8.de Araujo Ribeiro Alvares JB, Rodrigues R, de Azevedo Franke R, da Silva BG, Pinto RS, Vaz MA, et al. (2015) Inter-machine reliability of the Biodex and Cybex isokinetic dynamometers for knee flexor/extensor isometric, concentric and eccentric tests. Phys Ther Sport 16:59–65 [DOI] [PubMed] [Google Scholar]
- 9.DeJong G, Tian W, Smout RJ, Horn SD, Putman K, Smith P, et al. (2009) Use of rehabilitation and other health care services by patients with joint replacement after discharge from skilled nursing and inpatient rehabilitation facilities. Arch Phys Med Rehabil 90:1297–1305 [DOI] [PubMed] [Google Scholar]
- 10.Croce Della U, Leardini A, Chiari L, Cappozzo A (2005) Human movement analysis using stereophotogrammetry. Part 4: assessment of anatomical landmark misplacement and its effects on joint kinematics. Gait Posture 21:226–237 [DOI] [PubMed] [Google Scholar]
- 11.Drouin JM, Valovich-mcLeod TC, Shultz SJ, Gansneder BM, Perrin DH (2004) Reliability and validity of the Biodex system 3 pro isokinetic dynamometer velocity, torque and position measurements. Eur J Appl Physiol 91:22–29 [DOI] [PubMed] [Google Scholar]
- 12.Eichelberger P, Ferraro M, Minder U, Denton T, Blasimann A, Krause F, et al. (2016) Analysis of accuracy in optical motion capture - A protocol for laboratory setup evaluation. J Biomech 49:2085–2088 [DOI] [PubMed] [Google Scholar]
- 13.Fritz JM, Hunter SJ, Tracy DM, Brennan GP (2011) Utilization and clinical outcomes of outpatient physical therapy for medicare beneficiaries with musculoskeletal conditions. Phys Ther 91:330–345 [DOI] [PubMed] [Google Scholar]
- 14.Gaffney BM, Harris MD, Davidson BS, Stevens-Lapsley JE, Christiansen CL, Shelburne KB (2016) Multi-Joint Compensatory Effects of Unilateral Total Knee Arthroplasty During High-Demand Tasks. Ann Biomed Eng 44:2529–2541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Grindstaff TL, Palimenio MR, Franco M, Anderson D, Bagwell JJ, Katsavelis D (2018) Optimizing Between-Session Reliability for Quadriceps Peak Torque and Rate of Torque Development Measures. J Strength Cond Res; 10.1519/jsc.0000000000002821 [DOI] [PubMed] [Google Scholar]
- 16.Hong SW, Wang TM, Lu TW, Li JD, Leu TH, Ho WP (2014) Redistribution of intra- and inter-limb support moments during downhill walking on different slopes. J Biomech 47:709–715 [DOI] [PubMed] [Google Scholar]
- 17.Kline PW, Morgan KD, Johnson DL, Ireland ML, Noehren B (2015) Impaired Quadriceps Rate of Torque Development and Knee Mechanics After Anterior Cruciate Ligament Reconstruction With Patellar Tendon Autograft. Am J Sports Med 43:2553–2558 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Loyd BJ, Jennings JM, Judd DL, Kim RH, Wolfe P, Dennis DA, et al. (2017) Influence of Hip Abductor Strength on Functional Outcomes Before and After Total Knee Arthroplasty: Post Hoc Analysis of a Randomized Controlled Trial. Phys Ther 97:896–903 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Manal K, McClay I, Stanhope S, Richards J, Galinat B (2000) Comparison of surface mounted markers and attachment methods in estimating tibial rotations during walking: an in vivo study. Gait Posture 11:38–45 [DOI] [PubMed] [Google Scholar]
- 20.McClelland JA, Feller JA, Menz HB, Webster KE (2014) Patterns in the knee flexion-extension moment profile during stair ascent and descent in patients with total knee arthroplasty. J Biomech 47:1816–1821 [DOI] [PubMed] [Google Scholar]
- 21.McClelland JA, Feller JA, Webster KE (2018) Sex Differences in Gait After Total Knee Arthroplasty. J Arthroplasty 33:897–902 [DOI] [PubMed] [Google Scholar]
- 22.Nakahara H, Okazaki K, Mizu-Uchi H, Hamai S, Tashiro Y, Matsuda S, et al. (2015) Correlations between patient satisfaction and ability to perform daily activities after total knee arthroplasty: why aren’t patients satisfied? J Orthop Sci 20:87–92 [DOI] [PubMed] [Google Scholar]
- 23.Oatis CA, Li W, DiRusso JM, Hoover MJ, Johnston KK, Butz MK, et al. (2014) Variations in Delivery and Exercise Content of Physical Therapy Rehabilitation Following Total Knee Replacement Surgery: A Cross-Sectional Observation Study. Int J Phys Med Rehabil Suppl 5: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Papakostidou I, Dailiana ZH, Papapolychroniou T, Liaropoulos L, Zintzaras E, Karachalios TS, et al. (2012) Factors affecting the quality of life after total knee arthroplasties: a prospective study. BMC Musculoskelet Disord 13:116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Parvizi J, Nunley RM, Berend KR, Lombardi AV Jr., Ruh EL, Clohisy JC, et al. (2014) High level of residual symptoms in young patients after total knee arthroplasty. Clin Orthop Relat Res 472:133–137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Paterson KL, Sosdian L, Hinman RS, Wrigley TV, Kasza J, Dowsey M, et al. (2017) The influence of sex and obesity on gait biomechanics in people with severe knee osteoarthritis scheduled for arthroplasty. Clin Biomech (Bristol, Avon) 49:72–77 [DOI] [PubMed] [Google Scholar]
- 27.Pinzone O, Schwartz MH, Thomason P, Baker R (2014) The comparison of normative reference data from different gait analysis services. Gait Posture 40:286–290 [DOI] [PubMed] [Google Scholar]
- 28.Piva SR, Teixeira PE, Almeida GJ, Gil AB, DiGioia AM 3rd, Levison TJ, et al. (2011) Contribution of hip abductor strength to physical function in patients with total knee arthroplasty. Phys Ther 91:225–233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pozzi F, Marmon AR, Snyder-Mackler L, Zeni J Jr. (2016) Lower leg compensatory strategies during performance of a step up and over task in patient six-months after total knee arthroplasty. Gait Posture 49:41–46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Pozzi F, Snyder-Mackler L, Zeni J Jr. (2015) Relationship between biomechanical asymmetries during a step up and over task and stair climbing after total knee arthroplasty. Clin Biomech (Bristol, Avon) 30:78–85 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rasnick R, Standifird T, Reinbolt JA, Cates HE, Zhang S (2016) Knee Joint Loads and Surrounding Muscle Forces during Stair Ascent in Patients with Total Knee Replacement. PLoS One 11:e0156282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ren L, Jones RK, Howard D (2008) Whole body inverse dynamics over a complete gait cycle based only on measured kinematics. J Biomech 41:2750–2759 [DOI] [PubMed] [Google Scholar]
- 33.Schache MB, McClelland JA, Webster KE (2014) Lower limb strength following total knee arthroplasty: a systematic review. Knee 21:12–20 [DOI] [PubMed] [Google Scholar]
- 34.Sveikata T, Porvaneckas N, Kanopa P, Molyte A, Klimas D, Uvarovas V, et al. (2017) Age, Sex, Body Mass Index, Education, and Social Support Influence Functional Results After Total Knee Arthroplasty. Geriatr Orthop Surg Rehabil 8:71–77 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Winter DA. Biomechanics and Motor Control of Human Movement. 3rd ed. Hoboken, NJ, USA: John Wiley & Sons; 2005. [Google Scholar]
- 36.Zeni JA, Higginson JS (2011) Knee osteoarthritis affects the distribution of joint moments during gait. Knee 18:156–159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zeni JA Jr, Flowers P, Bade M, Cheuy V, Stevens-Lapsley J, Snyder-Mackler L (2019) Stiff knee gait may increase risk of second total knee arthroplasty. J Orthop Res 37:397–402 [DOI] [PMC free article] [PubMed] [Google Scholar]