

Abstract
Objective:
To derive findings from different studies done on drug related hospital admissions and comprehensively express the incidence and preventability of drug related hospital admissions; identify the common types of drug related problems that caused hospital admission, and identify factors associated with drug related hospital admission.
Methods:
Literatures that assessed hospitalization due to drug related problems were searched online using Pub Med and Google Scholar databases. The relevant reference lists of retrieved articles were also searched manually on Google. Prospective and retrospective studies conducted anywhere in the world on drug related hospitalization, published from January 2012 to January 2017 as an original article and written in English language were included.
Result:
The prevalence of drug related hospital admission varies from 1.3% to 41.3% with the average rate of 15.4%. Among hospitalized patients 2.7% were died due to drug-related problems (DRPs). Drugs that were frequently reported as causing drug related admission were antithrombotic drugs, antihypertensive drugs, analgesics, anti-diabetics, antipsychotics, and anti-neoplastic drugs. Poly pharmacy, old age and female sex were mentioned as determinants for drug related hospitalization by a number of studies. About one third of drug related hospital admissions were definitely preventable and more than 40% were also potentially preventable.
Conclusion:
Drug related problems contribute for more than 15% of hospital admissions. Higher risk of admission due to DRPs was observed in patients who were on poly pharmacy and those who were old. As most of drug related hospital admissions were preventable an emphasis should be given for preventive strategies to avoid complications and costs associated with admission.
Key Words: Drug related problems, Hospital admission, Adverse drug reaction, Review, Emergency visit.
Introduction
World-wide, medication use is increasing. This can be explained as a result of production of more types of medications by the advancing pharmaceutical industries and the ever increasing types of diseases that amplified needs of pharmaceuticals. Possible outcomes of medication use may range from the intended beneficial effect interventions to minor side effects and even death. Drug related problem (DRP) is defined as an event or circumstance that involves a patient’s drug treatment that actually, or potentially, interferes with the achievement of an optimal outcome [1, 2]. This can be inappropriate drug selection, adverse drug reactions, untreated indication, drug interactions, inappropriate dosage, drug use without indication and non-compliance.
Admissions due to DRPs have been reported as growing over the past decades [3]. In United States, estimates suggested that Drug-related problems (DRPs) accounted for 17 million emergency department visits and 8.7 million hospital admissions annually [4]. Evaluation of studies on DRPs which leads to hospital admission have indicated that DRPs are responsible for approximately 5-15% of all hospitalizations, of which 25-75% were avoidable [5-11]. Those medications with narrow therapeutic index and medications which require continuous and regular monitoring are the one most implicated in avoidable adverse drug events (ADEs) [5]. A number of factors have been implicated to be risk factors for drug related hospital admission. Examples include being old [3, 7, 12, 13], Poly pharmacy [3, 14], poly physician [14], being female [15], and presence of co morbidities [5, 16, 17]. Drug related hospitalization will have negative consequences on patients and society. It increases mortality and morbidity rates, health care cost, decreases income and household productivity and reduced quality of life [5, 18].
Different studies across the world reported varying level of incidence and preventability of drug related hospital admission based on the settings, methods used and populations addressed. It is very important to see the current overall picture of drug related hospitalization to understand the nature and extent of the problem and to devise strategies for preventing its harm. So the aim of this review is to derive findings from different studies done on drug related hospital admissions and comprehensively expresses the incidence and preventability of drug related hospital admissions; identify the common types of DRPs that caused hospital admission, and identify factors responsible for drug related hospital admission.
Materials and Methods
Search strategy
Literatures that assessed admission to an emergency department or other units of the hospital due to adverse drug reactions or any other drug related problems were searched online using Pub-med and Google Scholar databases. The following words were used in different combinations during online search; Drug related problem(s), hospitalization, emergency department visit, adverse drug reaction, hospital admission and drug related admission. The relevant reference lists of retrieved articles were also searched manually on Google.
Article selection
All of the identified articles were independently reviewed by three authors to assess eligibility for inclusion in the review. Disagreements were resolved by consensus. Prospective and retrospective studies conducted anywherein the world on drug related hospitalization, published in January 2012 to January 2017 as an original article and written in English language were included in the study. Studies conducted in the pediatric population were excluded.
Data extraction
Information regarding study characteristics (study area, study design, subjects and sample size) and main findings (frequency of hospital admission and death due to drug related problems, type, severity, casualty and preventability of DRPs, drugs and drug classes responsible for admission and factors associated with drug related admission) were extracted from each studies.
Results
Literature search results
A total of 326 articles were obtained from Pub med, Google Scholar and manual Google search. After adjusting for duplicates 263 articles remained. Of these 214 studies were found irrelevant after reviewing their titles. Thirty-one studies were discarded as they do not satisfy the inclusion criteria after reviewing their abstracts. The full text of the remaining 18 studies was reviewed in detail. Two studies were removed after the full text was reviewed since it did not address many of the needed information. Finally, as shown in Figure 1, sixteen studies were found convenient to be included in this review.
Fig. 1.
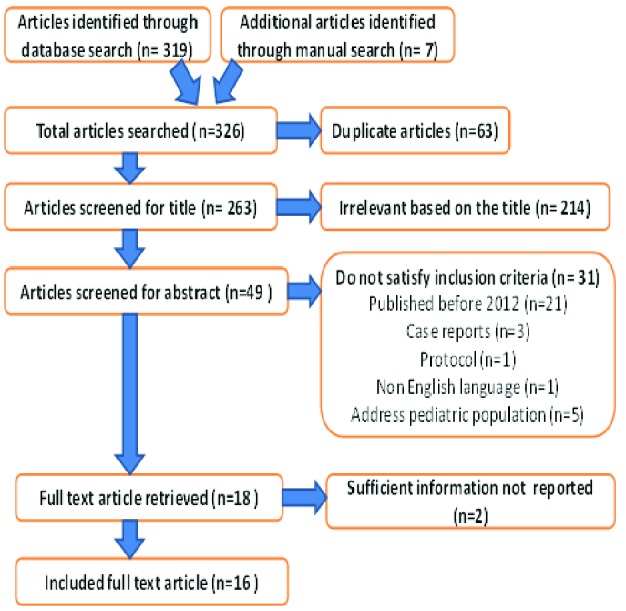
Flow diagram of study selection
Study characteristics
Among the 16 studies reviewed majority (12) assessed admission to any department of the hospital while 4 assessed admissions to emergency department only. Nine of the studies reported hospitalization due to any type of drug related problems and the other 7 assessed admissions due to adverse drug reactions only. Nine of the studies included all adult patients while others include only specific patient groups like cancer patients (1), cardiac transplanted patients (1), elderly patients with dementia (1), patient who are age 65 or more (2), age 60 or more (1) and age 55 or more (1). As shown in Table 1, the studies were conducted in different parts of the world on samples of 48 –2,127,133 patients. Most (11) of the studies were prospective in design.
Table 1.
Individual study characteristics
| Sr. no. | Author, year of publication | Study area/country | Study subjects | Study design | Sample size |
|---|---|---|---|---|---|
| 1 | Alghamdy M. et al, 2015 [20] | Saudi Arabia | Admitted patients at emergency department | Retrospective record review | 5622 |
| 2 | Chan A. et al, 2014 [21] | Singapore General Hospital | cancer patients admitted to two oncology wards | prospective, observational study | 1274 |
| 3 | Schmiedl, S et al, 2014 [22] | German | patients admitted to the internal medicine departments | multi-centre, Prospective study | 212,000 |
| 4 | Benard-laribiere A. etal, 2015 [23] | 61 Medical wards in public hospitals of France | Patients admitted to the medical wards | Prospective study | 2692 |
| 5 | ReppK.. et al, 2012 [5] | Saint Luke's North Hospital, Kansas City, USA | cardiac transplant patients | prospective longitudinal - single center study | 48 |
| 6 | Al-Arifi M. et al, 2014 [4] | Saudi Arabia | Patients visiting emergency department | prospective cohort observational study | 300 |
| 7 | Nickel C. et al, 2013 [26] | University Hospital Basel , Switzerland | non-trauma patients presenting to the ED with non-specific complaints | Prospective crossectional study | 633 |
| 8 | Gustafsson M. et al, 2016[16] | Sweden | Elderly patients with dementia or cognitive impairment admitted orthopedic and internal medicine wards | NR | 458 |
| 9 | Jatau A. et al, 2015 [18] | UniversitiSains Hospital, Malaysia | patients who visited the ED | Prospective cross-sectional study | 434 |
| 10 | Ruiter Ret al, 2012 [10] | Hospitals in Netherlands | patients >55 years of age with an acute, non-planned admission to a Dutch hospital | Retrospective study | 2, 127,133 |
| 11 | Pedrós C.et al, 2016 [24] | Bellvitge University hospital, Barcelona, Spain. | Patients aged >65 years who were urgently admitted at the hospital | prospective cross-sectional study | 60,263 |
| 12 | Ahern F, et al, 2013 [32] | Cork University Hospital (CUH) emergency department, Ireland | Patients admitted to the ED | retrospective study | 856 |
| 13 | Pedrós C. et al, 2014 [25] | Bellvitge University Hospital, Spain | patients admitted through the emergency room | prospective cross-sectional study | 4,403 |
| 14 | Karuppannan M. et al, 2013 [27] | Two medical wards at a government hospital in Malaysia. | Patients admitted to medical wards | Prospective study | 1200 |
| 15 | Skoldunger A. et al, 2015 [34] | four sites in Sweden | individuals aged ≥60 years | Longitudinal prospective cohort study | 4108 |
| 16 | Marcum Z. et al, 2012 [33] | Veterans Affairs (VA) Medical Centers, USA | older (aged ≥65) | Retrospective cohort | 678 |
aUSA; United States of America
Drug related hospitalization and death
There is no significant difference in the rate of drug related hospitalization between the large and small sample size studies (p=0.268). As indicated in Table 2, the rate of drug related hospital admission varies from 1.3% in Netherlands to 41.3% in Sweden. The average rate of drug related hospital admission is 15.4%. Seven studies reported that 0% up to 5.7% of patients hospitalized due to drug related problems were died. The average death rate due to DRPs in hospitalized patients is 2.7 %.
Table 2.
Rate of drug related hospital admission and death and types of DRPs causing hospitalization
| Sr. no. | Author, year of publication | Admission to Hospital (reason) | Death due to DRPs | Types of DRPs that causes admission |
|---|---|---|---|---|
| 1 | Alghamdy M. et al, 2015 [20] | 253 (4.5%) (due to DRP) |
10 (4%) | Noncompliance 112 (44.3%) Toxicity and SEs 50 (19.8%) Drug-drug interactions 29 (11.5%) Accidental and suicidal drug ingestions 26 (10.3%) Drug abuse 18 (7.1%) Drug allergy 10 (4%) Super-infections 8 (3.2%) |
| 2 | Chan A. et al, 2014 [21] | 158 (12.4 %) (due to DRP) |
5 (3%) | Adverse reaction 155 (94.5%) Drug interactions 3 (1.8%) Dosing problem 3 (1.8%) Drug use problem 3 (1.8%) |
| 3 | Schmiedl, S et al, 2014 [22] | 6887(3.2%) (due to ADR) |
1.32% | NR |
| 4 | Benard-laribiere A. et al, 2015 [23] | 97(3.6%) (due to ADR) |
1% | Type A reactions 67 (69.1%) Vascular disorders 20 (20.6%) CNS disorders 11 (11.3%) Gastrointestinal disorders 9 (9.3%) General disorders 9 (9.3%). |
| 5 | ReppK. et al, 2012 [5] | 40% (19/48) (due to DRP) |
0% | Adverse drug reactions 6 (32%) Supra-therapeutic doses 6 (32%) Sub-therapeutic doses 3 (16%) Untreated indication 1 (5%) Non-adherence 2 (11%) Drug interactions 1 (5%) |
| 6 | Al-Arifi M. et al, 2014 [4] | 56 (18.7%) (due to DRPs) |
NR | Adverse drug reactions (30.4%) non-compliance (30.4%) Untreated indication (10.7%) Drug interactions (7.1%) Supra-therapeutic (7.1%) Sub-therapeutic dose (7.1%) Improper drug selection (5.4%) drug use without indication (1.8%) |
| 7 | Nickel C. et al, 2013 [26] | 77 (12.2%) (due to DRPs) |
NR | Adverse drug reactions 42 (56%) Drug choice problem 9 (12%) Dosing problems 16 (21%) Drug use problems 2 (3%) Drug interactions 3 (4%) |
| 8 | Gustafsson M. et al, 2016 [16] | 189 (41.3 %) (due to DRPs) | NR | Dosage too high (12.7 %) Noncompliance (10.6 %) Ineffective drug 10.6 % interactions 6.9 % Needs additional drug (6.3%) Dosage too low (4.8 %) Unnecessary drug therapy (2.6 %) |
| 9 | Jatau A. et al, 2015 [18] | 133 (30.6 %) (due to ADE) |
NR | Therapeutic failure74 (55.6 %) ADR 43 (32.3 %) Accidental overdose 7 (5.2 %) Intentional overdose 6 (4.5 %) Untreated indication 3 (3.2 %) |
| 10 | Ruiter Ret al, 2012 [10] | 26852 (1.3%) (Due to ADR) | ADR | |
| 11 | Pedrós C.et al, 2016 [24] | 1976 (3.3%) (Due to ADR) | 113 (5.7 %) | Acute renal failure (22.9 %) Upper GI bleeding (16.6%) Lower GI bleeding (11.2 %) Intracranial bleeding (9.3%) Digitalis intoxication (3.7 %) |
| 12 | Ahern F, et al, 2013 [32] | 75 (8.8%) (due to ADR) | NR | NR |
| 13 | Pedrós C. et al, 2014 [25] | 4.2 % (due to ADR) | 3.2 % | Type A reactions 171 (91.9 %) Type B 15 (8.1 %) Renal & urinary disorder 59 (29.4 %) Gastrointestinal disorders 53 (26.4 %) Nervous system disorders 21 (10.4 %) |
| 14 | Karuppannan M. et al, 2013 [27] | 443 (39%) (ADR) |
NR | Treatment Failure 351 (79%) ADR 94 (21%) Drug overdose 21 (5%) Medication error 15 (3%) |
| 15 | Skoldunger A. et al, 2015 [34] | 536 (13%) | NR | NR |
| 16 | Marcum Z. et al, 2012 [33] | 68 (10%) (due to ADR) |
NR | Bradycardia (n = 6) hypoglycemia (n = 6) falls (n = 6) mental status changes (n = 6) |
Drug related problems that cause hospital admission
As shown in Table 3 the common drug related problems that caused hospital admission were adverse drug reaction, dosing problems, noncompliance, untreated indication and improper drug selection.
Table 3.
drugs and other factors that are associated with drug related hospitalization
| Author, year of publication | Drugs that cause DRP | Factors significantly associated with admission due to DRPs |
|---|---|---|
| Alghamdy M. et al, 2015 [20] | Antiepileptic drugs Paracetamol Opioid Benzodiazepine Antibiotics Antisecratory drugs Antipsychotic drugs Antihypertensive drugs |
NR |
| Chan A. et al, 2014 [21] | Cyclophosphamide (n=35), Doxorubicin (n=25), Cisplatin (n=25), Docetaxel (n=18), Paclitaxel (n=16). |
Young age (p=0.03) Female sex (P=0.015) |
| Schmiedl, S et al, 2014[22] | Antithrombotic agents drugs used in diabetes NSAIDs Paracetamol |
NR |
| Benard-laribiere A. etal, 2015 [23] | Antithrombotic 12.6% Antineoplastic agents 12.6% Diuretics 9.0% Analgesics 9.0% Anxiolytics/hypnotics/antipsychotics 6.6% |
Old age (P<0.001) |
| ReppK. et al, 2012 [5] | Immunosuppressant (63%) Antimicroblal (11%) Electrolyte/Fuid (11%) Anticoagulant (5%) |
NR |
| Al-Arifi M. et al, 2014 [4] | Antihypertensive agents (21.5%) Anticoagulants (14.3%)Immunosuppressant (12.5%) Chemotherapeutic agents (10.7%) |
NR |
| Nickel C. et al, 2013 [26] | Thiazides Benzodiazepines Antidepressants Anticonvulsants |
NR |
| Gustafsson M. et al, 2016 [16] | Cardiovascular drugs (29.5 %) Psychotropic drugs (27.3 %) | Poly-pharmacy |
| Jatau A. et al, 2015 [18] | Antidiabetics (23.3 %) Antihypertensives (21.1 %) Antibiotics (9.8 %) Anti-asthmatics (8.3 %) Diuretics (6.0 %) |
NR |
| Ruiter Ret al, 2012 [10] | Anticoagulants Antineoplastic and immunosuppressive drugs Antidiabetic agents High-ceiling diuretics Salicylates Antirheumatics |
Age >75 years Female sex |
| Pedrós C.et al, 2016 [24] | High-ceiling diuretics ACE inhibitors Cardiac glycosides |
NR |
| Ahern F, et al, 2013 [32] | Diuretics (n=22), Aspirin (n=5) Warfarin (n=4) |
Poly-pharmacy |
| Pedrós C. et al, 2014 [25] | Diuretics 69 (18.1 %) Antithrombotic drugs 63 (16.5 %) RAAS inhibitors 56 (14.7 %) NSAIDs 43 (11.3 %) |
Age >65 years Poly-pharmacy |
| Karuppannan M. et al, 2013 [27] | Antidiabetic 36 (38.3%) Antiplatelet 10 (10.6%) Thiazide diuretic 10 (10.6%) ACE Inhibitor 10 (10.6%) CCB 10 (10.6%) |
NR |
| Skoldunger A. et al, 2015 [34] | NR | Old age, Male sex, Living at home (community dwelling), Lower educational level, Functional dependence, Multiple co-morbidity. |
| Marcum Z. et al, 2012 [33] | Beta-blocker Oral hypoglycemic agent Thiazide diuretic Anticoagulant Antidepressant NSAIDs |
Poly-pharmacy |
Drugs and other factors that are associated with drug related hospitalization
Drugs that were frequently reported as causing drug related admission were antithrombotic drugs, antihypertensive drugs, analgesics, anti-diabetics, antipsychotics, and anti-neoplastic drugs. Poly pharmacy, old age and female sex are mentioned as factors for drug related hospitalization by a number of studies. Presence of multiple co morbidity, lower educational level, functional dependence, young age and male sex were also mentioned in some studies as a factor that influence hospital admission due to drug related problems.
Preventability of DRPs that caused hospital admission
Around one third of drug related hospital admissions were definitely preventable and more than 40 % were potentially preventable. Report of the reviewed studies on the Preventability of Drug related hospitalization is indicated in Table 4.
Table 4.
Preventability of DRPs that caused hospital admission
| Author, year | Not preventable (%) | Potentially preventable (%) | Definitely preventable (%) |
|---|---|---|---|
| Alghamdy M. et al, 2015 [20] | NR | 70 | NR |
| Chan A. et al, 2014 [21] | 45.7 | 52.4 | 15.2 |
| Benard-laribiere A. et al, 2015 [23] | 16.5 | 16.5 | 32 |
| ReppK. et al, 2012 [5] | NR | NR | 58 |
| Al-Arifi M. et al, 2014 [4] | 14.3 | 53.6 | 32.1 |
| Jatau A. et al, 2015 [18] | 33.1 | 11.3 | 55.5 |
| Ahern F, et al, 2013 [32] | 33.3 | 52 | 5.3 |
| Marcum Z. et al, 2012 [33] | NR | NR | 36.8 |
| Average | 28.6% | 42.6% | 33.6% |
Discussion
This systematic review summarizes prevalence of hospital admissions due to drug-related problems and preventability of drug related hospital admissions. In addition, the study has also extorted findings to identify the common types of DRPs that caused hospital admission, and associated factors responsible for drug related hospital admission from 16 different studies published recently.
The rate of drug related hospital admission varies from 1.3% to 41.3% with the average rate of 15.4%. This figure indicated that the burden of DRPs as a cause of hospitalization is very significant. In addition to hospital admission, DRP may contribute to poor patients’ clinical outcome at discharge such as disability or death. Chiefly ADRs can be potentially lethal and are a main cause of mortality [19]. The mortality rate among patients hospitalized due to drug related problems as reported in the seven studies included in this review [5, 20-25] was up to 5.7% with the average death rate of 2.7 %.
The types of DRPs causing hospital admission varied across the studies reviewed. Among the twelve studies that have reported types of DRPs causing hospital admission, six [4, 5, 16, 20, 21, 26] have explicitly reported the frequencies of each type of DRPs responsible for hospital admission. As a result, ADR in 4 studies [4, 5, 21, 26], noncompliance in Alghamdyet al., [20]study and dosage too high in Gustafssonet al. [16] study were identified as the most frequently occurring types of DRPs that caused hospital admission. However, Jatauet al., [18] and Karuppannanet al., [27] have assessed prevalence of admissions due to ADE and both studies identified treatment failure as the most frequent cause of admission, which is in contrast to previous studies published before 2012 where ADRs was most common type of ADE accounted for 53-90% of ADE related admissions [1, 28-30] followed by therapeutic failure [31]. The other four studies [10, 23-25] in this review have determined ADR specific hospital admission and hence, Type A reaction in two studies [23, 25] and acute renal failure in Pedróset al.,[24] study have been reported to be the most common subtypes of ADR that caused hospital admission.
There have not been any standardized methods of classifying drugs making it difficult for comparisons as to which drug causes drug related hospital admission across different studies. Concordant with the studies included in the present review [10, 16, 18, 24, 25, 32] a previous review that took studies published before 2012 mentions, cardiovascular drugs (antithrombotic drugs, antihypertensive drug), antineoplastic agents, anti-inflammatory and antidiabetic agents as a commonly reported drug classes causing hospital admission [3].
Age is the most frequently mentioned factor for drug related hospital admission. In line with the result of this review old age was identified as a major risk factor for drug related hospital admission in many other studies [3, 7, 12, 13, 17]. The main reason for geriatric population to be more susceptible for admission due to DRPs could be due to physiological and pathological changes occurred at advanced age which leads to a change in pharmacodynamics and pharmacokinetics of a drug in elderly. Drug absorption, distribution metabolism and excretion will be significantly affected in older people which may subsequently lead to toxicity and complication which necessitates hospitalization. In addition polypharmacy [16, 25, 32, 33], gender [10, 21], presence of multiple co morbidity [34], lower educational level and functional dependence [34] were also mentioned as a factor that influence hospital admission due to drug related problems. Similarly previous studies also agree that the above mentioned factors have significant association with drug related hospital admission [3, 5, 7, 12-17].
According to the current review significant numbers of DRPs were found to be either potentially or definitely preventable. Hence, several strategies can be designed to minimize those preventable DRPs, thereby curbing the risk of hospital admission. Health care providers should be aware of the common risk factors so as to lower hospital admission due to DRPs. Furthermore, prescribers are in a better position to lessen inappropriate prescribing and identifying the associated factors with DRPs. Pharmacists should also be involved in medication review and reconciliation and actively participate in minimizing poly pharmacy so as to lower the incidence of drug related admissions.
Drug related problems contribute for more than 15% of hospital admissions. Higher risk of admission due to DRPs was observed in patients who were on poly pharmacy and those who were old. As most of drug related hospital admissions were preventable an emphasis should be given for preventive strategies to avoid costs and complications associated with admission.
Acknowledgments
We would like to thank University of Gondar for providing us an internet access for searching literatures to realize this review.
Author contributions:
All authors contributed toward literaturesearching, drafting and critically revising the paper and agree to be accountable forall aspects of the work.
Conflict of Interest:
The author reports no conflicts of interest in this work.
References
- 1.Bhalla N, Duggan C, Dhillon S. The incidence and nature of drug-related admissions to hospital. Pharmaceutical Journal. 2003 [Google Scholar]
- 2.Roxburgh A, Degenhardt L. Characteristics of drug-related hospital separations in Australia. Drug Alcohol Depend. 2008;92(1-3):149–55. doi: 10.1016/j.drugalcdep.2007.07.020. [DOI] [PubMed] [Google Scholar]
- 3.Nivya K, Sri Sai Kiran V, Ragoo N, Jayaprakash B, Sonal Sekhar M. Systemic review on drug related hospital admissions - A pubmed based search. Saudi Pharm J. 2015;23(1):1–8. doi: 10.1016/j.jsps.2013.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Al-Arifi M, Abu-Hashem H, Al-Meziny M, Said R, Aljadhey H. Emergency department visits and admissions due to drug related problems at Riyadh military hospital (RMH), Saudi Arabia. Saudi Pharm J. 2014;22(1):17–25. doi: 10.1016/j.jsps.2013.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Repp KL, Hayes C 3rd, Woods TM, Allen KB, Kennedy K, Borkon MA. Drug-related problems and hospital admissions in cardiac transplant recipients. Ann Pharmacother. 2012;46(10):1299–307. doi: 10.1345/aph.1R094. [DOI] [PubMed] [Google Scholar]
- 6.Conforti A, Costantini D, Zanetti F, Moretti U, Grezzana M, Leone R. Adverse drug reactions in older patients: an Italian observational prospective hospital study. Drug Healthc Patient Saf. 2012;4:75–80. doi: 10.2147/DHPS.S29287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Davies EC, Green CF, Mottram DR, Rowe PH, Pirmohamed M. Emergency re-admissions to hospital due to adverse drug reactions within 1 year of the index admission. Br J Clin Pharmacol. 2010;70(5):749–55. doi: 10.1111/j.1365-2125.2010.03751.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pérez Menéndez-Conde C, Bermejo Vicedo T, Delgado Silveira E, Carretero Accame E. Adverse drug reactions which provoke hospital admission. Farm Hosp. 2011;35(5):236–43. doi: 10.1016/j.farma.2010.08.003. [DOI] [PubMed] [Google Scholar]
- 9.osthumus AA, Alingh CC, Zwaan CC, van Grootheest KK, Hanff LL, Witjes BB, et al. Adverse drug reaction-related admissions in paediatrics, a prospective single-centre study. BMJ Open. 2012;2(4): e000934. doi: 10.1136/bmjopen-2012-000934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ruiter R, Visser LE, Rodenburg EM, Trifiró G, Ziere G, Stricker BH. Adverse drug reaction-related hospitalizations in persons aged 55 years and over: a population-based study in the Netherlands. Drugs Aging. 2012;29(3):225–232. doi: 10.2165/11599430-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 11.Stausberg J, Hasford J. Drug-related admissions and hospital-acquired adverse drug events in Germany: a longitudinal analysis from 2003 to 2007 of ICD-10-coded routine data. BMC Health Serv Res. 2011;11:134. doi: 10.1186/1472-6963-11-134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hartholt KA, van der Velde N, Looman CW, Panneman MJ, van Beeck EF, Patka P, et al. Adverse drug reactions related hospital admissions in persons aged 60 years and over, The Netherlands, 1981-2007: less rapid increase, different drugs. PLoS One. 2010;5(11):e13977. doi: 10.1371/journal.pone.0013977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Carrasco-Garrido P, de Andrés LA, Barrera VH, de Miguel GA, Jiménez-García R. Trends of adverse drug reactions related-hospitalizations in Spain (2001-2006) BMC Health Serv Res. 2010;10:287. doi: 10.1186/1472-6963-10-287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wu C, Bell CM, Wodchis WP. Incidence and economic burden of adverse drug reactions among elderly patients in Ontario emergency departments: a retrospective study. Drug Saf. 2012;35(9):769–81. doi: 10.1007/BF03261973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rodenburg EM, Stricker BH, Visser LE. Sex-related differences in hospital admissions attributed to adverse drug reactions in the Netherlands. Br J Clin Pharmacol. 2011;71(1):95–104. doi: 10.1111/j.1365-2125.2010.03811.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gustafsson M, Sjölander M, Pfister B, Jonsson J, Schneede J, Lövheim H. Drug-related hospital admissions among old people with dementia. Eur J Clin Pharmacol. 2016;72(9):1143–53. doi: 10.1007/s00228-016-2084-3. [DOI] [PubMed] [Google Scholar]
- 17.Wu TY, Jen MH, Bottle A, Molokhia M, Aylin P, Bell D, et al. Ten-year trends in hospital admissions for adverse drug reactions in England 1999-2009. J R Soc Med. 2010;103(6):239–50. doi: 10.1258/jrsm.2010.100113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jatau AI, Aung MM, Kamauzaman TH, Rahman AF. Prevalence of Drug-Related Emergency Department Visits at a Teaching Hospital in Malaysia. Drugs Real World Outcomes. 2015;2(4):387–395. doi: 10.1007/s40801-015-0045-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998;279(15):1200–5. doi: 10.1001/jama.279.15.1200. [DOI] [PubMed] [Google Scholar]
- 20.Alghamdy MS, Randhawa MA, Al-Wahhas MH, Al-Jumaan MA. Admissions for drug-related problems at the Emergency Department of a University Hospital in the Kingdom of Saudi Arabia. J Family Community Med. 2015;22(1):44–8. doi: 10.4103/2230-8229.149590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chan A, Soh D, Ko Y, Huang YC, Chiang J. Characteristics of unplanned hospital admissions due to drug-related problems in cancer patients. Support Care Cancer. 2014;22(7):1875–81. doi: 10.1007/s00520-014-2160-0. [DOI] [PubMed] [Google Scholar]
- 22.Schmiedl S, Rottenkolber M, Hasford J, Rottenkolber D, Farker K, Drewelow B, et al. Self-medication with over-the-counter and prescribed drugs causing adverse-drug-reaction-related hospital admissions: results of a prospective, long-term multi-centre study. Drug Saf. 2014;37(4):225–35. doi: 10.1007/s40264-014-0141-3. [DOI] [PubMed] [Google Scholar]
- 23.Bénard-Laribière A, Miremont-Salamé G, Pérault-Pochat MC, Noize P, Haramburu F. EMIR Study Group on behalf of the French network of pharmacovigilance centres Incidence of hospital admissions due to adverse drug reactions in France: the EMIR study. Fundam Clin Pharmacol. 2015;29(1):106–11. doi: 10.1111/fcp.12088. [DOI] [PubMed] [Google Scholar]
- 24.Pedrós C, Formiga F, Corbella X, Arnau JM. Adverse drug reactions leading to urgent hospital admission in an elderly population: prevalence and main features. Eur J Clin Pharmacol. 2016;72(2):219–26. doi: 10.1007/s00228-015-1974-0. [DOI] [PubMed] [Google Scholar]
- 25.Pedrós C, Quintana B, Rebolledo M, Porta N, Vallano A, Arnau JM. Prevalence, risk factors and main features of adverse drug reactions leading to hospital admission. Eur J Clin Pharmacol. 2014;70(3):361–7. doi: 10.1007/s00228-013-1630-5. [DOI] [PubMed] [Google Scholar]
- 26.Nickel CH, Ruedinger JM, Messmer AS, Maile S, Peng A, Bodmer M, et al. Drug-related emergency department visits by elderly patients presenting with non-specific complaints. Scand J Trauma Resusc Emerg Med. 2013;21:15. doi: 10.1186/1757-7241-21-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Karuppannan M, Nee TK, Ali SM, Thong WK, Boardman H. The prevalence of adverse drug event-related admissions at a local hospital in Malaysia. Archives of Pharmacy Practice. 2013;4(4):160. [Google Scholar]
- 28.Saha L, Pandhi P, Malhotra S, Sharma N. Adverse Drug Event (ADE) related Medical Emergency Department visits and hospital admissions: a prospective study from a North Indian Referral Hospital. J Clin Diag Res. 2008;2(2):600–4. [Google Scholar]
- 29.Chan M, Nicklason F, Vial JH. Adverse drug events as a cause of hospital admission in the elderly. Intern Med J. 2001;31(4):199–205. doi: 10.1046/j.1445-5994.2001.00044.x. [DOI] [PubMed] [Google Scholar]
- 30.Hallas J, Gram LF, Grodum E, Damsbo N, Brøsen K, Haghfelt T, et al. Drug related admissions to medical wards: a population based survey. Br J Clin Pharmacol. 1992;33(1):61–8. doi: 10.1111/j.1365-2125.1992.tb04001.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zargarzadeh AH, Emami MH, Hosseini F. Drug-related hospital admissions in a generic pharmaceutical system. Clin Exp Pharmacol Physiol. 2007;34(5-6):494–8. doi: 10.1111/j.1440-1681.2007.04600.x. [DOI] [PubMed] [Google Scholar]
- 32.Ahern F, Sahm LJ, Lynch D, McCarthy S. Determining the frequency and preventability of adverse drug reaction-related admissions to an Irish University Hospital: a cross-sectional study. Emerg Med J. 2014;31(1):24–9. doi: 10.1136/emermed-2012-201945. [DOI] [PubMed] [Google Scholar]
- 33.Marcum ZA, Amuan ME, Hanlon JT, Aspinall SL, Handler SM, Ruby CM, et al. Prevalence of unplanned hospitalizations caused by adverse drug reactions in older veterans. J Am Geriatr Soc. 2012;60(1):34–41. doi: 10.1111/j.1532-5415.2011.03772.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sköldunger A, Fastbom J, Wimo A, Fratiglioni L, Johnell K. Impact of Inappropriate Drug Use on Hospitalizations, Mortality, and Costs in Older Persons and Persons with Dementia: Findings from the SNAC Study. Drugs Aging. 2015;32(8):671–8. doi: 10.1007/s40266-015-0287-4. [DOI] [PMC free article] [PubMed] [Google Scholar]