

Abstract
Anastomotic dehiscence and leak are dreaded complications after a colorectal resection and can often present with rectal bleeding and pelvic abscess or sepsis. Although most cases of bleeding after gastrointestinal anastomoses are minor and self-limited, major bleeding, as defined by hemodynamic instability or the need for blood transfusions, poses a significant challenge for management. Here we report a case in which a patient presenting with profuse rectal bleeding and pelvic hematoma secondary to a colorectal anastomotic leak was treated endoscopically with 50% dextrose spray then enema.
Keywords: Endoscopy, gastrointestinal bleeding, dextrose
Introduction
Anastomotic leaks after colorectal resection can cause morbidity and mortality [1, 2]. Most leaks become apparent 2–7 days after surgery, and may be either intra- or extra-peritoneal. Clinical presentation may vary, including subclinical leaks, rectal bleeding, localized or generalized peritonitis and pelvic hematoma/abscess. Management includes observation, bowel rest, antibiotics, percutaneous drainage, endoscopic therapies, surgical revision or bowel diversion [3]. Endoscopic therapy is the mainstay in the management of major anastomotic bleeding, employing conventional modalities such as irrigation with isotonic saline, electrocoagulation, epinephrine injection or hemostatic clips [4–8]. However, bleeding from anastomotic sites is usually diffuse mucosal in origin, and can be challenging to control using such conventional modalities. In addition, it is often technically difficult to secure good apposition of the unhealthy tissue at these anastomotic margins with sutures or clips. We report a unique case where hypertonic dextrose spray followed by dextrose enema was used successfully to treat anastomotic bleeding and hematoma.
Case presentation
The patient was a 63-year-old male who was transferred to Cleveland Clinic for an opinion regarding management of a colorectal anastomotic leak with hematochezia and a pelvic hematoma. He had a history of congestive heart failure, atrial fibrillation (on warfarin) and prostate cancer for which he underwent prostatectomy and radiation in 2009. He underwent low anterior resection with diverting loop ileostomy at another facility for recently diagnosed rectal cancer and was discharged home on enoxaparin on Day 6 after surgery. He was readmitted on the same day with profuse hematochezia with anemia requiring blood transfusion. Computed tomography (CT) scan of pelvis initially demonstrated a 9-cm pre-sacral collection, which was later confirmed to be a pelvic hematoma. Anticoagulation was discontinued but hematochezia persisted. Subsequent CT scan showed persistent organized hemorrhage with increasing air lucency concerning abscess/leak, and the patient elected to come to us for a second opinion. On presentation to our emergency room, he had persistent hematochezia with passage of staples per rectum, with no other gastrointestinal symptoms, and stable vital signs. The ileostomy site looked healthy and non-infected. Anorectal exam revealed dark and bright blood, otherwise unrevealing. Other systemic exam was unremarkable. The results of lab examinations showed as follows: hemoglobin concentration, 124 g/L; mean corpuscular volume (MCV), 88.1 fL; platelet count, 158 000/µL; activated partial thromboplastin time (aPTT), 25.4 s; and international normalized ratio (INR), 1.2. Hepatic and renal function panels were within normal limits.
CT-guided percutaneous aspiration of pelvic collection revealed non-purulent bloody fluid, with culture revealing poly-microbial growth, for which he was treated with ciprofloxacin and metronidazole. Flexible sigmoidoscopy revealed a defect about 5–6 cm long with a 1-cm orifice at the colorectal anastomotic site and hematoma in the lumen (Figure 1). The bleeding source was not identified. Therefore, conventional endoscopic approaches, such as hemo-clips and thermotherapy, were not feasible. Fibrous tissue was noted at the anastomotic site as a result of anastomotic tension and recent radiation therapy for prostate cancer. Unhealthy tissue at the margins of the anastomotic leak precluded the deployment of endoscopic sutures, as tissue apposition would have been suboptimal. For a similar reason, over-the-scope clip (OTSC) would not have been adequate. Moreover, OTSC often migrates due to intestinal peristalsis [9]. We decided not to use sutures or clips to treat the defect due to the above-mentioned reasons. During the procedure, the defect and bleeding hematoma was sprayed with 50% dextrose. The bleeding was temporarily controlled (Figure 2). Twelve hours after the hypertonic dextrose spray, bleeding recurred. He was readmitted and received 250 mL of 50% dextrose enema twice, with progressive reduction and cessation of bleeding. He had no recurrence of bleeding and was discharged home with 250 mL of 50% dextrose enema twice daily for the following 10 days. The patient had persistent bleeding for close to 20 days before the endoscopic intervention. Spraying of 50% dextrose at the bleeding site resulted in significant control, and the subsequent administration of hypertonic dextrose enema for 2 weeks resulted in permanent cessation of the bleeding, making it unlikely that the bleeding stopped spontaneously. We did not use hemospray to treat the bleed because it is not yet approved by the Food and Drug Administration (FDA) and is used only for research purposes at our institution. During the follow-up, he has not had re-bleeding and the anastomotic leak has healed (Figure 3), although the previous hematoma was replaced by a pre-sacral sinus, at the colorectal anastomotic site. The pre-sacral sinus was treated subsequently with endoscopic needle knife sinusotomy.
Figure 1.
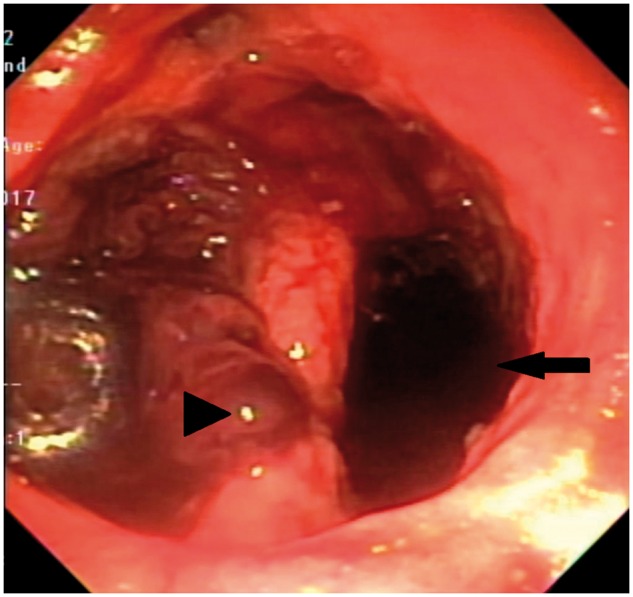
Pre-sacral hematoma from anastomotic leak before hypertonic dextrose treatment. Arrow indicates colonic lumen and arrowhead shows the site of the defect.
Figure 2.
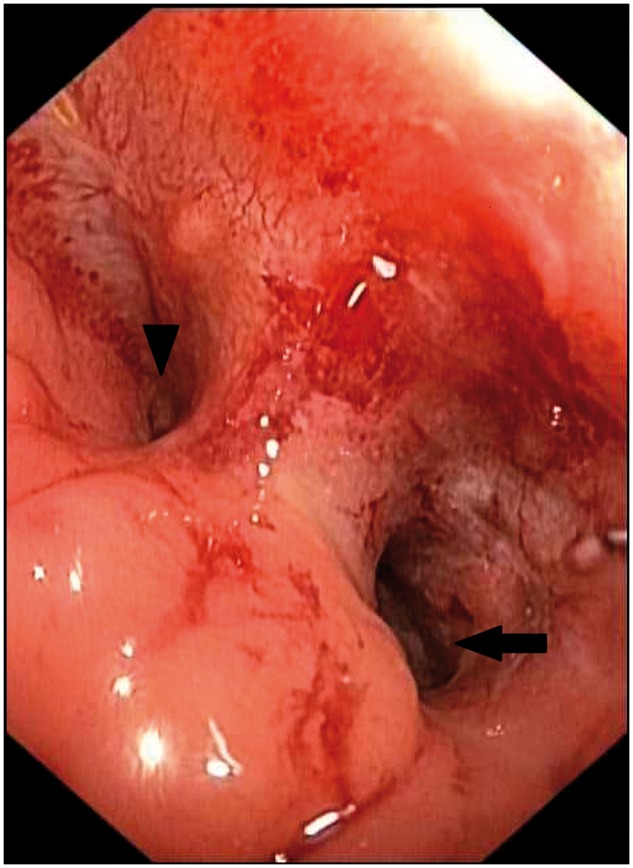
Healed anastomotic leak after hypertonic dextrose. Arrow shows colon lumen and arrowhead indicates the pre-sacral sinus.
Figure 3.

Barium enema after hypertonic dextrose treatment showing resolution of the anastomotic leak.
Discussion
Major anastomotic bleeding is a dangerous complication after colorectal resection, with incidence rates of 0.5–4.2% [5, 7]. No specific risk factors have been identified. Initial management is supportive with blood transfusions and correction of any underlying coagulopathy [10]. In stable patients with persistent bleeding, endoscopic management is the first-line treatment, with surgical intervention reserved for unstable patients or those who fail conservative treatment [5, 7, 10]. Endoscopic techniques to achieve hemostasis in this setting have included irrigation with isotonic saline, electrocoagulation, epinephrine injection and hemostatic clips [4–8]. Angiographic localization with intra-arterial vasopressin injection may also be used, but complications like ischemia and anastomotic dehiscence may occur [11]. If these measures fail, reoperation with resection of bleeding anastomosis may be performed as a last resort [6, 10].
We report a unique case of major anastomotic bleeding controlled with endoscopic hypertonic dextrose spray and enema. There is not much evidence supporting the use of dextrose in anastomotic bleeding, although it has been employed with remarkable success in other types of gastrointestinal bleeding. Hypertonic dextrose endoscopic injection has been used successfully to treat bleeding gastric varices [12], peptic ulcers [13] and hemorrhoids [14] with no significant increase in complications such as re-bleeding or the need for subsequent surgeries compared to other available techniques and sclerosants. In a prospective randomized trial, hypertonic glucose was found to be superior to sodium tetradecyl sulphate as a sclerosant in treating gastric variceal bleeding in advanced liver cirrhosis patients [15]. Our group previously reported two cases where hypertonic dextrose spray was used successfully for bleeding—one from radiation enteritis [16] and the other in diversion pouchitis [17]. It has also been used as an adjuvant treatment of residual gastric varices after tissue adhesive injections, thereby reducing risk of re-bleeding [18]. Hypertonic dextrose spray could be a safe, effective and easily available alternative to other hemostatic measures, particularly when there is diffuse mucosal bleeding, which may be challenging to control. In our patient, the combined treatment with hypertonic dextrose spray and enema also assisted in the healing of the anastomotic defect without the need for surgical repair. Hypertonic dextrose causes osmotic dehydration, thereby inducing mural necrosis of blood vessels, resulting in their obliteration, along with inflammation and fibrosis in the perivascular space. This has previously been shown to promote control of bleeding and also to help in the coaptation of tissue margins, thereby promoting mucosal healing [14–17]. Theoretical concerns regarding widening of a mucosal defect due to vascular mural necrosis have not been borne out in previous studies [18, 19]. It may cause mild hyperglycemia, particularly in diabetic patients, but it is usually transient and not of much concern [16, 17].
In conclusion, we describe a case where hypertonic dextrose was successfully used to treat anastomotic bleeding. Further studies need to be conducted to validate the effectiveness of this modality.
Acknowledgements
B.S. is supported by the Ed and Joey Story Endowed Chair. Informed consent was obtained from the patient for publication of case details. P.S. gathered the data and drafted the manuscript, G.K. critically revised the manuscript and B.S. conceived of this study, performed the endoscopic procedure and critically revised the manuscript.
Conflicts of interest
None declared.
References
- 1. Blumetti J, Abcarian H.. Management of low colorectal anastomotic leak: preserving the anastomosis. World J Gastrointest Surg 2015;7:378–83 [PMID: 26730283 PMCID: PMC4691718 DOI: 10.4240/wjgs.v7.i12.378]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Daams F, Luyer M, Lange JF.. Colorectal anastomotic leakage: aspects of prevention, detection and treatment. World J Gastroenterol 2013;19:2293–7 [PMID: 23613621 PMCID: PMC3631979 DOI: 10.3748/wjg.v19.i15.2293]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Phitayakorn R, Delaney CP, Reynolds HL. et al. International Anastomotic Leak Study G. Standardized algorithms for management of anastomotic leaks and related abdominal and pelvic abscesses after colorectal surgery. World J Surg 2008;32:1147–56 [PMID: 18283511 DOI: 10.1007/s00268-008-9468-1]. [DOI] [PubMed] [Google Scholar]
- 4. Besson R, Christidis C, Denet C. et al. Management of postoperative bleeding after laparoscopic left colectomy. Int J Colorectal Dis 2016;31:1431–6 [PMID: 27270479 DOI: 10.1007/s00384-016-2612-8]. [DOI] [PubMed] [Google Scholar]
- 5. Cirocco WC, Golub RW.. Endoscopic treatment of postoperative hemorrhage from a stapled colorectal anastomosis. Am Surg 1995;61:460–3 [PMID: 7733557]. [PubMed] [Google Scholar]
- 6. Davis B, Rivadeneira DE.. Complications of colorectal anastomoses: leaks, strictures, and bleeding. Surg Clin North Am 2013;93:61–87 [PMID: 23177066 DOI: 10.1016/j.suc.2012.09.014]. [DOI] [PubMed] [Google Scholar]
- 7. Malik AH, East JE, Buchanan GN. et al. Endoscopic haemostasis of staple-line haemorrhage following colorectal resection. Colorectal Dis 2008;10:616–8 [PMID: 18215199 DOI: 10.1111/j.1463-1318.2007.01459.x]. [DOI] [PubMed] [Google Scholar]
- 8. Lou Z, Zhang W, Yu E. et al. Colonoscopy is the first choice for early postoperative rectal anastomotic bleeding. World J Surg Oncol 2014;12:376 [PMID: 25481545 PMCID: PMC4295568 DOI: 10.1186/1477-7819-12-376]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kochhar GS, Shen B.. Endoscopic treatment of leak at the tip of the ‘J’ ileal pouch. Endosc Int Open 2017;5:E64–6 [PMID: 28180150 PMCID: PMC5283172 DOI: 10.1055/s-0042-121664]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Martinez-Serrano MA, Pares D, Pera M. et al. Management of lower gastrointestinal bleeding after colorectal resection and stapled anastomosis. Tech Coloproctol 2009;13:49–53 [PMID: 19288245 DOI: 10.1007/s10151-009-0458-6]. [DOI] [PubMed] [Google Scholar]
- 11. Atabek U, Pello MJ, Spence RK. et al. Arterial vasopressin for control of bleeding from a stapled intestinal anastomosis: report of two cases . Dis Colon Rectum 1992;35:1180–2 [PMID: 1473423]. [DOI] [PubMed] [Google Scholar]
- 12. Chang KY, Wu CS, Chen PC.. Endoscopic treatment of bleeding fundic varices with 50% glucose injection. Endoscopy 1996;28:398 [PMID: 8813512 DOI: 10.1055/s-2007-1005490]. [DOI] [PubMed] [Google Scholar]
- 13. Lin HJ, Chan CY, Lee FY. et al. Endoscopic injection to arrest peptic ulcer hemorrhage: a prospective, randomized controlled trial; preliminary results. Hepatogastroenterology 1991;38:291–4 [PMID: 1937373]. [PubMed] [Google Scholar]
- 14. Alatise OI, Arigbabu OA, Lawal OO. et al. Endoscopic hemorrhoidal sclerotherapy using 50% dextrose water: a preliminary report. Indian J Gastroenterol 2009;28:31–2 [PMID: 19529900 DOI: 10.1007/s12664-009-0007-2]. [DOI] [PubMed] [Google Scholar]
- 15. Chang KY, Wu CS, Chen PC.. Prospective, randomized trial of hypertonic glucose water and sodium tetradecyl sulfate for gastric variceal bleeding in patients with advanced liver cirrhosis. Endoscopy 1996;28:481–6 [PMID: 8886633 DOI: 10.1055/s-2007-1005527]. [DOI] [PubMed] [Google Scholar]
- 16. Tian C, Mehta P, Shen B.. Endoscopic therapy of bleeding from radiation enteritis with hypertonic glucose spray. ACG Case Rep J 2014;1:181–3 [PMID: 26157869 PMCID: PMC4435317 DOI: 10.14309/crj.2014.45]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Nyabanga CT, Shen B.. Endoscopic treatment of bleeding diversion pouchitis with high-concentration dextrose spray. ACG Case Rep J 2017;4:e51 [PMID: 28377939 PMCID: PMC5371723 DOI: 10.14309/crj.2017.51]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Kuo MJ, Yeh HZ, Chen GH. et al. Improvement of tissue-adhesive obliteration of bleeding gastric varices using adjuvant hypertonic glucose injection: a prospective randomized trial. Endoscopy 2007;39:487–91 [PMID: 17354182 DOI: 10.1055/s-2007-966267]. [DOI] [PubMed] [Google Scholar]
- 19. Nyabanga CT, Obusez EC, Purysko A. et al. Healing of a chronic anal stump sinus after administration of combined high-concentration dextrose and doxycycline solution. Int J Colorectal Dis 2016;31:775–6 [PMID: 26077670 DOI: 10.1007/s00384-015-2281-z]. [DOI] [PubMed] [Google Scholar]