

Abstract
Background
Epilepsy is one of the most common neurological disorders with about 30% treatment failure rate. An interindividual variations in efficacy of antiepileptic drugs (AEDs) make the treatment of epilepsy challenging, which can be attributed to genetic factors such as ATP-Binding Cassette sub-family B, member1 (ABCB1) gene polymorphisms.
Objective
The main objective of the present study is to evaluate the association of ABCB1 C1236T, G2677T, and C3435T polymorphisms with treatment response among Tunisian epileptic patients.
Materials and Methods
One hundred epileptic patients, originated from north of Tunisia, were recruited and categorized into 50 drug-resistant and 50 drug-responsive patients treated with antiepileptic drugs (AEDs) as per the International League Against Epilepsy. DNA of patients was extracted and ABCB1 gene polymorphisms studied using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method.
Results
The C1236T, G2677T, and C3435T polymorphisms were involved into AED resistance. Significant genotypic (C1236T TT (p ≤ 0.001); G2677T TT (p = 0.001); C3435T TT (p ≤ 0.001)) and allelic associations (C1236T T (3.650, p ≤ 0.001); G2677TT (1.801, p = 0.044); C3435T T (4.730, p ≤ 0.001)) with drug resistance epilepsy (DRE) were observed. A significant level of linkage disequilibrium (LD) was also noted between ABCB1 polymorphisms. Patients with the haplotypes CT and TT (C1236T-G2677T); GT, TC, and TT (G2677T-C3435T); CT and TT (C1236T-C3435T); CTT, TTC, TGT, and TTT (C1236T-G2677T-C3435T) were also significantly associated to AED resistance.
Conclusions
The response to antiepileptics seems to be modulated by TT genotypes, T alleles, and the predicted haplotypes for the tested SNPs in our population. Genetic analysis is a valuable tool for predicting treatment response and thus will contribute to personalized medicine for Tunisian epileptic patients.
1. Introduction
Epilepsy is one of the prevalent serious neurological disorders [1] affecting approximately 50 million people worldwide [2].
During the last years, a large variety of antiepileptic drugs (AEDs) with different mechanisms of action were developed, which makes the epilepsy treatment a big challenge [3–5]. In fact, at least one-third of epileptic patients are or become resistant to treatment and experience recurrent seizures [6, 7]. This pharmacoresistance depends on several factors primarily age, epileptic etiology, type, and syndrome, AEDs [8].
Moreover, genetic factors play an important role in the development of refractory epilepsy. Indeed, the prediction of the individual's response to AEDs is very helpful for knowing drug resistance mechanisms which will allow the selection of the appropriate type of drug treatment and early epilepsy surgical evaluation. Several studies focused on identifying the potential genetic markers affecting the pharmacoresistance. They provided several genetic variations affecting pharmacokinetics or pharmacodynamics of AEDs in the treatment of epilepsy. These research works also evaluated the association between variations in drug transporter and their target receptor genes and the occurrence of refractory seizures [9, 10].
One of the best studied drug transporters is the transmembrane P-glycoprotein (P-gp). This ATP-dependent efflux-pump protein ensuring the transport and elimination of diverse AEDs at the blood-brain barrier (BBB) is expressed in the brain (astrocytes, endothelial cells, and neurons) [11–16]. P-gp overexpression reduces the AEDs bioavailability in the epileptic cells, which contributes to refractory epilepsy. Some studies suggested that its altered function could be a result of genetic variants especially SNPs located in the ABCB1 gene [4, 17–25]. The most studied SNPs in this gene are C1236T (rs1128503) in exon 12, G2677T (rs2032582) in exon 21, and C3435T (rs1045642) in exon 26 [26–32].
The C3435T is commonly considered as a critical SNP in AED resistance [33–36]. Results of assessing the association of ABCB1 polymorphisms with the resistance to AEDs are discordant. An initial study reported that patients with drug resistance epilepsy (DRE), compared to AED responders, were more likely to have CC genotype (27.5% vs. 15.7%, respectively) than TT genotype (19.5% vs. 29.6%, respectively) [37]. This finding was confirmed in some studies [21, 27, 38, 39], while others showed an opposite result [29, 40–42]. Likewise, other studies [6, 43–47] and meta-analyses revealed no significant association between genetic profile and refractory epilepsy [35, 48–53]. These conflicting findings are essentially due to heterogeneity, phenotyping and genotyping errors, bias, etc.
Despite the fact that there was a significant interest in showing the associations between drug resistance and ABCB1 3435 genotypes, the clinical practice of a ABCB1 SNPs routine testing to predict the patient's response to the therapy has not been yet examined [32, 49, 54]. Therefore, we focus, in this work, on evaluating the relationship between the ABCB1 C1236T, G2677T, and C3435T polymorphisms and the pharmacoresistant epilepsy in Tunisian patients.
2. Materials and Methods
2.1. Study Population
The present study includes 100 Tunisian epileptic patients, originated from north of Tunisia (56 males and 44 females) with a mean age of 6.710 ± 4.358. All epilepsy patients were evaluated in the Neuro-pediatric Department at Mongi Ben Hamida National Institute of Neurology. They were diagnosed for epilepsy after a follow-up of one year or more and treated by AED monotherapy or bitherapy.
This study was conducted in accordance with the ethical standards of the declaration of Helsinki [55]. It was approved by a local human research ethics committee (HTHEC-2016-30). An informed consent was signed by all patients and/or their parents.
All subjects were examined by a qualified epilepsy neurologist and had a confirmed diagnosis based on the operational clinical definition of epilepsy [8] and classified according to the guidelines specified in the International League Against Epilepsy (ILAE) [56, 57].
Information on demographic and clinical characteristics were obtained from structured questionnaires and medical records database. The collected information included sex, age, age at seizure onset, family history of epilepsy, types and etiology of seizures, epileptic syndromes, treatment therapy, and the number of prescribed AEDs (Table 1).
Table 1.
General characteristics of the study population.
| Variables | Epileptic patients (N = 100) | Patient group (N = 50) | Control group (N = 50) | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex ratio | Male | 56 | 56 | 28 | 56 | 28 | 56 |
| Female | 44 | 44 | 22 | 44 | 22 | 44 | |
|
| |||||||
| Age (years) | 6.710 ± 4.358 | 6.220 ± 4.432 | 7.200 ± 4.271 | ||||
|
| |||||||
| Age at seizure onset (years) | 3.820 ± 3.362 | 2.680 ± 2.470 | 4.960 ± 3.752 | ||||
|
| |||||||
| Type of seizure | Generalized | 75 | 75 | 42 | 84 | 33 | 66 |
| Focal | 20 | 20 | 3 | 6 | 17 | 34 | |
| Focal to bilateral tonic-clonic | 5 | 5 | 5 | 10 | 0 | 0 | |
|
| |||||||
| Epileptic syndrome | Yes | 26 | 26 | 19a | 38 | 7b | 14 |
| No | 74 | 74 | 31 | 62 | 43 | 86 | |
|
| |||||||
| Etiology of epilepsy | Autoimmune | 0 | 0 | 0 | 0 | 0 | 0 |
| Genetic | 31 | 31 | 24 | 48 | 7 | 14 | |
| Infectious | 1 | 1 | 0 | 0 | 1 | 2 | |
| Metabolic | 1 | 1 | 0 | 0 | 1 | 2 | |
| Structural | 10 | 10 | 0 | 0 | 10 | 20 | |
| Unknown | 57 | 57 | 26 | 52 | 31 | 62 | |
|
| |||||||
| Medical history | Yes | 16 | 16 | 8c | 16 | 8d | 16 |
| No | 84 | 84 | 42 | 84 | 42 | 84 | |
|
| |||||||
| Antiepileptic treatment | Monotherapy | 34 | 34 | 0 | 0 | 34e | 68 |
| Bitherapy | 24 | 24 | 8f | 16 | 16g | 32 | |
| Polytherapy | 42 | 42 | 42h | 84 | 0 | 0 | |
Values (n and %). aAbsences, Angelman, continuous spikes and waves during sleep (CSWS), Dalla Benardina, Doose, Dravet, Ohtahara, early myoclonic encephalopathy (EME), generalized epilepsy with febrile seizures plus (GEFS+), juvenile myoclonic epilepsy (JME), Lennox-Gastaut, WEST. bAbsences, benign epilepsy with centro-temporal spikes (BECTS), early myoclonic encephalopathy (EME), idiopathic generalized epilepsies (IGE), tuberous sclerosis of Bourneville (STB). cAppendectomy, bronchopneumopathy, dehydration and gastroenteritis, febrile seizures, mental retardation with behavioral disorder, neonatal cyanosis, recurrent bilateral otitis media, recurrent urinary tract infections, varicella dAppendectomy, bilateral hernia, bilateral testicular ectopia, enuresis, febrile seizures, gastroesophageal reflux, trauma, maternal-feotal infection, mumps, neonatal hypoglycemia, strabismus, stunting delay. eControls were prescribed single AED (carbamazepine or valproic acid). fPatients were prescribed a combination of 2 AEDs (carbamazepine, clonazepam, lamotrigine, phenobarbital, valproic acid, vigabatrin). gControls were prescribed a combination of 2 AEDs (carbamazepine, clonazepam, phenobarbital, valproic acid). hPatients were prescribed a combination of diverse AEDs (carbamazepine, clobazam, clonazepam, diazepam, ethosuximide, lamotrigine, levetiracetam, phenobarbital, phenytoin, topiramate, valproic acid, vigabatrin).
2.1.1. Definition of Drug Resistance
According to the definition set by the ILAE, patients were considered as drug-resistant to epilepsy if the adequate trials of two tolerated and appropriately used AED schedules (whether monotherapies or combination) failed to achieve sustained seizure freedom [58].
The nonresponders must not have a lesional pharmacoresistant epilepsy [42, 59, 60].
All associated pathologies that might promote the occurrence of epileptic seizures and may lead to wrong diagnosis of epilepsy were excluded from this study (imaging abnormalities including tumor, progressive or degenerative neurological or systemic disorders, tuberculoma, multiple neurocysticercosis, vascular malformations, and atrophic lesions; hepatic, renal [42, 59, 60], gross neurological deficits (mental retardation, motor/speech), diabetes mellitus [60], hematopoietic [61], cardiac insufficiency [42, 62]; infectious, traumatic, metabolic, and deep psychiatric disorders [62]; cancers [42] or secondary metastases [31]).
On the other hand, any subject who neglected the treatment regimen or presented any exclusion criteria (verified poor compliance by performing blood tests of MAEs [63]; adverse drug reactions of AEDs [61]; alcohol, addiction [59], or drug intake (inducers or inhibitors of enzymes that metabolize MAEs; substrates or inhibitors of P-gp [63]), was also excluded from this work.
2.1.2. Definition of Drug Responsiveness
The patients were considered as drug-responsive if they did not have any type of seizures for, at least, 1 year during AED treatment [58, 64].
In our population, 50 drug-responsive patients constituting “the control group” (males : females = 28 : 22) were matched according to sex, age, and geographic region [42] with 50 drug-resistant patients constituting “the patient group” (males : females = 28 : 22). Refractory and responsive patients were unrelated (Table 1).
2.2. DNA Extraction and Genetic Analysis
Blood samples (5-10 ml) were collected in ethylenediamine tetraacetic acid (EDTA) tubes from each patient and control. Genomic DNA was isolated from whole blood samples. For all patients and controls, 3 SNPs of ABCB1 gene (C1236T, G2677T, and C3435T) were genotyped by polymerase chain reaction (PCR) assay using a SimpliAmp™ (Applied Biosystems-Life Technologies) followed by restriction fragment length polymorphism (RFLP) analysis. The fragments were amplified with 0.4 mM dNTPs, 4 mM MgCl2, nuclease-free water, reaction buffer, 20 μmol/l of primers, and 0.05 U Taq polymerase in a final volume of 50 μl using a PCR Master Mix (Thermo Fisher Scientific) using the following program for the 3 SNPs (rs1128503, rs2032582, rs1045642): 94°C for 2 min, 35 cycles (94°C for 30s, 60°C for 30s, 72°C for 30s), and 72°C for 7 min [65] (Table 2).
Table 2.
Sequences of F and R primers used in the study, Tm, and size of the amplicons for each SNP [65].
| SNP | Exon | Primer F | Primer R | Tm (°C) | Amplicon size (bp) |
|---|---|---|---|---|---|
| ABCB1 C1236T | 12 | TATCCTGTGTCTGTGAATTGCC | CCTGACTCACCACACCAATG | 60 | 366 |
| ABCB1 G2677T | 21 | TGCAGGCTATAGGTTCCAGG | TTTAGTTTGACTCACCTTCCCG | 60 | 224 |
| ABCB1 C3435T | 26 | TGTTTTCAGCTGCTTGATGG | AAGGCATGTATGTTGGCCTC | 60 | 197 |
F: forward; R: reverse; Tm: melting temperature; bp: base pair.
After amplification, PCR products were digested using 2 μl specific restriction endonucleases (HaeIII, BanI, and Sau3A1 (Thermo Fisher Scientific)), 9.5 μl nuclease-free water, 4.5 μl restriction enzyme buffer, and 4 μl PCR products in a final volume of 20 μl. The separated fragments were visualized on 3% agarose gel after incubation at 37°C for 16 h. The restriction specific sites and sizes of digested fragments are summarized in Table 3.
Table 3.
Size and restriction recognition sites of digested fragments for each SNP [65].
| SNP | Enzyme∗ | Unit size∗(U) | Restriction site∗ | Size of digested fragment (bp) |
|---|---|---|---|---|
| ABCB1 C1236T | HaeIII (BsuRI) | 3000 | 5′…GG⬇CC…3′ 3′…CC⬆GG…5′ |
Wild type: 269 + 62 + 35 |
| Mutated type: 269 + 97 | ||||
|
| ||||
| ABCB1 G2677T | BanI (BshNI) | 2000 | 5′…G⬇GYRCC…3′ 3′…CCRYG⬆G…5′ |
Wild type: 198 + 26 |
| Mutated type: 224 | ||||
|
| ||||
| ABCB1 C3435T | Sau3A1 (Bsp143I) | 1500 | 5′…⬇GATC…3′ 3′…CTAG⬆…5′ |
Wild type: 158 + 39 |
| Mutated type: 197 | ||||
∗ https://www.thermofisher.com/tn/en/home.html; U: units; bp: base pair.
2.3. Statistical Analysis
The chi-square (X2) test (2 × 2 contingency tables) was performed to compare allelic and genotypic distribution of ABCB1 C1236T, G2677T, and C3435T polymorphisms between drug-resistant group (patients group) and drug-responsive group (control group). The association is statistically significant when p-value is ≤0.05 [66]. The statistical analysis was conducted with logiciel Epi info™ 7 [67].
Linkage disequilibrium (LD) analysis and haplotype construction were carried out by SHEsis online software [68]. The r2 (correlation index) and D (LD coefficient) were calculated, to test the LD among the 3 loci. If r2 and ∣D′∣ = 1, the alleles are in a complete LD (separated by recombination). If r2 and ∣D′∣ < 1, the LD is disrupted. Associations between allelic, genotype, haplotype, and drug response were estimated by odds ratio (OR) with 95% confidence interval (CI).
3. Results
3.1. Demographics and Clinic Characteristics
The sex ratio was predominantly male (56 vs. 44%) with a mean age in years of 6.710 ± 4.358 and a mean age at seizure onset of 3.820 ± 3.362.
For patients group, the mean age was 6.220 ± 4.432 vs. 7.200 ± 4.271 for control one.
The mean age at seizure onset for nonresponders is 2.680 ± 2.470 and 4.960 ± 3.752 for responders.
Overall, the most common seizure type was generalized (75%). Focal and focal to bilateral tonic-clonic seizures were minoritary (20% and 5%, respectively).
In the drug-resistant group, 84% patients presented generalized seizures, 6% focal and 10% focal to bilateral tonic-clonic ones, whereas in the drug-responder group, 66% of patients presented generalized and 34% of focal seizures, but no focal to bilateral tonic-clonic seizures were observed.
The syndromes (such as absences, continuous spikes, and waves during sleep (CSWS), Lennox-Gastaut...) constituted only 26% of our epileptic patients: 38% in drug-resistant group vs. 14% in drug-responsive group.
The epileptic etiology for the epileptic patients was mainly unknown (57%). The main factor seems to be genetic (48%) for the drug-resistant patients with known etiology, whereas it seems to be a structural one (20%) for the drug-responsive patients.
The medical history observed is low (16%) in epileptic patients, drug responders, and none.
The patients enrolled in this study received mainly a polytherapy AEDs (42%) as well in drug-resistant patients (84%), while for the drug-responsive patients, it was a monotherapy (68%).
3.2. Polymorphisms Analysis and Susceptibility to DRE
3.2.1. Genotypic and Allelic Analysis
We found a significant allelic and genotypic association between C1236T, G2677T, and C3435T polymorphisms and response to AEDs (Figure 1). In fact, we observed that the TT genotypes and (p ≤ 0.001 for C1236T, p = 0.001 for G2677T, p ≤ 0.001 for C3435T) the T allele of the 3 SNPs (T vs. C, OR = 3.650, 2.029-6.563, p ≤ 0.001 for C1236T; T vs. C, OR = 1.801, 1.016-3.192, p = 0.044 for G2677T; T vs. C, OR = 4.730, 2.604-8.591, p ≤ 0.001 for C3435T) were significantly more frequent in drug-resistant patients than in drug-responsive patients. The ABCB1 genotype and allele frequencies are shown in Tables 4 and 5, respectively.
Figure 1.
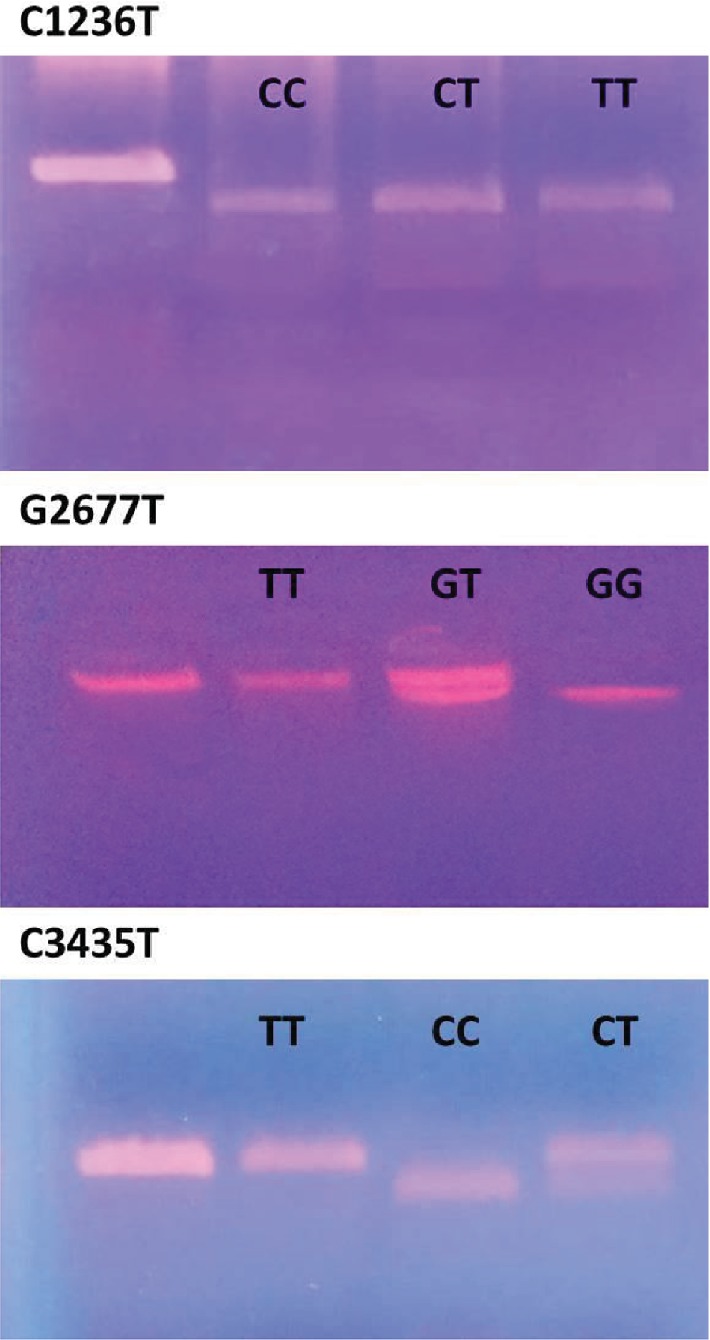
Results of digestion for the three SNPs. For C1236T, well 1: PCR product, well 2: homozygous wild-type CC, well 3: heterozygous CT, and well 4: homozygous mutant type TT. For G2677T, well 1: PCR product, well 2: homozygous mutant-type TT, well 3: heterozygous CT, and well 4: homozygous wild-type GG. For C3435T, well 1: PCR product, well 2: homozygous mutant-type TT, well 3: homozygous wild-type CC, and well 4: heterozygous CT.
Table 4.
Distribution of ABCB1 genotypes frequencies in drug-responsive and drug-resistant patients.
| SNP | ABCB1 genotype | Drug-resistant patients (N = 50) | Drug-responsive patients (N = 50) |
ORs | 95% CI | p value | X 2 | ||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||||
| ABCB1 C1236T | CC vs. CT+TT | 6 | 12 | 17 | 34 | 0.265 | 0.094-0.745 | 0 .012 | 6.830 |
| CT vs. CC+TT | 18 | 56 | 27 | 54 | 0.479 | 0.215-1.068 | 0.072 | 3.270 | |
| TT vs. CC+CT | 26 | 52 | 6 | 12 | 7.944 | 2.872-21.978 | ≤0.001 | 18.380 | |
| TT vs. CC | 26 | 52 | 6 | 12 | 12.278 | 3.393-44.433 | ≤0.001 | 16.740 | |
| CT vs. CC | 18 | 56 | 27 | 54 | 1.889 | 0.625-5.705 | 0.260 | 2.890 | |
| TT vs. CT | 26 | 52 | 6 | 12 | 6.500 | 2.231-18.940 | ≤0.001 | 12.990 | |
|
| |||||||||
| ABCB1 G2677T | GG vs. GT+TT | 10 | 20 | 3 | 6 | 3.917 | 1.008-15.220 | 0.049 | 4.330 |
| GT vs. GG+TT | 13 | 26 | 41 | 82 | 0.077 | 0.030-0.201 | ≤0.001 | 31.560 | |
| TT vs. GG+GT | 27 | 54 | 6 | 12 | 8.609 | 3.110-23.832 | ≤0.001 | 19.950 | |
| TT vs. GG | 27 | 54 | 6 | 12 | 1.350 | 0.282-6.453 | 0.707 | 0.140 | |
| GT vs. GG | 13 | 26 | 41 | 82 | 0.095 | 0.023-0.399 | 0.001 | 12.980 | |
| TT vs. GT | 27 | 54 | 6 | 12 | 14.192 | 4.808-41.895 | 0.001 | 27.500 | |
|
| |||||||||
| ABCB1 C3435T | CC vs. CT+TT | 11 | 22 | 24 | 48 | 0.306 | 0.128-0.729 | 0.008 | 7.430 |
| CT vs. CC+TT | 9 | 18 | 20 | 40 | 0.329 | 0.132-0.824 | 0.018 | 5.880 | |
| TT vs. CC+CT | 30 | 60 | 6 | 12 | 11 | 3.952-30.614 | ≤0.001 | 25 | |
| TT vs. CC | 30 | 60 | 6 | 12 | 10.909 | 3.523-33.782 | ≤0.001 | 19.590 | |
| CT vs. CC | 9 | 18 | 20 | 40 | 0.982 | 0.339-2.840 | 0.973 | 0 | |
| TT vs. CT | 30 | 60 | 6 | 12 | 11.111 | 3.422-36.081 | ≤0.001 | 18.300 | |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 5.
Distribution of ABCB1 allele frequencies in drug-responsive and drug-resistant patients.
| SNP | ABCB1 allele | Drug-resistant patients (N = 50) (%) | Drug-responsive patients (N = 50) (%) | ORs | 95% CI | p value | X 2 |
|---|---|---|---|---|---|---|---|
| ABCB1 C1236T | C | 30 | 61 | 0.274 | 0.152-0.493 | ≤0.001 | 19.380 |
| T | 70 | 39 | 3.650 | 2.029-6.563 | ≤0.001 | ||
|
| |||||||
| ABCB1 G2677T | G | 33 | 47 | 0.555 | 0.313-0.985 | 0.044 | 4.080 |
| T | 67 | 53 | 1.801 | 1.016-3.192 | 0.044 | ||
|
| |||||||
| ABCB1 C3435T | C | 31 | 68 | 0.211 | 0.116-0.384 | ≤0.001 | 27.380 |
| T | 69 | 32 | 4.730 | 2.604-8.591 | ≤0.001 | ||
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
3.2.2. Haplotypic Analysis
The obtained results showed a significant degree of LD between C1236T and G2677T (∣D′∣ = 0.211), G2677T and C3435T (∣D′∣ = 0.035), and C1236T and C3435T (∣D′∣ = 0.236). In fact, the r2 coefficient between C1236T and G2677T, G2677T and C3435T, and C1236T and C3435T were 0.033, 0.001, and 0.039, respectively.
The ORs of CT and TT haplotypes (C1236T and G2677T); GT, TC, and TT haplotypes (G2677T and C3435T); and CT and TT haplotypes (C1236T and C3435T) were significantly higher in nonresponder patients than in responder patients: 3.500, 1.152-10.633, p = 0.027 and 19.056, 2.395-151.604, p = 0.005; 3.778, 1.343-10.628, p = 0.012, 2.852, 0.995-8.174, p = 0.051, and 36.360, 2.095-631.209, p = 0.014; 4.929, 1.503-16.158, p = 0.009 and 10.286, 2.209-47.902, p = 0.003. The more significant OR was observed in TT haplotype for the 3 combinations of SNPs.
Compared to CGC haplotype, ORs of the association between CTT, TGT, TTC, and TTT haplotypes and drug refractory were 17.414, 0.967-313.749, p = 0.053; 5.268, 1.077-25.780, p = 0.040; 9.333, 1.121-77.707, p = 0.039; 18.910, 1.061-337.144, p = 0.046, respectively. The most significant effect was noted in TTT haplotype. The distribution of all ABCB1 haplotypes is represented in Tables 6–9.
Table 6.
Haplotype frequencies of the ABCB1 C1236T and G2677T polymorphisms in drug-responsive and drug-resistant patients.
| ABCB1 C1236T-G2677T haplotype | Drug-resistant patients (N = 50) | Drug-responsive patients (N = 50) | ORs | 95% CI | p value | X 2 | ||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| CG | 10 | 20 | 39 | 78 | 0.071 | 0.027-0.185 | ≤0.001 | 33.650 |
| CT | 14 | 28 | 5 | 10 | 3.500 | 1.152-10.633 | 0.027 | 5.260 |
| TG | 12 | 24 | 5 | 10 | 2.842 | 0.919-8.791 | 0.070 | 3.470 |
| TT | 14 | 28 | 1 | 2 | 19.056 | 2.395-151.604 | 0.005 | 10.700 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 7.
Haplotype frequencies of the ABCB1 G2677T and C3435T polymorphisms in drug-responsive and drug-resistant patients.
| ABCB1 G2677T-C3435T haplotype | Drug-resistant patients (N = 50) | Drug-responsive patients (N = 50) | ORs | 95% CI | p value | X 2 | ||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| GC | 6 | 12 | 38 | 76 | 0.043 | 0.015-0.126 | ≤0.001 | 41.560 |
| GT | 17 | 34 | 6 | 12 | 3.779 | 1.343-10.628 | 0.019 | 6.830 |
| TC | 14 | 28 | 6 | 12 | 2.852 | 0.995-8.174 | 0.051 | 4 |
| TT | 13 | 26 | 0 | 0 | 36.360 | 2.095-631.209 | 0.014 | 14.940 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 8.
Haplotype frequencies of the ABCB1 C1236T and C3435T polymorphisms in drug-responsive and drug-resistant patients.
| ABCB1 C1236T-C3435T haplotype | Drug-resistant patients (N = 50) | Drug-responsive patients (N = 50) | ORs | 95% CI | p value | X 2 | ||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| CC | 9 | 18 | 40 | 80 | 0.055 | 0.020-0.149 | ≤0.001 | 38.460 |
| CT | 15 | 30 | 4 | 8 | 4.929 | 1.503-16.158 | 0.009 | 7.860 |
| TC | 11 | 22 | 4 | 8 | 3.244 | 0.956-11.001 | 0.059 | 3.840 |
| TT | 15 | 30 | 2 | 4 | 10.286 | 2.209-47.902 | 0.003 | 11.980 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 9.
Haplotype frequencies of the ABCB1 C1236T, G2677T, and C3435T polymorphisms in drug-responsive and drug-resistant patients.
| ABCB1 C1236T-G2677T-C3435T haplotype | Drug-resistant patients (N = 50) | Drug-responsive patients (N = 50) | ORs | 95% CI | p value | X 2 | ||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| CGC | 3 | 6 | 35 | 70 | 0.027 | 0.0073-0.1019 | ≤0.001 | 43.460 |
| TTC | 8 | 16 | 1 | 2 | 9.333 | 1.1210-77.7072 | 0.039 | 5.980 |
| TGC | 1 | 2 | 3 | 6 | 0.320 | 0.0321-3.1837 | 0.331 | 1.040 |
| CTT | 7 | 14 | 0 | 0 | 17.414 | 0.9665-313.7492 | 0.053 | 7.530 |
| CGT | 8 | 16 | 4 | 8 | 2.191 | 0.6145-7.8082 | 0.227 | 1.520 |
| TTT | 8 | 16 | 0 | 0 | 18.910 | 1.0607-337.1442 | 0.046 | 8.700 |
| CTC | 6 | 12 | 5 | 10 | 1.227 | 0.3490-4.3158 | 0.750 | 0.100 |
| TGT | 9 | 18 | 2 | 4 | 5.268 | 1.0766-25.7798 | 0.040 | 5.010 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
3.3. Polymorphisms and Patient Data Correlation
We further correlated separately each collected data factor with each genotype, allele, and haplotypes for the studied SNPs (all significant associations are shown in Tables 10–15).
Table 10.
Association of ABCB1 polymorphisms and drug resistance in male and female epileptic subgroups.
| Male | Drug-resistant patients (N = 28) | Drug-responsive patients (N = 28) | ORs | 95% CI | p value | X 2 | |||
| n | % | n | % | ||||||
| ABCB1 C1236T genotypes | TT vs. CC+CT | 16 | 57.143 | 3 | 10.714 | 11.111 | 2.707-45.613 | 0.001 | 13.460 |
| TT vs. CC | 16 | 84.211 | 3 | 25 | 16.000 | 2.654-96.472 | 0.003 | 10.870 | |
| TT vs. CT | 16 | 64 | 3 | 15.789 | 9.482 | 2.160-41.612 | 0.003 | 10.230 | |
| ABCB1 G2677T genotypes | TT vs. GG+GT | 15 | 53.571 | 4 | 14.286 | 6.923 | 1.900-25.228 | 0.003 | 9.640 |
| ABCB1 C3435T genotypes | TT vs. CC+CT | 18 | 64.286 | 4 | 14.286 | 10.800 | 2.912-40.057 | ≤0.001 | 14.670 |
| TT vs. CC | 18 | 78.261 | 4 | 22.222 | 12.600 | 2.843-55.841 | 0.001 | 12.750 | |
| ABCB1 C1236T alleles | T vs. C | 41 | 73.214 | 22 | 39.286 | 4.224 | 1.901-9.386 | ≤0.001 | 13.100 |
| ABCB1 C3435T alleles | T vs. C | 41 | 73.214 | 18 | 32.143 | 5.770 | 2.554-13.037 | ≤0.001 | 18.950 |
| ABCB1 G2677T-C3435T | TT | 7 | 25 | 0 | 0 | 19.884 | 1.076-367.565 | 0.045 | 8 |
|
| |||||||||
| Female | Drug-resistant patients (N = 22) | Drug-responsive patients (N = 22) | ORs | 95% CI | p value | X 2 | |||
| n | % | n | % | ||||||
| ABCB1 G2677T genotypes | TT vs. GT | 12 | 75 | 2 | 9.524 | 28.500 | 4.504-180.326 | ≤0.001 | 16.550 |
| ABCB1 C3435T genotypes | TT vs. CT | 12 | 75 | 2 | 16.667 | 15.000 | 2.258-99.643 | 0.005 | 9.330 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 11.
Association of ABCB1 polymorphisms and drug resistance in generalized and focal epileptic subgroups.
| Generalized | Drug-resistant patients (N = 42) | Drug-responsive patients (N = 33) | ORs | 95% CI | p value | X 2 | |||
| n | % | n | % | ||||||
| ABCB1 C1236T genotypes | TT vs. CC+CT | 23 | 54.762 | 2 | 6.061 | 18.763 | 3.968-88.729 | ≤0.001 | 19.720 |
| TT vs. CC | 23 | 82.143 | 2 | 14.286 | 27.600 | 4.644-164.027 | ≤0.001 | 17.840 | |
| ABCB1 G2677T genotypes | TT vs. GG+GT | 24 | 57.143 | 4 | 12.121 | 7.250 | 2.209-23.800 | 0.001 | 12.410 |
| TT vs. GT | 24 | 68.571 | 4 | 12.903 | 14.727 | 4.137-52.423 | ≤0.001 | 20.860 | |
| ABCB1 C3435T genotypes | TT vs. CC+CT | 26 | 61.905 | 3 | 9.091 | 16.250 | 4.254-62.079 | ≤0.001 | 21.740 |
| TT vs. CC | 26 | 72.222 | 3 | 16.667 | 13.000 | 3.086-54.773 | 0.001 | 14.900 | |
| TT vs. CT | 26 | 81.250 | 3 | 16.667 | 21.667 | 4.717-99.530 | ≤0.001 | 19.720 | |
| ABCB1 C1236T alleles | TT vs. CT | 23 | 61.162 | 2 | 9.524 | 15.607 | 3.147-77.409 | 0.001 | 15.140 |
| T vs. C | 60 | 71.429 | 23 | 34.848 | 4.674 | 2.337-9.348 | ≤0.001 | 20.010 | |
| ABCB1 G2677T alleles | T vs. G | 59 | 70.238 | 35 | 53.030 | 2.090 | 1.067-4.096 | 0.032 | 4.680 |
| ABCB1 C1236T-G2677T | TG | 9 | 21.429 | 1 | 3.030 | 8.727 | 1.045-72.888 | 0.045 | 5.410 |
| TT | 14 | 33.333 | 1 | 3.030 | 16.000 | 1.977-129.518 | 0.009 | 10.610 | |
| ABCB1 G2677T-C3435T | GT | 13 | 30.952 | 3 | 9.091 | 4.483 | 1.156-17.382 | 0.030 | 5.260 |
| TT | 12 | 28.571 | 0 | 0 | 27.459 | 1.559-483.811 | 0.024 | 11.220 | |
| ABCB1 C1236T-C3435T | TC | 10 | 23.810 | 2 | 6.061 | 4.844 | 0.981-23.908 | 0.053 | 4.330 |
| TT | 13 | 30.952 | 0 | 0 | 30.661 | 1.746-538.489 | 0.019 | 12.360 | |
|
| |||||||||
| Focal | Drug-resistant patients (N = 3) | Drug-responsive patients (N = 17) | ORs | 95% CI | p value | X 2 | |||
| n | % | n | % | ||||||
| ABCB1 C3435T alleles | T vs. C | 5 | 83.333 | 11 | 32.353 | 10.455 | 1.087-100.599 | 0.042 | 5.520 |
| ABCB1 C1236T-C3435T | CT | 2 | 66.667 | 1 | 5.882 | 32.000 | 1.389-737.501 | 0.030 | 7.390 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 12.
Association of ABCB1 polymorphisms and drug resistance in epileptic syndrome subgroups.
| Presence of syndrome | Drug-resistant patients (N = 19) | Drug-responsive patients (N = 7) | ORs | 95% CI | p value | X 2 | |||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||||
| ABCB1 C1236T genotypes | TT vs. CC+CT | 11 | 57.895 | 0 | 0 | 20.294 | 1.014-406.357 | 0.049 | 7.020 |
| TT vs. CT | 11 | 69.750 | 0 | 0 | 27.182 | 1.286-574.353 | 0.034 | 8.250 | |
| ABCB1 G2677T genotypes | TT vs. GT | 9 | 64.286 | 0 | 0 | 22.455 | 1.051-479.955 | 0.046 | 7.010 |
| ABCB1 C3435T genotypes | TT vs. CT | 11 | 91.667 | 1 | 20 | 44.000 | 2.193-882.709 | 0.013 | 8.730 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 13.
Association of ABCB1 polymorphisms and drug resistance in unknown and genetic epileptic subgroups.
| Genetic | Drug-resistant patients (N = 24) | Drug-responsive patients (N = 7) | ORs | 95% CI | p value | X 2 | |||
| n | % | n | % | ||||||
| ABCB1 C1236T genotypes | TT vs. CC+CT | 14 | 58.333 | 0 | 0 | 20.714 | 1.062-404.123 | 0.046 | 7.450 |
| TT vs. CT | 14 | 70 | 0 | 0 | 24.539 | 1.175-512.647 | 0.039 | 7.950 | |
| ABCB1 G2677T genotypes | TT vs. GT | 12 | 60 | 0 | 0 | 19.118 | 0.947-386.136 | 0.054 | 6.690 |
| ABCB1 C3435T genotypes | TT vs. CC+CT | 16 | 66.667 | 1 | 14.286 | 12.000 | 1.226-117.417 | 0.033 | 6 |
| TT vs. CT | 16 | 100 | 1 | 20 | 99.000 | 3.418-2867.633 | 0.008 | 15.810 | |
| ABCB1 C1236T alleles | T vs. C | 33 | 68.750 | 5 | 35.714 | 3.960 | 1.132-13.850 | 0.031 | 4.990 |
|
| |||||||||
| Unknown | Drug-resistant patients (N = 26) | Drug-responsive patients (N = 31) | ORs | 95% CI | p value | X 2 | |||
| n | % | n | % | ||||||
| ABCB1 G2677T genotypes | GG vs. GT+TT | 6 | 23.077 | 1 | 3.226 | 9.000 | 1.006-80.525 | 0.049 | 5.170 |
| TT vs. GG+GT | 15 | 57.692 | 5 | 16.129 | 7.091 | 2.066-24.344 | 0.002 | 10.730 | |
| ABCB1 C3435T genotypes | TT vs. CC | 14 | 82.353 | 3 | 16.667 | 23.333 | 4.021-135.391 | ≤0.001 | 15.100 |
| ABCB1 C3435T alleles | T vs. C | 37 | 71.154 | 19 | 30.645 | 5.583 | 2.491-12.513 | ≤0.001 | 18.570 |
| ABCB1 C1236T-G2677T | TT | 6 | 23.077 | 1 | 3.226 | 9.000 | 1.006-80.525 | 0.049 | 5.170 |
| ABCB1 G2677T-C3435T | TT | 6 | 23.077 | 0 | 0 | 19.976 | 1.067-374.011 | 0.045 | 8 |
| ABCB1 C1236T-C3435T | CT | 8 | 30.769 | 2 | 6.452 | 6.444 | 1.229-33.805 | 0.028 | 5.780 |
| TT | 6 | 23.077 | 1 | 3.226 | 9.000 | 1.006-80.525 | 0.049 | 5.170 | |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 14.
Association of ABCB1 polymorphisms and drug resistance in medical history subgroups.
| Presence of medical history | Drug-resistant patients (N = 10) | Drug-responsive patients (N = 11) | ORs | 95% CI | p value | X 2 | |||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||||
| ABCB1 C1236T genotypes | TT vs. CC+CT | 6 | 60 | 1 | 9.090 | 15.000 | 1.342-167.645 | 0.028 | 6.110 |
| TT vs. CC | 6 | 100 | 1 | 20 | 39.000 | 1.277-1190.913 | 0.036 | 7.540 | |
| ABCB1 G2677T genotypes | TT vs. GG+GT | 6 | 60 | 1 | 9.090 | 15.000 | 1.342-167.645 | 0.028 | 6.110 |
| TT vs. GT | 6 | 66.667 | 1 | 10 | 18.000 | 1.496-216.630 | 0.023 | 6.540 | |
| ABCB1 C3435T genotypes | TT vs. CC+CT | 6 | 60 | 1 | 9.090 | 15.000 | 1.342-167.645 | 0.028 | 6.110 |
| TT vs. CT | 6 | 85.714 | 1 | 12.5 | 42.000 | 2.136-825.760 | 0.014 | 8.040 | |
| ABCB1 C1236T alleles | T vs. C | 16 | 80 | 8 | 36.364 | 7.000 | 1.729-28.337 | 0.006 | 8.150 |
| ABCB1 C1236T-G2677T | TT | 5 | 50 | 0 | 0 | 23.000 | 1.070-494.601 | 0.045 | 7.220 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
Table 15.
Association of ABCB1 polymorphisms and drug resistance in epileptic patients with AEDs bitherapy subgroups.
| AEDs bitherapy | Drug-resistant patients (N = 8) | Drug-responsive patients (N = 16) | ORs | 95% CI | p value | X 2 | |||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||||
| ABCB1 G2677T genotypes | TT vs. GG+GT | 6 | 75 | 2 | 12.500 | 21.000 | 2.372-185.937 | 0.006 | 9.380 |
| TT vs. GT | 6 | 75 | 2 | 12.500 | 21.000 | 2.372-185.937 | 0.006 | 9.380 | |
| ABCB1 G2677T alleles | T vs. G | 14 | 87.500 | 18 | 56.250 | 5.444 | 1.058-28.011 | 0.043 | 4.690 |
Values (n and %). ORs: odds ratio; 95% CI: confidence interval; significant p value ≤ 0.05; X2: chi-square.
3.3.1. ABCB1 Polymorphisms and Gender
After a gender-based stratification, a significant association between male patients and C1236T, G2677T, and C3435T TT genotypes, C1236T and C3435T T alleles, and TT (G2677T-C3435T) haplotype was observed. We also noted an important association between female patients and G2677T and C3435TTT genotypes (Table 10).
3.3.2. ABCB1 Polymorphisms and Generalized/Focal Epilepsy
The distribution according to the epileptic etiology led to a significant association between generalized seizures and C1236T, G2677T, and C3435T TT genotypes, C1236T and G2677TT alleles, and TG, TT (C1236T-G2677T), GT, TT (G2677T-C3435T), and TC, TT (C1236T-C3435T) and TGT (C1236T-G2677T-C3435T) haplotypes. In contrast, a significant association was obtained between focal seizures and T allele of C3435T and CT (C1236T-C3435T) haplotype (Table 11).
3.3.3. ABCB1 Polymorphisms and Epileptic Syndromes
The C1236T, G2677T, and C3435T TT genotypes were considerably higher in nonresponders with epileptic syndromes vs. responders (Table 12).
3.3.4. ABCB1 Polymorphisms and Unknown/Genetic Epileptic Etiology
Significant associations were noticed between genetic etiology and C1236T, G2677T, and C3435T TT genotypes, C1236T T alleles, and TT (C1236T-G2677T), GT, TT (G2677T-C3435T), and CT, TT (C1236T-C3435T) haplotypes. An association between unknown etiology and G2677T GG, TT genotypes and C3435T T alleles was also observed (Table 13).
3.3.5. ABCB1 Polymorphisms and Medical History
The association analysis of the ABCB1 gene revealed that C1236T, G2677T, and C3435T TT genotypes, C1236T T alleles, and TT (C1236T-G2677T) haplotypes were significantly associated with medical history (Table 14).
3.3.6. ABCB1 Polymorphisms and AED Therapy
We evaluated the association of drug responders and nonresponders with ABCB1 SNPs according to the individual monotherapy, bitherapy, and polytherapy. We only noted a significant association between bitherapy and G2677T TT genotypes and G2677TT alleles (Table 15).
4. Discussion
The response to medications varies greatly from one individual to another [69]. The term “drug resistance” is a commonly encountered complication in clinical practice. The concept of DRE existed since the intake of AEDs and the failure of treatment (persistence of seizures). It was observed that patients became resistant to most or to all broad range AEDs with different mechanisms of action [70]. The reported frequency of nonresponders is approximately 30% [4, 10, 71, 72].
According to the obtained results, males were more likely to develop DRE in our study population. This results is in accordance with other reported studies [73–75].
In accordance with epilepsy type, drug-resistant and drug-responsive patients showed a predominance of generalized seizures (84% vs. 66%), compared to focal (6% vs. 34%) and focal to bilateral tonic-clonic seizures (10% vs. 0%). Some studies provided the same results [74, 76, 77], while many others showed the opposite [32, 73, 75, 78–82] due to some changes recently made in the classifications of epilepsies taken into account the type of onset seizures [32, 56]. Epileptic syndromes represented only 26% of our epileptic patients, in fact that most of our patients with isolated seizures have no EEG results or have an EEG with no specific electroclinical syndrome. This result is similar to another study from the center of Tunisia (18.3%) [32]. The etiology remained unknown in 57% of our cases, in drug-resistant patients and drug-responsive ones (52% and 62%). The same result was observed in the study of Banerjee et al. [74].
Medical history was heterogeneous (not only epileptic seizures but other different types of medical histories) and low for epileptic patients and the 2 other groups. It was also observed that the epilepsy drug resistance was frequent in patients treated with more than two AED molecules (84%), while drug-responsive patients responded more to monotherapy treatment (68%). Ajmi et al. [32] have shown the same results as ours except for the result of the polytherapy because they enrolled in their study only patients treated with first-generation AEDs.
As it was previously indicated, the development of DRE depends on several factors [70] such as the genetic differences between individuals. In previous works, the polymorphisms of the ABCB1 gene, encoding P-gp, were extensively examined in patients with DRE but with conflicting results.
In the present study, we noted a significant association of ABCB1 C3435T polymorphism with drug resistance in epilepsy. In fact, epileptic seizure recurrence was higher in nonresponders with TT genotype and T allele in comparison with responders.
These findings corroborate those obtained by some studies showing that TT genotype [21, 29, 40, 41] and T allele [71, 72] play an important role in seizure recurrence in drug-resistant patients compared to drug-responsive patients. However, Siddiqui et al. [37] were the first to investigate the association between C3435T polymorphism and refractory epilepsy in 315 Caucasians. They reported that DRE might be genetically determined. In fact, they proved that patients with drug-resistant epilepsy are more likely to have the CC genotype than the TT genotype (OR = 2.66; 95% CI (1.32-5.38), p = 0.006). The same results were mentioned in other studies demonstrating a higher percentage of C3435T CC genotype [33, 83] and C allele [84] carriers in nonresponders to AEDs. The study of Ajmi et al. [32] from the center of Tunisia found a significant association between CT, TT genotypes, and DRE. On the other hand, several works and meta-analyses could not establish an association between C3435T polymorphism and resistant epilepsy [30, 31, 40, 45, 49, 71, 85, 86].
The P-gp is mainly found at BBB and in various normal tissues with excretory functions. It plays a central role in the transport of the planar lipophilic agents (AEDs), whose majority are ABCB1gene substrates. Considering the presence of some genetic variations in this gene, ABCB1 overexpression may lead to prevent AEDs from attaining the sites of action and to have the therapeutic effect.
Even if the common genetic variant C3435T is a silent polymorphism that does not alter the amino acid sequence of P-gp, it may influence the transport and the distribution of AEDs, reducing the levels of AEDs in the brain and leading to refractory epilepsy.
It was hypothesized that the CC genotype is associated with overexpression of P-gp near the epileptogenic brain foci [37]. This overexpression together with other efflux transporters in the cerebrovascular endothelium may cause DRE [21].
On the other hand, other studies demonstrated that TT genotype is crucial in P-gp activity influencing the oral bioavailability at the BBB, which based on the assumption that patients bearing this genotype could be more resistant to treatment than those bearing CC genotype [37]. Similar results implied that T allele ensures the overexpression of ABCB1 in endothelial cells [54, 70, 87].
Thereby, the presence of C3435T SNP may lead to a high P-gp expression in endothelium tissues and in neurons of epileptic patients [18], resulting in pharmacoresistant epilepsy which can be treated by surgery [21, 88]. However, other studies failed to confirm that C3435T SNP is associated to altered P-gp molecular expression and functional activity [32].
The C1236T polymorphism seems likewise to influence the response to AEDs. In fact, we found a significant association between the C1236T TT genotype or T allele and the resistance to AEDs. Contrariwise, the results in the study of Siddiqui et al. [37] showed that the proportion of CC genotype in nonresponders was significantly higher than that in responders (27.5 and 15.7%, respectively), but the proportion of TT genotype was significantly lower in nonresponders than that in responders (19.5 and 29.6%, respectively).
Li et al. [89] failed to find any association in 6324 drug-responsive vs. 6083 drug-resistant patients. The same results were published by Ajmi et al. [32]. As a silent C1236T SNP, no report has until now investigated its possible effect on P-gb activity [32].
A number of studies showed the relation between the variation of the ABCB1 gene expression and/or the P-gp activities and ABCB1 G2677T (Ala893Thr) SNP [18, 21, 27]. Our results demonstrated that the drug-resistant patients are more likely to have the TT genotype than the GG genotype. These findings confirm those presented in the study of Seo et al. [29] showing that the risk of drug resistance was more significant in Japanese patients with the TT genotype than those with the GG genotype. In the study of Ajmi et al. [32], the GT and TT genotypes were present in patients with DRE. However, these results contrast with those obtained in other works. For instance, Sánchez et al. [90] found that the distribution of the GG genotype was more higher in the Caucasian adults drug-resistant than drug-responsive.
In the meta-analysis of Li et al. [89], no association was observed in Asians and Caucasians. Overall, serine/alanine amino acid of the coding polymorphism increases P-gp activity, even so other studies failed to demonstrate this effect on P-gp intracellular location, expression level, and function [32].
The discordant results of all these studies could be explained by [91, 92]:
The small sizes of the studied populations [63]
The heterogeneity in selection criteria for study populations (different used study designs and subject definitions, recurrent epileptic seizures, variation in duration which precedes the identification of drug resistance...) [63]
The variable methodologies applied for phenotyping and genotyping [63]
The association between ABCB1 C3435T polymorphism and AEDs might be not real [93, 94]
The different ethnicities of patients may be correlated to the modification the P-gp expression. Ajmi et al. [32] reported that the level of expression of the T allele of the most studied SNP ABCB1 C3435T in DRE varied from one ethnic group to another. Moreover, its lowest frequencies were found in Tunisian (0.2) and Egyptian (0.3) [95] populations compared to the other ethnicities (Chinese and Iranian)
The heterogeneity of epilepsy including multiple syndromes with various etiologies [40, 95, 96]
The different other actors, such as age, various epileptic etiologies, and variability in drug response to a large AEDs number, should be taken into account
Indeed, Sánchez et al. [90] found a lower risk associated with ABCB1 3435TT or 2677TT genotypes in the subgroup of patients (>12 years). Nevertheless, drug-resistant and drug-responsive groups had different origins of epilepsy and treatments [93, 94]. The most used AEDs were P-gp substrates (phenytoin and phenobarbital) in adults with symptomatic epilepsy (Engel classification). On the other hand, the most employed AED in the patients (<12 years) with idiopathic epilepsy was a nonsubstrate P-gp (VPA) due to the fact that CBZ and VPA have not been yet reported to be a drug substrates of P-gp [97].
Thus, it becomes necessary to confirm the association between ABCB1 polymorphisms and the levels of P-gp expression and activity in brain tissue in patients with refractory epilepsy before admitting the role of SNPs in resistance to MAEs [98]. So far, no conclusive evidence of C3435T-dependent P-gp expression at the BBB level has substantiated the relationship between ABCB1 polymorphisms and the expression levels of ABCB1 brain mRNA or P-gp proteins in refractory epilepsy [6, 98–100].
Haplotypic analysis indicated that CT and TT haplotypes (C1236T and G2677T) were significantly higher in patients with DRE. The GT, TC, and TT haplotypes (G2677T and C3435T) increased considerably the risk of drug-resistant epilepsy. Only the TT haplotype was shown in 3 other studies [30, 32, 39]. Nevertheless, no association was observed in other population [101]. The patients with DRE were more likely to have CT and TT haplotypes (C1236T and C3435T), compared to drug-responsive patients.
A significant level LD was observed between the C1236T, G2677T, and C3435T SNPs, indicating that these loci reacted as a complex haplotypic system. The haplotype combination CTT, TGT, TTC, and TTT was significantly associated with poor response, while the haplotype combination of CGC was related to good drug response. However, Siddiqui et al. [37] as well as Zimprich et al. [27] showed that the resistance to AEDs therapy was significantly influenced by the presence of the CGC haplotype in Caucasians.
The haplotypic analysis, in another study, [28] demonstrated that Asians with the CGC, TGC, and TTT haplotypes were more likely to be drug resistant. Other studies failed to report any significant association between haplotypes and DRE [29, 30, 102]. As an example, a meta-analysis for haplotype that included a total of 26 publications (n = 7,831 patients) did not reveal any significant associations between polymorphisms and their haplotypes and the response to AEDs whether in the general population or in ethnic subgroups. In addition, the data available in this meta-analysis did not allow carrying out subgroup analyses by the used types of AEDs or epilepsy [35].
Some major reported factors, such as the complex haplotype system, the low sample size, the clinical and genetic heterogeneity in epilepsy, and the environment [29, 35], could explain these contradictory results.
Based on our findings, the importance of ABCB1 haplotype system was highlighted. Screening for these SNPs, which are in high LD, could be related to a significant decrease in intracellular substrate concentration leading to the P-gp overactivity in the BBB [89, 103–107] and could be a stronger marker. Therefore, the combinations of bi- and triallelic haplotypes should be studied.
As in the most incidence and prevalence studies of epilepsy, the disease is more frequent in male than in female patients [108–110] due to the fact that the majority of men refuse to marry women with epilepsy, which leads to a strong concealment of the pathology.
Nevertheless, we found significant results in female patients with DRE. Indeed, Sidenvall et al. [111] reported that the incidence of infantile epilepsy was rather raised in girls than in boys.
Another study reported that there is no difference between the two sexes as far as DRE is concerned [112].
We also found an increased frequency of focal epilepsies. The same results were obtained in many other works [32, 78, 79, 81, 82]. We observed a more significant predominance of generalized seizures compared to focal seizures, in our study. Opposite findings were found in others which classified patients based on of the previous classification [74, 76, 77]. It is important to notice that recently some changes were made on the classification of epilepsies which include the beginning of seizures. This update was taken into account for our study.
Epileptic syndromes are determined by clinical context, epileptic symptoms, and EEG abnormalities. We noted a limited frequency of resistant patients with epileptic syndromes (38%) due to the lack of access to the EEG. On the other hand, significant associations were found in genotypes.
Obviously, we found that the unknown etiology was also important, which concords to the study of Banerjee et al. [74], reviewing many studies reporting a preponderance of seizures of unknown cause. In addition, the genetic research has evolved to identify multiple genes and genetic variations in epileptic patients, which in turn has led to very significant results concerning genetic etiology (48%) in our drug-resistant patients.
We also noted a significant association between the DRE and the medical history. Indeed, different medical histories may occur in epileptic patients, which does not necessarily explain the resistance to AEDs. According to Hitiris et al. [113], the risk of developing DRE is more important with stroke history or severe trauma. However, in our study, resistant patients did not have a lesional DRE contrarily to the study of Ajmi et al. [32] where the frequency of structural etiology was more common.
Finally, patients enrolled in our study were resistant to all the different administered AEDs. The stratification by each type of AEDs was useless because it can distort results. Our results showed that only bitherapy seems to be concerned by the association of resistance with genetic biomarkers. The same result was showed in the studies of Ajmi et al. [32] and Kwan and Brodie [114]. They noted that the patients who could be predisposed to refractory epilepsy justify the need of a bitherapy.
5. Conclusion
Epilepsy was intensively studied in a large number of research works that used pharmacogenetics in an attempt to improve the therapeutic response relying on a personalized therapy. We found that ABCB1 polymorphism increases the risk of developing AED resistance. The obtained findings support in part those provided by previous Tunisian study. The screening for the detection of these polymorphisms may be an effective method to a better therapeutic management of the epilepsy by choosing the best treatment option for each patient and predicting the treatment outcome of the newly diagnosed Tunisian patients before the administration of medication. This will, in the long term, reduce the morbidity among them.
Acknowledgments
The authors are grateful to the study participants. They acknowledge the members of Neuropediatric Department at Mongi Ben Hamida National Institute of Neurology.
Data Availability
The data underlying the findings of the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
- 1.Depont C. The potential of pharmacogenetics in the treatment of epilepsy. European Journal of Paediatric Neurology. 2006;10(2):57–65. doi: 10.1016/j.ejpn.2005.11.009. [DOI] [PubMed] [Google Scholar]
- 2.Franco V., Perucca E. The pharmacogenomics of epilepsy. Expert Review of Neurotherapeutics. 2015;15(10):1161–1170. doi: 10.1586/14737175.2015.1083424. [DOI] [PubMed] [Google Scholar]
- 3.Elger C. E., Schmidt D. Modern management of epilepsy: a practical approach. Epilepsy & Behavior. 2008;12(4):501–539. doi: 10.1016/j.yebeh.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 4.Naimo G. D., Guarnaccia M., Sprovieri T., et al. A systems biology approach for personalized medicine in refractory epilepsy. International Journal of Molecular Sciences. 2019;20(15, article E3717):p. 3717. doi: 10.3390/ijms20153717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Thijs R. D., Surges R., O'Brien T. J., Sander J. W. Epilepsy in adults. Lancet. 2019;393(10172):689–701. doi: 10.1016/S0140-6736(18)32596-0. [DOI] [PubMed] [Google Scholar]
- 6.Sills G. J., Mohanraj R., Butler E., et al. Lack of association between the C3435T polymorphism in the human multidrug resistance (MDR1) gene and response to antiepileptic drug treatment. Epilepsia. 2005;46(5):643–647. doi: 10.1111/j.1528-1167.2005.46304.x. [DOI] [PubMed] [Google Scholar]
- 7.Moshe S. L., Perucca E., Ryvlin P., Tomson T. Epilepsy: new advances. The Lancet. 2015;385(9971):884–898. doi: 10.1016/S0140-6736(14)60456-6. [DOI] [PubMed] [Google Scholar]
- 8.Fisher R. S., Acevedo C., Arzimanoglou A., et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482. doi: 10.1111/epi.12550. [DOI] [PubMed] [Google Scholar]
- 9.Chouchi M., Kaabachi W., Klaa H., Tizaoui K., Turki I. B., Hila L. Relationship between ABCB1 3435TT genotype and antiepileptic drugs resistance in epilepsy: updated systematic review and meta-analysis. BMC Neurology. 2017;17(1):p. 32. doi: 10.1186/s12883-017-0801-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leandro K., Bicker J., Alves G., Falcão A., Fortuna A. ABC transporters in drug-resistant epilepsy: mechanisms of upregulation and therapeutic approaches. Pharmacological Research. 2019;144:357–376. doi: 10.1016/j.phrs.2019.04.031. [DOI] [PubMed] [Google Scholar]
- 11.Dallas S., Miller D. S., Bendayan R. Multidrug resistance-associated proteins: expression and function in the central nervous system. Pharmacological Reviews. 2006;58(2):140–161. doi: 10.1124/pr.58.2.3. [DOI] [PubMed] [Google Scholar]
- 12.Marzolini C., Paus E., Buclin T., Kim R. B. Polymorphisms in human MDR1 (P-glycoprotein): recent advances and clinical relevance. Clinical Pharmacology and Therapeutics. 2004;75(1):13–33. doi: 10.1016/j.clpt.2003.09.012. [DOI] [PubMed] [Google Scholar]
- 13.Potschka H., Fedrowitz M., Löscher W. P-glycoprotein and multidrug resistance-associated protein are involved in the regulation of extracellular levels of the major antiepileptic drug carbamazepine in the brain. Neuroreport. 2001;12(16):3557–3560. doi: 10.1097/00001756-200111160-00037. [DOI] [PubMed] [Google Scholar]
- 14.Loscher W., Potschka H. Blood-brain barrier active efflux transporters: ATPbinding cassette gene family. NeuroRx. 2005;2(1):86–98. doi: 10.1602/neurorx.2.1.86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fromm M. F. Importance of P-glycoprotein at blood-tissue barriers. Trends in Pharmacological Sciences. 2004;25(8):423–429. doi: 10.1016/j.tips.2004.06.002. [DOI] [PubMed] [Google Scholar]
- 16.Sarkadi B., Homolya L., Szakács G., Váradi A. Human multidrug resistance ABCB and ABCG transporters: participation in a chemoimmunity defense system. Physiological Reviews. 2006;86(4):1179–1236. doi: 10.1152/physrev.00037.2005. [DOI] [PubMed] [Google Scholar]
- 17.Potschka H., Brodie M. J. Pharmacoresistance. Handbook of Clinical Neurology. 2012;108:741–757. doi: 10.1016/B978-0-444-52899-5.00025-3. [DOI] [PubMed] [Google Scholar]
- 18.Löscher W. Mechanisms of drug resistance. Epileptic Disorders. 2005;7(1):3–9. [PubMed] [Google Scholar]
- 19.Tishler D. M., Weinberg K. I., Hinton D. R., Barbaro N., Annett G. M., Raffel C. MDR1 gene expression in brain of patients with medically intractable epilepsy. Epilepsia. 1995;36(1):1–6. doi: 10.1111/j.1528-1157.1995.tb01657.x. [DOI] [PubMed] [Google Scholar]
- 20.Beck H. Plasticity of antiepileptic drug targets. Epilepsia. 2007;48(s1):14–18. doi: 10.1111/j.1528-1167.2007.00994.x. [DOI] [PubMed] [Google Scholar]
- 21.Kwan P., Brodie M. J. Potential role of drug transporters in the pathogenesis of medically intractable epilepsy. Epilepsia. 2005;46(2):224–235. doi: 10.1111/j.0013-9580.2005.31904.x. [DOI] [PubMed] [Google Scholar]
- 22.Remy S., Beck H. Molecular and cellular mechanisms of pharmacoresistance in epilepsy. Brain. 2006;129(1):18–35. doi: 10.1093/brain/awh682. [DOI] [PubMed] [Google Scholar]
- 23.Maleki M., Sayyah M., Kamgarpour F., et al. Association between ABCB1-T1236C polymorphism and drug-resistant epilepsy in Iranian female patients. Iranian Biomedical Journal. 2010;14(3):89–96. [PMC free article] [PubMed] [Google Scholar]
- 24.Loscher W., DelantyN MDR1/ABCB1polymorphisms and multidrug resistance in epilepsy: in and out of fashion. Pharmacogenomics. 2009;10(5):711–713. doi: 10.2217/pgs.09.47. [DOI] [PubMed] [Google Scholar]
- 25.Tate S. K., Sisodiya S. M. Multidrug resistance in epilepsy: a pharmacogenomic update. Expert Opinion on Pharmacotherapy. 2007;8(10):1441–1449. doi: 10.1517/14656566.8.10.1441. [DOI] [PubMed] [Google Scholar]
- 26.Marchi N., Hallene K. L., Kight K. M., et al. Significance of MDR1 and multiple drug resistance in refractory human epileptic brain. BMC Medicine. 2004;2(1):37–47. doi: 10.1186/1741-7015-2-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zimprich F., Sunder-Plassmann R., Stogmann E., et al. Association of an ABCB1 gene haplotype with pharmacoresistance in temporal lobe epilepsy. Neurology. 2004;63(6):1087–1089. doi: 10.1212/01.wnl.0000141021.42763.f6. [DOI] [PubMed] [Google Scholar]
- 28.Hung C. C., Tai J. J., Lin C. J., Lee M. J., Liou H. H. Complex haplotypic effects of the ABCB1 gene on epilepsy treatment response. Pharmacogenomics. 2005;6(4):411–417. doi: 10.1517/14622416.6.4.411. [DOI] [PubMed] [Google Scholar]
- 29.Seo T., Ishitsu T., Ueda N., et al. ABCB1 polymorphisms influence the response to antiepileptic drugs in Japanese epilepsy patients. Pharmacogenomics. 2006;7(4):551–561. doi: 10.2217/14622416.7.4.551. [DOI] [PubMed] [Google Scholar]
- 30.Kim Y. O., Kim M. K., Woo Y. J., et al. Single nucleotide polymorphisms in the multidrug resistance 1 gene in Korean epileptics. Seizure. 2006;15(1):67–72. doi: 10.1016/j.seizure.2005.11.001. [DOI] [PubMed] [Google Scholar]
- 31.Lakhan R., Misra U. K., Kalita J., et al. No association of ABCB1 polymorphisms with drug-refractory epilepsy in a north Indian population. Epilepsy & Behavior. 2009;14(1):78–82. doi: 10.1016/j.yebeh.2008.08.019. [DOI] [PubMed] [Google Scholar]
- 32.Ajmi M., Boujaafar S., Zouari N., et al. Association between ABCB1 polymorphisms and response to first-generation antiepileptic drugs in a Tunisian epileptic population. The International Journal of Neuroscience. 2018;128(8):705–714. doi: 10.1080/00207454.2017.1412964. [DOI] [PubMed] [Google Scholar]
- 33.Hoffmeyer S., Burk O., Von Richter O., et al. Functional polymorphisms of the human multidrug-resistance gene: multiple sequence variations and correlation of one allele with P-glycoprotein expression and activity in vivo. Proceedings of the National Academy of Sciences. 2000;97(7):3473–3478. doi: 10.1073/pnas.97.7.3473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Löscher W., Klotz U., Zimprich F., Schmidt D. The clinical impact of pharmacogenetics on the treatment of epilepsy. Epilepsia. 2009;50(1):1–23. doi: 10.1111/j.1528-1167.2008.01716.x. [DOI] [PubMed] [Google Scholar]
- 35.Haerian B. S., Lim K. S., Tan C. T., Raymond A. A., Mohamed Z. Association of ABCB1 gene polymorphisms and their haplotypes with response to antiepileptic drugs: a systematic review and metaanalysis. Pharmacogenomics. 2011;12(5):713–725. doi: 10.2217/pgs.10.212. [DOI] [PubMed] [Google Scholar]
- 36.Wei-Ping L., Han R.-F., Shu Z.-R. Associations between the C3435T polymorphism of the ABCB1 gene and drug resistance in epilepsy: a meta-analysis. International Journal of Clinical and Experimental Medicineis. 2014;7(11):3924–3932. [PMC free article] [PubMed] [Google Scholar]
- 37.Siddiqui A., Kerb R., Weale M. E., et al. Association of multidrug resistance in epilepsy with a polymorphism in the drug-transporter gene ABCB1. The New England Journal of Medicine. 2003;348(15):1442–1448. doi: 10.1056/NEJMoa021986. [DOI] [PubMed] [Google Scholar]
- 38.Schmidt D., Loscher W. Drug resistance in epilepsy: putative neurobiologic and clinical mechanisms. Epilepsia. 2005;46(6):858–877. doi: 10.1111/j.1528-1167.2005.54904.x. [DOI] [PubMed] [Google Scholar]
- 39.Hung C. C., Jen Tai J., Kao P. J., Lin M. S., Liou H. H. Association of polymorphisms in NR1I2 and ABCB1 genes with epilepsy treatment responses. Pharmacogenomics. 2007;8(9):1151–1158. doi: 10.2217/14622416.8.9.1151. [DOI] [PubMed] [Google Scholar]
- 40.Tan N. C., Heron S. E., Scheffer I. E., et al. Failure to confirm association of a polymorphism in ABCB1 with multidrug-resistant epilepsy. Neurology. 2004;63(6):1090–1092. doi: 10.1212/01.wnl.0000137051.33486.c7. [DOI] [PubMed] [Google Scholar]
- 41.Kwan P., Baum L., Wong V., et al. Association between ABCB1 C3435T polymorphism and drug-resistant epilepsy in Han Chinese. Epilepsy & Behavior. 2007;11(1):112–117. doi: 10.1016/j.yebeh.2007.04.013. [DOI] [PubMed] [Google Scholar]
- 42.Shaheen U., Prasad D. K., Sharma V., et al. Significance of MDR1 gene polymorphism C3435T in predicting drug response in epilepsy. Epilepsy Research. 2014;108(2):251–256. doi: 10.1016/j.eplepsyres.2013.11.009. [DOI] [PubMed] [Google Scholar]
- 43.Manna I., Gambardella A., Labate A., et al. Polymorphism of the multidrug resistance 1 gene MDR1/ABCB1 C3435T and response to antiepileptic drug treatment in temporal lobe epilepsy. Seizure. 2015;24:124–126. doi: 10.1016/j.seizure.2014.09.010. [DOI] [PubMed] [Google Scholar]
- 44.Chen L., Liu C. Q., Hu Y., Xiao Z. T., Chen Y., Liao J. X. Association of a polymorphism in MDR1 C3435T with response to antiepileptic drug treatment in ethic Han Chinese children with epilepsy. Zhongguo Dang Dai Er Ke Za Zhi. 2007;9(1):11–14. [PubMed] [Google Scholar]
- 45.Grover S., Bala K., Sharma S., et al. Absence of a general association between ABCB1 genetic variants and response to antiepileptic drugs in epilepsy patients. Biochimie. 2010;92(9):1207–1212. doi: 10.1016/j.biochi.2010.04.008. [DOI] [PubMed] [Google Scholar]
- 46.Ozgon G. O., Bebek N., Gul G., Cine N. Association of MDR1 (C3435T) polymorphism and resistance to carbamazepine in epileptic patients from Turkey. European Neurology. 2009;59(1-2):67–70. doi: 10.1159/000109264. [DOI] [PubMed] [Google Scholar]
- 47.Ufer M., Mosyagin I., Muhle H., et al. Non-response to antiepileptic pharmacotherapy is associated with the ABCC2 -24C>T polymorphism in young and adult patients with epilepsy. Pharmacogenetics and Genomics. 2009;19(5):353–362. doi: 10.1097/fpc.0b013e328329940b. [DOI] [PubMed] [Google Scholar]
- 48.Bournissen F. G., Moretti M. E., Juurlink D. N., Koren G., Walker M., Finkelstein Y. Polymorphism of the MDR1/ABCB1 C3435T drug-transporter and resistance to anticonvulsant drugs: a meta-analysis. Epilepsia. 2009;50(4):898–903. doi: 10.1111/j.1528-1167.2008.01858.x. [DOI] [PubMed] [Google Scholar]
- 49.Haerian B. S., Roslan H., Raymond A. A., et al. ABCB1 C3435T polymorphism and the risk of resistance to antiepileptic drugs in epilepsy: a systematic review and meta-analysis. Seizure. 2010;19(6):339–346. doi: 10.1016/j.seizure.2010.05.004. [DOI] [PubMed] [Google Scholar]
- 50.Nurmohamed L., Garcia-Bournissen F., Buono R. J., Shannon M. W., Finkelstein Y. Predisposition to epilepsy—does the ABCB1 gene play a role? Epilepsia. 2010;51(9):1882–1885. doi: 10.1111/j.1528-1167.2010.02588.x. [DOI] [PubMed] [Google Scholar]
- 51.Li S. X., Liu Y. Y., Wang Q. B. ABCB1 gene C3435T polymorphism and drug resistance in epilepsy: evidence based on 8,604 subjects. Medical Science Monitor. 2015;21:861–868. doi: 10.12659/MSM.894023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Lv W. P., Han R. F., Shu Z. R. Associations between the C3435T polymorphism of the ABCB1 gene and drug resistance in epilepsy: a meta-analysis. International Journal of Clinical and Experimental Medicine. 2014;7(11):3924–3932. [PMC free article] [PubMed] [Google Scholar]
- 53.Nakamura T., Sakaeda T., Horinouchi M., et al. Effect of the mutation (C3435T) at exon 26 of the MDR1 gene on expression level of MDR1 messenger ribonucleic acid in duodenal enterocytes of healthy Japanese subjects. Clinical Pharmacology and Therapeutics. 2002;71(4):297–303. doi: 10.1067/mcp.2002.122055. [DOI] [PubMed] [Google Scholar]
- 54.Sakaeda T., Nakamura T., Horinouchi M., et al. MDR1 genotype-related pharmacokinetics of digoxin after single oral administration in healthy Japanese subjects. Pharmaceutical Research. 2001;18(10):1400–1404. doi: 10.1023/a:1012244520615. [DOI] [PubMed] [Google Scholar]
- 55.General Assembly of the World Medical, A. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. The Journal of the American College of Dentists. 2014;81:14–18. [PubMed] [Google Scholar]
- 56.Fisher R. S., Cross J. H., French J. A., et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58(4):522–530. doi: 10.1111/epi.13670. [DOI] [PubMed] [Google Scholar]
- 57.Scheffer I. E., Berkovic S., Capovilla G., et al. ILAE classification of the epilepsies: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58(4):512–521. doi: 10.1111/epi.13709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Kwan P., Arzimanoglou A., Berg A. T., et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51(6):1069–1077. doi: 10.1111/j.1528-1167.2009.02397.x. [DOI] [PubMed] [Google Scholar]
- 59.Ma C. L., Wu X. Y., Zheng J., Wu Z. Y., Hong Z., Zhong M. K. Association of SCN1A, SCN2A and ABCC2 gene polymorphisms with the response to antiepileptic drugs in Chinese Han patients with epilepsy. Pharmacogenomics. 2014;15(10):1323–1336. doi: 10.2217/pgs.14.89. [DOI] [PubMed] [Google Scholar]
- 60.Grover S., Talwar P., Gourie-Devi M., et al. Genetic polymorphisms in sex hormone metabolizing genes and drug response in women with epilepsy. Pharmacogenomics. 2010;11(11):1525–1534. doi: 10.2217/pgs.10.120. [DOI] [PubMed] [Google Scholar]
- 61.Wang P., Zhou Q., Sheng Y., Tang B., Liu Z., Zhou B. Association between two functional SNPs of SCN1A gene and efficacy of carbamazepine monotherapy for focal seizures in Chinese Han epileptic patients. Zhong Nan Da Xue Xue Bao. Yi Xue Ban. 2014;39(5):433–441. doi: 10.3969/j.issn.1672-7347.2014.05.001. [DOI] [PubMed] [Google Scholar]
- 62.Subenthiran S., Abdullah N. R., Joseph J. P., et al. Linkage disequilibrium between polymorphisms of ABCB1 and ABCC2 to predict the treatment outcome of Malaysians with complex partial seizures on treatment with carbamazepine mono-therapy at the Kuala Lumpur Hospital. PLoS One. 2013;8(5, article e64827) doi: 10.1371/journal.pone.0064827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Taur S. R., Kulkarni N. B., Gandhe P. P., et al. Association of polymorphisms of CYP2C9, CYP2C19, and ABCB1, and activity of P-glycoprotein with response to anti-epileptic drugs. Journal of Postgraduate Medicine. 2014;60(3):265–269. doi: 10.4103/0022-3859.138739. [DOI] [PubMed] [Google Scholar]
- 64.Abe T., Seo T., Ishitsu T., Nakagawa T., Hori M., Nakagawa K. Association between SCN1A polymorphism and carbamazepine-resistant epilepsy. British Journal of Clinical Pharmacology. 2008;66(2):304–307. doi: 10.1111/j.1365-2125.2008.03203.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Cascorbi I., Gerloff T., Johne A., et al. Frequency of single nucleotide polymorphisms in the P‐glycoprotein drug transporter MDR1 gene in white subjects. Clinical Pharmacology and Therapeutics. 2001;69(3):169–174. doi: 10.1067/mcp.2001.114164. [DOI] [PubMed] [Google Scholar]
- 66.Andrade C. The P value and statistical significance: Misunderstandings, explanations, challenges, and alternatives. Indian Journal of Psychological Medicine. 2019;41(3):210–215. doi: 10.4103/ijpsym.ijpsym_193_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Nieves E., Jones J. Epi Info™: Now an Open-source application that continues a long and productive "life" through CDC support and funding. Pan Afr Med J. 2009;2:p. 6. [PMC free article] [PubMed] [Google Scholar]
- 68.Shi Y. Y., He L. SHEsis, a powerful software platform for analyses of linkage disequilibrium, haplotype construction, and genetic association at polymorphism loci. Cell Research. 2005;15(2):97–98. doi: 10.1038/sj.cr.7290272. [DOI] [PubMed] [Google Scholar]
- 69.Sharma P., Hussain A., Greenwood R. Precision in pediatric epilepsy. F1000Research. 2019;8 doi: 10.12688/f1000research.16494.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Regesta G., Tanganelli P. Clinical aspects and biological bases of drug-resistant epilepsies. Epilepsy Research. 1999;34(2-3):109–122. doi: 10.1016/s0920-1211(98)00106-5. [DOI] [PubMed] [Google Scholar]
- 71.Vahab S. A., Sen S., Ravindran N., et al. Analysis of genotype and haplotype effects of ABCB1 (MDR1) polymorphisms in the risk of medically refractory epilepsy in an Indian population. Drug Metabolism and Pharmacokinetics. 2009;24(3):255–260. doi: 10.2133/dmpk.24.255. [DOI] [PubMed] [Google Scholar]
- 72.Ponnala S., Chaudhari J. R., Jaleel M. A., et al. Role of MDR1 C3435T and GABRG2 C588T gene polymorphisms in seizure occurrence and MDR1 effect on anti-epileptic drug (phenytoin) absorption. Genetic Testing and Molecular Biomarkers. 2012;16(6):550–557. doi: 10.1089/gtmb.2011.0225. [DOI] [PubMed] [Google Scholar]
- 73.Yu P., Zhou D., Liao W., et al. An investigation of the characteristics of outpatients with epilepsy and antiepileptic drug utilization in a multicenter cross-sectional study in China. Epilepsy & Behavior. 2017;69:126–132. doi: 10.1016/j.yebeh.2016.09.021. [DOI] [PubMed] [Google Scholar]
- 74.Banerjee P. N., Filippi D., Hauser W. A. The descriptive epidemiology of epilepsy—A review. Epilepsy Research. 2009;85(1):31–45. doi: 10.1016/j.eplepsyres.2009.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Forsgren L., Beghi E., Oun A., Sillanpaa M. The epidemiology of epilepsy in Europe–a systematic review. European Journal of Neurology. 2005;12(4):245–253. doi: 10.1111/j.1468-1331.2004.00992.x. [DOI] [PubMed] [Google Scholar]
- 76.Berg A. T., Millichap J. J. The 2010 revised classification of seizures and epilepsy. Continuum: Lifelong Learning in Neurology. 2013;19(3 Epilepsy):571–597. doi: 10.1212/01.con.0000431377.44312.9e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Camfield P. Issues in epilepsy classification for population studies. Epilepsia. 2012;53(s2):10–13. doi: 10.1111/j.1528-1167.2012.03552.x. [DOI] [PubMed] [Google Scholar]
- 78.Giussani G., Canelli V., Bianchi E., et al. A population-based study of active and drug-resistant epilepsies in Northern Italy. Epilepsy & Behavior. 2016;55:30–37. doi: 10.1016/j.yebeh.2015.11.021. [DOI] [PubMed] [Google Scholar]
- 79.Picot M. C., Baldy-Moulinier M., Daurès J. P., Dujols P., Crespel A. The prevalence of epilepsy and pharmacoresistant epilepsy in adults: a population‐based study in a Western European country. Epilepsia. 2008;49(7):1230–1238. doi: 10.1111/j.1528-1167.2008.01579.x. [DOI] [PubMed] [Google Scholar]
- 80.Orozco-Hernández J. P., Quintero-Moreno J. F., Marín-Medina D. S., et al. Perfil clinico y sociodemografico de la epilepsia en adultos de un centro de referencia de Colombia. Neurología (English Edition) 2019;34(7):437–444. doi: 10.1016/j.nrleng.2017.02.012. [DOI] [PubMed] [Google Scholar]
- 81.Fray S., Ben A. N., Kchaou M., Chebbi S., Belal S. Les critères prédictifs d’une épilepsie pharmacorésistante chez l’enfant. Revue Neurologique. 2015;171(10):730–735. doi: 10.1016/j.neurol.2015.06.004. [DOI] [PubMed] [Google Scholar]
- 82.Choi H., Hayat M. J., Zhang R., et al. Drug-resistant epilepsy in adults: outcome trajectories after failure of two medications. Epilepsia. 2016;57(7):1152–1160. doi: 10.1111/epi.13406. [DOI] [PubMed] [Google Scholar]
- 83.Mann M. W., Pons G. Various pharmacogenetic aspects of antiepileptic drug therapy: a review. CNS Drugs. 2007;21(2):143–164. doi: 10.2165/00023210-200721020-00005. [DOI] [PubMed] [Google Scholar]
- 84.Qiang L. U., Liwen W. U., Liri J. I. N. Association analysis of a polymorphism of MDR1 gene and refractory temporal lobe epilepsy in a Chinese population. Neurology Asia. 2007;12(Supplement 1):94–95. [Google Scholar]
- 85.Szoeke C., Sills G. J., Kwan P., et al. Multidrug‐resistant genotype (ABCB1) and seizure recurrence in newly treated epilepsy: data from international pharmacogenetic cohorts. Epilepsia. 2009;50(7):1689–1696. doi: 10.1111/j.1528-1167.2009.02059.x. [DOI] [PubMed] [Google Scholar]
- 86.Leschziner G., Jorgensen A. L., Pirmohamed M., et al. Clinical factors and ABCB1 polymorphisms in prediction of antiepileptic drug response: a prospective cohort study. The Lancet Neurology. 2006;5(8):668–676. doi: 10.1016/S1474-4422(06)70500-2. [DOI] [PubMed] [Google Scholar]
- 87.Sakaeda T., Nakamura T., Okumura K. MDR1 genotype related pharmacokinetics and pharmacodynamics. Biological & Pharmaceutical Bulletin. 2002;25(11):1391–1400. doi: 10.1248/bpb.25.1391. [DOI] [PubMed] [Google Scholar]
- 88.Sisodiya S., Lin W. R., Harding B., Squier M. V., Thom M. Drug resistance in epilepsy: expression of drug resistance proteins in common causes of refractory epilepsy. Brain. 2002;125(1):22–31. doi: 10.1093/brain/awf002. [DOI] [PubMed] [Google Scholar]
- 89.Li H., Wang B., Chang C., Wu M., Xu Y., Jiang Y. The roles of variants in human multidrug resistance (MDR1) gene and their haplotypes on antiepileptic drugs response: a meta-analysis of 57 studies. PLoS One. 2015;10(3, article e0122043) doi: 10.1371/journal.pone.0122043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Sánchez M. B., Herranz J. L., Leno C., et al. Genetic factors associated with drug-resistance of epilepsy: Relevance of stratification by patient age and aetiology of epilepsy. Seizure. 2010;19(2):93–101. doi: 10.1016/j.seizure.2009.12.004. [DOI] [PubMed] [Google Scholar]
- 91.Chhun S. Transport des médicaments antiépileptiques par les transporteurs ABC et implication dans l’épilepsie pharmacorésistante chez l’enfant. La Lettre du Pharmacologue. 2011;25(4):150–156. [Google Scholar]
- 92.Tang F., Hartz A. M. S., Bauer B. Drug-resistant epilepsy: multiple hypotheses, few answers. Frontiers in Neurology. 2017;8:p. 301. doi: 10.3389/fneur.2017.00301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Shahwan A., Murphy K., Doherty C., et al. The controversial association of _ABCB1_ polymorphisms in refractory epilepsy: an analysis of multiple SNPs in an Irish population. Epilepsy Research. 2007;73(2):192–198. doi: 10.1016/j.eplepsyres.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 94.Soranzo N., Goldstein D. B., Sisodiya S. M. The role of common variation in drug transporter genes in refractory epilepsy. Expert Opinion on Pharmacotherapy. 2005;6(8):1305–1312. doi: 10.1517/14656566.6.8.1305. [DOI] [PubMed] [Google Scholar]
- 95.Ebid A.-H. I. M., Ahmed M. M., Mohammed S. A. Therapeutic drug monitoring and clinical outcomes in epileptic Egyptian patients: a gene polymorphism perspective study. Therapeutic Drug Monitoring. 2007;29(3):305–312. doi: 10.1097/FTD.0b013e318067ce90. [DOI] [PubMed] [Google Scholar]
- 96.French J. A. Refractory epilepsy: clinical overview. Epilepsia. 2007;48(s1):3–7. doi: 10.1111/j.1528-1167.2007.00992.x. [DOI] [PubMed] [Google Scholar]
- 97.Xu T., Yu X., Ou S., et al. Risk factors for posttraumatic epilepsy: a systematic review and meta-analysis. Epilepsy & Behavior. 2017;67:1–6. doi: 10.1016/j.yebeh.2016.10.026. [DOI] [PubMed] [Google Scholar]
- 98.Mosyagin I., Runge U., Schroeder H. W., et al. Association of ABCB1 genetic variants 3435C>T and 2677G>T to ABCB1 mRNA and protein expression in brain tissue from refractory epilepsy patients. Epilepsia. 2008;49(9):1555–1561. doi: 10.1111/j.1528-1167.2008.01661.x. [DOI] [PubMed] [Google Scholar]
- 99.Vogelgesang S., Kunert-Keil C., Cascorbi I., et al. Expression of multidrug transporters in dysembryoplastic neuroepithelial tumors causing intractable epilepsy. Clinical Neuropathology. 2004;23(5):223–231. [PubMed] [Google Scholar]
- 100.Kwan P., Wong V., Ng P. W., et al. Gene-wide tagging study of association between ABCB1 polymorphisms and multidrug resistance in epilepsy in Han Chinese. Pharmacogenomics. 2009;10(5):723–732. doi: 10.2217/pgs.09.32. [DOI] [PubMed] [Google Scholar]
- 101.Seven M., Batar B., Unal S., Yesil G., Yuksel A., Guven M. The drug-transporter gene MDR1 C3435T and G2677T/A polymorphisms and the risk of multidrug-resistant epilepsy in Turkish children. Molecular Biology Reports. 2014;41(1):331–336. doi: 10.1007/s11033-013-2866-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Meng H., Guo G., Ren J., Zhou H., Ge Y., Guo Y. Effects of ABCB1 polymorphisms on plasma carbamazepine concentrations and pharmacoresistance in Chinese patients with epilepsy. Epilepsy & Behavior. 2011;21(1):27–30. doi: 10.1016/j.yebeh.2011.02.015. [DOI] [PubMed] [Google Scholar]
- 103.Hitzl M., Schaeffeler E., Hocher B., et al. Variable expression of P-glycoprotein in the human placenta and its association with mutations of the multidrug resistance 1 gene (MDR1, ABCB1) Pharmacogenetics and Genomics. 2004;14(5):309–318. doi: 10.1097/00008571-200405000-00006. [DOI] [PubMed] [Google Scholar]
- 104.Johne A., Köpke K., Gerloff T., et al. Modulation of steady‐state kinetics of digoxin by haplotypes of the P‐glycoprotein MDR1 gene. Clinical Pharmacology and Therapeutics. 2002;72(5):584–594. doi: 10.1067/mcp.2002.129196. [DOI] [PubMed] [Google Scholar]
- 105.Tang K., Ngoi S.-M., Gwee P.-C., et al. Distinct haplotype profiles and strong linkage disequilibrium at the MDR1 multidrug transporter gene locus in three ethnic Asian populations. Pharmacogenetics and Genomics. 2002;12(6):437–450. doi: 10.1097/00008571-200208000-00004. [DOI] [PubMed] [Google Scholar]
- 106.Kroetz D. L., Pauli-Magnus C., Hodges L. M., et al. Sequence diversity and haplotype structure in the human ABCB1 (MDR1, multidrug resistance transporter) gene. Pharmacogenetics and Genomics. 2003;13(8):481–494. doi: 10.1097/00008571-200308000-00006. [DOI] [PubMed] [Google Scholar]
- 107.Tan N. C., Mulley J. C., Berkovic S. F. Genetic association studies in epilepsy: “the truth is out there”. Epilepsia. 2004;45(11):1429–1442. doi: 10.1111/j.0013-9580.2004.22904.x. [DOI] [PubMed] [Google Scholar]
- 108.Joensen P. Prevalence, incidence, and classification of epilepsy in the Faroes. Acta Neurologica Scandinavica. 1986;74(2):150–155. doi: 10.1111/j.1600-0404.1986.tb04642.x. [DOI] [PubMed] [Google Scholar]
- 109.Olafsson E., Hauser W. A., Ludvigsson P., Gudmundsson G. Incidence of epilepsy in rural Iceland: a population‐based study. Epilepsia. 1996;37(10):951–955. doi: 10.1111/j.1528-1157.1996.tb00532.x. [DOI] [PubMed] [Google Scholar]
- 110.Hauser W. A., Annegers J. F., Kurland L. T. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935–1984. Epilepsia. 1993;34(3):453–458. doi: 10.1111/j.1528-1157.1993.tb02586.x. [DOI] [PubMed] [Google Scholar]
- 111.Sidenvall R., Forsgren L., Blomquist H. K., Heijbel J. A community‐based prospective incidence study of epileptic seizures in children. Acta Paediatrica. 1993;82(1):60–65. doi: 10.1111/j.1651-2227.1993.tb12518.x. [DOI] [PubMed] [Google Scholar]
- 112.Forsgren L., Bucht G., Eriksson S., Bergmark L. Incidence and clinical characterization of unprovoked seizures in adults: a prospective population‐based study. Epilepsia. 1996;37(3):224–229. doi: 10.1111/j.1528-1157.1996.tb00017.x. [DOI] [PubMed] [Google Scholar]
- 113.Hitiris N., Mohanraj R., Norrie J., Sills G. J., Brodie M. J. Predictors of pharmacoresistant epilepsy. Epilepsy Research. 2007;75(2-3):192–196. doi: 10.1016/j.eplepsyres.2007.06.003. [DOI] [PubMed] [Google Scholar]
- 114.Kwan P., Brodie M. J. Early identification of refractory epilepsy. The New England Journal of Medicine. 2000;342(5):314–319. doi: 10.1056/NEJM200002033420503. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data underlying the findings of the current study are available from the corresponding author on reasonable request.