

Abstract
E-mental health is an emerging area of research that has the potential to overcome some of the current barriers to progress in working with people at clinical high risk for psychosis (CHR-P). This article provides an overview of how e-mental health could be used in the detection, prediction, and treatment in the CHR-P population. Specifically, we evaluate e-detection, e-prediction, and e-therapeutics for this clinical population. E-mental health holds great promise to improve current management of CHR-P individuals.
Keywords: psychotic disorders, schizophrenia, prognosis, treatment, clinical high risk, digital, e-health, internet, smartphone, mobile phone
Introduction
The identification of people at clinical high risk for psychosis (CHR-P) [1] offers a unique opportunity to alter the illness course of psychotic disorders [2]. These individuals often have several risk factors for psychosis [3] and typically present with attenuated psychotic symptoms in the context of a recent decline in functioning [4]. They display symptoms and functional impairments that are qualitatively similar to those observed in established mental disorders [5]. The risk of transition to psychosis within 2 years in these individuals is approximately 20% [6]. This risk is not the same across the different CHR-P subgroups. In particular, individuals meeting criteria for short-lived psychotic episode show a distinctive and very high risk of developing persistent psychotic disorders that cumulates to about 50% at 2 years [7]. CHR-P individuals presenting with a short-lived psychotic episode that is spontaneously remitting but characterized by disorganized behavior have an even higher risk of developing a persistent psychotic disorder, cumulating at 89% at 5 years [8]. These individuals also have unmet clinical needs not typically addressed by the current configuration of mental health services [9,10]. Overall, the risk for the development of psychosis from a CHR-P stage has declined from 29% [11] to 20% [6] in recent years, although not across all sites [12]. This variable transition risk is due to different sampling strategies being adopted to recruit these individuals [13]. Emerging evidence indicates that the method of recruitment prior to a CHR-P assessment is fundamental in enriching their actual level of risk for psychosis [13].
Although the CHR-P paradigm has been adopted in various countries worldwide [14-17], a number of challenges have arisen, hindering its penetrance into mainstream clinical practice. The real-world success of the CHR-P paradigm rests on three core components: an efficient detection of at risk cases, accurate prediction of their outcomes, and effective preventative treatments to alter the course of these outcomes Figure 1.
Core clinical and research components for effective prevention of psychosis, from Fusar-Poli et al [35].
There are currently barriers to the implementation of each component. First, well-established CHR-P services [17] detect as low as 5% of first episode psychosis (FEP) patients before illness onset [18]. Even within national youth mental health services, the proportion of FEP cases detected at their CHR-P stage is only 12% [19]. Second, although the prognostic performance of the current CHR-P psychometric tools is excellent [20], it is highly dependent on the way CHR-P individuals are recruited [21]. Furthermore, prognostic outcomes in this population are mostly based on group-level predictions, and it is not yet possible to forecast the onset of psychosis at the individual-subject level [22]. This is a substantial limitation given that the CHR-P group is highly heterogenous and includes different subpopulations with differing outcomes [7]. Third, no specific preventive treatment appears to be more effective than others in preventing onset of psychosis [23], treating attenuated positive symptoms [24,25], treating attenuated negative symptoms [26], treating depressive symptoms [27], reducing distress [28], or improving social functioning [29]. Again, the lack of evidence may partially reflect the fact that one-size-fits-all approaches for this population do not work and individualized treatments should be offered instead.
E-Mental health is a new approach that may be uniquely suited to overcome some of these barriers. Individuals at CHR-P have a young age range (most criteria are set at 14 to 35 years) and as such tend to be highly engaged with the digital world [30]. Although previous reviews have highlighted the emerging potential for e-mental health in psychosis [31-34], there is currently no overview focusing on the potential and prospects specifically in CHR-P. In this article, we provide an overview how e-mental health can be applied to the detection, prediction, and treatment of CHR-P. Studies included in this overview are summarized in Table 1. Although this is not a systematic review and there is no assumption that the literature surveyed is comprehensive, we provide our search strategy and inclusion criteria in Multimedia Appendix 1.
Table 1.
Summary of included studies of e-mental health in clinical high risk for psychosis.
| Study and type | Summary | Results | |
| E-Detection | |||
| McDonald et al 2018 [47] | Web-based community screening for CHR-Pa. | Good to moderate sensitivity and specificity for predicting CHR status based on online screening. | |
| Fusar-Poli et al 2017 [18] | Risk calculator based on routine clinical data of patients accessing secondary health services. | Acceptable predictive performance; Harrell C of 0.80 (0.79-0.82). | |
| Fusar-Poli et al 2018 [51] | External validation of the above study in a second NHSb trust. | Acceptable predictive performance; Harrell C of 0.73. | |
| Fusar-Poli et al 2019 [52] | Protocol for implementation study of the above into routine clinical care. | N/A. | |
| Cannon et al 2016 [53] | Risk calculator based on specialized clinical assessment. | Acceptable predictive performance; Harrell C of 0.71. | |
| Carrión et al 2016 [54] | External valiation of the above study in a second cohort. | Good discrimination area under the curve of 0.790 (0.644-0.937). | |
| E-Prognosis | |||
| Palmier-Claus et al 2012 [59] | Feasibility of smartphone self-report of symptoms using the ClinTouch app. | A total of 82% (36/42) of participants were compliant with the smartphone measures. | |
| Klippel et al 2017 [60] | ESMc study of stress and psychotic symptoms using the PsyMate app. | Effects of stress on psychotic experiences were mediated through affective disturbance. | |
| Reininghaus et al 2016 [61] | ESM study of threat perception and psychotic experiences using PsyMate app. | Outsider status and threat anticipation were associated with more intensive psychotic experiences in those who experienced sexual abuse compared with those exposed to low levels of sexual abuse. | |
| Reininghaus et al 2016 [62] | ESM study of sensitivity to outsider status, salient experiences, and psychotic experiences using the PsyMate app. | Elevated stress sensitivity, aberrant salience, and enhanced threat anticipation were associated with increased intensity of psychotic experiences. | |
| van der Steen et al 2017 [63] | ESM study of affective and psychotic experiences in response to stress using a digital wrist watch to instruct participants to enter written self-report at random time points. | Greater associations between negative affect and stress compared with psychotic patients (P=.008) and controls (P<.001). | |
| E-Treatment | |||
| Alvarez-Jimenez et al 2018 [77] | Pilot study of the online social therapy intervention, Momentum. | Of the 70% actively engaged during the study, all reported positive experiences, considered it safe, and would recommend it to others; 93% reported it to be helpful. Large improvements in social functioning (d=1.83, P<.001) and subjective well-being (d=0.75, P=.03). | |
| Rice et al 2018 [84] | Study protocol for enhanced moderated online social therapy (MOST). | N/A. | |
| Loewy et al 2019 [92] | Randomized trial investigating the effectiveness of auditory-processing exercises administered through laptops in CHR-participants compared to the effects of computer games (CG) training. | Targeted cognitive training showed a significant improvement in verbal memory compared to CG participants (effect size = 0.61). Positive and total symptoms improved in both groups over time. | |
| Hooker et al 2014 [93] | Pilot uncontrolled study of online cognitive training. | Significant improvements in processing speed (P=.01, d=0.63) and nonsignificant improvements in visual learning and memory (P=.06, d=0.54) and global cognition (P=.06, d=0.45). | |
| Valmaggia et al 2007 [99] | Study of the feasibility and safety of VRe environments. | No adverse events; no increase in mean anxiety score (P=.29). | |
| Valmaggia et al 2015 [101] | VR study assessing childhood bullying and paranoid ideation in a simulation of the London underground. | More paranoid appraisals of VR simulations compared with controls (P<.001). | |
| Valmaggia et al 2015 [100] | VR study assessing social defeat and paranoid appraisals in a simulation of the London underground. | More paranoid ideation during VR simulation compared with controls χ2(1)=21.06, (P<.001). | |
| Shaikh et al 2016 [102] | VR study assessing ethnic discrimination and persecutory paranoia in a simulation of the London underground. | Higher levels of perceived ethnic discrimination correlated with greater paranoid persecutory ideation in VR environment r=0.25, P=.009. | |
| Geraets et al 2018 [103] | VR study assessing interpersonal distance regulation in a simulated café. | Interpersonal distance increased when social stressors were present in the environment F=3.02, P=.02. | |
| Veling et al 2016 [104] | VR study assessing paranoia in a simulated bar environment. | Increased paranoia compared with controls, regression coefficient 3.80 (95%CI 0.24–7.37) P=.04. | |
aCHR-P: clinical high risk of psychosis.
bNHS: National Health Service.
cESM: experience sampling method.
dVR: virtual reality.
E-Detection
Detecting individuals at risk prior to the onset of psychosis has been a key research priority over the past two decades since the Personal Assessment and Crisis Evaluation study first developed the concept of the CHR-P [16]. Typical inclusion in the CHR-P group is based on attenuated psychotic symptoms, brief episodes of psychosis, or functional deterioration in those with genetic vulnerability for psychosis [35,36]. A distinct approach to the identification of CHR-P individuals is the basic symptom concept proposed by Huber and colleagues [37]. Basic symptoms involve self-experienced perceptual and cognitive anomalies that are thought to represent the earliest manifestation of psychosis risk [38]. More recent studies have shown that the combined presence of both basic symptom and CHR-P criteria increases the predictive power significantly [39]. However, it should also be noted that CHR-P participants who do not make the transition to psychosis are characterized by extensive psychiatric comorbidity and reduced occupational and social functioning [40]. Accordingly, these two domains are also potentially important for targets for e-mental health applications, in terms of both prediction and preventive treatments.
Recruitment strategies have a significant impact on subsequent transition rates of CHR-P cohorts, with self-referrals, assertive community outreach, and population screening associated with lower rates of transition to psychosis [41]. Despite the expansion of CHR-P services, only a small proportion of FEP patients are detected [42]. It is thus a key priority for CHR-P to improve detection of individuals prior to the FEP while not diluting the sample’s baseline risk of psychosis. As the majority of FEP patients actively seek information regarding mental health issues online as their symptoms first develop [43], early identification of CHR-P individuals may be possible through digital detection strategies. These could include online screening as well as use of social media information. Recent evidence, for example, suggests that references to sadness, loneliness, hostility, rumination, and increased self-reference on Facebook predict later onset of depression [44]. A similar approach may be useful in CHR-P as the development of psychosis is characterized by linguistic anomalies that can be detect by automated speech analysis [45,46].
Online screening has the potential to reach a greater number of individuals compared with traditional routes of referral to CHR-P services. McDonald et al [47] used a website for detection of CHR-P in the community. Potential participants were invited via email, flyers, and posters to a website [48] and then asked to complete the 16-item version of the prodromal questionnaire (PQ-16) and 9-item questionnaire of perceptual and cognitive aberrations (PCA) for basic symptoms. This allowed screening of a large number of individuals, 52.3% (1202/2296) of whom met PQ-16 cutoff criteria and 73.6% (1691/2296) of whom met PCA cutoff criteria. Of those meeting screening cutoff criteria who then attended a clinic interview, 31.2% (101/324) met clinical CHR-P criteria. Importantly, a subset of 8 individuals (2.5%) also met criteria for FEP. Receiver operating characteristic curve analysis revealed good to moderate sensitivity and specificity for predicting CHR-P status based on the online results [47]. A machine-learning approach that selected all 25 items from both the PQ-16 and the PCA in addition to demographic variables lead to an improved specificity of 57% while only marginally affecting sensitivity (81%), compared with the original online screening tool.
This study suggests that online screening of community samples for emerging psychosis is possible, potentially identifying a large number of people meeting CHR-P criteria. However, it is currently unclear how many of these participants meeting CHR-P criteria will actually develop psychosis. Accordingly, 2-year transition rates are needed to validate whether the sample detected are truly at risk of developing a psychotic disorder or whether they are false positives. A similar approach to McDonald et al [47] has been implemented using the 32-item self-screen prodrome questionnaire [49], although, again, long-term transition rates are not known. Furthermore, the validity of self-screening questionnaires, particularly when conducted in nonclinical populations, has been questioned [50] due to poor prognostic performance in predicting subsequent psychosis.
More targeted screening of populations accessing secondary mental health services that use electronic health records is also possible through online screening. Our group developed a psychosis risk calculator for patients already accessing secondary mental health services [18]. This tool uses routine clinical data including International Classification of Diseases, Tenth Revision (ICD-10), spectra diagnoses to predict future risk of developing a psychotic disorder and has been externally validated twice in different National Health Service (NHS) Trusts [51] showing an acceptable prognostic performance (Harrell C of 0.73). Patients who have accessed secondary mental health services have a 5-fold increased risk compared with the general population [18], suggesting this may be an efficient way of detecting new cases of psychosis while not diluting the level of risk in the sample. As it uses routine clinical data, the calculator could be used to automatically screen electronic health records for those at increased risk of future psychosis. However, it does rely on the assessment of health professionals to provide ICD-10 diagnoses, and therefore it cannot be used universally for self-screening. The calculator is one of the few eHealth tools in the CHR-P population that is being implemented into clinical routine practice [52].
The North American Prodrome Longitudinal Study has produced an online risk calculator for individuals meeting CHR-P criteria [53]. It showed an overall accuracy of 72% in predicting psychosis when validated in an independent external data set [54]. However, it requires input in the form of a structured interview to confirm CHR-P status and neuropsychological testing, limiting its applicability to wider clinical populations.
E-Mental health offers the opportunity for efficient, scalable screening of those at risk of psychosis across populations that are currently not reached by conventional recruitment, potentially allowing better detection of individuals prior to their FEP. Preliminary evidence suggests that it is indeed feasible. The next step is determining whether these tools can be implemented in practice to identify individuals at increased risk of psychosis while not diluting the overall risk of the sample with false positives.
E-Prognosis
The risk of transition to psychosis from CHR-P is maximal within the first 2 years [55]. This period is therefore a crucial time for predicting onset of psychosis. Traditionally, this has been achieved through regular clinical monitoring from CHR-P services to assess for transition to psychosis, but advances in mobile phone technology offer the opportunity for a far greater temporal resolution in monitoring changes in mental state that may occur on a daily or even momentary basis.
The experience sampling method (ESM) uses mobile phones to measure self-rated changes in mental state on a daily basis [56]. It has excellent ecological validity and allows close monitoring of mental state, particularly in regard to predictors of transition to psychosis. ESM techniques in CHR-P were initially rudimentary, requiring participants to fill out responses in a paper diary when prompted by a wristwatch alarm [57,58]. Palmier et al [59] demonstrated that it is feasible to monitor symptoms through a mobile phone app in a small sample (n=12) of CHR-P individuals, paving the way for further cross-sectional ESM studies. Klippel et al [60] showed in 46 CHR-P individuals that momentary stress increased psychotic experiences via affective disturbance using the PsyMate app. Reininghaus et al [61] used ESM to link threat perception to psychotic experiences in 44 CHR-P individuals and in another study [62] to show an association with sensitivity to outsider status and aberrantly salient experiences with psychotic experiences. Van der Steen et al [63] used ESM to demonstrate an association between affective and psychotic experiences in response to stress in CHR-P individuals, showing an association between stress and psychotic experiences. ESM has shown potential utility in monitoring fine-grained changes in psychopathology during the development of psychosis; however, longitudinal studies are needed to determine its significance for predicting the onset of psychosis. To date, one longitudinal study has been registered: Booij et al [64] plan to predict outcome in various stages of psychosis using mobile phone diary measures of symptoms, stress, emotions, and functioning.
Digital phenotyping, also known as personal sensing, is a novel investigational technique whereby passive measures of mobile phone activity are recorded in real-time [65], which has been postulated to provide a digital phenotype of psychiatric disorders [66]. These measures may include the participant’s interaction with their phone (eg, call logs, number of messages, keyboard use) as well as measures of their activity and movement (eg, through accelerometers or Global Positioning System tracking). Passive data provide a continuous readout every day and require no active role by the participant, thus providing significant advantages over traditional, episodic cross-sectional data. Passive data are also potentially more ecologically valid than symptom ratings elicited by standard questionnaires or interviews, and there is reduced risk of subject attrition.
However, the use of passive mobile phone measures warrants some important ethical considerations [65]. As with any investigation, informed consent, data security, and anonymization are crucial. Additionally, in those with psychotic disorders, care must be taken not to exacerbate paranoia when using participants’ personal devices. Passive measures therefore may be particularly suited to CHR-P individuals, who retain insight, particularly for the prediction of psychosis onset. Unlike ESM, they do not require continual user input and may therefore be less burdensome to participants. A pilot study suggests digital phenotyping could predict relapse in schizophrenia based on anomalies in patient behavior [67]; further studies in CHR-P populations are underway, for example, using the MindStrong app [68].
ESM and digital phenotypes have complementary strengths. ESM provides explicit information about a patient’s state of mind and as such is key to understanding their motivations and behaviors, whereas digital phenotyping has the important advantage of placing minimal burden on the patient apart from keeping their mobile phone charged and as such is ideal for clinical translation. Initial studies suggest that it might be possible to use passive data generated via digital phenotyping as a proxy for active data collected via ESM [69]; in the context of CHR-P, this could enable the background monitoring of risk of transition to psychosis with minimal interference on the day-to-day life of patients.
In addition to informing diagnosis, prognosis, and treatment, e-tools could be used to gain greater understanding of the mechanisms that underlie transition to psychosis. For example, our research team is currently using the Urban Mind app [70] to investigate the impact of the surrounding social and physical environment on risk of transition to psychosis in individuals at CHR-P (see Figure 2 for user interface).
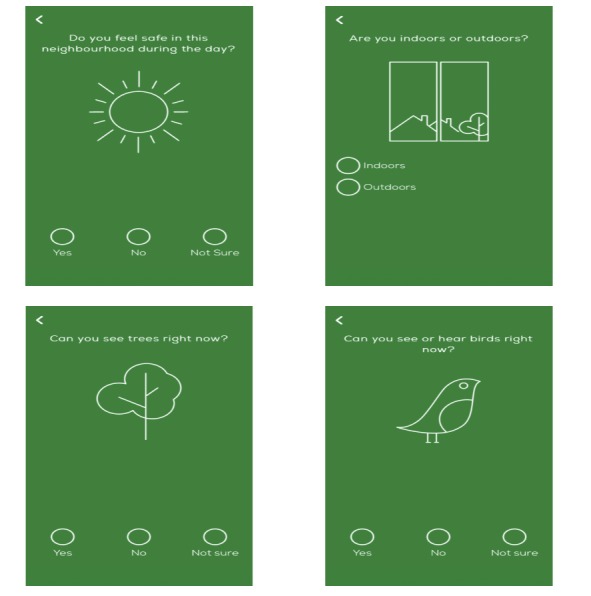
Urban Mind app user interfaces.
These studies suggest that e-mental health has potential value in identifying risk factors for subsequent transition to psychosis and predicting the onset of psychosis. In addition, these approaches may also be applied toward prognosis for outcomes other than transition to psychosis, such as functional outcomes and development of nonpsychotic disorders. ESM and digital phenotyping are two appealing methodologies with great promise and are ideally suited to longitudinal designs to examine the development of clinical trajectories in CHR-P populations.
E-Treatment
One criticism of CHR construct is that there is no treatment conclusively shown to prevent the onset of psychosis [71]. However, there are several promising therapeutic strategies currently under investigation that could significantly reduce psychosis risk and address important additional areas of impairment—in particular, cognitive deficits and social and occupational functioning.
Since individuals at CHR-P do not have a mental disorder as such, any treatment has to be well tolerated and acceptable. Moreover, by definition these individuals retain a degree of insight into their symptoms [72], offering a significant therapeutic window of opportunity prior to the onset of psychosis. Guidelines currently suggest psychological therapy and recommend not treating with antipsychotic medication [73]. As various psychological therapies can be delivered online, e-mental health has the potential to enhance access to treatments and reduce costs. A systematic review and meta-analysis suggested that guided online cognitive behavioral therapy (CBT) for various psychiatric disorders had equivalent effect sizes compared with face-to-face interventions [74], highlighting the potential utility of administering CBT through digital modalities. Other psychological interventions such as mindfulness, which has shown some efficacy for psychosis [75], may also be effective when provided online [76]. Alvarez-Jiminez et al [77] conducted a novel strengths and mindfulness-based online social therapy for individuals at CHR-P. Participants found the intervention acceptable and showed an improvement in social functioning and subjective well-being, warranting further study.
Digital interventions showing promise in established psychosis, relevant to CHR-P, include avatar therapy [78], online CBT skills program for hallucinations [79], mobile phone apps delivering therapeutic interventions [80-82], and online peer-to-to peer support networks, reported to increase feelings of social connectedness [83]. Indeed, Rice et al [84] have developed an e-mental health service providing clinician-delivered Web chat counseling, a moderated peer-to-peer social network, and user directed online therapy. This enhanced moderated online social therapy is seeded in eheadspace, part of headspace, a flagship Australian youth mental health program with an integrated early intervention in psychosis component [85].
An important aspect of the clinical presentation of CHR-P is cognitive deficits across a range of domains associated with transition to psychosis [86,87]. One way of targeting cognitive deficits in CHR participants could be cognitive remediation (CR)–based treatments [88] that can be administered via computerized training procedures [89]. These approaches improve neural circuits underlying cognitive deficits with significant impact on social functioning [90], especially if administered in the early stages of schizophrenia [91]. There is emerging evidence that CR treatments may be effective in targeting cognitive dysfunctions in CHR participants. Loewy et al [92] examined the effects of CR administered through laptop and home computers on verbal learning and memory. CR significantly improved verbal memory (effect size = 0.61) as well as positive symptoms. Hooker et al [93] presented a pilot uncontrolled study of cognitive training delivered online for CHR-P, showing this intervention is feasible and appears to provide improvements in the global cognition in response to training.
Digital interventions could also be extended to address functional impairments in CHR-P individuals. In a recent study, Schlosser et al [82] examined a mobile-based digital health intervention designed to improve motivation and quality of life in young people with schizophrenia. Compared to the control group, the active treatment arm demonstrated significant improvements in levels of depression, defeatist beliefs, and self-efficacy as well as a trend for improved negative symptoms. These improvements were maintained 3 months after the end of trial. Accordingly, these data suggest that mobile-based interventions could be useful for addressing important domains of functioning in CHR-P populations.
Virtual reality (VR) is an emerging tool for the treatment of a wide range of mental disorders that involves interactive computer-generated worlds in which therapeutic strategies can be implemented and tested [94]. In established schizophrenia, VR approaches have shown preliminary efficacy in targeting positive symptoms, such as delusions [95] and hallucinations [96], as well as increasing social participation [97]. VR has also shown potential as a treatment adjunct in psychosis in modalities such as cognitive remediation and social skills training [98], showing preliminary promising results.
Following successful pilot research demonstrating the safety of VR in the CHR-P population [99], this technique has been used to investigate the effect of various simulated social environments on psychopathology. A simulation of the London underground transport system has been used to investigate paranoid ideation [100,101] and perceived ethnic discrimination [102], while café [103] and bar simulations [104] have been used to investigate the effect of social stress on interpersonal distance and paranoid ideation, respectively. These studies show the possibilities of using VR to study psychopathology in a simulated environment. Arguably, VR may be better suited as a treatment modality in CHR-P compared with more established stages of psychosis.
Conclusion
Digital technologies are at present underused as a research or clinical tool for CHR-P and may be ideally placed to address the current challenges of the field. These include detecting those at risk of psychosis outside specialized CHR-P clinics, monitoring to predict future development of psychosis, identifying digital biomarkers for psychosis and other clinical outcomes, and delivering novel treatment modalities. Furthermore, individuals at CHR-P, by definition young and help-seeking, are ideally suited to digital interventions. However, longitudinal studies of digital technologies are required to assess which measures are useful for predicting risk of psychosis in individuals identified by online screening. Future research is required to rigorously test whether digital interventions have a place in the detection or management in people at CHR-P. In addition, we need greater understanding of the relationship between the different types of measures (eg, active and passive data collected via ESM and digital phenotyping, respectively) in order to develop and validate e-tools that provide maximal information while minimizing burden on the patient.
Acknowledgments
This study was supported by the King’s College London Confidence in Concept award from the Medical Research Council (MC_PC_16048) to PFP. This study also represents independent research partially funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London, Maudsley NHS Foundation Trust, and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care. The funders had no influence on the design, collection, analysis and interpretation of the data, writing of the report, or decision to submit this article for publication.
Abbreviations
- CBT
cognitive behavioral therapy
- CHR-P
clinical high risk for psychosis
- CR
cognitive remediation
- ESM
experience sampling method
- FEP
first episode psychosis
- ICD-10
International Classification of Diseases, Tenth Revision
- NHS
National Health Service
- NIHR
National Institute for Health Research
- PCA
9-item perceptive and cognitive aberrations questionnaire
- PQ-16
16-item prodromal questionnaire
- VR
virtual reality
Appendix
Search strategy and inclusion criteria.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Fusar-Poli P. The clinical high-risk state for psychosis (CHR-P), version II. Schizophr Bull. 2017 Dec;43(1):44–47. doi: 10.1093/schbul/sbw158. http://europepmc.org/abstract/MED/28053129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Millan MJ, Andrieux A, Bartzokis G, Cadenhead K, Dazzan P, Fusar-Poli P, Gallinat J, Giedd J, Grayson DR, Heinrichs M, Kahn R, Krebs M, Leboyer M, Lewis D, Marin O, Marin P, Meyer-Lindenberg A, McGorry P, McGuire P, Owen MJ, Patterson P, Sawa A, Spedding M, Uhlhaas P, Vaccarino F, Wahlestedt C, Weinberger D. Altering the course of schizophrenia: progress and perspectives. Nat Rev Drug Discov. 2016 Dec;15(7):485–515. doi: 10.1038/nrd.2016.28. [DOI] [PubMed] [Google Scholar]
- 3.Radua J, Ramella-Cravaro V, Ioannidis JPA, Reichenberg A, Phiphopthatsanee N, Amir T, Yenn Thoo H, Oliver D, Davies C, Morgan C, McGuire P, Murray RM, Fusar-Poli P. What causes psychosis? An umbrella review of risk and protective factors. World Psychiatry. 2018 Feb;17(1):49–66. doi: 10.1002/wps.20490. doi: 10.1002/wps.20490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fusar-Poli P, Borgwardt S, Bechdolf A, Addington J, Riecher-Rössler A, Schultze-Lutter F, Keshavan M, Wood S, Ruhrmann S, Seidman LJ, Valmaggia L, Cannon T, Velthorst E, De Haan L, Cornblatt B, Bonoldi I, Birchwood M, McGlashan T, Carpenter W, McGorry P, Klosterkötter J, McGuire P, Yung A. The psychosis high-risk state: a comprehensive state-of-the-art review. JAMA Psychiatry. 2013 Jan;70(1):107–120. doi: 10.1001/jamapsychiatry.2013.269. http://europepmc.org/abstract/MED/23165428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fusar-Poli P, Rocchetti M, Sardella A, Avila A, Brandizzi M, Caverzasi E, Politi P, Ruhrmann S, McGuire P. Disorder, not just state of risk: meta-analysis of functioning and quality of life in people at high risk of psychosis. Br J Psychiatry. 2015 Sep;207(3):198–206. doi: 10.1192/bjp.bp.114.157115. [DOI] [PubMed] [Google Scholar]
- 6.Fusar-Poli P, Cappucciati M, Borgwardt S, Woods SW, Addington J, Nelson B, Nieman DH, Stahl DR, Rutigliano G, Riecher-Rössler A, Simon AE, Mizuno M, Lee TY, Kwon JS, Lam MML, Perez J, Keri S, Amminger P, Metzler S, Kawohl W, Rössler W, Lee J, Labad J, Ziermans T, An SK, Liu C, Woodberry KA, Braham A, Corcoran C, McGorry P, Yung AR, McGuire PK. Heterogeneity of psychosis risk within individuals at clinical high risk: a meta-analytical stratification. JAMA Psychiatry. 2016 Feb;73(2):113–120. doi: 10.1001/jamapsychiatry.2015.2324. [DOI] [PubMed] [Google Scholar]
- 7.Fusar-Poli P, Cappucciati M, Bonoldi I, Hui LMC, Rutigliano G, Stahl DR, Borgwardt S, Politi P, Mishara AL, Lawrie SM, Carpenter WT, McGuire PK. Prognosis of brief psychotic episodes: a meta-analysis. JAMA Psychiatry. 2016 Mar;73(3):211–220. doi: 10.1001/jamapsychiatry.2015.2313. [DOI] [PubMed] [Google Scholar]
- 8.Fusar-Poli P, Cappucciati M, De Micheli A, Rutigliano G, Bonoldi I, Tognin S, Ramella-Cravaro V, Castagnini A, McGuire P. Diagnostic and prognostic significance of brief limited intermittent psychotic symptoms (BLIPS) in individuals at ultra high risk. Schizophr Bull. 2017 Dec;43(1):48–56. doi: 10.1093/schbul/sbw151. http://europepmc.org/abstract/MED/28053130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rutigliano G, Merlino S, Minichino A, Patel R, Davies C, Oliver D, De Micheli A, McGuire P, Fusar-Poli P. Long term outcomes of acute and transient psychotic disorders: the missed opportunity of preventive interventions. Eur Psychiatry. 2018 Dec;52:126–133. doi: 10.1016/j.eurpsy.2018.05.004. [DOI] [PubMed] [Google Scholar]
- 10.Minichino A, Rutigliano G, Merlino S, Davies C, Oliver D, De Micheli A, Patel R, McGuire P, Fusar-Poli P. Unmet needs in patients with brief psychotic disorders: too ill for clinical high risk services and not ill enough for first episode services. Eur Psychiatry. 2019 Dec;57:26–32. doi: 10.1016/j.eurpsy.2018.12.006. [DOI] [PubMed] [Google Scholar]
- 11.Fusar-Poli P, Bonoldi I, Yung AR, Borgwardt S, Kempton MJ, Valmaggia L, Barale F, Caverzasi E, McGuire P. Predicting psychosis: meta-analysis of transition outcomes in individuals at high clinical risk. Arch Gen Psychiatry. 2012 Mar;69(3):220–229. doi: 10.1001/archgenpsychiatry.2011.1472. [DOI] [PubMed] [Google Scholar]
- 12.Fusar-Poli P, Palombini E, Davies C, Oliver D, Bonoldi I, Ramella-Cravaro V, McGuire P. Why transition risk to psychosis is not declining at the OASIS ultra high risk service: the hidden role of stable pretest risk enrichment. Schizophr Res. 2018 Dec;192:385–390. doi: 10.1016/j.schres.2017.06.015. [DOI] [PubMed] [Google Scholar]
- 13.Fusar-Poli P, Rutigliano G, Stahl D, Schmidt A, Ramella-Cravaro V, Hitesh S, McGuire P. Deconstructing pretest risk enrichment to optimize prediction of psychosis in individuals at clinical high risk. JAMA Psychiatry. 2016 Dec 01;73(12):1260–1267. doi: 10.1001/jamapsychiatry.2016.2707. [DOI] [PubMed] [Google Scholar]
- 14.Cannon TD, Cadenhead K, Cornblatt B, Woods SW, Addington J, Walker E, Seidman LJ, Perkins D, Tsuang M, McGlashan T, Heinssen R. Prediction of psychosis in youth at high clinical risk: a multisite longitudinal study in North America. Arch Gen Psychiatry. 2008 Jan;65(1):28–37. doi: 10.1001/archgenpsychiatry.2007.3. http://europepmc.org/abstract/MED/18180426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Addington J, Heinssen R. Prediction and prevention of psychosis in youth at clinical high risk. Annu Rev Clin Psychol. 2012;8:269–289. doi: 10.1146/annurev-clinpsy-032511-143146. [DOI] [PubMed] [Google Scholar]
- 16.Yung AR, McGorry PD, McFarlane CA, Patton GC. The Pace Clinic: development of a clinical service for young people at high risk of psychosis. Australas Psychiatry. 2016 Jun 25;3(5):345–349. doi: 10.3109/10398569509085280. [DOI] [Google Scholar]
- 17.Fusar-Poli P, Byrne M, Badger S, Valmaggia LR, McGuire PK. Outreach and support in south London (OASIS), 2001-2011: ten years of early diagnosis and treatment for young individuals at high clinical risk for psychosis. Eur Psychiatry. 2013 Jun;28(5):315–326. doi: 10.1016/j.eurpsy.2012.08.002. https://linkinghub.elsevier.com/retrieve/pii/S0924-9338(12)00098-3. [DOI] [PubMed] [Google Scholar]
- 18.Fusar-Poli P, Rutigliano G, Stahl D, Davies C, Bonoldi I, Reilly T, McGuire P. Development and validation of a clinically based risk calculator for the transdiagnostic prediction of psychosis. JAMA Psychiatry. 2017 Dec 01;74(5):493–500. doi: 10.1001/jamapsychiatry.2017.0284. http://www.psychosis-risk.net/step1.asp. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McGorry PD, Hartmann JA, Spooner R, Nelson B. Beyond the “at risk mental state” concept: transitioning to transdiagnostic psychiatry. World Psychiatry. 2018 Jun;17(2):133–142. doi: 10.1002/wps.20514. doi: 10.1002/wps.20514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fusar-Poli P, Cappucciati M, Rutigliano G, Schultze-Lutter F, Bonoldi I, Borgwardt S, Riecher-Rössler A, Addington J, Perkins D, Woods SW, McGlashan TH, Lee J, Klosterkötter J, Yung AR, McGuire P. At risk or not at risk? A meta-analysis of the prognostic accuracy of psychometric interviews for psychosis prediction. World Psychiatry. 2015 Oct;14(3):322–332. doi: 10.1002/wps.20250. doi: 10.1002/wps.20250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fusar-Poli P, Davies C, Bonoldi I. A case of a college student presenting with mild mental health problems. JAMA Psychiatry. 2018 Dec 01;75(12):1298–1299. doi: 10.1001/jamapsychiatry.2018.2486. [DOI] [PubMed] [Google Scholar]
- 22.Fusar-Poli P, Hijazi Z, Stahl D, Steyerberg EW. The science of prognosis in psychiatry: a review. JAMA Psychiatry. 2018 Dec 01;75(12):1289–1297. doi: 10.1001/jamapsychiatry.2018.2530. [DOI] [PubMed] [Google Scholar]
- 23.Davies C, Cipriani A, Ioannidis JPA, Radua J, Stahl D, Provenzani U, McGuire P, Fusar-Poli P. Lack of evidence to favor specific preventive interventions in psychosis: a network meta-analysis. World Psychiatry. 2018 Jun;17(2):196–209. doi: 10.1002/wps.20526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Davies C, Radua J, Cipriani A, Stahl D, Provenzani U, McGuire P, Fusar-Poli P. Efficacy and acceptability of interventions for attenuated positive psychotic symptoms in individuals at clinical high risk of psychosis: a network meta-analysis. Front Psychiatry. 2018;9:187. doi: 10.3389/fpsyt.2018.00187. doi: 10.3389/fpsyt.2018.00187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Devoe DJ, Farris MS, Townes P, Addington J. Attenuated psychotic symptom interventions in youth at risk of psychosis: a systematic review and meta-analysis. Early Interv Psychiatry. 2019 Dec;13(1):3–17. doi: 10.1111/eip.12677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Devoe DJ, Peterson A, Addington J. Negative symptom interventions in youth at risk of psychosis: a systematic review and network meta-analysis. Schizophr Bull. 2018 Dec 06;44(4):807–823. doi: 10.1093/schbul/sbx139. http://europepmc.org/abstract/MED/29069511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Stafford MR, Jackson H, Mayo-Wilson E, Morrison AP, Kendall T. Early interventions to prevent psychosis: systematic review and meta-analysis. BMJ. 2013 Jan 18;346:f185. doi: 10.1136/bmj.f185. http://europepmc.org/abstract/MED/23335473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hutton P, Taylor PJ. Cognitive behavioural therapy for psychosis prevention: a systematic review and meta-analysis. Psychol Med. 2014 Feb;44(3):449–468. doi: 10.1017/S0033291713000354. [DOI] [PubMed] [Google Scholar]
- 29.Devoe DJ, Farris MS, Townes P, Addington J. Interventions and social functioning in youth at risk of psychosis: a systematic review and meta-analysis. Early Interv Psychiatry. 2019 Apr;13(2):169–180. doi: 10.1111/eip.12689. [DOI] [PubMed] [Google Scholar]
- 30.Sugawara E, Nikaido H. Properties of AdeABC and AdeIJK efflux systems of Acinetobacter baumannii compared with those of the AcrAB-TolC system of Escherichia coli. Antimicrob Agents Chemother. 2014 Dec;58(12):7250–7257. doi: 10.1128/AAC.03728-14. http://aac.asm.org/cgi/pmidlookup?view=long&pmid=25246403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Firth J, Torous J. Smartphone apps for schizophrenia: a systematic review. JMIR Mhealth Uhealth. 2015;3(4):e102. doi: 10.2196/mhealth.4930. http://mhealth.jmir.org/2015/4/e102/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Alvarez-Jimenez M, Alcazar-Corcoles MA, González-Blanch C, Bendall S, McGorry PD, Gleeson JF. Online, social media and mobile technologies for psychosis treatment: a systematic review on novel user-led interventions. Schizophr Res. 2014 Jun;156(1):96–106. doi: 10.1016/j.schres.2014.03.021. [DOI] [PubMed] [Google Scholar]
- 33.Firth J, Cotter J, Torous J, Bucci S, Firth JA, Yung AR. Mobile phone ownership and endorsement of “mhealth” among people with psychosis: a meta- analysis of cross-sectional studies. Schizophr Bull. 2015 Sep 22;42(2):448–455. doi: 10.1093/schbul/sbv132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Torous J, Woodyatt J, Keshavan M, Tully LM. A new hope for early psychosis care: the evolving landscape of digital care tools. Br J Psychiatry. 2019 May;214(5):269–272. doi: 10.1192/bjp.2019.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Miller TJ, McGlashan TH, Rosen JL, Cadenhead K, Cannon T, Ventura J, McFarlane W, Perkins DO, Pearlson GD, Woods SW. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703–715. doi: 10.1093/oxfordjournals.schbul.a007040. [DOI] [PubMed] [Google Scholar]
- 36.Yung AR, Yuen HP, McGorry PD, Phillips LJ, Kelly D, Dell'Olio M, Francey SM, Cosgrave EM, Killackey E, Stanford C, Godfrey K, Buckby J. Mapping the onset of psychosis: the Comprehensive Assessment of At-Risk Mental States. Aust N Z J Psychiatry. 2005;39(11-12):964–971. doi: 10.1080/j.1440-1614.2005.01714.x. [DOI] [PubMed] [Google Scholar]
- 37.Koehler K, Sauer H. Huber's basic symptoms: another approach to negative psychopathology in schizophrenia. Compr Psychiatry. 1984;25(2):174–182. doi: 10.1016/0010-440x(84)90006-3. [DOI] [PubMed] [Google Scholar]
- 38.Schultze-Lutter F, Ruhrmann S, Berning J, Maier W, Klosterkötter J. Basic symptoms and ultrahigh risk criteria: symptom development in the initial prodromal state. Schizophr Bull. 2010 Jan;36(1):182–191. doi: 10.1093/schbul/sbn072. http://europepmc.org/abstract/MED/18579555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Schultze-Lutter F, Klosterkötter J, Ruhrmann S. Improving the clinical prediction of psychosis by combining ultra-high risk criteria and cognitive basic symptoms. Schizophr Res. 2014 Apr;154(1-3):100–106. doi: 10.1016/j.schres.2014.02.010. [DOI] [PubMed] [Google Scholar]
- 40.Rutigliano G, Valmaggia L, Landi P, Frascarelli M, Cappucciati M, Sear V, Rocchetti M, De Micheli A, Jones C, Palombini E, McGuire P, Fusar-Poli P. Persistence or recurrence of non-psychotic comorbid mental disorders associated with 6-year poor functional outcomes in patients at ultra high risk for psychosis. J Affect Disord. 2016 Oct;203:101–110. doi: 10.1016/j.jad.2016.05.053. [DOI] [PubMed] [Google Scholar]
- 41.Fusar-Poli P, Schultze-Lutter F, Cappucciati M, Rutigliano G, Bonoldi I, Stahl D, Borgwardt S, Riecher-Rössler A, Addington J, Perkins DO, Woods SW, McGlashan T, Lee J, Klosterkötter J, Yung AR, McGuire P. The dark side of the moon: meta-analytical impact of recruitment strategies on risk enrichment in the clinical high risk state for psychosis. Schizophr Bull. 2016 May;42(3):732–743. doi: 10.1093/schbul/sbv162. http://europepmc.org/abstract/MED/26591006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ajnakina O, Morgan C, Gayer-Anderson C, Oduola S, Bourque F, Bramley S, Williamson J, MacCabe JH, Dazzan P, Murray RM, David AS. Only a small proportion of patients with first episode psychosis come via prodromal services: a retrospective survey of a large UK mental health programme. BMC Psychiatry. 2017 Dec 25;17(1):308. doi: 10.1186/s12888-017-1468-y. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-017-1468-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Birnbaum ML, Rizvi AF, Faber K, Addington J, Correll CU, Gerber C, Lahti AC, Loewy RL, Mathalon DH, Nelson LA, Voineskos AN, Walker EF, Ward E, Kane JM. Digital trajectories to care in first-episode psychosis. Psychiatr Serv. 2018 Dec 01;69(12):1259–1263. doi: 10.1176/appi.ps.201800180. http://europepmc.org/abstract/MED/30256181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Eichstaedt JC, Smith RJ, Merchant RM, Ungar LH, Crutchley P, Preoţiuc-Pietro D, Asch DA, Schwartz HA. Facebook language predicts depression in medical records. Proc Natl Acad Sci USA. 2018 Dec 30;115(44):11203–11208. doi: 10.1073/pnas.1802331115. http://www.pnas.org/cgi/pmidlookup?view=long&pmid=30322910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bedi G, Carrillo F, Cecchi GA, Slezak DF, Sigman M, Mota NB, Ribeiro S, Javitt DC, Copelli M, Corcoran CM. Automated analysis of free speech predicts psychosis onset in high-risk youths. NPJ Schizophr. 2015;1:15030. doi: 10.1038/npjschz.2015.30. http://europepmc.org/abstract/MED/27336038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Corcoran CM, Carrillo F, Fernández-Slezak D, Bedi G, Klim C, Javitt DC, Bearden CE, Cecchi GA. Prediction of psychosis across protocols and risk cohorts using automated language analysis. World Psychiatry. 2018 Feb;17(1):67–75. doi: 10.1002/wps.20491. doi: 10.1002/wps.20491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Krishnan R, Natarajan BB, Warren S. Two-stage approach for detection and reduction of motion artifacts in photoplethysmographic data. IEEE Trans Biomed Eng. 2010 Aug;57(8):1867–1876. doi: 10.1109/TBME.2009.2039568. [DOI] [PubMed] [Google Scholar]
- 48.Your Study. [2019-06-29]. https://www.your-study.org.uk/
- 49.Müller M, Vetter S, Buchli-Kammermann J, Stieglitz R, Stettbacher A, Riecher-Rössler A. The self-screen-prodrome as a short screening tool for pre-psychotic states. Schizophr Res. 2010 Nov;123(2-3):217–224. doi: 10.1016/j.schres.2010.08.018. [DOI] [PubMed] [Google Scholar]
- 50.Fusar-Poli P, Raballo A, Parnas J. What is an attenuated psychotic symptom? On the importance of the context. Schizophr Bull. 2017 Dec 01;43(4):687–692. doi: 10.1093/schbul/sbw182. http://europepmc.org/abstract/MED/28039421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Fusar-Poli P, Werbeloff N, Rutigliano G, Oliver D, Davies C, Stahl D, McGuire P, Osborn D. Transdiagnostic risk calculator for the automatic detection of individuals at risk and the prediction of psychosis: second replication in an independent national health service trust. Schizophr Bull. 2018 Jun 12; doi: 10.1093/schbul/sby070. http://europepmc.org/abstract/MED/29897527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Fusar-Poli P, Oliver D, Spada G, Patel R, Stewart R, Dobson R, McGuire P. Real world implementation of a transdiagnostic risk calculator for the automatic detection of individuals at risk of psychosis in clinical routine: study protocol. Front Psychiatry. 2019;10:109. doi: 10.3389/fpsyt.2019.00109. doi: 10.3389/fpsyt.2019.00109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cannon TD, Yu C, Addington J, Bearden CE, Cadenhead KS, Cornblatt BA, Heinssen R, Jeffries CD, Mathalon DH, McGlashan TH, Perkins DO, Seidman LJ, Tsuang MT, Walker EF, Woods SW, Kattan MW. An individualized risk calculator for research in prodromal psychosis. Am J Psychiatry. 2016 Oct 01;173(10):980–988. doi: 10.1176/appi.ajp.2016.15070890. http://riskcalc.org:3838/napls/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Carrión RE, Cornblatt BA, Burton CZ, Tso IF, Auther AM, Adelsheim S, Calkins R, Carter CS, Niendam T, Sale TG, Taylor SF, McFarlane WR. Personalized prediction of psychosis: external validation of the NAPLS-2 psychosis risk calculator with the EDIPPP project. Am J Psychiatry. 2016 Oct 01;173(10):989–996. doi: 10.1176/appi.ajp.2016.15121565. http://europepmc.org/abstract/MED/27363511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kempton MJ, Bonoldi I, Valmaggia L, McGuire P, Fusar-Poli P. Speed of psychosis progression in people at ultra-high clinical risk: a complementary meta-analysis. JAMA Psychiatry. 2015 Jun;72(6):622–623. doi: 10.1001/jamapsychiatry.2015.0094. [DOI] [PubMed] [Google Scholar]
- 56.Dubad M, Winsper C, Meyer C, Livanou M, Marwaha S. A systematic review of the psychometric properties, usability and clinical impacts of mobile mood-monitoring applications in young people. Psychol Med. 2018 Jan;48(2):208–228. doi: 10.1017/S0033291717001659. [DOI] [PubMed] [Google Scholar]
- 57.Palmier-Claus JE, Dunn G, Lewis SW. Emotional and symptomatic reactivity to stress in individuals at ultra-high risk of developing psychosis. Psychol Med. 2012 May;42(5):1003–1012. doi: 10.1017/S0033291711001929. [DOI] [PubMed] [Google Scholar]
- 58.Palmier-Claus JE, Dunn G, Taylor H, Morrison AP, Lewis SW. Cognitive-self consciousness and metacognitive beliefs: stress sensitization in individuals at ultra-high risk of developing psychosis. Br J Clin Psychol. 2013 Mar;52(1):26–41. doi: 10.1111/j.2044-8260.2012.02043.x. [DOI] [PubMed] [Google Scholar]
- 59.Palmier-Claus JE, Ainsworth J, Machin M, Barrowclough C, Dunn G, Barkus E, Rogers A, Wykes T, Kapur S, Buchan I, Salter E, Lewis SW. The feasibility and validity of ambulatory self-report of psychotic symptoms using a smartphone software application. BMC Psychiatry. 2012;12:172. doi: 10.1186/1471-244X-12-172. http://www.biomedcentral.com/1471-244X/12/172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Klippel A, Myin-Germeys I, Chavez-Baldini U, Preacher KJ, Kempton M, Valmaggia L, Calem M, So S, Beards S, Hubbard K, Gayer-Anderson C, Onyejiaka A, Wichers M, McGuire P, Murray R, Garety P, van Os J, Wykes T, Morgan C, Reininghaus U. Modeling the interplay between psychological processes and adverse, stressful contexts and experiences in pathways to psychosis: an experience sampling study. Schizophr Bull. 2017 Dec 01;43(2):302–315. doi: 10.1093/schbul/sbw185. http://europepmc.org/abstract/MED/28204708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Reininghaus U, Gayer-Anderson C, Valmaggia L, Kempton MJ, Calem M, Onyejiaka A, Hubbard K, Dazzan P, Beards S, Fisher HL, Mills JG, McGuire P, Craig TKJ, Garety P, van Os J, Murray RM, Wykes T, Myin-Germeys I, Morgan C. Psychological processes underlying the association between childhood trauma and psychosis in daily life: an experience sampling study. Psychol Med. 2016 Dec;46(13):2799–2813. doi: 10.1017/S003329171600146X. http://europepmc.org/abstract/MED/27400863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Reininghaus U, Kempton MJ, Valmaggia L, Craig TKJ, Garety P, Onyejiaka A, Gayer-Anderson C, So SH, Hubbard K, Beards S, Dazzan P, Pariante C, Mondelli V, Fisher HL, Mills JG, Viechtbauer W, McGuire P, van Os J, Murray RM, Wykes T, Myin-Germeys I, Morgan C. Stress sensitivity, aberrant salience, and threat anticipation in early psychosis: an experience sampling study. Schizophr Bull. 2016 May;42(3):712–722. doi: 10.1093/schbul/sbv190. http://europepmc.org/abstract/MED/26834027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.van der Steen Y, Gimpel-Drees J, Lataster T, Viechtbauer W, Simons CJP, Lardinois M, Michel TM, Janssen B, Bechdolf A, Wagner M, Myin-Germeys I. Clinical high risk for psychosis: the association between momentary stress, affective and psychotic symptoms. Acta Psychiatr Scand. 2017 Dec;136(1):63–73. doi: 10.1111/acps.12714. [DOI] [PubMed] [Google Scholar]
- 64.Booij SH, Wichers M, de Jonge P, Sytema S, van Os J, Wunderink L, Wigman JTW. Study protocol for a prospective cohort study examining the predictive potential of dynamic symptom networks for the onset and progression of psychosis: the Mapping Individual Routes of Risk and Resilience (Mirorr) study. BMJ Open. 2018 Dec 21;8(1):e019059. doi: 10.1136/bmjopen-2017-019059. http://bmjopen.bmj.com/cgi/pmidlookup?view=long&pmid=29358438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Onnela J, Rauch SL. Harnessing smartphone-based digital phenotyping to enhance behavioral and mental health. Neuropsychopharmacology. 2016 Jun;41(7):1691–1696. doi: 10.1038/npp.2016.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Insel TR. Digital phenotyping: technology for a new science of behavior. JAMA. 2017 Oct 03;318(13):1215–1216. doi: 10.1001/jama.2017.11295. [DOI] [PubMed] [Google Scholar]
- 67.Barnett I, Torous J, Staples P, Sandoval L, Keshavan M, Onnela J. Relapse prediction in schizophrenia through digital phenotyping: a pilot study. Neuropsychopharmacology. 2018 Jul;43(8):1660–1666. doi: 10.1038/s41386-018-0030-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Insel TR. Digital phenotyping: a global tool for psychiatry. World Psychiatry. 2018 Oct;17(3):276–277. doi: 10.1002/wps.20550. doi: 10.1002/wps.20550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Staples P, Torous J, Barnett I, Sandoval L, Keshavan M, Onnela JP. Characterizing the clinical relevance of digital phenotyping data quality with applications to a cohort with schizophrenia. Biol Psychiatry. 2018 May;83(9):S61. doi: 10.1016/j.biopsych.2018.02.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Bakolis I, Hammoud R, Smythe M, Gibbons J, Davidson N, Tognin S, Mechelli A. Urban Mind: using smartphone technologies to investigate the impact of nature on mental well-being in real time. Bioscience. 2018 Feb 01;68(2):134–145. doi: 10.1093/biosci/bix149. https://www.urbanmind.info/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Ajnakina O, David AS, Murray RM. 'At risk mental state' clinics for psychosis - an idea whose time has come - and gone! Psychol Med. 2018 Dec 26;:1–6. doi: 10.1017/S0033291718003859. [DOI] [PubMed] [Google Scholar]
- 72.Kimhy D, Jobson-Ahmed L, Ben-David S, Ramadhar L, Malaspina D, Corcoran CM. Cognitive insight in individuals at clinical high risk for psychosis. Early Interv Psychiatry. 2014 May;8(2):130–137. doi: 10.1111/eip.12023. http://europepmc.org/abstract/MED/23343417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.National Institute for Health and Clinical Excellence. 2014. Feb 12, [2019-08-16]. Psychosis and schizophrenia in adults: preprevention and management https://nice.org.uk/guidance/cg178.
- 74.Andersson G, Cuijpers P, Carlbring P, Riper H, Hedman E. Guided Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: a systematic review and meta-analysis. World Psychiatry. 2014 Oct;13(3):288–295. doi: 10.1002/wps.20151. doi: 10.1002/wps.20151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Louise S, Fitzpatrick M, Strauss C, Rossell SL, Thomas N. Mindfulness- and acceptance-based interventions for psychosis: our current understanding and a meta-analysis. Schizophr Res. 2018 Dec;192:57–63. doi: 10.1016/j.schres.2017.05.023. [DOI] [PubMed] [Google Scholar]
- 76.Sevilla-Llewellyn-Jones J, Santesteban-Echarri O, Pryor I, McGorry P, Alvarez-Jimenez M. Web-based mindfulness interventions for mental health treatment: systematic review and meta-analysis. JMIR Ment Health. 2018 Sep 25;5(3):e10278. doi: 10.2196/10278. http://mental.jmir.org/2018/3/e10278/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Alvarez-Jimenez M, Gleeson JF, Bendall S, Penn DL, Yung AR, Ryan RM, Eleftheriadis D, D'Alfonso S, Rice S, Miles C, Russon P, Lederman R, Chambers R, Gonzalez-Blanch C, Lim MH, Killackey E, McGorry PD, Nelson B. Enhancing social functioning in young people at Ultra High Risk (UHR) for psychosis: a pilot study of a novel strengths and mindfulness-based online social therapy. Schizophr Res. 2018 Dec;202:369–377. doi: 10.1016/j.schres.2018.07.022. [DOI] [PubMed] [Google Scholar]
- 78.Craig TK, Rus-Calafell M, Ward T, Leff JP, Huckvale M, Howarth E, Emsley R, Garety PA. AVATAR therapy for auditory verbal hallucinations in people with psychosis: a single-blind, randomised controlled trial. Lancet Psychiatry. 2018 Dec;5(1):31–40. doi: 10.1016/S2215-0366(17)30427-3. https://linkinghub.elsevier.com/retrieve/pii/S2215-0366(17)30427-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Arranz MJ, Kerwin RW. Neurotransmitter-related genes and antipsychotic response: pharmacogenetics meets psychiatric treatment. Ann Med. 2000 Mar;32(2):128–133. doi: 10.3109/07853890009011762. [DOI] [PubMed] [Google Scholar]
- 80.Bucci S, Barrowclough C, Ainsworth J, Machin M, Morris R, Berry K, Emsley R, Lewis S, Edge D, Buchan I, Haddock G. Actissist: proof-of-concept trial of a theory-driven digital intervention for psychosis. Schizophr Bull. 2018 Mar 16;44(5):1070–1080. doi: 10.1093/schbul/sby032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Kim S, Lee G, Yu H, Jung E, Lee J, Kim S, Kim J, Shin I, Yoon J. Development and feasibility of smartphone application for cognitive-behavioural case management of individuals with early psychosis. Early Interv Psychiatry. 2017 May 18;12(6):1087–1093. doi: 10.1111/eip.12418. [DOI] [PubMed] [Google Scholar]
- 82.Schlosser DA, Campellone TR, Truong B, Etter K, Vergani S, Komaiko K, Vinogradov S. Efficacy of PRIME, a mobile app intervention designed to improve motivation in young people with schizophrenia. Schizophr Bull. 2018 Dec 20;44(5):1010–1020. doi: 10.1093/schbul/sby078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Naslund JA, Aschbrenner KA, Marsch LA, Bartels SJ. The future of mental health care: peer-to-peer support and social media. Epidemiol Psychiatr Sci. 2016 Apr;25(2):113–122. doi: 10.1017/S2045796015001067. http://europepmc.org/abstract/MED/26744309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Rice S, Gleeson J, Leicester S, Bendall S, D'Alfonso S, Gilbertson T, Killackey E, Parker A, Lederman R, Wadley G, Santesteban-Echarri O, Pryor I, Mawren D, Ratheesh A, Alvarez-Jimenez M. Implementation of the enhanced moderated online social therapy (MOST+) model within a national youth e-mental health service (eHeadspace): protocol for a single group pilot study for help-seeking young people. JMIR Res Protoc. 2018 Feb 22;7(2):e48. doi: 10.2196/resprot.8813. http://www.researchprotocols.org/2018/2/e48/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Rickwood DJ, Telford NR, Parker AG, Tanti CJ, McGorry PD. Headspace—Australia's innovation in youth mental health: who are the clients and why are they presenting? Med J Aust. 2014 Feb 3;200(2):108–111. doi: 10.5694/mja13.11235. [DOI] [PubMed] [Google Scholar]
- 86.Fusar-Poli P, Deste G, Smieskova R, Barlati S, Yung AR, Howes O, Stieglitz R, Vita A, McGuire P, Borgwardt S. Cognitive functioning in prodromal psychosis: a meta-analysis. Arch Gen Psychiatry. 2012 Jun;69(6):562–571. doi: 10.1001/archgenpsychiatry.2011.1592. [DOI] [PubMed] [Google Scholar]
- 87.Seidman LJ, Shapiro DI, Stone WS, Woodberry KA, Ronzio A, Cornblatt BA, Addington J, Bearden CE, Cadenhead KS, Cannon TD, Mathalon DH, McGlashan TH, Perkins DO, Tsuang MT, Walker EF, Woods SW. Association of neurocognition with transition to psychosis: baseline functioning in the second phase of the north american prodrome longitudinal study. JAMA Psychiatry. 2016 Dec 01;73(12):1239–1248. doi: 10.1001/jamapsychiatry.2016.2479. http://europepmc.org/abstract/MED/27806157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Wykes T, Huddy V, Cellard C, McGurk SR, Czobor P. A meta-analysis of cognitive remediation for schizophrenia: methodology and effect sizes. Am J Psychiatry. 2011 May;168(5):472–485. doi: 10.1176/appi.ajp.2010.10060855. [DOI] [PubMed] [Google Scholar]
- 89.Biagianti B, Fisher M, Brandrett B, Schlosser D, Loewy R, Nahum M, Vinogradov S. Development and testing of a web-based battery to remotely assess cognitive health in individuals with schizophrenia. Schizophr Res. 2019 Jun;208:250–257. doi: 10.1016/j.schres.2019.01.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Subramaniam K, Luks TL, Fisher M, Simpson GV, Nagarajan S, Vinogradov S. Computerized cognitive training restores neural activity within the reality monitoring network in schizophrenia. Neuron. 2012 Feb 23;73(4):842–853. doi: 10.1016/j.neuron.2011.12.024. https://linkinghub.elsevier.com/retrieve/pii/S0896-6273(12)00049-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Eack SM, Hogarty GE, Cho RY, Prasad KMR, Greenwald DP, Hogarty SS, Keshavan MS. Neuroprotective effects of cognitive enhancement therapy against gray matter loss in early schizophrenia: results from a 2-year randomized controlled trial. Arch Gen Psychiatry. 2010 Jul;67(7):674–682. doi: 10.1001/archgenpsychiatry.2010.63. http://europepmc.org/abstract/MED/20439824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Loewy R, Fisher M, Schlosser DA, Biagianti B, Stuart B, Mathalon DH, Vinogradov S. Intensive auditory cognitive training improves verbal memory in adolescents and young adults at clinical high risk for psychosis. Schizophr Bull. 2016 Dec;42 Suppl 1:S118–S126. doi: 10.1093/schbul/sbw009. http://europepmc.org/abstract/MED/26903238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Hooker CI, Carol EE, Eisenstein TJ, Yin H, Lincoln SH, Tully LM, Dodell-Feder D, Nahum M, Keshavan MS, Seidman LJ. A pilot study of cognitive training in clinical high risk for psychosis: initial evidence of cognitive benefit. Schizophr Res. 2014 Aug;157(1-3):314–316. doi: 10.1016/j.schres.2014.05.034. http://europepmc.org/abstract/MED/24954429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Freeman D, Reeve S, Robinson A, Ehlers A, Clark D, Spanlang B, Slater M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol Med. 2017 Oct;47(14):2393–2400. doi: 10.1017/S003329171700040X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Freeman D, Bradley J, Antley A, Bourke E, DeWeever N, Evans N, Černis E, Sheaves B, Waite F, Dunn G, Slater M, Clark DM. Virtual reality in the treatment of persecutory delusions: randomised controlled experimental study testing how to reduce delusional conviction. Br J Psychiatry. 2016 Dec;209(1):62–67. doi: 10.1192/bjp.bp.115.176438. http://europepmc.org/abstract/MED/27151071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.du Sert OP, Potvin S, Lipp O, Dellazizzo L, Laurelli M, Breton R, Lalonde P, Phraxayavong K, O'Connor K, Pelletier J, Boukhalfi T, Renaud P, Dumais A. Virtual reality therapy for refractory auditory verbal hallucinations in schizophrenia: a pilot clinical trial. Schizophr Res. 2018 Feb 24; doi: 10.1016/j.schres.2018.02.031. [DOI] [PubMed] [Google Scholar]
- 97.Pot-Kolder RMCA, Geraets CNW, Veling W, van Beilen M, Staring ABP, Gijsman HJ, Delespaul PAEG, van der Gaag M. Virtual-reality-based cognitive behavioural therapy versus waiting list control for paranoid ideation and social avoidance in patients with psychotic disorders: a single-blind randomised controlled trial. Lancet Psychiatry. 2018 Dec;5(3):217–226. doi: 10.1016/S2215-0366(18)30053-1. [DOI] [PubMed] [Google Scholar]
- 98.Rus-Calafell M, Garety P, Sason E, Craig TJK, Valmaggia LR. Virtual reality in the assessment and treatment of psychosis: a systematic review of its utility, acceptability and effectiveness. Psychol Med. 2018 Feb;48(3):362–391. doi: 10.1017/S0033291717001945. [DOI] [PubMed] [Google Scholar]
- 99.Valmaggia LR, Freeman D, Green C, Garety P, Swapp D, Antley A, Prescott C, Fowler D, Kuipers E, Bebbington P, Slater M, Broome M, McGuire PK. Virtual reality and paranoid ideations in people with an 'at-risk mental state' for psychosis. Br J Psychiatry Suppl. 2007 Dec;51:s63–S68. doi: 10.1192/bjp.191.51.s63. [DOI] [PubMed] [Google Scholar]
- 100.Valmaggia LR, Day FL, Kroll J, Laing J, Byrne M, Fusar-Poli P, McGuire P. Bullying victimisation and paranoid ideation in people at ultra high risk for psychosis. Schizophr Res. 2015 Oct;168(1-2):68–73. doi: 10.1016/j.schres.2015.08.029. [DOI] [PubMed] [Google Scholar]
- 101.Valmaggia LR, Day F, Garety P, Freeman D, Antley A, Slater M, Swapp D, Myin-Germeys I, McGuire P. Social defeat predicts paranoid appraisals in people at high risk for psychosis. Schizophr Res. 2015 Oct;168(1-2):16–22. doi: 10.1016/j.schres.2015.07.050. [DOI] [PubMed] [Google Scholar]
- 102.Shaikh M, Ellett L, Dutt A, Day F, Laing J, Kroll J, Petrella S, McGuire P, Valmaggia LR. Perceived ethnic discrimination and persecutory paranoia in individuals at ultra-high risk for psychosis. Psychiatry Res. 2016 Jul 30;241:309–314. doi: 10.1016/j.psychres.2016.05.006. [DOI] [PubMed] [Google Scholar]
- 103.Geraets CNW, van Beilen M, Pot-Kolder R, Counotte J, van der Gaag M, Veling W. Social environments and interpersonal distance regulation in psychosis: a virtual reality study. Schizophr Res. 2018 Dec;192:96–101. doi: 10.1016/j.schres.2017.04.034. [DOI] [PubMed] [Google Scholar]
- 104.Veling W, Pot-Kolder R, Counotte J, van Os J, van der Gaag M. Environmental social stress, paranoia and psychosis liability: a virtual reality study. Schizophr Bull. 2016 Dec;42(6):1363–1371. doi: 10.1093/schbul/sbw031. http://europepmc.org/abstract/MED/27038469. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy and inclusion criteria.