

Abstract
Background
Skeletal muscle atrophy commonly occurs in critically ill patients, and decreased muscle mass is associated with worse clinical outcomes. Muscle mass can be assessed using various tools, including ultrasound and bioelectrical impedance analysis (BIA). However, the effectiveness of muscle mass monitoring is unclear in critically ill patients. This study was conducted to compare ultrasound and BIA for the monitoring of muscle mass in critically ill patients.
Methods
We recruited adult patients who were expected to undergo mechanical ventilation for > 48 h and to remain in the intensive care unit (ICU) for > 5 days. On days 1, 3, 5, 7, and 10, muscle mass was evaluated using an ultrasound and two BIA devices (Bioscan: Malton International, England; Physion: Nippon Shooter, Japan). The influence of fluid balance was also evaluated between each measurement day.
Results
We analyzed 93 images in 21 patients. The age of the patients was 69 (interquartile range, IQR, 59–74) years, with 16 men and 5 women. The length of ICU stay was 11 days (IQR, 9–25 days). The muscle mass, monitored by ultrasound, decreased progressively by 9.2% (95% confidence interval (CI), 5.9–12.5%), 12.7% (95% CI, 9.3–16.1%), 18.2% (95% CI, 14.7–21.6%), and 21.8% (95% CI, 17.9–25.7%) on days 3, 5, 7, and 10 (p < 0.01), respectively, with no influence of fluid balance (r = 0.04, p = 0.74). The muscle mass did not decrease significantly in both the BIA devices (Bioscan, p = 0.14; Physion, p = 0.60), and an influence of fluid balance was observed (Bioscan, r = 0.37, p < 0.01; Physion, r = 0.51, p < 0.01). The muscle mass assessment at one point between ultrasound and BIA was moderately correlated (Bioscan, r = 0.51, p < 0.01; Physion, r = 0.37, p < 0.01), but the change of muscle mass in the same patient did not correlate between these two devices (Bioscan, r = − 0.05, p = 0.69; Physion, r = 0.23, p = 0.07).
Conclusions
Ultrasound is suitable for sequential monitoring of muscle atrophy in critically ill patients. Monitoring by BIA should be carefully interpreted owing to the influence of fluid change.
Trial registration
UMIN000031316. Retrospectively registered on 15 February 2018.
Keywords: Muscle mass, Ultrasound, Bioelectrical impedance analysis, Fluid balance, Critically ill patients
Introduction
Skeletal muscle atrophy commonly occurs in critically ill patients. The muscles of critically ill patients can rapidly atrophy after admission in the intensive care unit (ICU). During intensive care, a noticeable reduction in muscle mass, starts within 3 days and progressively worsens thereafter [1]. Our previous report suggested that the upper- and lower-limb muscle mass of intensive care patients decrease by 13–21% within 7 days of admission [2]. Moreover, decreased muscle mass is associated with prolonged weaning from mechanical ventilation and length of ICU stay, as well as higher mortality [3].
Although monitoring of muscle mass is important, identification of an optimal method of estimating muscle mass remains difficult. There are many methods that can estimate muscle mass. In recent years, the use of ultrasound and bioelectrical impedance analysis (BIA) has become more widely accepted in the ICU [4]. A recent study by Kim et al. reported that BIA could be used for whole-body muscle mass assessment at one point in critically ill patients [5]. However, sequential muscle mass monitoring capability of BIA in the same critically ill patients, not muscle mass assessment at one point, has not been investigated. Patients in the ICU are generally under abnormal fluid status. Because BIA indirectly estimates muscle mass using electrical resistance, and the resistance is affected by fluid status, the hypothesis that BIA could not accurately monitor the change of muscle mass in critically ill patients is reasonable.
This study aimed to compare the use of ultrasound and BIA for muscle mass monitoring in critically ill patients. The influence of fluid shift was also analyzed because edema may complicate these measurements and few studies cleared the complication. In addition, muscle mass was retrospectively evaluated using computed tomography (CT) to compare with previous studies.
Materials and methods
Study design and setting
We conducted a prospective observational single-center study at the mixed medical/surgical ICU of Tokushima University Hospital from May 2016 to May 2017. This study was approved by the clinical research ethics committee at Tokushima University Hospital (approval number 2593). At enrollment, written informed consent was obtained from patients or from an authorized surrogate.
Study population
We consecutively recruited adult patients who were expected to require mechanical ventilation for > 48 h and to remain in the ICU for > 5 days. The patients were prospectively recruited within 24 h of ICU admission. We excluded patients who fell under one or more of the following categories: age younger than 18 years; pregnant; exhibiting trauma to or amputation of upper or lower limbs; diagnosed with primary neuromuscular disease; embedded electronic devices, such as a pacemaker or implanted cardiac defibrillator because the current from BIA could affect the device activity.
Ultrasonographic measurement
For sonography, we used a HI VISION Preirus with B-mode imaging, which was connected to a 6.5 MHz 3.8-cm linear transducer (EUP-L73S Features; both Hitachi Medical Corporation, Tokyo, Japan). All scanning was performed with patients in the supine position and elbows and knees in passive extension. Generous amounts of contact gel were applied to avoid compression of the muscles by the transducer. The transducer was placed perpendicular relative to the long axis of the limbs. The sum of biceps brachii and rectus femoris cross-sectional area was used for the comparison because of the improved whole-body muscle mass assessment with the sum of the upper and lower limb [6]. The cross-sectional area at the dominant limb was evaluated on days 1, 3, 5, 7, and 10 (Additional file 1: Figs. S1, S2). The subcutaneous tissue thickness was also evaluated for the assessment of edema (Additional file 1: Fig. S2). The sum of subcutaneous tissue thickness at the biceps brachii and rectus femoris muscles was used for the assessment. Before commencing the study, the intra- and inter-observer reproducibilities were 0.93–0.99 and 0.93–0.98, and 0.83–0.99 and 0.90–0.99 for the muscle and subcutaneous tissue, respectively, as assessed by two ICU physicians (Additional file 1: Table S1). Therefore, each measurement was performed by the same investigator. The investigator performing measurements was not blinded to patients’ condition, but image analyses were blinded by concealing patients’ name and measurement days.
Bioelectrical impedance analysis
BIA is a noninvasive tool that measures impedance by sending a weak electric current through the body. BIA indirectly estimates body composition, including fat, water, bone mass, lean body mass, and muscle. BIA was used on days 1, 3, 5, 7, and 10. Two different BIA devices were used as follows: Bioscan 920-2 (Malton International, Essex, United Kingdom) and Physion MD (Nippon Shooter Ltd., Tokyo, Japan). BIA measurements were also conducted on days 1, 3, 5, 7, and 10, with the patients in the supine position with extended limbs and 30° abduction of the shoulder and hip.
Bioscan 920-2
Bioscan can measure muscle mass by using four to eight electrodes. We used four electrodes for hemi-lateral upper and lower extremities. The electrodes were attached to the dorsum of the wrists and third metacarpi of the hand, and the anterior surface of the ankles and third metacarpi of the foot. Bioscan has multi-frequency measurement (5, 50, 100, and 200 kHz) with low-amplitude current (700 μA). The range of impedance is 2–1200 Ω. The data obtained included total body water, intracellular water, extracellular water, and skeletal muscle mass.
Physion MD
Physion MD can measure site-specific muscle mass, including the upper arms, forearms, thighs, lower legs, and trunk by using a four-limb 12-lead electrode. The measuring frequency and current are 50 kHz and 500 μA, respectively. The range of impedance is 10–1500 Ω. The data obtained included total body water (no data regarding intra- or extracellular water) and skeletal muscle mass.
Computed tomography
We retrospectively evaluated the muscle mass using the transverse plane in CT because previous studies have compared the muscle mass assessment between BIA and CT [5, 7]. CT examinations were performed for clinical purpose. Therefore, the examination day is not consistent among included patients. The muscle mass at the L3 spine level correlates well with whole-body muscle mass. Therefore, the muscle mass area at L3 was measured by outlining the muscle area using Image J software (National Institutes of Health, Bethesda, MD, USA, Additional file 1: Fig. S3).
Fluid balance
Fluid balance was evaluated during ICU stay because the fluid status may interfere with the assessment of muscle mass. Fluid intake included intravenous fluids, total parenteral and enteral nutrition, blood products, and intravenous medications. Fluid output included urine, excrement, blood loss, output from drains and other body cavities, and gastric aspirate. Other fluid losses, such as sweat and respiratory evaporation, were excluded. We used fluid balance from a measurement day to the day before the next measurement. We compared the fluid balance with the change of measured variables in the same intervals. Additionally, the change of balance was analyzed from the admission to each measurement days. Fluid balance was classified into interval fluid balance between each measurement day or accumulated fluid balance from day 1 to measurement days (Additional file 1: Fig. S4).
Outcomes
The primary outcome was the time course of muscle atrophy, evaluated using ultrasound and two BIA devices. To assess the changes in muscle mass, we calculated the atrophy rate, defined as the percent variation of muscle mass as compared with values on day 1.
The secondary outcome was a comparison of muscle mass assessment between ultrasound and BIA. We analyzed the muscle mass assessment at one point and subsequent muscle mass change from day 1 to each study day. Then, we retrospectively compared these muscle mass assessment methods with CT evaluation in a limited number of patients. Finally, we evaluated the association of these measurement methods and fluid balance.
Statistical analyses
Mixed-effects models for repeated measures (MMRM) was used to assess the changes in muscle mass over time: statistical significance of muscle mass atrophy at each time point was also tested using 95% confidence intervals (CIs), with intervals excluding zero considered to be statistically significant. Data were presented as mean (95% CI). The Pearson correlation coefficient was used to investigate relationships among measured variables. Due to the exploratory research, the sample size was not calculated a priori but determined upon feasible size. Data analyses were conducted using JMP statistical software version 13.1.0 (SAS Institute Inc., Cary, NC, USA). All statistical tests were two-tailed, and the chosen type 1 error rate was p < 0.05.
Results
Twenty-one patients were enrolled, and all patients participated in the study on day 3, 19 patients on day 5, 19 on day 7, and 13 on day 10 (Fig. 1). The age of the patients was 69 (interquartile range, IQR, 59–74) years, and 16 patients were men (patient characteristics are summarized in Table 1). The APACHE II score was 28 (IQR, 23–30). The duration of mechanical ventilation was 7 days (IQR, 5–18 days). The reasons for admission were surgical (29%) and non-surgical (71%).
Fig. 1.
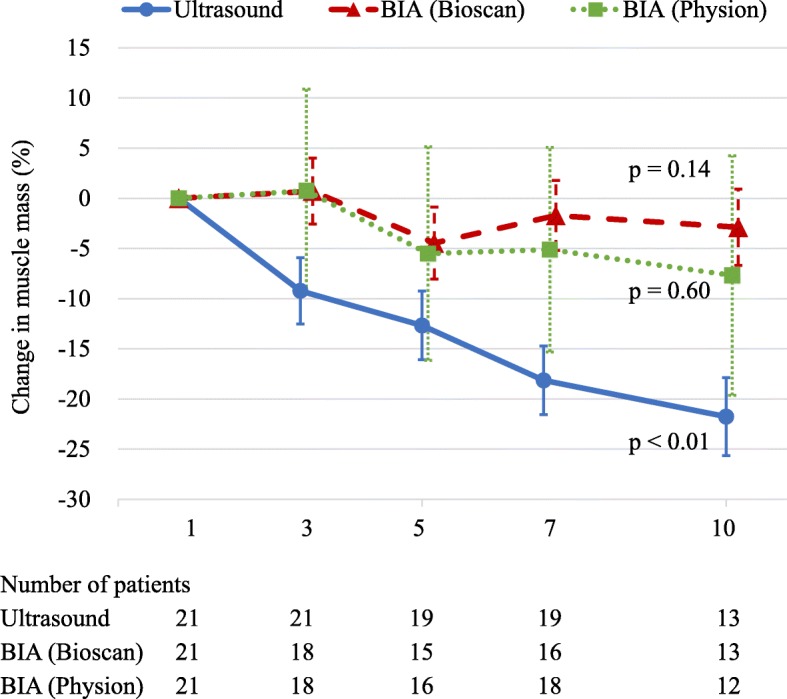
Percentage change in muscle mass, monitored by an ultrasound and two BIAs. Percentage change in muscle mass was calculated in the comparison with the value of day 1. Muscle mass, monitored by an ultrasound, statistically significantly (p < 0.01) decreased, whereas muscle mass, monitored by two BIAs, did not statistically significantly decrease (Bioscan, p = 0.14; Physion, p = 0.60). p values were derived from mixed-effects models for repeated measures. Data are presented as means and 95% confidence intervals. The number of patients daily is displayed below the graph. BIA bioelectrical impedance analysis
Table 1.
Patients’ characteristics (n = 21)
| Variables | Overall |
|---|---|
| Age, years | 69 (59–74) |
| Gender (men), n (%) | 16 (76%) |
| Body mass index, kg/m2 (mean (SD)) | 22.9 ± 3.8 |
| APACHE II score | 28 (23–30) |
| ICU length of stay, days | 11 (9–25) |
| Duration of mechanical ventilation, days | 7 (5–18) |
| Hospital length of stay, days | 43 (26–117) |
| Mortality in the ICU, n (%) | 6 (29%) |
| ICU admission reasons | |
| Surgical, n (%) | 6 (29%) |
| Non-surgical, n (%) | 15 (71%) |
Data were presented as median (IQR) unless otherwise indicated. SD standard deviation, APACHE Acute Physiology and Chronic Health Evaluation, ICU intensive care unit, IQR interquartile range
Percentage changes in muscle mass
We analyzed 93 ultrasound images in 21 patients. The muscle mass decreased progressively by 9.2% (95% CI, 5.9–12.5%), 12.7% (95% CI, 9.3–16.1%), 18.2% (95% CI, 14.7–21.6%), and 21.8% (95% CI, 17.9–25.7%) on days 3, 5, 7, and 10, respectively (p < 0.01; MMRM, Fig. 1). Using Bioscan, 83 tests in 21 patients were analyzed. Ten tests were missing data (7 tests were measurement errors and 3 tests were unable to be performed). The muscle mass had changed by 0.7% (95% CI, − 2.6 to 4.0%), − 4.5% (95% CI, − 8.1 to − 0.9%), − 1.7% (95% CI, − 5.2 to 1.8%), and − 2.9% (95% CI, − 6.7 to 0.9%) on days 3, 5, 7, and 10, respectively (p = 0.14; MMRM). Using Physion, 8 tests were missing data (5 tests were measurement errors and 3 tests were unable to be performed). In 85 measurements, the muscle mass had changed by 0.7% (95% CI, − 9.4% to 10.9%), − 5.5% (95% CI, − 16.2% to 5.1%), − 5.1% (95% CI, − 15.3% to 5.1%), and − 7.7% (95% CI, − 19.6 to 4.3%) on days 3, 5, 7, and 10, respectively (p = 0.60; MMRM).
Relationship between ultrasound and BIA in muscle mass evaluation
In muscle mass assessment at one point, BIA was correlated with ultrasound in some examination days (Bioscan, days 1, 5, 7, and 10; Physion, days 1 and 5, Fig. 2a). In sum, average correlation was r = 0.51, p < 0.01 in Bioscan (n = 83) and r = 0.37, p < 0.01 in Physion (n = 85). In contrast, the percentage change of muscle mass in BIA did not correlate with the findings using ultrasound (Fig. 2b). The average correlation was r = − 0.05, p = 0.69 in Bioscan (n = 62) and r = 0.23, p = 0.07 in Physion (n = 64).
Fig. 2.

Relationship between ultrasound and BIA in muscle mass evaluation. The correlation between ultrasound and two BIAs. a Muscle mass. b Muscle mass change. a Muscle mass was compared at one point in each measurement day. BIA was correlated with ultrasound in some measurement days (Bioscan, days 1, 5, 7, and 10; Physion, days 1 and 5). b Muscle mass change was compared from day 1 to each measurement day. The percentage change of muscle mass in BIA did not correlate with the findings using ultrasound. The correlations were shown under every graph. Pearson correlation coefficient was used to investigate the relationships. BIA bioelectrical impedance analysis
Relationship among ultrasound, BIA, and CT in muscle mass evaluation
We analyzed 17 CT images in 17 patients at day 1 and 8 patients with the subsequent examination (1, 2, 3, 2 patients at days 3, 5, 7, 10). At day 1, ultrasound showed a strong correlation with CT measurement (r = 0.84, p < 0.01, Fig. 3a). BIA was moderately correlated with CT measurement (Bioscan, r = 0.60, p = 0.01; Physion, r = 0.55, p = 0.02). The percentage change of muscle mass in CT correlated only with ultrasound (ultrasound, r = 0.76, p = 0.03; Bioscan, r = − 0.54, p = 0.17; Physion, r = 0.35, p = 0.39, Fig. 3b).
Fig. 3.

Relationship among ultrasound, BIA, and CT in muscle mass evaluation. The correlation among ultrasound, BIA, and CT. a Muscle mass. b Muscle mass change. a Muscle mass was compared in 17 patients at day 1. Both ultrasound and BIA were correlated with CT measurements. b Muscle mass change was compared from day 1 to each measurement day (1, 2, 3, and 2 patients at days 3, 5, 7, and 10). Ultrasound, not BIA, was correlated with CT measurements. The correlations were shown under both graphs. Pearson correlation coefficient was used to investigate the relationships. BIA bioelectrical impedance analysis, CT computed tomography
Relationship against fluid balance
In ultrasound, the percentage change of muscle mass was not correlated with interval fluid balance in the ICU (r = 0.04, p = 0.74), whereas subcutaneous tissue was correlated with interval fluid balance (r = 0.38, p < 0.01, Table 2, Additional file 1: Fig. S5). The measurements of BIA and body weight change were positively correlated with interval fluid balance (r = 0.34–0.57, p < 0.01). In accumulated fluid balance, fluid shift and body weight were also correlated (r = 0.29–0.57, p ≦ 0.02, Additional file 1: Fig. S6). In ultrasound, the change of muscle mass was not correlated with accumulated fluid balance in the ICU (r = 0.16, p = 0.18), and subcutaneous tissue was also not correlated with accumulated fluid balance (r = 0.20, p = 0.09). Furthermore, the muscle mass assessment of Bioscan was not correlated with accumulated fluid balance, (r = 0.15, p = 0.25), although it was correlated at day 3 (r = 0.69, p < 0.01).
Table 2.
Relationship against fluid balance (interval and accumulated)
| Percentage change (%) | Interval | Accumulated | ||||
|---|---|---|---|---|---|---|
| n | r | p value | n | r | p value | |
| Muscle mass | ||||||
| Ultrasound | 72 | 0.04 | 0.74 | 72 | 0.16 | 0.18 |
| BIA (Bioscan) | 55 | 0.37 | < 0.01 | 62 | 0.15 | 0.25* |
| BIA (Physion) | 60 | 0.51 | < 0.01 | 64 | 0.45 | < 0.01 |
| Subcutaneous tissue by ultrasound | 72 | 0.38 | < 0.01 | 72 | 0.20 | 0.09 |
| Fluid shift measured by BIA (Bioscan) | 55 | 0.56 | < 0.01 | 62 | 0.56 | < 0.01 |
| Extracellular water | 55 | 0.55 | < 0.01 | 62 | 0.57 | < 0.01 |
| Intracellular water | 55 | 0.47 | < 0.01 | 62 | 0.29 | 0.02 |
| Fluid shift measured by BIA (Physion) | 60 | 0.34 | < 0.01 | 64 | 0.34 | < 0.01 |
| Body weight | 67 | 0.57 | < 0.01 | 65 | 0.43 | < 0.01 |
Interval: all variables are the changes (%) between each measurement day. Accumulated: all variables are the changes (%) from day 1 to measurement days. The Pearson correlation coefficient was used to investigate the relationships. BIA bioelectrical impedance analysis
*The correlation of Bioscan was significant only at day 3 (r = 0.69, p < 0.01 at day 3, r = − 0.06, p = 0.83 at day 5, r = 0.18, p = 0.51 at day 7, r = − 0.12, p = 0.71 at day 10)
Discussion
In this observational study, we found muscle mass monitoring by BIA was complicated by the fluid shift and could not monitor the change of muscle mass in critically ill patients, although muscle mass assessment at one point moderately correlated with ultrasound and CT. In contrast, the use of ultrasound monitored progressive muscle atrophy over the ICU stay without the influence of fluid shift. To our knowledge, this is the first study to investigate muscle mass monitoring capacity by BIA and ultrasound with the assessment of fluid balance.
In our study, the reference standard of muscle mass evaluation was based on ultrasound. The accuracy of muscle mass evaluation by ultrasound has been established in many researches [1, 8]. In this study, days over ICU stay resulted in an atrophy rate similar to the one previously reported (21.8% on day 10 in our study vs. 17.7% in Puthucheary’s study, and vs. 29.9% in Parry’s study) [1, 8]. Furthermore, we found that muscle mass assessment by ultrasound was strongly correlated with CT (r = 0.76–0.84, p ≤ 0.03). Because CT can separate muscle, fat, and other tissues, CT is considered as an accurate and precise method for muscle mass assessment [9]. Therefore, the value of ultrasound assessment is reliable.
In a previous study, Kim et al. found that muscle mass assessment by using BIA correlated with CT assessment (n = 135, r = 0.58–0.73, p < 0.0001), suggesting that BIA can be used for muscle mass assessment of critically ill patients [5]. Another previous study by Kuchnia et al. reported that phase angle and impedance ratio measured by BIA correlated with muscle mass in CT (n = 71, r = 0.67–0.78, p < 0.05) [7]. Consistent with these findings, muscle mass assessment by BIA was moderately correlated at one point in our study. However, no study investigated the usefulness of BIA for the muscle mass monitoring in the same critically ill patients. Hosono et al. successfully used BIA for follow-up measurements of muscle mass with rheumatologic patients [10], but its use in critically ill patients is still unknown because patients in the ICU are exposed to abnormal fluid status. In the edematous condition, the use of BIA for muscle mass monitoring may overestimate the muscle mass in critically ill patients. In a previous study by Kim et al., BIA measurement was complicated by edema and overestimated muscle mass in critically ill patients. Extracellular-to-total body water (ECW/TBW) is often used for the assessment of edema with the cutoff value of 0.40 [11]. In this study, the median extracellular-to-total body water (ECW/TBW) was 0.48 (IQR, 0.46–0.51). Similarly, in previous reports, most critically ill patients had increased amount of extracellular fluid [5, 11]. Therefore, the results of BIA for muscle mass monitoring should be carefully interpreted in critically ill patients.
However, the estimation of muscle mass may differ among BIA devices [12]. In this two-device comparison study, Physion was possibly more influenced by fluid balance because it had greater CI (Fig. 1) and higher correlation with fluid balance than Bioscan (Physion, r = 0.45–0.51; Bioscan, r = 0.15–0.37). In Bioscan, the muscle mass assessment was not influenced by accumulated fluid balance at the later stage in the ICU. We cannot conclude our results can be applied to all the BIA devices because Inbody S10 (InBody Corp, South Korea) or MF-BIA QuadScan 4000 (Bodystas LTD, United Kingdom) were used in previous studies [5, 7].
Edema is also of concern for the muscle mass evaluation by ultrasound. Intramuscular edema may complicate muscle mass evaluation. In our study, the interval fluid balance affected subcutaneous thickness and did not affect the muscle mass significantly, implying that the increased amount of water may increase extracellular water and accumulate in the subcutaneous tissue. Cartwright’s study, the thickness of subcutaneous tissue increased over the ICU stay, and the results indicated that the ultrasound of the subcutaneous tissue may detect edema in ICU patients [13]. Similarly, Campbell found muscle thickness correlated with fat-free mass in edematous patients, and speculated that most fluid was not retained in the body of muscle [14]. In our research, subcutaneous thickness was associated with interval fluid balance, not accumulated fluid balance. In prolonged ICU stay, subcutaneous tissue thickness is influenced by the change of adipose tissue and muscle mass. Therefore, interval fluid balance was more sensible to the change of edema. Although the influence of edema needs further investigation, our results indicate that ultrasound is suitable for the muscle mass monitoring in edematous critically ill patients.
There are advantages and limitations among measurement methods. CT, MRI, and dual-energy X-ray absorptiometry may be more accurate in evaluating muscle mass, but critically ill patients need to be transferred to the examination room with some risks to perform these methods. In contrast, ultrasound and BIA can be used noninvasively at the bedside. Because BIA does not need measurement skills and can easily be used by any operator, it is clinically useful if we can apply the device for muscle mass monitoring. However, the result of this study was contrary to the use for monitoring. We may need to clarify some formula to use BIA in critically ill patients because muscle mass estimation was derived from healthy volunteers in most BIAs [15]. Conclusively, in our research, ultrasound was more useful for muscle mass monitoring in the ICU although it will need measurement skill for accurate measurements. Acquisition of ultrasound measurement skill may be necessary for muscle mass monitoring for better nutritional and metabolic support during critical illness.
Our findings suggest that it is worthwhile to use ultrasound for muscle mass monitoring. Although BIA may be useful to assess muscle mass at one point, the results of BIA for muscle mass monitoring should be carefully interpreted in critically ill patients. To improve nutritional support and rehabilitation, further evidence is needed for the monitoring of muscle mass in critically ill patients.
Limitations
Our study has several limitations. First, the study has a small sample size in a single center. Particularly, the number of CT scan was limited due to the retrospective nature to avoid extra radiation exposure; consequently, our observations need to be validated by study of a larger population. Second, some data on BIA measurement were missing mostly due to the measurement error, whereas ultrasound measurement did not have missing data.
Conclusions
We evaluated muscle mass monitoring methods in critically ill patients and found that ultrasound is suitable for sequential monitoring of muscle atrophy. Monitoring by BIA should be carefully interpreted due to the fluid change.
Supplementary information
Additional file 1: Table S1. Reproducibility of measurements. Figure S1. Ultrasound sites for the upper and lower limbs. (a) Biceps brachii muscle was measured at two-thirds of the way between the acromion and the antecubital crease. (b) Rectus femoris muscle was measured at midway between the anterior superior iliac spine and the proximal end of the patella. Figure S2. Ultrasound image of muscle and subcutaneous tissue. (a) The cross-sectional area of biceps brachii was measured by outlining the muscle area shown in the transverse plane. (b) The cross-sectional area of rectus femoris was measured by outlining the muscle area shown in the transverse plane. (c) Subcutaneous tissue thickness of biceps brachii was defined as depth between the skin and the superficial fascia of the biceps brachii muscle. (d) Subcutaneous tissue thickness of rectus femoris was defined as depth between the skin and the superficial fascia of the rectus femoris muscle. Figure S3. CT image of muscle. Muscle mass area was evaluated from computed tomography at the L3 spine level by using image J software (National Institutes of health, Bethesda, MD, USA). Figure S4. Fluid balance calculation. The upper side depicts interval fluid balance between measurement days. On the other hand, the lower side depicts accumulated fluid balance from day 1 to measurement days. Figure S5. Relationship between measurements and interval fluid balance. Interval fluid balance was compared with variable measurements between each measurement day. Figure S6. Relationship between measurements and accumulated fluid balance. Accumulated fluid balance was compared with variable measurements from day 1 to measurement days.
Acknowledgements
Not applicable.
Abbreviations
- APACHE II
Acute physiology and chronic health evaluation II
- BIA
Bioelectrical impedance analysis
- CI
Confidence interval
- CT
Computed tomography
- ECW
Extracellular water
- ICU
Intensive care unit
- IQR
Interquartile range
- MMRM
Mixed-effects models for repeated measures
- MRI
Magnetic resonance imaging
- TBW
Total body water
Authors’ contributions
NN was involved in study design, analysis and interpretation of the data, and drafting of the manuscript. TR took part in study design, acquisition of the data, and analysis. OY provided statistical advice on study design and analyzed the data. TT and UY were involved in acquisition of the data. IT did analyze and interpreted the data. TY took part in study design and drafting of the manuscript. SH took part in the concept and interpretation of the data. OJ took part in study design, analysis, and drafting of the manuscript. All authors read and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Ethics approval was obtained from the clinical research ethics committee at Tokushima University Hospital (approval number 2593). Informed consent to participate in the study was also obtained from patients or from an authorized surrogate.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Nobuto Nakanishi, Email: nakanishi.nobuto@tokushima-u.ac.jp.
Rie Tsutsumi, Email: rtsutsumi@tokushima-u.ac.jp.
Yoshihiro Okayama, Email: y-okayama@tokushima-u.ac.jp.
Takuya Takashima, Email: t.takashima0405@gmail.com.
Yoshitoyo Ueno, Email: ueno.yoshitoyo@tokushima-u.ac.jp.
Taiga Itagaki, Email: taiga@tokushima-u.ac.jp.
Yasuo Tsutsumi, Email: tsutsumi@tokushima-u.ac.jp.
Hiroshi Sakaue, Email: hsakaue@tokushima-u.ac.jp.
Jun Oto, Email: joto@tokushima-u.ac.jp.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s40560-019-0416-y.
References
- 1.Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, Hopkinson NS, Phadke R, Dew T, Sidhu PS, et al. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310(15):1591–1600. doi: 10.1001/jama.2013.278481. [DOI] [PubMed] [Google Scholar]
- 2.Nakanishi N, Oto J, Tsutsumi R, Iuchi M, Onodera M, Nishimura M. Upper and lower limb muscle atrophy in critically ill patients: an observational ultrasonography study. Intensive Care Med. 2018;44(2):263–264. doi: 10.1007/s00134-017-4975-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Weijs PJ, Looijaard WG, Dekker IM, Stapel SN, Girbes AR, Oudemans-van Straaten HM, Beishuizen A. Low skeletal muscle area is a risk factor for mortality in mechanically ventilated critically ill patients. Crit Care. 2014;18(2):R12. doi: 10.1186/cc13189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Looijaard W, Molinger J, Weijs PJM. Measuring and monitoring lean body mass in critical illness. Curr Opin Crit Care. 2018;24(4):241–247. doi: 10.1097/MCC.0000000000000511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim Dongha, Sun Joo Sung, Lee Yeon Hee, Lee Ji Hyun, Hong Jeong, Lee Jae-Myeong. Comparative assessment of skeletal muscle mass using computerized tomography and bioelectrical impedance analysis in critically ill patients. Clinical Nutrition. 2019;38(6):2747–2755. doi: 10.1016/j.clnu.2018.12.002. [DOI] [PubMed] [Google Scholar]
- 6.Paris MT, Lafleur B, Dubin JA, Mourtzakis M. Development of a bedside viable ultrasound protocol to quantify appendicular lean tissue mass. J Cachexia Sarcopenia Muscle. 2017;8(5):713–726. doi: 10.1002/jcsm.12213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kuchnia A, Earthman C, Teigen L, Cole A, Mourtzakis M, Paris M, Looijaard W, Weijs P, Oudemans-van Straaten H, Beilman G, et al. Evaluation of bioelectrical impedance analysis in critically ill patients: results of a multicenter prospective study. JPEN J Parenter Enteral Nutr. 2017;41(7):1131–1138. doi: 10.1177/0148607116651063. [DOI] [PubMed] [Google Scholar]
- 8.Parry SM, El-Ansary D, Cartwright MS, Sarwal A, Berney S, Koopman R, Annoni R, Puthucheary Z, Gordon IR, Morris PE, et al. Ultrasonography in the intensive care setting can be used to detect changes in the quality and quantity of muscle and is related to muscle strength and function. J Crit Care. 2015;30(5):1151. doi: 10.1016/j.jcrc.2015.05.024. [DOI] [PubMed] [Google Scholar]
- 9.Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi: 10.1093/ageing/afq034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hosono O, Yoshikawa N, Shimizu N, Kiryu S, Uehara M, Kobayashi H, Matsumiya R, Kuribara A, Maruyama T, Tanaka H. Quantitative analysis of skeletal muscle mass in patients with rheumatic diseases under glucocorticoid therapy—comparison among bioelectrical impedance analysis, computed tomography, and magnetic resonance imaging. Mod Rheumatol. 2015;25(2):257–263. doi: 10.3109/14397595.2014.935078. [DOI] [PubMed] [Google Scholar]
- 11.Malbrain ML, Huygh J, Dabrowski W, De Waele JJ, Staelens A, Wauters J. The use of bio-electrical impedance analysis (BIA) to guide fluid management, resuscitation and deresuscitation in critically ill patients: a bench-to-bedside review. Anaesthesiol Intensive Ther. 2014;46(5):381–391. doi: 10.5603/AIT.2014.0061. [DOI] [PubMed] [Google Scholar]
- 12.Wang JG, Zhang Y, Chen HE, Li Y, Cheng XG, Xu L, Guo Z, Zhao XS, Sato T, Cao QY, et al. Comparison of two bioelectrical impedance analysis devices with dual energy X-ray absorptiometry and magnetic resonance imaging in the estimation of body composition. J Strength Cond Res. 2013;27(1):236–243. doi: 10.1519/JSC.0b013e31824f2040. [DOI] [PubMed] [Google Scholar]
- 13.Cartwright MS, Kwayisi G, Griffin LP, Sarwal A, Walker FO, Harris JM, Berry MJ, Chahal PS, Morris PE. Quantitative neuromuscular ultrasound in the intensive care unit. Muscle Nerve. 2013;47(2):255–259. doi: 10.1002/mus.23525. [DOI] [PubMed] [Google Scholar]
- 14.Campbell IT, Watt T, Withers D, England R, Sukumar S, Keegan MA, Faragher B, Martin DF. Muscle thickness, measured with ultrasound, may be an indicator of lean tissue wasting in multiple organ failure in the presence of edema. Am J Clin Nutr. 1995;62(3):533–539. doi: 10.1093/ajcn/62.3.533. [DOI] [PubMed] [Google Scholar]
- 15.Miyatani M, Kanehisa H, Masuo Y, Ito M, Fukunaga T. Validity of estimating limb muscle volume by bioelectrical impedance. J Appl Physiol. 2001;91(1):386–394. doi: 10.1152/jappl.2001.91.1.386. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Table S1. Reproducibility of measurements. Figure S1. Ultrasound sites for the upper and lower limbs. (a) Biceps brachii muscle was measured at two-thirds of the way between the acromion and the antecubital crease. (b) Rectus femoris muscle was measured at midway between the anterior superior iliac spine and the proximal end of the patella. Figure S2. Ultrasound image of muscle and subcutaneous tissue. (a) The cross-sectional area of biceps brachii was measured by outlining the muscle area shown in the transverse plane. (b) The cross-sectional area of rectus femoris was measured by outlining the muscle area shown in the transverse plane. (c) Subcutaneous tissue thickness of biceps brachii was defined as depth between the skin and the superficial fascia of the biceps brachii muscle. (d) Subcutaneous tissue thickness of rectus femoris was defined as depth between the skin and the superficial fascia of the rectus femoris muscle. Figure S3. CT image of muscle. Muscle mass area was evaluated from computed tomography at the L3 spine level by using image J software (National Institutes of health, Bethesda, MD, USA). Figure S4. Fluid balance calculation. The upper side depicts interval fluid balance between measurement days. On the other hand, the lower side depicts accumulated fluid balance from day 1 to measurement days. Figure S5. Relationship between measurements and interval fluid balance. Interval fluid balance was compared with variable measurements between each measurement day. Figure S6. Relationship between measurements and accumulated fluid balance. Accumulated fluid balance was compared with variable measurements from day 1 to measurement days.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.