

Abstract
Aim
To determine development curves of communication and social interaction from childhood into adulthood for individuals with cerebral palsy (CP).
Method
This Pediatric Rehabilitation Research in the Netherlands (PERRIN)‐DECADE study longitudinally assessed 421 individuals with CP, aged from 1 to 20 years at baseline, after 13 years (n=121 at follow‐up). Communication and social interactions were assessed using the Vineland Adaptive Behavior Scales. We estimated the average maximum performance limit (level) and age at which 90% of the limit was reached (age90) using nonlinear mixed‐effects modeling.
Results
One‐hundred individuals without intellectual disability were aged 21 to 34 years at follow‐up (39 females, 61 males) (mean age [SD] 28y 5mo [3y 11mo]). Limits of individuals without intellectual disability, regardless of Gross Motor Function Classification System (GMFCS) level, approached the maximum score and were significantly higher than those of individuals with intellectual disability. Ages90 ranged between 3 and 4 years for receptive communication, 6 and 7 years for expressive communication and interrelationships, 12 and 16 years for written communication, 13 and 16 years for play and leisure, and 14 and 16 years for coping. Twenty‐one individuals with intellectual disability were between 21 and 27 years at follow‐up (8 females, 13 males) (mean age [SD] 24y 7mo [1y 8mo]). Individuals with intellectual disability in GMFCS level V showed the least favourable development, but variation between individuals with intellectual disability was large.
Interpretation
Individuals with CP and without intellectual disability show developmental curves of communication and social interactions similar to typically developing individuals, regardless of their level of motor function. Those with intellectual disability reach lower performance levels and vary largely in individual development.
What this paper adds
Communication and social interactions in individuals with cerebral palsy without intellectual disability develop similarly to typically developing individuals.
Communication and social interactions of individuals with intellectual disability develop less favourably and show large variation.
What this paper adds
Communication and social interactions in individuals with cerebral palsy without intellectual disability develop similarly to typically developing individuals.
Communication and social interactions of individuals with intellectual disability develop less favourably and show large variation.
This article's abstract has been translated into Spanish and Portuguese.
Follow the links from the http://onlinelibrary.wiley.com/doi/10.1111/dmcn.14351/abstract to view the translations.
Resumen
Curvas de desarrollo de comunicación e interacción social en niños con parálisis cerebral
Objetivo
Determinar las curvas de desarrollo de la comunicación y la interacción social desde la infancia hasta la edad adulta para las personas con parálisis cerebral (PC).
Método
Esta Investigación de Rehabilitación Pediátrica en el Estudio de los Países Bajos (PERRIN)‐DECADE evaluó longitudinalmente 421 individuos con PC, de 1 a 20 años en el inicio, después de 13 años (n=121 en el seguimiento). La comunicación y las interacciones sociales se evaluaron utilizando la Escala de comportamiento adaptativo de Vineland. Estimamos el límite promedio de rendimiento máximo (nivel) y la edad a la que se alcanzó el 90% del límite (edad90) utilizando un modelo no lineal de efectos mixtos.
Resultados
Cien individuos sin discapacidad intelectual tenían entre 21 y 34 años en el seguimiento (39 mujeres, 61 varones; edad media [DS] 28 y 5 meses [3 años y 11meses]). Los límites de las personas sin discapacidad intelectual, independientemente del nivel del Sistema de Clasificación de la Función Motora Gruesa (GMFCS), se acercaron a la puntuación máxima y fueron significativamente superiores a los de personas con discapacidad intelectual. Edad 90s entre 3 y 4 años para la comunicación receptiva, 6 y 7 años para la comunicación expresiva y las interrelaciones, 12 y 16 años para la comunicación escrita, 13 y 16 años por juego y ocio, y 14 y 16 años por sobrellevarlo. Veintiún individuos con discapacidad intelectual tenían entre 21 y 27 años en seguimiento (8 mujeres, 13 hombres; edad media [DS] 24 años y 7 meses [1 año y 8 meses]). Las personas con discapacidad intelectual en el nivel V de GMFCS mostraron el desarrollo menos favorable, pero la variación entre las personas con discapacidad intelectual fue grande.
Interpretación
Las personas con PC sin discapacidad intelectual muestran curvas de desarrollo de comunicación e interacciones sociales similares a las personas con desarrollo típico, no considerando su nivel de función motora. Las personas con PC y discapacidad intelectual alcanzan niveles de rendimiento más bajos y varían en gran medida en el desarrollo individual.
Resumo
Curvas de desenvolvimento da comunicação e interação social em crianças com paralisia cerebral
Objetivo
Determinar as curvas de desenvolvimento e interação social da infância para a adolescência para indivíduos com paralisia cerebral (PC).
Método
Este estudo Europeu de Reabilitação Pediátrica na Holanda (PERRIN)‐DECADE avaliou longitudinalmente 421 indivíduos com PC, com idades de 1 a 20 anos na linha de base, após 13 anos, (n=121 no acompanhamento). A comunicação e interação social foram avaliadas usando as Escalas Vineland de Compartamento Adaptativo. Estimamos o limite máximo de desempenho médio (nível) e idade em que 90% do limite foi atingido (idade90) usando modelos não‐lineares de efeitos mistos.
Resultados
Cem indivíduos sem deficiência intelectual com idades entre 21 e 34 anos no acompanhamento (39 do sexo feminino, 61 do sexo masculino; média de idade [DP] 28a 5m [3a 11m]). Os limites de indivíuduos sem deficiência intelectual, independente do nível do Sistema de Classificação da Função Motora Grossa (GMFCS), se aproximou da pontuação maxima e foram significativamente maiores do que os valores de indivíduos com deficiência intelectual. A idade 90s variou entre 3 e 4 anos para comunicação receptiva, 6 e 7 anos para comunicação expressiva e intercomunicações, 12 e 16 anos para comunicação escrita, 12 e 16 years para brincadeiras e lazer, e 14 e 16 anos para adaptabilidade. Vinte e um indivíduos com deficiência intelectual estavam entre 21 e 27 anos no acompanhamento (8 do sexo feminino, 13 do sexo masculino; média de idade [DP] 24a 7m [1a 8m]). Indivíduos com deficiência intelectual no nível GMFCS V mostraram o desenvolvimento menos favorável, mas a variação entre indivíduos com deficiência intelectual foi grande.
Interpretação
Indivíduos com PC com e sem deficiência intelectual mostram curvas desenvolvimentais de comunicação e interação social similares a indivíduos com desempenho típico, independente do nível de função motora. Aqueles com deficiência intelectual tiveram menores níveis de performance e variaram amplamente no desenvolvimento individual.
Abbreviations
- PERRIN
Pediatric Rehabilitation Research in the Netherlands
- VABS
Vineland Adaptive Behavior Scales
The majority of children with cerebral palsy (CP) currently approach the life expectancy of the general population.1 Clinical and research interest now focuses on understanding activity and participation outcomes. Children socially interact with their family, peers, and others which contributes to their development towards optimal participation in adult roles. Receptive and expressive communication are considered essential for these social interactions. Communication difficulties are associated with problems in social interaction with familiar partners.2, 3
The Pediatric Rehabilitation Research in the Netherlands (PERRIN) programme was set up to study the longitudinal development of activities and participation of individuals with CP.4, 5, 6, 7 Development of communication was described by the type of CP and social interactions by Gross Motor Function Classification System (GMFCS) level in a Dutch population of 421 individuals with CP aged 1 to 24 years.8, 9 Individuals without intellectual disability eventually reached similar levels of communication and social interactions as typically developing individuals. The development of individuals with intellectual disability was studied up to age 16 years and was found to be less favorable than that of individuals without intellectual disability. Communication curves were less favorable for individuals with bilateral spastic CP or non‐spastic CP compared with individuals with unilateral spastic CP.9 Social interaction curves were less favorable for individuals in GMFCS level V compared with those in GMFCS levels I to IV.8
To better inform young individuals with CP and their families regarding their future functioning, the results of the PERRIN study could be improved in some respects. In line with other studies that relate communication to GMFCS level,10, 11 the long‐term development of communication may also be determined by GMFCS level. In addition, our knowledge may gain clinical relevance by addressing aspects of social interaction in more detail. Furthermore, it is not yet known at what age the maximal performance of communication and social interaction is reached. Motor development curves are widely used to monitor and predict the future gross motor capacity of individuals with CP.12, 13 These gross motor curves were established using a nonlinear mixed‐effects model, assuming a rapid development at first that slows towards a (stable) limit. This model has also been used to estimate development curves for gross and fine motor skills, daily activity performance, mobility, and self‐care capability in individuals with CP.14, 15 Using this model in the present study allowed us to compare the long‐term development in communication and social interactions with those of other outcomes.
Following up part of the PERRIN population 13 years after the first measurement provided the unique opportunity to: (1) estimate the maximal performance and rate of development of communication and social interactions more accurately; and (2) provide insight into the development of communication and social interactions in individuals without intellectual disability beyond the age of 24 years, and in individuals with intellectual disability beyond the age of 16 years. Thus, the present study aimed to determine the development curves of communication and social interactions into adulthood in a Dutch population of individuals with CP aged between 1 and 34 years. Based on the previous results for a smaller age range and the recent publication on other domains, we hypothesized that the development curves of individuals with CP without intellectual disability would reach similar limits to those of the reference population, but that development would be delayed.8, 9, 14 Furthermore, we hypothesized that the limits of development of individuals with intellectual disability would be less favourable compared with those of individuals without intellectual disability.
Method
This study was performed as part of the Dutch PERRIN‐DECADE study, for which the participants of the two oldest cohorts of the PERRIN programme have been followed for up to 13 years after their last measurement. The recruitment process of the PERRIN programme has been described in detail elsewhere.4, 7 Briefly, the programme longitudinally measured 421 participants over 3 or 4 years between 2000 and 2007 in four age cohorts: PERRIN 0 to 5 years, PERRIN 5 to 9 years, PERRIN 9 to 16 years, and PERRIN 16 to 24 years. Individuals were invited when they had a confirmed diagnosis of CP. Individuals were excluded if they were diagnosed with additional disorders affecting motor function or where they or their caregiver lacked basic knowledge of the Dutch language. In the PERRIN 16 to 24 years cohort, individuals with intellectual disability (IQ<70) were also excluded.4 Written informed consent was obtained from each participant (or their parent or caregiver, in the case of participants with intellectual disability) and ethical approval was granted from the medical ethics committees of the Amsterdam UMC (Amsterdam) and the Erasmus MC University Medical Center (Rotterdam).
A 13‐year follow‐up assessment of the PERRIN 9 to 16 years and PERRIN 16 to 24 years cohorts was completed in 2016, extending the database with observations of individuals without intellectual disability up to 34 years and individuals with intellectual disability up to 27 years. Figure S1 (online supporting information) shows a flow‐diagram of inclusion of observations in the data analyses and Appendix S1 (online supporting information) shows the number of observations by cohort. A trained researcher conducted face‐to‐face, self‐reported, semi‐structured interviews using the Dutch language version of the Vineland Adaptive Behavior Scales (VABS) survey.16 The interviews took about 30 minutes per individual. For the follow‐up assessment, self‐reported scores were used for individuals without intellectual disability and caregiver‐reported scores for individuals with intellectual disability. The caregiver concerned was the person most closely involved in the daily care of the individual with intellectual disability.
The VABS is a reliable and valid instrument to assess adaptive behaviour of typical development between the ages 0 and 19 years, and is suitable for individuals with and without disabilities.16, 17 The survey comprises four domains, among which are communication and socialization. Activities are listed in developmental order with starting points for particular ages; answers are categorized as 0 (never performed) to 2 (usually or habitually performed). The communication domain describes how an individual uses receptive communication (13 activities; score range 0–26), expressive communication (31; 0–62), and uses and understands written language (23; 0–26). The domain of socialization describes how an individual interacts with others (‘interrelationships’; 28 activities), plays or uses leisure time (‘play and leisure’; 20; 0–40), and demonstrates responsibility and sensitivity to others (‘coping’; 18; 0–36). With respect to ‘interrelationships’, four items regarding ‘dating’ were erroneously skipped in the 9 to 16 years cohort and, therefore, discarded (score range 0–48). In agreement to the VABS guidelines, subdomain scores were considered as ‘missing’ if more than four items within the subdomain were missing.
The PERRIN 0 to 5 years cohort completed the VABS screener covering relevant activities of the survey for this age group.18 Inherent to their age, the screener did not include items on written communication. VABS screener scores were linearly transformed to reflect VABS survey scores. Reference values of typically developing individuals derived in Northwest America17 were compared with our results.
Intellectual disability was defined as IQ less than 70, as assessed by the Snijders‐Oomen Nonverbal Intelligence Test (0–5y cohort) or the Raven's Colored Progressive Matrices (5–9y cohort).19, 20 For the PERRIN 9 to 16 years and 16 to 24 years cohorts, individuals attending special education at a daycare center for children with severe disabilities or school for children with intellectual disability were classified as having intellectual disability.4, 7 The level of gross motor function was assessed using the GMFCS, which addresses five levels of gross motor function: level I (walks without limitations) to level V (transported in a manual wheelchair).21 Type of CP (unilateral spastic, bilateral spastic, or non‐spastic) was classified according to the Surveillance of Cerebral Palsy in Europe guidelines.22 Communication function was assessed using the Communication Function Classification System, which addresses five categories of everyday communication performance: level I (effective sending/receiving with unfamiliar and familiar partners) to level V (seldom effective sending/receiving even with familiar partners).23
Statistical analysis
Descriptive statistics were performed in SPSS software, version 22 (IBM SPSS Statistics, Armonk, NY, USA) and mixed‐effects models were fitted using the ‘nlme’ package in R 3.2.5 (R Foundation for Statistical Computing, Vienna, Austria). Appendix S2 (online supporting information) shows details on the nonlinear model that we used. Development curves for each subdomain of communication and social interactions were determined separately for each GMFCS level (communication, social interactions) and each type of CP (communication). Owing to the low number of observations, observations for individuals without intellectual disability in GMFCS level V were discarded. With this asymptotic regression model, communication and social interaction subdomains were estimated as a function of age, approaching a limit of maximal potential performance with a rapid development rate at first but levelling off towards reaching the limit. The model has two parameters with straightforward clinical interpretations: the rate (speed of development) and limit (average maximal performance level). Random effects were included, accounting for dependency between repeated measurements within the same individual. To enhance interpretation, the rate parameter was transformed to age90, (i.e. the average age at which individuals reached 90% of their limit). The 95% confidence intervals (CIs) around age90 and limit were calculated: if the CIs around ages90 or limits of subgroups did not overlap, differences between these subgroups were statistically significant (p<0.05). From the random variance around the estimated limits for each subdomain of communication and social interactions, 50% ranges around the limits were constructed. The 50% ranges around the limits cover the limits of 50% of the scores of individuals in a subgroup. The residual standard deviation (SD) of the models provide an indication of the model fit, with lower SD referring to a better fit. Since development does not start at birth for all subdomains, a start age of development was chosen based on the best model fit, according to the Akaike information criterion, determined using all observations of the subdomain scores.24
Results
Overall, 421 participants (73% without intellectual disability, 50% GMFCS level I, 48% bilateral spastic CP) contributed to 1428 VABS observations at ages 1 to 34 years. At 13‐year follow‐up, 121 adults with CP participated (47 females, 74 males; mean age [SD] 27y 10mo [3y 11mo]; age range 21–34y). Of those, 69% were classified in Communication Function Classification System level I. One individual without intellectual disability and four individuals with intellectual disability used a communication aid (i.e. communication device, communication cards/images, and/or sign language). Table 1 presents the characteristics of the participants in each cohort. Figure S1 describes dropouts. Dropouts did not significantly differ from non‐dropouts regarding sex or CP characteristics. Figure 1 shows the development curves by GMFCS level. As the curves for individuals in GMFCS levels I to IV were not significantly different and looked very similar, Figure 1 summarizes the four curves into one. Tables 2 and 3 reports the corresponding limits, ages90, and 50% range around the limits. Finally, Appendix S3 (online supporting information) presents raw observations, Appendix S4 (online supporting information) presents parameters of development in communication by type of CP, and Appendix S5 (online supporting information) presents scatter plots by Communication Function Classification System levels for individuals with intellectual disability.
Table 1.
Participant characteristics of study population and for subgroups at 13‐year follow‐up
| PERRIN 0–5y | PERRIN 5–9y | PERRIN 9–16y | PERRIN 16–24y | |||
|---|---|---|---|---|---|---|
| Baseline | Baseline | Baseline | 13y follow‐up | Baseline | 13y follow‐up | |
| Participants (n) | 97 | 116 | 107 | 67 | 101 | 54 |
| Observations (n) | 314 | 328 | 399 | 67 | 260 | 54 |
| Age (y:mo) at baseline or 13y follow‐up, mean (SD) | 1:7 (0:2) | 6:3 (1:0) | 11:2 (1:8) | 24:7 (1:7) | 18:6 (1:6) | 31:8 (1:5) |
| Sex, n (%) | ||||||
| Males | 56 (58) | 76 (65) | 67 (63) | 45 (67) | 60 (59) | 29 (54) |
| Females | 41 (42) | 40 (35) | 40 (37) | 22 (33) | 41 (41) | 25 (46) |
| Intellectual disability, n (%) | ||||||
| No | 50 (52)a | 79 (68)a | 75 (70) | 46 (69) | 101 (100) | 54 (100) |
| Yes | 45 (46) | 35 (30) | 32 (30) | 21 (31) | 0 (0) | 0 (0) |
| Level of gross motor function, n (%) | ||||||
| GMFCS level I | 30 (31) | 56 (48) | 49 (46) | 30 (45) | 74 (73) | 38 (70) |
| GMFCS level II | 13 (13) | 20 (17) | 14 (13) | 7 (10) | 8 (8) | 4 (7) |
| GMFCS level III | 23 (24) | 17 (15) | 13 (12) | 8 (12) | 6 (6) | 4 (7) |
| GMFCS level IV | 21 (22) | 9 (8) | 13 (12) | 9 (13) | 12 (12) | 7 (13) |
| GMFCS level V | 10 (10) | 14 (12) | 18 (17) | 13 (19) | 1 (1) | 1 (2) |
| Type of CP, n (%) | ||||||
| Unilateral spastic CP | 41 (42) | 42 (36) | 37 (35) | 21 (31) | 41 (41) | 21 (39) |
| Bilateral spastic CP | 53 (55) | 56 (48) | 49 (46) | 31 (46) | 47 (47) | 25 (46) |
| Non‐spastic CP | 3 (3) | 18 (16) | 22 (20) | 15 (23) | 13 (12) | 8 (15) |
| Communication function, n (%)b | ||||||
| CFCS level I | – | – | – | 37 (55) | – | 46 (85) |
| CFCS level II | – | – | – | 17 (25) | – | 7 (13) |
| CFCS level III | – | – | – | 9 (13) | – | 1 (2) |
| CFCS level IV | – | – | – | 2 (3) | – | 0 (0) |
| CFCS level V | – | – | – | 2 (3) | – | 0 (0) |
aUnknown in n=2. bCommunication Function Classification System (CFCS) was only available at the 13‐year follow‐up. PERRIN, Pediatric Rehabilitation Research in the Netherlands; GMFCS, Gross Motor Function Classification System; CP, cerebral palsy.
Figure 1.
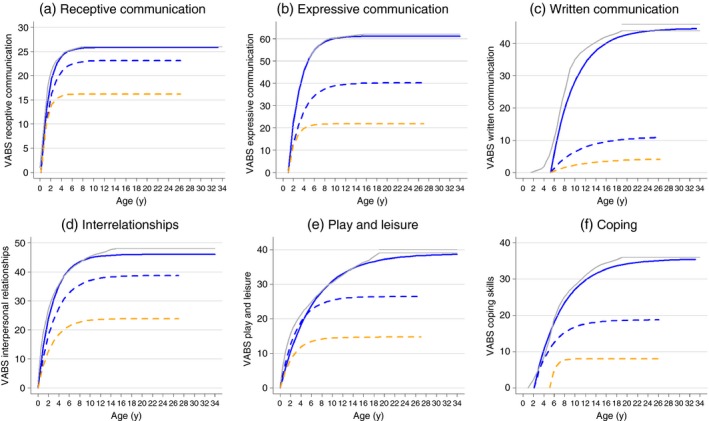
The development curves of communication and social interactions by intellectual disability and Gross Motor Function Classification System (GMFCS) level. VABS, Vineland Adaptive Behavior Scales.
Table 2.
Parameters of development in communication by intellectual disability and Gross Motor Function Classification System (GMFCS) level
| GMFCS level | n | Limit | (95% CI) | 50% range around limit | Age90 (y:mo) | (95% CI) | Residual SDs | Offseta | |
|---|---|---|---|---|---|---|---|---|---|
| Receptive communication | |||||||||
| No intellectual disability | I | 194 | 25.8 | (25.7–25.9) | 25.8 | 3:6 | (3:4–3:7) | 1.1 | 0.2 |
| II | 42 | 25.6 | (25.3–25.9) | 25.1–26.0 | 3:6 | (3:3–3:9) | 0.9 | 0.2 | |
| III | 36 | 25.7 | (25.5–26.0) | 25.7 | 3:3 | (3:0–3:6) | 1.1 | 0.2 | |
| IV | 28 | 25.8 | (25.5–26.0) | 25.8 | 3:5 | (3:2–3:9) | 1.1 | 0.2 | |
| Intellectual disability | I–IV | 72 | 23.1 | (22.1–24.1) | 21.0–25.3 | 4:0 | (3:6–4:7) | 2.2 | 0.2 |
| V | 37 | 16.2 | (13.5–18.9) | 11.0–21.5 | 2:6 | (1:6–4:4) | 3.1 | 0.2 | |
| Expressive communication | |||||||||
| No intellectual disability | I | 193 | 61.1 | (60.6–61.6) | 59.6–62.0 | 6:1 | (5:11–6:3) | 2.2 | 1.0 |
| II | 42 | 61.0 | (59.5–62.4) | 59.2–62.0 | 6:8 | (6:2–7:2) | 3.7 | 1.0 | |
| III | 36 | 60.9 | (59.3–58.7) | 58.7–62.0 | 6:4 | (5:11–6:10) | 2.7 | 1.0 | |
| IV | 28 | 61.1 | (59.3–62.5) | 58.7–62.0 | 7:1 | (6:7–7:7) | 3.3 | 1.0 | |
| Intellectual disability | I–IV | 71 | 40.1 | (34.6–45.7) | 28.6–51.7 | 7:0 | (5:6–9:0) | 5.7 | 1.0 |
| V | 37 | 21.7 | (14.5–28.9) | 7.3–36.1 | 3:10 | (2:6–6:6) | 5.3 | 1.0 | |
| Written communication | |||||||||
| No intellectual disability | I | 166 | 44.7 | (43.6–45.8) | 42.3–46.0 | 16:1 | (15:4–16:10) | 4.4 | 5.3 |
| II | 34 | 41.6 | (37.5–45.6) | 37.0–46.0 | 15:9 | (14:0–17:11) | 4.0 | 5.3 | |
| III | 25 | 40.9 | (35.0–46.7) | 35.0–46.0 | 12:9 | (11:4–14:6) | 4.3 | 5.3 | |
| IV | 20 | 37.2 | (32.9–41.5) | 31.7–42.7 | 15:0 | (13:0–17:6) | 3.7 | 5.3 | |
| Intellectual disability | I–IV | 38 | 11.0 | (6.3–15.8) | 2.5–19.6 | 17:8 | (14:8–21:8) | 2.9 | 5.3 |
| V | 29 | 4.2 | (0.7–7.6) | 0.0–9.9 | 19:2 | (15:0–25:2) | 2.5 | 5.3 | |
Offset refers to the start age of development in years. CI, confidence interval; SD, standard deviation.
Table 3.
Parameters of development in social interactions by intellectual disability and Gross Motor Function Classification System (GMFCS) level
| GMFCS level | n | Limit | (95% CI) | 50% range around limit | Age90 (y:mo) | (95% CI) | Residual SDs | Offseta | |
|---|---|---|---|---|---|---|---|---|---|
| Interrelationships | |||||||||
| No intellectual disability | I | 194 | 46.0 | (45.4–46.6) | 43.9–48.0 | 6:4 | (5:11–6:9) | 2.4 | 0.0 |
| II | 42 | 45.8 | (44.4–47.2) | 44.0–47.6 | 7:6 | (6:9–8:4) | 2.8 | 0.0 | |
| III | 36 | 44.6 | (43.0–46.2) | 42.7–46.6 | 6:3 | (5:7–7:1) | 2.9 | 0.0 | |
| IV | 28 | 46.1 | (44.6–47.5) | 44.1–48.0 | 6:10 | (6:1–7:9) | 2.1 | 0.0 | |
| Intellectual disability | I–IV | 38 | 38.7 | (36.0–41.4) | 35.8–41.7 | 7:4 | (5:4–10:3) | 4.1 | 0.0 |
| V | 29 | 23.9 | (18.7–29.0) | 15.7–32.0 | 6:2 | (2:0–19:2) | 4.7 | 0.0 | |
| Play and leisure | |||||||||
| No intellectual disability | I | 194 | 38.8 | (38.1–39.5) | 37.1–40.0 | 14:6 | (13:10–15:2) | 2.4 | 0.0 |
| II | 42 | 40.3 | (38.7–41.8) | 39.5–40.0 | 16:7 | (15:2–18:3) | 2.8 | 0.0 | |
| III | 36 | 37.7 | (35.6–39.9) | 35.8–39.7 | 13:8 | (12:1–15:4) | 2.4 | 0.0 | |
| IV | 28 | 37.2 | (35.1–39.4) | 35.2–39.3 | 14:0 | (11:11–16:5) | 3.1 | 0.0 | |
| Intellectual disability | I–IV | 38 | 26.5 | (23.2–29.7) | 23.2–29.7 | 10:4 | (7:2–14:10) | 3.7 | 0.0 |
| V | 29 | 14.7 | (10.7–18.7) | 8.4–21.1 | 5:8 | (1:0–32:11) | 4.0 | 0.0 | |
| Coping | |||||||||
| No intellectual disability | I | 192 | 35.6 | (34.5–36.7) | 32.7–38.4 | 14:8 | (13:9–15:9) | 3.5 | 2.1 |
| II | 42 | 36.6 | (34.0–39.2) | 34.3–38.9 | 16:2 | (14:3–18:6) | 3.2 | 2.1 | |
| III | 36 | 34.4 | (30.5–38.3) | 30.9–37.9 | 15:7 | (13:0–18:10) | 3.6 | 2.1 | |
| IV | 28 | 35.1 | (32.6–37.5) | 32.7–37.5 | 14:0 | (11:10–16:8) | 3.6 | 2.1 | |
| Intellectual disability | I–IV | 38 | 18.8 | (14.5–23.0) | 13.6–23.9 | 10:2 | (6:5–17:2) | 5.3 | 2.1 |
| V | 29 | 8.0 | (4.0–12.1) | 0.9–15.1 | 7:1 | (5:2–46:9) | 4.3 | 5.1b | |
aOffset refers to the start age of development in years. bWith respect to coping, the model for individuals with intellectual disability and GMFCS level V did not fit when the offset was determined based on all observations. Therefore, the offset for this subgroup was based on the observations of the subgroup (5y 1mo).
In all subdomains, estimated limits were higher for individuals without intellectual disability compared with those with intellectual disability, according to the 95% CIs (Table 2). For individuals without intellectual disability, estimated limits were comparable to those of typically developing individuals. The greatest lag compared with typically developing individuals was observed in written communication during childhood. The limits indicated that 9‐year‐old children with CP scored 6 VABS points lower, meaning that they performed three fewer VABS activities than 9‐year‐old typically developing individuals.
For individuals with intellectual disability, estimated limits for individuals in GMFCS level I to IV were higher than for individuals in GMFCS level V. This difference was significant for all subdomains, except for written communication (Table 2), and may address the most difficult items, such as: giving complex directions to others, going to evening events with friends without adult supervision, or independently weighing consequences of actions before making decisions.
For receptive communication, individuals with intellectual disability in GMFCS levels I to IV reach 90% and individuals with intellectual disability in GMFCS level V reach 63% of the score of individuals without intellectual disability in GMFCS level I. These proportions are 66% and 36% for expressive communication, 25% and 9% for written communication, 84% and 52% for interrelationships, 68% and 38% for play and leisure, and 53% and 22% for coping. Compared to individuals without intellectual disability, interindividual variances of the limits (50% ranges around the limits) were much wider for individuals with intellectual disability, for the communication subdomains in particular. With respect to social interactions, this was especially so for those in GMFCS level V. These wide interindividual variances indicate that the maximal development for individuals in this subgroup shows large variability.
The average age at which individuals with CP reached 90% of their limit in most cases did not differ significantly between individuals with and without intellectual disability nor between GMFCS levels. For individuals without intellectual disability, the mean age90 ranged between 3 years 3 months and 3 years 6 months for receptive communication (vs 3y 3mo for typically developing individuals); between 6 years 1 month and 7 years 1 month for expressive communication (vs 6y 5mo); between 12 years 9 months and 16 years 1 month for written communication (vs 14y 0mo); between 6 years 3 months and 7 years 6 months for interrelationships (vs 7y 10mo); between 13 years 8 months and 16 years 7 months for play and leisure (vs 15y 0mo); and between 14 years 0 months and 16 years 2 months for coping (vs 13y 0mo).
Addressing maximal performance levels for receptive and expressive communication, individuals with intellectual disability in GMFCS levels I to IV reach their (lower) limits at a similar age to individuals without intellectual disability. Compared with individuals without intellectual disability and individuals with intellectual disability in GMFCS levels I to IV, individuals with intellectual disability in GMFCS level V on average reach a lower limit at a young age, indicating poorer development. For written communication, the age90 of individuals with intellectual disability was higher than that of individuals without intellectual disability, but the large 95% CIs around the age90 (Table 2) and the raw observations (Appendix S3) indicate ample development for individuals with intellectual disability in this subdomain.
For play and leisure and coping, individuals with intellectual disability in GMFCS levels I to IV reach their lower limit on average at a younger age than individuals without intellectual disability, and individuals with intellectual disability in GMFCS level V at an even younger age. However, large 95% CIs around the age90 of individuals with intellectual disability (especially those in GMFCS level V) suggest that there was no rate of development to characterize average longitudinal curves.
Discussion
In communication and social interactions, individuals without intellectual disability in GMFCS levels I to IV follow development curves comparable to typically developing individuals. Development stabilizes in childhood for receptive communication, in adolescence for expressive communication and interrelationships, and in early adulthood for written communication, play and leisure, and coping. GMFCS level is only a marker of gross motor function. Although poor gross motor function may affect communication and social interactions, it does not reflect communicative and social capabilities. Therefore, healthcare professionals should not underestimate the communicative and social capabilities of young individuals with CP based on GMFCS levels. As expected, individuals with intellectual disability develop to lower maximal levels and their development shows large individual variation.
The long‐term follow‐up of individuals with CP resulted in more accurate estimates of the maximal performance levels compared with previous PERRIN studies.8, 9 In addition, with the additional measurement, nonlinear mixed‐effects models fit the data well and enabled quantitative estimations of the rate of development and a more direct comparison with other development curves. Hence, not only the maximal level but also the rate of development of individuals with CP without intellectual disability seems comparable to reference data of typically developing individuals.17 In interpreting this finding it should be noted that the study was carried out in the Netherlands where the environmental context is relatively accommodating towards individuals with impairments and their families. Other studies have shown wide variations in social interactions across regions within European countries, ascribing an estimated one‐third of the unexplained variation in communication activities to variation between regions.25 The finding is in contrast to our hypothesis of delayed development and is different from the development of motor capacity, motor performance, and daily activities in individuals with CP, where limits are lower for those with lower levels of motor function and development seems delayed.12, 14 We conclude that individuals with CP without intellectual disability develop well in the domains of communication and social interactions, despite limitations in motor capacity and activity performance. This underlines the need to address the different activity and participation domains specifically.
In line with previous PERRIN studies,8, 9 development curves were less favorable for individuals with intellectual disability. GMFCS level was related to maximal performance levels of each subdomain. Those in GMFCS level V performed poorer than those in GMFCS levels I to IV. Compared with other subdomains of communication, the average maximal performance level of receptive communication (e.g. following instructions requiring an action, listening to a teacher) was relatively high for individuals with intellectual disability. This suggests that individuals with intellectual disability perform relatively well in understanding spoken language. This may be because their conversational partners adapt their message to an appropriate level. Also, a discrepancy may be present between understanding spoken language and what individuals are able to communicate as understood.26 Lastly, individuals with intellectual disability in GMFCS levels I to IV perform relatively well in interrelationships (e.g. initiating conversations, buying gifts for someone). This finding may primarily reflect relationships with close relatives, as the VABS does not differentiate between relationships with familiar or unfamiliar people.
Interindividual variability was much larger for individuals with intellectual disability, as indicated by a larger 50% range around the limits and raw observations. This was particularly true for receptive and expressive communication, where some individuals in GMFCS level V reached the maximum score, while others hardly developed and had very low scores. These differences are also reflected by a broad distribution over Communication Function Classification System levels and Manual Ability Classification System levels, whose stratification modes have been shown to strongly correlate with GMFCS levels.2, 27 The large variation indeed seems partly attributed to communication function (see Appendix S5). In addition, it may be caused partly by different intellectual levels within those categorized with IQ less than 70. The large variation indicates a need for a personalized approach in rehabilitation for individuals with intellectual disability.
The present study has some limitations. The VABS lists activities in developmental order for children aged between 0 and 19 years; there may be relevant activities that develop after the ceiling age. Therefore, development may be ongoing even though a plateau on the VABS scores is reached. Since the most difficult items of interrelationships were discarded, the activities in that domain reflect development between 0 and 15 years. Consequently, performance may particularly develop after the reported limit is reached. Second, the VABS addresses attendance of participation by asking whether or not a person usually performs activities, regardless of the use of assistive devices, adaptations, or supervision. Clinical experience and studies using concepts of participation other than attendance, such as difficulty of participation, or addressing other aspects, such as romantic relationships, indicate that individuals with CP do face restrictions in social interactions.28, 29 Furthermore, the present study did not consider the quality of communication and satisfaction or preferences in social interactions, which are relevant to clinical decision‐making. Third, the VABS addresses objectively assessed basic skills. More complex skills or subjective aspects may develop differently. For example, individuals at risk of less favorable development of communication may also be assessed with more in‐depth examination of language, speech, and motor function30 and questioned on their subjective experience of social interactions. Finally, no Dutch reference data were available and comparison to reference data from the USA was descriptive rather than statistically tested.
Our findings may be used to inform individuals with CP on their future functioning in communication and social interactions. Healthcare professionals may use the development curves for setting and adequate timing of specific treatment goals for individuals that seem to lag behind expected development. Future studies should examine which factors measured in childhood predict communication and social interactions at adult age, especially for individuals with intellectual disability who currently show wide interindividual variability.
Supporting information
Figure S1: Flow diagram of inclusion.
Appendix S1: Number of observations by age group.
Appendix S2: Statistical appendix.
Appendix S3: Raw observations.
Appendix S4: Parameters of development in communication by intellectual disability and type of cerebral palsy.
Appendix S5: Scatter plots by Communication Function Classification System level for individuals with intellectual disability.
Acknowledgements
The members of the PERRIN‐DECADE study group are as follows: AJ Dallmeijer, M van Gorp, L van Wely, V de Groot (VU University Medical Center, Amsterdam); ME Roebroeck, SS Tan, J van Meeteren, W van der Slot, H Stam (Erasmus MC, University Medical Center and Rijndam Rehabilitation, Rotterdam); M Ketelaar, JM Voorman (University Medical Center Utrecht and Rehabilitation Center De Hoogstraat, Utrecht); HA Reinders‐Messelink (Revalidatie Friesland and University Medical Center Groningen, Groningen); JW Gorter (McMaster University, Hamilton, Canada); J Verheijden (BOSK, Association of Physically Disabled Persons and their Parents, Utrecht).
The authors would like to thank Marjolein van der Spek‐Sturrus (Rijndam Rehabilitation, Rotterdam) for her contribution to the recruitment and interviewing of participants at the 13‐year follow‐up. The authors particularly thank the individuals with CP and their caregivers who provided data for the analyses. This research was performed as part of the PERRIN research programme and was supported by Fonds NutsOhra (grant number 1403‐030) and Rijndam Rehabilitation, Rotterdam, the Netherlands.
The authors have stated that they had no interests that might be perceived as posing a conflict or bias.
Contributor Information
Siok Swan Tan, Email: s.s.tan@erasmusmc.nl.
Perrin‐Decade study group:
AJ Dallmeijer, L van Wely, V de Groot, J van Meeteren, W van der Slot, H Stam, JW Gorter, and J Verheijden
References
- 1. Strauss D, Brooks J, Rosenbloom L, Shavelle R. Life expectancy in cerebral palsy: an update. Dev Med Child Neurol 2008; 50: 487–93. [DOI] [PubMed] [Google Scholar]
- 2. Hidecker MJ, Ho NT, Dodge N, et al. Inter‐relationships of functional status in cerebral palsy: analyzing gross motor function, manual ability, and communication function classification systems in children. Dev Med Child Neurol 2012; 54: 737–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Pennington L, McConachie H. Predicting patterns of interaction between children with cerebral palsy and their mothers. Dev Med Child Neurol 2001; 43: 83–90. [DOI] [PubMed] [Google Scholar]
- 4. Donkervoort M, Roebroeck M, Wiegerink D, et al. Determinants of functioning of adolescents and young adults with cerebral palsy. Disabil Rehabil 2007; 29: 453–63. [DOI] [PubMed] [Google Scholar]
- 5. Holsbeeke L, Ketelaar M, Schoemaker MM, Gorter JW. Capacity, capability, and performance: different constructs or three of a kind? Arch Phys Med Rehabil 2009; 90: 849–55. [DOI] [PubMed] [Google Scholar]
- 6. Smits DW, Ketelaar M, Gorter JW, et al. Development of daily activities in school‐age children with cerebral palsy. Res Dev Disabil 2011; 32: 222–34. [DOI] [PubMed] [Google Scholar]
- 7. Voorman JM, Dallmeijer AJ, Van Eck M, Schuengel C, Becher JG. Social functioning and communication in children with cerebral palsy: association with disease characteristics and personal and environmental factors. Dev Med Child Neurol 2010; 52: 441–7. [DOI] [PubMed] [Google Scholar]
- 8. Tan SS, Wiegerink DJ, Vos RC, et al. Developmental trajectories of social participation in individuals with cerebral palsy: a multicentre longitudinal study. Dev Med Child Neurol 2014; 56: 370–7. [DOI] [PubMed] [Google Scholar]
- 9. Vos RC, Dallmeijer AJ, Verhoef M, et al. Developmental trajectories of receptive and expressive communication in children and young adults with cerebral palsy. Dev Med Child Neurol 2014; 56: 951–9. [DOI] [PubMed] [Google Scholar]
- 10. Parkes J, Hill N, Platt MJ, Donnelly C. Oromotor dysfunction and communication impairments in children with cerebral palsy: a register study. Dev Med Child Neurol 2010; 52: 1113–9. [DOI] [PubMed] [Google Scholar]
- 11. Sigurdardottir S, Vik T. Speech, expressive language, and verbal cognition of preschool children with cerebral palsy in Iceland. Dev Med Child Neurol 2011; 53: 74–80. [DOI] [PubMed] [Google Scholar]
- 12. Rosenbaum PL, Walter SD, Hanna SE, et al. Prognosis for gross motor function in cerebral palsy: creation of motor development curves. JAMA 2002; 288: 1357–63. [DOI] [PubMed] [Google Scholar]
- 13. Smits DW, Gorter JW, Hanna SE, et al. Longitudinal development of gross motor function among Dutch children and young adults with cerebral palsy: an investigation of motor growth curves. Dev Med Child Neurol 2013; 55: 378–84. [DOI] [PubMed] [Google Scholar]
- 14. van Gorp M, Roebroeck ME, Swan Tan S, et al. Activity performance curves of individuals with cerebral palsy. Pediatrics 2018; 142: pii:e20173723. [DOI] [PubMed] [Google Scholar]
- 15. Smits DW, Gorter JW, Riddell CA, et al. Mobility and self‐care trajectories for individuals with cerebral palsy (aged 1‐21 years): a joint longitudinal analysis of cohort data from the Netherlands and Canada. Lancet Child Adolesc Health 2019; 3: 548–57. [DOI] [PubMed] [Google Scholar]
- 16. de Bildt AAK, Vineland‐Z DW. Dutch Version of the Vineland Adaptive Behavior Scales Survey Form (Manual). Leiden: PITS; 2003. [Google Scholar]
- 17. Sparrow SS, Balla D, Ciccetti DV. Vineland Adaptive Behavior, survey ed. Circle Pines, MN: American Guidence Service, 1984. [Google Scholar]
- 18. van Duijn G, Dijkxhoorn Y, Noens I, Scholte E,van Berckelaer‐Onnes I. Vineland Screener 0‐12 years research version (NL). Constructing a screening instrument to assess adaptive behaviour. Int J Methods Psychiatr Res 2009; 18: 110–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Tellegen P, Winkel M, Wijnberg‐Williams B, Laros J. [Snijders‐Oomen Non‐verbal Intelligence Test SON‐R Manual and Research Report]. Lisse, the Netherlands: Swets & Zeitlinger, 1998. [In Dutch] [Google Scholar]
- 20. Raven J, Raven JC, Court JH. The Coloured Progressive Matrices. Manual for Raven's Progressive Matrices and Vocabulary Scale. San Antonio, TX: Harcourt Assessment, 1998. [Google Scholar]
- 21. Palisano RJ, Hanna SE, Rosenbaum PL, et al. Validation of a model of gross motor function for children with cerebral palsy. Phys Ther 2000; 80: 974–85. [PubMed] [Google Scholar]
- 22. Surveillance of Cerebral Palsy in Europe . Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy surveys and registers. Dev Med Child Neurol 2000; 42: 816–24. [DOI] [PubMed] [Google Scholar]
- 23. Hidecker MJ, Paneth N, Rosenbaum PL, et al. Developing and validating the Communication Function Classification System for individuals with cerebral palsy. Dev Med Child Neurol 2011; 53: 704–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Burnham KPAD. Model Selection and Multi‐model Inference: A Practical Information‐theoretic Approach, 2nd ed New York: Springer, 2002. [Google Scholar]
- 25. Fauconnier J, Dickinson HO, Beckung E, et al. Participation in life situations of 8‐12 year old children with cerebral palsy: cross sectional European study. BMJ 2009; 338: b1458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Geytenbeek JJ, Vermeulen RJ, Becher JG, Oostrom KJ. Comprehension of spoken language in non‐speaking children with severe cerebral palsy: an explorative study on associations with motor type and disabilities. Dev Med Child Neurol 2015; 57: 294–300. [DOI] [PubMed] [Google Scholar]
- 27. van Meeteren J, Nieuwenhuijsen C, de Grund A, et al. Using the manual ability classification system in young adults with cerebral palsy and normal intelligence. Disabil Rehabil 2010; 32: 1885–93. [DOI] [PubMed] [Google Scholar]
- 28. van Gorp M, Van Wely L, Dallmeijer AJ, et al. Long‐term course of difficulty in participation of individuals with cerebral palsy aged 16 to 34 years: a prospective cohort study. Dev Med Child Neurol 2019; 61: 194–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Wiegerink DJ, Stam HJ, Gorter JW, et al. Development of romantic relationships and sexual activity in young adults with cerebral palsy: a longitudinal study. Arch Phys Med Rehabil 2010; 91: 1423–8. [DOI] [PubMed] [Google Scholar]
- 30. Coleman A, Fiori S, Weir KA, Ware RS, Boyd RN. Relationship between brain lesion characteristics and communication in preschool children with cerebral palsy. Res Dev Disabil 2016; 58: 55–64. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1: Flow diagram of inclusion.
Appendix S1: Number of observations by age group.
Appendix S2: Statistical appendix.
Appendix S3: Raw observations.
Appendix S4: Parameters of development in communication by intellectual disability and type of cerebral palsy.
Appendix S5: Scatter plots by Communication Function Classification System level for individuals with intellectual disability.