

Abstract
BACKGROUND
Temporary deferral of whole blood donors is essential for a safe blood supply, yet deferral may impact donor return. Different deferral reasons may differently affect return, and donor experience may interfere with this. Therefore, we studied the joint effect of deferral reason and donor experience on return.
STUDY DESIGN AND METHODS
We used a large‐scale retrospective cohort design including all Dutch donors with a whole blood donation attempt in 2013 to 2015 (n = 343,825). We established details of the target donation (including deferral reason if applicable), details of attendances in the 2 years after the target donation, donor characteristics (blood type, sex, age), and donor experience (first‐time, novice, experienced, reactivated). Descriptive statistics as well as time‐to‐events methods were used.
RESULTS
Experienced donors were most likely to return, even after deferral (nondeferred 96% vs. deferred 92%). First‐time and reactivated donors were less likely to return after deferral (69 and 61%, respectively) compared to their nondeferred counterparts (82 and 76%, respectively). First‐time hemoglobin (Hb)‐deferred donors were less likely to return and slower to return than other donors. Similar results were found for reactivated donors deferred for short‐term medical reasons.
CONCLUSION
Deferral reason and donor experience individually as well as jointly impacted donor return. Particularly first‐time and reactivated donors were at risk of nonreturn, especially when deferred for Hb or short‐term medical reasons, respectively. Blood banks designing and implementing donor retention strategies should thus not only take successful but also unsuccessful donation experiences and different experience levels into account.
Successful blood donations are essential to the blood supply, yet there is always the possibility that a blood donor is not eligible to donate at the moment of presenting to a collection site. Deferrals function to protect either the donor's own health (e.g., deferral for low hemoglobin [Hb], the most common reason for deferral1) or that of the donation recipient (e.g., deferral due to travel to virus‐endemic areas). In many cases, donors self‐defer by contacting the blood bank ahead of their intended donation, yet still many donations are deferred on site (for example, approx. 10% at Dutch collection centers every year2). The current paper focuses on on‐site deferrals of whole blood donations.
Depending on the reason for deferral, the donor is deferred for a period of time ranging from a single day to indefinitely.3 Temporarily deferred donors are welcome to donate again once the deferral period has ended. However, research consistently showed that deferred donors are less likely to return than nondeferred donors.4, 5, 6
Thus far, not much is known about the effects of different deferral reasons on donor return. One study found that deferral for low hematocrit (Hct) or Hb led to the highest return rate among all deferral reasons, whereas needle‐related deferral (e.g., recent tattoo, piercing, or electrolysis) was associated to the lowest return.5 Moreover, the same study showed that deferrals associated with a relatively shorter deferral duration were generally associated with higher return rates.5 Another study found that return rates were higher for donor safety–related deferrals (including Hb, blood pressure, and pulse) than for deferrals for recipient safety (e.g., blood‐borne pathogen risk, miscellaneous blood exposure, and malaria risk).7 Hb‐related deferral thus generally appears to be associated with relatively high return. Results for other deferral reasons are mixed, and there is a need to better understand exactly how different deferral reasons affect donor return.
Donor return after deferral may also be influenced by the donor's donation experience. First‐time donors who are temporarily deferred may be confused5, 8 and disappointed,9 which may lead to the decision not to return for a new donation attempt once eligible again. More experienced donors, however, already know the drill and realize that deferral is something that might just happen every now and then. Prior research showed that these first‐time donors are indeed less likely to return than more experienced donors,4, 5, 10, 11 yet the transition from rookie first‐time donor to seasoned experienced donor does not happen overnight. It takes time and experience to form donation habits and to internalize the new blood donor identity.12 Therefore, and in line with previous work,13 we distinguish a group of novice donors beside first‐time and experienced donors. Furthermore, there may be registered donors without any recent donation experience that somehow decide to return. Being out of the donation habit potentially means that they have to rebuild their donor identity and get reacquainted with the donation process and (potentially) with new blood bank policies. We dub this group of donors reactivated donors. Empirical studies of return among novice and reactivated donors are currently lacking.
Donor experience may interact with the different reasons for deferral. Two studies about the difference between first‐time versus other donors provide pointers for such differential effects.4, 5 Among first‐time donors, return did not seem to differ too much between different deferral reasons (i.e., return was low for all deferral reasons), whereas return among other donors ranged from 90% (for deferral because of feeling unwell) to 58% (for needle‐related and medication‐related deferral).4 Additionally, the difference in odds of returning between first‐time and other donors was much smaller after deferral for needle events and travel to malaria‐endemic areas than after deferral for low Hct/Hb, blood pressure/pulse, feeling unwell, or on‐site self‐deferral.5 We analyzed the combined effect of different deferral reasons and donation experience on return, based on the entire whole blood donor population in the Netherlands. The Dutch donor population is (to a certain extent) representative for the general population: donors of non‐Dutch origin being underrepresented and donors being somewhat healthier than the general Dutch population.14, 15
MATERIALS AND METHODS
We used a retrospective study design (approved by the institutional review board) in which we included all Dutch donors that presented for whole blood donation at least once between 2013 and 2015. They gave permission to (anonymously) use their data as stored in the Dutch donor registry. In the Netherlands, Sanquin is solely responsible for the country's blood supply, including all steps from collecting to issuing blood products. Sanquin invites registered donors (by sending out postcards) to donate during a 2‐week walk‐in period at a fixed or mobile donation location. After registration, first‐time donors are invited (via phone) for a screening appointment at one of the collection sites, including an interview and blood tests. When screening is complete, eligible donors receive a postcard to invite them to donate based on demand for their blood type.
For all included donors, we identified their first whole blood donation attempt in the period 2013 to 2015 as target donation. Donor nonreturn (or lapse, as it is often called in the literature16, 17, 18) was defined as not returning for a new donation attempt within 2 years after the donor was eligible to donate again after the target donation. Hence, the follow‐up period was as long as the ineligibility period plus 2 years or until the end of the inclusion period (December 31, 2017). We excluded donors that were permanently deferred, whose deferral lasted until after the inclusion period, or who did not receive any invitations after their target donation. The remaining 343,825 donors presented for a whole blood donation at least once between 2013 and 2015 (i.e., the target donation) and were invited for a next donation at least once. The target donation could also be an attempt only, if the donor was deferred on site.
Measures
Nonreturn was defined as the absence of a next donation attempt within 2 years after the donor was eligible again after the target donation. Time to return was either calculated as time to next visit for returning donors (not including the mandatory 56‐day ineligibility period) or censored at 2 years after the donor was eligible again.
Deferral
For each target donation, we assessed whether the donor was deferred (0/1, 1 = deferred) and, if so, for what reason. All deferral reasons are associated with a standard deferral period cf. Sanquin policy. For instance, donors with Hb levels below the cutoff are deferred for 91 days by default, while donors who traveled to infection risk areas are deferred for up to 183 days after return, depending on the area visited. We collapsed deferral reasons into five categories: Hb (median deferral duration 91 days), travel related (median deferral duration 26 days), medical short term (standard deferral term of 28 days or less; median deferral duration 28 days), medical long term (standard deferral term of more than 28 days; median deferral duration 129 days), or miscellaneous (including pregnancy, risk behavior, needle events, and other reasons; median deferral duration 101 days).
Donor experience
Based on registration information and attendance history, we assessed for each donor his or her experience at the time of the target donation. We distinguished four categories: first time, novice, experienced, and reactivated donors. First‐time donors were newly registered without any prior donations, novice donors had donated one to five times in the 3 years before the target donation,13 and experienced donors had donated at least five times. Reactivated donors had no donations in the 3 years before the target donation, but had registered donations previously.
Demographic information
We retrieved information about the donors' sex, blood group information (ABO and D), and age at the time of the target donation from the blood bank registry.
Donation site
For all donations, we retrieved whether the donor presented at a fixed or mobile donation site. Mobile donation sites are relocated throughout the country, and donors at these sites are invited to donate on the particular day(s) the mobile location is there.
Statistical analysis
We report on descriptive statistics related to demographics, deferral reason, donor experience, and return. Similar to previous researchers,1, 4, 19 we then report on Kaplan‐Meier survival curves to visually examine the effects of different deferral reasons and experience on donor return. For sake of interpretation, the survival curves presented in this paper are inverse survival curves (i.e., one minus survival), meaning that a higher line reflects a larger number of returned donors. On the Y‐axis, the cumulative proportion of donors who have (already) returned is shown; 0 means that no donors have returned, and 1 means that all donors have returned. These survival analyses are not adjusted for potential confounding variables. Next, the survival curves for deferral reasons were stratified by donor experience. Finally, Cox proportional hazards regression was used to examine the interaction effect of different deferral reasons and experience categories on the time to return.
RESULTS
A total of 343,825 donors were included in the final sample. Of these donors, 58% were female, 75% donated at fixed sites, 48% had blood group O, and 78% were D+ (see Table 1). Donation site was not associated to any of our key variables and thus not further considered. Fig. 1 presents an overview of our sample in terms of deferral, experience, and return. Overall, 49,444 (14%) of all donors did not return after the target donation. Our sample consisted of 25% first‐time donors, 41% novice donors, 30% experienced donors, and 4% reactivated donors. Of all target donations, 38,069 (11%) were deferred. Of these deferred donations, 40% were deferred for low Hb, 23% for short‐term medical reasons, 19% for travel‐related infection risk, 14% for miscellaneous reasons, and 5% for long‐term medical reasons. First‐time donors were relatively young (mean 29.8 years) compared to the other experience categories (means >40 years). Experienced donors were more often male (59%) than donors in the other three categories (32%‐36% male). Nondeferred donors were older (mean 45.7 years) than deferred donors (all means <43 years) and more often male (55%) than female (45%). The majority of all donors deferred for Hb was female (82%).
Table 1.
Demographics of the donor population used for analyses
| All donors (n = 343,825) | First‐time donors (n = 87,314) | Novice donors (n = 139,915) | Experienced donors (n = 102,324) | Reactivated donors (n = 14,272) | Not deferred (n = 305,756) | Hb deferral (n = 15,132) | Travel‐related deferral (n = 7,135) | Short‐term medical deferral (n = 8,583) | Long‐term medical deferral (n = 1,906) | Misc. deferral (n = 5,313) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean age (years) | 41.3 | 29.8 | 42.6 | 49.4 | 40.8 | 45.7 | 37.7 | 36.8 | 42.6 | 41.5 | 31.2 |
| Sex | |||||||||||
| Male | 42% | 32% | 35% | 59% | 36% | 55% | 18% | 40% | 40% | 39% | 26% |
| Female | 58% | 68% | 65% | 41% | 64% | 45% | 82% | 60% | 60% | 61% | 74% |
| Collection site | |||||||||||
| Fixed | 75% | 82% | 67% | 81% | 76% | 75% | 77% | 81% | 72% | 75% | 82% |
| Mobile | 25% | 18% | 33% | 19% | 24% | 25% | 23% | 19% | 28% | 25% | 18% |
| Blood group (ABO) | |||||||||||
| A | 39% | 40% | 39% | 39% | 39% | 39% | 42% | 39% | 39% | 39% | 39% |
| B | 9% | 10% | 11% | 6% | 9% | 8% | 8% | 10% | 9% | 10% | 10% |
| AB | 3% | 4% | 4% | 2% | 4% | 3% | 4% | 4% | 4% | 4% | 4% |
| O | 48% | 46% | 46% | 54% | 47% | 51% | 46% | 47% | 49% | 48% | 46% |
| Blood type (D) | |||||||||||
| Positive | 78% | 81% | 80% | 73% | 80% | 77% | 79% | 80% | 79% | 80% | 80% |
| Negative | 22% | 19% | 20% | 27% | 20% | 24% | 21% | 20% | 21% | 20% | 20% |
Figure 1.
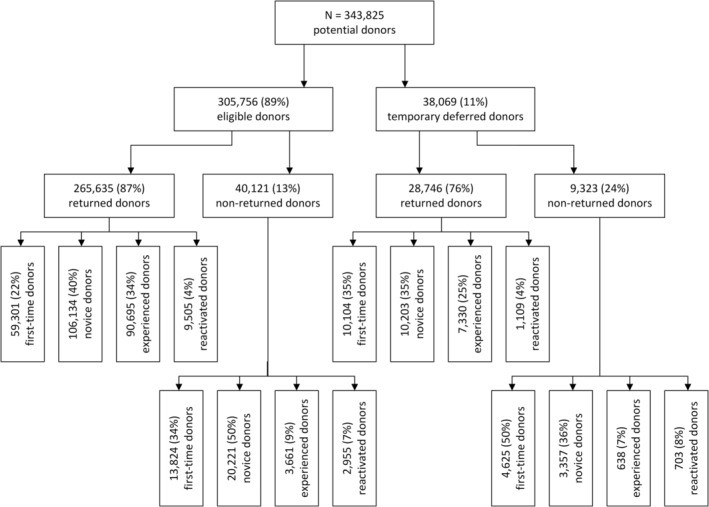
Overview of study population with regard to (non‐)deferral, (non‐)return, and experience.
The association between deferral and return
Deferral affected return: 24% of the donors whose donations were deferred did not return after the target donation, compared to 13% of nondeferred donors (Fig. 1). Among the most prevalent deferral reasons (low Hb, short‐term medical, and travel‐related deferral), the percentage of returned donors was average to higher (i.e., 78, 75, and 79%, respectively) compared to the overall return rate among deferred donors (76%; Table 2). Long‐term medical deferral was the least common deferral reason, yet it was associated with a relatively low percentage of returning donors (73%). Return was lowest (65%) among donors deferred for miscellaneous reasons. The median time to return (i.e., the moment in time at which 50% of the donors in that group has returned; displayed by the dotted horizontal line in Fig. 2) was lowest for nondeferred donors and donors deferred for Hb (79 and 77 days, respectively), and highest for donors deferred for miscellaneous reasons (159 days).
Table 2.
Number of on‐site deferrals on the target donation and returned donors in each group by donation experience category
| All donors | First‐time donors | Novice donors | Experienced donors | Reactivated donors | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number at target | Number returned | Number at target | Number returned | Number at target | Number returned | Number at target | Number returned | Number at target | Number returned | |
| Not deferred | 305,756 | 265,635 (87%) | 72,585 | 59,301 (82%) | 126,355 | 106,134 (84%) | 94,356 | 90,695 (96%) | 12,460 | 9,505 (76%) |
| Deferred | 38,069 | 28,746 (76%) | 14,729 | 10,104 (69%) | 13,560 | 10,203 (75%) | 7,968 | 7,330 (92%) | 1,812 | 1,109 (61%) |
| Hb | 15,132 | 11,817 (78%) | 4,828 | 3,216 (67%) | 5,592 | 4,371 (78%) | 4,168 | 3,889 (93%) | 544 | 341 (63%) |
| Travel‐related | 7,135 | 5,619 (79%) | 3,630 | 2,730 (75%) | 2,242 | 1,769 (79%) | 982 | 927 (94%) | 281 | 193 (69%) |
| Short‐term medical | 8,583 | 6,439 (75%) | 1,872 | 1,321 (71%) | 3,965 | 2,856 (72%) | 2,114 | 1,911 (90%) | 632 | 351 (56%) |
| Long‐term medical | 1,906 | 1,395 (73%) | 799 | 529 (66%) | 666 | 492 (74%) | 355 | 314 (88%) | 86 | 60 (70%) |
| Miscellaneous | 5,313 | 3,476 (65%) | 3,600 | 2,308 (64%) | 1,095 | 715 (65%) | 349 | 289 (83%) | 269 | 164 (61%) |
Figure 2.
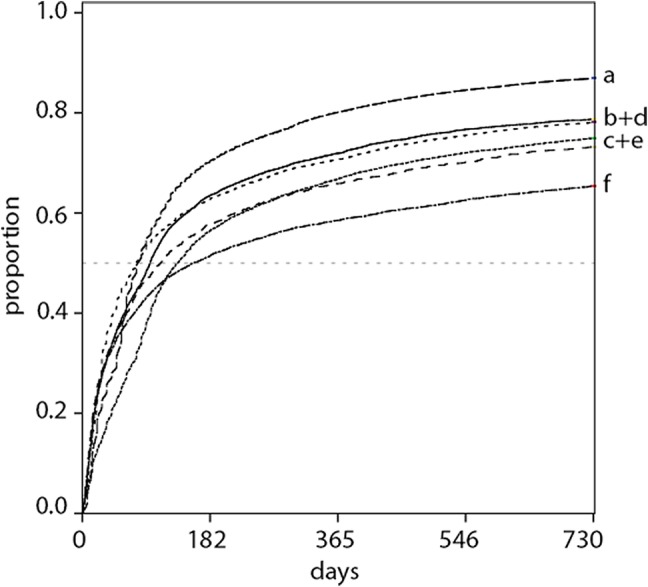
Cumulative proportion of donors returning and time to return for deferred and nondeferred donors. The dotted horizontal line is the 50% return mark. a = nondeferred; b = travel‐related deferral; c = short‐term medical deferral; d = Hb deferral; e = long‐term medical deferral; f = miscellaneous deferral. [Color figure can be viewed at http://wileyonlinelibrary.com]
The association between experience and return
Donor experience had an impact on (the timing of) return behavior (Fig. 3). First‐time and novice donors returned less often (79 and 82%, respectively) than experienced donors (96%). Reactivated donors returned even less: 74% returned. Even though experienced donors were most likely to return, their time to return was longer (median 63 days) than among first‐time donors (median 39 days). Novice and reactivated donors were slower in returning (medians 129 and 142 days, respectively).
Figure 3.
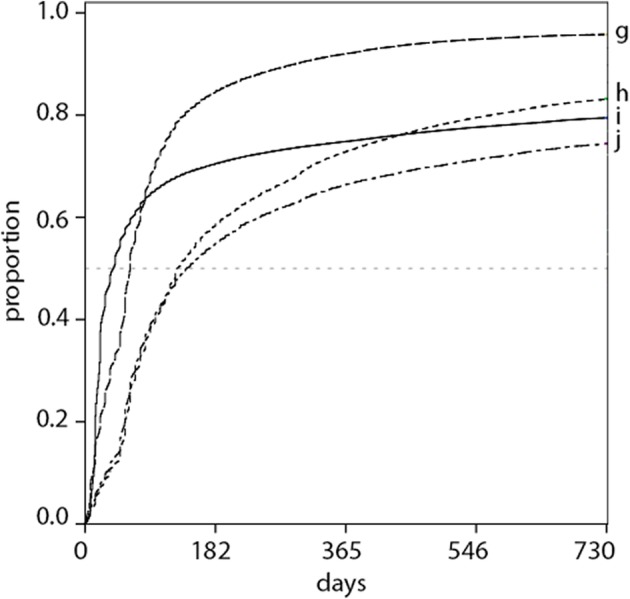
Cumulative proportion of donors returning and time to return for experience categories. The dotted horizontal line is the 50% return mark. g = experienced donors; h = novice donors; i = first‐time donors; j = reactivated donors. [Color figure can be viewed at http://wileyonlinelibrary.com]
The interaction of deferral and experience on return
First‐time and reactivated donors were deferred more often (17 and 13%, respectively) than novice (10%) and experienced donors (8%; Table 2). Deferral reasons also differed: First‐time donors were more often deferred for travel‐related and miscellaneous reasons than other donors. First‐time donors were less often deferred for Hb and short‐term medical reasons than novice and experienced donors. Reactivated donors show a pattern similar to that of first‐time donors for Hb and short‐term medical related deferrals, but not for travel‐related and miscellaneous deferrals.
Stratified analyses for donor experience showed differences between the deferred and nondeferred donor curves for different experience categories (Fig. 4). Within all experience categories, nondeferred donors are most likely to return, although the difference between nondeferred and deferred donors is much more pronounced among first‐time, novice, and reactivated donors (i.e., the difference in return after 2 years between nondeferred and donors deferred for miscellaneous reasons varies from 15‐19 percentage points) than among experienced donors (where this difference is 13 percentage points). The influence of different deferrals on donor return seems to be rather similar among experience categories—deferral for miscellaneous reasons leads to a relatively high number of donors not returning, whereas nonreturn after travel‐related deferral was relatively less common among donors in all experience categories. There were two exceptions. Short‐term medical deferral had a stronger effect on return among reactivated donors (Fig. 4 bottom right) than within the other experience categories. Hb‐related deferral resulted in lower return among first‐time (Fig. 4 top left) and reactivated donors compared to novice and experienced donors (Fig. 4 top right and bottom left, respectively).
Figure 4.
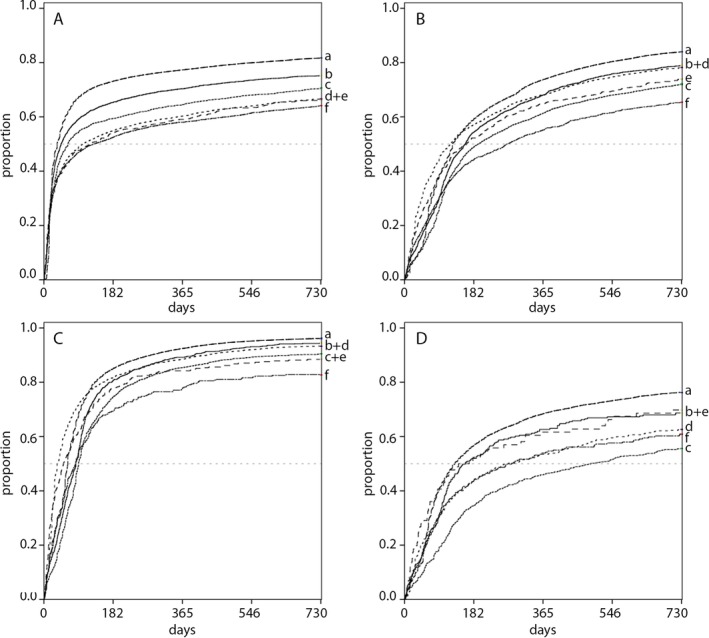
Cumulative proportion of donors returning and time to return for (A) first‐time, (B) novice, (C) experienced, and (D) reactivated donors. The dotted horizontal line is the 50% return mark. a = nondeferred; b = travel‐related deferral; c = short‐term medical deferral; d = Hb deferral; e = long‐term medical deferral; f = miscellaneous deferral. [Color figure can be viewed at http://wileyonlinelibrary.com]
Finally, the Cox proportional hazards models (adjusted for age, sex, and blood type; Table 3) showed that Hb deferral further decreased time to return among first‐time, novice, and reactivated donors (odds ratios [ORs] 0.55‐0.92). For first‐time donors, long‐term medical deferral also led to slower return (OR 0.70; CI 0.55‐0.89), which was already slower for first‐time donors compared to experienced donors (OR 0.87; CI 0.86‐0.89). For reactivated donors, the interaction with short‐term medical deferral further decreased speed of return (OR 0.80; CI 0.66‐0.97), on top of the already very low return rate for reactivated donors in general (OR 0.51; CI 0.49‐0.53). Finally, travel‐related or miscellaneous deferrals did not affect the odds that any of the experience groups returned at a different rate in addition to the main effects of experience and deferral.
Table 3.
Multivariate Cox proportional hazards model predicting rate of return for a subsequent donation attempt*
| Predictor | OR (99.9% CI) | p value |
|---|---|---|
| Deferral reason | ||
| Not deferred | (Reference) | |
| Hb | 1.12 (1.06‐1.18) | <0.001 |
| Travel related | 0.84 (0.76‐0.94) | <0.001 |
| Short‐term medical | 0.69 (0.64‐0.74) | <0.001 |
| Long‐term medical | 0.81 (0.68‐0.98) | <0.001 |
| Miscellaneous | 0.66 (0.55‐0.81) | <0.001 |
| Experience | ||
| Experienced donors | (Reference) | |
| First‐time donors | 0.87 (0.86‐0.89) | <0.001 |
| Novice donors | 0.57 (0.56‐0.58) | <0.001 |
| Reactivated donors | 0.51 (0.49‐0.53) | <0.001 |
| Interaction of deferral reason and experience | ||
| First‐time donor × Hb deferral | 0.55 (0.51‐0.60) | <0.001 |
| First‐time donor × travel‐related deferral | 0.94 (0.83‐1.07) | 0.120 |
| First‐time donor × short‐term medical deferral | 0.97 (0.86‐1.09) | 0.368 |
| First‐time donor × long‐term medical deferral | 0.70 (0.55‐0.89) | <0.001 |
| First‐time donor × miscellaneous deferral | 0.83 (0.67‐1.02) | 0.003 |
| Novice donor × Hb deferral | 0.92 (0.86‐1.00) | <0.001 |
| Novice donor × travel‐related deferral | 1.03 (0.90‐1.18) | 0.469 |
| Novice donor × short‐term medical deferral | 1.06 (0.96‐1.17) | 0.044 |
| Novice donor × long‐term medical deferral | 1.02 (0.80‐1.29) | 0.820 |
| Novice donor × miscellaneous deferral | 1.05 (0.83‐1.32) | 0.503 |
| Reactivated donor × Hb deferral | 0.68 (0.56‐0.82) | <0.001 |
| Reactivated donor × travel‐related deferral | 0.97 (0.74‐1.26) | 0.674 |
| Reactivated donor × short‐term medical deferral | 0.80 (0.66‐0.97) | <0.001 |
| Reactivated donor × long‐term medical deferral | 1.07 (0.67‐1.71) | 0.627 |
| Reactivated donor × miscellaneous deferral | 1.04 (0.75‐1.43) | 0.725 |
| Age | 1.00 (1.00‐1.00) | <0.001 |
| Blood group: ABO | ||
| O | (Reference) | |
| A | 0.95 (0.94‐0.96) | <0.001 |
| B | 0.86 (0.84‐0.88) | <0.001 |
| AB | 0.80 (0.78‐0.83) | <0.001 |
| Blood type: D | ||
| Negative | (Reference) | |
| Positive | 0.92 (0.90‐0.93) | <0.001 |
| Sex | ||
| Male | (Reference) | |
| Female | 0.80 (0.79‐0.81) | <0.001 |
A total of 177 donors had missing data on sex, blood type, and/or donation location, the majority of whom were first‐time donors (97%). We therefore removed these donors for this analysis only.
DISCUSSION
Temporary deferral led to lower donor return compared to nondeferred donors. However, donors deferred for miscellaneous reasons (including needle‐related events, pregnancy, and risk behavior) were less likely to return than donors deferred for other reasons. Donor experience also affects nonreturn: experienced donors returned most often, followed by novice and first‐time donors. Generally, we found that the rate of return was rather similar among all experience categories, first‐time donors deferred for Hb and reactivated donors deferred for short‐term medical reasons excepted. Below, we discuss these results in more detail in relation to the existing literature, followed by limitations, suggestions for future research, and implications.
With regard to the effects of deferral on return, our results corroborate previous findings that the reason for deferral affects donor return, yet we also found differences. Similar to previous research,5 we found that Hb deferral led to relatively high numbers of returning donors and deferral for needle‐related events (captured within the miscellaneous deferral category in our study) was related to lower numbers of returning donors. In our study, travel‐related deferral led to similar return rates as Hb deferral, which was in contrast to previous findings suggesting that malaria risk led to less return than Hb deferral.7 Finally, we did not observe that deferrals of shorter duration were associated with higher return. Based on the median deferral duration, the shortest deferrals in our study are short‐term medical and travel related (28 and 26 days, respectively), followed by Hb‐related deferral (91 days). In our study, Hb‐related deferral had a higher return rate than short‐term medical and travel‐related deferrals, which contrasts the idea that shorter deferrals lead to higher return.5
In line with previous findings, we found that experience affected return. First‐time donors are less likely to return than novice and experienced donors.1, 4, 5 In our study, deferral (regardless of reason) had a much larger impact on the return of first‐time donors compared to experienced donors. By also studying the return patterns of novice and reactivated donors separately, we show that not all “more experienced” donors are similar in their return behavior. Novice and reactivated donors showed unique patterns of (speed of) return, which underscores the importance of recognizing the level of experience among donors. For instance, novice and first‐time donors showed similarities in their numbers of return, yet differed in the speed at which donors returned. A similar difference in speed of return was observed between novice and experienced donors, as experienced donors returned more quickly (and also in larger numbers) than novice donors. This supports the idea that donor identity at the start of a donor career still needs to form. For reactivated donors, we found that they were also slow in returning and even less likely to return for a new donation than novice and first‐time donors. As previous researchers suggested that a higher number of donations in the period before the deferred donation may lead to increased resilience to the effects of temporary deferral,1 it might be the case that reactivated donors might actually be less resilient to temporary deferral compared to novice donors.
Finally, our results showed that deferral reasons had a similar effect on return in all experience categories, with two exceptions. To our knowledge, this study is the first to show this interaction effect of experience and deferral reason on donor (non‐)return for novice and reactivated donors.
Overall, we found relatively low numbers of nonreturning donors compared to other studies. For instance, we found that 13% of nondeferred donors did not return, which is similar to the rate in Australia,1 but much lower than the 26% and 49% nonreturn among eligible donors in the United States.4, 5 The number of deferred and nondeferred first‐time donors that did not return in our study (31% and 18%, respectively) was also much lower than the 75% to 59% for deferred and 30% to 53% for nondeferred first‐time donors found elsewhere.1, 4 These large differences might be related to different policies with regard to deferral reasons, deferral length, and length of postdonation intervals,1 but it also might be due to the Dutch context or Sanquin's system of explicitly inviting donors based on demand.
In our study, we focused only on whole blood donors, yet deferral led some donors in our sample to switch to non–whole blood donations. For instance, a donor deferred for malaria‐endemic travel might be asked to switch to plasmapheresis. In that case, the travel‐related deferral is basically bypassed and the donor is allowed to return much earlier than otherwise would have been the case, which may have affected their return behavior. Furthermore, for some of these non–whole blood donations donors are not invited via mail but rather make an appointment at the location or are contacted via phone, which may have affected their return behavior as well.
Future research efforts should be directed at the potentially additive effect of repeated deferrals. Furthermore, we need to understand why deferred donors do not return. Only few researchers thus far studied how donors emotionally experience temporary deferral at the location site and how those experiences relate to nonreturn.9, 20 Finally, future research could look into whether experienced donors are indeed more resilient to temporary deferral than less experienced donors or rather that nonresilient donors are filtered out early on in the donor career.
In all, our study showed that different reasons for temporary whole blood donor deferral may differently impact donor return depending on donor experience. For some donors receiving a temporary deferral—and thus a disruption of their donation pattern—may lead them to stop donating permanently. Even though all reasons for temporary deferral lead to lower return, some reasons are associated to even lower return or slower rates of return. Additionally, a lack of donor experience further decreases the odds of return. Donor nonreturn creates a necessity for blood banks to recruit new donors, while previous research has shown that retaining existing donors is cheaper and safer.21 However, this does not mean that retention is easy or cheap, and thus it might be wise for blood banks to take not only successful but also unsuccessful donation experiences into account, as well as different experience levels when designing and implementing donor retention strategies.
CONFLICTS OF INTEREST
The authors have disclosed no conflicts of interest.
ACKNOWLEDGMENT
The authors thank Femmeke Prinsze for her help with preparing the data set.
This work was funded by Sanquin Blood Supply (PPOC 17‐13). EMM's contribution has received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program (Grant Agreement 802227).
REFERENCES
- 1. Hillgrove T, Moore V, Doherty K, et al. The impact of temporary deferral due to low hemoglobin: future return, time to return and frequency of subsequent donation. Transfusion 2011;51:539‐47. [DOI] [PubMed] [Google Scholar]
- 2. De Kort W, Van den Burg P, Geerligs H, et al. Cost‐effectiveness of questionnaires in preventing transfusion‐transmitted infections. Transfusion 2014;54:879‐88. [DOI] [PubMed] [Google Scholar]
- 3. Masser BM, Bove LL, White KM, et al. Negative experiences and donor return: an examination of the role of asking for something different. Transfusion 2016;56:605‐13. [DOI] [PubMed] [Google Scholar]
- 4. Custer B, Chinn A, Hirschler NV, et al. The consequences of temporary deferral on future whole blood donation. Transfusion 2007;47:1514‐23. [DOI] [PubMed] [Google Scholar]
- 5. Custer B, Schlumpf KS, Wright D, et al. Donor return after temporary deferral. Transfusion 2011;51:1188‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Halperin D, Baetens J, Newman B. The effect of short‐term, temporary deferral on future blood donation. Transfusion 1998;38:181‐3. [DOI] [PubMed] [Google Scholar]
- 7. Zou S, Musavi F, Notari EP, et al. Donor deferral and resulting donor loss at the American Red Cross Blood Services, 2001 through 2006. Transfusion 2008;48:2531‐9. [DOI] [PubMed] [Google Scholar]
- 8. Mathew SM, King MR, Glynn SA, et al. Opinions about donating blood among those who never gave and those who stopped: a focus group assessment. Transfusion 2007;47:729‐35. [DOI] [PubMed] [Google Scholar]
- 9. Hillgrove T, Doherty KV, Moore VM. Understanding non‐return after a temporary deferral from giving blood: a qualitative study. BMC Public Health 2012;12:1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Noonan AE, Menitove JE, Franzmeier R. Temporarily deferred donors: do you love them or leave them. Transfusion 1981;21:591. [Google Scholar]
- 11. Piliavin JA. Temporary deferral and donor return. Transfusion 1987;27:199‐200. [DOI] [PubMed] [Google Scholar]
- 12. Masser BM, White KM, Hyde MK, et al. The psychology of blood donation: current research and future directions. Transfus Med Rev 2008;22:215‐33. [DOI] [PubMed] [Google Scholar]
- 13. Ferguson E, Atsma F, de Kort W, et al. Exploring the pattern of blood donor beliefs in first‐time, novice, and experienced donors: differentiating reluctant altruism, pure altruism, impure altruism, and warm glow. Transfusion 2012;52:343‐55. [DOI] [PubMed] [Google Scholar]
- 14. Goldman M, Steele WR, Di Angelantonio E, et al. Comparison of donor and general population demographics over time: a BEST Collaborative group study. Transfusion 2017;57:2469‐76. [DOI] [PubMed] [Google Scholar]
- 15. Atsma F, Veldhuizen I, de Vegt F, et al. Cardiovascular and demographic characteristics in whole blood and plasma donors: results from the Donor InSight study. Transfusion 2011;51:412‐20. [DOI] [PubMed] [Google Scholar]
- 16. Charbonneau J, Cloutier MS, Carrier E. Why do blood donors lapse or reduce their donation's frequency? Transfus Med Rev 2016;30:1‐5. [DOI] [PubMed] [Google Scholar]
- 17. Piersma TW, Bekkers R, de Kort W, et al. Blood donation across the life course: the influence of life events on donor lapse. J Health Soc Behav 2019;60:257‐72. [DOI] [PubMed] [Google Scholar]
- 18. Gemelli CN, Hayman J, Waller D. Frequent whole blood donors: understanding this population and predictors of lapse. Transfusion 2017;57:108‐14. [DOI] [PubMed] [Google Scholar]
- 19. James RC, Matthews DE. Analysis of blood donor return behaviour using survival regression methods. Transfus Med 1996;6:21‐30. [DOI] [PubMed] [Google Scholar]
- 20. Gemelli CN, Thijsen A, Van Dyke N, et al. Emotions experienced when receiving a temporary deferral: perspectives from staff and donors. ISBT Sci Ser 2018;13:394‐404. [Google Scholar]
- 21. Bagot KL, Murray AL, Masser BM. How can we improve retention of the first‐time donor? A systematic review of the current evidence. Transfus Med Rev 2016;30:81‐91. [DOI] [PubMed] [Google Scholar]