

Abstract
Emotional distress during pregnancy is likely influenced by both maternal history of adversity and concurrent prenatal stressors, but prospective longitudinal studies are lacking. Guided by a lifespan model of pregnancy health and stress sensitization theories, this study investigated the influence of intimate partner violence (IPV) during pregnancy on the association between childhood adversity and prenatal emotional distress. Participants included an urban, community-based sample of 200 pregnant women (aged 18-24) assessed annually from age 8-17 for a range of adversity domains, including traumatic violence, harsh parenting, caregiver loss, and compromised parenting. Models tested both linear and nonlinear effects of adversity as well as their interactions with IPV on prenatal anxiety and depression symptoms, controlling for potential confounds such as poverty and childhood anxiety and depression. Results showed that the associations between childhood adversity and pregnancy emotional distress were moderated by prenatal IPV, supporting a lifespan conceptualization of pregnancy health. Patterns of interactions were nonlinear, consistent with theories conceptualizing stress sensitization through an ‘adaptive calibration’ lens. Furthermore, results diverged based on adversity subdomain and type of prenatal IPV (physical vs. emotional abuse). Findings are discussed in the context of existing stress sensitization theories and highlight important avenues for future research and practice.
Keywords: early adversity, adverse childhood experiences, pregnancy stress, intimate partner violence, stress sensitization
A growing body of evidence suggests that maternal exposure to stress and adversity early in life can have enduring effects on mental health in adulthood, including emotional distress during pregnancy (Li, Long, Cao, & Cao, 2017; McDonnell & Valentino, 2016). Indeed, exposure to adverse childhood experiences (ACEs; Centers for Disease Control and Prevention, 2016) such as maltreatment and domestic violence can have lasting effects on neurobiological development and psychological outcomes across multiple stages of development (Anda et al., 2006; Danese & McEwen, 2012; Neigh, Gillespie, & Nemeroff, 2009). Emerging evidence guided by a lifespan model of pregnancy health (Misra, Guyer, & Allston, 2003) suggests that women with histories of adversity may be particularly vulnerable to emotional distress during pregnancy, including prenatal depression and anxiety (Madigan et al., 2014; Yildiz Inanici, Inanici, & Yoldemir, 2017). Given that emotional distress during pregnancy is linked to impairments in multiple domains of infant development (Dunkel Schetter & Tanner, 2012; Glynn et al., 2018), understanding the conditions by which maternal history of adversity impacts emotional health during pregnancy is critical to preventing adverse perinatal and postnatal outcomes for mothers and their children (Sara & Lappin, 2017).
Dimensions of Early Adversity
Despite the plausibility that history of adversity increases risk for emotional distress during pregnancy, most studies of prenatal women have only had access to adult retrospective reports of adversity, which are more prone to memory errors and recall bias compared to prospective measures of childhood adversity (Hardt & Rutter, 2004; Naicker, Norris, Mabaso, & Richter, 2017; Newbury et al., 2017; Reuben et al., 2016). Furthermore, rather than differentiate between types of stressors, most studies either focus on one specific ACE (e.g., sexual abuse) or combine a list of exposures into a cumulative adversity score (Atkinson et al., 2015; Centers for Disease Control and Prevention, 2016; Felitti et al., 1998). The cumulative adversity approach has led to important knowledge advancements regarding the disruptive impact of ‘toxic stress’ on long-term health (Hughes et al., 2017; Kalmakis & Chandler, 2015; Mersky, Topitzes, & Reynolds, 2013). However, some have argued that reliance on cumulative adversity scores has hindered clarification of the specific mechanisms underlying the impact of adversity on health outcomes, given that potential subdomains of adversity may differentially influence physiological and neurobiological processes underlying psychopathology (Humphreys & Zeanah, 2015; McLaughlin & Sheridan, 2016).
For example, guided by the neural bases of fear learning and sensory deprivation, McLaughlin and colleagues differentiated between adversities characterized by threat (e.g., abuse, violence) versus deprivation (e.g., neglect; McLaughlin & Sheridan, 2016; McLaughlin, Sheridan, & Lambert, 2014). Whereas amplified emotional reactivity to stress was specific to threat-based adversity (McLaughlin & Sheridan, 2016), severe deprivation was linked to a blunted stress profile (McLaughlin et al., 2015). In addition to these direct experiences of abuse and neglect, several common parent-related stressors including parent mental illness, substance use, and domestic violence, have also been indirectly linked to negative developmental outcomes by compromising parenting behavior (e.g., increasing household dysfunction or inconsistent parenting; Bailey et al., 2013; Huang, Wang, & Warrener, 2010; Neger & Prinz, 2015; Turney, 2011). Although most studies treat ACES as a single cumulative measure, factor analytic evidence indicates that childhood abuse loads onto a separate factor from parent-related stressors (Karatekin & Hill, 2018; Mersky, Janczewski, & Topitzes, 2017) and is differentially associated with adult health outcomes (Chartier, Walker, & Naimark, 2010). Some studies have found further distinctions between sexual abuse and physical/emotional abuse (Ford et al., 2014), and ACES pertaining to family loss and separation (i.e., incarceration, caregiver separation) have loaded onto a distinct factor as well (Mersky et al., 2017). Distinguishing between subdomains of adversity has important implications for understanding the mechanisms through which early adversity impacts later vulnerability to prenatal emotional distress, a critical step for identifying targets for screening and intervention.
Stress Sensitization During Pregnancy
The impact of early adversity on emotional distress during pregnancy may be further amplified for women re-exposed to traumatic stressors during pregnancy (Mezey, Bacchus, Bewley, & White, 2005), reflecting a broader theory of ‘stress sensitization’ (Hammen, Henry, & Daley, 2000). That is, early adversity may contribute to enduring emotional distress and psychopathology in adulthood by heightening an individual’s overall sensitivity to stress across the lifespan, including the prenatal period (Glaser, van Os, Portegijs, & Myin-Germeys, 2006; McLaughlin, Conron, Koenen, & Gilman, 2010). The plausibility of early-life stress sensitization is supported by evidence that early adversity alters the reactivity and regulation of stress physiology (e.g., HPA axis and autonomic nervous system; Bunea, Szentagotai-Tatar, & Miu, 2017; Hunter, Minnis, & Wilson, 2011) and is associated with higher emotional reactivity (i.e., tendency to react to stressors with increased negative affect and interpret events negatively; Shapero et al., 2019). Women with previous adversity exposure may perceive, react to, and respond to stressors differently in adulthood, thus magnifying the negative effects of adult stressors on psychological outcomes (Gunnar, 2000). Indeed, a growing number of studies have detected interactive effects between early adversity and adult stressors, whereby the magnitude of stress effects on mood and anxiety outcomes varied depending on history of early adversity (McLaughlin et al., 2010; Dienes et al., 2006; Harkness et al., 2006). Importantly, these synergistic effects of early adversity and later adult stress were evident beyond the simple additive effects of early adversity or adult stressors alone, suggesting that early adversity increases vulnerability for later emotional distress by changing the way later stressors are experienced (Harkness et al., 2006).
Although most studies testing stress sensitization have reported a ‘kindling effect,’ whereby previous adversity heightens sensitivity to later stressors, a number of studies have observed an opposite pattern, such that moderate levels of adversity predicted decreased emotional distress to subsequent stressors (Ellis & Boyce, 2008; Lovallo, Farag, Sorocco, Cohoon, & Vincent, 2012; M. Rutter, 1987; Michael Rutter, 2013). Several overlapping theoretical models based on evolutionary biology have been proposed to explain these seemingly contradictory patterns of stress reactivity. The ‘adaptive calibration’ model (Del Giudice, Ellis, & Shirtcliff, 2011), an extension of the ‘biological sensitivity to context’ theory (Boyce & Ellis, 2005), posits that childhood adversity may impact responses to stress in a nonlinear pattern to optimize fit with the expected future environment. For children who grow up with moderate stress exposure, a dampened stress response system may be advantageous to buffer the negative effects of stress (Ruttle et al., 2011), sometimes called a “steeling effect.” However, if the environment is characterized by more extreme levels of stress characterized by danger and unpredictability, a heightened sensitivity to threat may be more advantageous for survival in the short-term, although this response style may contribute to long-term consequences in psychological health (Frankenhuis & Del Giudice, 2012).
Tests of the adaptive calibration model in humans are still emerging, but a number of studies have provided support for a physiological “steeling effect” resulting from moderate early stress exposure (Del Giudice, Hinnant, Ellis, & El-Sheikh, 2012; Ellis, Oldehinkel, & Nederhof, 2017; Gunnar, Frenn, Wewerka, & Van Ryzin, 2009). Similar patterns of findings are emerging for studies measuring psychological/emotional responses to stress. For example, a longitudinal study of 163 adolescents found that individuals exposed to moderate life stress in childhood (e.g., parent-child conflict, parental hardship) had reduced risk for depression in the context of later environmental stressors than adolescents with few early stress exposures (Shapero et al., 2015). Although it is possible that these effects were influenced by differences in self-reporting of depression by individuals exposed to moderate life stress, these results suggest that some childhood adversity may promote ‘resilience’ to later depression by promoting adaptive psychological responses to stress. Similarly, a national sample of adults found that individuals with moderate lifetime adversity were less affected psychologically by adverse events in adulthood than individuals with zero or high levels of previous adversity (Seery, Holman, & Silver, 2010). Although no studies have compared linear versus quadratic models of stress sensitization specifically during the pregnancy period, these results suggest that when measuring a full range of exposures, some types of early adversity may influence prenatal emotional outcomes in a nonlinear pattern. For example, some studies have reported nonlinear associations between the threat-domain of adversity and later socioemotional outcomes; moderate harsh parenting has been linked with lower offspring behavioral problems in some studies of African-American youth, whereas severe violence exposure and maltreatment is linked with elevated psychological problems (Deater-Deckard & Dodge, 1997; Ripoll-Núñez & Rohner, 2006; Simons, Wu, Lin, Gordon, & Conger, 2000). Thus, studies that test both linear and nonlinear models are needed to clarify how best to operationalize and statistically model the long-term influence of early adversity on prenatal emotional distress.
Intimate Partner Violence
Together, studies based on stress sensitization and the adaptive calibration model highlight the importance of considering the joint contributions of early adversity and concurrent stressors when predicting emotional distress during pregnancy. One of the most common serious stressors experienced during pregnancy is intimate partner violence (IPV), including physical violence (e.g., hitting, punching, slapping) and emotional abuse (e.g., verbal abuse, frequent humiliation; Centers for Disease Control, 2018). At least 3-15% of women experience IPV during pregnancy (Bailey, 2010), and pregnant women living in low-income environments and those who are unmarried have even greater risk (10-36%; Alhusen, Lucea, Bullock, & Sharps, 2013; Bailey & Daugherty, 2007; Taillieu & Brownridge, 2010). IPV during pregnancy can have serious implications for both maternal and offspring health (Alhusen, Frohman, & Purcell, 2015; Alhusen, Ray, Sharps, & Bullock, 2015), and these risk processes may be particularly heightened for women who already have a history of early victimization (Narayan, Hagan, Cohodes, Rivera, & Lieberman, 2016). Compared to women who have not experienced IPV, victims of IPV are three times more likely to experience major depressive disorder (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012) and nearly three times more likely to be diagnosed with an anxiety disorder (Bonomi et al., 2009). Most studies of IPV have focused on physical violence exposure, but emotional abuse is more prevalent (Smith et al., 2018) and may be linked to more severe depression symptoms (Martin et al., 2006; Pico-Alfonso et al., 2006). Few studies, however, have distinguished the relative impact of these IPV subtypes on prenatal mental health or considered how these effects may differ for women with and without a history of adversity. Importantly, from a biological stress sensitization perspective, re-exposure effects may be even more powerful during pregnancy due to changes in reproductive hormones that also influence maternal responses to stress (Brummelte & Galea, 2010).
Present Study
Although maternal emotional distress during pregnancy is likely influenced by both maternal history of adversity and concurrent stressors during pregnancy, few studies have had the capacity to prospectively examine how different subdomains of early adversity interact with traumatic stressors during pregnancy to influence prenatal emotional distress. Our study is based on a large population-based sample of urban-living women who were assessed annually from age 8-17 for a range of adversity domains, including traumatic violence exposure (e.g., sexual assault, victim of violent crime), harsh parenting (e.g., corporal punishment, psychological aggression), caregiver loss (e.g., caregiver separation or incarceration), and compromised parenting (e.g., parent depression, parent substance abuse). The present study aimed to examine the linear and nonlinear associations between these differentiated domains of adversity and prenatal depression and anxiety symptoms in a subsample of pregnant women between the ages of 18-24.
We hypothesized that the association between childhood threat-based adversity (i.e., traumatic violence) and prenatal emotional distress would be moderated by physical and emotional IPV during pregnancy in a linear pattern consistent with stress sensitization theory. For history of harsh parenting, a more moderate and common threat-based stressor, we expected a nonlinear association such that some history of harsh parenting would predict decreased associations between prenatal IPV and emotional distress, but that high levels of harsh parenting would predict heightened emotional distress in response to prenatal IPV. Given the dearth of literature specific to other subdomains of adversity, we did not make any directional hypotheses for loss or compromised parenting but expected the patterns of interactions between prenatal IPV and these early adversity domains to differ from interactions with early threat exposure.
Method
Sample and Procedures
Participants were drawn from an ongoing longitudinal study of 2,450 urban-living women, who were initially recruited in childhood (citation masked for review). The original sample was identified in 1999-2000 based on a stratified, random household sampling of 103,238 city households that oversampled low-income neighborhoods. In wave 1, the girls were relatively evenly distributed across four age cohorts (5, 6, 7 and 8 years old), and the sample was racially diverse (52% African-American, 41% European American, 7% multiracial or other), with 39% of households receiving public assistance. Since then, participants have been assessed annually in the home, and sample retention has remained very high over the past 17 years (mean = 89%). The present study employed prospectively gathered measures of early adversity from age 8 (youngest age with full participant data) through age 17.
Participants in the primary analyses included a subsample of 200 young pregnant women (aged 18-24) who delivered a live birth while participating in the larger longitudinal study. To assess emotional distress and IPV exposure during pregnancy, data from the assessment wave immediately prior to each participant’s date of delivery were identified. Participants were included in analyses if they had completed their annual interview while pregnant and were aged 18 years or older during their assessment. Pregnancy data from the first birth were used for women with multiple births since age 18. Although exact gestational age data were unavailable, the mean length of time between the pregnancy assessment and baby’s date of birth was 19.26 weeks (SD = 11.23; range = 0.50-39.93), with approximately 31% of women assessed in their first trimester, 26% in the second trimester, and 33% in their third trimester of pregnancy. Compared to the original sample, women in this pregnant subsample were significantly more likely than non-participants to be of minority race (79.5%; χ2=38.70, p < .001), they received more years of public assistance (t = 4.46, p < .001), and experienced significantly more early life stressors from age 8-17, including more exposure to violent trauma (t = 3.53, p = .001), harsh parenting (t = 2.84, p =.005), and compromised parenting (t = 2.24, p =.026).
All study procedures were approved by the Institutional Review Board. Prior to data collection at each time point, written informed consent was obtained. Caregivers provided written consent and participants provided verbal assent prior to age 18, after which participants provided their own written consent. Trained interviewers collected interview data separately from participants and caregivers during annual home visits using laptop computers. Interview data regarding parent incarceration were additionally supplemented by official records from publicly-accessible criminal justice system dockets (link masked for review). Families received a monetary reimbursement for their research participation.
Measures
Childhood adversity
Data on childhood adversity were prospectively gathered annually from ages 8-17 based on self-report, parent-report, and available legal records. See Table 1 for an overview of the measures, items, and criteria used to assess each domain of adversity. Ten total ACE variables were measured: five exposures (parent depression, substance use, domestic violence, caregiver separation, parent incarceration) corresponded directly to the traditional ACE categories (Centers for Disease Control and Prevention, 2016). Measures of corporal punishment (e.g., spanking, hitting), psychological aggression (e.g., yelling), and sexual assault (by peers or adults) were collected as related proxies for the three traditional ACE categories of physical abuse, emotional abuse, and sexual abuse, respectively. Two additional experiences reflecting exposure to community violence were also included due to its relevance to this high-risk urban sample (Cronholm et al., 2015). Each ACE was first coded as present or absent during each year of assessment based on criteria summarized in Table 1, and scores were summed to produce the total number of years exposed to each ACE from ages 8-17. An ‘or rule’ was used when multiple informant data were available, e.g., participants were coded as exposed to an ACE if either the parent or child endorsed exposure that year. To account for study attrition, we used the proportion of years exposed to each ACE out of the total number of years the child participated in the study from age 8-17 for analyses. Based on these 10 total ACEs, the present study differentiated between four subdomains of adversity based on subscales empirically identified in the full population-based sample using a principal component analysis (components with eigenvalues > 1 and item loadings > .40). Adversity scores within each subscale were summed to reflect the number and duration of adversity exposures in that subdomain, including: (1) violent trauma (i.e., sexual assault, victim of violent crime, witnessed violent crime), (2) harsh parenting (i.e., corporal punishment, psychological aggression), (3) compromised parenting (i.e., parent depression, substance use, domestic violence), and (4) caregiver loss/separation (i.e., caregiver separation, parent incarceration).
Table 1.
Adverse childhood experiences (ACEs) assessed annually from age 8-17
| Adversity domain and ACEs included | Sample items | Measures (Informant a/# items) | Criteria | Prevalence (N=200) | Traditional ACE criteria for comparison b (CDC, 2016) |
|---|---|---|---|---|---|
| 1. Violent Trauma | |||||
| Sexual assault | Victim of statutory rape or forcible rape, sexually molested, sexually assaulted, someone touched your private parts when didn’t want them to, took pictures of private parts, made to touch others’ private parts, made to watch sex | ABUQ (C/4) CPSS (C/4) CPC (P/4, C/3) |
Any sexual assault item endorsed in past year | 12% | Sexual abuse: An adult, relative, family friend, or stranger who was at least 5 years older than you ever touched or fondled your body in a sexual way, made you touch his/her body in a sexual way, attempted to have any type of sexual intercourse with you |
| Victim of violent crime | Physically assaulted, badly hurt/nearly killed, or victim of homicide, robbery, aggravated assault, other assault, or shooting including drive by | CPSS (C/5) CPC (C/3, P/4) |
Any violent victimization item endorsed in past year | 18% | Not included in traditional ACE list |
| Witnessed violent crime | Saw someone killed, murdered, beaten, loved one badly hurt/nearly killed, or witnessed homicide, robbery, aggravated assault, other assault, or shooting including drive by | CPSS (C/4) CPC (C/3, P/4) |
Any witnessing of violence item endorsed in past year | 31% | Not included in traditional ACE list |
| 2. Harsh Parenting | |||||
| Corporal punishment | Frequency that any parent hit or spank child | CTS-PC (P/1 C/2) | Spanking or hitting endorsed as “often” by parent or child in the past year | 35.5% | Physical abuse: An adult living in your home pushed, grabbed, slapped, threw something at you, or hit you so hard that you had marks or were injured |
| Psychological aggression | Parent threatens to hit, shouts, swears, calls names, or threatens to kick out | CTS-PC (C/10, P/5) | Parent or child endorsed 3 or more psychologically aggressive behaviors as “often” occurring in the past year | 61% | Emotional abuse: A parent, stepparent, or adult living in your home swore at you, insulted you, put you down, or acted in a way that made you afraid that you might be physically hurt |
| 3. Compromised Parenting | |||||
| Parent depression | Depression symptoms, e.g., “I am sad all the time,” “I would like to kill myself,” “I have lost most of my interest in other people or things” | BDI (P/21) | Parent’s depression clinical severity score was “moderate” or “severe” | 35.5% | Household member was depressed or mentally ill or attempted suicide |
| Parent substance abuse | Alcohol use disorder symptoms keyed to DSM-IV, e.g., “how often do you have a drink containing alcohol?” “has a relative, friend, or doctor ever been concerned about your drinking or suggested you cut down?”; Frequency of using marijuana, cocaine, stimulants, sedatives, opioids, or hallucinogens | AUDIT (P/10) SUI (P/6) |
Parent scored above published cutoff for AUDIT alcohol problem or endorsed use of any “street drugs” on SUI | 40.5% | Household member was a problem drinker or alcoholic or a household member used street drugs |
| Parent domestic violence | Victim of domestic violence; endorsed physical abuse by partner; Number of times either caregiver threatened to hit or throw something at partner, threw, smashed, hit, or kicked something, slapped partner | CPC (P/4, C/3) DLC (P/1) CTS-2 (P/6) |
Police contact for domestic violence or mother reported being physically hurt by partner or any CTS-2 items occurred “more than 5 times” in the past year | 27.5% | Caregiver was pushed, grabbed, slapped, had something thrown at her, kicked, bitten, hit with a fist, hit with something hard, repeatedly hit for over at least a few minutes, or ever threatened or hurt by a knife or gun by partner |
| 4. Caregiver Loss | |||||
| Caregiver separation | Was there a change in caregivers in past year? | DQ (P/1) | Any change in caregiver | 13% | Your parents were ever separated or divorced |
| Parent incarceration | Court record of caregiver incarceration; “Is your partner in jail?” | Court records (R) DLC (P/1) |
Any records of incarceration or parent reported partner is in jail | 16% | Household member went to prison |
Note.
Informant: C = child, P = parent, R = records.
Criteria for the most similar ACE from the CDC list is included for comparison.
Note that the current study did not formally assess physical, sexual, or emotional abuse. Measures in alphabetical order: ABUQ = Abuse Questionnaire (Keenan, Hipwell, & Stouthamer-Loeber, 2004) , AUDIT = Alcohol Use Disorders Identification Test (Babor, de la Fuente, Saunders, & Grant, 1989), BDI = Beck Depression Inventory-II (Beck, Steer, & Brown, 1996), CPC = Child Police Contact (Loeber, Farrington, Stouthamer-Loeber, & Van Kammen, 1998), CPSS = Child PTSD Symptom Scale (Foa et al., 2001), CTS-2 = Conflict Tactics Scale - Revised (Straus et al., 1996), CTS-PC = Parent-Child Conflict Tactics Scale (Straus, Hamby, Finkelhor, Moore, & Runyan, 1998), DLC = Difficult Life Circumstances (Barnard, 1988), DQ = Demographics questionnaire (study-specific), SUI = Substance Use Inventory (White, Hipwell, & Mizelle, 2002).
Prenatal IPV
During pregnancy, women were evaluated for exposure to IPV using the Conflict Tactics Scale-2 (CTS-2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). Women first answered if they had romantic relationships in the past year, and women with no partners in the past year (n = 41) were coded as ‘no IPV.’ Women with at least one partner in the past year then rated items on the frequency of exposure to any intimate partner violence on 7-point scales (0 = this never happened to 6 = more than 20 times in the past year). The CTS-2 includes subscales that have been validated in community-based samples of women (Yun, 2011), including physical and psychological abuse across multiple levels of severity. The present study used the total psychological aggression construct as a continuous variable (sum of 8 items; e.g., “shouted or yelled at me,” “threatened to hit me”) to represent the severity of emotional IPV. Physical IPV was measured using the physical assault minor severity construct (5 items; e.g., “pushed/shoved,” “slapped,” “twisted my arm”). Given the low frequency of physical assault items endorsed, physical assault was dichotomized to represent the presence (14.8%) or absence (85.2%) of any physical IPV in the past year.
Prenatal emotional distress
Symptoms of emotional distress were assessed using the Adult Self-Report Inventory-4 (Gadow, Sprafkin, & Weiss, 2004), which includes DSM-IV symptoms of major depressive disorder and generalized anxiety disorder (American Psychiatric Association, 2000). Eight items corresponded to the eight symptoms of generalized anxiety disorder and were scored on a 4-point Likert scale (0 = never to 3 = very often). For depression, participants rated the frequency of DSM symptoms of major depressive disorder plus two related symptoms: low self-esteem and hopelessness. Seven symptoms were rated on the 4-point Likert scale, whereas four symptoms (change in appetite, sleep, activity, and concentration) were scored as 0.5 = absent or 2.5 = present. Scores were initially summed to form separate depression and anxiety scales (Gadow et al., 2004). The ASRI-4 depression and anxiety scales demonstrate convergent and discriminant validity and have been shown to differentiate between clinical and non-clinical samples (Gadow et al., 2004). Reflecting the frequent comorbidity between prenatal anxiety and depression, the anxiety and depression scales in the ASRI-4 were strongly correlated (r = .66, p < .05). To preserve parsimony, the scales were combined to create a total emotional distress scale.
Covariates
Severity of childhood depression and anxiety were assessed annually in childhood and adolescence based on parent and child reports. From age 10-17, children and their caregivers completed the Child Symptom Inventory-4 (CSI-4; Gadow & Sprafkin, 1994), a child version of the ASRI-4. Similar to the ASRI-4, parents and children rated symptoms of major depressive disorder plus two related symptoms (low self-esteem and hopelessness). Seven symptoms were rated on a 4-point Likert scale and considered present if either parent or child rated the symptom as occurring for the child “a lot” or “all the time”, whereas four symptoms (change in appetite, sleep, activity, concentration) were answered as present or absent. We included the average number of depression symptoms from age 10-17 in the analysis. Childhood anxiety was assessed from age 8-17 using the Screen for Child Anxiety and Related Emotional Disorders (SCARED; Birmaher et al., 1997). Parents and children rated 29 items about the child’s anxiety symptoms on a 3-point Likert scale (0 = not true or hardly ever true to 2 = very true), including nine items keyed to DSM criteria for generalized anxiety disorder. The total generalized anxiety score averaged from age 8-17 was included in models of prenatal anxiety as a covariate. Post-traumatic stress disorder (PTSD) symptoms were assessed using the Child PTSD Symptom Scale (CPSS; Foa et al., 2001), a 24-item scale keyed to DSM criteria for PTSD. Participants were first asked about any exposure to a traumatic event in the past year; positive endorsement of at least one traumatic event were followed up by rating the frequency of PTSD symptoms on a 4-point Likert scale (0 = not at all, 1 = once a week or less, 2 = 2-4 times a week, and 3 = 5 or more times a week). PTSD total scores from the year of pregnancy were included in analyses to covary for co-occurring PTSD. Given that ACEs are correlated with poverty (Evans, 2004) and minority race status (Roxburgh & MacArthur, 2014), we coded each participant’s exposure to childhood poverty, measured as the proportion of years that the family received public assistance out of the total number of years the family participated in the study from age 8-17, as well as minority race (non-White) status. Age at the time of conception was approximated by subtracting 40 weeks from the woman’s age at date of delivery. Education level was measured as the total number of years of schooling completed by conception. Given that women reporting no intimate partners during their pregnancy may have experienced additional stress from lack of a partner, we included presence of intimate partner as a covariate.
Data Analytic Plan
All analyses were conducted in Stata 13 using full information maximum likelihood (FIML) estimation with robust standard errors to handle missing data. Of the 200 women in our sample, 86% had complete data including all primary variables and covariates; most variables included in the study (e.g., all adversity and IPV variables) did not have any missing data, with variable missingness ranging from 0-23%. Compared to other methods of handling missing data (e.g., listwise or pairwise deletion, mean imputation), FIML produces significantly less biased parameter estimates and decreases Type 1 error (Collins, Schafer, & Kam, 2001). All adversity and IPV variables were centered prior to generating interaction terms to aid interpretation of parameter estimates.
In the first regression step, prenatal emotional distress was regressed on the linear and quadratic effects of the four adversity domains (violent trauma, harsh parenting, compromised parenting, and caregiver loss) as well as the main effects of prenatal physical and emotional IPV, controlling for childhood anxiety, childhood depression, childhood poverty, minority race, age cohort, age at conception, education level, prenatal PTSD symptoms, and presence of intimate partner as covariates. Next, in we tested each adversity subdomain’s interaction with physical and emotional IPV while controlling for the main effects of any other adversity domain. Given that analyses included four full models reflecting each early adversity domain, a Bonferroni correction was used to interpret the significance of results (threshold of p < .0125) to reduce the chance of Type 1 error due to multiple testing. Power analyses based on our sample size of n = 200 were conducted to aid interpretation of effect sizes (Soper, 2019), confirming sufficient power (.80) to detect medium effect sizes (f2≥.16) at the Bonferroni-adjusted probability level of p = .0125.
Significant early adversity × prenatal physical IPV interactions were probed by examining the linear and quadratic simple slopes of the adversity variable on prenatal emotional distress for women with and without physical IPV exposure during pregnancy. Following standard guidelines for continuous moderators, significant interactions by prenatal emotional IPV were probed based on standard deviation at 0 = −1 SD (‘no emotional IPV’), 1 = grand mean (‘moderate IPV’), 2 = +1 SD (‘high IPV’) (West & Aiken, 1991). In addition, regions of significance were identified to reveal the specific threshold of the moderator (emotional IPV) in which the association between adversity and prenatal emotional distress became significant (Preacher, Curran, & Bauer, 2006).
Results
Preliminary analyses
Descriptive statistics and bivariate correlations among study variables are shown in Table 2. Compared to population averages of ACES (Centers for Disease Control and Prevention, 2016), our sample had higher rates of childhood exposure to compromised parenting (i.e., parent depression, substance use, and domestic violence). Corporal punishment and psychological aggression were more frequent in our sample compared to population rates of physical and emotional abuse, likely due to the less severe nature of our measures. Rates of traumatic sexual violence history were comparable to other studies of pregnant women with similar racial and socioeconomic backgrounds (Chung et al., 2010), although our sample included higher rates of community violence exposure. Rates of separation through parent incarceration were higher in our sample than in the general population (Centers for Disease Control and Prevention, 2016), but other forms of caregiver separation (e.g., divorce) were lower, potentially due to the high rate of single mothers in our sample. Rates of IPV during pregnancy in our sample were congruent with statistics reported in other studies (Bailey, 2010), but somewhat lower than some studies that focused specifically on low-income women (Alhusen, Lucea, Bullock, & Sharps, 2013; Bailey & Daugherty, 2007; Taillieu & Brownridge, 2010). Finally, the mean score of emotional distress in our sample was slightly higher than symptom scores reported in mixed gender community samples (Sprafkin, Gadow, Weiss, Schneider, & Nolan, 2007), which may reflect higher rates of anxiety and depression in women compared to men.
Table 2.
Descriptive statistics and bivariate correlations among study variables
| M(SD) or % | Range | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Minority race | 79.5% | -- | 1 | ||||||||||||||
| 2. | Childhood poverty | .45 (.36) | 0-1.00 | .25* | 1 | |||||||||||||
| 3. | Violent trauma | .09 (.13) | 0-0.67 | .08 | .08 | 1 | ||||||||||||
| 4. | Harsh parenting | .22 (.24) | 0-1.00 | .09 | .03 | .25* | 1 | |||||||||||
| 5. | Compromised parenting | .32 (.43) | 0-1.80 | .06 | .20* | .19* | .24* | 1 | ||||||||||
| 6. | Caregiver loss | .04 (.09) | 0-0.56 | .07 | .08 | .12 | .03 | .13 | 1 | |||||||||
| 7. | Childhood anxiety | 5.05 (2.35) | 0.35-11.58 | .02 | .12 | .18* | .30* | .34* | .08 | 1 | ||||||||
| 8. | Childhood depression | 2.22 (1.26) | 0.13-6.38 | .01 | .13 | .31* | .33* | .29* | .03 | .58* | 1 | |||||||
| 9. | Age at conception | 19.76 (1.28) | 17.96-23.71 | .02 | −.02 | −.01 | .12 | .03 | .11 | −.03 | −.04 | 1 | ||||||
| 10. | Education (years) | 11.94 (1.13) | 8-15 | .04 | −.22* | −.09 | .13 | −.09 | .01 | .01 | −.03 | .27* | 1 | |||||
| 11. | Prenatal PTSD | 0.34 (2.45) | 0-28 | .04 | .01 | .13 | .10 | .02 | .13 | .18* | .20* | −.04 | .03 | 1 | ||||
| 12. | Intimate partner | 79.5% | -- | −.07 | −.04 | −.21* | .02 | −.08 | −.06 | −.15* | −.05 | .16* | .13 | −.12 | 1 | |||
| 13. | Prenatal physical IPV | 15.0% | -- | .11 | .00 | −.04 | .04 | .03 | −.02 | .02 | .11 | .09 | .05 | −.01 | .21* | 1 | ||
| 14. | Prenatal emotional IPV | 6.46 (7.04) | 0-36 | .11 | −.08 | −.12 | .11 | −.01 | −.04 | .03 | .12 | .17* | .06 | −.05 | .47* | .59* | 1 | |
| 15. | Prenatal emotional distress | 14.62 (8.17) | 0-41 | −.10 | −.02 | .01 | .14 | .06 | −.03 | .30* | .38* | .08 | −.06 | .22* | .01 | .22* | .27* | 1 |
Note.
p < .05
Exposure to violent trauma, harsh parenting, and compromised parenting were correlated with childhood anxiety and depression severity. Childhood anxiety and depression, in turn, were significantly correlated with prenatal emotional distress. On a bivariate level, early adversity domains were not linearly correlated with emotional distress during pregnancy, supporting the need to examine nonlinear associations and moderating effects of prenatal stress. Both physical and emotional IPV during pregnancy were significantly and positively correlated with prenatal emotional distress. Finally, none of the early adversity variables (independent variables) were associated with prenatal physical or emotional IPV (moderator variables), suggesting that significant interactions predicting prenatal emotional distress are not purely due to victims of IPV having more severe histories of adversity.
Predicting prenatal emotional distress
Physical IPV
Regression results appear in Table 3. Controlling for all covariates, physical IPV significantly moderated the nonlinear association between history of harsh parenting and prenatal emotional distress (Figure 1), even after accounting for Bonferroni correction. Specifically, history of harsh parenting in childhood did not predict later prenatal emotional distress for women without concurrent prenatal physical IPV exposure (B = 1.72, SE = 8.67, p =.843), whereas history of harsh parenting was associated with prenatal emotional distress in a positive quadratic pattern for women re-exposed to physical violence during pregnancy (B = 81.78, SE = 25.16, p =.001). As shown in Figure 2, stress sensitization for women re-exposed to violence during pregnancy was characterized by a positive quadratic pattern, such that moderate levels of harsh parenting in childhood decreased prenatal emotional distress during pregnancy, whereas a history of frequent harsh parenting increased risk for prenatal emotional distress. The moderating effect of physical IPV was specific to the association between history of harsh parenting and prenatal emotional distress; physical IPV did not interact with history of violent trauma, compromised parenting, or caregiver loss.
Table 3.
Linear regressions predicting prenatal emotional distress from early adversity domains, prenatal IPV, and their interactions
| B (SE) | β | p | |
|---|---|---|---|
| Violent trauma (VT) | |||
| VT | −2.57 (7.23) | −0.03 | .722 |
| VT 2 | −10.63 (22.41) | −0.08 | .635 |
| Prenatal physical IPV | 4.57 (2.42) | 0.22 | .070 |
| Prenatal emotional IPV | .11 (0.13) | 0.09 | .384 |
| VT × Physical IPV | 22.66 (24.90) | 0.12 | .363 |
| VT2 × Physical IPV | −169.97 (103.01) | −0.25 | .099 |
| VT × Emotional IPV | −1.15 (1.28) | −0.12 | .372 |
| VT2 × Emotional IPV | 12.78 (4.20) | 0.31 | .002 |
| Harsh parenting (HP) | |||
| HP | −2.23 (3.17) | −0.06 | .482 |
| HP 2 | 13.72 (7.03) | 0.14 | .051 |
| Prenatal physical IPV | −1.91 (2.38) | −0.09 | .422 |
| Prenatal emotional IPV | 0.14 (0.12) | 0.11 | .265 |
| HP × Physical IPV | −29.34 (9.10) | −0.34 | .001 |
| HP2 × Physical IPV | 80.06 (29.31) | 0.39 | .006 |
| HP × Emotional IPV | −0.23 (0.50) | −0.07 | .651 |
| HP2 × Emotional IPV | 1.62 (1.35) | 0.16 | .229 |
| Compromised parenting (CP) | |||
| CP | −1.95 (1.95) | −0.09 | 0.318 |
| CP 2 | 1.96 (2.44) | 0.04 | 0.422 |
| Prenatal physical IPV | 1.65 (2.23) | 0.07 | 0.461 |
| Prenatal emotional IPV | 0.17 (0.13) | 0.13 | 0.201 |
| CP × Physical IPV | 0.02 (6.80) | −0.02 | 0.998 |
| CP2 × Physical IPV | 0.38 (6.54) | <.01 | 0.954 |
| CP × Emotional IPV | −0.03 (0.34) | −0.02 | 0.926 |
| CP2 × Emotional IPV | 0.67 (0.45) | 0.20 | 0.134 |
| Caregiver loss (CL) | |||
| CL | 9.04 (12.40) | 0.14 | 0.466 |
| CL 2 | −56.33 (52.77) | −0.20 | 0.286 |
| Prenatal physical IPV | 0.38 (3.69) | 0.02 | 0.919 |
| Prenatal emotional IPV | 0.32 (0.12) | 0.27 | 0.007 |
| CL × Physical IPV | −51.55 (69.94) | −0.17 | 0.461 |
| CL2 × Physical IPV | 223.97 (346.40) | 0.12 | 0.518 |
| CL × Emotional IPV | 2.32 (1.89) | 0.16 | 0.222 |
| CL2 × Emotional IPV | −8.38 (7.10) | −0.16 | 0.238 |
Note. B = unstandardized coefficient. β = standardized coefficient. Significant interactions after Bonferroni correction (threshold p < .0125) are bolded for emphasis. Each model included the following covariates: age cohort, minority race, childhood anxiety, childhood depression, childhood poverty, education level at conception, age at conception, presence of intimate partner during pregnancy, co-occurring PTSD symptoms during pregnancy, and other subscales of early adversity.
Figure 1.
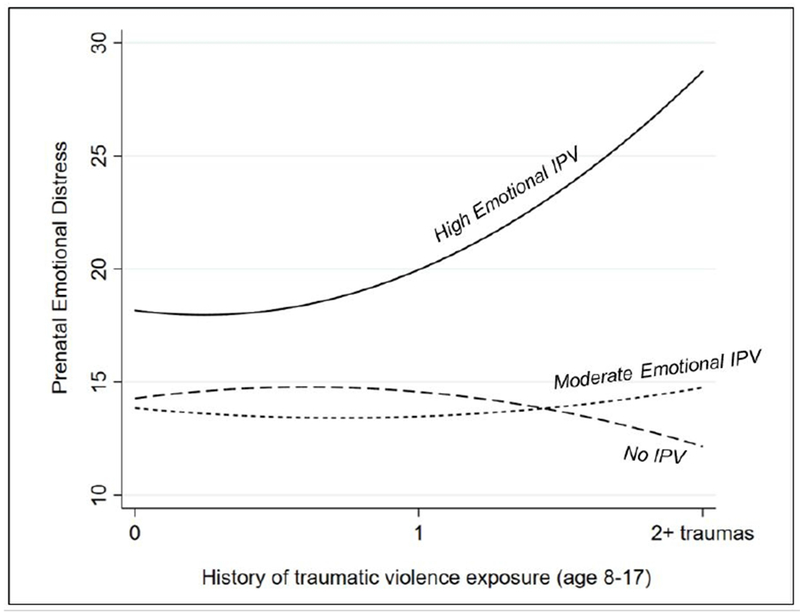
Emotional IPV during pregnancy moderated the nonlinear association between history of traumatic violence and prenatal emotional distress. For ease of interpretability, history of traumatic violence exposure in the figure above represents the total number of traumatic exposures from age 8-17 (recoded from the proportion score sums used in analyses).
Figure 2.
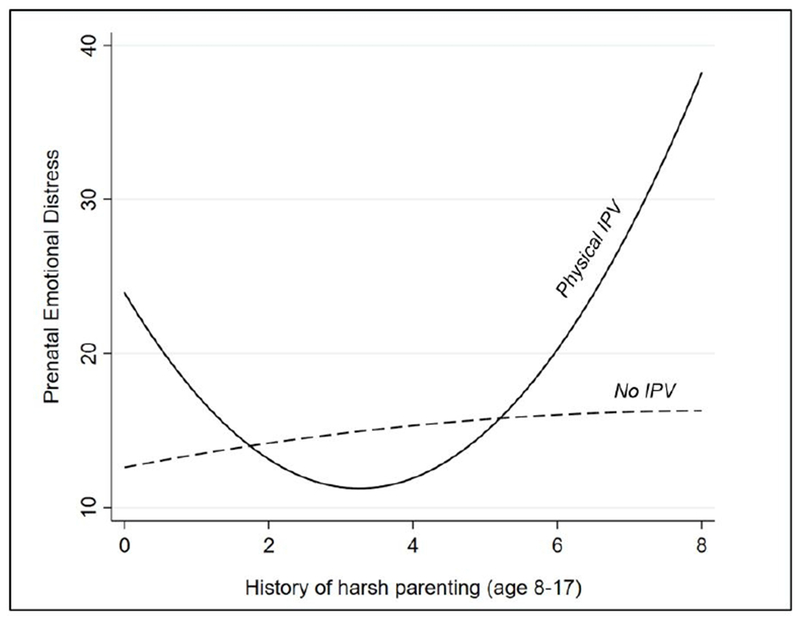
Physical IPV during pregnancy moderated the nonlinear association between history of harsh parenting and prenatal emotional distress. For ease of interpretability, history of harsh parenting in the figure above represents the total number of traumatic exposures from age 8-17 (recoded from the proportion score sums used in analyses).
Emotional IPV
Emotional IPV moderated the nonlinear association between history of violent trauma and prenatal emotional distress (Figure 2). Violent trauma history increased risk for prenatal emotional distress in a positive quadratic pattern, but only for women exposed to high levels of emotional IPV during pregnancy (B = 147.60, SE = 51.44, p =.004): as history of violent trauma increased, risk for prenatal emotional distress also increased, and the rate of increase accelerated significantly for women with history of multiple traumas. Specifically, regions of significance analyses revealed a significant nonlinear association between history of violent trauma and prenatal emotional distress for women whose emotional IPV score surpassed a score of 8 (sample mean = 6.46, SD = 7.04). In contrast, the effect of violent trauma history on prenatal distress was not significant for women exposed to average/moderate levels of emotional IPV (B = 22.54, SE = 22.22, p = .310). For women with no emotional IPV exposure during pregnancy, history of violent trauma was associated with prenatal anxiety in a negative quadratic pattern (B = −.102.51, SE = 42.54, p =.016), although changes in emotional distress were minimal from a clinical significance perspective (Figure 2). None of the other early adversity subdomains (i.e., harsh parenting, compromised parenting, caregiver loss) had a main effect nor interacted with emotional IPV to predict prenatal emotional distress.
Discussion
In a community-based sample of pregnant women assessed annually since childhood, this study investigated how exposure to physical and emotional IPV during pregnancy influenced the association between maternal history of adversity and later vulnerability to emotional distress during pregnancy. Whereas most studies of prenatal health focus exclusively on stressors during the pregnancy period, our study was guided by a lifespan model of pregnancy health and integrated both current stressors (physical and emotional IPV) and history of adversity (Misra et al., 2003). To reflect prevailing theories of stress sensitization, we modeled both linear and nonlinear effects of adversity (Boyce & Ellis, 2005; Del Giudice et al., 2011), differentiated between subdomains of adversity (McLaughlin & Sheridan, 2016), and rigorously controlled for potential confounding factors including history of poverty and childhood psychopathology. Several key findings emerged that were partially supportive of hypotheses: First, consistent with hypotheses, the associations between history of adversity and prenatal emotional distress were moderated by prenatal IPV, supporting a lifespan conceptualization of pregnancy health. Patterns of interactions were best characterized by nonlinear patterns and generally consistent with theories of ‘adaptive calibration’ (Boyce & Ellis, 2005; Del Giudice et al., 2011), such that moderate early stress appeared associated with a “steeling effect” whereas more extreme and traumatic stress magnified sensitivity to stress during pregnancy. However, results diverged based on subdomain of early adversity (e.g., threat vs. loss) and type of IPV.
Two aspects of the early adversity results were notable. First, although early adversity was significantly correlated with childhood anxiety and depression, none of the early adversity variables directly predicted prenatal emotional distress symptoms after accounting for childhood symptoms, demographic characteristics, and IPV exposure during pregnancy. Instead, early adversity only predicted later prenatal emotional distress when this vulnerability was ‘activated’ by later traumatic stress exposure during pregnancy. These results are consistent with psychophysiological studies of stress showing that the effects of early adversity on cortisol are more apparent during acute phases of the stress response (i.e., peak and recovery phases of lab-based stress tasks) versus baseline HPA axis functioning (e.g., resting cortisol; Bunea, Szentágotai-Tătar, & Miu, 2017). Results also point to the importance of considering patterns of stress continuity and discontinuity from preconception through pregnancy when evaluating risk for prenatal emotional distress. Given that most studies of prenatal health focus on stressors at single time-points, our findings highlight a need to examine environmental stress from a more dynamic perspective, considering the interplay between past and current environment.
Second, patterns of interactions differed between subdomains of adversity, such that significant interactions were specific to threat-based adversity (i.e., harsh parenting and traumatic violence), but did not generalize to experiences of caregiver loss/separation or exposure to compromised parenting. Specifically, history of harsh parenting and violent trauma predicted prenatal emotional distress only for women re-exposed to prenatal physical and emotional violence, respectively. Overall, these results are consistent with emerging literature indicating that different domains of adversity have unique influences on stress neurobiology (McLaughlin & Sheridan, 2016). Given that the present study focused specifically on threat during pregnancy (physical and emotional IPV), the specificity of the sensitization effects to childhood threat experiences may reflect a domain-specific pattern of stress sensitization. Most studies of early adversity conceptualize stress along a single dimension ranging from low to high severity, but the physiological stress response includes general- as well as stimulus-specific pathways (Vogel & Wagner, 2005). Individuals may be more likely to respond to adult stressors that resemble stressful events that were experienced in childhood, potentially through stimulus-specific social learning processes and/or the shaping of domain-specific schemas through early experience (Baldwin, 1992; Baldwin & Meunier, 1999; Pine et al., 2005). Although no studies to our knowledge have tested domain-specific patterns of stress sensitization during pregnancy, our results are consistent with a recent longitudinal study of African-American men and women that found childhood adversity to interact with adult adversity in a domain-specific fashion: childhood experiences of harsh parenting heightened the association between adult exposure to intimate partner hostility and chronic inflammation, whereas childhood discrimination specifically heightened inflammation responses to adult discrimination (Simons et al., 2019). These domain-specific patterns of stress sensitization may be particularly heightened during pregnancy, when emotions are influenced by rapid changes in reproductive hormones that directly influence maternal sensitivity to stress (Brummelte & Galea, 2010). Follow-up studies are needed to elucidate the specific physiological mechanisms underlying our results and to examine if patterns differ during the sensitive period of pregnancy.
Within the threat domain of adversity, patterns of interactions differed between severe traumatic threats (e.g., sexual assault, violent victimization) and more common experiences of harsh parenting (corporal punishment, psychological aggression). Starting at the lower end of the threat severity spectrum, harsh parenting was only associated with prenatal emotional distress for women re-exposed to physical violence during pregnancy. For these women, moderate levels of harsh parenting in childhood was associated with slightly lower levels of emotional distress during pregnancy, whereas a history of frequent and chronic harsh parenting increased risk for prenatal emotional distress. These curvilinear results are consistent with the adaptive calibration model (Del Giudice et al., 2011), in which mild to moderate stress in childhood appears to buffer later sensitivity to stress in adulthood through a “steeling effect” (Rutter, 2012). It is important to highlight that our results are specific to prenatal emotional distress (anxiety and depression symptoms). It is unclear if this steeling effect generalizes to other health outcomes. For example, some evidence suggests that there may be a physiological cost to adaptation and resilience, such that individuals who exhibit high psychosocial competence and few adjustment problems despite socioeconomic risk also have higher levels of allostatic load, a measure of physiological “wear and tear” on the body (Brody et al., 2013) . More research is needed to elucidate the mechanisms underlying the steeling effect observed in our study.
When examining the severe end of the threat-domain, history of traumatic violence, reexposure to emotional IPV (but not physical IPV) uniquely moderated vulnerability to emotional distress during pregnancy in a pattern consistent with stress sensitization theory. Specifically, the association between childhood trauma and prenatal emotional distress was significant only for women with a score above 8 (out of a maximum possible score of 48) on the emotional IPV scale. This was a relatively modest level of stress in our sample – only two points above the sample mean – suggesting that even a moderate level of verbal or psychological abuse from an intimate partner can activate stress sensitization effects from childhood exposure to traumatic violence. Furthermore, effects were nonlinear, such that risk for emotional distress accelerated rapidly for women with a history of multiple traumatic events. This was significant even after accounting for childhood history of anxiety and depression as well as co-occurring PTSD symptoms during pregnancy. These results highlight the importance of screening for history of violent traumas as well as current exposure to emotional IPV during pregnancy. Compared to physical IPV, emotional IPV is greatly understudied, despite being more prevalent (Smith et al., 2018). Our findings are consistent with some studies reporting that emotional IPV is more closely linked to depression symptoms than physical IPV (Martin et al., 2006; Pico-Alfonso et al., 2006), and further suggest that this may particularly be the case for women with a history of traumatic sexual or physical violence.
The results of this study should be interpreted in the context of several study limitations. First, IPV and prenatal emotional distress were measured concurrently, precluding temporal conclusions, although we did control for history of anxiety and depression as covariates to increase specificity to the pregnancy period. IPV and prenatal psychopathology likely reciprocally influence each other (Kessler, Molnar, Feurer, & Appelbaum, 2001), and future studies employing cross-lagged models of both constructs across a shorter time frame will help shed light on their association during the prenatal period. Second, although our study prospectively measured a variety of ACEs typically included in previous studies, measures of physical and emotional neglect were unavailable, and thus we cannot speak to the impact of early deprivation (McLaughlin & Sheridan, 2016). Furthermore, whereas other studies have focused on severe exposures to physical and sexual abuse, our measure of harsh parenting included a range of exposures including more common experiences (e.g., spanking), and our measure of sexual assault included any sexual violence (vs. being specific to sexual abuse by a family member); future studies must further differentiate between these factors when examining nonlinear effects of early adversity. Of note, although the adversity variables measured in our study were not correlated with prenatal IPV, other studies have reported links between severe adversity (e.g., maltreatment) and later risk for IPV (Castro, Peek-Asa, García, Ruiz, & Kraus, 2003; Huth-Bocks, Krause, Ahlfs-Dunn, Gallagher, & Scott, 2013). Future studies that include more specific measures of child abuse and neglect may find direct associations with prenatal IPV and can test alternative frameworks (e.g., prenatal IPV as a mediator between adversity and prenatal distress). In interpreting our results, it is important to note that our study focused on a relatively high-risk sample of young perinatal women. Although the focus on this understudied population is a strength of our study due to their elevated risk for prenatal health problems, our results may not generalize to other samples of women (e.g., older pregnant women, higher SES samples). Similarly, because we used a DSM-keyed measure of depression and anxiety symptom severity, our results may not capture effects of adversity on non-clinical measures of mood and anxiety. Finally, although our findings are consistent with theoretical models implicating a “steeling effect” of moderate harsh parenting exposure on later vulnerability to emotional distress, more work is needed before conclusions can be made about the implications of this profile. It is unclear from our study if stress-related adaptations to severe early adversity led to “inoculation” to later stressors during pregnancy (Rutter, 1987), or if this effect was accompanied by other social-emotional, behavioral, or physical health costs. Indeed, resilience is a dynamic process, and what appears to be protective in one context may not represent resilience in other contexts or for other outcomes (Michael Rutter, 2006; Wood & Bhatnagar, 2015). More studies that consider the dynamic nature of stress and characterize global outcomes are needed to better understand the implications of these individual differences in emotional distress during pregnancy.
Acknowledgements:
This project was supported by grants funded through the National Institute of Mental Health (MH056630, MH071790), the Eunice Kennedy Shriver Institute of Child Health and Human Development (HD067185) and the National Institute of Drug Abuse (DA012237). During the preparation of this manuscript, I.T. also received support from the National Institute on Alcohol Abuse and Alcoholism (T32AA00745). Special thanks go to the families of the Pittsburgh Girls Study for their participation in this research, and to our dedicated research team for their continued efforts.
References
- Alhusen JL, Frohman N, & Purcell G (2015). Intimate partner violence and suicidal ideation in pregnant women. Archives of Women’s Mental Health, 18(4), 573–578. 10.1007/s00737-015-0515-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alhusen JL, Lucea MB, Bullock L, & Sharps P (2013). Intimate partner violence, substance use, and adverse neonatal outcomes among urban women. The Journal of Pediatrics, 163(2), 471–476. 10.1016/jjpeds.2013.01.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alhusen JL, Ray E, Sharps P, & Bullock L (2015). Intimate partner violence during pregnancy: Maternal and neonatal outcomes. Journal of Women’s Health, 24(1), 100–106. 10.1089/jwh.2014.4872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association (APA). (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington: American Psychiatric Association. [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield C, Perry BD, … Giles WH (2006). The enduring effects of abuse and related adverse experiences in childhood. European Archives of Psychiatry and Clinical Neuroscience, 256(3), 174–186. 10.1007/s00406-005-0624-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Atkinson L, Beitchman J, Gonzalez A, Young A, Wilson B, Escobar M, … Villani V (2015). Cumulative risk, cumulative outcome: A 20-year longitudinal study. PloS One, 10(6), e0127650 10.1371/journal.pone.0127650 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Babor TF, de la Fuente JR, Saunders JB, & Grant M (1989). The alcohol use disorders identification test: Guidelines for use in primary health care. World Health Organization, Geneva. [Google Scholar]
- Bailey BA (2010). Partner violence during pregnancy: Prevalence, effects, screening, and management. International Journal of Women’s Health, 2, 183–197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey BA, & Daugherty RA (2007). Intimate partner violence during pregnancy: Incidence and associated health behaviors in a rural population. Maternal and Child Health Journal, 11(5), 495–503. 10.1007/s10995-007-0191-6 [DOI] [PubMed] [Google Scholar]
- Bailey JA, Hill KG, Guttmannova K, Oesterle S, Hawkins JD, Catalano RF, & McMahon RJ (2013). The association between parent early adult drug use disorder and later observed parenting practices and child behavior problems: Testing alternate models. Developmental Psychology, 49(5), 887–899. 10.1037/a0029235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baldwin MW. (1992). Relational schemas and the processing of social information. Psychological Bulletin, 112(3), 461–484. 10.1037/0033-2909.112.3.461 [DOI] [Google Scholar]
- Baldwin MW, & Meunier J (1999). The cued activation of attachment relational schemas. Social Cognition, 17(2), 209–227. 10.1521/soco.1999.17.2.209 [DOI] [Google Scholar]
- Barnard K (1988). Difficult Life Circumstances scale. University of Washington, Seattle. [Google Scholar]
- Beck AT, Steer RA, & Brown GK (1996). Beck Depression Inventory-II (BDI-II). San Antonio, TX: Psychological Corporation. [Google Scholar]
- Beydoun HA, Beydoun MA, Kaufman JS, Lo B, & Zonderman AB (2012). Intimate partner violence against adult women and its association with major depressive disorder, depressive symptoms and postpartum depression: A systematic review and meta-analysis. Social Science & Medicine (1982), 75(6), 959–975. 10.1016/j.socscimed.2012.04.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonomi AE, Anderson ML, Reid RJ, Rivara FP, Carrell D, & Thompson RS (2009). Medical and psychosocial diagnoses in women with a history of intimate partner violence. Archives of Internal Medicine, 169(18), 1692–1697. 10.1001/archinternmed.2009.292 [DOI] [PubMed] [Google Scholar]
- Boyce WT, & Ellis BJ (2005). Biological sensitivity to context: I. An evolutionary-developmental theory of the origins and functions of stress reactivity. Development and Psychopathology, 17(2), 271–301. 10.1017/S0954579405050145 [DOI] [PubMed] [Google Scholar]
- Brody GH, Yu T, Chen E, Miller GE, Kogan SM, & Beach SRH (2013). Is resilience only skin deep?: Rural African Americans’ socioeconomic status–related risk and competence in preadolescence and psychological adjustment and allostatic load at age 19. Psychological Science, 24(7), 1285–1293. 10.1177/0956797612471954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brummelte S, & Galea LAM (2010). Depression during pregnancy and postpartum: Contribution of stress and ovarian hormones. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 34(5), 766–776. https://doi.Org/10.1016/j.pnpbp.2009.09.006 [DOI] [PubMed] [Google Scholar]
- Bunea IM, Szentágotai-Tătar A, & Miu AC (2017). Early-life adversity and cortisol response to social stress: A meta-analysis. Translational Psychiatry, 7(12), 1274 10.1038/s41398-017-0032-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castro R, Peek-Asa C, García L, Ruiz A, & Kraus JF (2003). Risks for abuse against pregnant Hispanic women: Morelos, Mexico and Los Angeles County, California. American Journal of Preventive Medicine, 25(4), 325–332. https://doi.Org/10.1016/S0749-3797(03)00211-3 [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control. (2018, May 17). Intimate partner violence. Retrieved May 21, 2018, from https://www.cdc.gov/violenceprevention/intimatepartnerviolence/index.html
- Centers for Disease Control and Prevention. (2016). About the CDC-Kaiser ACE Study. Retrieved April 28, 2018, from https://www.cdc.gov/violenceprevention/acestudy/about.html
- Chartier MJ, Walker JR, & Naimark B (2010). Separate and cumulative effects of adverse childhood experiences in predicting adult health and health care utilization. Child Abuse & Neglect, 34(6), 454–464. 10.1016/jxhiabu.2009.09.020 [DOI] [PubMed] [Google Scholar]
- Chung EK, Nurmohamed L, Mathew L, Elo IT, Coyne JC, & Culhane JF (2010). Risky health behaviors among mothers-to-be: The impact of adverse childhood experiences. Academic Pediatrics, 10(4), 245–251. 10.1016/j.acap.2010.04.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins LM, Schafer JL, & Kam C-M (2001). A comparison of inclusive and restrictive strategies in modern missing data procedures. Psychological Methods, 6(4), 330–351. 10.1037/1082-989X.6A330 [DOI] [PubMed] [Google Scholar]
- Cronholm PF, Forke CM, Wade R, Bair-Merritt MH, Davis M, Harkins-Schwarz M, … Fein JA (2015). Adverse childhood experiences: Expanding the concept of adversity. American Journal of Preventive Medicine, 49(3), 354–361. 10.1016/j.amepre.2015.02.001 [DOI] [PubMed] [Google Scholar]
- Danese A, & McEwen BS (2012). Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiology & Behavior, 106(1), 29–39. 10.1016/j.physbeh.2011.08.019 [DOI] [PubMed] [Google Scholar]
- Deater-Deckard K, & Dodge KA (1997). Externalizing behavior problems and discipline revisited: Nonlinear effects and variation by culture, context, and gender. Psychological Inquiry, 8(3), 161–175. 10.2307/1448881 [DOI] [Google Scholar]
- Del Giudice M, Ellis BJ, & Shirtcliff EA (2011). The Adaptive Calibration Model of stress responsivity. Neuroscience & Biobehavioral Reviews, 35(7), 1562–1592. https://doi.Org/10.1016/j.neubiorev.2010.11.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Del Giudice M, Hinnant JB, Ellis BJ, & El-Sheikh M (2012). Adaptive patterns of stress responsivity: A preliminary investigation. Developmental Psychology, 48(3), 775–790. 10.1037/a0026519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunkel Schetter C, & Tanner L (2012). Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Current Opinion in Psychiatry, 25(2), 141–148. 10.1097/YC0.0b013e3283503680 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis BJ, & Boyce WT (2008). Biological sensitivity to context. Current Directions in Psychological Science, 17(3), 183–187. 10.1111/j.1467-8721.2008.00571.x [DOI] [Google Scholar]
- Ellis BJ, Oldehinkel AJ, & Nederhof E (2017). The adaptive calibration model of stress responsivity: An empirical test in the Tracking Adolescents’ Individual Lives Survey study. Development and Psychopathology, 29(3), 1001–1021. 10.1017/S0954579416000985 [DOI] [PubMed] [Google Scholar]
- Evans GW (2004). The environment of childhood poverty. The American Psychologist, 59(2), 77–92. 10.1037/0003-066X.59.2.77 [DOI] [PubMed] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, … Marks JS (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. 10.1016/S0749-3797(98)00017-8 [DOI] [PubMed] [Google Scholar]
- Foa EB, Johnson KM, Feeny NC, & Treadwell KRH (2001). The Child PTSD Symptom Scale: A preliminary examination of its psychometric properties. Journal of Clinical Child & Adolescent Psychology, 30(3), 376–384. 10.1207/S15374424JCCP3003_9 [DOI] [PubMed] [Google Scholar]
- Ford DC, Merrick MT, Parks SE, Breiding MJ, Gilbert LK, Edwards VJ, … Thompson WW (2014). Examination of the factorial structure of adverse childhood experiences and recommendations for three subscale scores. Psychology of Violence, 4(4), 432–444. 10.1037/a0037723 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frankenhuis WE, & Del Giudice M (2012). When do adaptive developmental mechanisms yield maladaptive outcomes? Developmental Psychology, 48(3), 628–642. 10.1037/a0025629 [DOI] [PubMed] [Google Scholar]
- Gadow KD, & Sprafkin J (1994). Child Symptom Inventories Manual. Stony Brook, NY: Checkmate Plus. [Google Scholar]
- Gadow KD, Sprafkin J, & Weiss MD (2004). Adult Self-Report Inventory-4 Manual. Stony Brook, NY: Checkmate Plus. [Google Scholar]
- Glaser J-P, van Os J, Portegijs PJM, & Myin-Germeys I (2006). Childhood trauma and emotional reactivity to daily life stress in adult frequent attenders of general practitioners. Journal of Psychosomatic Research, 61(2), 229–236. 10.1016/jjpsychores.2006.04.014 [DOI] [PubMed] [Google Scholar]
- Glynn LM, Howland MA, Sandman CA, Davis EP, Phelan M, Baram TZ, & Stern HS (2018). Prenatal maternal mood patterns predict child temperament and adolescent mental health. Journal of Affective Disorders, 228, 83–90. 10.1016/jjad.2017.11.065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gunnar MR (2000). Early adversity and the development of stress reactivity and regulation In Nelson CA (Ed.), The effects of early adversity on neurobehavioral development (Vol. 31, pp. 163–200). Psychology Press. [Google Scholar]
- Gunnar MR, Frenn K, Wewerka SS, & Van Ryzin MJ (2009). Moderate versus severe early life stress: Associations with stress reactivity and regulation in 10–12-year-old children. Psychoneuroendocrinology, 34(1), 62–75. 10.1016/j.psyneuen.2008.08.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammen C, Henry R, & Daley SE (2000). Depression and sensitization to stressors among young women as a function of childhood adversity. Journal of Consulting and Clinical Psychology, 68(5), 782–787. [PubMed] [Google Scholar]
- Hardt J, & Rutter M (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. 10.1111/j.1469-7610.2004.00218.x [DOI] [PubMed] [Google Scholar]
- Huang C-C, Wang L-R, & Warrener C (2010). Effects of domestic violence on behavior problems of preschool-aged children: Do maternal mental health and parenting mediate the effects? Children and Youth Services Review, 32(10), 1317–1323. 10.1016/j.childyouth.2010.04.024 [DOI] [Google Scholar]
- Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, … Dunne MP (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet. Public Health, 2(8), e356–e366. 10.1016/S2468-2667(17)30118-4 [DOI] [PubMed] [Google Scholar]
- Humphreys KL, & Zeanah CH (2015). Deviations from the expectable environment in early childhood and emerging psychopathology. Neuropsychopharmacology: Official Publication of the American College of Neuropsychopharmacology, 40(1), 154–170. 10.1038/npp.2014.165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hunter AL, Minnis H, & Wilson P (2011). Altered stress responses in children exposed to early adversity: A systematic review of salivary cortisol studies. Stress, 14(6), 614–626. 10.3109/10253890.2011.577848 [DOI] [PubMed] [Google Scholar]
- Huth-Bocks AC, Krause K, Ahlfs-Dunn S, Gallagher E, & Scott S (2013). Relational trauma and posttraumatic stress symptoms among pregnant women. Psychodynamic Psychiatry, 41(2), 277–301. 10.1521/pdps.2013.4L2.277 [DOI] [PubMed] [Google Scholar]
- Kalmakis KA, & Chandler GE (2015). Health consequences of adverse childhood experiences: A systematic review. Journal of the American Association of Nurse Practitioners, 27(8), 457–465. 10.1002/2327-6924.12215 [DOI] [PubMed] [Google Scholar]
- Karatekin C, & Hill M (2018). Expanding the Original Definition of Adverse Childhood Experiences (ACEs). Journal of Child & Adolescent Trauma. 10.1007/s40653-018-0237-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keenan K, Hipwell AE, & Stouthamer-Loeber M (2004). The Abuse Questionnaire. Pittsburgh Girls Study: University of Pittsburgh. [Google Scholar]
- Kessler RC, Molnar BE, Feurer ID, & Appelbaum M (2001). Patterns and mental health predictors of domestic violence in the United States: Results from the National Comorbidity Survey. International Journal of Law and Psychiatry, 24(4), 487–508. 10.1016/S0160-2527(01)00080-2 [DOI] [PubMed] [Google Scholar]
- Li Y, Long Z, Cao D, & Cao F (2017). Maternal history of child maltreatment and maternal depression risk in the perinatal period: A longitudinal study. Child Abuse & Neglect, 63(Supplement C), 192–201. 10.1016/j.chiabu.2016.12.001 [DOI] [PubMed] [Google Scholar]
- Loeber R, Farrington DP, Stouthamer-Loeber M, & Van Kammen WB (1998). Antisocial behavior and mental health problems: Risk factors in childhood and adolescence. Hillsdale, NJ: Lawrence Erlbaum. [Google Scholar]
- Lovallo WR, Farag NH, Sorocco KH, Cohoon AJ, & Vincent AS (2012). Lifetime adversity leads to blunted stress axis reactivity: Studies from the Oklahoma family health patterns project. Biological Psychiatry, 71(4), 344–349. 10.1016/j.biopsych.2011.10.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madigan S, Wade M, Plamondon A, Vaillancourt K, Jenkins JM, Shouldice M, & Benoit D (2014). Course of depression and anxiety symptoms during the transition to parenthood for female adolescents with histories of victimization. Child Abuse & Neglect, 38(7), 1160–1170. 10.1016/j.chiabu.2014.04.002 [DOI] [PubMed] [Google Scholar]
- Martin SL, Li Y, Casanueva C, Harris-Britt A, Kupper LL, & Cloutier S (2006). Intimate partner violence and women’s depression before and during pregnancy. Violence Against Women, 12(3), 221–239. 10.1177/1077801205285106 [DOI] [PubMed] [Google Scholar]
- McDonnell CG, & Valentino K (2016). Intergenerational effects of childhood trauma: Evaluating pathways among maternal ACEs, perinatal depressive symptoms, and infant outcomes. Child Maltreatment, 21(4), 317–326. 10.1177/1077559516659556 [DOI] [PubMed] [Google Scholar]
- McLaughlin KA, Conron KJ, Koenen KC, & Gilman SE (2010). Childhood adversity, adult stressful life events, and risk of past-year psychiatric disorder: A test of the stress sensitization hypothesis in a population-based sample of adults. Psychological Medicine, 40(10), 1647–1658. 10.1017/S0033291709992121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin Katie A., & Sheridan MA (2016). Beyond cumulative risk: A dimensional approach to childhood adversity. Current Directions in Psychological Science, 25(4), 239–245. 10.1177/0963721416655883 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin Katie A., Sheridan MA, & Lambert HK (2014). Childhood adversity and neural development: Deprivation and threat as distinct dimensions of early experience. Neuroscience & Biobehavioral Reviews, 47, 578–591. 10.1016/j.neubiorev.2014.10.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin Katie A., Sheridan MA, Tibu F, Fox NA, Zeanah CH, & Nelson CA (2015). Causal effects of the early caregiving environment on development of stress response systems in children. Proceedings of the National Academy of Sciences, 112(18), 5637–5642. 10.1073/pnas.1423363112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mersky JP, Topitzes J, & Reynolds AJ (2013). Impacts of adverse childhood experiences on health, mental health, and substance use in early adulthood: A cohort study of an urban, minority sample in the U.S. Child Abuse & Neglect, 37(11), 917–925. 10.1016/j.chiabu.2013.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mersky Joshua P., Janczewski CE, & Topitzes J (2017). Rethinking the measurement of adversity: Moving toward second-generation research on adverse childhood experiences. Child Maltreatment, 22(1), 58–68. 10.1177/1077559516679513 [DOI] [PubMed] [Google Scholar]
- Mezey G, Bacchus L, Bewley S, & White S (2005). Domestic violence, lifetime trauma and psychological health of childbearing women. BJOG: An International Journal of Obstetrics & Gynaecology, 112(2), 197–204. 10.1111/j.1471-0528.2004.00307.x [DOI] [PubMed] [Google Scholar]
- Misra DP, Guyer B, & Allston A (2003). Integrated perinatal health framework: A multiple determinants model with a life span approach. American Journal of Preventive Medicine, 25(1), 65–75. 10.1016/S0749-3797(03)00090-4 [DOI] [PubMed] [Google Scholar]
- Naicker SN, Norris SA, Mabaso M, & Richter LM (2017). An analysis of retrospective and repeat prospective reports of adverse childhood experiences from the South African Birth to Twenty Plus cohort. PLOS ONE, 12(7), e0181522 10.1371/journal.pone.0181522 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neger EN, & Prinz RJ (2015). Interventions to address parenting and parental substance abuse: Conceptual and methodological considerations. Clinical Psychology Review, 39, 71–82. 10.1016/j.cpr.2015.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neigh GN, Gillespie CF, & Nemeroff CB (2009). The neurobiological toll of child abuse and neglect. Trauma, Violence, & Abuse, 10(4), 389–410. 10.1177/1524838009339758 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newbury JB, Arseneault L, Moffitt TE, Caspi A, Danese A, Baldwin JR, & Fisher HL (2017). Measuring childhood maltreatment to predict early-adult psychopathology: Comparison of prospective informant-reports and retrospective self-reports. Journal of Psychiatric Research, 96, 57–64. 10.1016/jjpsychires.2017.09.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pico-Alfonso MA, Garcia-Linares MI, Celda-Navarro N, Blasco-Ros C, Echeburúa E, & Martinez M (2006). The impact of physical, psychological, and sexual intimate male partner violence on women’s mental health: Depressive symptoms, posttraumatic stress disorder, state anxiety, and suicide. Journal of Women’s Health, 15(5), 599–611. 10.1089/jwh.2006.15.599 [DOI] [PubMed] [Google Scholar]
- Pine DS, Mogg K, Bradley BP, Montgomery L, Monk CS, McClure E, … Kaufman J (2005). Attention bias to threat in maltreated children: Implications for vulnerability to stress-related psychopathology. American Journal of Psychiatry, 162(2), 291–296. 10.1176/appi.ajp.162.2.291 [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Curran PJ, & Bauer DJ (2006). Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics, 31(4), 437–448. 10.3102/10769986031004437 [DOI] [Google Scholar]
- Reuben A, Moffitt TE, Caspi A, Belsky DW, Harrington H, Schroeder F, … Danese A (2016). Lest we forget: Comparing retrospective and prospective assessments of adverse childhood experiences in the prediction of adult health. Journal of Child Psychology and Psychiatry, 57(10), 1103–1112. 10.1111/jcpp.12621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ripoll-Núñez KJ, & Rohner RP (2006). Corporal punishment in cross-cultural perspective: Directions for a research agenda. Cross-Cultural Research, 40(3), 220–249. 10.1177/1069397105284395 [DOI] [Google Scholar]
- Roxburgh S, & MacArthur KR (2014). Childhood adversity and adult depression among the incarcerated: Differential exposure and vulnerability by race/ethnicity and gender. Child Abuse & Neglect, 38(8), 1409–1420. 10.1016/j.chiabu.2014.02.007 [DOI] [PubMed] [Google Scholar]
- Rutter M (1987). Psychosocial resilience and protective mechanisms. The American Journal of Orthopsychiatry, 57(3), 316–331. [DOI] [PubMed] [Google Scholar]
- Rutter Michael. (2006). Implications of resilience concepts for scientific understanding. Annals of the New York Academy of Sciences, 1094, 1–12. 10.1196/annals.1376.002 [DOI] [PubMed] [Google Scholar]
- Rutter Michael. (2012). Resilience as a dynamic concept. Development and Psychopathology, 24(2), 335–344. 10.1017/S0954579412000028 [DOI] [PubMed] [Google Scholar]
- Rutter Michael. (2013). Annual research review: Resilience--clinical implications. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 54(4), 474–487. 10.1111/j.1469-7610.2012.02615.x [DOI] [PubMed] [Google Scholar]
- Ruttle PL, Shirtcliff EA, Serbin LA, Fisher DB-D, Stack DM, & Schwartzman AE (2011). Disentangling psychobiological mechanisms underlying internalizing and externalizing behaviors in youth: Longitudinal and concurrent associations with cortisol. Hormones and Behavior, 59(1), 123–132. 10.1016/j.yhbeh.2010.10.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sara G, & Lappin J (2017). Childhood trauma: Psychiatry’s greatest public health challenge? The Lancet Public Health, 2(7), e300–e301. 10.1016/S2468-2667(17)30104-4 [DOI] [PubMed] [Google Scholar]
- Seery MD, Holman EA, & Silver RC (2010). Whatever does not kill us: Cumulative lifetime adversity, vulnerability, and resilience. Journal of Personality and Social Psychology, 99(6), 1025–1041. 10.1037/a0021344 [DOI] [PubMed] [Google Scholar]
- Shapero BG, Farabaugh A, Terechina O, DeCross S, Cheung JC, Fava M, & Holt DJ (2019). Understanding the effects of emotional reactivity on depression and suicidal thoughts and behaviors: Moderating effects of childhood adversity and resilience. Journal of Affective Disorders, 245, 419–427. 10.1016/jjad.2018.11.033 [DOI] [PubMed] [Google Scholar]
- Shapero BG, Hamilton JL, Stange JP, Liu RT, Abramson LY, & Alloy LB (2015). Moderate childhood stress buffers against depressive response to proximal stressors: A multi-wave prospective study of early adolescents. Journal of Abnormal Child Psychology, 43(8), 1403–1413. 10.1007/s10802-015-0021-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons RL, Woodring D, Simons LG, Sutton TE, Lei M-K, Beach SRH, … Gibbons FX (2019). Youth adversities amplify the association between adult stressors and chronic inflammation in a domain specific manner: Nuancing the early life sensitivity model. Journal of Youth and Adolescence. 10.1007/s10964-018-0977-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons RL, Wu C-I, Lin K-H, Gordon L, & Conger RD (2000). A cross-cultural examination of the link between corporal punishment and adolescent antisocial behavior. Criminology, 38(1), 47–80. 10.1111/j.1745-9125.2000.tb00883.x [DOI] [Google Scholar]
- Smith SG, Zhang X, Basile KC, Merrick MT, Wang J, Kresnow M, & Chen J (2018). National intimate partner and sexual violence survey: 2015 data brief. Centers for Disease Control and Prevention; Retrieved from https://www.cdc.gov/violenceprevention/nisvs/2015NISVSdatabrief.html [Google Scholar]
- Soper DS (2019). A-priori sample size calculator for multiple regression. Retrieved from http://www.danielsoper.com/statcalc
- Sprafkin J, Gadow KD, Weiss MD, Schneider J, & Nolan EE (2007). Psychiatric comorbidity in ADHD symptom subtypes in clinic and community adults. Journal of Attention Disorders, 11(2), 114–124. 10.1177/1087054707299402 [DOI] [PubMed] [Google Scholar]
- Straus MA, Hamby SL, Boney-McCoy S, & Sugarman DB (1996). The Revised Conflict Tactics Scales (CTS2): Development and preliminary psychometric data. Journal of Family Issues, 17(3), 283–316. 10.1177/019251396017003001 [DOI] [Google Scholar]
- Straus MA, Hamby SL, Finkelhor D, Moore DW, & Runyan D (1998). Identification of child maltreatment with the Parent-Child Conflict Tactics Scales: Development and psychometric data for a national sample of American parents. Child Abuse & Neglect, 22(4), 249–270. 10.1016/S0145-2134(97)00174-9 [DOI] [PubMed] [Google Scholar]
- Taillieu TL, & Brownridge DA (2010). Violence against pregnant women: Prevalence, patterns, risk factors, theories, and directions for future research. Aggression and Violent Behavior, 15(1), 14–35. 10.1016/j.avb.2009.07.013 [DOI] [Google Scholar]
- Turney K (2011). Labored love: Examining the link between maternal depression and parenting behaviors. Social Science Research, 40(1), 399–415. 10.1016/j.ssresearch.2010.09.009 [DOI] [Google Scholar]
- Vogel EH, & Wagner AR (2005). Stimulus specificity in the habituation of the startle response in the rat. Physiology & Behavior, 86(4), 516–525. 10.1016/j.physbeh.2005.08.042 [DOI] [PubMed] [Google Scholar]
- West SG, & Aiken LS (1991). Multiple Regression: Testing and Interpreting Interactions. SAGE. [Google Scholar]
- Wood SK, & Bhatnagar S (2015). Resilience to the effects of social stress: Evidence from clinical and preclinical studies on the role of coping strategies. Neurobiology of Stress, 1, 164–173. 10.1016/j.ynstr.2014.11.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yildiz Inanici S, Inanici MA, & Yoldemir AT (2017). The relationship between subjective experience of childhood abuse and neglect and depressive symptoms during pregnancy. Journal of Forensic and Legal Medicine, 49(Supplement C), 76–80. 10.1016/jjflm.2017.05.016 [DOI] [PubMed] [Google Scholar]
- Yun SH (2011). Factor structure and reliability of the revised conflict tactics scales’ (CTS2) 10-factor model in a community-based female sample. Journal of Interpersonal Violence, 26(4), 719–744. 10.1177/0886260510365857 [DOI] [PubMed] [Google Scholar]