

Supplemental Digital Content is available in the text
Keywords: cardiovascular outcomes, meta-analysis, mortality, SGLT2 inhibitors, type 2 diabetes
Abstract
Background:
Optimal glycemic control is required to restrain the increase of cardiovascular events in patients with type 2 diabetes. The effects of sodium-glucose cotransporter-2 (SGLT-2) inhibitors on cardiovascular events and mortality in those patients are not well established. This meta-analysis was conducted to assess the effects of SGLT2 inhibitors on cardiovascular events and mortality in patients with type 2 diabetes.
Methods:
We conducted a systematic literature search of Medline, Embase and Cochrane Library and included randomized controlled trials (RCTs) of 3 different SGLT2 inhibitors (canagliflozin, dapagliflozin and empagliflozin) that evaluated the effects on cardiovascular outcomes and mortality in the final meta-analysis. The intervention arm was defined either as SGLT2 inhibitor monotherapy or as SGLT2 inhibitor add-on to other non-SGLT2 inhibitor antidiabetic agents (ADAs).
Results:
Forty-two trials with a total of 61,076 patients with type 2 diabetes were included in the meta-analysis. Compared with the control, SGLT2 inhibitor treatment was associated with a reduction in the incidence of major adverse cardiovascular events (MACEs) (OR = 0.86, 95% CI 0.80–0.93, P < .0001), myocardial infarction (OR = 0.86, 95% CI 0.79–0.94, P = .001), cardiovascular mortality (OR = 0.74, 95% CI 0.67–0.81, P < .0001) and all cause mortality (OR = 0.85, 95% CI 0.79–0.92, P < .0001). However, the risk of ischemic stroke was not reduced after SGLT2 inhibitor treatment in patients with type 2 diabetes (OR = 0.95, 95% CI 0.85–1.07, P = .42).
Conclusion:
These data suggest a decreased risk of harm with SGLT2 inhibitor as a class with respect to cardiovascular events and mortality.
1. Introduction
Type 2 diabetes (T2DM), one of the most severe public health disorders, had a worldwide prevalence of 10% in the general population and affected more than 415 million adults in 2013, and this number has been projected to increase to 592 million by 2035.[1,2] Cardiovascular disease, a serious complication of type 2 diabetes, is primarily associated with excess mortality and morbidity in these patients.[3] More than 70% of type 2 diabetes patients die of cardiovascular causes.[4] The main contributors to the increased risk of cardiovascular disease include chronic hyperglycemia, insulin sensitivity reduction, visceral adiposity, and in particular, the comorbidities of hypertension and increased arterial stiffness.[5]
Existing antidiabetic agents (ADAs) lower blood glucose either by enhancing insulin secretion or by improving insulin sensitivity. Sodium-glucose cotransporter-2 (SGLT2) inhibitors lower blood glucose via an insulin-independent mode of action by reducing glucose renal reabsorption at the S1 segment of the proximal tubules in the kidney.[6,7] Phlorizin, the first SGLT2 inhibitor derived from the bark of apple trees, can cause severe gastrointestinal symptoms due to its property of nonselectively inhibiting SGLT1 and SGLT2.[8] In recent years, SGLT2-specific inhibitors (mainly including canagliflozin, dapagliflozin and empagliflozin) that could avoid gastrointestinal effects have been developed.[9] SGLT2 inhibitors have been recommended by clinical guidelines as potential pharmacological approaches for second-line therapy following metformin failure or intolerance.[10] SGLT2 inhibitors were proven to be effective in glycemia and/or HbA1c reduction and were additionally beneficial in terms of weight loss, blood pressure reduction, and intracranial hemodynamics.[11]
Increasing placebo-controlled trials suggested that the risk of cardiovascular outcomes such as major adverse cardiovascular events (MACEs) or at least several of their components were significantly reduced after SGLT2 inhibitor treatment in patients with type 2 diabetes.[12] SGLT2 inhibitors have a protective effect on the myocardium by improving the differentiation of epicardial adipose tissue (EAT) and subsequently reducing the secretion of proinflammatory chemokines.[13,14] This effect would probably be due to their impact on reducing body weight, especially body fat.[14] However, recent work has prompted a novel hypothesis that SGLT2 inhibitors may directly act on cardiac myocytes.[15] Experimental studies demonstrated that SGLT2 inhibitors have positive effects on cardiac function by reducing the overload of intracellular sodium (Na+), subsequently restoring mitochondrial function and the redox state in the failing heart.[15]
In a recent large multicenter randomized trial (EMPA-REG Outcome Trial), empagliflozin treatment demonstrated a relative risk reduction in MACEs (14%), cardiovascular mortality (38%) and all-cause mortality (32%), which supports the use of empagliflozin in patients with type 2 diabetes and increased cardiovascular risk.[16] The CANVAS Program demonstrated that canagliflozin reduced cardiovascular events compared with placebo.[17] Furthermore, the DECLARE-TIMI 58 trials indicated that dapagliflozin treatment resulted in a lower rate of cardiovascular death in patients with type 2 diabetes who had or were at risk for atherosclerotic cardiovascular disease; however, no difference in the MACE rate was seen between the dapagliflozin and placebo groups.[18] Thus far, it remains unconfirmed whether this cardiovascular benefit is extended to the entire class of SGLT2 inhibitors. Here, we assess the effect of SGLT2 inhibitors on cardiovascular events via a comprehensive meta-analysis of data from 42 randomized placebo-controlled trials, including sensitivity and subgroup analyses.
2. Methods
The meta-analysis was performed based on the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.[19] The authors declare that all supporting data are available within the article and/or its Supplementary materials. This study did not require ethical approval since all analyses were based on previously published studies.
2.1. Data sources and searches
Two investigators (Zou and Liu) performed a systematic search of scientific literature in the databases (from conception through May 12, 2019), including PubMed, Embase, and Cochrane Central Register of Controlled Trials. A combination of the following terms was used: “sodium-glucose cotransporter”, “sodium-glucose cotransporter-2 inhibitors”, “sglt-2”, “sglt2”, “canagliflozin”, “Invokana”, “dapagliflozin”, “Farxiga”, “empagliflozin”, “Jardiance” AND “major adverse cardiovascular events”, “mace”, “cardiovascular disease”, “coronary artery disease”, “coronary heart disease”, “myocardial infarction”, “macrovascular disease”, “stroke”, “cerebrovascular disease”, “cerebral ischemia”, “mortality”, and “safety”. The search terms were used in Text Word and in different combinations as MeSH terms in PubMed, Emtree in Embase and MeSH descriptors in the Cochrane library. There was a limitation regarding language in that we considered only English publications. The search strategy is listed in the Supplemental Digital Content. The citations in the selected trials and meta-analyses were searched manually to find relevant original studies, and study authors were contacted for additional information when necessary. Finally, an electronic search alert was created to cover recent studies.
2.2. Inclusion and exclusion criteria
All relevant data from randomized controlled trials (RCTs) comparing the effects of SGLT2 inhibitors in type 2 diabetes with reported cardiovascular outcomes were eligible for inclusion. The intervention arm was defined either as SGLT2 inhibitor monotherapy or as SGLT2 inhibitor add-on therapy to other non-SGLT2 inhibitor ADAs. The control arm was defined as placebo or non-SGLT2 inhibitor ADAs. The trials were included if they met the following criteria:
-
(1)
all subjects enrolled in individual studies had type 2 diabetes irrespective of sex, age, race, or nationality;
-
(2)
SGLT2 inhibitors, including canagliflozin, dapagliflozin or empagliflozin, were employed in the treatment of patients;
-
(3)
the treatment intervention was SGLT2 inhibitor monotherapy or add-on therapy with any approved agent, and the matching control was defined as type 2 diabetes patients treated with placebo or any other ADAs;
-
(4)
the intervention duration was at least 12 weeks;
-
(5)
the safety outcomes included MACEs (defined as cardiovascular outcomes including no less than one of the following: myocardial infarction, ischemic stroke, or cardiovascular death)[18] or all-cause mortality.
Studies that met the following criteria were excluded:
-
(1)
letters, case reports, editorials, preclinical studies, and trials enrolling patients without diabetes or with type 1 diabetes;
-
(2)
studies describing duplicate data; and
-
(3)
studies lacking key information for further analysis.
2.3. Data extraction and quality assessment
Records retrieved from electronic searches were imported into reference management software EndNote X8 (Thomson Reuters, New York, NY). Two independent investigators (Zou and Liu) evaluated all the references and extracted data, including trial design, population size and demographics, various treatment strategies and cardiovascular outcomes. The decision to include a study was made by consensus, and discrepancies between the two investigators at any stage of the study selection process were arbitrated by a third reviewer (Liang) and resolved by consensus. The full-text versions of all publications that potentially qualified for the meta-analysis were scanned and assessed in detail according to the predefined inclusion and exclusion criteria.
The quality assessment of the trials included was undertaken independently as part of the data extraction process. The Jadad scale for reporting randomized clinical trials was used to assess the quality of each article.[20] In this scale, articles are evaluated based on randomization (mentioned as randomized gets 1 point and mentioning randomization methods receives another point), blinding (mentioned as double blind gets 1 point and mentioning blinding methods receives another point), and inclusion of participants (mentioning withdrawals and dropouts receives 1 point). Studies with 3 points or more are ranked as high quality.[20]
2.4. Statistical analysis
This meta-analysis was conducted using RevMan statistical software (version 5.3; Nordic Cochrane Center, Copenhagen, Denmark) for dichotomous data with a Mantel-Haenszel fixed-effects model. Pooled odds ratios (ORs) with a 95% confidence interval (95% CI) were estimated to calculate the effect size of categorical data. Subgroup analyses were conducted based on medication for type 2 diabetes patients (SGLT2 inhibitors vs placebo; SGLT2 inhibitor add-on therapy vs placebo; and SGLT2 inhibitor add-on therapy vs ADAs). The heterogeneity across studies was examined using the Chi-squared test and qualified by I2 statistics, with I2≥50% and P < .10 indicating significant heterogeneity. The likelihood of publication bias was assessed graphically by generating a funnel plot. All reported P values are two-tailed. Variables with P values < .05 were considered statistically significant.
3. Results
3.1. Characteristics of the included studies
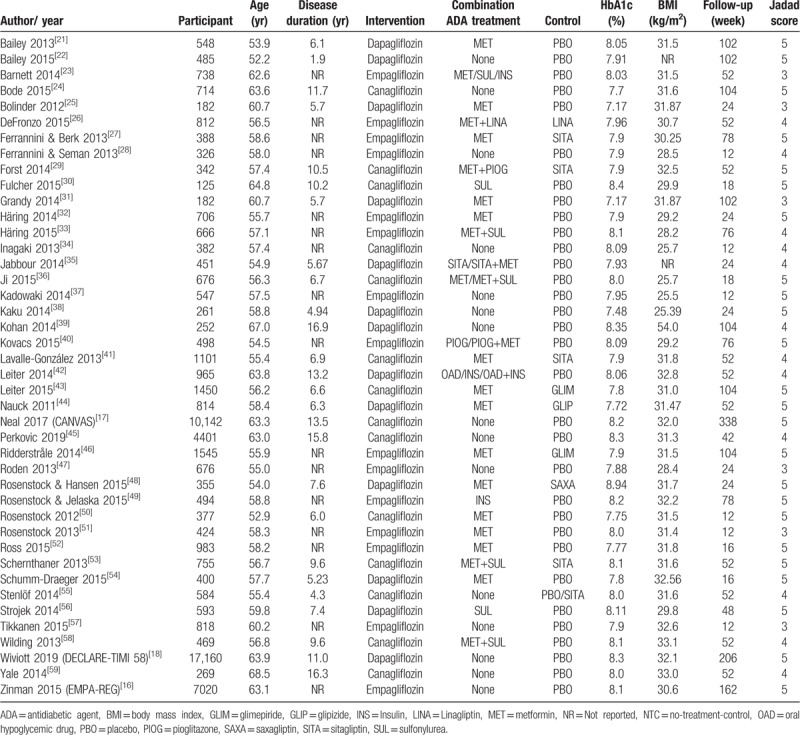
The flowchart of the literature search is shown in Figure 1. The initial implementation of the search strategy yielded 1027 potentially relevant citations. According to the predetermined criteria, a total of 42 studies[16–18,21–59] including 61,076 patients with type 2 diabetes published between 2010 and 2019 were included in the meta-analysis. Among these studies, SGLT2 inhibitor monotherapy was used in 15 studies[16–18,22,24,28,34,37–39,45,47,55,57,59], while add-on therapy with SGLT2 inhibitors and other ADAs was used in 27 studies.[21,23,25–27,29–33,35,36,40–44,46,48–54,56,58] The baseline characteristics included age, ranging from 52.20 to 68.50 years; disease duration, from 1.9 to 16.9 years; HbA1c, from 7.17% to 8.94%; body mass index (BMI), from 25.39 to 54.00; and follow-up period, from 12 to 338 weeks. All trials were high quality with more than 3 points according to the Jadad scale. The main characteristics of the selected trials are reported in Table 1.
Figure 1.
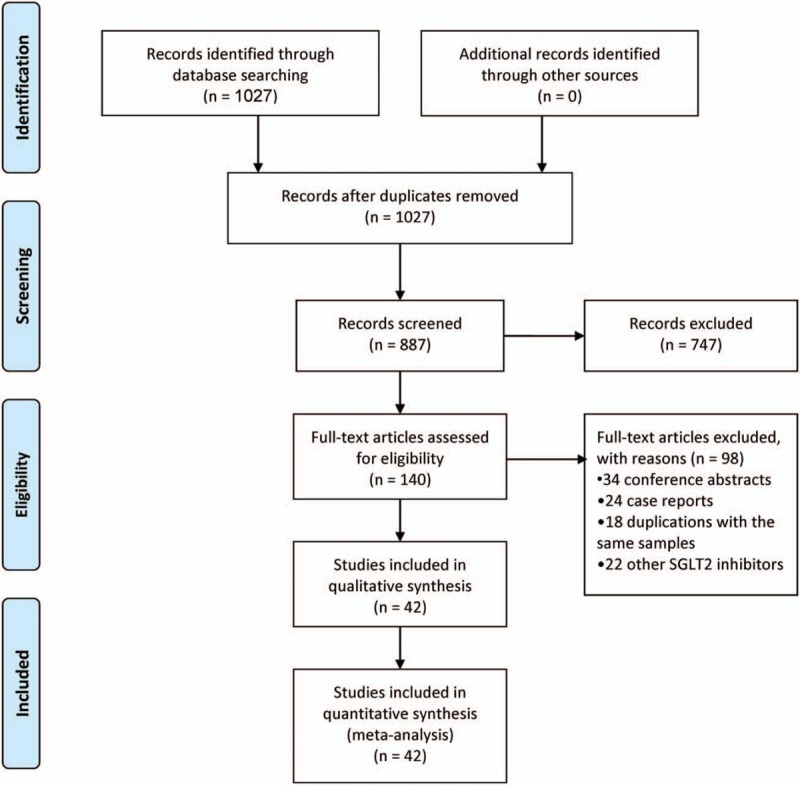
Flowchart of the study selection.
Table 1.
Baseline characteristics of included studies.
3.2. Major adverse cardiovascular events
Of the 42 trials fulfilling the inclusion criteria, 37 studies compared the effects of SGLT2 inhibitors and control treatments on cardiovascular outcomes. The results demonstrated that SGLT2 inhibitors significantly reduced the incidence of MACEs compared with control treatment (OR = 0.86, 95% CI 0.80–0.93, P < .0001). The subgroup analysis demonstrated that the comparisons of the effects of SGLT2 inhibitor add-on therapy vs placebo and SGLT2 inhibitor add-on therapy vs other ADAs on the risk of MACE also showed significant differences (OR = 0.67, 95% CI 0.47–0.96, P = .03; OR = 0.74, 95% CI 0.63–0.88, P = .0007, respectively) (Fig. 2 A). The sensitivity analysis, by iteratively removing 2 studies[16,18] with larger sample sizes, suggested that the SGLT2 inhibitors also decreased the incidence of MACEs compared with the control treatment (OR = 0.72, 95% CI 0.63–0.84, P < .001). These results confirm that our findings were not driven by any single study. Heterogeneity testing revealed a very low degree of heterogeneity, with I2 = 10% (Phetero = .29) (Fig. 2 A). Publication bias was evaluated by a funnel plot, which showed no significant evidence of asymmetry (Fig. 3 A).
Figure 2.
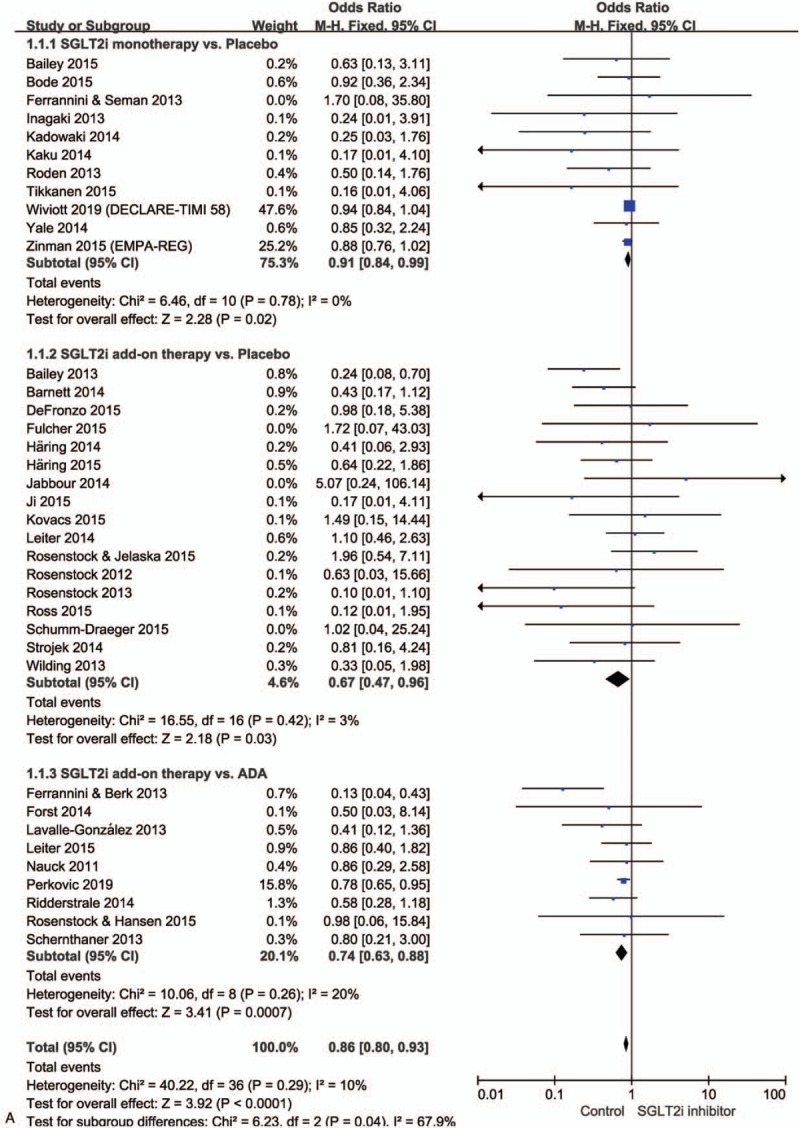
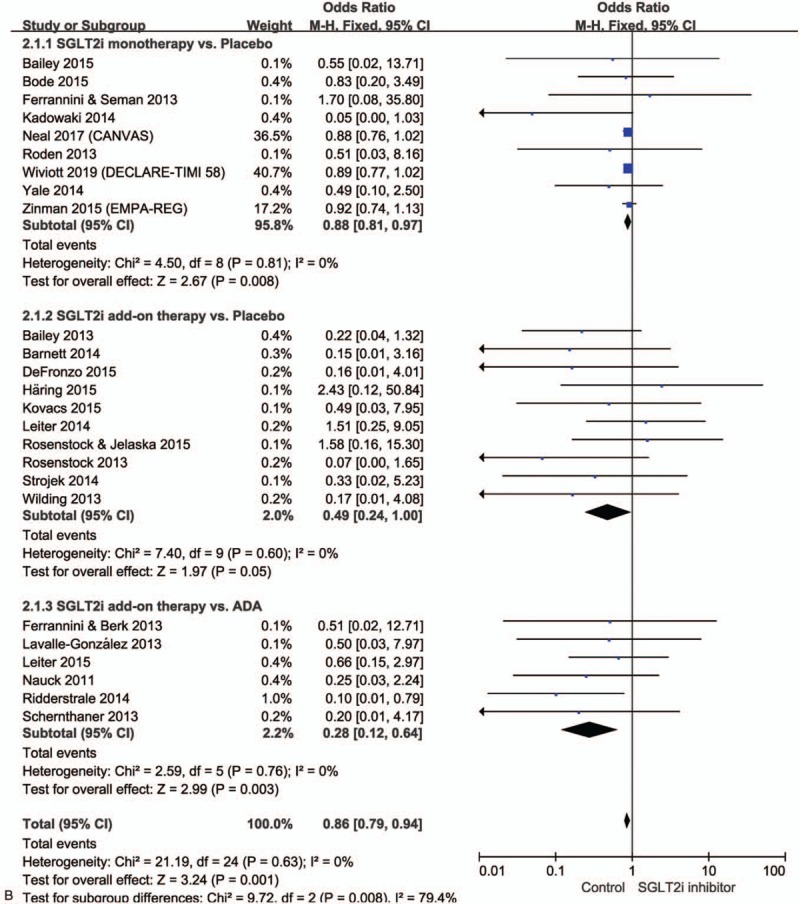
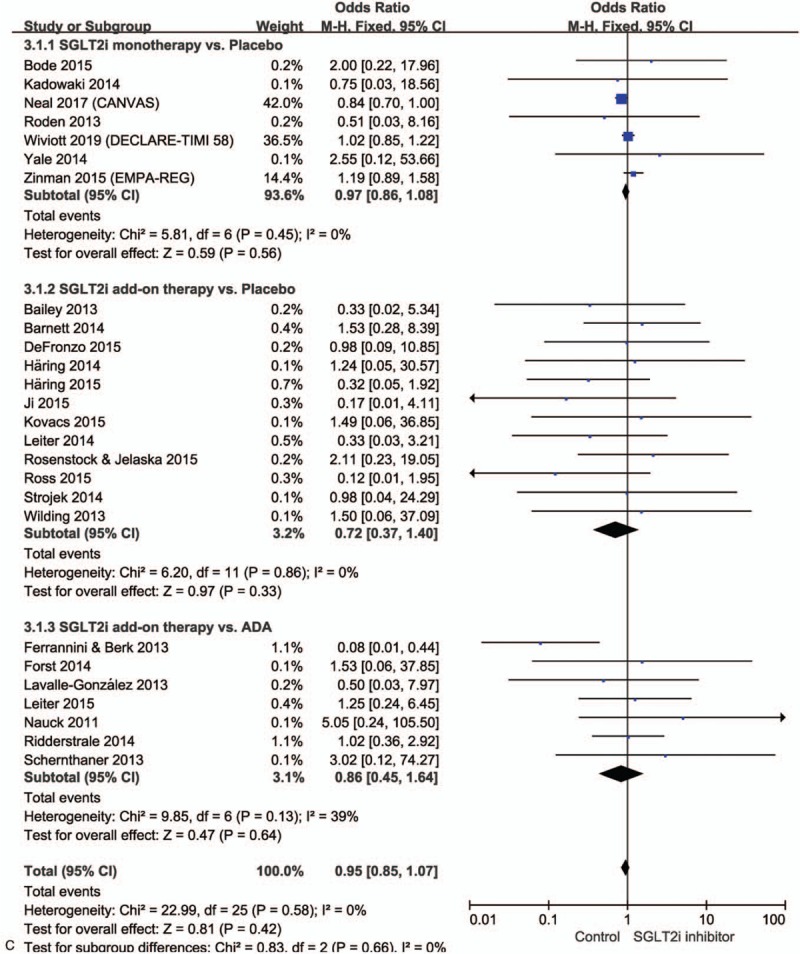
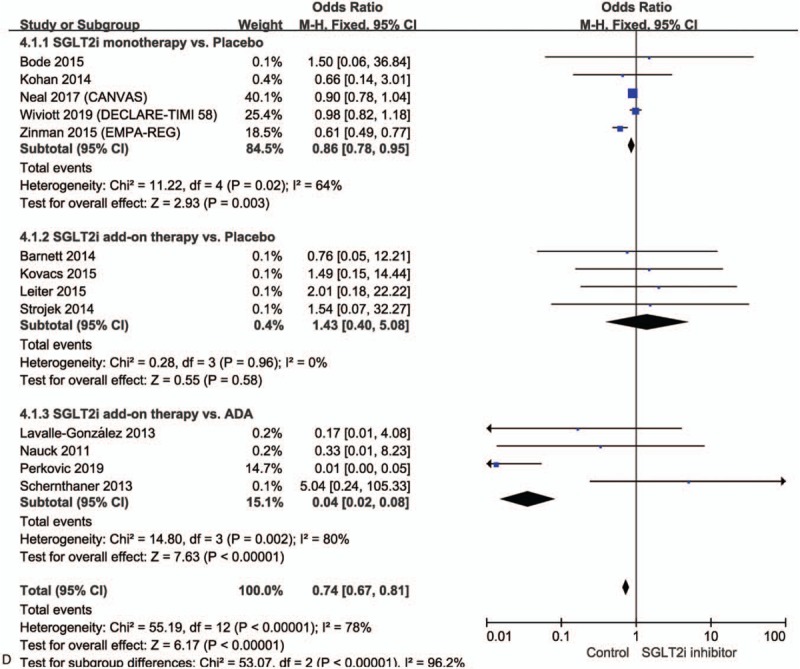
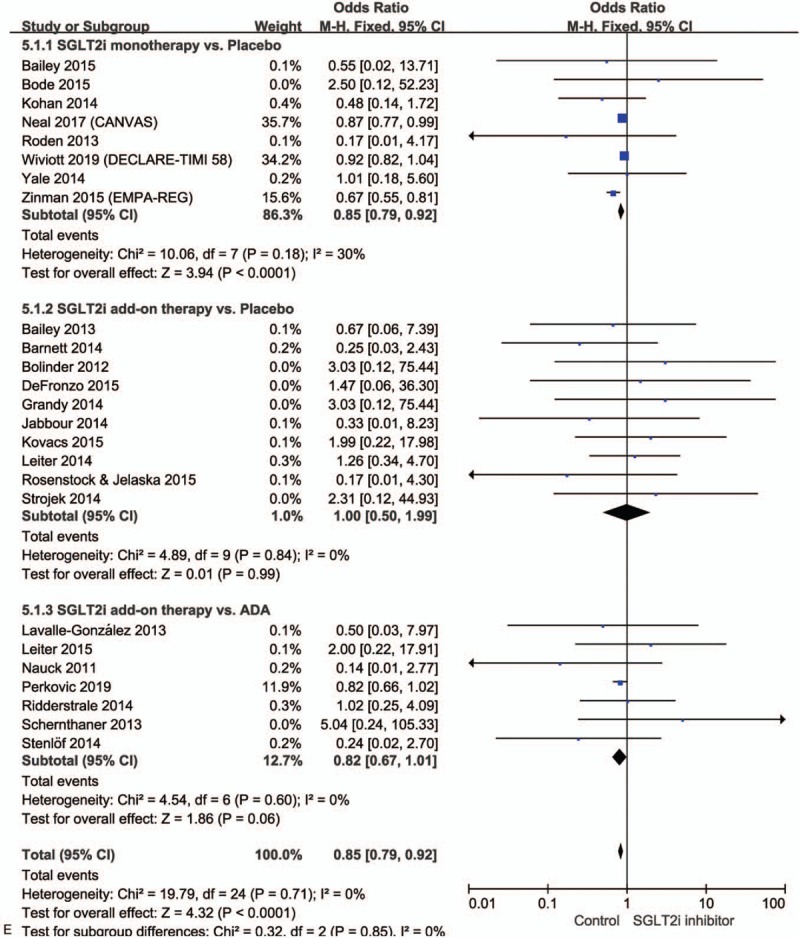
Forest plots for meta-analysis of the effects of SGLT2 inhibitors on cardiovascular outcomes in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes. Summary effects for all drugs were obtained from a fixed-effects meta-analysis.
Figure 2 (Continued).
Forest plots for meta-analysis of the effects of SGLT2 inhibitors on cardiovascular outcomes in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes. Summary effects for all drugs were obtained from a fixed-effects meta-analysis.
Figure 2 (Continued).
Forest plots for meta-analysis of the effects of SGLT2 inhibitors on cardiovascular outcomes in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes. Summary effects for all drugs were obtained from a fixed-effects meta-analysis.
Figure 2 (Continued).
Forest plots for meta-analysis of the effects of SGLT2 inhibitors on cardiovascular outcomes in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes. Summary effects for all drugs were obtained from a fixed-effects meta-analysis.
Figure 2 (Continued).
Forest plots for meta-analysis of the effects of SGLT2 inhibitors on cardiovascular outcomes in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes. Summary effects for all drugs were obtained from a fixed-effects meta-analysis.
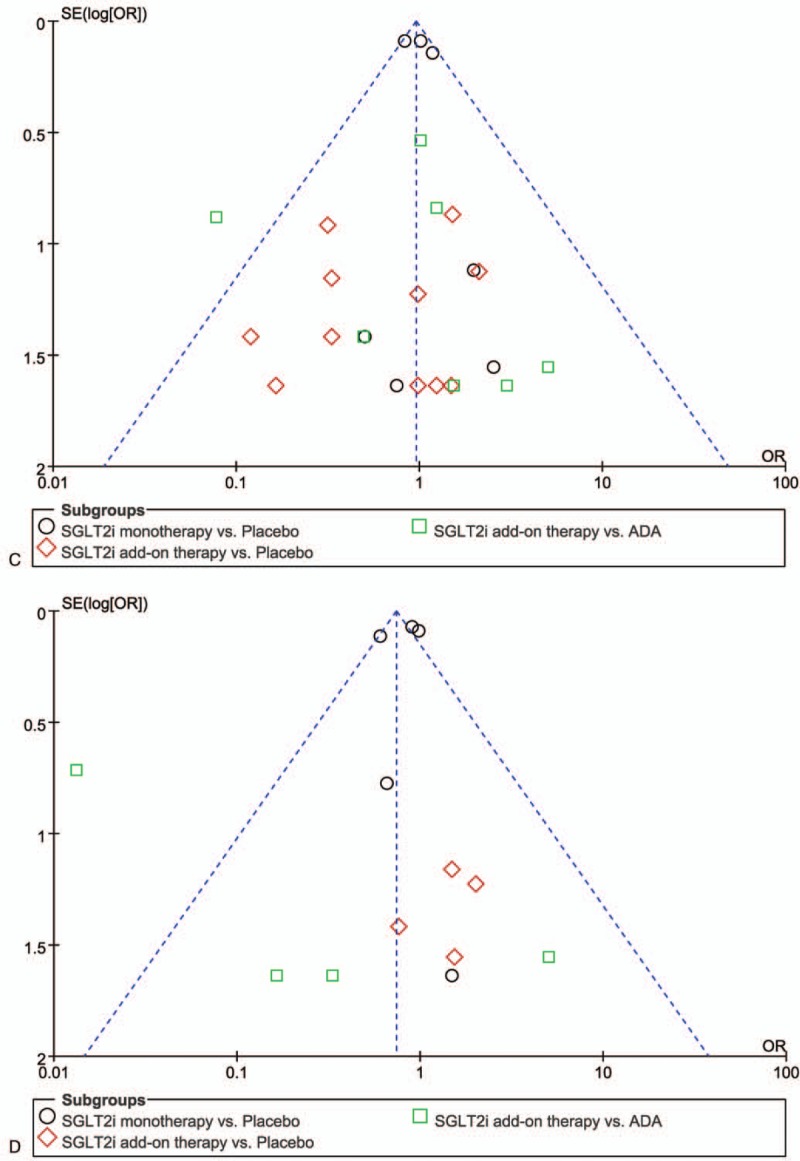
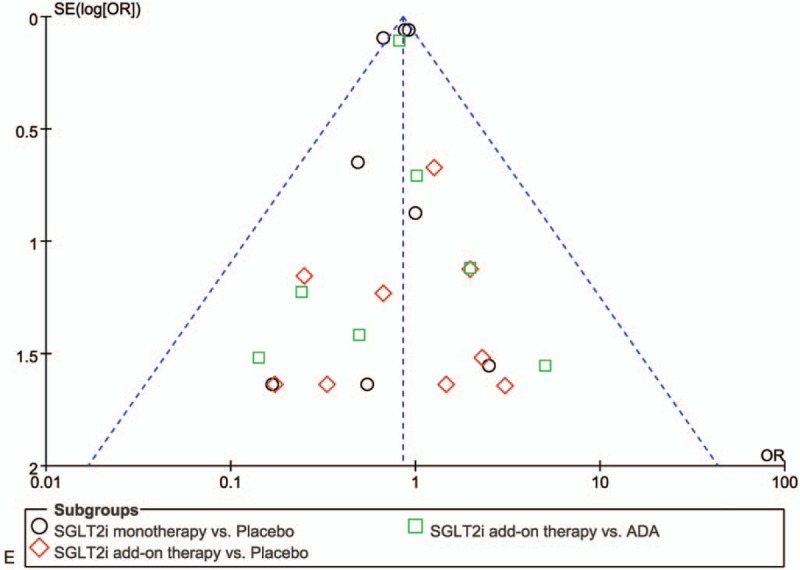
Figure 3.
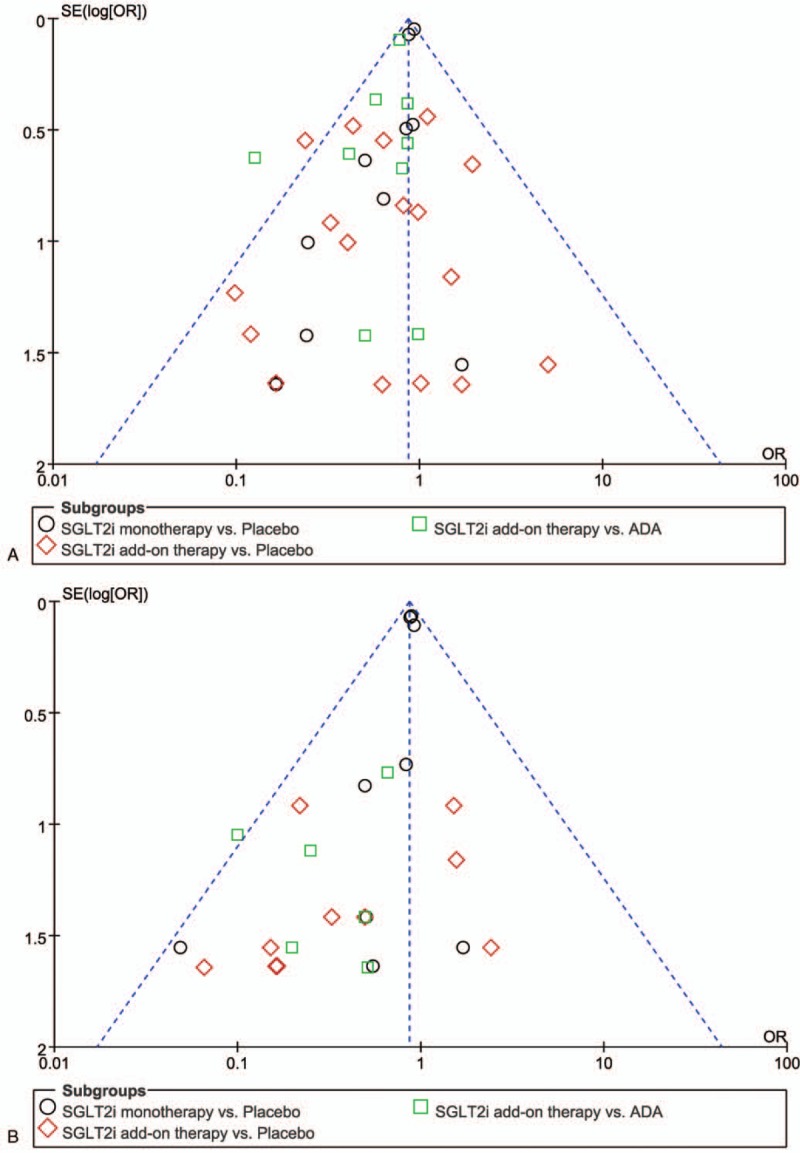
Funnel plot of standard error for SGLT2 inhibitors and control groups to detect publication bias in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes.
Figure 3 (Continued).
Funnel plot of standard error for SGLT2 inhibitors and control groups to detect publication bias in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes.
Figure 3 (Continued).
Funnel plot of standard error for SGLT2 inhibitors and control groups to detect publication bias in MACEs (A), myocardial infarction (B), ischemic stroke (C), cardiovascular death (D), and all-cause mortality (E) in patients with type 2 diabetes.
3.3. Myocardial infarction
Twenty-five studies evaluated the effects of SGLT2 inhibitors on the risk of myocardial infarction in patients with type 2 diabetes. The findings indicated that the incidence of myocardial infarction in patients with type 2 diabetes was lower with SGLT2 inhibitor treatment than with controls (OR = 0.86, 95% CI 0.79–0.94, P = .001) especially in the comparison between SGLT2 inhibitor monotherapy vs placebo (OR = 0.88, 95% CI 0.81–0.97, P = .008) and SGLT2 inhibitor add-on therapy vs ADA treatment (OR = 0.28, 95% CI 0.12–0.64, P = .003). However, no reduction in the risk of myocardial infarction was observed in comparisons between SGLT2 inhibitor add-on therapy vs placebo (OR = 0.49, 95% CI 0.24–1.00, P = .05) (Fig. 2 B). The sensitivity analysis removing 3 studies[16–18] suggested that SGLT2 inhibitors also decreased the incidence of myocardial infarction compared with the control treatment (OR = 0.42, 95% CI 0.27–0.65, P < .001). There was no heterogeneity among the trials in analyzing the effects of SGLT2 inhibitors on myocardial infarction, with I2 = 0% (Phetero = .63) (Fig. 2 B). The funnel plot showed no significant evidence of asymmetry (Fig. 3 B).
3.4. Ischemic stroke
Twenty-six studies were analyzed to assess the effects of SGLT2 inhibitors on the risk of ischemic stroke in patients with type 2 diabetes. SGLT2 inhibitors did not reduce the risk of ischemic stroke compared with control treatment (OR = 0.95, 95% CI 0.85–1.07, P = .42). The subgroup analysis also demonstrated that there was no difference in the incidence of ischemic stroke between SGLT2 inhibitor monotherapy vs placebo (OR = 0.97, 95% CI 0.86–1.08, P = .56), SGLT2 inhibitor add-on therapy vs placebo (OR = 0.72, 95% CI 0.37–1.40, P = .33) or SGLT2 inhibitor add-on therapy vs other ADAs (OR = 0.86, 95% CI 0.45–1.64, P = .64) (Fig. 2 C). The sensitivity analysis also revealed that the SGLT2 inhibitors had no impact on the incidence of stroke (OR = 0.84, 95% CI 0.55–1.30, P = .44). There was no substantial heterogeneity across trials, as all P values were larger than .05 and I2 < 50% (Fig. 2 C). The funnel plot did not reveal obvious asymmetry (Fig. 3 C).
3.5. Cardiovascular death
Thirteen studies were employed to evaluate the effects of SGLT2 inhibitors on the risk of cardiovascular mortality. SGLT2 inhibitors significantly reduced cardiovascular mortality compared with control in patients with type 2 diabetes (OR = 0.74, 95% CI 0.67–0.81, P < .00001), especially comparing SGLT2 inhibitor monotherapy vs placebo (OR = 0.86, 95% CI 0.78–0.95, P = .003) and SGLT2 inhibitor add-on therapy vs ADA treatment (OR = 0.04, 95% CI 0.02–0.008, P < .00001). However, no difference in effects on cardiovascular death was found between SGLT2 inhibitor add-on therapy vs placebo (OR = 1.43, 95% CI 0.40–5.08, P = .58) in patients with type 2 diabetes (Fig. 2 D). After removing 3 studies[16–18] with larger sample sizes, the sensitivity analysis suggested that SGLT2 inhibitors also significantly decreased the incidence of cardiovascular death compared with the control treatment (OR = 0.72, 95% CI 0.63–0.84, P < .001). For the analysis of the effects of SGLT2 inhibitors on cardiovascular mortality, I2 = 78% (Phetero < .001), suggesting significant heterogeneity (Fig. 2 D). Funnel plot analysis also suggested a relevant publication bias (Fig. 3 D).
3.6. All-cause mortality
Twenty-five studies evaluated the effects of SGLT2 inhibitors and control treatments on the risk of all-cause mortality in patients with type 2 diabetes. SGLT2 inhibitors significantly reduced the risk of all-cause mortality compared with control (OR = 0.85, 95% CI 0.79–0.92, P < 0.0001), especially in the subgroup analysis of the comparison between SGLT2 inhibitor monotherapy vs placebo (OR = 0.85, 95% CI 0.79–0.92, P < .001). There was no difference in comparison between SGLT2 inhibitor add-on therapy vs placebo (OR = 1.00, 95% CI 0.50–1.99, P = .99) and SGLT2 inhibitor add-on therapy vs other ADA therapy (OR = 0.82, 95% CI 0.67–1.01, P = .06). However, the sensitivity analysis performed by iteratively removing 3 studies[16–18] with larger sample sizes revealed that SGLT2 inhibitors had no impact on the incidence of all-cause mortality compared with the control treatment (OR = 0.82, 95% CI 0.68–1.00, P = .05). The induction effects of SGLT2 inhibitors on the incidence of all-cause mortality were mainly contributed by the 3 recent studies.[16–18] Additionally, there was no evidence of substantial heterogeneity between contributing studies (I2 = 0%; Phetero = .71) (Fig. 2 E). The funnel plot showed no significant evidence of asymmetry (Fig. 3 E).
4. Discussion
In our meta-analysis of 42 RCTs with 61,076 participants worldwide, we compared SGLT2 inhibitors with placebo or standard ADA treatment in people with type 2 diabetes. In the majority of trials of type 2 diabetes patients in this meta-analysis, SGLT2 inhibitors were associated with decreases in MACEs, myocardial infarction, and cardiovascular death compared with controls. The pooled results also revealed that SGLT2 inhibitor treatment, mainly derived from the SGLT2 inhibitor add-on therapy compared with ADA therapy in the subgroup analysis, reduced the risk of MACEs, myocardial infarction, and cardiovascular mortality. Compared with the placebo, SGLT2 inhibitor add-on therapy was associated only with the incidence reduction in MACEs, and SGLT2 inhibitor monotherapy had no effects on cardiovascular events or all-cause mortality. SGLT2 inhibitor treatment, either as monotherapy or add-on therapy, had no impact on the risk of ischemic stroke, which was consistent with a previous meta-analysis.[60] The main implications of our findings suggest that SGLT2 inhibitor administration, especially SGLT2 inhibitor add-on therapy, is beneficial for type 2 diabetes patients.
In several meta-analyses, favorable effects of SGLT2 inhibitors on reducing fasting blood sugar, HbA1c, body weight, and acute kidney injury were also observed.[61–65] Another meta-analysis assessed the long-term efficacy and safety of SGLT2 inhibitors in the management of type 2 diabetes, and the results showed that SGLT2 inhibitors significantly reduced systolic and diastolic blood pressures after 52 and 104 weeks significantly better than non-SGLT2 inhibitors.[4] However, these previous studies did not evaluate cardiovascular outcomes. Recently, several large trials[16,18,66] and meta-analyses[67,68] were conducted to evaluate the effects of SGLT2 inhibitors on cardiovascular outcomes and mortality in patients with type 2 diabetes. These data suggested the protection of SGLT2 inhibitors against cardiovascular events and death. However, SGLT2 inhibitor monotherapy was used as the intervention in these meta-analyses and clinical trials, and whether SGLT2 inhibitor add-on therapy has similar effects on cardiovascular events was unconfirmed. Interestingly, no clear evidence that individual types of drugs in this class have different effects on cardiovascular outcomes or death was demonstrated. It is plausible that individual agents within this class of drugs, including canagliflozin, dapagliflozin, and empagliflozin, have similar functional effects on cardiovascular events because SGLT2 inhibitors share the same mechanism of action.[60]
Our meta-analysis was conducted on SGLT2 inhibitor trials, including both monotherapy and add-on therapy, and our findings showed possible differences in cardiovascular outcomes, especially MACEs, depending on whether monotherapy or add-on therapy was administered. The overall class of SGLT2 inhibitors is a prominent option in the treatment of type 2 diabetes patients due to its value as add-on therapy to current ADA treatment.[69] A more significant improvement in HbA1c, FPG, body weight, and systolic and diastolic blood pressures was indicated in SGLT2 inhibitor add-on therapy compared with placebo or other ADAs, including metformin or DPP4 inhibitors.[70] In the longer term, SGLT2 inhibitors are more effective than sulfonylurea as an add-on to metformin in reducing HbA1c, weight and blood pressure.[71] Consequently, SGLT2 inhibitor add-on therapy seems to be more cost effective than traditional treatment with generic medications for patients who fail to achieve their glycemic goal on metformin.[72] Although the long-term effects of SGLT2 inhibitors on cardiovascular outcomes are still unclear, our overview analysis suggested that SGLT2 inhibitors as a drug class delivering cardiovascular protection will be supported by accumulating evidence in the future. To our knowledge, this report is the first systematic meta-analysis to include SGLT2 inhibitor add-on therapy compared with non-SGLT2 inhibitors or placebo, thus providing a reliable analysis of the cardiovascular outcomes of this class of medications.
Although we conducted a comprehensive systematic review of RCTs of SGLT2 inhibitors, several limitations need to be considered when interpreting our findings. First, none of the included trials were designed specifically to assess cardiovascular outcomes of SGLT2 inhibitors, even though all trials intended to evaluate the safety of SGLT2 inhibitors in patients with type 2 diabetes. In addition, the included trials had a wide range of clinical characteristics, such as age, disease duration, and follow-up duration, which will inevitably lead to heterogeneity. Second, only 42 studies met the predefined inclusion criteria and were included in the final meta-analysis. The included studies were almost all single-center trials with a relatively small number of patients. In addition, due to the limited number of studies, the latest approved SGLT2 inhibitors, such as ertugliflozin, were not enrolled in this meta-analysis to reduce the heterogeneity that might be derived from excessive interventions. These limitations may impair the power of our study. However, after a comprehensive literature search covering 3 databases was performed and eligible studies were selected by two different investigators according to strict inclusion criteria, most of the included studies had moderate-to-high quality. Therefore, we believe that it is reasonable to draw conclusions from this meta-analysis. Third, several of the endpoints, including cardiovascular and all-cause mortality, occur infrequently, resulting in these individual outcomes being at a higher risk of selective reporting bias than the more common adverse effects.
In summary, our meta-analysis evaluated the effects of SGLT2 inhibitors on cardiovascular outcomes in patients with type 2 diabetes, and the results demonstrated that patients treated with SGLT2 inhibitors, especially as add-on therapy, experienced significant cardioprotective effects and a potential favorable outcome for all-cause mortality. Due to the potential heterogeneity among the included studies, the results of this analysis should be confirmed with new and larger trials in the future.
Author contributions
Conceptualization: Cai-Yan Zou, Jun Liang.
Data curation: Cai-Yan Zou, Xue-Kui Liu, Jun Liang.
Formal analysis: Xue-Kui Liu, Yi-Quan Sang.
Funding acquisition: Jun Liang.
Investigation: Cai-Yan Zou, Jun Liang.
Methodology: Xue-Kui Liu, Ben Wang.
Project administration: Cai-Yan Zou, Jun Liang.
Writing – original draft: Cai-Yan Zou, Xue-Kui Liu.
Writing – review & editing: Cai-Yan Zou, Xue-Kui Liu, Yi-Quan Sang, Ben Wang, Jun Liang.
Supplementary Material
Footnotes
Abbreviations: ADA = antidiabetic agent, SGLT2 = Sodium-glucose-cotransporter-2, EAT = epicardial adipose tissue, MACE = major adverse cardiovascular event, PRISMA = Preferred Reporting Items for Systematic Reviews, RCT = randomized controlled trial.
How to cite this article: Zou CY, Liu XK, Sang YQ, Wang B, Liang J. Effects of SGLT2 inhibitors on cardiovascular outcomes and mortality in type 2 diabetes: A meta-analysis. Medicine. 2019;98:49(e18245).
This work was supported The Jiangsu Provincial Bureau of Health Foundation (H201356 & BRA2014058), The Jiangsu Six Talent Peaks Program (2013-WSN-013), and The Social Development Project of the Xuzhou Municipal Science and Technology Bureau (KC18195).
The authors have no conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].Guariguata L, Whiting DR, Hambleton I, et al. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract 2014;103:137–49. [DOI] [PubMed] [Google Scholar]
- [2].Alberti KG, Zimmet P, Shaw J. International Diabetes Federation: a consensus on Type 2 diabetes prevention. Diabet Med 2007;24:451–63. [DOI] [PubMed] [Google Scholar]
- [3].Taimour S, Franzen S, Zarrouk M, et al. Nationwide comparison of long-term survival and cardiovascular morbidity after acute aortic aneurysm repair in patients with and without type 2 diabetes. J Vasc Surg 2019;pii: S0741-5214(19)30330-1. (Epub ahead of print). [DOI] [PubMed] [Google Scholar]
- [4].Devi R, Mali G, Chakraborty I, et al. Efficacy and safety of empagliflozin in type 2 diabetes mellitus: a meta-analysis of randomized controlled trials. Postgrad Med 2017;129:382–92. [DOI] [PubMed] [Google Scholar]
- [5].Inzucchi SE, Zinman B, Wanner C, et al. SGLT-2 inhibitors and cardiovascular risk: proposed pathways and review of ongoing outcome trials. Diab Vasc Dis Res 2015;12:90–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Ferrannini E, Solini A. SGLT2 inhibition in diabetes mellitus: rationale and clinical prospects. Nat Rev Endocrinol 2012;8:495–502. [DOI] [PubMed] [Google Scholar]
- [7].Bakris GL, Fonseca VA, Sharma K, et al. Renal sodium-glucose transport: role in diabetes mellitus and potential clinical implications. Kidney Int 2009;75:1272–7. [DOI] [PubMed] [Google Scholar]
- [8].Ehrenkranz JR, Lewis NG, Kahn CR, et al. Phlorizin: a review. Diabetes Metab Res Rev 2005;21:31–8. [DOI] [PubMed] [Google Scholar]
- [9].Kalra S. Sodium Glucose Co-Transporter-2 (SGLT2) inhibitors: a review of their basic and clinical pharmacology. Diabetes Ther 2014;5:355–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Canadian Diabetes Association Clinical Practice Guidelines Expert C.. Pharmacologic management of type 2 diabetes: 2016 interim update. Can J Diabetes 2016;40:484–6. [DOI] [PubMed] [Google Scholar]
- [11].Bays H. Sodium Glucose Co-transporter Type 2 (SGLT2) inhibitors: targeting the kidney to improve glycemic control in diabetes mellitus. Diabetes Ther 2013;4:195–220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Zelniker TA, Wiviott SD, Raz I, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019;393:31–9. [DOI] [PubMed] [Google Scholar]
- [13].Mazurek T, Zhang L, Zalewski A, et al. Human epicardial adipose tissue is a source of inflammatory mediators. Circulation 2003;108:2460–6. [DOI] [PubMed] [Google Scholar]
- [14].Aeddula NR, Cheungpasitporn W, Thongprayoon C, et al. Epicardial adipose tissue and renal disease. J Clin Med 2019;8:pii: E299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Bertero E, Prates Roma L, Ameri P, et al. Cardiac effects of SGLT2 inhibitors: the sodium hypothesis. Cardiovasc Res 2018;114:12–8. [DOI] [PubMed] [Google Scholar]
- [16].Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117–28. [DOI] [PubMed] [Google Scholar]
- [17].Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644–57. [DOI] [PubMed] [Google Scholar]
- [18].Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347–57. [DOI] [PubMed] [Google Scholar]
- [19].Stewart LA, Clarke M, Rovers M, et al. Preferred reporting items for systematic review and meta-analyses of individual participant data: the PRISMA-IPD Statement. JAMA 2015;313:1657–65. [DOI] [PubMed] [Google Scholar]
- [20].Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996;17:1–2. [DOI] [PubMed] [Google Scholar]
- [21].Bailey CJ, Gross JL, Hennicken D, et al. Dapagliflozin add-on to metformin in type 2 diabetes inadequately controlled with metformin: a randomized, double-blind, placebo-controlled 102-week trial. BMC Med 2013;11:43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Bailey CJ, Morales Villegas EC, Woo V, et al. Efficacy and safety of dapagliflozin monotherapy in people with Type 2 diabetes: a randomized double-blind placebo-controlled 102-week trial. Diabet Med 2015;32:531–41. [DOI] [PubMed] [Google Scholar]
- [23].Barnett AH, Mithal A, Manassie J, et al. Efficacy and safety of empagliflozin added to existing antidiabetes treatment in patients with type 2 diabetes and chronic kidney disease: a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol 2014;2:369–84. [DOI] [PubMed] [Google Scholar]
- [24].Bode B, Stenlof K, Harris S, et al. Long-term efficacy and safety of canagliflozin over 104 weeks in patients aged 55∗–∗80 years with type 2 diabetes. Diabetes Obes Metab 2015;17:294–303. [DOI] [PubMed] [Google Scholar]
- [25].Bolinder J, Ljunggren O, Kullberg J, et al. Effects of dapagliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin. J Clin Endocrinol Metab 2012;97:1020–31. [DOI] [PubMed] [Google Scholar]
- [26].DeFronzo RA, Lewin A, Patel S, et al. Combination of empagliflozin and linagliptin as second-line therapy in subjects with type 2 diabetes inadequately controlled on metformin. Diabetes Care 2015;38:384–93. [DOI] [PubMed] [Google Scholar]
- [27].Ferrannini E, Berk A, Hantel S, et al. Long-term safety and efficacy of empagliflozin, sitagliptin, and metformin: an active-controlled, parallel-group, randomized, 78-week open-label extension study in patients with type 2 diabetes. Diabetes Care 2013;36:4015–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Ferrannini E, Seman L, Seewaldt-Becker E, et al. A Phase IIb, randomized, placebo-controlled study of the SGLT2 inhibitor empagliflozin in patients with type 2 diabetes. Diabetes Obes Metab 2013;15:721–8. [DOI] [PubMed] [Google Scholar]
- [29].Forst T, Guthrie R, Goldenberg R, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes on background metformin and pioglitazone. Diabetes Obes Metab 2014;16:467–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Fulcher G, Matthews DR, Perkovic V, et al. Efficacy and safety of canagliflozin used in conjunction with sulfonylurea in patients with type 2 diabetes mellitus: a randomized, controlled trial. Diabetes Ther 2015;6:289–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Grandy S, Hashemi M, Langkilde AM, et al. Changes in weight loss-related quality of life among type 2 diabetes mellitus patients treated with dapagliflozin. Diabetes Obes Metab 2014;16:645–50. [DOI] [PubMed] [Google Scholar]
- [32].Haring HU, Merker L, Seewaldt-Becker E, et al. Empagliflozin as add-on to metformin in patients with type 2 diabetes: a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care 2014;37:1650–9. [DOI] [PubMed] [Google Scholar]
- [33].Haering HU, Merker L, Christiansen AV, et al. Empagliflozin as add-on to metformin plus sulphonylurea in patients with type 2 diabetes. Diabetes Res Clin Pract 2015;110:82–90. [DOI] [PubMed] [Google Scholar]
- [34].Inagaki N, Kondo K, Yoshinari T, et al. Efficacy and safety of canagliflozin in Japanese patients with type 2 diabetes: a randomized, double-blind, placebo-controlled, 12-week study. Diabetes Obes Metab 2013;15:1136–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Jabbour SA, Hardy E, Sugg J, et al. Dapagliflozin is effective as add-on therapy to sitagliptin with or without metformin: a 24-week, multicenter, randomized, double-blind, placebo-controlled study. Diabetes Care 2014;37:740–50. [DOI] [PubMed] [Google Scholar]
- [36].Ji L, Han P, Liu Y, et al. Canagliflozin in Asian patients with type 2 diabetes on metformin alone or metformin in combination with sulphonylurea. Diabetes Obes Metab 2015;17:23–31. [DOI] [PubMed] [Google Scholar]
- [37].Kadowaki T, Haneda M, Inagaki N, et al. Empagliflozin monotherapy in Japanese patients with type 2 diabetes mellitus: a randomized, 12-week, double-blind, placebo-controlled, phase II trial. Adv Ther 2014;31:621–38. [DOI] [PubMed] [Google Scholar]
- [38].Kaku K, Kiyosue A, Inoue S, et al. Efficacy and safety of dapagliflozin monotherapy in Japanese patients with type 2 diabetes inadequately controlled by diet and exercise. Diabetes Obes Metab 2014;16:1102–10. [DOI] [PubMed] [Google Scholar]
- [39].Kohan DE, Fioretto P, Tang W, et al. Long-term study of patients with type 2 diabetes and moderate renal impairment shows that dapagliflozin reduces weight and blood pressure but does not improve glycemic control. Kidney Int 2014;85:962–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Kovacs CS, Seshiah V, Merker L, et al. Empagliflozin as add-on therapy to pioglitazone with or without metformin in patients with type 2 diabetes mellitus. Clin Ther 2015;37:1773–88. e1. [DOI] [PubMed] [Google Scholar]
- [41].Lavalle-Gonzalez FJ, Januszewicz A, Davidson J, et al. Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial. Diabetologia 2013;56:2582–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Leiter LA, Cefalu WT, de Bruin TW, et al. Dapagliflozin added to usual care in individuals with type 2 diabetes mellitus with preexisting cardiovascular disease: a 24-week, multicenter, randomized, double-blind, placebo-controlled study with a 28-week extension. J Am Geriatr Soc 2014;62:1252–62. [DOI] [PubMed] [Google Scholar]
- [43].Leiter LA, Yoon KH, Arias P, et al. Canagliflozin provides durable glycemic improvements and body weight reduction over 104 weeks versus glimepiride in patients with type 2 diabetes on metformin: a randomized, double-blind, phase 3 study. Diabetes Care 2015;38:355–64. [DOI] [PubMed] [Google Scholar]
- [44].Nauck MA, Del Prato S, Meier JJ, et al. Dapagliflozin versus glipizide as add-on therapy in patients with type 2 diabetes who have inadequate glycemic control with metformin: a randomized, 52-week, double-blind, active-controlled noninferiority trial. Diabetes Care 2011;34:2015–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019;380:2295–306. [DOI] [PubMed] [Google Scholar]
- [46].Ridderstråle M, Andersen KR, Zeller C, et al. Comparison of empagliflozin and glimepiride as add-on to metformin in patients with type 2 diabetes: a 104-week randomised, active-controlled, double-blind, phase 3 trial. Lancet Diabetes Endocrinol 2014;2:691–700. [DOI] [PubMed] [Google Scholar]
- [47].Roden M, Weng J, Eilbracht J, et al. Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol 2013;1:208–19. [DOI] [PubMed] [Google Scholar]
- [48].Rosenstock J, Hansen L, Zee P, et al. Dual add-on therapy in type 2 diabetes poorly controlled with metformin monotherapy: a randomized double-blind trial of saxagliptin plus dapagliflozin addition versus single addition of saxagliptin or dapagliflozin to metformin. Diabetes Care 2015;38:376–83. [DOI] [PubMed] [Google Scholar]
- [49].Rosenstock J, Jelaska A, Zeller C, et al. Impact of empagliflozin added on to basal insulin in type 2 diabetes inadequately controlled on basal insulin: a 78-week randomized, double-blind, placebo-controlled trial. Diabetes Obes Metab 2015;17:936–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Rosenstock J, Aggarwal N, Polidori D, et al. Dose-ranging effects of canagliflozin, a sodium-glucose cotransporter 2 inhibitor, as add-on to metformin in subjects with type 2 diabetes. Diabetes Care 2012;35:1232–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Rosenstock J, Seman LJ, Jelaska A, et al. Efficacy and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, as add-on to metformin in type 2 diabetes with mild hyperglycaemia. Diabetes Obes Metab 2013;15:1154–60. [DOI] [PubMed] [Google Scholar]
- [52].Ross S, Thamer C, Cescutti J, et al. Efficacy and safety of empagliflozin twice daily compared with once daily in patients with type 2 diabetes inadequately controlled on metformin: a 16-week, randomized, placebo-controlled trial. Diabetes Obes Metab 2015;17:699–702. [DOI] [PubMed] [Google Scholar]
- [53].Schernthaner G, Gross JL, Rosenstock J, et al. Canagliflozin compared with sitagliptin for patients with type 2 diabetes who do not have adequate glycemic control with metformin plus sulfonylurea: a 52-week randomized trial. Diabetes Care 2013;36:2508–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].P-M SD, Burgess L, Korányi L, et al. Twice-daily dapagliflozin co-administered with metformin in type 2 diabetes: a 16-week randomized, placebo-controlled clinical trial. Diabetes Obes Metab 2015;17:42–51. [DOI] [PubMed] [Google Scholar]
- [55].Stenlof K, Cefalu WT, Kim KA, et al. Long-term efficacy and safety of canagliflozin monotherapy in patients with type 2 diabetes inadequately controlled with diet and exercise: findings from the 52-week CANTATA-M study. Curr Med Res Opin 2014;30:163–75. [DOI] [PubMed] [Google Scholar]
- [56].Strojek K, Yoon KH, Hruba V, et al. Dapagliflozin added to glimepiride in patients with type 2 diabetes mellitus sustains glycemic control and weight loss over 48 weeks: a randomized, double-blind, parallel-group, placebo-controlled trial. Diabetes Ther 2014;5:267–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [57].Ilkka T, Kirsi N, Cordula Z, et al. Empagliflozin reduces blood pressure in patients with type 2 diabetes and hypertension. Diabetes Care 2015;38:420–8. [DOI] [PubMed] [Google Scholar]
- [58].Wilding JP, Charpentier G, Hollander P, et al. Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and sulphonylurea: a randomised trial. Int J Clin Pract 2013;67:1267–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Yale JF, Bakris G, Cariou B, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes mellitus and chronic kidney disease. Diabetes Obes Metab 2014;16:1016–27. [DOI] [PubMed] [Google Scholar]
- [60].Guo M, Ding J, Li J, et al. SGLT2 inhibitors and risk of stroke in patients with type 2 diabetes: a systematic review and meta-analysis 2018;20:1977–82. [DOI] [PubMed] [Google Scholar]
- [61].Liu XY, Zhang N, Chen R, et al. Efficacy and safety of sodium-glucose cotransporter 2 inhibitors in type 2 diabetes: a meta-analysis of randomized controlled trials for 1 to 2years. J Diabetes Complications 2015;29:1295–303. [DOI] [PubMed] [Google Scholar]
- [62].Sun YN, Zhou Y, Chen X, et al. The efficacy of dapagliflozin combined with hypoglycaemic drugs in treating type 2 diabetes mellitus: meta-analysis of randomised controlled trials. BMJ Open 2014;4:e004619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [63].Musso G, Gambino R, Cassader M, et al. Efficacy and safety of dual SGLT 1/2 inhibitor sotagliflozin in type 1 diabetes: meta-analysis of randomised controlled trials. BMJ 2019;365:l1328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [64].Yang T, Lu M, Ma L, et al. Efficacy and tolerability of canagliflozin as add-on to metformin in the treatment of type 2 diabetes mellitus: a meta-analysis. Eur J Clin Pharmacol 2015;71:1325–32. [DOI] [PubMed] [Google Scholar]
- [65].Liakos A, Karagiannis T, Athanasiadou E, et al. Efficacy and safety of empagliflozin for type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes Metab 2014;16:984–93. [DOI] [PubMed] [Google Scholar]
- [66].Neuen BL, Ohkuma T, Neal B, et al. Cardiovascular and renal outcomes with canagliflozin according to baseline kidney function. Circulation 2018;138:1537–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Wu JH, Foote C, Blomster J, et al. Effects of sodium-glucose cotransporter-2 inhibitors on cardiovascular events, death, and major safety outcomes in adults with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol 2016;4:411–9. [DOI] [PubMed] [Google Scholar]
- [68].Singh AK, Singh R. Heart failure hospitalization with SGLT-2 inhibitors: a systematic review and meta-analysis of randomized controlled and observational studies. Expert Rev Clin Pharmacol 2019;12:299–308. [DOI] [PubMed] [Google Scholar]
- [69].Carlson CJ, Santamarina ML. Update review of the safety of sodium-glucose cotransporter 2 inhibitors for the treatment of patients with type 2 diabetes mellitus. Expert Opin Drug Saf 2016;15:1401–12. [DOI] [PubMed] [Google Scholar]
- [70].Li J, Gong Y, Li C, et al. Long-term efficacy and safety of sodium-glucose cotransporter-2 inhibitors as add-on to metformin treatment in the management of type 2 diabetes mellitus: a meta-analysis. Medicine 2017;96:e7201–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [71].Chen Z, Li G. Sodium-glucose co-transporter 2 inhibitors compared with sulfonylureas in patients with type 2 diabetes inadequately controlled on metformin: a meta-analysis of randomized controlled trials. Clin Drug Investig 2019;39:521–31. [DOI] [PubMed] [Google Scholar]
- [72].Pawaskar M, Bilir SP, Kowal S, et al. Cost-effectiveness of DPP-4 inhibitor and SGLT2 inhibitor combination therapy for type 2 diabetes. Am J Manag Care 2019;25:231–8. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.