

Abstract
Is parents’ support for mandating HPV vaccination for their adolescent children influenced by how the policy advocacy message is framed? In this research we conducted an experiment in which a group of African American parents were exposed to messages advocating HPV vaccination mandates that were framed in either gains or losses. Our results demonstrate the importance of considering the personality trait – Consideration of Future Consequences – when assessing the efficacy of gain- and loss-framed health advocacy. We found that parents responded more positively to gain-frames if they focused on the distant future and to loss-frames if they focused on the immediate future. Thus, it is important to recognize that public support of HPV vaccination policy is not only contingent on the message-based educational strategy employed to parent, but on the degree to which parents consider how present behaviors influence future well-being.
Keywords: message framing, HPV vaccination mandate, consideration of future consequences, persuasion
In June 2006, the Food and Drug Administration (FDA) approved the first human papillomavirus (HPV) vaccine for the prevention of HPV infections, which are the primary cause of cervical and various other types of cancers. The CDC recommends that the HPV vaccine be administered routinely to girls and boys 11–12 years of age prior to sexual activity (CDC, 2016; Saslow et al., 2016). Since 2007, policymakers in 24 states have introduced legislation to make the HPV vaccine mandatory in attempts to increase vaccination rates (Keim-Malpass, Mitchell, DeGuzman, Stoler, & Kennedy, 2017; National Conference of State Legislatures [NCSL], 2018). Early attempts to mandate the HPV vaccine were mired in controversies of government and pharmaceutical collusion as well as sexual promiscuity (Gollust, Dempsey, Lantz, Ubel, & Fowler, 2010). As of 2017, only two states (Virginia and Rhode Island) and Washington, D.C. mandate the vaccine for school entry in sixth or seventh grade (NCSL, 2018). In a national survey of parents of children ages 11–17, Calo, Gilkey, Shah, Moss, and Brewer (2016) found that 54% of parents disagreed with the statement that laws requiring HPV vaccination for school attendance “are a good idea.” Without the support of the public, it is unlikely that additional states will adopt HPV vaccine mandates.
Improving government communication about health policies in order to promote public support is an important yet challenging task, which unfortunately has been met with very limited research attention. In the current study, we turn to prospect theory (Tversky & Kahneman, 1981) and investigate whether emphasizing the benefits of passing a policy (i.e., gain frames) or the consequences of failing to implement a policy (i.e., loss frames) is more persuasive. We specifically assess African American parents’ support of HPV vaccination mandates as shaped by message framing. African-American female populations have higher rates of HPV infections and diagnoses of cervical cancer, and higher death rates due to cervical cancer than non-Hispanic white females (CDC, 2016). We also examine how the relative impact of gain vs. loss frames on policy support might be moderated by parents’ Consideration of Future Consequences (CFC), the extent which parents consider the future consequences of their current behaviors. As such, the current study advances theoretical understanding of message framing effects and their practical implications for promoting important public policies such as HPV vaccination mandates.
Message Framing Research: An Overview
Over the past few decades, a body of research has compared the relative effectiveness of messages that present the costs of not performing a behavior (loss-framed messages) vs. those that emphasize the benefits of performing a behavior (gain-framed messages) (for reviews see Gallagher & Updegraff, 2011; O’Keefe & Jensen, 2006; Rothman, Bartels, Wlaschin, & Salovey, 2006). Prospect theory, which postulates that individuals prefer taking risks when considering losses and favor certainty when considering gains, serves as the theoretical foundation for much of this work (Tversky & Kahneman, 1981). Using prospect theory as a guide, scholars have put forth a message-framing postulate that argues loss-framed messages will be more persuasive when people perceive an advocated action as risky and that gain-framed messages will be more persuasive when people perceive a promoted action to be of low risk or safe (Meyerowitz & Chaiken, 1987; Rothman et al., 2006; Rothman & Salovey, 1997; Rothman & Updegraff, 2010). Research testing the effects of gain- versus loss-framed messages has provided some empirical support for the moderating role of perceived risk (Hull, 2012; Lee & Aaker, 2004).
From the tenets of the message-framing postulate of prospect theory, researchers seeking to persuade individuals to adopt specific health behaviors developed a heuristic to guide message design (Rothman & Salovey, 1997). Specifically, Rothman and colleagues argued loss-framed messages are more persuasive than gain-framed messages when promoting detection behaviors, such as breast cancer screening and HIV testing, because these behaviors may be perceived as risky given the potential of finding an unpleasant health problem. Additionally, gain-framed messages should be more persuasive when advocating prevention behaviors, such as wearing sunscreen or eating healthy, as these behaviors are mostly of low risk or safe (Rothman & Salovey, 1997; Rothman et al., 2006).
Hypotheses relying on the detection–prevention dichotomy to predict the relative effectiveness of gain- and loss-frame messages have found support in individual studies (e.g., Banks et al., 1995; Cox & Cox, 2001; Rothman, Martino, Bedell, Detweiler, & Salovey, 1999). However, a series of meta-analyses by O’Keefe and Jensen provided limited support for the advantage of loss-framed messages for detection behaviors and gain-framed messages for prevention behaviors (2006, 2007, 2009). Additionally, a meta-analysis by O’Keefe and Nan (2012) looking specifically at the effects of message framing in the context of vaccination, which is a prevention behavior, found no significant difference in the persuasiveness of gain- versus loss-framed messages. Some scholars have specifically critiqued the misuse of the detection-prevention dichotomy in message framing research (Van’t Riet et al., 2014, 2016).
In view of the mixed results, scholars (Bartels, Kelly, & Rothman, 2010; Gallagher, Updegraff, Rothman, & Sims, 2011) have argued that people’s unique judgments of the riskiness of behaviors should be used to predict framing effects, rather than the presumed function of a behavior. Various antecedents can influence individual risk-perceptions, such as attentional style (Miller et al., 1999), approach and avoidance motivations (Mann, Sherman, & Updegraff, 2004), cultural worldview (Nan & Madden, 2014), sensation seeking (Hull & Hong, 2016), political predisposition (Lee & Kim, 2016), and Consideration of Future Consequences (Nan, 2012). Identifying and understanding the effects of these antecedents on risk perceptions have helped to clarify the field’s theoretical understanding of message framing effects and their practical implications.
Consideration of Future Consequences and Vaccination Decisions
Consideration of Future Consequences (CFC) is a personality trait that has been intricately linked to health behaviors in general and vaccination decisions in particular. CFC was first defined by Strathman and colleagues as “the extent to which individuals consider the potential distant outcomes of their current behaviors and the extent to which they are influenced by these potential outcomes” (Strathman, Gleicher, Boninger, & Edwards, 1994, p. 743). Strathman et al. proposed that a person who is high in CFC is more likely to consider the future consequences of his or her behavior and a person who is low in CFC is more likely to focus on immediate outcomes. Scholars have studied the role of CFC in influencing decisions about health and health beliefs (Chapman, 2005; Dorr, Krueckeburg, Strathman, & Wood, 1999; Joireman, 1999; Kim & Nan, 2015; Nan, 2012; Peters, Joireman, & Ridgeway, 2005; Rothspan & Read, 1996; Strathman et al., 1994) and have found that those high in CFC are more likely to complete a variety of preventative health behaviors, including HIV testing and greater condom usage as well as completing colorectal screenings and type 2 diabetes screenings (Burns & Dillon, 2005; Orbell, Perugini, & Rakow, 2004; Orbell & Hagger, 2006). Scholars have argued that individuals high in CFC are more likely to complete preventive behaviors because preventive health behaviors involve an immediate cost in return for a delayed benefit.
Research has also examined the role of CFC and similar constructs in influencing decision-making about vaccination (Chapman & Coups, 1999; Chapman et al., 2001; Kim & Nan, 2015; Morison, Cozzolino, & Orbell, 2010; Nan, 2012). In a 1999 article, Chapman and Coups proposed that the benefits of vaccinations, similarly to other preventive health measures, are often seen in the future, while the costs or inconvenience (such as pain of the injection) are immediate. It might then be expected that individuals high in CFC might focus on the future benefits of a vaccine, while individuals low in CFC would focus on the immediate consequences of a vaccine. In two studies, Chapman and colleagues (1999, 2001) found that an individual’s tendency to consider future outcomes (i.e., individuals high in CFC) was associated with a greater likelihood of receiving a flu vaccine.
Morison et al. (2010) explored the role of CFC in the context of deciding to vaccinate one’s daughter against HPV. Morison and colleagues found that parents high in CFC, compared with those low in CFC, were more likely to intend to vaccinate their daughter against HPV and to perceive the vaccine as more effective. A more recent study by Kim and Nan (2015) found indirect effects of CFC on H1N1 vaccine uptake. Kim and Nan (2015) found that higher CFC was associated with higher perceived vaccine efficacy and less safety concerns and that CFC exerted a significant indirect effect on the decision to vaccinate through perceived vaccine efficacy.
Overall, research suggests that people low in CFC may overemphasize the short-term costs of vaccination (e.g., pain, inconvenience), may not fully appreciate the long-term benefits of vaccination, and may actually perceive vaccinating themselves or their children against a disease as risky (e.g., unsafe and ineffective). With these arguments, we propose the following hypothesis:
H1: Individuals low (vs. high) in CFC will perceive greater risks associated with vaccination in general.
CFC and Message Framing
In a limited number of studies, researchers investigated how CFC might moderate the relative impact of gain- vs. loss-framed messages. O’Connor and colleagues (O’Connor, Warttig, Conner, & Lawton, 2009) examined the moderating influence of CFC on seeking information about high blood pressure in a message framing study. The findings revealed that those high in CFC, after being exposed to a loss-framed (vs. gain-framed), spent more time seeking additional information, while those low in CFC were more motivated to seek additional information after being presented with a gain-framed message. O’Connor and colleagues did not offer a clear theoretical explanation for the observed effects, concluding simply that “the psychological processes that may underpin these effects are unknown” (p. 218).
In a more recent study, Nan (2012) examined CFC as a moderator for gain- and loss-framed messages specifically in the context of HPV vaccination. Results showed that for participants low in CFC, loss-framed messages led to more favorable attitudes toward HPV vaccination. Among participants high in CFC, there was no clear advantage to a gain- or loss-framed message. In line with past research that shows reduced tendency of low CFC individuals to adopt preventive behaviors, Nan argues that people low in CFC are more likely to emphasize the short-term costs of vaccination, less likely to appreciate the long-term health benefits of vaccination, and more likely to perceive the behavior of vaccinating oneself or one’s children against HPV as risky, considering it unsafe and not effective. As the message framing postulate of prospect theory proposes, loss-framed messages should be more effective for people who perceive a behavior as risky.
CFC, Message Framing, and Health Policy
The vast majority of research on message framing has been done in the context of individual decision-making about health behaviors. Emerging research is beginning to address the role of message framing in promoting health policies (Lee & Kim, 2016; Nan & Madden, 2014). In recent studies that have explored the relative effectiveness of gain- and loss-framed messages in the context of health policies, scholars have proposed that cultural worldviews and political predisposition influence an individual’s perception of the riskiness of a policy. Nan and Madden (2014) proposed that a loss-framed message would be more persuasive for individuals who perceived HPV vaccination mandates as risky and gain-framed messages would be more persuasive for individuals who perceived the mandates as less risky. Nan and Madden relied on research related to cultural worldviews that demonstrated that people with hierarchical (i.e., prefer a society in which resources and opportunities are available and distributed based on an individual’s position in society) and individualistic (i.e., prefer individuals in a society to fend for themselves) worldviews perceive vaccination mandates as risky. In contrast, people with egalitarian (i.e., prefer a society in which social position does not determine availability of resources or opportunities) and communitarian (i.e., prefer individuals in a society to support and rely on one another) worldviews have been shown to find mandatory vaccination policies less risky. Nan and Madden found support for the hypothesis that risk perceptions were significantly different between hierarchical and egalitarian individuals and this led to differences in the influence of message framing on policy support. Those with a hierarchical worldview were more likely to support mandatory HPV vaccination policy when exposed to the loss-framed message, while those with an egalitarian worldview were more likely to support the policy when exposed to the gain-framed message. No differences were found in risk perceptions of the policy between those with individualistic and communitarian worldviews.
Lee and Kim (2016) explored the influence of gain- and loss-framed messages on support for policies aimed at reducing obesity. Relying on research that demonstrates Republicans tend to highlight or perceive greater risk than Democrats, Lee and Kim hypothesized that a loss-framed message would be more persuasive for Republicans and that a gain-framed message would be more persuasive for Democrats. Lee and Kim found an advantage for gain-framed messages among Democrats, but little difference between the effectiveness of gain- and loss-framed messages among Republicans.
Our research adds to the limited studies on the role of message framing in shaping policy attitudes by investigating how message framing might interact with parents’ tendency to consider future consequences to influence their support for HPV vaccination mandates. People low in CFC who perceive vaccination as risky should also perceive a mandatory policy requiring the vaccine as risky. Opponents of mandatory HPV vaccination tend to report fears associated with vaccine safety (Yeganeh, Curtis, & Kuo, 2010), and thus a loss-framed message should be superior than a gain-framed message for garnering support for HPV vaccination mandates from people low in CFC. In contrast, a gain-framed message should be more effective in promoting policy support among those high in CFC. Research by Nan (2012) demonstrates that a loss-framed message tends to be more persuasive for individuals low in CFC in the context of promoting vaccination behavior. We attempt to extend these findings to a health policy context and thus propose an interaction between consideration of future consequences and message framing:
H2: CFC will interact with message framing to influence parental support for HPV vaccination mandates such that a loss-framed (vs. gain-framed) message will result in stronger policy support among individuals low in CFC, whereas a gain-framed (vs. loss-framed) message will result in stronger policy support among those high in CFC.
Method
Participants and Procedures
Participants were recruited by trained researchers at community outlets, such as shopping malls and Laundromats, located in the Maryland suburbs outside of Washington, DC. The study protocol was approved by an institutional review board. Participants for this study were at least 18 years of age, identified their racial background as Black or African American, and were custodial parents of at least one child between the ages of 9 and 17 who had not yet initiated the HPV vaccine series. A total of 211 eligible adults participated in this study. The sample was 73% female and 27% male. Participants’ ages ranged from 22 to 71 years old (M = 35.97, SD = 9.09). Education levels varied, with 2% having completed some levels of high school, 16% completing high school, 38% having some college courses, 32% completing college, and 12% having post-graduate education.
Participants were told that the purpose of the study was to evaluate educational materials about HPV vaccination. Once participants gave informed consent, they were given a booklet that contained pre- and post-test survey questionnaires and a pamphlet about HPV vaccination that was either gain-framed or loss-framed. The booklets were pre-shuffled so participants randomly received the gain version or the loss version. After answering a few baseline questions, including those pertaining to demographic background, perceived risks of vaccination in general, trust in health information from government agencies, and baseline support for HPV vaccination mandates, people proceeded to read one of two promotional bi-fold pamphlets about the HPV vaccine. After reading the pamphlet, participants reported their attitudes toward an HPV vaccination mandate for school girls entering the sixth grade and answered questions designed to measure consideration of future consequences as an individual trait. After returning the survey, participants were thanked and compensated with a $25 gift card. On average, the survey took 20 minutes to complete.
Message Stimuli
The pamphlets contained a photographic montage of African American adult-child dyads along with four numbered content sections informing the reader about, in order, HPV, the HPV vaccine, reasons for vaccinating one’s child, and contact information for the Centers for Disease Control and Prevention. All information was identical between the gain and loss versions except for in the third section, in which message frame was experimentally manipulated. The text in this section was exclusively bolded and inset in a highlighted border. While the graphics of the pamphlets were developed by the authors, the informational content was adapted from published materials available on the CDC’s website. The framing manipulation entailed four bulleted reasons to vaccinate one’s child against HPV. All reasons conveyed support for vaccination in a consistent gain- or loss-frame. In the gain-framed message, the advantages of vaccinating one’s child against HPV were emphasized, whereas in the loss-framed message, the disadvantages of not vaccinating one’s child against HPV were highlighted (e.g., By having/not having your child receive the HPV vaccine, you make it much less/more likely for him/her to get genital HPV).
Measures
Consideration of Future Consequences (CFC).
CFC was measured by the 12-item scale developed by Strathman and colleagues (1994). Participants indicated their level of agreement with 12 statements on 1–5 scales with “strongly disagree” and “strongly agree” as endpoints. After recoding of reverse-worded items, an index for CFC was constructed by averaging the 12 items, with higher scores indicating higher tendency in CFC (α = .80, M = 3.47, SD = 0.62).
Perceived risks of vaccination in general.
Perceived risks of vaccination in general were measured by six items adapted from previous research (Brabin, Roberts, Farzaneh, & Kitchener, 2006; Busse, Kulkarni, Campbell, & Injeyan, 2002). Participants indicated their level of agreement with six statements on 1–5 scales with “strongly disagree” and “strongly agree” as endpoints. Items were averaged to form an index for perceived risks (α = .70, M = 2.46, SD = .66).
Support for the HPV vaccination mandate.
Participants’ overall support for the HPV vaccination mandate was gauged by three questions asking about their attitudes toward a policy that requires HPV vaccination of all girls entering the sixth grade in their state. Participants indicated their sentiments on three 1–5 semantic differential scales (negative/positive, unfavorable/favorable, against/favoring) (α = .97, M = 3.10, SD = 1.45).
Control variables.
In addition to sex, age, and education, the following variables were measured as control variables. Baseline policy support was measured by this question: “Some states in the U.S. require girls to get the HPV vaccine that prevents cervical cancer in order to attend school. Do you support or oppose this type of law?” Responses were recorded on a 1–5 scale (strongly oppose/strongly support) (M = 3.12, SD = 1.22). Trust in health information from governmental agencies was also measured as a control variable as past research has found this variable to be significantly correlated with willingness to vaccinate one’s children against HPV (Nan, Zhao & Briones, 2014). Participants were asked this question: In general, how much would you trust information about health or medical topics from government health agencies? Responses were recorded on a 1–4 scale (not at all/a lot) (M = 2.70, SD = .94).
Results
Randomization Check
A series of chi-square tests and one-way analyses of variance (ANOVA) were conducted to check the success of random assignment. No significant demographic (sex, age, education), attitudinal (trust in government health information, perceived risks of vaccination), or dispositional (consideration of future consequences) differences were found between the gain and loss conditions. There was significant difference in baseline policy support between the two experimental conditions (p = .043). Including baseline policy support as a control variable in relevant analyses would address this issue. All analyses were performed with SPSS v22.
Hypothesis Testing
H1 predicted that individuals low (vs. high) in CFC would perceive greater risks associated with vaccination in general. To test this hypothesis, we conducted a hierarchical multiple regression, where the dependent variable was perceived risk. The predictors in the first block included demographic and other control variables (sex, age, education, trust in health information from government agencies). The second block contained the key predictor – CFC.
The regression analysis revealed that the predictors as a whole explained 6.1% of variance in the dependent variable. Of interest, CFC was a significant predictor of perceived risks of vaccination (β = −.167, p = .03, ∆R2 = 2.5%), after controlling for the effects of demographic and other control variables. As predicted, lower CFC was associated with greater perceived risks of vaccination. H1 was supported.
H2 predicted that CFC would interact with message framing to influence parental support for HPV vaccination mandates such that a loss-framed (vs. gain-framed) message would result in stronger policy support among individuals low in CFC, whereas a gain-framed (vs. loss-framed) message would result in stronger policy support among those high in CFC. To test this hypothesis, we conducted another hierarchical multiple regression, where the dependent variable was support for the HPV vaccination mandate. The regression model had a 3-block structure. The first block contained demographic and other control variables, including sex, age, education, trust in health information from governmental agencies, and baseline support for the HPV vaccination mandate. The predictors of main interest to this research – message framing and CFC – were entered into the second block. The final and third block contained a two-way interaction term – the product of framing and CFC. To reduce multicollinearity, the component variables were mean-centered and the interaction term was formed based on the centered scores. Diagnostic analysis revealed no multicollinearity problems in the regression model.
Results of the regression analysis are summarized in Table 1. The predictors as a whole explained 26.5% of variance in the dependent variable. Two control variables emerged as significant predictors of policy support. Greater trust in health information from government agencies was associated with stronger support for the mandates (b = .215, p = .04). Not surprisingly baseline policy support was a strong, positive predictor of post-exposure policy support (b = .506, p < .001). The effects of two other control variables approached significance. Younger parents reported greater support for the HPV vaccination mandate (b = −.018, p = .10). The more educated showed less support for the policy (b = −.204, p = .07).
Table 1.
Predictors of support for the HPV vaccination mandate
| b | SE | t | p | |
|---|---|---|---|---|
| Sex | −.2214 | .2174 | −1.0185 | .3099 |
| Age | −.0180 | .0109 | −1.6448 | .1019 |
| Education | −.2037 | .1124 | −1.8119 | .0718 |
| Trust in government | .2152 | .1061 | 2.0287* | .0441 |
| Baseline policy support | .5063 | .0791 | 6.4013*** | .0000 |
| Message framing | −.0538 | .1945 | −.2765 | .7825 |
| CFC | −.1086 | .1648 | −.6588 | .5109 |
| Framing X CFC | −.7814 | .3117 | −2.5069* | .0131 |
Note. b=standardized regression coefficients; Sex: male=1, female=2; Age: higher scores indicate older ages; Education: 1=some levels of high school, 2=completed high school, 3=some college, 4=completed college, 5=post-graduate education; Trust in government: higher scores indicate greater trust in health information from government agencies; Baseline policy support: higher scores indicate greater policy support; Framing: gain=1, loss=2; CFC: higher scores indicate higher CFC;
p < .10
p < .05
p < .01
p < .001.
Neither message framing nor CFC independently predicted policy support. Results of the regression analysis showed a significant interaction between message framing and CFC, however (b = −.781, p = .01, ∆R2 = 2.8%). To further probe the nature of the interaction, we performed the Johnson-Neyman (J-N) analysis through Hayes and Matthes’ (2009) SPSS macro. The J-N analysis mathematically derives the point or points along the continuum of the moderator where the effect of the predictor transitions between statistically significant and nonsignificant, thus providing rich information about how the moderator affects the relationship between the predictor variable and the criterion variable. In the current analysis, the predictor variable was message framing. The moderator was CFC. The criterion variable was support for the HPV vaccination mandate. With all control variables held constant, the J-N analysis revealed two critical points of transition: −1.016 (b = .740, p = .05) and .614 (b = −.533, p = .05) (see Table 2 for the full results). The results suggested that when CFC was at or lower than −1.016 (centered score), the loss-framed message resulted in significantly greater policy support than the gain-framed message, whereas when CFC was at or higher than .614 (centered score), the gain-framed message led to significantly greater policy support than the loss-framed message (see Figure 1). H2 was supported.
Table 2.
Conditional effect of focal predictor (message framing) at values of moderator variable (CFC) on the criterion variable (support for the HPV vaccination mandate)
| CFC | b | SE | t | p | LLCI(b) | ULCI(b) |
|---|---|---|---|---|---|---|
| −1.9672 | 1.4833 | .6469 | 2.2931 | .0231 | .2063 | 2.7604 |
| −1.8047 | 1.3564 | .5988 | 2.2653 | .0248 | .1743 | 2.5384 |
| −1.6422 | 1.2294 | .5511 | 2.2308 | .0270 | .1414 | 2.3174 |
| −1.4797 | 1.1024 | .5040 | 2.1872 | .0301 | .1074 | 2.0974 |
| −1.3172 | .9754 | .4577 | 2.1311 | .0345 | .0718 | 1.8791 |
| −1.1547 | .8485 | .4124 | 2.0573 | .0412 | .0343 | 1.6627 |
| −1.0158 | .7399 | .3748 | 1.9742 | .0500 | .0000 | 1.4799 |
| −.9922 | .7215 | .3685 | 1.9577 | .0519 | −.0061 | 1.4491 |
| −.8297 | .5945 | .3266 | 1.8203 | .0705 | −.0503 | 1.2393 |
| −.6672 | .4675 | .2875 | 1.6262 | .1058 | −.1000 | 1.0351 |
| −.5047 | .3406 | .2525 | 1.3486 | .1793 | −.1580 | .8391 |
| −.3422 | .2136 | .2237 | .9550 | .3409 | −.2279 | .6551 |
| −.1797 | .0866 | .2035 | .4257 | .6708 | −.3151 | .4883 |
| −.0172 | −.0403 | .1947 | −.2072 | .8361 | −.4247 | .3440 |
| .1453 | −.1673 | .1989 | −.8414 | .4013 | −.5599 | .2253 |
| .3078 | −.2943 | .2152 | −1.3675 | .1733 | −.7192 | .1306 |
| .4703 | −.4213 | .2413 | −1.7460 | .0826 | −.8976 | .0551 |
| .6137 | −.5333 | .2702 | −1.9742 | .0500 | −1.0667 | .0000 |
| .6328 | −.5482 | .2743 | −1.9986 | .0473 | −1.0898 | −.0067 |
| .7953 | −.6752 | .3121 | −2.1634 | .0319 | −1.2914 | −.0591 |
| .9578 | −.8022 | .3531 | −2.2716 | .0244 | −1.4993 | −.1050 |
| 1.1203 | −.9292 | .3964 | −2.3441 | .0202 | −1.7117 | −.1466 |
| 1.2828 | −1.0561 | .4412 | −2.3937 | .0178 | −1.9272 | −.1851 |
Figure 1.
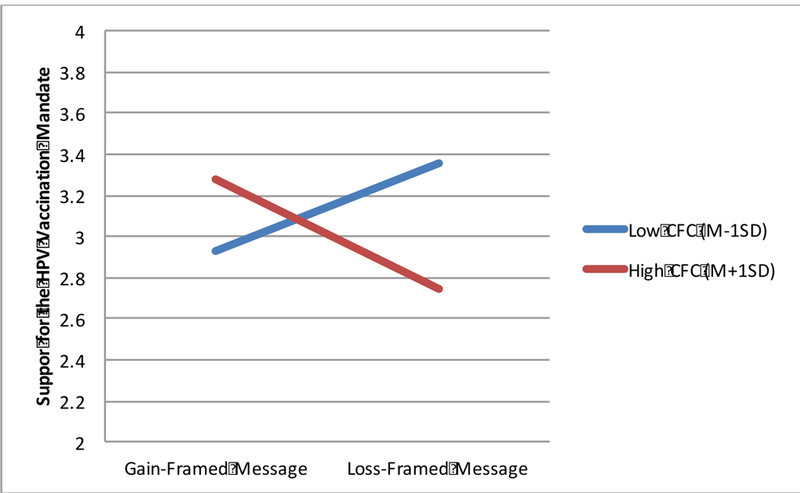
Interaction of Message Framing and CFC
Discussion
This study examined how message framing influenced African American parents’ policy positions about mandated HPV vaccination according to their tendencies to consider future consequences. African Americans are both disproportionately affected by HPV (CDC, 2016) and wary of health agencies that establish such policies (Boulware, Cooper, Ratner, LaVeist, & Power, 2003; Gamble, 1997). From a public health perspective, it is important to determine, then, how communication interventions might best facilitate support of regulations intended to improve HPV vaccination rates. We argued that CFC—the tendency to focus on distant rather than immediate outcomes of behavior (Strathman et al., 1994)—is a predictor of perceived HPV vaccination risk and has implications for the persuasiveness of advocacy that emphasizes either the positive consequences of vaccination or the negative outcomes of non-vaccination. In particular, we expected that parents higher in CFC would perceive the HPV vaccine to be more beneficial and less risky for their children. We therefore predicted that levels of CFC among parents would moderate the effect of gain- and loss-frames in promotional materials about the HPV vaccine.
As expected, CFC negatively associated with parents’ perceptions of risk of the HPV vaccine. This result concurs with other research about CFC and vaccination in general (Chapman & Coups, 1999; Chapman et al., 2001; Kim & Nan, 2015) as well as HPV vaccination in particular (Morison et al., 2010). In addition to CFC’s effect on risk perceptions about the HPV vaccine, our experiment showed that support for HPV vaccination mandates in response to gain- and loss-framed messages differed according to levels of CFC. In particular, we found that loss-framed messages elicited more policy support among parents low in CFC. These results replicate Nan’s (2012) finding among unvaccinated young adults: Present-minded people experienced more favorable attitudes and intentions toward HPV vaccination in response to loss-framed rather than gain-framed messages. However, we also supported our prediction that people high in CFC were more supportive of vaccination policy after a gain- rather than loss-framed message, whereas Nan (2012) found no significant differences between frames for future-minded people on persuasive outcomes (although those data generally trended in a similar direction to the current results). In contrast, in a recent study about exercising, researchers found a loss-framed message to be more effective for people high in CFC and a gain-framed message to be more persuasive for those low in CFC (Jensen et al., 2018). The differences in findings may be due to the different topics investigated. People may see exercising as riskless, regardless of their CFC. As such a gain-framed message is expected to be more persuasive for both groups. However, for those very high in CFC, “greater attention to long-term consequences could amplify the perceived costs of not adhering to a recommendation” (Jensen et al., 2018, p. 250), hence the loss frame advantage for them.
Overall, it appears that CFC functions as a marker of perceived HPV vaccination risk to moderate message-framing effects according to tenets of prospect theory (Tversky & Kahneman, 1981). Because parents high in CFC privilege future benefits associated with vaccination, they are better persuaded by messages that emphasize the advantages of HPV vaccination. Because parents low in CFC privilege immediate hazards associated with vaccination, they are better persuaded by messages that emphasize the costs of HPV vaccination. Like other individual differences known to function on perceived risk (e.g., political partisanship, Lee & Kim, 2016; cultural worldview, Nan & Madden, 2014; sensation seeking, Hull & Hong, 2016), CFC appears to be an important determinant of the efficacy of message-frames about health risk behaviors. Thus, this research adds to an understanding of how gain- and loss-frames persuade according to an individual’s construal of risks associated with the behavior, and not necessarily whether the health behavior itself is preventive or diagnostic (see Bartels, Kelly, & Rothman, 2010).
Although we considered CFC as an individual difference, our results suggest an interesting possibility about the strategic use of future-orientation within a campaign as a message feature. Perhaps it is possible to prime the consideration of future consequences by emphasizing the far or near outcomes associated with a health behavior. For instance, some forms of HPV cause cancers that do not develop tumors until ten to thirty years after initial infection (National Cancer Institute, 2015). Other forms of the virus can cause genital warts that appear as soon as two weeks after infection (Oriel, 1971). Therefore, it is possible for HPV vaccination messages to strategically emphasize the distant or proximal onset of symptomatic consequences of the disease. Similar to how we found that CFC moderated message-framing, this strategy may result in different persuasive outcomes when paired with more traditional gain- and loss-frames. A recent study found the pairing of gain frame with a present focus and that of loss frame with a future focus tend to bolster message persuasiveness (Wen & Shen, 2016).
This study also has practical implications for the use of message framing when targeting particular groups in health campaigns. Communication interventionists should consider how populations of interest consider future consequences. A number of demographic characteristics have been shown to associate with CFC. For one, as CFC is thought to decline with age (Orbell et al., 2004), gain-frames may be more appropriate for advocacy aimed toward youth whereas loss-frames may be increasingly appropriate as message recipients advance in age. In addition, sex has also been shown to associate with CFC. On the one hand, men tend to report being more present-oriented whereas women tend to report being more future-oriented (e.g., Petrocelli, 2003; Zimbardo & Boyd, 1999; Zimbardo, Keough, & Boyd, 1997). In that regard, advocacy targeting men’s health (e.g., prostate cancer screening) may do well to use loss-frames while advocacy targeting women’s health (e.g., breast cancer screening) may do well to use gain-frames. On the other hand, some research paints a more complicated picture of how CFC differs by sex, with differences depending on the subdimension or wording by which CFC is assessed (Rappange, Brouwer, & Van Exel, 2009), leading some to speculate that age and sex together moderate CFC (Robbins & Burleson, 2015). Besides static demographic variables, CFC may also be considered in light of situational differences associated with the future orientation of the health context. For instance, palliative care patients or others with advanced terminal diagnoses, who may not anticipate extended life and might even desire an expedient death (Breitbart et al., 2000; Wilson et al., 2000), may respond less readily to gain-framed advocacy about end of life care. Future research would do well to explore CFC’s relationship to other characteristics of message targets—both trait- and state-like individual differences—when determining the efficacy of message-framing strategies.
As with all research, this study has its limitations. The sample included African American parents in Maryland suburbs surrounding Washington, DC. Compared to the national average, HPV vaccination rates are notably higher in DC and marginally higher in Maryland (Reagan-Steiner et al., 2016). Given these tendencies, it is possible that people respond to messages about HPV vaccination differently in other areas of the United States. In addition, these results may be particular to the ethnic background of the sample, as some evidence suggests that African Americans differ in temporal orientation from people of other ethnicities (Brown & Segal, 1996). Further, the convenience sample was gathered in public locations among people who consented to participate, which is not necessarily representative of all African American parents in the area. Relatedly, it is possible that a setting-treatment interaction could have occurred such that parents responded differently to message-frames about HPV in the public locations used in our study than they would if they reviewed such materials in the privacy of homes or health clinics. Finally, the key effect we were interested in documenting – the CFC by framing interaction was small. As such the practical significance of the effect cannot be overstated. While the small effect may be a limitation of this research, a small effect in response to a single message may add up to a large impact over a long period of time with multiple message exposures.
Acknowledgement:
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number 5R03CA150570–02. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Contributor Information
Xiaoli Nan, University of Maryland-College Park.
Kelly Daily, La Salle University.
Adam Richards, Texas Christian University.
Cheryl Holt, University of Maryland-College Park.
References
- American Cancer Society. (2018, Jan. 4). What are key statistics about cervical cancer? Retrieved from https://www.cancer.org/cancer/cervical-cancer/about/key-statistics.html
- Ball LK, Evans G, & Bostrom A (1998). Risky business: Challenges in vaccine risk communication. Pediatrics, 101, 453–458. 10.1542/peds.101.3.453 [DOI] [PubMed] [Google Scholar]
- Banks SM, Salovey P, Greener S, Rothman AJ, Moyer A, Beauvais J, & Epel E (1995). The effects of message framing on mammography utilization. Health Psychology, 14, 178–184. 10.1037/0278-6133.14.2.178 [DOI] [PubMed] [Google Scholar]
- Bartels RD, Kelly KM, & Rothman AJ (2010). Moving beyond the function of the health behaviour: The effect of message frame on behavioural decision-making. Psychology and Health, 25, 821–838. 10.1080/08870440902893708 [DOI] [PubMed] [Google Scholar]
- Boulware LE, Cooper LA, Ratner LE, LaVeist TA, & Power NR (2003). Race and trust in the health care system. Public Health Reports, 118, 358–365. 10.1016/S0033-3549(04)50262-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brabin L, Roberts SA, Farzaneh F, & Kitchener HC (2006). Future acceptance of adolescent human papillomavirus vaccination: a survey of parental attitudes. Vaccine, 24, 3087–3094. 10.1016/j.vaccine.2006.01.048 [DOI] [PubMed] [Google Scholar]
- Breitbart W, Rosenfeld B, Pessin H, Kaim M, Funesti-Esch J, Galietta M, … Brescia R (2000). Depression, hopelessness, and desire for hastened death in terminally ill patients with cancer. Journal of the American Medical Association, 284, 2907–2911. 10.1001/jama.284.22.2907 [DOI] [PubMed] [Google Scholar]
- Brown CM, & Segal R (1996). Ethnic differences in temporal orientation and its implications for hypertension management. Journal of Health and Social Behavior, 37, 350–361. 10.2307/2137262 [DOI] [PubMed] [Google Scholar]
- Burns MJ, & Dillon FR (2005). AIDS health locus of control, self-efficacy for safer sex practices, and future time orientation as predictors of condom use in African-American college students. Journal of Black Psychology, 31, 172–188. 10.1177/0095798404268288 [DOI] [Google Scholar]
- Calo WA, Gilkey MB, Shah PD, Moss JL, & Brewer NT (2016). Parents’ support for school-entry requirements for human papillomavirus vaccination: A national study. Cancer Epidemiology, Biomarkers & Prevention, 25, 1317–1325. 10.1158/1055-9965.EPI-15-1159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC). (2016, Dec. 16). Human Papillomavirus Retrieved from https://www.cdc.gov/hpv/parents/cancer.html
- Chapman GB (2005). Short-term cost for long-term benefit: Time preference and cancer control. Health Psychology, 24, S41–S48. 10.1037/0278-6133.24.4.S41 [DOI] [PubMed] [Google Scholar]
- Chapman GB, Brewer NT, Coups EJ, Brownlee S, Leventhal H, & Leventhal EA (2001). Value for the future and preventive health behavior. Journal of Experimental Psychology: Applied, 7, 235–250. 10.1037//1076-898X.7.3.235 [DOI] [PubMed] [Google Scholar]
- Chapman GB, & Coups EJ (1999). Time preferences and preventive health behavior: Acceptance of the influenza vaccine. Medical Decision Making, 19, 307–314. 10.1177/0272989X9901900309 [DOI] [PubMed] [Google Scholar]
- Cox D, & Cox AD (2001). Communicating the consequences of early detection: The role of evidence and framing. Journal of Marketing, 65, 91–103. 10.1509/jmkg.65.3.91.18336 [DOI] [Google Scholar]
- Debono KG (1987). Investigating the social-adjustive and value-expressive functions of attitudes: Implications for persuasion processes. Journal of Personality and Social Psychology, 52, 279–287. 10.1037//0022-3514.52.2.279 [DOI] [Google Scholar]
- Dorr N, Krueckeburg S, Strathman A, & Wood MD (1999). Psychosocial correlates of voluntary HIV antibody testing in college students. AIDS Education and Prevention, 11, 14–27. Retrieved from https://search.proquest.com/docview/198052760?accountid=14696 [PubMed] [Google Scholar]
- Freed GL, Clark SJ, Butchart AT, Singer DC, & Davis MM (2010). Parental vaccine safety concerns in 2009. Pediatrics, 125, 654–59. 10.1542/peds.2009-1962. [DOI] [PubMed] [Google Scholar]
- Gallagher KM, & Updegraff JA (2011). Health message framing effects on attitudes, intentions, and behavior: A meta-analytic review. Annals of Behavioral Medicine, 43, 101–116. 10.1007/s12160-011-9308-7 [DOI] [PubMed] [Google Scholar]
- Gallagher KM, Updegraff JA, Rothman AJ, & Sims L (2011). Perceived susceptibility to breast cancer moderates the effect of gain- and loss-framed messages on use of screening mammography. Health Psychology, 30, 145–152. 10.1037/a0022264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gamble VN (1997). Under the shadow of Tuskegee: African Americans and health care. American Journal of Public Health, 87, 1773–1778. 10.2105/AJPH.87.11.1773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gastil J, Braman D, Kahan DM, & Slovic P (2005, Oct. 28). The ‘Wildavsky Heuristic’: The cultural orientation of mass political opinion. Yale Law School, Public Law Working Paper No. 107. Retrieved from http://papers.ssrn.com/sol3/papers.cfm?abstract_id=834264
- Gerend MA, & Shepherd JE (2007). Using message framing to promote acceptance of the human papillomavirus vaccine. Health Psychology, 26, 745–752. 10.1037/0278-6133.26.6.745 [DOI] [PubMed] [Google Scholar]
- Gollust SE, Dempsey AF, Lantz PM, Ubel PA, & Fowler EF (2010). Controversy undermines support for state mandates on the human papillomavirus vaccine. Health Affairs, 29, 2041–2046. 10.1377/hlthaff.2010.0174 [DOI] [PubMed] [Google Scholar]
- Hayes AF, & Matthes J (2009). Computational procedures for probing interactions in OLS and logistic regression: SPSS and SAS implementations. Behavior Research Methods, 41, 924–936. 10.3758/BRM.41.3.924 [DOI] [PubMed] [Google Scholar]
- Hull SJ (2012). Perceived risk as a moderator of the effectiveness of framed HIV test promotion messages among women: A randomized controlled trial. Health Psychology, 31, 114–121. 10.1037/a0024702 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hull SJ, & Hong Y (2016). Sensation seeking as a moderator of gain- and loss-framed HIV test promotion message effects. Journal of Health Communication, 21, 46–55. 10.1080/10810730.2015.1033113 [DOI] [PubMed] [Google Scholar]
- Jensen JD, Ratcliff CL, Yale RN, Krakow M, Scherr CL, & Yeo SK (2018). Persuasive impact of loss and gain frames on intentions to exercise: A test of six moderators. Communication Monographs, 85, 245–262. 10.1080/03637751.2017.1353699 [DOI] [Google Scholar]
- Joireman JA, Kees J, & Sprott D (2010). Concern with immediate consequences magnifies the impact of compulsive buying tendencies on college students’ credit card debt. Journal of Consumer Affairs, 44, 155–178. doi: https://doi-org.proxy-um.researchport.umd.edu/10.1111/j.1745-6606.2010.01161.x [Google Scholar]
- Keim-Malpass J, Mitchell EM, DeGuzman PB, Stoler MH, & Kennedy C (2017). Legislative activity related to the human papillomavirus (HPV) vaccine in the United States (2006–2015): A need for evidence-based policy. Risk Management Healthcare Policy, 10, 29–32. 10.2147/RMHP.S128247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim J, & Nan X (2015). Consideration of Future Consequences and HPV vaccine uptake among young adults. Journal of Health Communication, 20, 1033–1040. 10.1080/10810730.2015.1018583 [DOI] [PubMed] [Google Scholar]
- Lee AY, & Aaker JL (2004). Bringing the frame into focus: The influence of regulatory fit on processing fluency and persuasion. Journal of Personality and Social Psychology, 86, 205–218. 10.1037/0022-3514.86.2.205 [DOI] [PubMed] [Google Scholar]
- Lee TK, & Kim HK (2016). Differential effects of message framing on obesity policy support between Democrats and Republicans. Health Communication, 32, 1481–1490. 10.1080/10410236.2016.1230810 [DOI] [PubMed] [Google Scholar]
- Mann T, Sherman D, & Updegraff J (2004). Dispositional motivations and message framing: A test of the congruency hypothesis in college students. Health Psychology, 23, 330–334. 10.1037/0278-6133.23.3.330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyerowitz BE, & Chaiken S (1987). The effect of message framing on breast self-examination attitudes, intentions, and behavior. Journal of Personality & Social Psychology, 52, 500–510. 10.1037/0022-3514.52.3.500 [DOI] [PubMed] [Google Scholar]
- Miller SM, Buzaglo JS, Simms SL, Green V, Bales C, Mangan CE, & Sedlacek TV (1999). Monitoring styles in women at risk for cervical cancer: Implications for the framing of health-relevant messages. Annals of Behavioral Medicine, 21, 27–34. doi: https://doi-org.proxy-um.researchport.umd.edu/10.1007/BF02895030 [DOI] [PubMed] [Google Scholar]
- Morison LA, Cozzolino PJ, & Orbell S (2010). Temporal perspective and parental intention to accept the Human Papillomavirus vaccination for their daughter. British Journal of Health Psychology, 15, 151–165. 10.1348/135910709X437092 [DOI] [PubMed] [Google Scholar]
- Nan X (2012). Relative persuasiveness of gain- versus loss-framed human papillomavirus vaccination messages for the present- and future-minded. Human Communication Research, 38, 72–94. 10.1111/j.1468-2958.2011.01419.x [DOI] [Google Scholar]
- Nan X, & Madden K (2014). The role of cultural worldviews and message framing in shaping public opinions about the human papillomavirus vaccination mandate. Human Communication Research, 40, 30–53. 10.1111/hcre.12016 [DOI] [Google Scholar]
- Nan X, Zhao X, & Briones R (2014). Parental cancer beliefs and trust in health information from medical authorities as predictors of HPV vaccine acceptability. Journal of Health Communication, 19, 100–114. 10.1080/10810730.2013.811319 [DOI] [PubMed] [Google Scholar]
- National Cancer Institute. (2015, Feb. 19). HPV and cancer Retrieved from https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-fact-sheet
- National Conference of State Legislatures. (2018, Jun. 12). HPV vaccine: State legislation and status Retrieved from http://www.ncsl.org/research/health/hpv-vaccine-state-legislation-and-statutes.aspx
- O’Connor DB, Warttig S, Conner M, & Lawton R (2009). Raising awareness of hypertension risk through a web-based framing intervention: does consideration of future consequences make a difference? Psychology, Health, & Medicine, 14, 213–219. 10.1080/13548500802291618 [DOI] [PubMed] [Google Scholar]
- O’Keefe DJ, & Jensen JD (2006). The advantages of compliance or the disadvantages of noncompliance? A meta-analytic review of the relative persuasive effectiveness of gain-framed and loss-framed messages. Communication Yearbook, 30, 1–43. 10.1207/s15567419cy3001_1 [DOI] [Google Scholar]
- O’Keefe DJ, & Jensen JD (2007). The relative persuasiveness of gain-framed and loss framed messages for encouraging disease prevention behaviors: A meta-analytic review. Journal of Health Communication, 12, 623–644. 10.1080/10810730701615198 [DOI] [PubMed] [Google Scholar]
- O’Keefe DJ, & Jensen JD (2009). The relative persuasiveness of gain-framed and loss-framed messages for encouraging disease detection behaviors: A meta-analytic review. Journal of Communication, 59, 296–316. 10.1111/j.1460-2466.2009.01417.x [DOI] [PubMed] [Google Scholar]
- O’Keefe DJ, & Nan X (2012). The relative persuasiveness of gain- and loss-framed messages for promoting vaccination: A meta-analytic review. Health Communication, 27, 776–783. 10.1080/10410236.2011.64097 [DOI] [PubMed] [Google Scholar]
- Orbell S, & Hagger M (2006). Temporal framing and the decision to take part in Type II Diabetes screening: Effects of individual difference in consideration of future consequences. Health Psychology, 25, 537–548. 10.1037/0278-6133.25.4.537 [DOI] [PubMed] [Google Scholar]
- Orbell S, Perugini M, & Rakow J (2004). Individual difference in sensitivity to health communications: Consideration of future consequences. Health Psychology, 23, 388–396. 10.1037/0278-6133.23.4.388 [DOI] [PubMed] [Google Scholar]
- Oriel JD (1971). Natural history of genital warts. British Journal of Venereal Diseases, 47, 1–13. 10.1136/sti.47.1.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters BR, Joireman J, & Ridgway RL (2005). Individual differences in the consideration of future consequences scale correlate with sleep habits, sleep quality, and GPA in university students. Psychological Reports, 96, 817–824. 10.2466/pr0.96.3.817-824 [DOI] [PubMed] [Google Scholar]
- Petrocelli JV (2003). Factor validation of the Consideration of Future Consequences Scale: Evidence for a short version. Journal of Social Psychology, 143, 405–413. 10.1080/00224540309598453 [DOI] [PubMed] [Google Scholar]
- Rappange D, Werner BF & Van Exel NJ (2009). Back to the consideration of the future consequences scale: Time to reconsider. Journal of Social Psychology, 149, 562–584. 10.1080/00224540903232324 [DOI] [PubMed] [Google Scholar]
- Reagan-Steiner S, Yankey D, Jeyarajah J, Elam-Evans LD, Curtis CR, MacNeil J, …Singleton JA (2016). National, regional, state, and selected local area vaccination coverage among adolescents aged 13–17 years - United States, 2015. MMWR. Morbidity and Mortality Weekly Report, 65, 850–858. 10.15585/mmwr.mm6533a4. [DOI] [PubMed] [Google Scholar]
- Robbins T, & Burleson J (2015). Consideration of future consequences: A closer look at gender and cultural differences. International Journal of Business and Social Science, 6, 1–6. 10.1111/j.1750-8606.2011.00206.x [DOI] [Google Scholar]
- Rothman AJ, Martino SC, Bedell BT, Detweiler JB, & Salovey P (1999). The systematic influence of gain- and loss-framed messages on interest in and use of different types of health behavior. Personality and Social Psychology Bulletin, 25, 1355–1369. 10.1177/0146167299259003 [DOI] [Google Scholar]
- Rothman AJ, Salovey P (1997). Shaping perceptions to motivate healthy behavior: The role of message framing. Psychological Bulletin, 121, 3–19. 10.1037/0033-2909.121.1.3 [DOI] [PubMed] [Google Scholar]
- Rothman AJ, Bartels RD, Wlaschin J, & Salovey P (2006). The strategic use of gain- and loss-framed messages to promote healthy behavior: How theory can inform practice. Journal of Communication, 56, S202–S220. 10.1111/j.1460-2466.2006.00290.x [DOI] [Google Scholar]
- Rothman AJ, & Updegraff JA (2010). Specifying when and how gain- and loss framed messages motivate healthy behavior: An integrated approach. In Keren G (Ed.), Perspectives on framing (pp. 257–278). London, UK: Psychology Press/Taylor & Francis. [Google Scholar]
- Rothspan S, & Read SJ (1996). Present versus future time perspective and HIV risk among heterosexual college students. Health Psychology, 15, 131–134. 10.1037//0278-6133.15.2.13 [DOI] [PubMed] [Google Scholar]
- Saslow D, Andrews KS, Manassaram-Baptiste D, Loomer L, Lam KE, Fisher-Borne M, ... American Cancer Society Guideline Development Group. (2016). Human papillomavirus vaccination guideline update: American Cancer Society guideline endorsement. CA: A Cancer Journal for Clinicians, 66, 375–385. doi: https://doi-org.proxy-um.researchport.umd.edu/10.3322/caac.21355 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder M, & Debano KG (1985). Appeals to image and claims about quality: Understanding the psychology of advertising. Journal of Personality and Social Psychology, 49, 586–597. 10.1037/0022-3514.49.3.586 [DOI] [Google Scholar]
- Strathman A, Gleicher F, Boninger DS, & Edwards CS (1994). The consideration of future consequences scale: Weighing immediate and distant outcomes of behavior. Journal of Personality and Social Psychology, 66, 742–752. 10.1037/0022-3514.66.4.742 [DOI] [Google Scholar]
- Tversky A, & Kahneman D (1981). The framing of decisions and the psychology of choice. Science, 211, 453–458. 10.1007/978-3-642-70634-9_6 [DOI] [PubMed] [Google Scholar]
- Van’t Riet J, Cox AD, Cox D, Zimet GD, De Bruijn GJ, Van den Putte B, ... Ruiter RA (2016). Does perceived risk influence the effects of message framing? Revisiting the link between prospect theory and message framing. Health Psychology Review, 10, 447–459. 10.1080/17437199.2016.1176865 [DOI] [PubMed] [Google Scholar]
- Van’t Riet J, Cox AD, Cox D, Zimet GD, De Bruijn GJ, Van den Putte B, ... Ruiter RA (2014). Does perceived risk influence the effects of message framing? A new investigation of a widely held notion. Psychology & Health, 29, 933–949. 10.1080/08870446.2014.896916 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wen N, & Shen F (2016). Communicating to young Chinese about human papillomavirus vaccination: Examining the impact of message framing and temporal distance. Asian Journal of Communication, 26, 387–404. 10.1080/01292986.2016.1162821 [DOI] [Google Scholar]
- Wildavsky A, & Dake K (1990). Theories of risk perception: Who fears what and why? Daedalus, 114, 41–60. Retrieved from http://www.jstor.org.proxyum.researchport.umd.edu/stable/20025337 [Google Scholar]
- Wilson KG, Scott JF, Graham ID, Kozak JF, Chater S, Viola RA, …Curran D (2000). Attitudes of terminally ill patients toward euthanasia and physician-assisted suicide. Archives of Internal Medicine, 160, 2454–2460. 10.1001/archinte.160.16.2454 [DOI] [PubMed] [Google Scholar]
- Yeganeh N, Curtis D, & Kuo A (2010). Factors influencing HPV vaccination status in a Latino population; and parental attitudes towards vaccine mandates. Vaccine, 28, 4186–4198. 10.1016/j.vaccine.2010.04.010 [DOI] [PubMed] [Google Scholar]
- Zimbardo PG, & Boyd JN (1999). Putting time in perspective: A valid, reliable individual differences metric. Journal of Personality and Social Psychology, 77, 1271–1288. 10.1037/0022-3514.77.6.1271 [DOI] [Google Scholar]
- Zimbardo PG, Keough KA, & Boyd JN (1997). Present time perspective as a predictor of risky driving. Personality and Individual Differences, 23, 1007–1023. 10.1016/S0191-8869(97)00113-X [DOI] [Google Scholar]