

Supplemental Digital Content is available in the text
Keywords: breathomics, diagnosis, electronic nose, volatile organic compounds
Abstract
Background:
Volatile organic compounds (VOC) are end products of human metabolism (normal and disease-associated) that can be mainly excreted in breath, urine, and feces. Therefore, VOC can be very useful as markers of diseases and helpful for clinicians since its sampling is noninvasive, inexpensive, and painless. Electronic noses, or eNoses, provide an easy and inexpensive way to analyze gas samples. Thus, this device may be used for diagnosis, monitoring or phenotyping diseases according to specific breathprints (breath profile).
Objective:
In this review, we summarize data showing the ability of eNose to be used as a noninvasive tool to improve diagnosis in clinical settings.
Methods:
A PRISMA-oriented search was performed in PubMed and Cochrane Library. Only studies performed in humans and published since 2000 were included.
Results:
A total of 48 original articles, 21 reviews, and 7 other documents were eligible and fully analyzed. The quality assessment of the selected studies was conducted according to the Standards for Reporting of Diagnostic Accuracy. Airway obstructive diseases were the most studied and Cyranose 320 was the most used eNose.
Conclusions:
Several case–control studies were performed to test this technology in diverse fields. More than a half of the selected studies showed good accuracy. However, there are some limitations regarding sampling methodology, analysis, reproducibility, and external validation that need to be standardized. Additionally, it is urgent to test this technology in intend-to-treat populations. Thus, it is possible to think in the contribution of VOC analysis by eNoses in a clinical setting.
Introduction
Biochemical and biomolecular diagnostic methods used in medicine have their focus on blood and urine analysis. Breath analysis using electronic nose technology (eNose) could integrate the current examination procedures to assist clinicians in diagnosis and monitoring, since it is a noninvasive sampling technique, painless, inexpensive and that can be easily performed by sick patients, children, and elderly alike.1 The potential of exhaled breath analysis appeared with Hippocrates when he described an odor of fetor hepaticus as a clinical marker which is now related with hepatic diseases.2,3 The compounds related with that smell were later discover by gas chromatography coupled with mass spectrometry (GC-MS). Breath of patients with hepatic conditions showed higher levels of dimethyl sulfide, acetone, 2-butanone, and 2-pentanone and lower levels of indole and dimethyl selenide.3
Nowadays, exhaled breath is not the only type of sample used for gas analysis which can include fecal and urine headspaces. The term “headspace” is referred as the gas directly surrounding a sample. The constituents of the sample which have a high volatility will generally be present in the headspace in higher concentrations.4 Low volatile compounds are less likely to be found in a sample. Consequently, the concentration of molecules present in the headspace is not proportional to the concentration of the same molecules in liquid or solid sample.
The electronic nose or eNose is “an instrument which comprises an array of electronic chemical sensors with partial specificity and an appropriate patter-recognition system, capable of recognizing simple or complex odours” (1994).5 This device mimics the mammalian olfactory system and can identify different complex odors comparing the incoming odor with patterns previously learnt.6 When an odor (chemical input) is presented to the eNose causes a physical change in the sensors which is detected by the transducers and converted into an electrical signal creating a specific signature or smellprint.5 The rise and decline of the signal depends on some parameters: nature of the odor (type and concentration of the compounds), reaction and diffusion between odor and sensors, type of sensor, and ambient conditions.5 Methods based on mass spectrometry analysis can detect and identify which compounds are present in air samples being useful for pathophysiologic research.7 Yet, these methods are time consuming, expensive, and depend on a skilled operator which makes them unpractical to be applied at clinical settings. Electronic noses have the potential to overcome these disadvantages because they are relatively inexpensive, easy to use and provide a rapid analysis.5 To achieve this goal, it is necessary to create a prediction model with a training set of samples and external validate the model for further application.
The aim of this systematic review was to investigate how eNose technology may be applied as a noninvasive tool to improve diagnostic in clinical settings, based on published evidence. The clinical application of eNoses has been reviewed by some authors with special focus on pulmonary diseases, cancer, and gastroenterology.8–10 In this review, all published studies using eNose to diagnosis, phenotyping or monitoring diseases, pulmonary and extra pulmonary, are listed and discuss.
Methods
Search strategy
This systematic review was conducted following the PRISMA statement for authors of systematic reviews by searching for studies using the eNose technology as a diagnostic tool in medicine.11 The search was performed until the end of September 2017 in PubMed and Cochrane Library. The keywords “electronic nose” or “enose” and “diagnosis” or “diagnostic” or “phenotyping” or “phenotype” or “monitoring” were used. Full-text manuscripts in English published since January 2000, independently of the type of document (original article, review, comment, conference paper, letters, and book chapters), were assessed for eligibility. The adopted inclusion criteria were (a) diagnosis using electronic nose technology in clinical and medical applications; and (b) clinical trials. The exclusion criteria consisted of (a) trials not performed on human patients.
Quality assessment
The quality assessment of the selected studies was conducted according to the Standards for Reporting of Diagnostic Accuracy (STARD).12 The STARD statement was created to improve the quality of reporting diagnostic accuracy studies and incorporates a checklist of 30 items divided in 5 groups, covering the main sections of a scientific article, that should be included in the report of those studies. To better represent the quality assessment, STARD quality scores were defined: items reported in the study were classified as “Yes” and added 1 point to the score; items not reported or unclear were classified as “No” and “Unclear,” respectively, and added 0 points to the score (see Supplemental Digital Content).
Results
Study selection, characterization, and quality assessment
The systematic search using the aforementioned methodology yielded 295 studies. After removal of duplicates, 286 studies were accepted for screening. However, this number was increased to 324 after the inclusion of studies found by reference list searching. During the screening of titles and abstracts using the prespecified inclusion criteria, 238 studies were rejected, yielding 86 studies for full revision. Each of those studies was then reviewed. Ten studies were later excluded: 4 articles were focused on eNose technology and other breath analysis methods, 3 were focused on volatile organic compounds (VOC) and associated diseases, and 3 studies regarded clinical application but not diagnosis or monitoring of a disease. Reasons to exclude the studies at this stage were discussed with members of the review team. Thus, 76 studies were included: 48 original articles, 21 reviews, and 7 other documents (comments, letters, and book chapter). Figure 1 shows the flow diagram of search and selection process.
Figure 1.
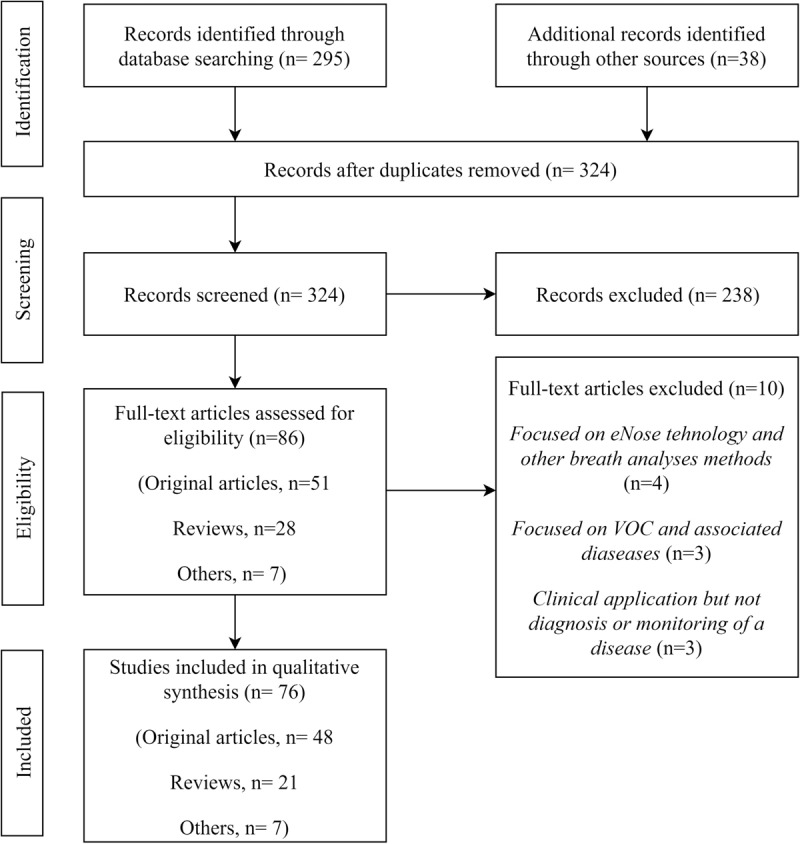
Summary of the literature search.
The eNose technology applied in health field was tested in several diseases to verify its potential on diagnosis or monitoring. The diseases in which this technology was tested can be divided into 5 groups: airway obstructions, respiratory infections, inflammatory diseases, cancer, and other diseases. Airway obstructions group is the one which includes more research and published studies (18 original articles). Chronic obstructive pulmonary disease (COPD) and asthma are the most studied diseases using the eNose technology as a diagnostic tool, followed by obstructive sleep apnea syndrome (OSAS). The second group with 9 studies includes ear, nose, and throat (ENT) infections, ventilator-associated pneumonia (VAP), invasive aspergillosis (IA), and late-onset sepsis (LOS). The inflammatory diseases with only 5 studies are sarcoidosis, inflammatory bowel disease, arthritis, inflammatory answer to ozone, and acute respiratory distress syndrome (ARDS). Furthermore, this technology has been applied to investigate the possibility of diagnosis different type of cancers, such as lung cancer, prostate cancer, colonrectal cancer, and malignant pleural mesothelioma (MPM). The other diseases that have been under investigation are cystic fibrosis, halitosis, amyotrophic lateral sclerosis (ALS), and renal dysfunction. The most commonly used eNose, in 81% of the studies, was the Cyranose 320 (Sensigent, Baldwin Park, CA) and the most current methodology for sampling collection consisted of using Tedlar Bags for trapping the exhaled breath after 5 minutes of tidal breathing through a VOC filter, to eliminate the influence of environmental VOC in the samples and was primarily described by Dragonieri et al.13 This methodology was used in 44% of the studies. Considering a cross-validation value (CVV) or an area under the curve (AUC) of 80% or more, 50% of the studies achieved those requirements (65% if we consider only studies that presented CVV or AUC values). However, only 10% of all studies performed external validation in a new recruited population. The summarized overview of the collected information is presented at Table 1 , and most important outcomes are presented in the discussion (Table 1 ). Table 2 presents the main results of reviews, comments, and book chapters found in the literature (Table 2 ).
Table 1.
Characteristics and main results of the included original studies
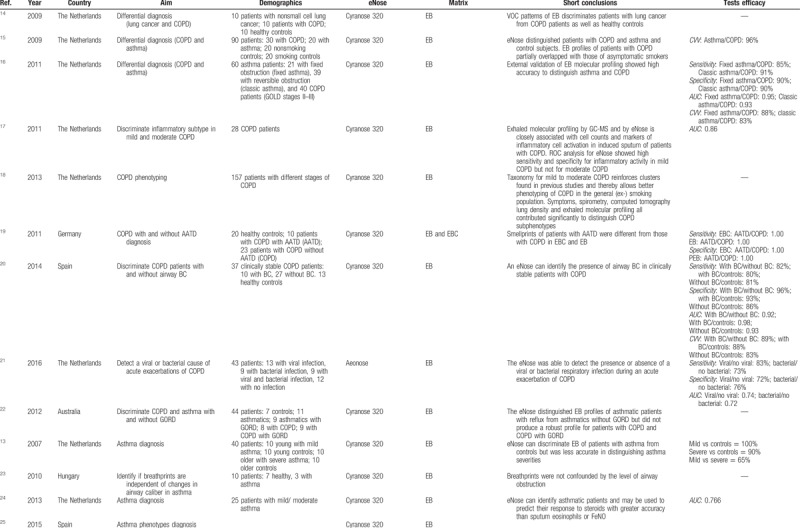
Table 1 (Continued).
Characteristics and main results of the included original studies
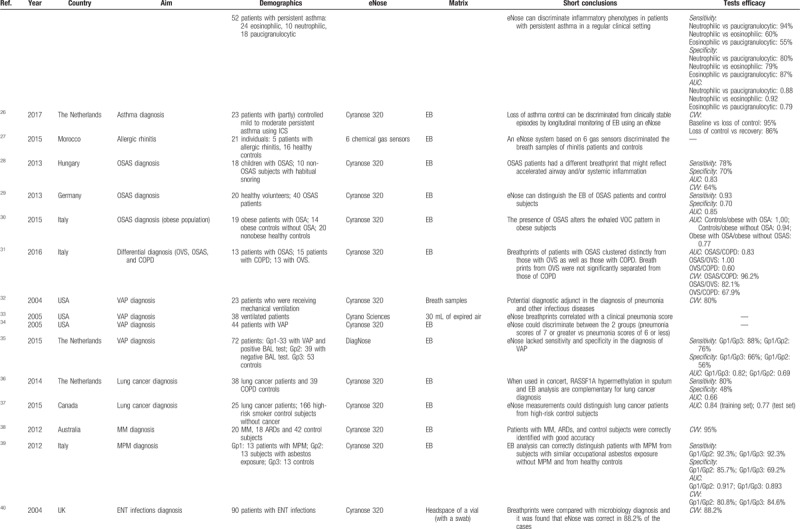
Table 1 (Continued).
Characteristics and main results of the included original studies
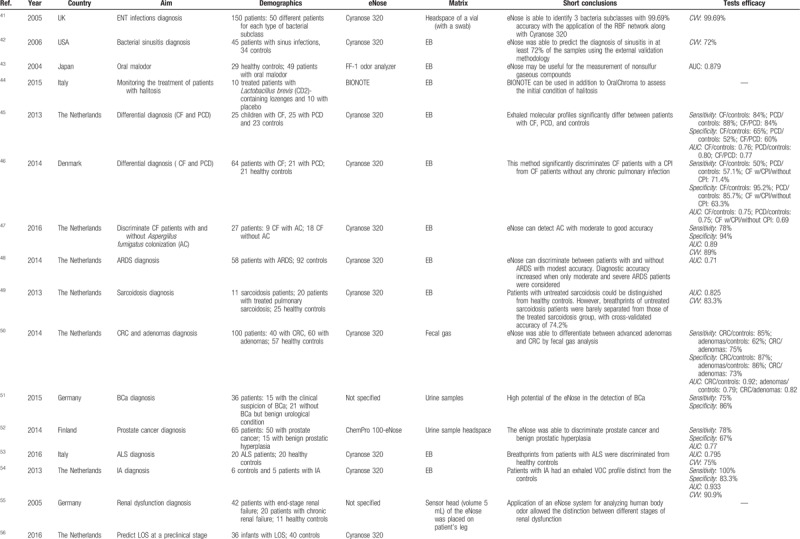
Table 1 (Continued).
Characteristics and main results of the included original studies
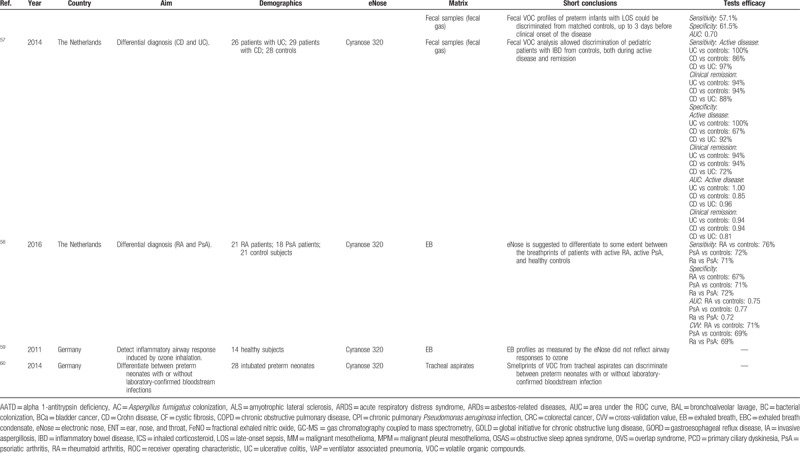
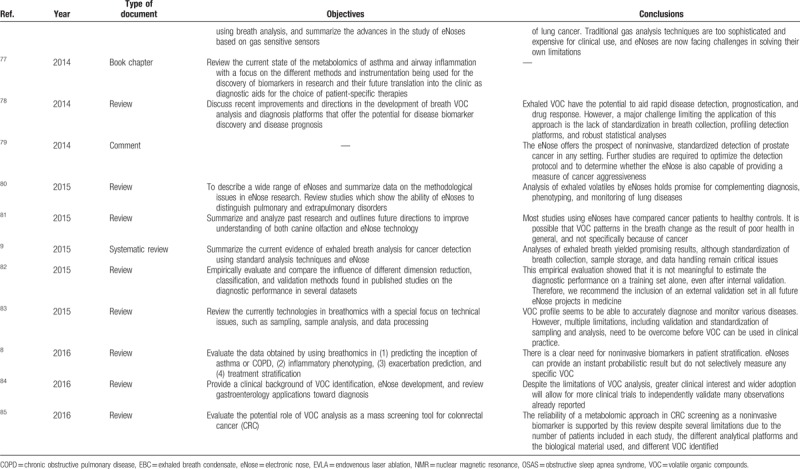
Table 2.
Characteristics and main results of the included studies (reviews, comments, and book chapters)
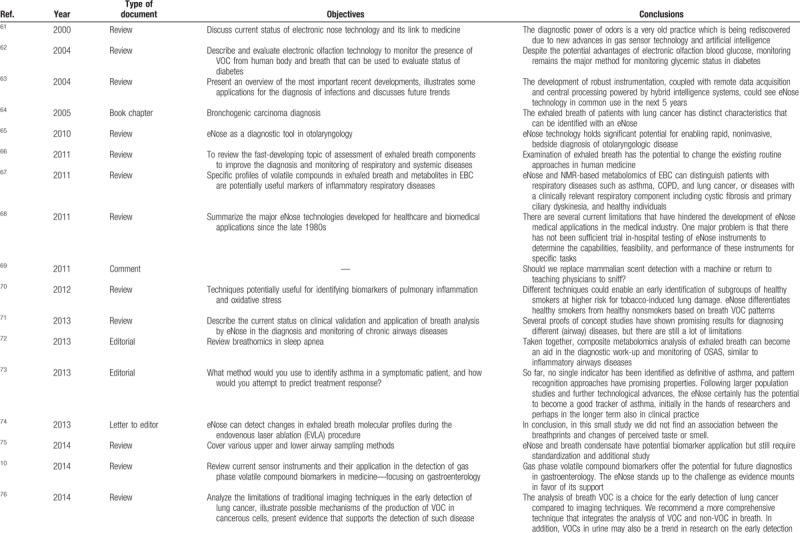
Table 2 (Continued).
Characteristics and main results of the included studies (reviews, comments, and book chapters)
Study population
An overview of the included studies is presented in Table 1 . The population used in each study vary significantly, from 10 (3 cases and 7 controls) to 171 participants (25 cases and 166 controls). In several studies, control group was composed by healthy subjects but in some cases participants with other health conditions or with smoking habits were included. The studies were conducted in several countries of Europe, North America, Asia, and Australia. The leader country with more investigation in this field was the Netherlands, with 19 studies. Seven studies evaluated more than 1 condition per survey, supporting the potential of using eNose for differential diagnosis.
Discussion
Diagnosis of airway obstructive diseases
The present review study presents an overview of eNose performance on diagnosis and phenotyping of diseases. Most of the included studies (18 original articles) concerned common airway obstructive diseases, such as COPD and asthma, and the VOC patterns were analyzed to differentiate these conditions, or to compare them with breathprints of other airway diseases, such as lung cancer.
Dragonieri et al found that COPD and nonsmall cell lung cancer have different exhaled VOC patterns which could be distinguished by eNose with a CVV of 85%.14 Furthermore, patients with nonsmall cell lung cancer could also be distinguished from healthy controls with a CVV of 80% or 90% when duplicates measurements were analyzed. At the same year, Fens et al published a study aiming to separate VOC profiles between COPD and asthma patients.15 They found different breath profiles between asthma subjects and COPD patients with an accuracy of 96%, as well as between nonsmoking controls and smoking controls with accuracies values of 95% and 92.5%, respectively. Later, the same group of authors conducted a study to externally validate the previous results, following STARD guidelines.16 The external validity of breath profiles showed that fixed asthma and classic asthma can be discriminated from COPD patients with high accuracy (88% and 83%, respectively) and sensitivity and specificity values varied from 85% up to 91% and 90%, respectively. Fens et al were able to differentiate mild and moderate types of COPD not only using eNose technology but also using mass spectrometry (GC-MS) and computed tomography scanning.18 Interestingly, the group found that eNose breathprints could be related with activation markers of eosinophils and neutrophils in mild asthma, suggesting that the eNose may not only be useful for asthma diagnosis, but also for phenotyping. Another successful application of the eNose was demonstrated in a study where individuals with COPD were discriminated according to their alpha 1-antitrypsin deficiency.19 The eNose was also able to discriminate COPD patients with and without airway bacterial colonization or identify the presence of a viral or bacterial cause in acute exacerbations.20,21
However, the first study using breathprint analysis of exhaled VOC by an eNose in airway obstructions was conducted in patients with mild and severe asthma.13 In this study, the degree of asthma severity was not discriminated by eNose, although it was able to distinguish asthma patients from controls with an accuracy of 90%. These results were further confirmed by another group and a sensitivity of 80% was reached, despite the low specificity of 65%.24 These results can be explained by the differences in methodologies, namely due to the effects of treatment that was discontinued in one of the studies. Nevertheless, changes in the airway caliber in asthma have been shown to not affect the breathprints.23 A recent study involving asthmatic subjects was conducted in Spain and aimed to phenotype the disease using the eNose.25 The eNose was able to differentiate inflammatory phenotypes (eosinophilic, neutrophilic, and paucigranulocytic) in patients with persistent asthma with sensitivities and specificities ranging from 55% up to 94% and 79% up to 87%, respectively. Exhaled breath profiles of patients with asthma were also evaluated in a longitudinal study using 2 different approaches to analyze breath samples (GC-MS and eNose).26 Both technologies were able to distinguish breathprints of patients collected during baseline, loss of control, and during recovery time. eNose technology had a higher accuracy than mass spectrometry (86–95% and 68–77%, respectively).
OSAS was primarily investigated by Benedek et al that discovered the potential of the eNose technology in discriminating OSAS from non-OSAS patients in a pediatric population (sensitivity: 78%, specificity: 70%, AUC: 0.80).28 These results are similar to those reported by Greulich et al (sensitivity: 93%, specificity: 70%, AUC: 0.85).29 Obesity was also found to affect the pattern of exhaled breath since obese patients with OSAS were discriminated from health controls (cross validation accuracy [CVA]: 97.4%), but were only moderate distinct from obese patients without OSAS (CVA: 67.6%).30 In a pilot study, OSAS breathprints were compared to OVS (overlap syndrome) and COPD.31 Patients with OSAS clustered distinctly from those with OVS as well as from those with COPD (AUC: 1.00 and 0.83), but patients with OVS were not significantly different from those with COPD (AUC: 0.60).
The significant interest of researchers in studying eNose technology as a diagnosis tool is notable, especially concerning airway obstructive diseases. Clinical diagnosis can be difficult because of related symptoms between different diseases, which makes breathprint analysis very useful if further research confirms these primary results. Diagnosis is not the only application of breathprint analysis, as it also appears to be promising for the phenotyping and monitoring of diseases.
Diagnosis of infectious diseases
Infectious diseases are caused by pathogenic microorganisms that are known to produce specific VOC. Several groups hypothesized that eNose could be used as a noninvasive tool to identify specific signatures of these health conditions.
The most studied condition was VAP, a type of lung infection. A group in the United States discovers that Cyranose 320 was capable to correlate different breathprints to a pneumonia score.34 However, it was Schnabel et al that presented a more detailed study revealing a sensitivity of 88% and a specificity of 66% in the discrimination between VAP patients with a positive bronchoalveolar lavage test and healthy controls.35
ENT infections are very common and the eNose technology, in a preliminary study with 90 patients, was able to identify the presence of bacterial infections in 88.2% of the cases.40 This result was also obtained by Dutta et al that, additionally, was capable to distinguish between 3 classes of Staphylococcus aureus infections (MRSA, MSSA, and C-NS).41 A more specific study was conducted in patients with a positive diagnosis for bacterial sinusitis.42 The eNose could predict the diagnosis of sinusitis in at least 72% of the samples using the external validation methodology. However, no further studies aiming to predict ENT infections by eNose in patients were conducted since 2006.
The most recent studies focused on diagnosis of IA and the prediction of LOS at a preclinical stage.54,56 In the first one, eNose could established distinct VOC profile in patients with IA and controls with an AUC of 0.93.54 In the last one, fecal VOC profile of preterm infants with LOS was discriminated from matched controls with a reasonable AUC of 0.70.56
Microorganisms produce different VOC that can be detected in air samples by eNose. These studies showed that exhaled breath can be analyzed by eNose, but also fecal gas which showed distinct VOC profiles. The results are promising but further investigation is required.
Diagnosis of inflammatory diseases
There is some recent research in this field; however, the number of studies is still low. Dragonieri et al started to study sarcoidosis in 11 untreated patients, 20 treated pulmonary sarcoidosis patients and 25 healthy controls.49 Patients with untreated sarcoidosis were distinguished from healthy controls with an AUC of 0.825 and a CVA of 83.3%. This number decreased when breathprints of untreated patients were compared with the treated group (CVA: 74.2%). ARDS was also a condition investigated in 58 patients and 92 controls.48 The 2 groups were separated with an AUC of 0.71. Differential diagnosis of Crohn disease and ulcerative colitis yielded a promising result in a pediatric population during active and remissive disease.57 The values of sensitivity and specificity varied from 88% up to 100% and 67% up to 100%, respectively. The eNose was also tested in rheumatoid arthritis and psoriatic arthritis yielded moderate to poor values of sensitivity and specificity.58
Inflammatory diseases are less investigated, and more studies are required to confirm the aforementioned observations. Nevertheless, these results are promising, especially for sarcoidosis.
Diagnosis of cancer
More recently, the eNose technology has been tested to diagnose some types of cancer. Surprisingly, lung cancer was not the first research target. An Australian group reported that, in 88% of the cases, eNose could separate MPM patients from controls.38 These results were similar to another study performed by Dragonieri et al.39 Both studies included patients with significant asbestos exposure but without MPM to compare with the MPM group. MPM subjects could be discriminated from those with asbestos exposure (sensitivity: 92.3%, specificity: 85.7%, AUC: 0.917) and from controls (sensitivity: 92.3%, specificity: 69.2%, AUC: 0.893).39 Lung cancer was then explored by McWilliams et al and it was found that in 80% of the cases, eNose measurements were able to distinguish lung cancer patients from high-risk smoking control subjects without cancer.37 These results were similar to a previous study where eNose reached a performance of 80% of sensitivity and 48% of specificity.36
Pilot studies in prostate, bladder, and colonrectal cancer using the air scape of urine and feces samples for analysis were conducted recently.50–52 The ChemPro 100-eNose could discriminate prostate cancer and benign prostatic hyperplasia with moderate values of sensitivity and specificity of 78% and 67%, respectively.52 Electronic nose could also separate bladder cancer and patients with benign urological condition with moderate to good sensitivity and specificity (75% and 86%, respectively).51 Finally, Cyranose 320 was able to distinguish the fecal gas profile of 40 patients with colonrectal cancer, 60 patients with advanced adenomas, and 57 healthy controls.50 Sensitivity and specificity varied from 62% up to 85% and 73% up to 87%.
Cancer diagnosis using air analysis of exhaled breath, urine, and fecal samples is a recent focus of investigation, revealing promising results. Although cancers related to the respiratory system have been further studied, only pilot studies have been performed so far, and a validation of these results is still required.
Other diseases
The diagnosis by eNose was also applied to differentiate breathprints of cystic fibrosis (CF) and primary ciliary dyskinesia (PCD) patients in 2 different studies, showing different results.45,46 The first reached a sensitivity of 84% and a specificity of 60%, when breathprints of both diseases were compared. Comparing both diseases with control group, similar results were observed (sensitivity: 88% and 84%; specificity: 52% and 60%).45 The other study did not compare the 2 diseases.46 Comparisons between CF or PCD and the control group showed a lower sensitivity when compared to the previous study (50% and 57%, respectively) but with a higher specificity (95% and 85%, respectively). The samples were analyzed with Cyranose 320 and both used a VOC filter to minimize the influence of environmental VOC on the breath profiles. The major difference was among the population, the first used children's breathing samples, while the last studied samples from young adults.
Only 1 study evaluated the capacity of eNose to separate healthy subjects from patients with renal failure, yielding a correct classification of 95.2%.55 However, a completely different methodology was used. Authors investigated body odor with the sensor head on the leg of patients. More recently, ALS was also investigated and breath profiles from patients were moderately discriminated from healthy controls (CVA: 75%).53 Finally, oral malodor was assessed, and an AUC of 0.879 was reached comparing control subjects and malodor patients.43
This technology can be explored and investigated to diagnose several diseases. Further research in other health conditions is expected to test the potential use of this diagnostic tool.
Limitations
There are some limitations in studies using eNose technology as a possible noninvasive diagnosis tool. The most evident is that eNose cannot identify and quantify the compounds present in the sample. Electronic noses are used to detect patterns and not individual molecules. Some studies have demonstrated an association between the eNose technology and mass spectrometry, yielding a more complete analysis.17,18 However, breathprint analysis allows the quick and easy assessment of an exhaled breath sample with thousands of volatile molecules. Another limitation is related to exhale breath sampling since exogenous VOC can be present in samples. Breathprints are critically dependent on the methods of collection and sampling of exhaled breath. The most commonly used technique was described by Dragonieri et al.13 Sample collection consists of asking patients to breath normally for 5 minutes through a 3-way nonrebreathing valve with a VOC filter at the inspiratory port and a silica filter at the expiratory port to promote inspiratory VOC filtering and air drying, respectively. Therefore, it is possible to minimize any influence of humidity and environmental VOC on exhaled VOC patterns.13,15 After a maximal deep inspiration, patients exhaled a single vital capacity volume into a 10 L Tedlar bag connected to the expiratory port and silica reservoir.13 Almost 50% of the studies described in this review used this sampling methodology. In addition to this method, researchers should also adopt a restrict protocol regarding to food and beverage intake prior to sampling. Sampling methods should be standardized to achieve comparable results between studies and to improve diagnostic accuracy.
As a pioneer area, much of research involves pilot studies to evaluate the potential of eNose to discriminate breathprints of controls from patients with a specific disease. However, in the airway obstructions group, there are some recent studies that try to distinguish different stages and severities of a disease (mainly COPD and asthma).17,25 This type of research is expected to increase once its clinical application becomes more evident, as well as studies to help in treatment management and guidance of therapies.
The external validation allows to confirm and provide robustness to the obtained results. Unfortunately, only 5 studies performed external validation. External validation requires a training set and a validation set with newly recruited patients to assess the diagnostic accuracy.16 In the future, this validation methodology should be more recurrent to give strength to the results and introduce this tool into real clinical practice. Additionally, STARD guidelines for diagnostic accuracy studies should be followed to increase transparency and strength of results.
There are some limitations regarding to the methodology that should be solved to enable comparisons of results across studies. Still, it is necessary to do studies in larger populations to achieve robust results and include pediatric subjects, not just adults.
Future perspectives
In the future, research in this field is expected to increase due to the promising results demonstrated in previous studies, especially in airway obstructive diseases. The main objective is to achieve a universal methodology, with adequate reproducibility and repeatability, to enable comparisons between studies. External validation should be performed to increase robustness of the results. Subsequently, studies on larger, representative, and intend-to-treat populations are needed to evaluate this technology in a real clinical setting in the presence of several confounders. It should be emphasized that pediatric population must be included in further studies. Thereby, it is possible to think about a clinical application of eNose technology, firstly as a complementary diagnostic approach for other traditional tools.
Conclusions
In conclusion, there is a need for a simple, noninvasive, inexpensive, and easy-to-perform technique to assess complex biological samples. GC-MS studies already proven that air analysis, especially of exhaled breath, can be a tool to evaluate an individual's metabolic status (normal or disease-associated). In recent years, several studies using eNose technology to analyze gas samples have shown promising results to diagnose different diseases, not only respiratory but also infectious and inflammatory diseases and various types of cancers. Electronic nose analysis could be useful in a clinical setting because they are portable, easy to perform, inexpensive, rapid and do not require a specialized technician. Many of the previous studies have shown the moderate to good accuracy of this technology to differentiate several conditions from controls, especially airway obstructive diseases. However, it is a priority to create guidelines for standardized breath sampling, analysis and interpretation of the results. Additionally, it is necessary to externally validate the results in independent datasets of newly recruited patients to strengthen the results. Finally, studies on larger and representative populations are needed to test this technology in a real clinical setting. Reproducibility and repeatability of measurements using eNoses should also be studied and optimized to ensure comparable results.
Acknowledgments
The authors gratefully acknowledge funding from Project NORTE-01-0145-FEDER-000010—Health, Comfort and Energy in the Built Environment (HEBE), cofinanced by Programa Operacional Regional do Norte (NORTE2020), through Fundo Europeu de Desenvolvimento Regional (FEDER).
The current work has been supported by the EXPOSE project, which is financed by FEDER/FNR and by Fundação para a Ciência e Tecnologia (EXPOSE 02/SAICT/2016—Project no. 023222).
Conflicts of interest
The authors declare no conflicts of interest.
Supplementary Material
References
- [1].Boots AW, Bos LD, van der Schee MP, et al. Exhaled molecular fingerprinting in diagnosis and monitoring: validating volatile promises. Trends Mol Med. 2015;21:633–644. [DOI] [PubMed] [Google Scholar]
- [2].Risby TH, Solga SF. Current status of clinical breath analysis. Appl Phys B. 2006;85:421–426. [Google Scholar]
- [3].Vandenvelde S, Nevens F, Vanhee P, et al. GC–MS analysis of breath odor compounds in liver patients. J Chromatogr B. 2008;875:344–348. [DOI] [PubMed] [Google Scholar]
- [4].Wahl HG, Hoffmann A, Luft D, et al. Analysis of volatile organic compounds in human urine by headspace gas chromatography–mass spectrometry with a multipurpose sampler. J Chromatogr A. 1999;847:117–125. [DOI] [PubMed] [Google Scholar]
- [5].Gardner JW, Bartlett PN. A brief history of electronic noses. Sens Actuators B Chem. 1994;18:210–211. [Google Scholar]
- [6].Persaud K, Dodd G. Analysis of discrimination mechanisms in the mammalian olfactory system using a model nose. Nature. 1982;299:352–355. [DOI] [PubMed] [Google Scholar]
- [7].Van Berkel JJBN, Dallinga JW, Möller GM, et al. A profile of volatile organic compounds in breath discriminates COPD patients from controls. Respir Med. 2010;104:557–563. [DOI] [PubMed] [Google Scholar]
- [8].Bos LD, Sterk PJ, Fowler SJ. Breathomics in the setting of asthma and chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138:970–976. [DOI] [PubMed] [Google Scholar]
- [9].Krilaviciute A, Heiss JA, Leja M, et al. Detection of cancer through exhaled breath: a systematic review. Oncotarget. 2015;6:38643–38657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Arasaradnam RP, Covington JA, Harmston C, et al. Review article: Next generation diagnostic modalities in gastroenterology—gas phase volatile compound biomarker detection. Aliment Pharmacol Ther. 2014;39:780–789. [DOI] [PubMed] [Google Scholar]
- [11].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Bossuyt PM, Reitsma JB, Bruns DE, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ. 2015;351:h5527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Dragonieri S, Schot R, Mertens BJA, et al. An electronic nose in the discrimination of patients with asthma and controls. J Allergy Clin Immunol. 2007;120:856–862. [DOI] [PubMed] [Google Scholar]
- [14].Dragonieri S, Annema JT, Schot R, et al. An electronic nose in the discrimination of patients with non-small cell lung cancer and COPD. Lung Cancer. 2009;64:166–170. [DOI] [PubMed] [Google Scholar]
- [15].Fens N, Zwinderman AH, van der Schee MP, et al. Exhaled breath profiling enables discrimination of chronic obstructive pulmonary disease and asthma. Am J Respir Crit Care Med. 2009;180:1076–1082. [DOI] [PubMed] [Google Scholar]
- [16].Fens N, Roldaan AC, van der Schee MP, et al. External validation of exhaled breath profiling using an electronic nose in the discrimination of asthma with fixed airways obstruction and chronic obstructive pulmonary disease. Clin Exp Allergy. 2011;41:1371–1378. [DOI] [PubMed] [Google Scholar]
- [17].Fens N, de Nijs SB, Peters S, et al. Exhaled air molecular profiling in relation to inflammatory subtype and activity in COPD. Eur Respir J. 2011;38:1301–1309. [DOI] [PubMed] [Google Scholar]
- [18].Fens N, van Rossum AGJ, Zanen P, et al. Subphenotypes of mild-to-moderate COPD by factor and cluster analysis of pulmonary function, CT imaging and breathomics in a population-based survey. COPD. 2013;10:277–285. [DOI] [PubMed] [Google Scholar]
- [19].Hattesohl ADM, Jorres RA, Dressel H, et al. Discrimination between COPD patients with and without alpha 1-antitrypsin deficiency using an electronic nose. Off J Asian Soc Respirol. 2011;16:1258–1264. [DOI] [PubMed] [Google Scholar]
- [20].Sibila O, Garcia-Bellmunt L, Giner J, et al. Identification of airway bacterial colonization by an electronic nose in chronic obstructive pulmonary disease. Respir Med. 2014;108:1608–1614. [DOI] [PubMed] [Google Scholar]
- [21].van Geffen WH, Bruins M, Kerstjens HAM. Diagnosing viral and bacterial respiratory infections in acute COPD exacerbations by an electronic nose: a pilot study. J Breath Res. 2016;10:036001. [DOI] [PubMed] [Google Scholar]
- [22].Timms C, Thomas PS, Yates DH. Detection of gastro-oesophageal reflux disease (GORD) in patients with obstructive lung disease using exhaled breath profiling. J Breath Res [Internet]. 2012;6: [cited 2017 Sep 11]. Available from: http://stacks.iop.org/1752-7163/6/i=1/a=016003?key=crossref.27660ac0c7241890bceec41e534d21a7. [DOI] [PubMed] [Google Scholar]
- [23].Lazar Z, Fens N, Maten J, et al. Electronic nose breathprints are independent of acute changes in airway caliber in asthma. Sensors. 2010;10:9127–9138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].van der Schee MP, Palmay R, Cowan JO, et al. Predicting steroid responsiveness in patients with asthma using exhaled breath profiling. Clin Exp Allergy. 2013;43:1217–1225. [DOI] [PubMed] [Google Scholar]
- [25].Plaza V, Crespo A, Giner J, et al. Inflammatory asthma phenotype discrimination using an electronic nose breath analyzer. J Investig Allergol Clin Immunol. 2015;25:431–437. [PubMed] [Google Scholar]
- [26].Brinkman P, van de Pol MA, Gerritsen MG, et al. Exhaled breath profiles in the monitoring of loss of control and clinical recovery in asthma. Clin Exp Allergy. 2017;47:1159–1169. [DOI] [PubMed] [Google Scholar]
- [27].Saidi T, Tahri K, El Bari N, et al. Detection of seasonal allergic rhinitis from exhaled breath VOCs using an electronic nose based on an array of chemical sensors. IEEE Sensors. 2015;1566–1569. South Korea. [Google Scholar]
- [28].Benedek P, Lázár Z, Bikov A, et al. Exhaled biomarker pattern is altered in children with obstructive sleep apnoea syndrome. Int J Pediatr Otorhinolaryngol. 2013;77:1244–1247. [DOI] [PubMed] [Google Scholar]
- [29].Greulich T, Hattesohl A, Grabisch A, et al. Detection of obstructive sleep apnoea by an electronic nose. Eur Respir J. 2013;42:145–155. [DOI] [PubMed] [Google Scholar]
- [30].Dragonieri S, Porcelli F, Longobardi F, et al. An electronic nose in the discrimination of obese patients with and without obstructive sleep apnoea. J Breath Res. 2015;9:026005. [DOI] [PubMed] [Google Scholar]
- [31].Dragonieri S, Quaranta VN, Carratu P, et al. Exhaled breath profiling in patients with COPD and OSA overlap syndrome: a pilot study. J Breath Res. 2016;10:041001. [DOI] [PubMed] [Google Scholar]
- [32].Hockstein NG, Thaler ER, Torigian D, et al. Diagnosis of pneumonia with an electronic nose: correlation of vapor signature with chest computed tomography scan findings. Laryngoscope. 2004;114:1701–1705. [DOI] [PubMed] [Google Scholar]
- [33].Hanson CW, Thaler ER. Electronic nose prediction of a clinical pneumonia score: biosensors and microbes. Anesthesiology. 2005;102:63–68. [DOI] [PubMed] [Google Scholar]
- [34].Hockstein NG, Thaler ER, Lin Y, et al. Correlation of pneumonia score with electronic nose signature: a prospective study. Ann Otol Rhinol Laryngol. 2005;114:504–508. [DOI] [PubMed] [Google Scholar]
- [35].Schnabel RM, Boumans MLL, Smolinska A, et al. Electronic nose analysis of exhaled breath to diagnose ventilator-associated pneumonia. Respir Med. 2015;109:1454–1459. [DOI] [PubMed] [Google Scholar]
- [36].Hubers AJ, Brinkman P, Boksem RJ, et al. Combined sputum hypermethylation and eNose analysis for lung cancer diagnosis. J Clin Pathol. 2014;67:707–711. [DOI] [PubMed] [Google Scholar]
- [37].McWilliams A, Beigi P, Srinidhi A, et al. Sex and smoking status effects on the early detection of early lung cancer in high-risk smokers using an electronic nose. Trans Biomed Eng. 2015;62:2044–2054. [DOI] [PubMed] [Google Scholar]
- [38].Chapman EA, Thomas PS, Stone E, et al. A breath test for malignant mesothelioma using an electronic nose. Eur Respir J. 2012;40:448–454. [DOI] [PubMed] [Google Scholar]
- [39].Dragonieri S, van der Schee MP, Massaro T, et al. An electronic nose distinguishes exhaled breath of patients with malignant pleural mesothelioma from controls. Lung Cancer. 2012;75:326–331. [DOI] [PubMed] [Google Scholar]
- [40].Shykhon ME, Morgan DW, Dutta R, et al. Clinical evaluation of the electronic nose in the diagnosis of ear, nose and throat infection: a preliminary study. J Laryngol Otol. 2004;118:706–709. [DOI] [PubMed] [Google Scholar]
- [41].Dutta R, Morgan D, Baker N, et al. Identification of Staphylococcus aureus infections in hospital environment: electronic nose based approach. Sens Actuators B Chem. 2005;109:355–362. [Google Scholar]
- [42].Thaler ER, Hanson CW. Use of an electronic nose to diagnose bacterial sinusitis. Am J Rhinol. 2006;20:170–172. [PubMed] [Google Scholar]
- [43].Tanaka M, Anguri H, Nonaka A, et al. Clinical assessment of oral malodor by the electronic nose system. J Dent Res. 2004;83:317–321. [DOI] [PubMed] [Google Scholar]
- [44].Marchetti E, Tecco S, Santonico M, et al. Multi-sensor approach for the monitoring of halitosis treatment via Lactobacillus brevis (CD2)-containing lozenges—a randomized, double-blind placebo-controlled clinical trial. Sensors. 2015;15:19583–19596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Paff T, van der Schee MP, Daniels JMA, et al. Exhaled molecular profiles in the assessment of cystic fibrosis and primary ciliary dyskinesia. J Cyst Fibros. 2013;12:454–460. [DOI] [PubMed] [Google Scholar]
- [46].Joensen O, Paff T, Haarman EG, et al. Exhaled breath analysis using electronic nose in cystic fibrosis and primary ciliary dyskinesia patients with chronic pulmonary infections. PLoS ONE. 2014;9:e115584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].de Heer K, Kok MGM, Fens N, et al. Detection of airway colonization by Aspergillus fumigatus by use of electronic nose technology in patients with cystic fibrosis. J Clin Microbiol. 2016;54:569–575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Bos LD, Schultz MJ, Sterk PJ. Exhaled breath profiling for diagnosing acute respiratory distress syndrome. BMC Pulm Med. 2014;14:72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Dragonieri S, Brinkman P, Mouw E, et al. An electronic nose discriminates exhaled breath of patients with untreated pulmonary sarcoidosis from controls. Respir Med. 2013;107:1073–1078. [DOI] [PubMed] [Google Scholar]
- [50].de Meij TG, Larbi IB, van der Schee MP, et al. Electronic nose can discriminate colorectal carcinoma and advanced adenomas by fecal volatile biomarker analysis: proof of principle study. Int J Cancer. 2014;134:1132–1138. [DOI] [PubMed] [Google Scholar]
- [51].Horstmann M, Steinbach D, Fischer C, et al. An electronic nose system detects bladder cancer in urine specimen: first results of a pilot study. J Urol. 2015;193:e560–e561. [Google Scholar]
- [52].Roine A, Veskimae E, Tuokko A, et al. Detection of prostate cancer by an electronic nose: a proof of principle study. J Urol. 2014;192:230–234. [DOI] [PubMed] [Google Scholar]
- [53].Dragonieri S, Quaranta VN, Carratu P, et al. An electronic nose may sniff out amyotrophic lateral sclerosis. Respir Physiol Neurobiol. 2016;232:22–25. [DOI] [PubMed] [Google Scholar]
- [54].de Heer K, van der Schee MP, Zwinderman K, et al. Electronic nose technology for detection of invasive pulmonary aspergillosis in prolonged chemotherapy-induced neutropenia: a proof-of-principle study. J Clin Microbiol. 2013;51:1490–1495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Voss A, Baier V, Reisch R, et al. Smelling renal dysfunction via electronic nose. Ann Biomed Eng. 2005;33:656–660. [DOI] [PubMed] [Google Scholar]
- [56].Berkhout DJC, Niemarkt HJ, Buijck M, et al. Detection of sepsis in preterm infants by fecal volatile organic compounds analysis: a proof of principle study. J Pediatr Gastroenterol Nutr [Internet]. 2016;30.Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/284/CN-01247284/frame.html. [DOI] [PubMed] [Google Scholar]
- [57].de Meij TGJ, de Boer NKH, Benninga MA, et al. Faecal gas analysis by electronic nose as novel, non-invasive method for assessment of active and quiescent paediatric inflammatory bowel disease: proof of principle study. J Crohns Colitis. 2014. [DOI] [PubMed] [Google Scholar]
- [58].Brekelmans MP, Fens N, Brinkman P, et al. Smelling the diagnosis: the electronic nose as diagnostic tool in inflammatory arthritis. A case-reference study. PLoS ONE [Internet]. 2016;11: [cited 2017 Sep 11]. Available from: http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0151715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Biller H, Holz O, Windt H, et al. Breath profiles by electronic nose correlate with systemic markers but not ozone response. Respir Med. 2011;105:1352–1363. [DOI] [PubMed] [Google Scholar]
- [60].Rogosch T, Herrmann N, Maier RF, et al. Detection of bloodstream infections and prediction of bronchopulmonary dysplasia in preterm neonates with an electronic nose. J Pediatr. 2014;165:622–624. [DOI] [PubMed] [Google Scholar]
- [61].Pavlou AK, Turner AP. Sniffing out the truth: clinical diagnosis using the electronic nose. Clin Chem Lab Med. 2000;38:99–112. [DOI] [PubMed] [Google Scholar]
- [62].Dalton P, Gelperin A, Preti G. Volatile metabolic monitoring of glycemic status in diabetes using electronic olfaction. Diabetes Technol Ther. 2004;6:534–544. [DOI] [PubMed] [Google Scholar]
- [63].Turner AP, Magan N. Electronic noses and disease diagnostics. Nat Rev Microbiol. 2004;2:161–166. [DOI] [PubMed] [Google Scholar]
- [64].Machado RF, Laskowski D, Deffenderfer O, et al. Detection of lung cancer by sensor array analyses of exhaled breath. Am J Respir Crit Care Med. 2005;171:1286–1291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [65].Charaklias N, Raja H, Humphreys ML, et al. The future of early disease detection? Applications of electronic nose technology in otolaryngology. J Laryngol Otol. 2010;124:823–827. [DOI] [PubMed] [Google Scholar]
- [66].Popov TA. Human exhaled breath analysis. Ann Allergy Asthma Immunol. 2011;106:451–456. [DOI] [PubMed] [Google Scholar]
- [67].Santini G, Mores N, Penas A, et al. Electronic nose and exhaled breath NMR-based metabolomics applications in airways disease. Curr Top Med Chem. 2016;16:1610–1630. [DOI] [PubMed] [Google Scholar]
- [68].Wilson AD, Baietto M. Advances in electronic-nose technologies developed for biomedical applications. Sensors. 2011;11:1105–1176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].Arasaradnam RP, Nwokolo CU, Bardhan KD, et al. Electronic nose versus canine nose: clash of the titans. Gut. 2011;60:1768. [DOI] [PubMed] [Google Scholar]
- [70].Malerba M, Montuschi P. Non-invasive biomarkers of lung inflammation in smoking subjects. Curr Med Chem. 2012;19:187–196. [DOI] [PubMed] [Google Scholar]
- [71].Fens N, van der Schee MP, Brinkman P, et al. Exhaled breath analysis by electronic nose in airways disease. Established issues and key questions. Clin Exp Allergy. 2013;43:705–715. [DOI] [PubMed] [Google Scholar]
- [72].Sterk PJ, Fens N, Carpagnano GE. Wake-up call by breathomics in sleep apnoea. Eur Respir J. 2013;42:1–4. [DOI] [PubMed] [Google Scholar]
- [73].Bjerg A, Lotvall J. Sniffing out steroid responsiveness in asthma using an electronic nose. Clin Exp Allergy. 2013;43:1198–1199. [DOI] [PubMed] [Google Scholar]
- [74].Gauw SA, Fens N, Knobel HH, et al. Analysing exhaled breath during endovenous laser ablation of varicose veins using an electronic nose and gas chromatography-mass spectrometry. Phlebology. 2013;28:114–116. [DOI] [PubMed] [Google Scholar]
- [75].Alexis NE. Biomarker sampling of the airways in asthma. Curr Opin Pulm Med. 2014;20:46–52. [DOI] [PubMed] [Google Scholar]
- [76].Li W, Liu H-Y, Jia Z-R, et al. Advances in the early detection of lung cancer using analysis of volatile organic compounds: from imaging to sensors. Asian Pac J Cancer Prev. 2014;15:4377–4384. [DOI] [PubMed] [Google Scholar]
- [77].Luxon BA. Metabolomics in asthma. Adv Exp Med Biol. 2014;795:207–220. [DOI] [PubMed] [Google Scholar]
- [78].Rattray NJW, Hamrang Z, Trivedi DK, et al. Taking your breath away: metabolomics breathes life in to personalized medicine. Trends Biotechnol. 2014;32:538–548. [DOI] [PubMed] [Google Scholar]
- [79].Phillips R. Prostate cancer: eNose-man's new best friend? Nat Rev Urol. 2014;11:187. [DOI] [PubMed] [Google Scholar]
- [80].Bikov A, Lazar Z, Horvath I. Established methodological issues in electronic nose research: how far are we from using these instruments in clinical settings of breath analysis? J Breath Res. 2015;9:034001. [DOI] [PubMed] [Google Scholar]
- [81].Brooks SW, Moore DR, Marzouk EB, et al. Canine olfaction and electronic nose detection of volatile organic compounds in the detection of cancer: a review. Cancer Invest. 2015;33:411–419. [DOI] [PubMed] [Google Scholar]
- [82].Leopold JH, Bos LDJ, Sterk PJ, et al. Comparison of classification methods in breath analysis by electronic nose. J Breath Res. 2015;9:046002. [DOI] [PubMed] [Google Scholar]
- [83].Scarlata S, Pennazza G, Santonico M, et al. Exhaled breath analysis by electronic nose in respiratory diseases. Expert Rev Mol Diagn. 2015;15:933–956. [DOI] [PubMed] [Google Scholar]
- [84].Chan DK, Leggett CL, Wang KK. Diagnosing gastrointestinal illnesses using fecal headspace volatile organic compounds. World J Gastroenterol. 2016;22:1639–1649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [85].Di Lena M, Porcelli F, Altomare DF. Volatile organic compounds as new biomarkers for colorectal cancer: a review. Colorectal Dis. 2016;18:654–663. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.