

Abstract
Avulsion fractures of the posterior cruciate ligament (PCL) are a rare, but serious, knee pathology. Early surgical treatment is regarded as necessary to maintain knee stability. Recommended management involves open reduction with internal fixation through a posterior approach. However, open surgeries are associated with a greater risk of complications. Current data suggest excellent outcomes for arthroscopic-assisted fixation, with a low complication rate. The purpose of this technical note is to present an all-arthroscopic PCL distal reattachment with extracortical fixation technique. This technique provides precise fracture reduction, is easily reproducible, and is relatively safe to treat PCL tibial avulsion fractures.
The posterior cruciate ligament (PCL) is the stronger of the 2 cruciate ligaments of the knee and has a major role in stabilizing the knee joint.1, 2 Functionally, the PCL is a primary restraint to posterior tibial translation at all flexion angles and also for internal rotation beyond 90° of flexion.3 Compared with the anterior cruciate ligament (ACL), the PCL has a high potential for spontaneous healing, and thus it requires different treatment approaches.4 Some studies have reported good outcomes after conservative treatment of partial PCL tears, whereas others have reported poor results at long-term follow-up, with disabling symptoms and functional limitations.5 Several techniques of reconstructions for mid-substance PCL injuries have been described in the literature, depending on tibial graft fixation (transtibial tunnel, tibial inlay techniques), the bundles addressed (single-bundle or double-bundle), and the type of graft used.6 However, the situation is even more complicated in case of rare condition, which is a PCL tibial avulsion fracture. It is proven that the proper approach should involve an anatomical reinsertion with internal fixation of the avulsed fragment.7, 8 Although there are many studies published on techniques and outcomes of the PCL avulsion treatment options, no optimal surgical technique has been established. In this paper and video, we present our minimally invasive approach to PCL tibial avulsion treatment. We propose an all-arthroscopic technique of PCL distal reattachment with extracortical fixation, which allows for precise reduction, firm stabilization, and early rehabilitation.
Surgical Technique
Indications
This technique is indicated for symptomatic PCL tibial avulsion.
Contraindications
Mid-substance PCL tears, knee flexion less than 90°, and changes in popliteal neurovascular bundle anatomy (aneurysm, varicose) contraindicate this technique.
Diagnostic Arthroscopy
The patient is positioned supine on the operating table. The procedure can be performed with the patient under either general or spinal anesthesia. A nonsterile tourniquet is placed high on the thigh and inflated to 350 mm Hg. The operated leg is placed in a leg holder and then prepared and draped in a sterile fashion for routine knee arthroscopy.
Typical anterolateral and anteromedial portals are used to inspect the knee joint. With a 30° arthroscope (Arthrex, Naples, FL) inserted through the anterolateral portal and the arthroscopic hook probe introduced through the anteromedial portal, the posterior horn of the lateral meniscus, the ACL, the posterior horn of the medial meniscus, and cartilage are inspected (Video 1). Then, the PCL is assessed (Fig 1, Video 1). When the diagnosis of a PCL tibial attachment avulsion is confirmed, a blunt trocar (Video 1) or bone chisel is introduced through the anteromedial portal and used to assess the possibility of anatomic reposition (Fig 2, Video 1). During this maneuver, the instrument is simultaneously used to determine the exact point for introducing the pin guide with the most advantageous distribution of forces and the best fragment reduction (Video 1). If the avulsed fragment is displaced and difficult to reposition, one should proceed to the next step of this technique instead of trying do it forcefully, which creates the risk of bone fragment damage.
Fig 1.
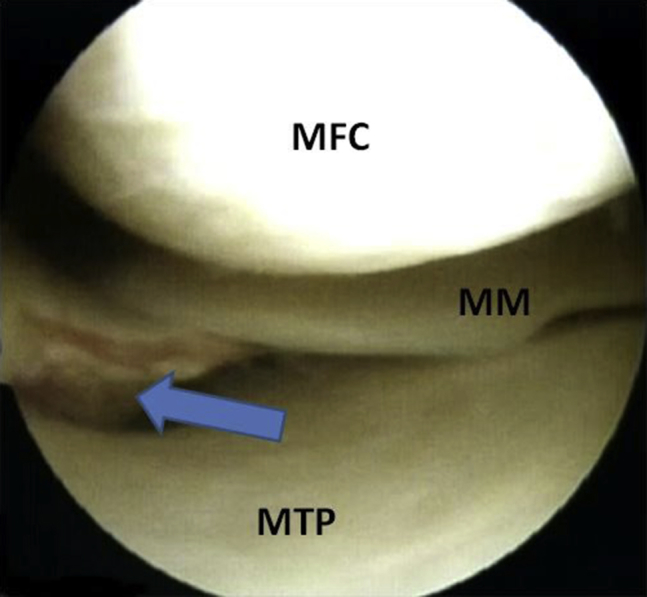
Arthroscopic view from anterolateral viewing portal in a right knee. Posterior cruciate ligament tibial avulsion fracture (blue arrow). (MFC, medial femoral condyle; MTP, medial tibial plateau, MM, medial meniscus.)
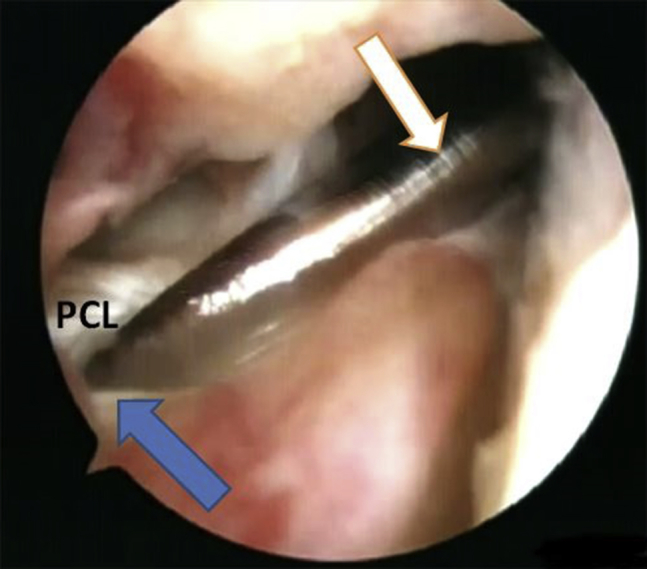
Fig 2.
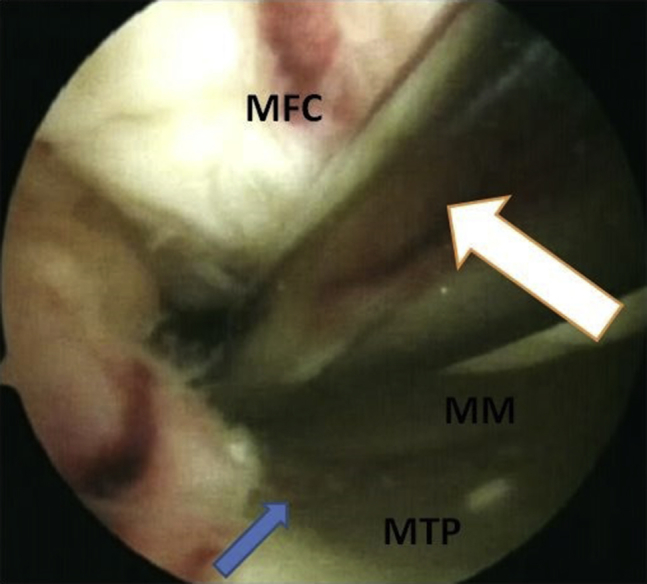
Arthroscopic view from anterolateral viewing portal in a right knee. A blunt trocar (white arrow) is used to assess for the potential of the PCL avulsion fracture reposition. The blue arrow presents avulsed fragment reduction. (MFC, medial femoral condyle; MTP, medial tibial plateau; MM, medial meniscus.)
All-Arthroscopic PCL Distal Reattachment With Extracortical Fixation
The arthroscope is introduced to the posteromedial compartment using a transnotch maneuver (Video 1). An additional high posteromedial portal is created in the soft spot about 2 cm above the posteromedial fold using a surgical no. 11 blade (Fig 3, Video 1). This is very important phase of this technique, because the position of the high posteromedial portal will determine the angle of attack at the avulsed fragment. The high posteromedial portal should be placed in the position that allows for freely introducing the pin guide in previously determined point and to drill the tibial tunnel from this point toward an anterolateral tibial cortex. The arthroscopic cannula (ConMed, Largo, FL) is inserted through the high posteromedial portal to maintain the approach and facilitate maneuvering (Fig 4, Video 1).
Fig 3.
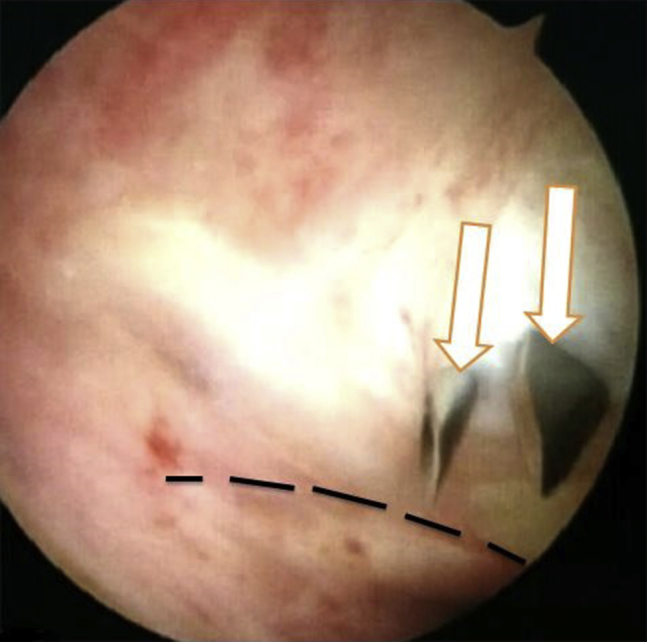
Arthroscopic view from anterolateral viewing portal in a right knee, trans- notch maneuver. An additional high posteromedial portal is placed 2 cm above the posteromedial synovial fold (dashed line) using a needle and surgical blade (white arrows).
Fig 4.
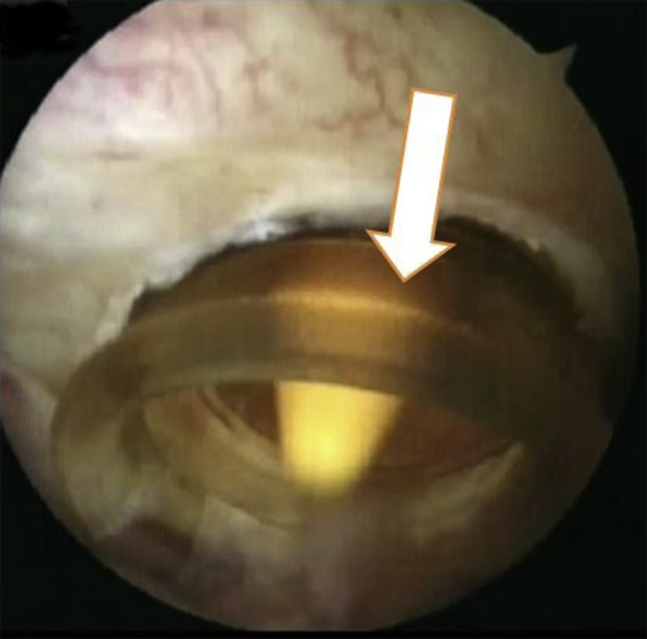
Arthroscopic view from anterolateral viewing portal in a right knee, transnotch maneuver. Arthroscopic canula (white arrow) is placed in the high posteromedial portal to facilitate maneuvering inside the joint.
When the avulsed fragment is displaced, the reduction can be performed at this moment. To do it, the K-wire is introduced under arthroscopic visualization through the cannula, placed in the center of the avulsed fragment, used as a “joystick” to position the fragment in a right place in the tibial plateau, and advanced as a temporary fixation. If the avulsed fragment is not displaced, under arthroscopic visualization, a 2.7-mm eyelet pin (PCL Position System; Aesculap, Tuttlingen, Germany) is introduced through the cannula, placed in the previously determined point in the avulsed PCL tibial attachment, and used to drill a tibial tunnel aimed toward the anterolateral tibial cortex (Fig 5, Video 1). Next, the eyelet pin (Aesculap) is used to pass a FiberTape (Arthrex GmBH, Munich, Germany) suspended on 4 × 12-mm Surgical Plate (PCL Position System; Aesculap) through the tibial tunnel until the plate reduces the avulsed fragment of the PCL tibial attachment (Fig 6, Video 1). The whole suspensory mechanism is fixed on the anterolateral tibial cortex with a 11-mm Suture Disc (PCL Position System; Aesculap). The tension is regulated under visual control using a Twister (PCL Position System; Aesculap) until the fracture reduction is complete. The stability of fixation is evaluated during full knee range of motion under arthroscopic visualization.
Fig 5.
Arthroscopic view from anterolateral viewing portal in the knee. An eyelet pin (white arrow) is placed in the native posterior cruciate ligament (PCL) tibial attachment (blue arrow) and used to drill the tibial tunnel running from the posteromedial to anterolateral part of the tibia.
Fig 6.

Arthroscopic view from anterolateral viewing portal in a right knee. The FiberTape (white arrow, A) suspended on the Surgical Plate (yellow arrow, B) is introduced through the previously prepared tibial tunnel for final reposition of the posterior cruciate ligament tibial avulsion fracture (blue arrow, C). (MFC, medial femoral condyle; MTP, medial tibial plateau; MM, medial meniscus.)
Rehabilitation
Walking on crutches for 6 weeks and an orthosis with limited extension (30°) and flexion (90°) is recommended for patients. Physiotherapy starts from the second postoperative day. If available, the patient can be placed into a dynamic PCL brace.
Discussion
PCL avulsion fractures are rare injuries that can lead to significant morbidity when not recognized and treated properly. Although traditionally treated with open reduction and internal fixation, more recent studies report successful outcomes with both open and arthroscopic-assisted treatment.8 The presented technique, as an arthroscopic procedure, uses the advantages of a minimally invasive approach. It requires only four 0.5- to 1-cm skin incisions—anterolateral, anteromedial, high posteromedial portals, and a small skin incision for fixation of the Suture Disc on the anterolateral tibial cortex. It diminishes the risk of infection, improper wound healing, and patient dissatisfaction according to esthetic considerations in comparison with open procedures.9, 10 It also allows for introducing early rehabilitation. Moreover, an open approach to PCL region is very complicated, carries a risk of neurovascular injury, and may provide poorer visualization than arthroscopy.11 By contrast, direct arthroscopic visualization facilitates an anatomical reposition, which is a key factor for restoring proper knee biomechanics.
Furthermore, all-arthroscopic PCL tibial reattachment with extracortical fixation, in hands of surgeons experienced in posteromedial portal formations, can be a very quick procedure, which reduces the risks associated with prolonged thigh tourniquet maintenance and postoperative pain.12, 13, 14, 15 The presented technique allows one also to treat concomitant intraarticular lesions during one-stage procedure. Approximately 60% of PCL injuries are associated with tears of the posterolateral corner structures, including the lateral collateral ligament, popliteofibular ligament, and popliteus tendon.8 When multiligament reconstructions are necessary, the position of the tibial tunnel from the native PCL tibial attachment to anterolateral tibial cortex should allow one to avoid tunnel convergence. However, it is worth noting that this position creates greater risk in comparison with the anteromedial position.
Finally, all-arthroscopic PCL tibial attachment stabilization with extracortical fixation is beneficial from an economic point of view. It requires a decreased length of hospital stay and minimal hardware placement. Typical systems for PCL (or ACL) reconstructions are sufficient.
However, there are also some potential disadvantages of an all-arthroscopic PCL tibial attachment avulsion fracture stabilization with extracortical fixation. Making a high posteromedial portal places the saphenous nerve at risk. To avoid its injury, the portal should be created with the knee in 90 to 100° of flexion. This position also diminishes the risk of popliteal neurovascular bundle injury during PCL tibial tunnel drilling, pushing the structures about 2.5 cm away the posterior tibial margin.16, 17 Thus, the procedure should not be performed in patients with knee flexion less than 90°. Moreover, because of hardware placement, there is always a minor risk of soft-tissue irritation, which may be a mild foreign body reaction. Some patients are likely to develop postoperative knee pain or discomfort around the tibial implant.14, 18 Therefore, sometimes the hardware removal is required.
Another situation that can complicate the procedure is significant avulsed fragment displacement or fragmentation. When the fragment is significantly displaced, a K-wire introduced through the high posteromedial portal can be used for reposition and temporary fixation, as described previously. In case of significant fragmentation, our method of choice is to use a Spectrum Suture Passer (ConMed) to pass the FiberTape (Arthrex) through the PCL substance applying a “lasso-loop” technique and introducing it to the tibial tunnel running from native PCL tibial attachment to anterolateral tibial cortex. The whole construct is fixed on the anterolateral tibial cortex with a 11-mm Suture Disc (PCL Position System; Aesculap).
To summarize, the presented PCL fracture avulsion technique is simple, reproducible and allows for restoring the knee anatomy and biomechanics. All advantages and disadvantages of all-arthroscopic PCL tibial attachment stabilization summarizes Table 1.
Table 1.
Advantages and Disadvantages of All-Arthroscopic PCL Tibial Reattachment With Extracortical Fixation
| Advantages | Disadvantages |
|---|---|
| • Minimally invasive procedure | • Challenging and demanding technique for beginning arthroscopists. |
| • Early rehabilitation possible | • High risk of neurovascular injury. |
| • Limited soft-tissue trauma | • At least 90° of flexion necessary. |
| • Diminished scar formation | • Possible irritation to hardware. |
| • Anatomical and biomechanical restoration of the knee function | • May not be possible if meniscal roots are avulsed with the fracture fragment. |
| • Quick procedure | |
| • Minimum morbidity | |
| • Concomitant intraarticular lesions can be treated in a one- stage procedure | |
| • Short hospital stay | |
| • Small amount of hardware placement |
Footnotes
The authors report the following potential conflict of interest or source of funding: R.F.L. is a consultant and receives royalties Arthrex, Ossur, and Smith and Nephew and is on the editorial boards of American Journal of Sports Medicine, Journal of Experimental Orthopaedics, and Knee Surgery, Sports Traumatology, Arthroscopy. K.M. is a consultant for Zimmer Biomet and is on the editorial board of PTArtro. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
All-arthroscopic posterior cruciate ligament distal reattachment with extracortical fixation in the right knee. Before surgery, a thorough clinical and radiologic examination should be performed. The surgery starts from inspection of concomitant intra-articular lesions: LM, ACL, MM, and cartilage are assessed. We can see the PCL tibial avulsion in the intercondylar eminence. A blunt trocar introduced through the anteromedial portal is used to check the potential of the avulsion fracture reposition. Then, the transnotch maneuver is performed and the arthroscope is inserted into the posteromedial compartment. An additional high posteromedial portal is created 2 cm above the posteromedial synovial fold. An arthroscopic cannula is placed in posteromedial portal to facilitate maneuvering. An eyelet pin is placed in the center of the avulsed fracture fragment and used to drill the tibial tunnel directed anterolaterally. Then, the same eyelet pin is used to introduce the FiberTape suspended on a Surgical Plate through the tibial tunnel. To complete the surgical fixation, an extracortical fixation is performed on the anterolateral tibial cortex with Surgical Disc and Twister. (LM, lateral meniscus; ACL, anterior cruciate ligament; PCL, posterior cruciate ligament; MM, medial meniscus.)
References
- 1.Rezazadeh S., Solooki S., Aboulhasani S. Midterm results of open reduction and internal fixation of isolated posterior cruciate ligament avulsion fracture. Eur Orthop Traumatol. 2011;1:191. [Google Scholar]
- 2.Khatri K., Sharma V., Lakhotia D., Bhalla R., Farooque K. Posterior cruciate ligament tibial avulsion treated with open reduction and internal fixation through the Burks and Schaffer approach. Malays Orthop J. 2015;9:2–8. doi: 10.5704/MOJ.1507.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kennedy N.I., Wijdicks C.A., Goldsmith M.T. Kinematic analysis of the posterior cruciate ligament, part 1: The individual and collective function of the anterolateral and posteromedial bundles. Am J Sports Med. 2013;41:2828–2838. doi: 10.1177/0363546513504287. [DOI] [PubMed] [Google Scholar]
- 4.Ahn J.H., Yang H.S., Jeong W.K., Koh K.H. Arthroscopic transtibial posterior cruciate ligament reconstruction with preservation of posterior cruciate ligament fibers: clinical results of minimum 2-year follow-up. Am J Sports Med. 2006;34:194–204. doi: 10.1177/0363546505279915. [DOI] [PubMed] [Google Scholar]
- 5.LaPrade R.F., Heikes C., Bakker A.J., Jakobsen R.B. The reproducibility andrepeatability of varus stress radiographs in the assessment of isolated fibular collateral ligament and grade-III posterolateral knee injuries. An in vitro biomechanical study. J Bone Joint Surg Am. 2008;90:2069–2076. doi: 10.2106/JBJS.G.00979. [DOI] [PubMed] [Google Scholar]
- 6.Ward B.D., Lubowitz J.H. Basic knee arthroscopy part 2: Surface anatomy and portal placement. Arthrosc Tech. 2013;2:e501–e502. doi: 10.1016/j.eats.2013.07.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Natarajan S., Anbarasi C., Meena R. Treatment of acute avulsion of posterior cruciate ligament of left knee with bony fragment by Siddha Varmam therapy and traditional bone setting method: A case report. J Ayurveda Integr Med. 2019;10:135–138. doi: 10.1016/j.jaim.2018.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Petrillo S., Volpi P., Papalia R., Maffulli N., Denaro V. Management of combined injuries of the posterior cruciate ligament and posterolateral corner of the knee: A systematic review. Br Med Bull. 2017;123:47–57. doi: 10.1093/bmb/ldx014. [DOI] [PubMed] [Google Scholar]
- 9.Bhattacharyya M., Bradley H. Intraoperative handling and wound healing of arthroscopic portal wounds: A clinical study comparing nylon suture with wound closure strips. J Perioper Pract. 2008;18:194–196, 198. doi: 10.1177/175045890801800502. [DOI] [PubMed] [Google Scholar]
- 10.Badran M.A., Elgeidi A.E., Elganiny A., Sallab R.M.E. Posterior cruciate ligament tibial avulsion fracture: A novel arthroscopic fixation technique versus open posteromedial fixation. Orthop Spine Sports Med. 2017;1:002. [Google Scholar]
- 11.Montgomery S.R., Johnson J.S., McAllister D.R., Petrigliano F.A. Surgical management of PCL injuries: Indications, techniques, and outcomes. Curr Rev Musculoskelet Med. 2013;6:115–123. doi: 10.1007/s12178-013-9162-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Konrad G., Markmiller M., Lenich A., Mayr E., Rüter A. Tourniquets may increase postoperative swelling and pain after internal fixation of ankle fractures. Clin Orthop Relat Res. 2005;433:189–194. doi: 10.1097/01.blo.0000151849.37260.0a. [DOI] [PubMed] [Google Scholar]
- 13.Johnson D.S., Stewart H., Hirst P., Harper N.J. Is tourniquet use necessary for knee arthroscopy? Arthroscopy. 2000;16:648–651. doi: 10.1053/jars.2000.4826. [DOI] [PubMed] [Google Scholar]
- 14.Drosos G.I., Stavropoulos N.I., Katsis A., Kesidis K., Kazakos K., Verettas D.A. Post-operative pain after knee arthroscopy and related factors. Open Orthop J. 2008;2:110–114. doi: 10.2174/1874325000802010110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kirkley A., Rampersaud R., Griffin S., Amendola A., Litchfield R., Fowler P. Tourniquet versus no tourniquet use in routine knee arthroscopy: A prospective, double-blind, randomized clinical trial. Arthroscopy. 2000;16:121–126. doi: 10.1016/s0749-8063(00)90024-0. [DOI] [PubMed] [Google Scholar]
- 16.Ahn J.H., Chung Y.S., Oh I. Arthroscopic posterior cruciate ligament reconstruction using the posterior trans-septal portal. Arthroscopy. 2003;19:101–107. doi: 10.1053/jars.2003.50017. [DOI] [PubMed] [Google Scholar]
- 17.Louisia S., Charrois O., Beaufils P. Posterior "back and forth" approach in arthroscopic surgery on the posterior knee compartments. Arthroscopy. 2003;19:321–325. doi: 10.1053/jars.2003.50082. [DOI] [PubMed] [Google Scholar]
- 18.Rosseland L.A., Helgesen K.G., Breivik H., Stubhaug A. Moderate-to-severe pain after knee arthroscopy is relieved by intraarticular saline: A randomized controlled trial. Anesth Analg. 2004;98:1546–1551. doi: 10.1213/01.ANE.0000112433.71197.FA. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
All-arthroscopic posterior cruciate ligament distal reattachment with extracortical fixation in the right knee. Before surgery, a thorough clinical and radiologic examination should be performed. The surgery starts from inspection of concomitant intra-articular lesions: LM, ACL, MM, and cartilage are assessed. We can see the PCL tibial avulsion in the intercondylar eminence. A blunt trocar introduced through the anteromedial portal is used to check the potential of the avulsion fracture reposition. Then, the transnotch maneuver is performed and the arthroscope is inserted into the posteromedial compartment. An additional high posteromedial portal is created 2 cm above the posteromedial synovial fold. An arthroscopic cannula is placed in posteromedial portal to facilitate maneuvering. An eyelet pin is placed in the center of the avulsed fracture fragment and used to drill the tibial tunnel directed anterolaterally. Then, the same eyelet pin is used to introduce the FiberTape suspended on a Surgical Plate through the tibial tunnel. To complete the surgical fixation, an extracortical fixation is performed on the anterolateral tibial cortex with Surgical Disc and Twister. (LM, lateral meniscus; ACL, anterior cruciate ligament; PCL, posterior cruciate ligament; MM, medial meniscus.)