

Abstract
Introduction:
Eating disorders have frequently been reported among young adults including university students. Detailed information on the prevalence and associated gender-specific determinants of eating disorders are lacking, particularly among students in the north western region of Pakistan. The current cross-sectional study was designed to fill this gap in the literature.
Methods:
Total of 672 students (female: 56%, age range: 18–26 years) were enrolled and data collected between October 2016 and December 2017. The 26 items Eating Attitude Test (EAT-26), Diet quality Index-International (DQI-I), 10 items Rosenberg’s self-esteem scale (SES), Stunkard Figure Rating Scale, 19-items Pittsburgh Sleep Quality Index (PSQI) and Global Physical Activity Questionnaire (GPAQ) were used. Body composition and anthropometry were determined using standardized tools. A cut-off of ≥20 EAT-26 score was used to assess the tendency towards eating disorders (EDT). Data was analyzed using appropriate statistical tests.
Results:
Mean (SD) age of the respondents was 21.7±2 years. Total of 103 (15.3%) students showed EDT with no statistical difference between sexes. Students with EDT had a much lower diet quality than normal students (p<0.001). Risk factors for EDT, in female students included young age (<20 years), on-campus residency, discordant body image and poor sleep quality, while those for males were vigorous lifestyle, insufficient monthly allowance, poor sleep quality and peer pressure.
Conclusions:
A significant number of students showed a tendency towards an unhealthy eating attitude with some sex-specific risk factors. These students had poorer diet quality than normal students. Support to encourage healthy attitudes to eating and better diet quality could help to avert the development of clinical eating disorders.
Keywords: Eating disorders, sex-specific risk factors, university students
INTRODUCTION
Eating disorders (ED), being characterized by a disturbed attitude to eating can develop into a major health problem for some adolescents and young adults. A growing body of evidence suggests that the prevalence of eating disturbance and excessive concerns regarding body weight are increasing among young populations including college and university students. Eating disorders were more common in advanced countries, but in recent years the burden of these disorders has been extended to the developing world as well. Diverse prevalence rates for a tendency towards ED have been reported in non-clinical populations ranging from 4 to 38% among youngsters in South Asian countries including India, Pakistan and Bangladesh (1–4). In extreme cases ED leads to serious mental, physical, physiological and psychosocial illnesses such as anorexia nervosa and anorexia bulimia (5).
Emerging adulthood, starting from late adolescence, is the distinct period between 18 and 25 years of age where adolescents become more independent and may adopt health behavior patterns on their own. This time period is thus irreducible because early adulthood is often associated with poor dietary habits (6). Previous research has identified a wide range of risk factors for ED among college and university students in different cultures and countries. The major factors identified for risk of ED in university populations included age, sex, cultural transition and globalization, urbanization, media-induced westernization, and psychological factors such as perceived stress and body shape concern (7, 8).
Studies on ED and associated risk factor among college and university students are scarce in Pakistan. The available literature on this topic focused on young adults from South and East Pakistan (3, 4). Pakistan is a country with wide cultural and ethnic variations. Information on ED and associated risk factors are not available in university students from the north western region. The aim of the current study is to explore the prevalence of the tendency towards ED (EDT) and associated risk factors among a university population in Peshawar-north western Pakistan.
METHODS
Setting and Participants
A cross-sectional survey was organized by the Department of Human Nutrition, the University of Agriculture, Peshawar-Pakistan. Graduates of the department were trained to collect relevant data from university students (n=672, age range: 18–26 year) between October 2016 and December 2017. Selection criteria included students currently enrolled in the university and free from any chronic disorders. Informed consents were obtained from all subjects prior to data collection. The study was ethically approved by the Ethics Committee of the Faculty of Nutrition Sciences, the University of Agriculture, Peshawar-Pakistan.
Data Collection
Eating attitude test and diet quality assessment
Eating attitudes of the students were evaluated using the Eating Attitude Test (EAT-26). The EAT-26 is composed of 26 items, arranged in a 4-point Likert scale. The responses on the 26 items are summed at the end and a total score, ranging from 0 to 78 is extracted. The respondents, who score ≥20, belong to the group of people who have a tendency to develop ED (EDT) (9). Previous literature has shown EAT-26 as an efficient screening instrument for the detection of a tendency towards ED among young adults in non-clinical populations (10).
Diet Quality Index-International (DQI-I) was used to evaluate diet quality of the respondents (11). DQI-I examines four components of diet quality: variety (overall variety in food groups and within-group variety for protein source), adequacy (cereals or grain group, fruits and vegetables groups, fiber, protein, iron, calcium, and vitamin C), moderation (total fat, saturated fat, cholesterol, sodium, and empty calorie foods), and balance (macronutrient ratio). Scores for each component were summarized in each of the 4 main categories and the scores for all 4 categories were summed, resulting in the total DQI-I score, ranging from 0 to 100 (0 being the lowest and 100 the highest level of diet quality).
Nutritional status assessment
Current nutritional status of the subjects was assessed by taking measurements on body weight, percent body fat (PBF) & height using standardized procedures. Height measurements were taken using a non-stretchable measuring tape to the nearest 0.1 cm. Subjects weight and PBF were measured in duplicate using a Tanita SC-331S body composition analyzer (Tanita, Tokyo, Japan). Body mass indexes (BMI) of the students were calculated as weight (kg)/height (m2). Information on other relevant parameters such as peer pressure to lose weight, and dieting in the family and/or friends were also obtained and recorded on a proforma.
Self-esteem assessment and body image perception
Rosenberg’s self-esteem scale, a 10-Item scale (SES) was applied to assess the level of self-esteem of the respondents. A total score of 0–30 was used for 10 items that were scored between 0 and 3. Respondents with a score of 15 or less were considered as low self-esteem, while those that scored more than 15 were considered as normal (12).
Participants’ body image perception was assessed by Stunkard Figure Rating Scale (13). The scale is composed of gender-specific body silhouettes ranging from 1 (extremely thin/very underweight) to 9 (very overweight/heavy). Participants were asked to rate how they perceived their current body shape by choosing an image that corresponded to theirfigure on the scale. To determine the discrepancy between body image perception and actual BMI, both indicators were standardized to z-scores. Body image discrepancy (BID) score was calculated by subtracting the standardized BMI value from the standardized body image perception value. The subjects were classified as satisfied when the BID values were zero while subjects with positive or negative BID values were considered as dissatisfied with their actual body size.
Socioeconomic status, sleep quality and life style of the respondents
Socioeconomic status of the respondents including information on their family characteristics and monthly living allowances were obtained using structured questionnaires. Subjects’ sleep quality was assessed using The Pittsburgh Sleep Quality Index (PSQI); a 19-item, self-reported questionnaire that explores subjective sleep quality over the past month (14). The PSQI contains 7 component scores indicating subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications and daytime dysfunction. These may be coalesced into 1 global score, with higher scores indicating poorer sleep quality. A global PSQI score >5 is considered to be a sensitive and specific measure of poor sleep quality.
Questions pertaining to levels of physical activity were based on “The Global Physical Activity Questionnaire” (GPAQ), developed by WHO (15). Total metabolic equivalents (METs) were calculated to express the intensity of the physical activity. METs were used to classify persons according to level of intensity, i. e. low (<600 METs), moderate (600–1.499 METs), and high (>1.500 METs).
Statistical Analysis
All data were entered into the computer using Statistical Package for Social science (SPSS, version 12.01, Chicago, IL, 2004) for statistical analysis. Appropriate statistical tests such as Chi-square for categorical or qualitative variables and Students’ t-test or Mann-Whitney U test for continuous variables were used to compare different outcomes between EAT groups; normal and eating disorder tendency (EDT) (based on an EAT-26 cut-off value of ≥20). Differences in characteristics between the groups with p-values ranging between 0.05–0.06 were considered marginally significant. Correlates of EDT among the students were identified using multiple logistic regression models. Regression analyses were performed separately for male and female students to identify the sex-specific risk factors associated with EDT. First the univariate analyses were performed to extract the contributing factors EDT. Factors potentially associated with the outcome (EDT) on univariate analysis (with p-values <0.1) were inserted in the multivariate logistic regression model to obtain adjusted odds ratios.
RESULTS
A total of 672 (56% female, 44% male) students participated in the study. Table 1 shows results of socio-demographic, lifestyle and nutritional characteristics by EAT group. Students were within the age range of 18 to 26 year, with mean age of 21.7±2 year. The majority of the students were in the range of 20–24 years (n=455, 68%). EAT scores ranged from 0 to 63 and 15.3% (n=103) of students had a score of ≥20 and were defined as EDT. Students with EDT were on average younger and had significantly lower DQI-I scores than the normal group (p<0.001). Compared to normal, significantly higher numbers of students with EDT had on-campus residency, poor self-esteem and poor sleep quality, higher peer pressure to lose weight and a less sedentary lifestyle (p<0.05). Furthermore, EDT students were marginally more likely to be female, have mothers with some school education, have a lower monthly allowance, a higher BMI, and a dissatisfied body image perception (p<0.06).
Table 1.
Socio-demographic, lifestyle and nutritional characteristics for the whole cohort and by EAT groups (Normal verses EDT)
| Characteristics | Cohort (n=672) | Normal (n=569) | EDT (n=103)* | p-values | |
|---|---|---|---|---|---|
| Mean ± SD/No. (%) | |||||
| EAT-Score | 12.9±6.3 | 10.8±4.2 | 24.6±2.1 | <0.001 | |
| Age (year) | 21.7±2 (Range: 18–26) | 21.9±2.0 | 21.0±1.3 | <0.001 | |
| Age groups | <20 | 129 (19%) | 99 (18%) | 30 (29%) | <0.01 |
| 20–24 | 455 (68%) | 388 (68%) | 67 (65%) | ||
| >24 | 88 (13%) | 82 (14%) | 6 (6%) | ||
| Sex | Female | 376 (56%) | 309 (54%) | 67 (65%) | 0.056 |
| Male | 296 (44%) | 260 (46%) | 36 (35%) | ||
| Marital Status, Single† | 607 (90%) | 511 (89.9%) | 96 (93%) | >0.05 | |
| Mothers’ education, No schooler at all‡ | 374 (55%) | 326 (57%) | 48 (47%) | 0.057 | |
| Fathers’ education, No schooler at all‡ | 117 (17%) | 104 (18%) | 13 (12%) | >0.05 | |
| Residency, On-Campus | 442 (66%) | 365 (64%) | 77 (75%) | <0.05 | |
| Smoking, Yes | 96 (14%) | 75 (13%) | 21 (20%) | >0.05 | |
| Monthly Allowance (PKR)** | 9.37±2.75 | 9.44±2.81 | 8.94±2.33 | 0.054 | |
| Self-esteem, poor | 125 (19%) | 98 (17%) | 27 (26%) | <0.05 | |
| BMI | 22.1±2.8 | 21.9±2.8 | 22.5±3.0 | 0.054 | |
| % body fat | 21.3±6.8 | 20.8±6.8 | 22.4±6.9 | 0.083 | |
| DQI-I Score | 60±4.2 | 66±4.8 | 53±3.6 | <0.001 | |
| Body image perception, dissatisfied | 150 (22%) | 119 (21%) | 31 (30%) | 0.053 | |
| Sleeping quality, poor | 142 (21%) | 108 (19%) | 34 (33%) | <0.05 | |
| Peer Pressure to lose weight, yes | 101 (15%) | 77 (13.5%) | 24 (23%) | <0.05 | |
| PAL | Sedentary | 275 (41%) | 245 (43%) | 30 (29%) | 0.05 |
| Moderate | 213 (32%) | 176 (31%) | 37 (36%) | ||
| Vigorous | 184 (27%) | 148 (26%) | 36 (35%) | ||
| Dieting in relatives/friends, Yes | 72 (11%) | 55 (10%) | 17 (16%) | >0.05 | |
SD, standard deviation.
Disordered: EAT-Score >20; Normal: EAT-Score ≤20
single (i.e., unmarried or not engaged)
respondents’ parents with no formal education
PKR. Pakistani Rupees (1 US$=PKR: 105 at time of data collection)-results shown in PKR (in thousands).
In Fig. 1 nutritional characteristics by EAT groups were compared separately in male and female students. Results on BMI indicate that female EDT students had on average higher BMI compared to the normal females (p<0.05), however no significant difference in mean BMI was evident between the male EAT groups. No significant differences were found in mean PBF between EAT groups in either males or females (p>0.05). Both male and female EDT students had significantly lower mean DQI scores than their normal counterparts (p<0.001). Scores were 19.0% lower in male and 19.6% lower in female EDT students compared to normal students indicating substantial differences in diet quality between the groups.
Figure 1.
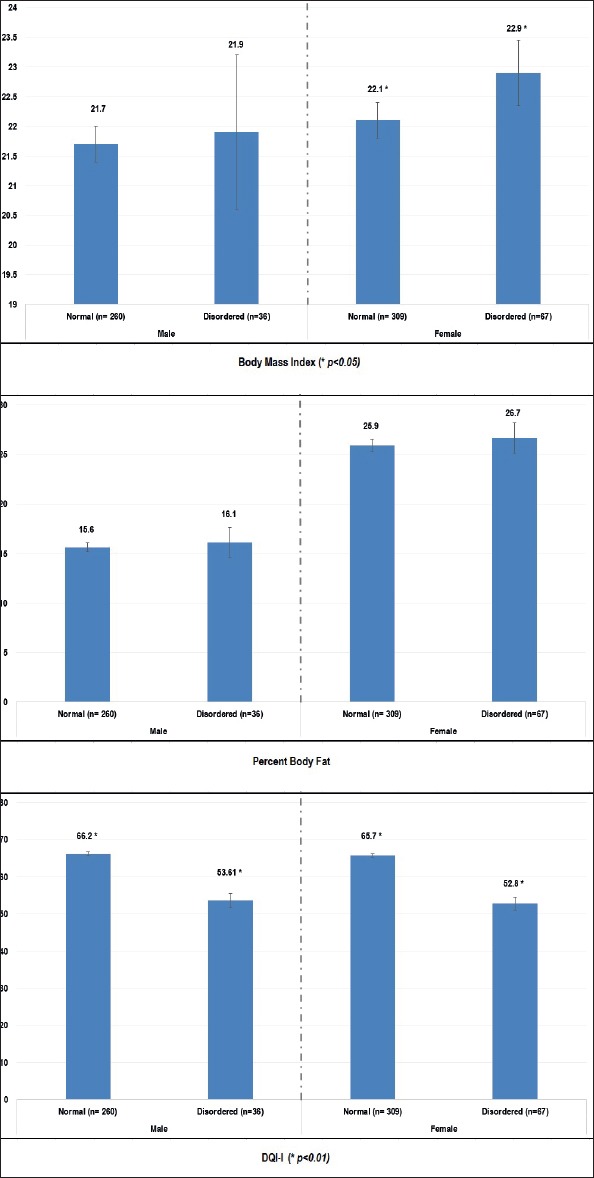
Comparison of nutritional characteristics by EAT groups in male and female subjects.
Multivariate logistic regression analysis results are presented for socio-demographic, nutritional and behavioural characteristics separately for female and male students (Fig. 2 and 3 respectively). Four variables were independently related to EDT in female students: young age (<20 years compared to >24 years), on-campus residency, body image discordance and poor sleep quality. Independent correlates of EDT among male students were strenuous lifestyle, insufficient monthly allowance, poor sleep quality, and peer pressure to lose weight.
Figure 2.
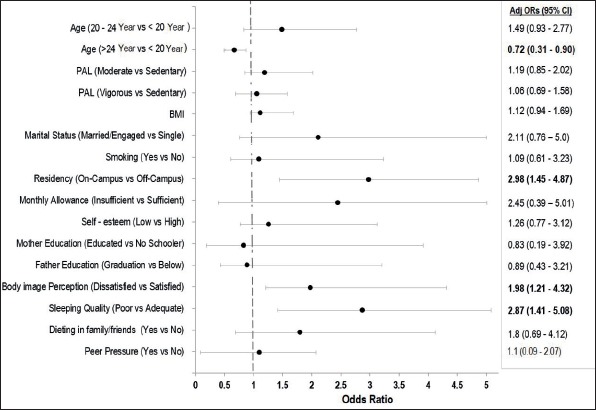
Correlates of disordered eating attitude in Female students.
Figure 3.
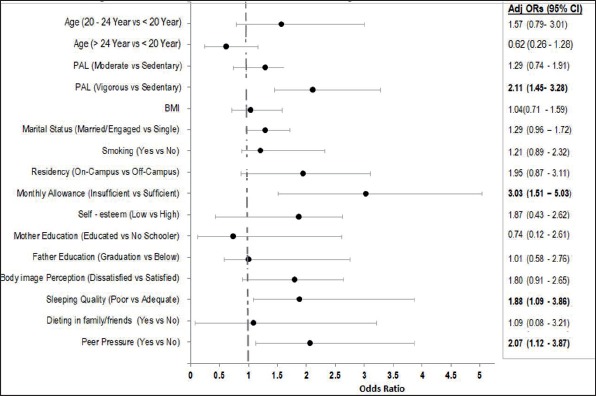
Correlates of disordered eating attitude in Male students.
DISCUSSION
The current cross-sectional study was conducted with the primary goal of examining the overall prevalence of ED risk and associated correlates in a cohort of university students in Northern Pakistan. The tendency towards ED in this cohort was 15.3% with only a marginal excess of females in this group. The strongest association with EDT was a low score on an eating quality index, around 19% lower, on average, in both males and females than in their normal counterparts. This suggests that EDT students were eating differently from normal students. Associations between EDT and a range of correlates, examined using multivariable logistic regression, showed some differences between males and females but in both sexes students with EDT were more likely to have poor sleep quality.
The EAT-26 questionnaire was used to assess the tendency towards unhealthy eating attitudes associated with eating disorders which can in extreme forms, such as clinically diagnosed anorexia nervosa or bulimia, can be very damaging to health and well-being. The EAT-26 is not a diagnostic tool in a non-clinical population but does identify a tendency towards disordered eating (EDT). Other studies have used the same assessment tool with mixed findings on the prevalence of ED in college/university graduates from different parts of Pakistan. A study conducted in Karachi, located in southern Pakistan, reported ED in 22.7% university students; and females were more likely to show tendency towards ED than males (4). Other studies have also demonstrated higher levels of poor eating attitudes in female students compared to their male counterparts (16). It has been suggested that compared to males, females are more likely to diet to control their weight, are more likely to have low self-esteem, which may increase their odds of developing disordered eating (7, 10, 16).
Overall students at risk of ED were younger, with poor self-esteem, and had lower DQI scores compared to normal students. The mean BMI of the ED group was marginally higher and they were more likely to have dissatisfied body image compared to normal students. This study has a unique feature of exploring a broad range of gender-specific ‘adjusted determinants’ of ED. Similarly mean differences in nutritional characteristics including BMI, PBF and DQI-I were examined by eating attitude and gender groups. Risk factors of ED, being identified for female EAT group included young age (<20 years compared to 24 years), on-campus residency, dissatisfied body image and poor sleeping quality, while those observed for male groups were vigorous lifestyle, insufficient monthly allowance, poor sleeping quality and peer pressure to lose weight. Our findings are in agreement with a wide body of evidence in the literature on eating attitude and associated risk factors as well as complications in adolescents and young adults, reporting more or less similar findings.
Age is one of the predominant factors; eating disorders are common in males and females of all ages. However, young adults have been reported in most of the studies to be at risk of eating disorders (17). In the current study, age was a significant predictor of ED in female students only; young girls were comparatively more at risk compared to their senior counterparts. These findings are in fair agreement with previous reported data which shows that the frequency of risky food behavior to ED is higher in young girls (18). A significant positive association was evident between poor sleep quality and ED among male and female students. Reduced sleep efficiency, and increased intermittent wake time and shallow sleep duration in patients of ED were observed in previous literature (19). No differences in means BMI were found across male EAT groups; however female students with higher BMI tended to have more eating problems than normal girls. A higher BMI have been reported as a significant predictor of greater body dissatisfaction, more so for female than male subjects (20). Previous literature has suggested that participants with disturbed eating (identified through EAT-26 scale) tended to have larger body sizes that may lead to body dissatisfaction. Body dissatisfaction is one of the most prominent risk factors in the onset and maintenance of eating pathology, along with dieting and negative affect (21). Both male and female ED groups had significantly lower means DQI-I scores than their respective normal counterparts. In agreement with previous literature, problematic eating style have been associated with intake of unhealthy foods (22). In the current study, body dissatisfaction was an important factor affecting eating disorder tendency among female students only. Disordered eating tended to be more common among the female group that was dissatisfied with their body size. Previous literature supported our findings on association between body dissatisfaction and ED among female gender. Most of the females were reported to be dissatisfied with their body shape compared to male counterparts (23). Body dissatisfaction in female was previously found to be associated with ED and low self-esteem (2, 3, 18).
Insufficient monthly allowance was found a strong predictor of ED in male students only. The monthly allowance of students is affected by the parents’ income. Mixed findings have been reported in previous research regarding the association between income status and ED. Some studies have reported an increased risk of ED in persons with lower household incomes (24) while some studies have shown no association between ED features and income (25). In Pakistan, although only a small proportion of women reach university education, however, because of social and cultural norms, parents facilitate them to maximum level compared to male siblings. Women in Pakistan, especially those from less affluent families, are often unable to demand access to higher education with constraints on mobility and economic activities. These facts may explain gender related differences on association between monthly allowance and ED in current study.
Peer pressure in the current study was a significant predictor of ED among male students only. Our findings are in contrast with most of the previous studies that reported a significant level of association between ED and peer pressure among female students compared to male counterparts (26, 27). Compared to female, male students in the current study area are more likely to be communal and have larger peer groups. Similarly, girls have more reciprocal peers because of the existing culture as well as religious influences. This may explain the association of peer pressure with eating habits of male students. This might put more students on physical exertion as we have shown that male students involved in vigorous physical activity were more at the risk of ED compared to those with sedentary lifestyle (figure-III). Men were more likely to involve in compulsive exercise than women in a study on eating attitudes in young students (28). Similarly, research findings of another study showed that collegiate athletes had higher adherence with eating disturbance including binge eating, use of laxatives, diuretics and self-induced vomiting (29).
Our study has certain strengths and limitations. One limitation of this study was that eating disorders were assessed with self-report questionnaires. The EAT-26 scale, however had previously been used in other parts of Pakistan while investigating eating related pathologies among university students (3, 4). To our knowledge, this is the first study in north western Pakistan, to investigate the prevalence and associated risk factors of ED by including a large sample of university students of both sexes. All of the data were collected by well-trained graduates of the university, using standardized and recommended tools.
CONCLUSIONS
Our findings revealed the existence of unhealthy diet related attitude among university students across both genders. Gender specific risk factors were observed. This is highly recommended to frequently organize early screening and timely treatment programs for university students with eating attitude disorders. Further research is needed to develop gender specific intervention programs to control eating disorders among university students in Pakistan.
Footnotes
Ethics Committee Approval: The study was ethically approved by the Ethics Committee of the Faculty of Nutrition Sciences, the University of Agriculture, Peshawar-Pakistan.
Informed Consent: Informed consents were obtained from all subjects prior to data collection.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - ZD, KI; Design - IK, ZI; Supervision - MA, FG, MI, M.ILYAS, HI; Resource - MA, FG, ZD, KI; Materials - MS, MI, M.ILYAS; Data Collection and/ or Processing - IK, ZI, ZD, MS; Analysis and/or Interpretation - ZD, KI; Literature Search - MA, M.ILYAS; Writing - ZD, KI; Critical Reviews - ZD KI.
Conflict of Interest: Authors declare no conflict of interest in this study.
Financial Disclosure: The authors acknowledge the financial and logistic support of the University of Agriculture-Peshawar, Pakistan.
REFERENCES
- 1.Pengpid S, Peltzer K, Ahsan GU. Risk of eating disorders among university students in Bangladesh. Int J Adolesc Med Health. 2015;27:93–100. doi: 10.1515/ijamh-2014-0013. [DOI] [PubMed] [Google Scholar]
- 2.Makino M, Tsuboi K, Dennerstein L. Prevalence of eating disorders:a comparison of Western and non-Western countries. MedGenMed. 2004;6:49. [PMC free article] [PubMed] [Google Scholar]
- 3.Suhail K, Zaib-u-Nisa Prevalence of eating disorders in Pakistan:relationship with depression and body shape. Eat Weight Disord. 2002;7:131–138. doi: 10.1007/BF03354439. [DOI] [PubMed] [Google Scholar]
- 4.Memon AA, Adil SE, Siddiqui EU, Naeem SS, Ali SA, Mehmood K. Eating disorders in medical students of Karachi, Pakistan-a cross-sectional study. BMC Res Notes. 2012;5:84. doi: 10.1186/1756-0500-5-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Klump KL, Bulik CM, Kaye WH, Treasure J, Tyson E. Academy for eating disorders position paper:eating disorders are serious mental illnesses. Int J Eat Disord. 2009;42:97–103. doi: 10.1002/eat.20589. [DOI] [PubMed] [Google Scholar]
- 6.Nour MM, McGeechan K, Wong AT, Partridge SR, Balestracci K, Roy R, Hebden L, Allman-Farinelli M. Diet quality of young adults enrolling in TXT2BFiT, a mobile phone-based healthy lifestyle intervention. JMIR Res Protoc. 2015;4:e60. doi: 10.2196/resprot.4484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mase T, Miyawaki C, Kouda K, Fujita Y, Ohara K, Nakamura H. Relationship of a desire of thinness and eating behavior among Japanese underweight female students. Eat Weight Disord. 2013;18:125–132. doi: 10.1007/s40519-013-0019-x. [DOI] [PubMed] [Google Scholar]
- 8.Becker AE, Fay KE, Agnew-Blais J, Khan AN, Striegel-Moore RH, Gilman SE. Social network media exposure and adolescent eating pathology in Fiji. Br J Psychiatry. 2011;198:43–50. doi: 10.1192/bjp.bp.110.078675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Garner DM, Garfinkel PE. The Eating Attitudes Test:An index of the symptoms of anorexia nervosa. Psychol Med. 1979;9:273–9. doi: 10.1017/s0033291700030762. [DOI] [PubMed] [Google Scholar]
- 10.Yu J, Lu M, Tian L, Lu W, Meng F, Chen C, Tang T, He L, Yao Y. Prevalence of Disordered Eating Attitudes among University Students in Wuhu, China. Nutr Hosp. 2015;32:1752–1757. doi: 10.3305/nh.2015.32.4.9187. [DOI] [PubMed] [Google Scholar]
- 11.Kim S, Haines PS, Siega-Riz AM, Popkin BM. The Diet Quality Index-International (DQI-I) provides an effective tool for cross-national comparison of diet quality as illustrated by China and the United States. J Nutr. 2003;133:3476–3484. doi: 10.1093/jn/133.11.3476. [DOI] [PubMed] [Google Scholar]
- 12.Rosenberg M. Rosenberg self-esteem scale (RSE) Acceptance and commitment therapy Measures package. 1965;61:52. [Google Scholar]
- 13.Stunkard AJ. Use of the Danish Adoption Resister for the study of obesity and thinness. Res Publ Assoc Res Nerv Ment Dis. 1983;60:115–120. [PubMed] [Google Scholar]
- 14.Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index:a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 15.Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire (GPAQ):nine country reliability and validity study. J Phys Act Health. 2009;6:790–804. doi: 10.1123/jpah.6.6.790. [DOI] [PubMed] [Google Scholar]
- 16.Şanlier N, Yabanci N, Alyakut Ö. An evaluation of eating disorders among a group of Turkish university students. Appetite. 2008;51:641–645. doi: 10.1016/j.appet.2008.05.058. [DOI] [PubMed] [Google Scholar]
- 17.Sanlier N, Navruz Varli S, Macit MS, Mortas H, Tatar T. Evaluation of disordered eating tendencies in young adults. Eat Weight Disord. 2017;22:623–631. doi: 10.1007/s40519-017-0430-9. [DOI] [PubMed] [Google Scholar]
- 18.Costarelli V, Demerzi M, Stamou D. Disordered eating attitudes in relation to body image and emotional intelligence in young women. J Hum Nutr Diet. 2009;22:239–245. doi: 10.1111/j.1365-277X.2009.00949.x. [DOI] [PubMed] [Google Scholar]
- 19.Allison KC, Spaeth A, Hopkins CM. Sleep and Eating Disorders. Curr Psychiatry Rep. 2016;18:92. doi: 10.1007/s11920-016-0728-8. [DOI] [PubMed] [Google Scholar]
- 20.Cash TF, Henry PE. Women's body images:The results of a national survey in the USA. Sex Roles. 1995;33:19–28. [Google Scholar]
- 21.Stice E, Shaw HE. Role of body dissatisfaction in the onset and maintenance of eating pathology:A synthesis of research findings. J Psychosom Res. 2002;53:985–993. doi: 10.1016/s0022-3999(02)00488-9. [DOI] [PubMed] [Google Scholar]
- 22.Gibson EL. Emotional influences on food choice:sensory, physiological and psychological pathways. Physiol Behav. 2006;89:53–61. doi: 10.1016/j.physbeh.2006.01.024. [DOI] [PubMed] [Google Scholar]
- 23.Gillen MM, Lefkowitz ES. Gender and racial/ethnic differences in body image development among college students. Body Image. 2012;9:126–130. doi: 10.1016/j.bodyim.2011.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pope HG, Champoux RF, Hudson JI. Eating disorder and socioeconomic class:Anorexia nervosa and bulimia in nine communities. J Nerv Ment Dis. 1987;175:620–623. doi: 10.1097/00005053-198710000-00007. [DOI] [PubMed] [Google Scholar]
- 25.Swanson SA, Crow SJ, Le Grange D, Swendsen J, Merikangas KR. Prevalence and correlates of eating disorders in adolescents:Results from the national comorbidity survey replication adolescent supplement. Arch Gen Psychiatry. 2011;68:714–723. doi: 10.1001/archgenpsychiatry.2011.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gondoli DM, Corning AF, Salafia EHB, Bucchianeri MM, Fitzsimmons EE. Heterosocial involvement, peer pressure for thinness, and body dissatisfaction among young adolescent girls. Body Image. 2011;8:143–148. doi: 10.1016/j.bodyim.2010.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.van den Berg P, Thompson JK, Obremski-Brandon K, Coovert M. The Tripartite Influence model of body image and eating disturbance. J Psychosom Res. 2002;53:1007–1020. doi: 10.1016/s0022-3999(02)00499-3. [DOI] [PubMed] [Google Scholar]
- 28.Guidi J, Pender M, Hollon SD, Zisook S, Schwartz FH, Pedrelli P, Farabaugh A, Fava M, Petersen TJ. The prevalence of compulsive eating and exercise among college students:An exploratory study. Psychiatry Res. 2009;165:154–162. doi: 10.1016/j.psychres.2007.10.005. [DOI] [PubMed] [Google Scholar]
- 29.Petrie TA, Greenleaf C, Reel JJ, Carter JE. An examination of psychosocial correlates of eating disorders among female collegiate athletes. Res Q Exerc Sport. 2009;80:621–632. doi: 10.1080/02701367.2009.10599601. [DOI] [PubMed] [Google Scholar]