

Abstract
Background
Pectoralis major (PM) rupture is an uncommon sports injury that has become more prevalent in the past 20 years as a result of an increase in recreational weight lifting and sports participation. Ruptures occur most commonly at the tendon insertion (65%) and musculotendinous junction (27%). This study describes an open technique and clinical outcomes after reconstruction of a PM rupture at the musculotendinous junction.
Methods
In this case series, 6 patients with PM ruptures at the musculotendinous junction were enrolled, with a 12-month follow-up period. The diagnosis was made with magnetic resonance imaging and correlated with clinical examination findings. All patients underwent PM reconstruction with a semitendinosus allograft, followed by a graduated rehabilitation protocol. Postoperative outcomes were assessed using the American Shoulder and Elbow Surgeons score, Constant score, visual analog scale score, cosmesis, return of strength, and overall satisfaction.
Results
The average age at the time of surgery was 39.5 years. At the 12-month follow-up visit, the average outcome scores were as follows: American Shoulder and Elbow Surgeons score, 98.3; Constant score, 98; and visual analog scale score, 0.67. All patients were pleased with their cosmetic outcomes, as well as return of strength, and showed overall satisfaction with their postoperative results.
Conclusions
On review of the literature, this study is the first to describe the use of an isolated semitendinosus allograft to reconstruct a PM tendon following rupture at the musculotendinous junction. The excellent clinical outcomes suggest that the described technique can be a reliable tool in the orthopedic surgeon's armamentarium when approaching this uncommon PM tear.
Keywords: Pectoralis major reconstruction, pectoralis major repair, pectoralis major rupture, chronic pectoralis major rupture, musculotendinous, shoulder, reconstruction
Pectoralis major (PM) rupture is an uncommon sports injury that has become more prevalent in the past 20 years, with more than half of all reported cases occurring in the past decade. This phenomenon can be attributed to the increase in recreational weight lifting and sports participation.2,6, 7, 8, 9, 10 Total and near-total rupture injuries occur most commonly at the tendon insertion (65%) and the musculotendinous junction (27%).6,9,10
The classic patient is a muscular man aged between 20 and 40 years. This injury typically occurs during eccentric contraction of the PM, most commonly while performing the bench-press exercise. Patients often describe an audible pop, tearing sensation, immediate pain, and localized swelling and ecchymosis at the time of injury. Physical examination will show a thin anterior axillary fold, bulging at the PM origin on the chest with active contraction, and weakness in adduction and internal rotation of the affected arm.8, 9, 10
Surgical repair is the treatment of choice for young active patients with acute or chronic ruptures. This has been correlated with improved patient satisfaction, strength, cosmesis, and a shorter time to return to competitive sports. It has also been associated with a lower incidence of strength deficiency, primarily loss of peak torque and strength impairment in shoulder adduction.9,10
The purpose of this study was to report a reconstruction technique to address a PM rupture at the musculotendinous junction along with the clinical outcomes. By use of a semitendinosus allograft, a new PM tendon was created and the muscle was reattached to its anatomic insertion along the humerus. To our knowledge, this technique has not been reported in the literature.
Materials and methods
Study population
This is a case series of 6 patients who underwent surgical reconstruction of PM ruptures at the sternal head musculotendinous junction from November 2016 to January 2018 with a minimum follow-up period of 1 year. All patients gave informed consent to be included in this study. PM rupture was initially detected on clinical examination and confirmed to be at the musculotendinous junction on subsequent magnetic resonance imaging (Fig. 1). All surgical procedures were performed by the 2 senior surgeons using the described technique.
Figure 1.
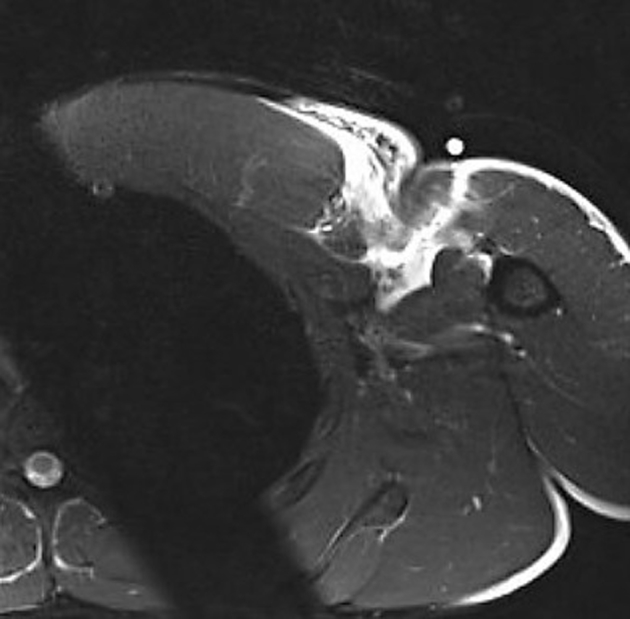
Axial magnetic resonance image showing complete tear of right pectoralis major muscle at musculotendinous junction.
Outcomes
Final follow-up data were collected during a routine postoperative visit at the 1-year mark. Patient-reported outcome measures included the American Shoulder and Elbow Surgeons (ASES) score, Constant score, visual analog scale (VAS) score for pain (0-10, with 0 indicating no pain), cosmesis, overall satisfaction, and return of strength. Return of strength was measured either by the weight the patient could bench press, in pounds, before injury and at 1 year postoperatively or by the ability to return to preinjury activities.
Surgical technique
The patient is seated in the beach-chair position after administration of an interscalene nerve block and establishment of general anesthesia. The affected arm is prepared and draped so that it can freely be moved in both abduction and rotation.
A 10-cm incision is made in line with the axillary crease after injection of 10 mL of 0.5% bupivacaine hydrochloride with epinephrine. Full-thickness subcutaneous flaps are raised medially and laterally. The deltopectoral interval is identified, and the cephalic vein is retracted laterally. The PM tendon defect is identified medially to confirm the location of the tear. Two No. 2 polyethylene braided sutures are placed in the PM to provide retraction (Fig. 2). The PM tendon is freed from its deep and superficial attachments. Any residual tendon is débrided from the humerus. The bone bed of the PM insertion site on the humerus is prepared with a motorized bur.
Figure 2.
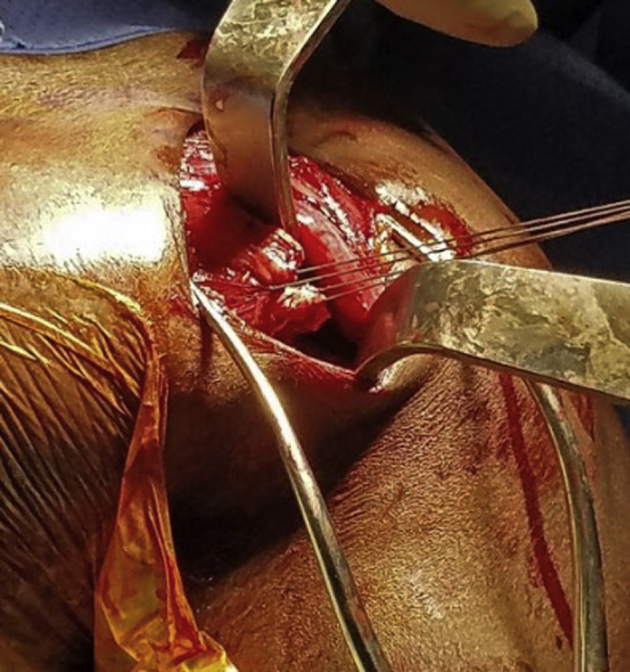
Pectoralis major rupture at musculotendinous junction.
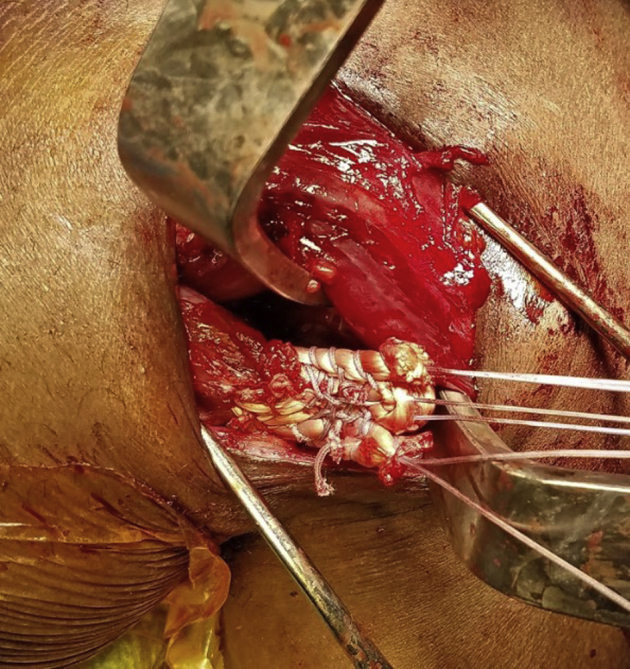
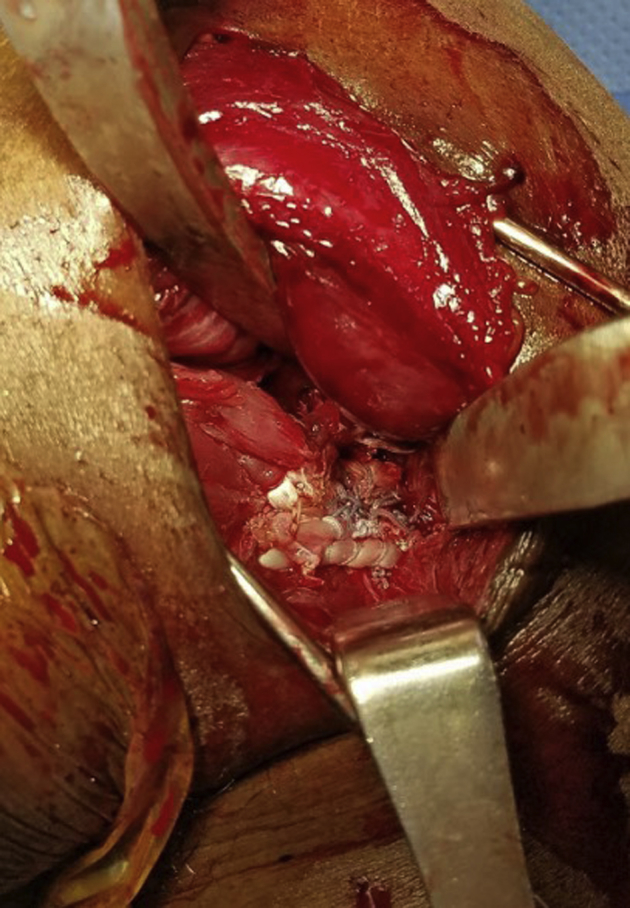
The semitendinosus graft is prepared (Fig. 3). A No. 2 polyethylene suture is placed in a Krackow whipstitch fashion on each end of the tendon. The graft is then weaved through the PM muscle by the Pulvertaft method, ensuring that the tendon is weaved through the robust posterior fascia if this is remaining. The tendon should be weaved into and out of the superior and inferior aspects of the PM, leaving 3 distinct limbs on the most lateral portion of the muscle (Fig. 4). For the middle limb, which is a loop of tendon, a No. 2 braided polyethylene suture is placed through the loop for the repair. At this point, there are 3 sets of sutures, 1 for each limb of the tendon graft that should be approximately 3 cm in length. Multiple sutures are placed to tie the tendon limbs together using a No. 2 polyethylene suture to create a new, robust large tendon. The tendon is secured to the muscle belly in multiple positions using a No. 2 polyethylene suture. The result is a flattened tendon resembling a normal PM tendinous attachment (Fig. 5). Tension is placed on the newly formed tendon to test its durability and pullout strength.
Figure 3.

Semitendinosus allograft chosen to reconstruct pectoralis major tendon.
Figure 4.

(A) The semitendinosus graft is weaved through the pectoralis major muscle by the Pulvertaft method, leaving 3 distinct limbs on the most lateral portion of the muscle. (B) Schema showing how the semitendinosus graft was weaved through the pectoralis major muscle. *Starting point of graft insertion.
Original illustration by Frank Scali, MD.
Figure 5.
Three tendon limbs sutured together in Krackow whipstitch technique, resulting in newly formed, flattened tendon resembling normal pectoralis major tendon.
Three holes are drilled in a vertical fashion in the humerus lateral to the biceps tendon. The three No. 2 polyethylene suture limbs are passed through 3 G2 Mitek suture anchors (DePuy Synthes, Warsaw, IN, USA) that are placed in their respective drill holes on the humerus. This reattaches the reconstructed PM tendon to the humerus (Fig. 6). Next, the additional suture in each anchor is passed through each limb of the graft and tied after tying of the Krackow limbs for each anchor. At the completion of the procedure, the tendon and muscle should be noted to be well fixed back to the humerus and under good tension. The wound is copiously irrigated with normal saline solution, and the subcutaneous tissue and skin are reapproximated. Following application of sterile dressings, the extremity is placed in a shoulder immobilizer.
Figure 6.
Newly formed tendon secured to humeral shaft by G2 anchors.
Rehabilitation
Postoperatively, the arm is immobilized in a sling for 4 weeks, allowing pendulum exercises and prohibiting external rotation beyond 30° and any abduction. Between 4 and 8 weeks, the patient is allowed full flexion while maintaining the same prohibitions as before for external rotation and abduction. Progressive strengthening is started at 10 weeks.
Results
Patient demographic characteristics and outcome data are summarized in Table I. The average patient age at the time of the operation was 39.5 years (range, 21-56 years). The PM rupture at the musculotendinous junction was on the left side in 3 patients and on the right side in 3. The average time to surgery was 4.33 weeks (range, 2-11 weeks). At the 12-month follow-up visit, the outcome scores were as follows: average ASES score, 98.3 (range, 95-100); Constant score, 98 for all patients; and average VAS score (on a 0-10 scale), 0.67 (range, 0-1). All patients were pleased with the cosmetic outcome of surgery at final follow-up (Fig. 7). Return of strength was measured either by the weight the patient could bench press, in pounds, before injury and at 1 year postoperatively or by the ability to return to preinjury activities, as summarized in Table II. All patients were very satisfied overall with their postoperative result.
Table I.
Demographic characteristics and outcome scores
| Patient No. | Age, yr | Laterality | ASES score | Constant score | VAS score |
|---|---|---|---|---|---|
| 1 | 40 | Left | 100 | 98 | 1 |
| 2 | 21 | Right | 100 | 98 | 1 |
| 3 | 56 | Left | 98 | 98 | 1 |
| 4 | 48 | Right | 100 | 98 | 1 |
| 5 | 44 | Left | 97 | 98 | 0 |
| 6 | 28 | Right | 95 | 98 | 0 |
ASES, American Shoulder and Elbow Surgeons; VAS, visual analog scale.
Figure 7.

Photograph showing overall cosmesis and muscle contour of injury site 12 months postoperatively.
Table II.
Return of strength
| Patient No. | Strength before injury (bench press) | Strength at 1 yr (bench press) |
|---|---|---|
| 1 | 124.7 kg max | 93.0 kg max |
| 2 | 179.2 kg max | 102.1 kg × 12 reps |
| 3 | 158.8 kg max | 102.1 kg × 30 reps |
| 4 | 124.7 kg × 3 reps (incline press) | 90.7 kg × 10 reps |
| 5 | 158.8 kg max | 133.8 kg max |
| 6∗ | Return to work at full capacity |
max, maximum; reps, repetitions.
Patient 6 had a work-related injury and was able to return to work at full capacity.
Discussion
This study demonstrates a technique for reconstruction of a PM rupture at the sternal head musculotendinous junction through the use of a semitendinosus allograft. Good outcomes at 1 year postoperatively show the viability of the described technique.
Patissier11 first published on PM ruptures in 1822, when describing injuries in artisans and craftsmen. The injured patient was an apprentice butcher who injured himself while at work and subsequently died, possibly due to an infected hematoma. Throughout the 1900s, only case reports were published regarding the incidence of PM ruptures. Bak et al1 published a meta-analysis in 2000 investigating reported cases from 1941 to 1998. Their results found only 150 cases of PM ruptures in the literature, with the mean age at the time of rupture being 28 years and a majority being due to work injuries until 1972, after which nearly all reported cases were related to sports injuries.
A majority of PM total and near-total ruptures occur at the tendon insertion site (65%) and the musculotendinous junction (27%).6,9,10 Bak et al1 found an increased tendency for bony avulsions to occur in younger individuals vs. tendon avulsions and ruptures at the musculotendinous junction. They also found a stronger relationship between the incidence of musculotendinous junction ruptures and work (41%) vs. sports (31%), although the data were not statistically significant.
Repair of PM ruptures is the recommended treatment for young active patients with acute or chronic ruptures owing to improved functional results. Nonoperative management has been shown to carry an unfavorable prognosis because of loss of peak torque and strength impairment in shoulder adduction.5,9 Conservative management is indicated in elderly patients and patients with partial tendon tears and muscle belly ruptures.4
Despite the uncommon nature of PM ruptures, there are a multitude of studies showing successful outcomes of PM repair at the tendon insertion. The 2 most commonly reported techniques for treating complete PM tendon rupture are transosseous sutures and suture anchors; both methods have shown excellent postoperative results, including a relatively reliable return to sports, a fast recovery, and a low complication rate.12 Both techniques are used for PM ruptures at the PM tendon insertion site.
Although PM ruptures at the musculotendinous junction are the second-most prevalent location of injury, there remains a paucity of literature regarding surgical techniques and outcomes. This article describes one technique to address a PM rupture at the musculotendinous junction and outcomes at 1 year postoperatively in 6 patients. In all patients, a new tendon was reconstructed using a semitendinosus tendon allograft. The new tendon allowed for reconstruction of a PM tendon following tears at the musculotendinous junction with subsequent reattachment to the humerus. All patients showed good outcomes as determined by their 1-year postoperative ASES score, Constant score, VAS score, satisfaction with their cosmetic outcome, return of strength, and excellent overall satisfaction. Regarding return of strength, 5 patients admitted to hesitance when testing their maximum bench-press weight and opted to attempt a lower weight. Despite moving less weight, all 5 patients were pleased with their physical performance at the 1-year follow-up visit. The last patient, who sustained his injury from a work accident, was able to return to work at full capacity.
Sikka et al14 described a similar technique using a fascia lata allograft to reconstruct a PM tendon owing to significant retraction of the tendon found intraoperatively. They reported a successful outcome with minimal cosmetic defect and no functional deficit at 5 years postoperatively. There are currently 2 case reports using a hamstring graft to address a PM tear: Baverel et al3 described the use of a semitendinosus and gracilis autograft as a bridge to reattach a retracted PM tendon to its humeral insertion. The semitendinosus was fanned on the PM side and fastened to the defect with suture. Schachter et al13 reconstructed the PM tendon by applying a gracilis-semitendinosus autograft draped and secured over the PM muscle belly with the opposing end fixated to the humerus via sutures across a drilled bone bridge. Both case reports showed optimal patient satisfaction regarding function and cosmesis. In contrast to the techniques used in these 2 case reports, our technique uses only a semitendinosus graft that is weaved through the muscle defect and secured with suture while the opposing end of the graft is attached to the humerus with suture anchors. The success of the case report of Baverel et al also demonstrates the possible utility of reconstructing a PM tendon with a semitendinosus graft in PM ruptures with a retracted tendon.
The limitations of our study are primarily focused on the small number of patients included. However, given the consistently good outcomes across all measurements in this study, we believe that the described technique is a viable treatment option for a PM tear at the musculotendinous junction. Future studies can be aimed toward increasing the sample size and performing chest magnetic resonance imaging at the final follow-up visit to evaluate incorporation of the reconstructed tendon at the musculotendinous junction.
With the rise of patients engaging in athletic activity and the subsequent growth in the PM rupture incidence, access to successful operative techniques to address this issue becomes ever more valuable. In this article, we have presented a technique to address the uncommon PM rupture at the musculotendinous junction. With its potential utility also in a retracted PM tendon from a chronic rupture, use of a semitendinosus allograft for PM tendon reconstruction can be added as a tool in the orthopedic surgeon's armamentarium.
Conclusion
On review of the literature, this study is the first to describe the use of an isolated semitendinosus allograft to reconstruct a PM tendon after rupture at the musculotendinous junction. The excellent clinical outcomes suggest that the described technique can be a reliable tool in the orthopedic surgeon's arsenal when approaching this uncommon PM tear.
Acknowledgments
The authors thank Frank Scali, MD, for his illustrative contributions.
Disclaimer
The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Footnotes
This study was performed in compliance with and received approval from the Institutional Review Board of Nassau Health Care Corporation at Nassau University Medical Center (study no. 17:171).
References
- 1.Bak K., Cameron E.A., Henderson I.J. Rupture of the pectoralis major: a meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc. 2000;8:113–119. doi: 10.1007/s001670050197. [DOI] [PubMed] [Google Scholar]
- 2.Balazs G.C., Brelin A.M., Donohue M.A., Dworak T.C., Rue J.P., Giuliani J.R. Incidence rate and results of the surgical treatment of pectoralis major tendon ruptures in active-duty military personnel. Am J Sports Med. 2016;44:1837–1843. doi: 10.1177/0363546516637177. [DOI] [PubMed] [Google Scholar]
- 3.Baverel L., Messedi K., Piétu G., Crenn V., Gouin F. Pectoralis major tear with retracted tendon: how to fill the gap? Reconstruction with hamstring autograft and fixation with an interference screw. Case Rep Orthop. 2017;2017:2095407. doi: 10.1155/2017/2095407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Beloosesky Y., Grinblat J., Weiss A., Rosenberg P.H., Weisbort M., Hendel D. Pectoralis major rupture in elderly patients: a clinical study of 13 patients. Clin Orthop Relat Res. 2003:164–169. doi: 10.1097/01.blo.0000076803.53006.12. [DOI] [PubMed] [Google Scholar]
- 5.de Castro Pochini A., Andreoli C.V., Belangero P.S., Figueiredo E.A., Terra B.B., Cohen C. Clinical considerations for the surgical treatment of pectoralis major muscle ruptures based on 60 cases: a prospective study and literature review. Am J Sports Med. 2014;42:95–102. doi: 10.1177/0363546513506556. [DOI] [PubMed] [Google Scholar]
- 6.ElMaraghy A.W., Devereaux M.W. A systematic review and comprehensive classification of pectoralis major tears. J Shoulder Elbow Surg. 2012;21:412–422. doi: 10.1016/j.jse.2011.04.035. [DOI] [PubMed] [Google Scholar]
- 7.Gregory J.M., Klosterman E.L., Thomas J.M., Hammond J., Shewman E.F., Wang V.M. Suture technique influences the biomechanical integrity of pectoralis major repairs. Orthopedics. 2015;38:e746–e752. doi: 10.3928/01477447-20150902-50. [DOI] [PubMed] [Google Scholar]
- 8.Guity M., Sharafat Vaziri A., Shafiei H., Farhoud A. Surgical treatment of pectoralis major tendon rupture (outcome assessment) Asian J Sports Med. 2014;5:129–135. [PMC free article] [PubMed] [Google Scholar]
- 9.Merolla G., Paladini P., Artiaco S., Tos P., Lollino N., Porcellini G. Surgical repair of acute and chronic pectoralis major tendon rupture: clinical and ultrasound outcomes at a mean follow-up of 5 years. Eur J Orthop Surg Traumatol. 2015;25:91–98. doi: 10.1007/s00590-014-1451-y. [DOI] [PubMed] [Google Scholar]
- 10.Mooers B.R., Westermann R.W., Wolf B.R. Outcomes following suture-anchor repair of pectoralis major tears: a case series and review of the literature. Iowa Orthop J. 2015;35:8–12. [PMC free article] [PubMed] [Google Scholar]
- 11.Patissier P. Chez J-B Baillere Libraire; Paris: 1822. Maladies des Bouchers: Traite des Maladies des Artisans [Butchers' diseases: treat diseases of craftsmen] [in French] [Google Scholar]
- 12.Provencher M.T., Handfield K., Boniquit N.T., Reiff S.N., Sekiya J.K., Romeo A.A. Injuries to the pectoralis major muscle: diagnosis and management. Am J Sports Med. 2010;38:1693–1705. doi: 10.1177/0363546509348051. [DOI] [PubMed] [Google Scholar]
- 13.Schachter A.K., White B.J., Namkoong S., Sherman O. Revision reconstruction of a pectoralis major tendon rupture using hamstring autograft: a case report. Am J Sports Med. 2006;34:295–298. doi: 10.1177/0363546505278697. [DOI] [PubMed] [Google Scholar]
- 14.Sikka R.S., Neault M., Guanche C.A. Reconstruction of the pectoralis major tendon with fascia lata allograft. Orthopedics. 2005;28:1199–1201. doi: 10.3928/0147-7447-20051001-19. [DOI] [PubMed] [Google Scholar]