

Abstract
Avulsion fractures of the tibial spine (also called “tibial eminence fractures” or “ACL avulsion fractures”), leading to discontinuity of anterior cruciate ligament (ACL) fibers, have been well described in the literature in both the pediatric and adult populations. To ensure the stability of the knee joint and good range of motion with minimal to no laxity, surgical reduction of the fracture and fixation are necessary to restore ACL length. Several arthroscopic techniques have been described to reduce and fix these fractures. We describe a technique using 2 anchors to fix the fractured tibial spine with no need to make any tibial tunnels or any extra leg wounds for the sutures.
Avulsion fractures of the tibial spine, leading to discontinuity of anterior cruciate ligament (ACL) fibers, have been well described in the literature in both pediatric and adult populations.1 This injury, which is usually caused by hyperextension of the knee associated with some lateral movement leading to increased stress on the ACL, is relatively rare in children (∼3 per 100,000 fractures) and is seen primarily at ages 8 to 14 years.2 The most common activity associated with this fracture is bicycle riding. The injury is virtually always to the anterior intercondylar eminence; the posterior intercondylar eminence is rarely fractured (10 times less common),3 and when this occurs, it is generally in skeletally mature individuals. Some authors say that if a knee injury with effusion occurs during a bike ride, a tibial spine fracture is present until proven otherwise.
Multiple techniques have been described for fixation of these fractures. Here we describe a technique using 2 anchors to fix the fractured tibial spine with no need to make any tibial tunnels or any extra leg wounds for the sutures.
Surgical Technique
Pearls and pitfalls of this technique are explained in Table 1 and advantages and disadvantages in Table 2. See Video 1 for detailed explanations.
Table 1.
Pearls and Pitfalls
| Step | Pearls | Pitfalls |
|---|---|---|
| Mobilization of bony avulsion and preparation | Panoramic view is obtained of the fracture site arthroscopically | Sometimes difficult to mobilize the fractured bone arthroscopically |
| Posterior anchor placement | Posterior fixation to the fracture gives more anatomic reduction and more stability | Technically demanding to place the anchor; needs an accessory portal |
| Suture passing | Sutures are passed through the bone and ACL itself anteriorly and posteriorly | Technically demanding to pass suture through the bone; needs special instruments to pass the suture (suture lasso); requires use of a cannula (increased cost) |
| Placement of the anterior anchor | Adds more stability and anatomic reduction | Extra cost; difficult visualization of the anterior cortex below tibial plateau; should be a knotless anchor |
Table 2.
Advantages and Disadvantages
| Advantages | Disadvantages |
|---|---|
| 1. Anatomic reduction | 1. Higher cost |
| 2. Stable construct | 2. Technically demanding |
| 3. No tibial tunnel needed | 3. Accessory portals and extra instrumentation (suture lasso, cannula) required |
| 4. No extra incision needed | 4. Increased operation time |
| 5. Two-point fixation | |
| 6. Early mobilization | |
| 7. Can be used for acute and chronic cases |
Preoperative Evaluation
Patients with a tibial spine avulsion will present with a swollen and painful knee with an inability to bear weight on the affected extremity. Lachman or anterior drawer tests may be positive, as with an ACL tear, but the pain can make it difficult to perform a proper physical examination of the affected knee. X-rays will show an avulsion fragment of the tibia. Diagnosis can be made with radiographs alone; computed tomography or magnetic resonance imaging is useful to determine the size of the fragment and any associated injuries.
Setup
Patient is placed supine on the operating table under general anesthesia with an upper thigh tourniquet and the knee in 90° flexion on the table. Painting is done from the end of the tourniquet to the foot, and then toweling is performed.
Portals
This technique uses 4 arthroscopy portals: anteromedial (just medial to the patellar tendon) (viewing portal); high anterolateral and far medial (working portals); and high anteromedial suprapatellar (accessory portal) for posterior anchor placement.
Operation
Diagnostic Arthroscopy
Normal diagnostic arthroscopy to the knee is performed starting from the high anterolateral portal. The medial portal is established for shaving and probing, which will show an avulsion of the ACL from the tibial spine. The ACL is probed to assess the tension and to check whether the femoral attachment of the ACL is intact. The far medial portal is then made for suture management and reduction of the fracture.
Tibial Spine Preparation
Viewing from the anterolateral portal, a periosteal elevator is used to elevate the fractured tibial piece (Fig 1). Using a radiofrequency ablator (CoolCut RF Ablator; Arthrex), ablation of the bone edges and removal of clots are performed at the site of avulsion to refresh the fracture edges (Fig 2). Reduction of the avulsed piece by probing is tried to ensure that the piece will be reduced in its place.
Fig 1.

Anterolateral portal, right knee in 90° of flexion, supine position; use of periosteal elevator to elevate the fracture tibial piece.
Fig 2.
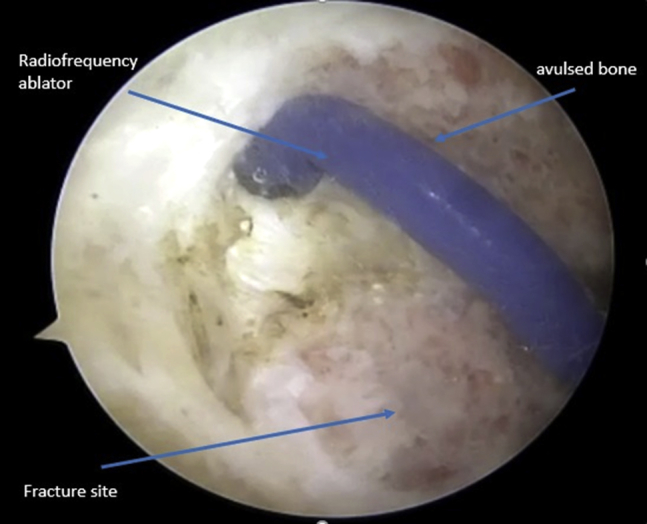
Anterolateral view, right knee in 90° of flexion, supine position. Using a radiofrequency ablator (CoolCut), ablation of the bone edges and removal of clots are performed at the site of avulsion to refresh fracture edges.
Reduction and Fixation
With the knee in 90° flexion and viewing from the medial portal, the accessory high anteromedial suprapatellar portal is established for inserting the anchor 45° to the tibial plateau. Using a guided knotted suture anchor, a double-loaded 3.0-mm suture (SutureTak; Arthrex) is fixed posterior to the avulsion fracture site. From the same portal, an 8-mm passport cannula (Arthrex) is introduced (Figs 3 and 4). Using a 45° lasso (Arthrex) curved to the left, 1 limb of the suture is passed through the anterior bone side and the other limb through the anterior fibers of the ACL. Then 1 limb suture is passed through the posterior part of the bone and the other limb through the posterior part of the ACL (Fig 5). Arthoscopic knots are tied (Fig 6). The knee is extended to 30° to allow viewing of the anterior compartment below the tibial plateau. From the same portal, shaving and ablation are done to clean the anterior surface of the upper tibia to prepare the bed for the anterior anchor (Fig 7).
Fig 3.
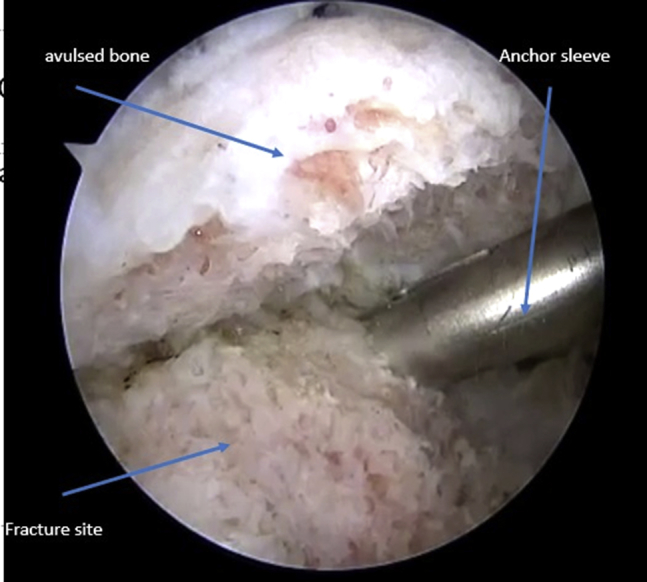
Anteromedial view, right knee in 90° of flexion, supine position. Using a guided knotted suture anchor, a double-loaded 3.0-mm anchor (SutureTak; Arthrex) is fixed posterior to the avulsion fracture site. From the same portal, an 8-mm passport cannula (Arthrex) is introduced.
Fig 4.
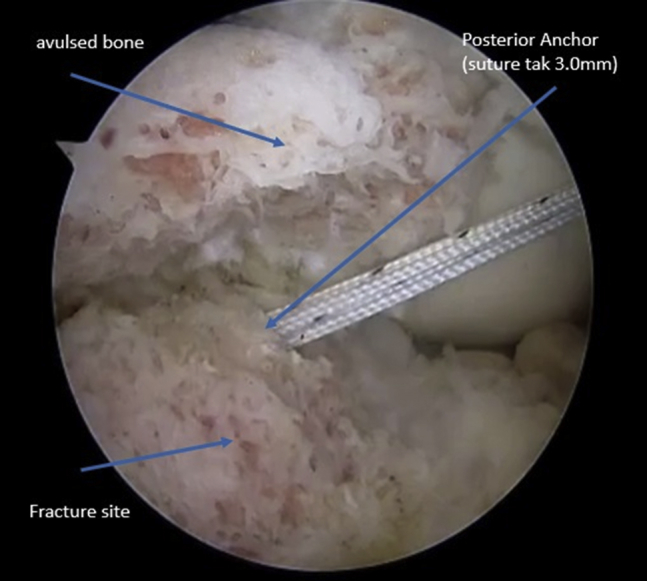
Anteromedial view, right knee in 90° of flexion, supine position. Posterior anchor is inserted and secured.
Fig 5.
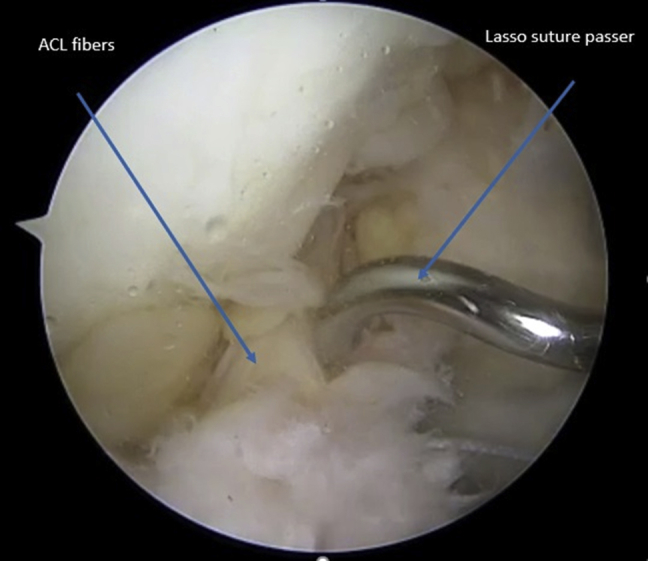
Anteromedial view, right knee in 90° of flexion, supine position. With a 45° lasso (Arthrex) curved to the left, 1 limb of the suture is passed though the anterior bone side and the other limb through the anterior fibers of the ACL. Then 1 limb of the suture is passed through the posterior part of the bone and the other limb through the posterior part of the ACL.
Fig 6.
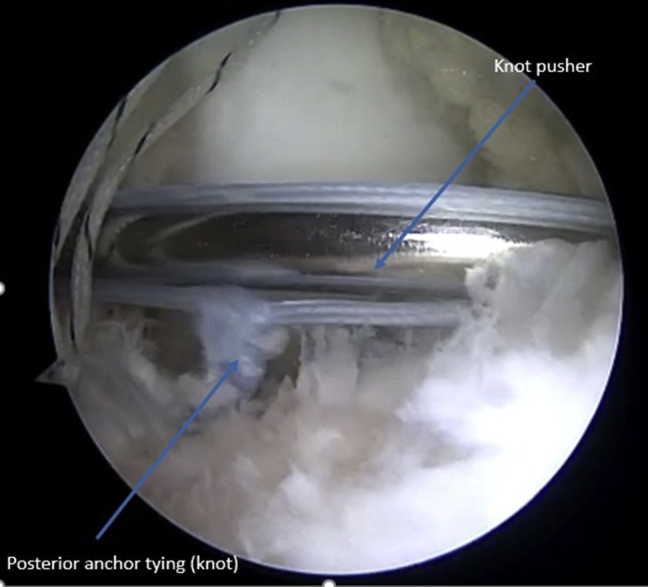
Anteromedial view, right knee in 90° of flexion, supine position. Arthroscopic knot tying of the suture.
Fig 7.
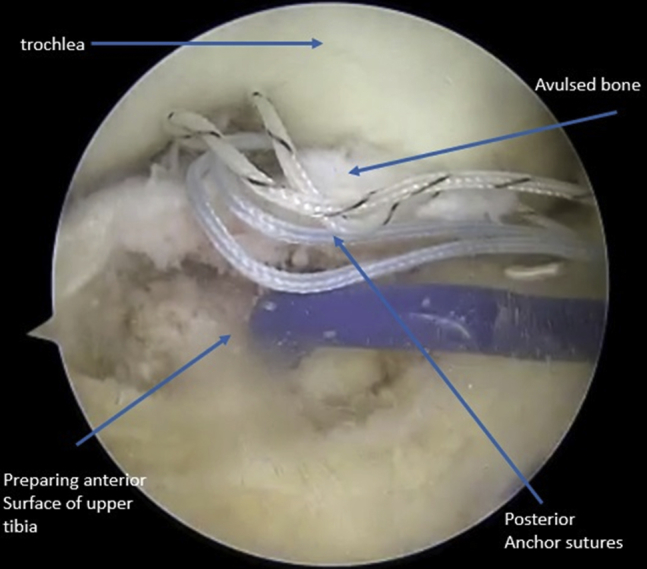
Anteromedial view, right knee in 90° of flexion, supine position. Shaving and ablation are done to clean the anterior surface of the upper tibia to prepare the bed for the anterior anchor.
The sutures coming out of the posterior anchor are loaded through a pushlock anchor (knotless) size 3.5 mm (Arthrex), and the anchor is fixed to the anterior part of the tibia using a double-row technique (Fig 8). The tension of the ACL is checked to make sure it is tight in extension and there is no impingement in extension (Fig 9).
Fig 8.
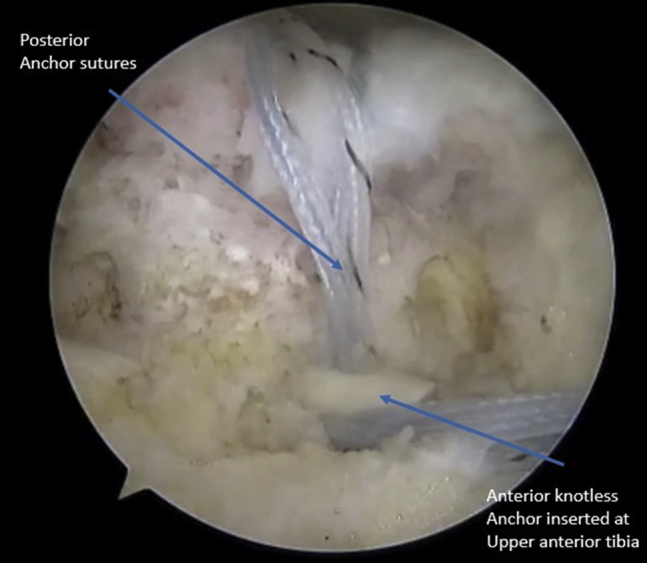
Anteromedial view, right knee in 90° of flexion, supine position. Loading of the sutures coming out of the posterior anchor with a pushlock anchor (knotless) size 3.5 mm (Arthrex). The anchor is fixed to the anterior part of the tibia using a double-row technique.
Fig 9.
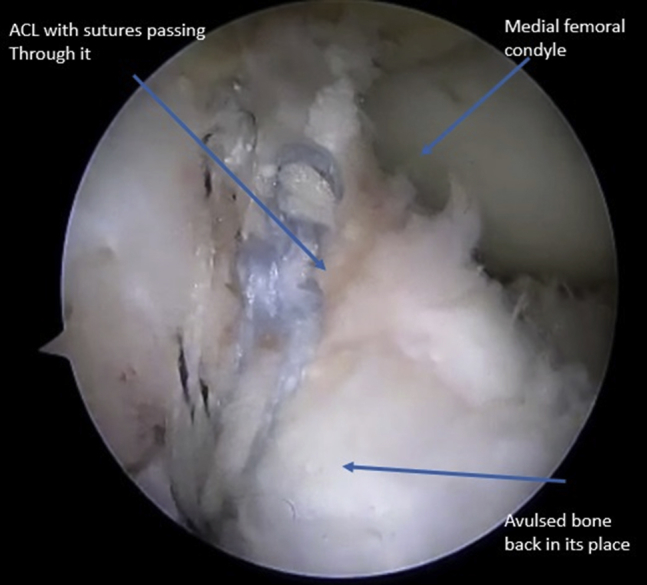
Anteromedial view, right knee in 90° of flexion, supine position. The fracture is reduced and fixed, and the tension of the ACL is checked to make sure it is tight in extension and there is no impingement in extension.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
Patient is placed supine on the table with foot over the table, knee flexed at 90°. Four portals are anteromedial, high anterolateral, far medial, and high anteromedial suprapatellar. The avulsion site is exposed by shaving, and the ACL is probed. The far medial portal is established for suture management and reduction of the fracture. Using a periosteal elevator to elevate the fracture tibial piece, ablation of the bone edges and removal of clots are performed at the site of avulsion to refresh the fracture edges. Reduction of the avulsed piece by probing is tried. With the knee in 90° flexion, from the accessory high anteromedial suprapatellar portal, we insert the anchor 45° to the tibial plateau. Using a guided knotted suture anchor, a double-loaded 3.0-mm suture is fixed posterior to the avulsion fracture site. Using a 45° lasso curved to the left, the ACL and the avulsed bone are sutured. The knee is then placed in 30° extension, and from the same portal, the anterior surface is prepared for anchor placement. After loading the sutures coming out of the posterior anchor through a pushlock anchor (knotless) size 3.5 mm, the anchor is fixed to the anterior part of the tibia using a double-row technique. The tension of the ACL is checked to make sure it is tight in extension and there is no impingement in extension.
References
- 1.Chouhan V. Arthroscopic fixation of tibial spine avulsion fracture in open physis. J Orthop Case Rep. 2016;6:86–88. doi: 10.13107/jocr.2250-0685.450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gamboa J.T., Durrant B.A., Pathare N.P., Shin E.C., Chen J.L. Arthroscopic reduction of tibial spine avulsion: suture lever reduction technique. Arthrosc Tech. 2017;6:e121–e126. doi: 10.1016/j.eats.2016.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Melugin H.P., Desai V.S., Camp C.L. Do tibial eminence fractures and anterior cruciate ligament tears have similar outcomes? Orthop J Sports Med. 2018;6 doi: 10.1177/2325967118811854. 2325967118811854. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Patient is placed supine on the table with foot over the table, knee flexed at 90°. Four portals are anteromedial, high anterolateral, far medial, and high anteromedial suprapatellar. The avulsion site is exposed by shaving, and the ACL is probed. The far medial portal is established for suture management and reduction of the fracture. Using a periosteal elevator to elevate the fracture tibial piece, ablation of the bone edges and removal of clots are performed at the site of avulsion to refresh the fracture edges. Reduction of the avulsed piece by probing is tried. With the knee in 90° flexion, from the accessory high anteromedial suprapatellar portal, we insert the anchor 45° to the tibial plateau. Using a guided knotted suture anchor, a double-loaded 3.0-mm suture is fixed posterior to the avulsion fracture site. Using a 45° lasso curved to the left, the ACL and the avulsed bone are sutured. The knee is then placed in 30° extension, and from the same portal, the anterior surface is prepared for anchor placement. After loading the sutures coming out of the posterior anchor through a pushlock anchor (knotless) size 3.5 mm, the anchor is fixed to the anterior part of the tibia using a double-row technique. The tension of the ACL is checked to make sure it is tight in extension and there is no impingement in extension.