

Abstract
Background: Injuries are increasingly recognized as a major component of the global burden of disease, as they tend to affect mainly youth and are usually followed by premature death or severe disability. The longstanding conflict in Iraq has resulted in a situation of continuous violence and ongoing instability, which has in turn led to an increasing incidence of injuries and a crippled health system. Objective: To sketch a trend of non-military accidents in Iraq (road traffic accidents [RTA], falls, burns, firearm injuries, assaults by sharp objects and sexual assaults) among civilians during the last 14 years associated with the period of conflict (2003–2016). Methods: This descriptive study was conducted during the period from January 1st through to December 31st, 2017 using already available surveillance data from the Ministry of Health in Iraq. The methodology was based on measuring the incidence of each accident for the period from 2003 through 2016 and plotting it against time. Linear regression was computed to estimate the trends of the disease. Results: The rate of RTAs significantly increased between 2003 and 2016, from 1.85 to 2.9 per 1000 (p ≤ 0.01), as did accidental falls especially after 2008 (males more than females) (p ≤ 0.01). By contrast, after a peak in 2011, burns dropped significantly from 4.19 to 3.42/1000, along with firearm accidents, which fell from 2.2/1000 in 2007 to 0.39 in 2016 (p ≤ 0.01), mostly among males. Assaults with sharp objects also decreased with time to a rate of 0.47/1000 (p = 0.0001). Sexual assaults showed a significant downward sloping trend over time to p = 0.037. Conclusion: Accidents still add a burden on the already deteriorated Iraqi health system. Understanding the impact of this burden is essential to better prepare for future plans and interventions that may help improve the quality of health services.
Keywords: trend, accidents, injuries, Iraq, conflict
Introduction
Injuries are increasingly recognized as a major component of the global burden of disease.1 The burden of accidents and injuries is immense, as they tend to affect mainly youth and are usually followed by premature death or severe disability. They represent the fourth leading cause of death globally and the number one cause of death in youth in developing countries.2 One quarter of the disabilities in some countries is estimated to be due to accidents and violence.3
Between 1990 and 2010 road traffic crashes, burns, falls, suicide, homicide, and violence resulted in approximately 5.1 million deaths annually.4
Injuries and violence represent a threat to health for every society, as they cause more than five million deaths worldwide every year, accounting for 9% of the total global mortality, of which road traffic accidents form approximately a quarter.5 Furthermore, many of those who survive attacks of violence, accidents and other injuries live with one or more disabilities that may negatively affect the quality of their lives.6 Injuries were responsible for an estimated 5% of the total years lived with disability in 2015.7
Road traffic accidents kill 1.25 million people worldwide each year, mainly among those aged 15–29 years. Approximately 90% of world fatalities on roads happen in low- and middle-income countries (LMICs), despite that these countries own only 54% of the world's vehicles.8–9 Falls are the second leading cause of unintentional injury worldwide and are increasingly frequent given aging populations,10 while burns are ubiquitous during conflict. Previous studies of civilian injuries in LMICs disrupted by conflict reported that burns were responsible for 4–10% of all injuries.11
The longstanding conflict in Iraq has resulted in a situation of continuous violence and ongoing instability, which has in turn led to an increasing incidence of injuries and a crippled health system with widely acknowledged rampant corruption. This ongoing conflict has led to continuous violence, wars, economic sanctions and sectarian divisions.12 Populations have been subdued due to mass executions, systematic rape, torment, and genocide. Children have been used as suicide bombers and human shields.13 Survivors often present with psychological trauma and depression with reports of elevated rates of suicide.14 In 2014, the estimated number of disabled people or those with special needs in Iraq was four million, a rate of 15% against a global rate of 10%.15 The figure reported for the rate of disabilities and special needs in Iraq is thought to constantly increase due to ongoing violence, conflicts and acts of terrorism.
Approximately 470,000 people died prematurely in 2015 as victims of homicide worldwide, registering a rate of 6.4 per 100,000.16 That year WHO estimated the homicide level in Iraq as 12.7/100,000,17 which was considered the leading cause of premature mortality in the country.18 Iraq also captured the first rank among the EMR countries in the “age-adjusted injury mortality rate due to war (252/100,000), exceeding that of Afghanistan, Sudan and Somalia.”19
Rationale
Data about civilian injuries in conflict are usually scarce.20–25 To the best of our knowledge, no study has attempted to estimate non-military related accidents among civilians during the years of conflict in Iraq. To fill this gap, we analyzed data from nationally reliable sources of surveillance in the Ministry of Health Iraq to establish baseline information.
The objective of this study was to determine a trend for the six main types of accidents (RTA, falls, burns, firearm injuries, assaults by sharp objects and sexual assaults) in Iraq during the last 14 years that represent a critical period of unrest since the United States invasion. It is hoped that the resulting baseline information obtained can be used by health authorities and policy makers to understand the impact and effects of accidents during conflict and to better prepare and plan for future interventions. This will strengthen measures of primary and secondary prevention by improving the quality and standards of the relevant health services.
Methods
This descriptive study was conducted during the period from January 1st through December 31st 2017 using and processing already available surveillance data from the Ministry of Health in Iraq. The methodology to determine the trend was based on measuring the incidence rate of each non-military related accident during the conflict period from 2003 till 2016.
Accidents were classified into six categories: Road traffic accidents (RTA), accidental falls, burns, firearm injuries, and assaults with sharp objects. Estimates of sexual assaults were also included within the study as these incidents were associated with the conflict and are usually causes of physical and/or psychological trauma. Injuries were defined as intentional or unintentional physical harm that required medical care and that resulted in a period of reduction or loss of normal daily activities.
Data were collected from data registries of the Department of Health and Vital Statistics of the Iraqi Ministry of Health. All data related to the years 2003–2016 were included in the study.
Data were gathered month by month, double-checked and confirmed against data from other health organizations, such as WHO and UNICEF reports and surveys.
To measure the rate of occurrence, the total population for each governorate, or province, and for Iraq as a whole, was obtained from the Central Statistical Organization to be used as denominators. These rates were then plotted against time to define the trend of each accident.
Data Analysis
A descriptive statistical analysis to estimate the rates was carried out using the Statistical Package for Social Sciences (SPSS version 23). Linear regression was computed to estimate the trends of the disease. The outcome depended on the slope—whether downward, upward, or flat—to assess the trend. Levels of significance were determined based on a value of p ≤ 0.05.
The incident percent change was calculated for the whole and mid-time periods as a measure of difference for each accident trend. The trends presented the rate of occurrence for the whole country, distributed by gender and age.
Official approvals were granted from the Iraqi Ministry of Health and the Central Statistical Organization (CSO). The ethical aspect was approved by the Ethical Committee in the College of Medicine, Mustansiriyah University. We used the anonymous database for the analysis.
Results
The rate of road traffic accidents increased significantly from 1.85/1000 in the year 2003 up to 2.9/1000 in 2016 (p = 0.004), with male predominance (ratio 3:1) (Figure 1).
Figure 1.
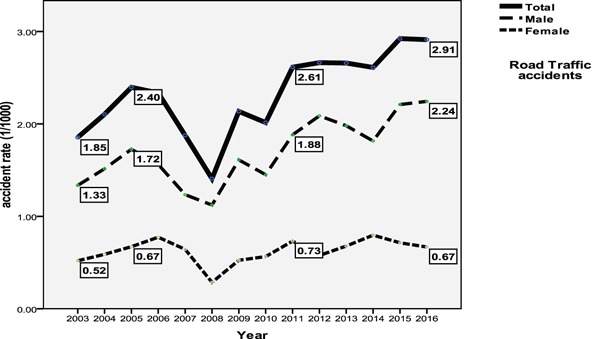
Trend of road traffic accidents by gender (2003–2016).
The trend of accidentalfalls showed a significant increase especially after 2008 (p ≤ 0.01) (males more than females) (Figure 2).
Figure 2.
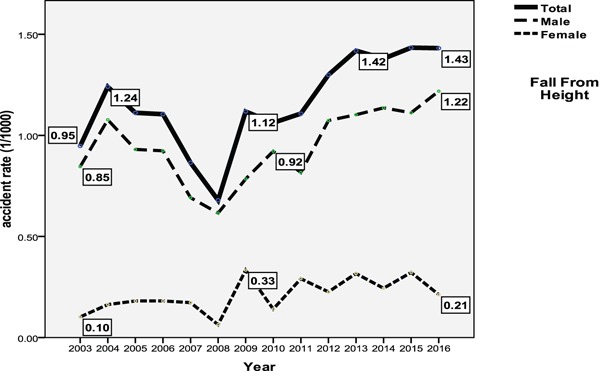
Trend of falls from a height by gender (2003–2016).
After a peak in 2011, burns dropped significantly from 4.19/1000 to 3.42/1000 (p ≤ 0.01) (Figure 3). Males and females were equally affected, but it was more prevalent among middle-aged and older adults (older than 40 years).
Figure 3.
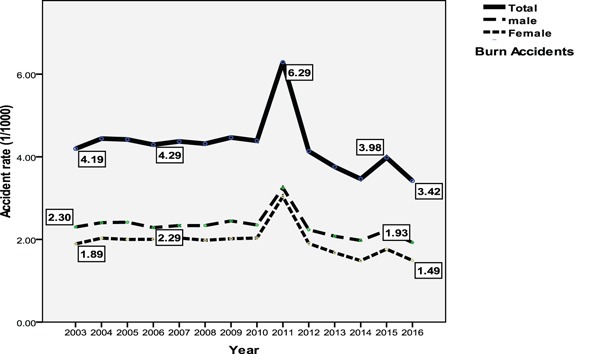
Trend of burns by gender (2003–2016).
Firearm accidents significantly decreased, starting with a rate of 2.2/1000 in 2007 and ending at 0.39 in 2016 (p ≤ 0.01), mostly among males (Figure 4).
Figure 4.
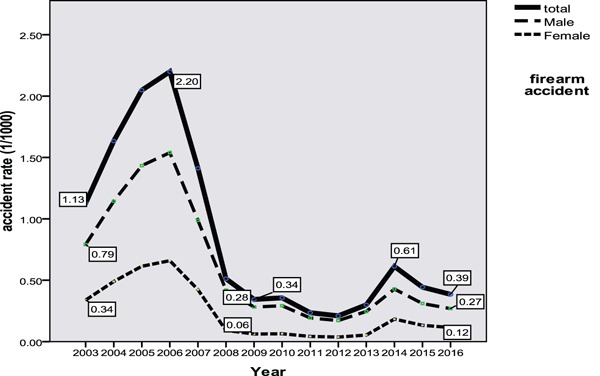
Trend of firearm accidents by gender (2003–2016).
The trend of assault by sharp object accidents also decreased with time to reach a rate of 0.47/1000 with p = 0.0001 (Figure 5). This type of accident affected males more than females. Sexual assaults showed a significant down-sloping trend over time with p = 0.037 and mostly against females (Figure 6).
Figure 5.
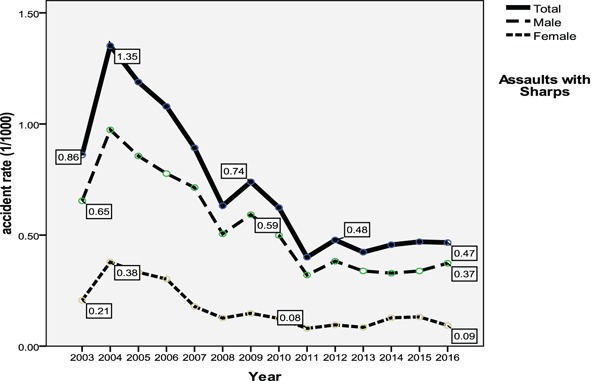
Trend of assaults with sharp objects by gender (2003–2016).
Figure 6.
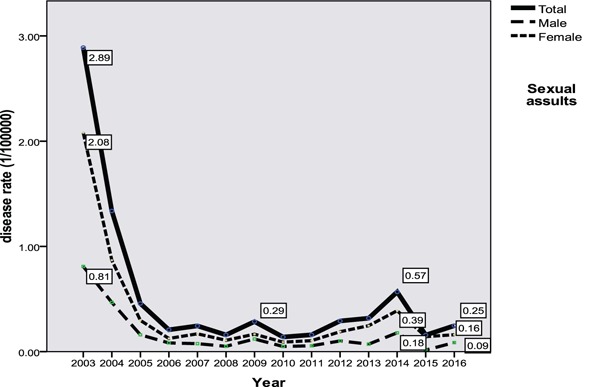
Trend of sexual assaults by gender/100,000 (2003–2016).
Table 1 shows the distribution of all accidents for the studied period (2003–2016) by age. RTA and firearm accidents were more prevalent among the age group 20–39 years, while falls were reported more in the young age groups (less than 20 years). Burns formed approximately half (46%) the total of accidents during the whole period.
Table 1.
Distribution of cases of accidents by age for the whole period (2003–2016).
| Type of accident | Age groups (years) | Totals by accident | |||||||
|
| |||||||||
| < 5 | 5–19 | 20-39 | 40+ | ||||||
|
| |||||||||
| No. | % | No. | % | No. | % | No. | % | ||
|
| |||||||||
| RTA | 9761 | 1.1 | 104,710 | 11.8 | 456,998 | 51.5 | 315,905 | 35.6 | 887,374 |
|
| |||||||||
| Accidental falls | 117,634 | 26.6 | 132,670 | 30.0 | 111,885 | 25.3 | 80,045 | 18.1 | 442,234 |
|
| |||||||||
| Burns | 207,556 | 12.8 | 295,118 | 18.2 | 484,839 | 29.9 | 634,019 | 39.1 | 1,621,532 |
|
| |||||||||
| Firearm accidents | 909 | 0.3 | 17,571 | 5.8 | 208,432 | 68.8 | 76,042 | 25.1 | 302,954 |
|
| |||||||||
| Assault by sharp objects | 0 | 0 | 26,140 | 9.9 | 142,852 | 54.1 | 95,058 | 36.0 | 264,050 |
|
| |||||||||
| Sexual assaults | 0 | 0 | 69 | 3.7 | 1336 | 71.1 | 474 | 25.2 | 1879 |
|
| |||||||||
| Total accidents by age | 335,860 | 576,278 | 1,406,342 | 1,201,543 | 3,529,023 | ||||
|
| |||||||||
Table 2 shows the percent change in the incidence rate of accidents during the periods 2003–2010, 2010–2016, and 2003–2016.
Table 2.
Percent change in incidence rate of accidents (2003–10), (2010–16), (2003–16).
| ID | Accident | Rate 2003 | Rate 2010 | Percent change 2003–10 | Rate 2016 | Percent change 2010–16 | Percent change 2003–16 |
|
| |||||||
| 1 | RTA | 1.85 | 2.01 | 8.65 | 2.91 | 44.78 | 57.30 |
|
| |||||||
| 2 | Fall from height | 0.95 | 1.06 | 11.57 | 1.43 | 34.9 | 50.53 |
|
| |||||||
| 3 | Burns | 4.19 | 4.39 | 4.77 | 3.42 | − 22.10 | − 18.38 |
|
| |||||||
| 5 | Firearm | 1.13 | 0.34 | − 69.9 | 0.39 | 12.8 | − 65.48 |
|
| |||||||
| 6 | Assaults with sharps | 0.86 | 0.62 | − 27.9 | 0.47 | − 24.19 | − 45.34 |
|
| |||||||
| 7 | Sexual assaults | 0.03 | 0.0028 | − 90.66 | .0025 | − 10.71 | − 91.66 |
|
| |||||||
| 8 | Total accidents | 6.44 | 6.02 | − 6.52 | 5.2 | − 13.62 | − 19.25 |
|
| |||||||
Discussion
The global trend of accidents witnessed a decrease during the period between 2005 and 2015,26 even as it was increasing in middle and low income countries such as Egypt and Iran.27–28 Whilst conditions in Iraq do not seem to be better, per se, the pattern however has shifted from intentional injuries (gunshot and explosions) to unintentional injuries (falls and road traffic accidents), which means that Iraqi civilians are still experiencing a high incidence of accidents, even after the relative decline in the acts of terrorism.
Road traffic accidents presented with the greatest change over the study period, especially after 2008, with an elevated total of 887,374 accidents, mainly affecting pedestrians. This could be explained by the rapid surge in the number of vehicles on the roads, including cars and motorcycles, accompanied by weak or absent traffic legislation.29 Generally, the Eastern Mediterranean region has the world's second highest road traffic accident incidence and death rate, after Africa.30
The estimated road traffic fatalities in Iraq were 3963 in 2013. In 2015 the rate was 20/100,000,31 with 60% of the survivors developing permanent disabilities that in turn affected their living and socioeconomic status.32 A study in Iraq in 2013 revealed a RTA fatality rate of 8.6 to 10.7 per 100,000, of whom 78.2 % were males and 28.5 % were children.29
Accidental falls showed an upward trend in Iraq, mainly in males. A similar increasing trend was noted by Bener et al., in Qatar (2012) but with a lower incidence rate (0.5/1000).33 The main affected age groups were children (attributed probably to parental unawareness) and adolescents who are pushed to work in building construction and other dangerous labor (with ignorance of safety measures), as they may become the principal breadwinners for their families, especially after the loss of many of the householders as a consequence of war-related violence, particularly after the 2003 USA invasion.
A community-based household survey conducted in Baghdad estimated the case fatality rate of falls to be 5%, where 75% of the cases left those injured with some type of life-limiting disability.34
Burns
The incidence of burns showed a stable rate. However, the prevalence of burns during the peak period in 2011 is considered very high when compared to the global (1/1000)35 and regional rates (1.87/1000).36 This high rate could be described as an epidemic. It arose from the security instability all over the country,37 added to the status of thousands of displaced families where 16% had no ordinary facilities for cooking and personal warming, a situation that increased the risk of burn accidents.38
In addition to the high rate of mortality and disability associated with burns, they are considered the most expensive of nonfatal injuries that affect the victim's income, the family's economic standards, and even their food security,39 not to mention the social stigma due to the physical disfigurement that in turn leads to isolation, psychological impairment, and reduced productivity.40 Surveys in Iraq revealed that the burn-related case fatality rate reached as high as 16%.37
Assaults with firearms and sharp objects
Firearm injuries witnessed a drop after a spike extended between 2003 and 2008. This trend mirrored the social situation in Iraq. The first peak occurred after the US invasion in 2003 and the subsequent sectarian conflict that witnessed a heightened level of combat and interpersonal violence with a complete absence of law in many Iraqi territories.12 The second peak started after 2013, after the rising activities of fighters belonging to what is called the Islamic State of Iraq and Sham (ISIS), with subsequent military operations, dubbed “liberation activities,” launched by the government and its allied forces that significantly raised the levels of such injuries among both civilians and combatants.14 The Lafta et al., study in 201513 estimated the mortality from intentional injuries at approximately 39%, with a disability rate of 77.1%. When these are added to the economic burden arising from subsequent hospitalization, surgical procedures and rehabilitations, it can draw a clearer picture of the resulting burden that often exhausts the already crippled healthcare system in general. This also affects the quality of living of the affected households as lost income from those previously working and who are subsequently injured can be devastating.41
Sexual assaults peaked in 2003 in the wake of the US invasion. It can be attributed to the chaos happening at that time, including assaults that were committed by the US army. People started to report such crimes in 2003 as they thought that there would be a democratic transition towards freedom, but then, as everything reverted to the old situation, the case reporting declined again. This explains why there was only a small increase in the incidence of assaults during 2014, the time of ISIS' occupation of Mosul, despite several nongovernmental reports of rape against women in the affected territories.42
The results revealed that accidents were more prevalent among adults, with the exception of accidental falls. It is understood that adults are more exposed to accidents as they are usually the breadwinners of their families, so being outside the house most of the day increases their exposure to different types of intentional and unintentional accidents. On the other hand, being a male in Iraq is still highly dangerous which means that even after the relative recession of violence, life is still difficult for Iraqi males.
The main limitations of this study are underreporting and incomplete registries. As the source of data was hospital records, the reported injuries were likely moderate-to-severe in order to require hospital admission, meaning that most minor injuries were not registered. On the other hand, fatal injuries were also not registered as they typically go directly to the morgue. Thus the reported incidence rates are bare minimum estimates due to underreporting. Scarce case information is a common problem when dealing with Ministry of Health registries. A house-to-house survey would be more informative but it would also be associated with recall bias.
Conclusion
Although some accidents in Iraq are sloping downward, such as those involving firearms, assault by sharp objects, and sexual assaults, other more prevalent accidents, such as RTA and accidental falls are increasing, meaning that accidents continue to burden an already deteriorated Iraqi healthcare system. Understanding the impact of this burden is essential to better prepare for future plans and interventions that can improve the standards of health services (including emergency units), upgrade their quality, and enhance accessibility and utilization.
Financial disclosure
None.
Conflict of interest
None.
Author contributions
Both authors contributed equally to the design, data collection, data analysis and writing of the final article.
References
- 1.Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–2223. doi: 10.1016/S0140-6736(12)61689-4. [DOI] [PubMed] [Google Scholar]
- 2.Norouzi V, Feizi I, Vatankhah S, Pourshaikhian M. Calculation of the Probability of Survival for Trauma Patients Based on Trauma Score and the Injury Severity Score Model in Fatemi Hospital in Ardabil. Arch Trauma Res. 2013;2(1):30–35. doi: 10.5812/atr.9411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. World Health Organization. Falls. Fact sheet 2018; March 22 2018 [Internet]. Geneva: Switzerland, World Health Organization; 2018. Available from: http://www.who.int/mediacentre/factsheets/fs344/en.
- 4.Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi: 10.1016/S0140-6736(12)61728-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. World Health Organization. Injuries. Health topics 2018 [Internet]. Geneva: Switzerland, World Health Organization; 2018. Available from: http://www.who.int/topics/injuries/about/en.
- 6. World Health Organization. Injuries and violence. The Facts 2014 [Internet]. Geneva: Switzerland, World Health Organization; 2018. Available from: http://www.who.int/violence_injury_prevention/media/news/2015/Injury_violence_facts_2014/en.
- 7.Global Burden of Disease Study. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2015;388(1005):1545–602. doi: 10.1016/S0140-6736(16)31678-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. World Health Organization. Road traffic injuries. Fact sheet 2018 [Internet]. Geneva: Switzerland, World Health Organization; 2018. Available from: http://www.who.int/mediacentre/factsheets/fs358/en/
- 9. World Health Organization. Facts on road safety 2018 [Internet]. Geneva: Switzerland, World Health Organization; 2018. Available from: http://www.who.int/features/factfiles/roadsafety/en.
- 10.World Health Organization. Geneva: Switzerland: World Health Organization; 2010. Injuries and violence: the facts [Internet] [Google Scholar]
- 11.Atiyeh BS, Gunn SW, Hayek SN. Military and civilian burn injuries during armed conflicts. Ann Burns Fire Disasters. 2007;20(4):203–215. [PMC free article] [PubMed] [Google Scholar]
- 12.Webster PC. Iraq's growing health crisis. Lancet. 2014;384(9938):119–120. doi: 10.1016/s0140-6736(14)61148-x. [DOI] [PubMed] [Google Scholar]
- 13.Lafta R, Al-Shatari S, Cherewick M, Galway L, Mock C, Hagopian A et al. Injuries, death, and disability associated with 11 years of conflict in Baghdad, Iraq: A randomized household cluster survey. Plos One. 2015;10(8):e0131834. doi: 10.1371/journal.pone.0131834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lancet Editor. Iraq's neglected health and humanitarian crisis. Lancet. 2015;385(9985):2324. doi: 10.1016/S0140-6736(15)61089-3. [DOI] [PubMed] [Google Scholar]
- 15. UNAMI/OHCHR. United Nations Assistance Mission for Iraq/Office of the High Commissioner for Human Rights. Report on the Rights of Persons with Disabilities in Iraq, December 2016 [Internet]. Available from: http://www.uniraq.org/index.php?option = com_k2&view = item&task = download&id = 2118_ba29368d4a62b7b36938b845a174394d&lang = en.
- 16. World Health Organization. Violence Info. Homicide, WHO Global Health Estimates (2015 update) [Internet]. Geneva: Switzerland, World Health Organization; 2018. Available from: http://apps.who.int/violence-info/homicide/
- 17. World Health Organization. Violence Info. Country Profiles, Iraq [Internet]. Geneva: Switzerland, World Health Organization; 2015. Available from: http://apps.who.int/violence-info/country/IQ.
- 18.GBD. Mortality and Causes of Death Collaborators Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2015;388(1005):1459. doi: 10.1016/S0140-6736(16)31012-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mandil A, Chaaya M, Saab D. Health status, epidemiological profile and prospects: eastern Mediterranean region. Int J Epidemiol. 2013;42(2):616–626. doi: 10.1093/ije/dyt026. [DOI] [PubMed] [Google Scholar]
- 20.Olawale OA, Owoaje ET. Incidence and pattern of injuries among residents of a rural area in South Western Nigeria: a community-based study. BMC Public Health. 2007;7:246. doi: 10.1186/1471-2458-7-246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cardona M, Joshi R, Ivers RQ, Iyengar S, Chow CK, Colman S et al. The burden of fatal and non-fatal injury in rural India. Inj Prev. 2008;14(4):232–237. doi: 10.1136/ip.2007.018259. [DOI] [PubMed] [Google Scholar]
- 22.Navaratne KV, Fonseka P, Rajapakshe L, Somatunga L, Ameratunga S, Ivers R et al. Population based estimates of injuries in Sri Lanka. Inj Prev. 2009;15(3):170–175. doi: 10.1136/ip.2008.019943. [DOI] [PubMed] [Google Scholar]
- 23.Stewart KA, Groen RS, Kamara TB, Farahzad MM, Samai M, Cassidy LD et al. Traumatic injuries in developing countries: report from a nationwide cross-sectional survey of Sierra Leone. JAMA Surg. 2013;148(5):463–469. doi: 10.1001/jamasurg.2013.1341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.El Tayeb SE, Abdalla S, Mørkve O, Heuch I, Van den Bergh G. Injuries in Khartoum state, the Sudan: a household survey of incidence and risk factors. Int J Inj Control Saf Promot. 2014;21(2):144–153. doi: 10.1080/17457300.2013.792283. [DOI] [PubMed] [Google Scholar]
- 25.Petroze RT, Joharifard S, Groen RS, Niyonkuru F, Ntaganda E, Kushner AL et al. Injury, disability and access to care in Rwanda: results of a nationwide cross-sectional population study. World J Surg. 2015;39(1):62–69. doi: 10.1007/s00268-014-2544-9. [DOI] [PubMed] [Google Scholar]
- 26.Haagsma JA, Graetz N, Bolliger I, Naghavi M, Higashi H, Mullany EC et al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj Prev. 2016;22(1):3–18. doi: 10.1136/injuryprev-2015-041616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mahran DG, Farouk O, Qayed MH, Berraud A. Pattern and trend of injuries among Trauma Unit Attendants in Upper Egypt. Trauma Mon. 2016;21(2):e20967. doi: 10.5812/traumamon.20967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Khaji A, Ghodsi SM, Eftekhar B, Karbakhsh M. Trauma research in Iran: a report of the Sina trauma data bank. Arch Iran Med. 2010;13(1):17–20. [PubMed] [Google Scholar]
- 29.Leidman E, Maliniak M, Sultan AS, Hassan A, Hussain SJ, Bilukha OO. Road traffic fatalities in selected governorates of Iraq from 2010 to 2013: prospective surveillance. Confl Health. 2016;10(2):2. doi: 10.1186/s13031-016-0070-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.World Health Organization. Geneva: Switzerland: World Health Organization; 2015. Global status report on road safety [Internet] [Google Scholar]
- 31.World Health Organization. Geneva: Switzerland: World Health Organization; 2018. Violence and injury prevention/road safety status. Ctry Profiles, Iraq [Internet] [Google Scholar]
- 32.Stewart BT, Lafta R, Cherewick M, Esa Al Shatari SA, Flaxman AD, Hagopian A et al. Road traffic injuries in Baghdad from 2003 to 2014: results of a randomised household cluster survey. Inj Prev. 2016;22(5):321–327. doi: 10.1136/injuryprev-2015-041707. [DOI] [PubMed] [Google Scholar]
- 33.Bener A, Abdul Rahman YS, Abdel Aleem EY, Khalid MK. Trends and characteristics of injuries in the State of Qatar: hospital-based study. Int J Inj Control Saf Promot. 2012;19(4):368–372. doi: 10.1080/17457300.2012.656314. [DOI] [PubMed] [Google Scholar]
- 34.Stewart BT, Lafta R, Esa Al Shatari SA, Cherewick M, Flaxman A, Hagopian A et al. Fall injuries in Baghdād from 2003 to 2014: results of a randomized household cluster survey. Injury. 2016;47(1):244–249. doi: 10.1016/j.injury.2015.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Rybarczyk MM, Schafer JM, Elm CM, Sarvepalli S, Vaswani PA, Balhara KS et al. A systematic review of burn injuries in low- and middle-income countries: epidemiology in the WHO-defined African Region. Afr J Emerg Med. 2017;7(1):30–37. doi: 10.1016/j.afjem.2017.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Othman N, Kendrick D. Epidemiology of burn injuries in the east Mediterranean Region: a systematic review. BMC Public Health. 2010;10:83. doi: 10.1186/1471-2458-10-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stewart B, Lafta RK, Al Shatari SA, Cherewick M, Burnham G, Hagopian A et al. Burns in Baghda¯d from 2003-2014: results of a randomized household cluster survey. Burns J Int Soc Burn Inj. 2016;42(1):48–55. doi: 10.1016/j.burns.2015.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lafta R, Aflouk NA, Dhiaa S, Lyles E, Burnham G. Needs of internally displaced women and children in Baghdad. Karbala, and Kirkuk, Iraq. Plos Curr. 2016:8. doi: 10.1371/currents.dis.fefc1fc62c02ecaedec2c25910442828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bataineh ZA, Al Quran TM, Al Balas H, Khammash MR. Pattern of burn injury at north of Jordan. Int J Burns Trauma. 2018;8(1):1–5. [PMC free article] [PubMed] [Google Scholar]
- 40.Golshan A, Patel C, Hyder AA. A systematic review of the epidemiology of unintentional burn injuries in South Asia. J Public Health. 2013;35(3):384–396. doi: 10.1093/pubmed/fds102. [DOI] [PubMed] [Google Scholar]
- 41. World Health Organization. Conflict and humanitarian crisis in Iraq. Public health risk assessment and interventions [Internet]. Geneva: Switzerland, World Health Organization; 2014. Available from: http://who.int/hac/crises/irq/iraq_phra_24october2014.pdf.
- 42. Human Rights Watch. Escapees describe systematic rape. Yezidi survivors in need of urgent Care 2015. Iraq: institute of strategic and international studies [Internet]. Available from: https://www.hrw.org/news/2015/04/14/iraq-isis-escapees-describe-systematic-rape.