

Abstract
Background
Tension-type headache (TTH) decreases the ability to concentrate and function during daily activities in affected patients. As most patients with TTH exhibit forward head posture (FHP). Various interventions have been proposed to resolve TTH. However, research regarding the efficacy of these interventions remains lacking. The present study aimed to investigate the association between FHP and TTH, and to evaluate the efficacy of various intervention methods on headache symptoms and other clinical variables in patients with TTH induced by FHP.
Material/Methods
Participants were randomly allocated to 3 groups: biofeedback (BF, n1=21), manual therapy (MT, n2=20) and, stretching (ST, n3=21). Interventions were conducted 3 times per week for 4 weeks. Craniovertebral angle (CVA), electroencephalographic findings for attention, stress, and pressure-pain threshold (PPT), headache on activities of daily living (Henry Ford Headache Disability Inventory, HDI), and quality of life (QoL) assessments were obtained pre-intervention, post-intervention, and at the 2-week follow-up.
Results
The correlation between CVA and HDI after intervention (R2=0.324, P<0.001), and at 2-week follow-up (R2=0.115, P<0.01) are significant. BF was associated with significant improvements in CVA (F2,59=3.393, P<0.001, ), attention (F2,59=5.186, P<0.01, ), stress [skin temperature (F2,59=6.005, P<0.001, ) and skin conductance (F2,59=4.900, P<0.01, )], PPT (F2,59=5.050, P<0.01, ), HDI (F2,59=3.303, P<0.01, ), and QoL (F2,59=3.409, P<0.05, ).
Conclusions
Our findings indicate that BF was more effective than MT and ST in the treatment of TTH due to FHP. Such findings highlight the need to develop and promote a controlled exercise program to facilitate a return to normal daily activities in patients with TTH due to FHP.
MeSH Keywords: Attention; Quality of Life; Stress, Physiological; Tension-Type Headache
Background
Headache is a very common condition that most people experience at least once in their lifetimes. Headache refers to the pain accompanied by discomfort in the face, neck and the head [1]. Approximately 80% of patients with headaches experience difficulty engaging in daily activities, and research has indicated that the incidence of headache accompanied by sleep disorders, depression, or anxiety continues to increase [2].
Among the representative types of headaches, tension-type headache (TTH) is the most common type in adults, with a reported prevalence between 36% to 78% [3]. Approximately 14% of adults experience TTH at least once per week, although symptoms occur almost every day in 3% of adult patients [1]. In affected patients, TTH occurs at a frequency of at least once per month and may be accompanied by moderate-to-severe sensations of pressure, with pain persisting from 30 minutes to 7 days [4]. Similar to migraine, TTH can be characterized as either episodic or chronic, although TTH does not present with nausea or vomiting [4]. Although various factors are likely involved, research has suggested that pathophysiological changes in muscular activity play a role in the development of TTH [5]. In accordance with this finding, abnormal spasms of the scalp and neck muscles have been observed in 70% of patients who experience TTH [6].
Abnormal muscle spasms can result from improper posture or abnormalities in posture regulation [7]. Forward head posture (FHP) represents the most common posture abnormality in adults and several studies have demonstrated an association between TTH and FHP [3,8]. FHP refers to the anterior displacement of the head relative to the trunk via upper cervical extension and lower cervical flexion [9]. Previous studies have reported that patients with FHP exhibit weakness in the extensor (suboccipital, semispinalis, splenius, and upper trapezius) and flexor muscles (longus colli, longus capitus, rectus capitis anterior) of the neck, as well as shortening of the sternocleidomastoid muscle [10]. Such changes lead to increased pressure between the cervical vertebrae and the development of tender points within the neck region. A study by Fernández-de-las-Peñas et al. [11] reported that all patients with TTH exhibit tender points over the suboccipital muscle, and that these tender points are associated with referred pain in the occipital and temporal regions.
Several studies have demonstrated a correlation between TTH and stress. A study by Kroll et al. [12] reported that stress exacerbates TTH pain and decreases physical activity, while additional studies have demonstrated that TTH is associated with decreased quality of life (QoL) [13] and increased levels of depression [14]. Despite the substantial health-related and socioeconomic impact of TTH, there is little evidence of effective interventions for reducing TTH.
Most previous studies regarding TTH have focused on reducing tender points over the contracted muscle caused by FHP through acupuncture [15], relaxation or manual therapy [5,16]. However, these methods provide only temporary relief and have demonstrated limited efficacy in improving posture and reducing TTH symptoms. Recently, in an effective way to FHP, Cervical sensory biofeedback training lead to a nearly 50% reduction in headache activity [8]. Biofeedback is improvement rates are similar for each treatment modality but substantially greater than those observed in untreated patients or patients with false or non-contingent biofeedback. And cervical sensory biofeedback can improve neuromuscular balance, postural alignment, increase functional mobility, and actively reduce pain [8,17].
Therefore, the present study aimed to develop a TTH more effective treatment program focused on improving posture in patients with FHP correlation, and to investigate the effects of various treatment methods on levels of attention, stress, and QoL in patients with TTH.
Material and Methods
Experimental design
Participants were divided into 3 groups based on the method of postural improvement: biofeedback group (BF), manual therapy group (MT), and stretching exercise group (ST), which was conducted in sessions of 20 to 30 minutes, 3 times per week. Each participant was randomly assigned to a group using the Random Allocation Software program for Windows 2.0 (Isfahan University, Iran). To determine the consistency of the effects based on elapsed time, patients were re-evaluated at the 2-week follow-up. The craniovertebral angle (CVA) was measured to investigate the correlation between changes in FHP and headache symptoms (primary outcome). Secondary outcomes included changes in clinical factors known to influence headache (e.g., attention, stress, and pressure threshold). In addition, we examined whether TTH relief was associated with changes in QoL. The protocol of the present study was approved by the Institutional Review Board of our university.
Patients
A total of 508 participants were recruited from among university students in G-city, all of whom met the requirements for initial selection. All participants had completed headache surveys and had been informed that they could withdraw from the study at any time. In order to identify participants with both headache and FHP, CVA measurements were obtained in accordance with the methods proposed by De et al. [18]. Participants with a CVA of 49° or below were considered to exhibit FHP [19]. TTH was defined based on the classification criteria outlined by the International Headache Society [4]. Inclusion criteria were as follows: 1) presence of 2 or more of the following: bilateral headache, pressure or squeezing pain, mild or intermediate pain intensity, and headache not elicited by daily physical activities; 2) less than 180 headache days per year or 15 headache days per month; 3) headache lasting between 30 minutes and 7 days; 4) headache unaccompanied by nausea or vomiting; 5) absence of photophobia or phonophobia during headache. Exclusion criteria were as follows: 1) headache onset greater than 6 months prior to initiation of the study; 2) receipt of headache or neck-related treatments within the past year; 3) use of headache medication or analgesics within the past 3 months; 4) history of injection treatments, surgery, severe cervical disc herniation, or fracture that may have influenced the intervention. A total of 508 consecutive patients were screened for study eligibility. Among them, 172 participants with CVA values above 49°, 128 participants who did not satisfy TTH eligibility criteria, 39 participants who had met additional exclusion criteria, and 107 patients who could not participate were excluded. A final total of 62 participants (26 male and 36 female) provided written informed consent and were included in the study. Sixty-two patients with TTH (mean age: 22.15±2.56 years; age range: 19–29 years; 67.1% female; headache time: 9.39 ± 2.81 weeks/year; range: 4–15 weeks; CVA: 47.34°±0.84°) satisfying the eligibility criteria agreed to participate and were randomly assigned to the biofeedback (n1=21), manual therapy (n2=20), and stretching (n3=21) groups.
The pretest demographic and self-report values for each treatment group are shown in Table 1.
Table 1.
The pretest demographic and self-report variables for each treatment group (N=62).
| BFG (n1=21) | MTG (n2=20) | STG (n3=21) | F/χ2 (P) | |
|---|---|---|---|---|
| Age (year) | 22.91 (2.84) | 21.40 (2.47) | 22.10 (2.39) | 1.824 (0.170) |
| Sex (Male/Female) | 7/14 | 6/14 | 6/15 | 2.052 (0.358) |
| Height (cm) | 167.99 (7.20) | 166.98 (9.18) | 166.74 (8.77) | 0.131 (0.878) |
| Weight (kg) | 60.24 (10.85) | 61.77 (13.05) | 61.47 (11.72) | 0.096 (0.909) |
| CVA(deg) | 47.53 (0.83) | 47.17 (0.80) | 47.29 (0.84) | 0.969 (0.385) |
| Headache time (wk/yr) | 9.38 (2.69) | 9.75 (2.73) | 9.05 (3.09) | 0.312 (0.733) |
Values are presented as mean (SD). BFG – biofeedback group; MTG – manual therapy group; STG – stretching group.
Sample size
The sample size was determined based on the large effect size (Cohen’s d: 0.47) reported in a previous study [3]. The calculations were then modified to fit the present study, resulting in an effect size of f(V) = 0.235. The effect size was calculated using G-power version 3.1 (Franz Faul, Universitiat Kiel, Germany). As the experimental design included 3 groups and 3 measurements, the sample size was calculated based on the following parameters: repeated-measures ANOVA, within-between interaction, α err prob: 0.05, power (1-β err prob): 0.80. This calculation resulted in a required sample size of 39 participants. Considering the dropout 10% rate, we included additional participants in the present study. Figure 1 depicts the flow diagram of participant selection.
Figure 1.

Flowchart according to the CONSORTS tatement for reporting randomizedrials.
Intervention
Biofeedback exercise
In accordance with the suggestions of Fernández-de-las-Peñas et al. [3] and Castien et al. [8], biofeedback exercise (Figure 2A) sessions were conducted by placing airbags inflated to 20 mmHg under the occipital bone. Participants were asked to exert pressure on the airbag by extending the chin. The pressure sensor of the device was observed to adjust the pressure by itself (Figure 2B). This motion results in contraction of the deep neck flexors (DNF) of the cervical spine. During the intervention, the pressure of the inflated bag was gradually increased to 30 mmHg by increments of 2 mmHg (Figure 2B). Thus, participants underwent a series of exercises at 22 mmHg, 24 mmHg, 26 mmHg, 28 mmHg, and 30 mmHg. Based on the progressive overload principle (Table 2). Participants rested 1 minute between each set, resulting in a total session length of approximately 13 minutes.
Figure 2.

Inflatable air-filled pressure sensor (A) and position of the patients during the exercise (B). Patient-specific criteria; craniovertebral angle, <49°.
Table 2.
Biofeedback programs.
| Intensity | Time | Methods | |
|---|---|---|---|
| 1st week | 22–26 mmHg | 3 set, 20 repeats | Concentric and eccentric contractions (3 sec) |
| 2st week | 22–26 mmHg | 3 set, 15 repeats | Concentric (3 sec) and isometric contractions (5 sec), eccentric, contractions (3 sec) |
| 3st week | 26–30 mmHg | 3 set, 20 repeats | Concentric and eccentric contractions (3 sec) |
| 4st week | 26–30 mmHg | 3 set, 15 repeats | Concentric (3 sec) and isometric contractions (5 sec), eccentric, contractions (3 sec) |
Manual therapy
In accordance with the suggestions of Monzani et al. [20] and Cho et al. [21], manual therapy was conducted using myofascial inhibitory (IT) and articulatory techniques (AT). The IT method aims to alleviate muscle spasms, which occur in patients with both TTH and FHP. IT treatment was applied to the soft tissue below the occipital region of the head, over the occiput-atlas-axis joint. Treatments were performed with the patient in the supine position, with the patient’s eyes closed and head resting in the therapist’s hands. The therapist reached his or her fingertips towards the arch behind the atlas, such that the patient’s head appeared to be hanging in the therapist’s hands. To reach the target muscle fibers, pressure was increased in a vertical fashion and applied until the therapist had detected a decrease in muscle tone. IT treatment was performed for 10 minutes, during which the therapist focused on cranio-cervical muscle tone.
The AT method has been used to improve disability of the neck joint and restore movement among the occiput, atlas, axis, and upper thoracic joints. AT treatment was performed in 2 stages with patients in the supine position, with each session lasting for 5 minutes. In the first stage, a slight rotation was induced in order to identify the joint barrier following distraction. While maintaining this tension, joint mobilization was performed at the level of the T1–C6 and C0–C1–C2 vertebrae. The second stage consisted of short, high-frequency oscillations. Without flexion or slight bending of the neck, the skull was rotated along the vertical axis. IT and AT treatments (10 minutes each) were conducted 3 times per week, respectively.
Stretching exercise
The stretching methods used in the present study were developed based on those described by Ylinen et al. [22]. In order to relax the pectoralis major and minor, scalene, sternocleidomastoid (SCM), upper trapezius, and suboccipital muscles, mentioned in the study, sessions consisted of 3 types of chest stretches and 3 types of neck stretches. While standing within a doorframe with their shoulders abducted to 90° and 120°, patients leaned forward using their body weight to stretch the chest muscles. To stretch the pectoralis minor, patients interlocked the fingers of both hands behind their back, resulting in retraction and depression of the scapula. The SCM was stretched via neck extension, contralateral flexion, and ipsilateral lateral rotation. In addition, lateral flexion of the upper trapezius muscle, ipsilateral flexion and rotation of the scalene muscle, and flexion of the extensor muscles were performed for 10 seconds each, followed by 5 seconds of rest. Extension of muscles in the neck region was performed bilaterally. Each set consisted of these 6 consecutive motions. During weeks 1–2, participants performed 10 sets per session, each of which lasted 25 minutes. Sessions were conducted 3 times per week, and participants were instructed to stretch to the greatest extent possible during each session. Muscle extensions were preceded and followed by light tapping of the neck and the shoulder using both hands. During weeks 3–4, a hold/relaxation phase was added to the end of the protocol used during weeks 1–2. To prevent muscle fatigue, the hold/relaxation phase was set to a maximum of 10 seconds. Each 10-second phase was composed of 2 seconds of concentric contraction, 6 seconds of hold, and 2 seconds of eccentric contraction.
Outcome measures
Forward head posture
Based on study by De-La-Llave-Rincón et al. [18], FHP was determined by measuring CVA. Participants were asked to sit facing forward with their arms placed naturally in their lap and neck held in the most comfortable position, while wearing clothing that exposed C7. Photographs of the C7 region (side view) were then obtained using a smartphone camera (Galaxy Note 5, Samsung, Korea). The camera was placed in a fixed location to ensure that all photos were taken at an identical distance. A goniometer was used to measure CVA on the printed images. The angle between the line from the outer bound of the tragus of the ear to the C7 vertebrae was measured. All efforts were made to ensure CVA was measured under identical conditions for each participant (Figure 3). According to reports by Subbarayalu [23] this method has an intra-class correlation coefficient (ICC) of 0.87, indicative of high reliability. Lower CVA values indicate advanced progression of FHP, which was defined as a CVA below 49°, based on the findings previous studies [19].
Figure 3.
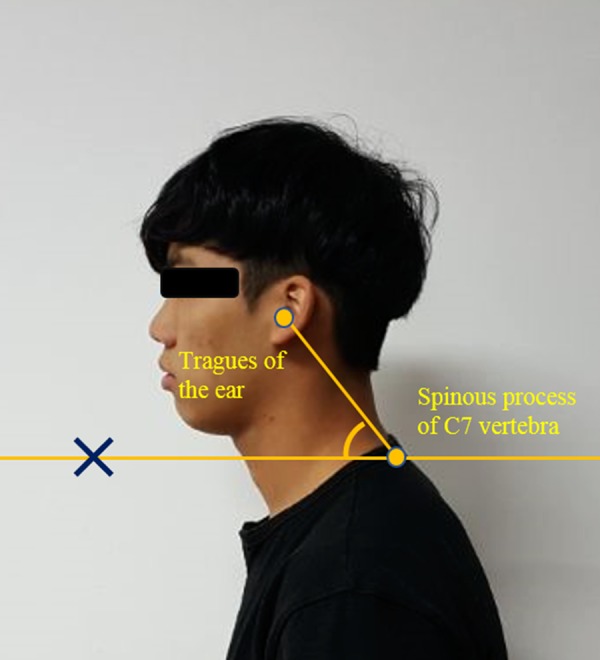
The craniovertebral angle was assessed directly from a side-view picture using a protractor and a straight edge.
Impact of headache on activities of daily living
To determine the impact of headache on activities of daily living, participants were asked to complete the Henry Ford Headache Disability Inventory (HDI). The HDI based on responses to 25 items associated with the functional and sensory aspects of headache experiences. Responses were scored as follows: yes, 4 points; sometimes, 2 points; no, 0 points. Overall scores were obtained by adding the point values for each of the 25 items, with higher scores indicate of more severe headache [24]. Previous studies have demonstrated that the HDI exhibits high test-retest reliability (Cronbach’s alpha: 0.94, Pearson correlation coefficient: 0.83) [25].
Attention
Electroencephalography (EEG; Pro-Comp Infiniti, Thought Technology, Canada) was used to assess levels of attention in each participant. Electrodes were placed in accordance with the international 10–20 system, with an effective frequency range of 1–40 Hz (unit: μV).
Monopole derivation was performed using the earlobe electrode, where EEG signals are not readily detected, as the reference for EEG measurement. In this method, several channels are combined into a single reference power to measure the absolute EEG activity from all channels [26].
To ensure the stability of measurements, participants to rest in the measurement facility for 10 minutes prior to assessments. The temperature and humidity of the testing environment were held constant for all participants, and levels of noise were minimized. Participants were asked to wear a blindfold during measurement to avoid the influence of visual stimulation (Figure 4). EEG recording was initiated when at least 10 second of stable EEG signals without artifacts were detected. The resistance of all electrodes (diameter: 8 mm; gold-plated) was set to less than 5 kΩ. To minimize the contact resistance on the skin, the forehead was wiped with cotton dipped in alcohol prior to fixation of the electrodes using gel and conductive grease (ElefixZ-401CE, Japan). Data were recorded for 20 minutes, although EEG was repeated the following day if participants stated that they had fallen asleep or experienced any changes in psychological state due external influences during the session. Previous studies have revealed that decreases in theta band activity (4–8 Hz) are observed during attentive states, along with increases in sensory motor rhythm (SMR and low-beta: 12–15 Hz) and middle-beta activity (15–22 Hz) [27]. Therefore, in the present study, we calculated the ratio of theta to SMR and middle-beta wave activity in order to investigate levels of attention [27]. The ratio is given by the following equation (1):
Figure 4.
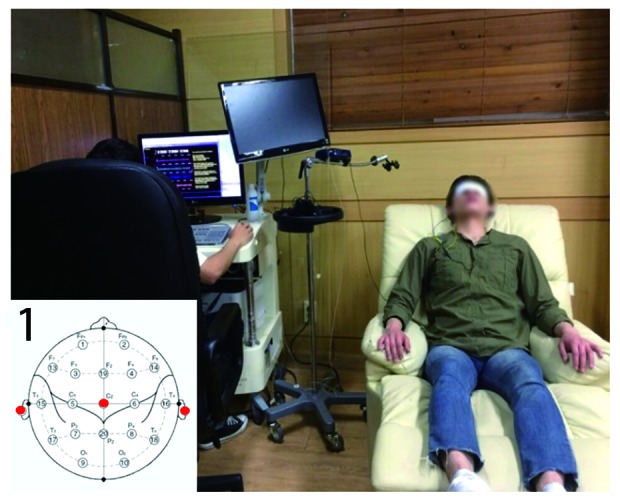
Eletroencephalogram and position of electrode placement (1).
| (1) |
EEG electrodes were placed in accordance with a method commonly used in neurofeedback experiments (Cz, A1, A2). The placement locations are shown in Figure 4(1) [28].
Stress
Increased levels of stress are accompanied by increases in respiration rate, heart rate, skin temperature, and skin conductance [29]. Therefore, in the present study, we evaluated levels of stress using an eight-channel, multi-modality Pro-Comp Infiniti biofeedback system, which was equipped with Biograph version 5.0 (Biofeedback, Thought Technology Ltd., Canada) for signal processing (Figure 5). This system exhibits sufficient power and flexibility for real-time, computerized biofeedback and data acquisition in a clinical setting.
Figure 5.

Stress measurement device and sensor: device (1), heart rate (A), skin conductance (B), skin temperature (C), and respiratory rate (D) sensor.
To minimize contact resistance with the skin, the sensors were wiped with cotton dipped in alcohol. As in previous experiments, participants were allowed to rest at the measurement facility for 10 minutes prior to recording. The temperature and humidity of the testing environment were held constant for all participants, and levels of noise were minimized. Participants were asked to wear a blindfold during measurement to avoid the influence of visual stimulation.
Heart rate (HR) was measured by fixing the HR sensor (measurement unit: frequency/minute) to the middle finger of the right hand (Figure 5(A)), while skin conductance (SC) was measured by fixing the SC sensor (measurement unit: microsiemens, μS) to the index and ring finger of the right hand (Figure 5(B)). Skin temperature (ST) was measured by fixing a thermistor to the little finger of the right little (measurement unit: °C) (Figure 5(C)). Respiratory rate (RR) was measured using piezo belts (Figure 5(D)). All physiological measurements were automatically recorded and stored by the biofeedback system.
Pressure pain thresholds
In the present study, we used a Commander Algometer TM device (J Tech Medical Industries, USA) to measure pressure-pain thresholds (PPTs) for each participant, in accordance with the methods proposed by Palacios-Cena et al. [30]. This algometer, which measures applied pressure in pounds (lb), is composed of a probe (10 x 10 mm), handle, and display screen. The desired location and placement of the algometer were confirmed with the participant in a relaxed, prone position. The central portion of the algometer was held by the experimenter for stability, and the pressure applied to the participant was gradually increased over the suboccipital muscle [11], near the headache region. Prior to measurement, participants were instructed to say “ah” when the pressure applied to the tender point produced pain. Previous studies have demonstrated that this method exhibits high test-retest reliability (R: 0.99) [31].
Quality of life (QoL)
The Headache Impact Test 6 (HIT-6) was used to evaluate the effect of various types of headache on QoL (e.g., TTH, migraine). The HIT-6 was created by the developers of the Short-form 36, based on items included on internet-based headache impact questionnaires, the Migraine Disability Assessment Scale (MIDAS), and migraine-specific QoL questionnaires. A total of 54 questions from the questionnaires and 35 questions from clinical assessments were selected based on content, relevance, item response theory, internal consistency, clinical relevance, contribution to total score, and linguistic analysis. The final questionnaire is composed of 6 questions related to pain, social function, role function, cognitive function, psychological pain, and activity [32]. Total scores on the HIT-6 range from 36–78 points, and participant responses are scored as follows: never, 6 points; rarely, 8 points; sometimes, 10 points; often, 11 points; always, 13 points. Scores of 49 or lower indicate no impact of headache on QoL, while scores of 50–55 indicated a mild impact on QoL. Scores of 56–60 indicate significantly reduced QoL due to headache, while scores of 60 or above indicate severely reduced QoL due to headache [32].
Previous studies have demonstrated that the HIT-6 exhibits high internal consistency (Cronbach’s alpha: 0.89) and test-retest reliability (ICC: 0.80) [32].
Statistical analysis
Data analyses were performed using SPSS (Version 18.0; SPSS Inc., Chicago, IL, USA) statistical software. Baseline demographic variables and scores on the self-report measures were compared between treatment groups via one-way analysis of variance (ANOVA) for continuous data and chi-square tests of independence for categorical data.
For the effects of treatment on various outcomes, primary outcome for a linear regression model (CVA and HDI) was used on the correlation between FHP and TTH. Secondary outcome for the effects of treatment on FHP, attention, stress, PPTs, ADL, and QoL were examined via 2-way repeated-measures ANOVA. For each ANOVA, 2-way (group x times) interactions were regarded as hypotheses of interest. Interactions were analyzed based on simple main effects for the between-group differences at each measurement point, with a Bonferroni-corrected α of 0.017 (3-point one-way ANOVA tests). Data were analyzed using 2 different approaches. First, an intention-to-treat (ITT) analysis was performed for all patients originally randomized in the trial. Missing data points for dropouts were imputed using the last-observation-carried-forward method. In addition, we analyzed only the data of those participants who had completed the trial (i.e., per-protocol analysis). Partial eta squared () was calculated to investigate the effect size based on treatment type. The level of statistical significance for all analyses was set to α=0.05.
Results
In the ITT analysis of primary outcomes, a significant correlation between increases in CVA and decreases in HDI was observed, with an explanatory power of 32.4%. This correlation remained significant during the 2-week follow-up period (R2=0.339, P=0.007), with an explanatory power of 11.5%. The result of the 3-point (pre-intervention to post-intervention; post-intervention to 2-week follow-up) and regression analyses are displayed in Table 3.
Table 3.
Mediation analysis (influence of tension type headach by increase of craniovertebral angle): results of linear regression Analysis (N=62).
| BFG (n1=21, A) | BFG (n2=20, B) | STG (n3=21, C) | ||||
|---|---|---|---|---|---|---|
| Base – follow up | fw – 2wk fw | Base – follow up | fw – 2wk fw | Base – follow up | fw – 2wk fw | |
| CVA (deg) | 2.66 (2.76) | 1.59 (3.72) | 2.40 (1.86) | −0.24 (1.75) | 1.16 (1.70) | −1.67 (1.65) |
| HDI (point) | 7.05 (6.53) | 2.48 (2.36) | 8.40 (6.12) | −1.30 (2.54) | 4.95 (6.92) | −0.714 (3.39) |
| Mediation analysis: results of linear regression analysis | ||||||
| Independent variable | R2 | F | Coefficient | |||
| B | t [95% CI] | |||||
| Constant | 0.324 | 28.720*** | ||||
| Base to fw | 0.187 | 5.043 [0.113–0.261]*** | ||||
| Constant | 0.115 | 7.792** | ||||
| fw to 2wk fw | 0.280 | 2.791 [0.079–0.481]** | ||||
Values are presented as mean (SD). BFG – biofeedback group; MTG – manual therapy group; STG – stretching group; CVA – Craniovertebral angle; HDI – Henry Ford headache disability inventory. Regression model change of CVA according to HDI (base to fw, fw to 2wk fw), CI – confidence interval.
P<0.01;
P<0.001.
In the ITT analysis of secondary outcomes, a significant effect of the interaction between time and group was observed on CVA (, indicative of a moderate group effect), attention (, indicative of a large group effect), PPTs (, indicative of a large group effect), HDI scores (, indicative of a moderate group effect), HIT-6 scores (, indicative of a moderate group effect). Significant differences in CVA, attention, HDI scores, and HIT-6 scores were also observed among the 3 points at the 2-week follow-up, while significant differences in PPT were observed among the 3 points post-intervention and at the 2-week follow up.
No significant time-by-group difference in HR was identified (, indicative of a moderate group effect). Significant differences were observed among the 3 points at the 2-week follow-up. However, significant time-by-group effects were observed with regard to ST (, indicative of a large group effect) and SC (, indicative of a large group effect). Significant differences in ST and SC were observed among the 3 points at the 2-week follow-up. However, no significant time-by-group difference in RR was identified (, indicative of a small group effect). No significant differences in RR were observed among the 3 points.
Patient values for pre-intervention, post-intervention, and 2-week follow-up assessments are displayed in Table 4.
Table 4.
Each therapy participants: potential mediators at pretest and 4 weeks and outcome after treatment by 2 Weeks (N=62).
| BFG (n1=21, A) | MTG (n2=20, B) | STG (n3=21, C) | Time×group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | 2wk fw | Pre | Post | 2wk fw | Pre | Post | 2wk fw | F [95% CI] | ||
| CVA (deg) | 47.53 (0.83) | 49.61 (2.73) | 51.20 (2.37)ac | 47.17 (.80) | 49.57 (1.58) | 49.33 (1.78) | 47.29 (0.84) | 48.46 (1.43) | 48.29 (1.36) | 3.393 [48.458–48.977]** | 0.130 |
| Attention (mV) | 1.74 (1.16) | 2.84 (1.35) | 4.15 (1.79)c | 1.84 (0.82) | 2.86 (1.35) | 2.97 (1.07) | 1.49 (0.74) | 2.66 0 (.88) |
2.28 (0.93) | 5.186 [2.327–2.751]** | 0.150 |
| PPT (lb) | 18.14 (1.31) | 19.54 (2.32) | 21.36 (2.28)c | 18.56 (1.55) | 20.91 (3.20)b | 19.71 (2.17) | 17.80 (1.24) | 18.53 (1.79) | 18.43 (1.58) | 5.050 [18.873–19.567]** | 0.146 |
| HDI (point) | 79.91 (3.49) | 68.86 (6.14) | 66.38 (5.81)c | 78.50 (4.63) | 70.10 (6.02) | 71.40 (6.35) | 77.57 (3.22) | 72.62 (6.74) | 73.33 (5.15) | 3.303 [71.622–73.859]** | 0.101 |
| HIT6 (point) | 53.47 (2.42) | 50.52 (2.94) | 49.05 (51.75)ac | 53.55 (2.24) | 51.10 (2.83) | 51.75 (2.86) | 54.76 (1.92) | 52.86 (2.17) | 52.91 (2.14) | 3.409 [51.734–52.704]* | 0.104 |
| Stress | |||||||||||
| HR (bpm/min) | 77.48 (1.79) | 76.38 (1.62) | 74.99 (1.95) | 78.35 (1.96) | 77.09 (1.52) | 76.03 (1.67) | 78.22 (1.66) | 77.50 (1.82) | 76.69 (1.81) | 2.433 [76.491–77.225] | 0.076 |
| ST (°C) | 33.65 (0.53) | 33.56 (0.61) | 32.79 (0.58)ac | 33.63 (0.58) | 33.58 (0.60) | 33.45 (0.63) | 33.66 (0.54) | 33.69 (0.63) | 33.68 (0.52) | 6.008 [33.382–33.614]*** | 0.169 |
| SC (μs) | 0.84 (0.45) | 0.81 (0.04) | 0.79 (0.06)c | 0.85 (0.03) | 0.83 (0.34) | 0.82 (0.05) | 0.85 (0.04) | 0.84 (0.05) | 0.84 (0.04) | 4.900 [0.820–0.839]** | 0.142 |
| RR (breath/min) | 14.48 (0.51) | 15.28 (0.51) | 15.26 (0.51) | 14.12 (0.75) | 14.65 (0.62) | 14.77 (0.46) | 13.69 (0.61) | 14.24 (0.53) | 14.18 (0.49) | 1.304 [14.399–14.638] | 0.042 |
Values are presented as mean (SD). BFG – biofeedback group; MTG – manual therapy group; STG – stretching group; CVA – craniovertebral angle; PPT – pressure-pain thresholds; HDI – Henry Ford headache disability inventory; HIT6 – headache impact test-6; SC – skin conductance; ST – skin temperature; RR – respiratory rate; HR – heart rate. – Partial Eta Squared; CI – confidence interval. Significant interaction time×group (* P<0.05; ** P< 0.01, *** P<0.001); Between-group differences at each point measurement Bonferroni correction (a P< 0.017: A>B, b P<.017: B>C, c P< 0.017: A>C).
Discussion
We aimed to investigate the correlation between decreases in FHP and TTH, and to determine the efficacy of various interventions in improving FHP. We further aimed to examine the effects of these treatments on attention, stress, tender points, headache symptoms, and QoL
Changes in TTH and CVA were significantly correlated post-treatment (R=0.569, P=0.000) and at the 2-week follow-up (R=0.339, P=0.007). A study by Fernández-de-las-Peñas et al. [8] reported that manual therapy reduced FHP, and that such decreases in FHP were associated with an 85% decrease in headache frequency (P<0.05). Furthermore, a study by César et al. [33] reported that decreases in CVA exacerbate TTH symptoms in affected patients when compared with healthy controls (P<0.001). Such findings suggest that TTH is caused by FHP-induced cervical musculoskeletal dysfunction.
In the present study, CVA was measured to investigate changes in FHP. Significant increases in CVA were observed following the intervention (F2, 59=3.393; P<0.001), although CVA values differed significantly between the BF and MT/ST groups at the 2-week follow-up (F2,59=3.393, P<0.017). A study by César et al. [3] demonstrated that patients with TTH exhibit significantly lower CVA values than healthy controls (P<0.01), and that weak DNF function was associated with increased TTH severity (P<0.001). However, Castien et al. [8] reported that patients with FHP exhibited significant increases in CVA following manual therapy. These results indicate that patients with TTH exhibit increases in FHP, which in turn weaken the DNFs and lead to cervical musculoskeletal dysfunction. The results of the present study suggest that patients of the BF group exhibited increases in CVA due to increased strength of the DNFs. Ylinen et al. [22] reported that significant changes in neck disability (P=0.013) and neck stiffness (P=0.01) occurred following 4 weeks of manual therapy and stretching in patients with neck pain. However, in accordance with the findings of the present study, no significant changes in neck disability and stiffness were observed at the 8-week follow-up, while symptoms had become exacerbated relative to pre-treatment conditions in some patients. In the present study, patients of the ST and MT groups received manual FHP alignment by a therapist, while those in the BF group were required to correct their own posture. Thus, patients of the BF group may have remembered the correct posture, even after some time had passed. In a study by Trewartha et al. [34] a significant difference in proprioceptive correction was observed between passive block-stacking training and active block-stacking training (P=0.007). The findings suggest that patients of the BF group improved their ability for proprioceptive correction to the proper posture via self-alignment.
In order to confirm whether TTH is associated with changes in attention levels, power ratios were obtained via EEG. EEG results indicated the presence of significant time-by-group effects (F2,59=5.186, P<0.01), and significant differences were observed between the BF and ST groups at the 2-week follow-up (F2,59=10.701, P<0.017). A study by Kuhajda et al. [35] examined attention levels in adult participants with headaches based on response time at encoding (word judgment task). In accordance with the findings of the present study, the authors reported that patients of the headache group exhibited significant decreases in attention relative to participants of the control group (P=0.008). Moreover, Carissa et al. [36] reported that the word count, which is used to evaluate attention, was significantly higher in participants of an upright posture group relative to that observed in a relaxed posture group (P=0.02). Another study by Zhavoronkova et al. [37] reported that upright body posture is associated with increased high-frequency brain activity (maximal power increase in the β-wave range). Similarly, our findings indicated that patients of the BF group were able to maintain the upright posture and increases in attention following treatment.
In the present study, we evaluated levels of stress by measuring HR, ST, SC, and RR. Although no significant differences in HR or RR were observed among the groups, significant differences were observed for ST (F2,59=6.005; P<0.001) and SC (F2,59=4.900; P<0.01). In addition, significant differences in ST were observed among the BF, MT, and ST groups at the 2-week follow-up (F2,59=13.605; P=0.000). Significant differences in SC were also observed between the BF and ST groups (F=7.705; P=0.001). A study by Roos et al. [38] reported that, as stress levels rise, increases in sympathetic nervous system activity produce increases in heart rate, respiration rate, temperature, and sweat production, thereby increasing SC. In a study of 12 988 Japanese patients, Yokoyama et al. [39] reported that increases in stress are proportional to increases in headache (P<0.0001). However, a study by Nair et al. [40] reported significant differences in heart rate and pulse pressure between an upright posture group and a slouching posture group (P=0.005), while additional research by Kraft and Pressman [41] indicated that an upright body posture is associated with decreases in HR. Chadha et al. [42] also observed that maintaining normal posture produces increases in thyroid stimulating hormone (TSH) secretion, while Hisar et al. [43] demonstrated that increases in thyroxine and cortisol levels following TSH secretion are significantly associated with stress relief. These findings suggest that the decreases in FHP and postural improvements observed in patients of the present study may have induced secretion of TSH, thereby leading to increases in thyroxine and cortisol levels and subsequent reductions in the level of stress.
A study by Palacios-Cena et al. [30] reported that myofascial trigger points (TrP) around the head and neck are more common in patients with TTH than in healthy controls. Moreover, a study by Fernández-de-las-Peñas et al. [11] reported a correlation between TTH and TrP of the suboccipital muscle, and that activation of TrP increases the frequency and intensity of TTH. To investigate changes in TrP activity in response to various interventions, we measured changes in suboccipital muscle PPTs on the affected side. Our analysis revealed a significant time-by-group interaction with regard to PPTs (F2,58=5.050, P<0.01). Fernández-de-las-Peñas et al. [11] reported that TrPs of the suboccipital muscle significantly increase along with increases in FHP (P<0.01). Similarly, we observed significant increases in FHP in patients of the present study (P<0.001). These findings suggest that decreases in PPT lead to FHP relief, consequently shortening the suboccipital muscle and reducing TrP activation. Nociceptive input from TrP of the suboccipital muscle can stimulate the afferent fibers of the trigeminal nerve nucleus caudalis [44]. Nociceptive input from the muscles surrounding C1–C3, including the suboccipital muscle, converge at the trigeminal nerve in the nucleus caudalis [44]. These findings indicate that repetitive nociceptive activation of the nucleus caudalis may result in central sensitization, potentially reducing the headache threshold in patients with TTH [45].
At each assessment point during the intervention of the present study, MT was more effective than BF and ST after intervention (F2.59=4.663; P<0.017). However, at the 2-week follow-up, BF was more effective than MT and ST (F2,59=10.904; P<0.017). A study by Jari et al. [22] reported that significant differences in neck disability (P=0.013) and neck stiffness (P=0.01) were occurred following 4 weeks of stretching and manual therapy. However, no significant differences were observed after 8 weeks. Boline et al. [46] reported that headache intensity (P=0.003) and frequency (P=0.004) had decreased in patients treated via chiropractic manipulation for 4 weeks, relative to those observed in patients treated with medication. Although the medication dosage in chiropractic group was reduced due to the observed improvements, after 4 weeks increases in headache intensity and frequency were observed following the intervention, necessitating increases in medication dosage. In a comparative study of patients treated via chiropractic adjustment or amitriptyline, Kassak et al. [47], reported that the chiropractic group exhibited decreased headache severity after 6 weeks of treatment. However, recurrence of headache 4 weeks after the end of the experiment required participants to resume amitriptyline treatment. These previous studies indicate that manual therapy and stretching exert no long-term effects following the intervention. Manual therapy involves direct manipulation of TrP and alignment of FHP. In contrast, participants engaging in BF treatment are trained to actively decrease FHP, increasing their ability to maintain the upright position long-term. In the present study, further increases in CVA were observed in the BF group at the 2-week follow-up. These results indicate that, although MT was more effective during the intervention period due to simultaneous manipulation of the joints and muscles, FHP returned at the 2-week follow-up. However, changes in CVA were maintained at follow-up in the BF group, likely due to reduced TrP activation associated with extension of the suboccipital muscle.
A study by Lai et al. [48] reported that presynaptic inhibition occurs on the agonist muscle when the antagonist muscles are contracted, which induces maintenance of correct posture. Suboccipital muscle is a representative upper cervical extensor muscle that can be considered an antagonist of the deep neck flexor. Based on the results, in can be inferred that BFG could maintain the CVA due to strengthening of the DNFs. Furthermore, the antagonist suboccipital could have contributed with presynaptic inhibition.
We utilized the HDI and HIT-6 to investigate the effects of headache on daily life QoL, respectively. Significant group-by-time effects were observed for both HDI (F2,59=3.303; P<0.01) and HIT-6 scores (F2,59=3.409; P<0.05). Two weeks after the intervention, significant decreases in HDI scores were observed in the BF and ST groups (F2,59=8.073; P<0.017), while significant decreases in HIT-6 were observed in the BF group, relative to values obtained for the MT and ST groups (F2,59=12.542; P<0.017). A study by Espi-Lopez et al. [13] reported that patients with headaches experience decreased QoL, based on responses obtained using Short Form-36, and that QoL was strongly influenced by the intensity of pain. Furthermore, a study by Penzien et al. [49] reported that 38% of patients with TTH are restricted in their ability to perform daily activities, while 4% face significant impairments at work. The authors also reported that friendship, school life, and family relationships are significantly affected in 8–9% of patients. These previous studies indicate that the decrease in TTH observed in the present study was due to decreases in FHP. Our results further suggest that decreases in TTH improve QoL and functioning during daily activities, and that BF is more effective than the other 2 methods for reducing FHP and TTH symptoms.
The present study is limited in that all participants were young adults belonging to a narrow age range. Future studies should include participants of a wider age range to improve the generalizability of the results.
Conclusions
Our findings indicated that FHP was significantly correlated with TTH, such that decreases in FHP production improved TTH. Moreover, improvements in TTH symptoms were associated with increased QoL and improvements in attention, stress, PPTs, ability to perform activities of daily living. Our findings suggest further demonstrated that alignment training via biofeedback was associated with significant improvements even after the intervention period. Thus, our findings may aid clinicians in determining the most effective treatment for improving symptoms and QoL in patients with TTH with significant functional and social limitations due to headache symptoms. Furthermore, the methods utilized in the present study can be adapted to treat FHP due to kyphosis in older adults.
Footnotes
Source of support: This work was supported by Sahmyook University and by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2017R1D1A1B03035018)
References
- 1.Falsiroli Maistrello L, Rafanelli M, Turolla A. Manual therapy and quality of life in people with headache: Systematic review and meta-analysis of randomized controlled trials. Current Pain Headache Rep. 2019;23(10):78. doi: 10.1007/s11916-019-0815-8. [DOI] [PubMed] [Google Scholar]
- 2.Macgregor EA. Headache in pregnancy. Continuum (Minneapolis, Minn) 2014;20(1):128–47. doi: 10.1212/01.CON.0000443841.40933.9e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fernández-de-las-Peñas C, Pérez-de-Heredia M, Molero-Sánchez A, Miangolarra-Page JC. Performance of the craniocervical flexion test, forward head posture, and headache clinical parameters in patients with chronic tension-type headache: A pilot study. J Orthop Sports Phys Ther. 2007;37(2):33–39. doi: 10.2519/jospt.2007.2401. [DOI] [PubMed] [Google Scholar]
- 4.Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders. Cephalalgia. 2004;24(1):1–160. [Google Scholar]
- 5.Liang Z, Galea O, Thomas L, et al. Cervical musculoskeletal impairments in migraine and tension type headache: A systematic review and meta-analysis. Musculoskelet Sci Pract. 2019;42:67–83. doi: 10.1016/j.msksp.2019.04.007. [DOI] [PubMed] [Google Scholar]
- 6.Ashina S, Bendtsen L, Lyngberg AC, et al. Prevalence of neck pain in migraine and tension-type headache: A population study. Cephalalgia. 2015;35(3):211–19. doi: 10.1177/0333102414535110. [DOI] [PubMed] [Google Scholar]
- 7.Nejati P, Lotfian S, Moezy A, Nejati M. The study of correlation between forward head posture and neck pain in Iranian office workers. Int J Occup Med Environ Health. 2015;28(2):295–303. doi: 10.13075/ijomeh.1896.00352. [DOI] [PubMed] [Google Scholar]
- 8.Castien R, Blankenstein A, van der Windt D, et al. The working mechanism of manual therapy in participants with chronic tension-type headache. J Orthop Sports Phys Ther. 2013;43(10):693–99. doi: 10.2519/jospt.2013.4868. [DOI] [PubMed] [Google Scholar]
- 9.Shaghayegh Fard B, Ahmadi A, Maroufi N, Sarrafzadeh J. Evaluation of forward head posture in sitting and standing positions. Eur Spine J. 2016;25(11):3577–82. doi: 10.1007/s00586-015-4254-x. [DOI] [PubMed] [Google Scholar]
- 10.Kocur P, Wilski M, Goliwas M, et al. Influence of forward head posture on myotonometric measurements of superficial neck muscle tone, elasticity, and stiffness in asymptomatic individuals with sedentary jobs. J Manipulative Physiol Ther. 2019;42(3):195–202. doi: 10.1016/j.jmpt.2019.02.005. [DOI] [PubMed] [Google Scholar]
- 11.Fernández-de-las-Peñas C, Alonso-Blanco C, Cuadrado ML, et al. Trigger points in the suboccipital muscles and forward head posture in tension-type headache. Headache. 2006;46(3):454–60. doi: 10.1111/j.1526-4610.2006.00288.x. [DOI] [PubMed] [Google Scholar]
- 12.Kroll LS, Hammarlund CS, Westergaard ML, et al. Level of physical activity, well-being, stress and self-rated health in persons with migraine and co-existing tension-type headache and neck pain. J Headache Pain. 2017;18(1):46. doi: 10.1186/s10194-017-0753-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Espi-Lopez GV, Rodriguez-Blanco C, Oliva-Pascual-Vaca A, et al. Do manual therapy techniques have a positive effect on quality of life in people with tension-type headache? A randomized controlled trial. Eur J Phys Rehabil Med. 2016;52(4):447–56. [PubMed] [Google Scholar]
- 14.Palacios-Cena M, Fernandez-Munoz JJ, Castaldo M, et al. The association of headache frequency with pain interference and the burden of disease is mediated by depression and sleep quality, but not anxiety, in chronic tension type headache. J Headache Pain. 2017;18(1):19. doi: 10.1186/s10194-017-0730-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Santesso N, Wieland LS. A summary of a cochrane review: Acupuncture for the prevention of tension-type headache. Eur J Integr Med. 2016;8(4):324–25. doi: 10.1016/j.eujim.2016.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mesa-Jimenez JA, Lozano-Lopez C, Angulo-Diaz-Parreno S, et al. Multimodal manual therapy vs. pharmacological care for management of tension type headache: A meta-analysis of randomized trials. Cephalalgia. 2015;35(14):1323–32. doi: 10.1177/0333102415576226. [DOI] [PubMed] [Google Scholar]
- 17.Lee J, Kim D, Yu K, et al. Comparison of isometric cervical flexor and isometric cervical extensor system exercises on patients with neuromuscular imbalance and cervical crossed syndrome associated forward head posture. Biomed Mater Eng. 2018;29(3):289–98. doi: 10.3233/BME-181728. [DOI] [PubMed] [Google Scholar]
- 18.De-La-Llave-Rincón AI, Fernández-De-Las-PeÑas C, Palacios-CeÑa D, Cleland JA. Increased forward head posture and restricted cervical range of motion in patients with carpal tunnel syndrome. J Orthop Sports Phys Ther. 2009;39(9):658–64. doi: 10.2519/jospt.2009.3058. [DOI] [PubMed] [Google Scholar]
- 19.Nemmers TM, Miller JW, Hartman MD. Variability of the forward head posture in healthy community-dwelling older women. J Geriatr Phys Ther. 2009;32(1):10–14. doi: 10.1519/00139143-200932010-00003. [DOI] [PubMed] [Google Scholar]
- 20.Monzani L, Espí-López GV, Zurriaga R, Andersen LL. Manual therapy for tension-type headache related to quality of work life and work presenteeism: Secondary analysis of a randomized controlled trial. Complement Ther Med. 2016;25:86–91. doi: 10.1016/j.ctim.2016.01.008. [DOI] [PubMed] [Google Scholar]
- 21.Cho J, Lee E, Lee S. Upper thoracic spine mobilization and mobility exercise versus upper cervical spine mobilization and stabilization exercise in individuals with forward head posture: a randomized clinical trial. BMC Musculoskelet Disord. 2017;18(1):525. doi: 10.1186/s12891-017-1889-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ylinen J, Kautiainen H, Wirén K, Häkkinen A. Stretching exercises vs. manual therapy in treatment of chronic neck pain: A randomized, controlled cross-over trial. J Rehabil Med. 2007;39(2):126–32. doi: 10.2340/16501977-0015. [DOI] [PubMed] [Google Scholar]
- 23.Subbarayalu AV. Measurement of craniovertebral angle by the Modified Head Posture Spinal Curvature Instrument: A reliability and validity study. Physiother Theory Pract. 2016;32(2):144–52. doi: 10.3109/09593985.2015.1099172. [DOI] [PubMed] [Google Scholar]
- 24.Cottrell D. Handbook of neurologic rating scales. New York, NY: Springer Science & Business Media; 2007. [Google Scholar]
- 25.Jacobson GP, Ramadan NM, Aggarwal SK, Newman CW. The Henry Ford hospital headache disability inventory (HDI) Neurology. 1994;44(5):837–42. doi: 10.1212/wnl.44.5.837. [DOI] [PubMed] [Google Scholar]
- 26.Lugger K, Flotzinger D, Schlögl A, et al. Feature extraction for on-line EEG classification using principal components and linear discriminants. Med Biol Eng Comput. 1998;36(3):309–14. doi: 10.1007/BF02522476. [DOI] [PubMed] [Google Scholar]
- 27.Lubar JF. Discourse on the development of EEG diagnostics and biofeedback for attention-deficit/hyperactivity disorders. Biofeedback Self Regul. 1991;16(3):201–25. doi: 10.1007/BF01000016. [DOI] [PubMed] [Google Scholar]
- 28.Harner P, Sannit T. A review of the international ten-twenty system of electrode placement. West Warwick: Grass Instrument Company; 1974. [Google Scholar]
- 29.Norris SL, Lee C-T, Burshteyn D, Cea-Aravena J. The effects of performance enhancement training on hypertension, human attention, stress, and brain wave patterns: A case study. J Neurother. 2000;4(3):29–44. [Google Scholar]
- 30.Palacios-Cena M, Wang K, Castaldo M, et al. Trigger points are associated with widespread pressure pain sensitivity in people with tension-type headache. Cephalalgia. 2018;38(2):237–45. doi: 10.1177/0333102416679965. [DOI] [PubMed] [Google Scholar]
- 31.Kinser AM, Sands WA, Stone MH. Reliability and validity of a pressure algometer. J Strength Cond Res. 2009;23(1):312–14. doi: 10.1519/jsc.0b013e31818f051c. [DOI] [PubMed] [Google Scholar]
- 32.Kosinski M, Bayliss M, Bjorner J, et al. A six-item short-form survey for measuring headache impact: the HIT-6™. Qual Life Res. 2003;12(8):963–74. doi: 10.1023/a:1026119331193. [DOI] [PubMed] [Google Scholar]
- 33.Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML, Pareja JA. Forward head posture and neck mobility in chronic tension-type headache: A blinded, controlled study. Cephalalgia. 2006;26(3):314–19. doi: 10.1111/j.1468-2982.2005.01042.x. [DOI] [PubMed] [Google Scholar]
- 34.Trewartha KM, Case S, Flanagan JR. Integrating actions into object location memory: A benefit for active versus passive reaching movements. Behav Brain Res. 2015;279:234–39. doi: 10.1016/j.bbr.2014.11.043. [DOI] [PubMed] [Google Scholar]
- 35.Kuhajda MC, Thorn BE, Klinger MR, Rubin NJ. The effect of headache pain on attention (encoding) and memory (recognition) Pain. 2002;97(3):213–21. doi: 10.1016/S0304-3959(01)00488-2. [DOI] [PubMed] [Google Scholar]
- 36.Wilkes C, Kydd R, Sagar M, Broadbent E. Upright posture improves affect and fatigue in people with depressive symptoms. J Behav Ther Exp Psychiatry. 2017;54:143–49. doi: 10.1016/j.jbtep.2016.07.015. [DOI] [PubMed] [Google Scholar]
- 37.Zhavoronkova L, Zharikova A, Kushnir E, Mikhalkova A. EEG markers of upright posture in healthy individuals. Hum Physiol. 2012;38(6):604–12. [PubMed] [Google Scholar]
- 38.Roos LE, Knight EL, Beauchamp KG, et al. Acute stress impairs inhibitory control based on individual differences in parasympathetic nervous system activity. Biol Psychol. 2017;125:58–63. doi: 10.1016/j.biopsycho.2017.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Yokoyama M, Yokoyama T, Funazu K, et al. Associations between headache and stress, alcohol drinking, exercise, sleep, and comorbid health conditions in a Japanese population. J Headache Pain. 2009;10(3):177–85. doi: 10.1007/s10194-009-0113-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Nair S, Sagar M, Sollers J, III, et al. Do slumped and upright postures affect stress responses? A randomized trial. Health Psycho. 2015;34(6):632–41. doi: 10.1037/hea0000146. [DOI] [PubMed] [Google Scholar]
- 41.Kraft TL, Pressman SD. Grin and bear it: The influence of manipulated facial expression on the stress response. Psychol Sci. 2012;23(11):1372–78. doi: 10.1177/0956797612445312. [DOI] [PubMed] [Google Scholar]
- 42.Chadha C, Deshmukh M, Gugle AS. Study of thyroid function tests in cases of polymorphic light eruption in tertiary care institute. MVP Journal of Medical Sciences. 2018;5(1):101–3. [Google Scholar]
- 43.Hisar SA, Sahin T, Hisar O, Arslan G. Effects of low temperature and starvation on plasma cortisol, triiodothyronine, thyroxine, thyroid-stimulating hormone and prolactin levels of juvenile common carp (Cyprinus carpio) Mar Sci Tech Bull. 2015;4(2):5–9. [Google Scholar]
- 44.Bogduk N. The anatomical basis for cervicogenic headache. J Manipulative Physiol Ther. 1992;15(1):67–70. [PubMed] [Google Scholar]
- 45.Bendtsen L. Central sensitization in tension-type headache – possible pathophysiological mechanisms. Cephalalgia. 2000;20(5):486–508. doi: 10.1046/j.1468-2982.2000.00070.x. [DOI] [PubMed] [Google Scholar]
- 46.Boline PD, Kassak K, Bronfort G, et al. Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: A randomized clinical trial. J Manipulative Physiol Ther. 1995;18(3):148–54. [PubMed] [Google Scholar]
- 47.Kassak K, Anderson A, Assment P, Edina M. Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: A randomized clinical trial. J Manipulative Physiol Ther. 1995;3:148–54. [PubMed] [Google Scholar]
- 48.Lai AKM, Arnold AS, Wakeling JM. Why are antagonist muscles co-activated in my simulation? a musculoskeletal model for analysing human locomotor tasks. Ann Biomed Eng. 2017;45(12):2762–74. doi: 10.1007/s10439-017-1920-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Penzien DB, Rains JC, Andrasik F. Behavioral management of recurrent headache: 3 decades of experience and empiricism. Appl Psychophysiol Biofeedback. 2002;27(2):163–81. doi: 10.1023/a:1016247811416. [DOI] [PubMed] [Google Scholar]