

Abstract
Interatrial conduction disorders are frequent in patients with structural heart diseases, including hypertension, coronary disease, and hypertrophic cardiomyopathy, and they are strongly associated with atrial tachyarrhythmias, especially atrial fibrillation and flutter. Conduction delays lead to dispersion of refractory periods and participate in initiating and maintaining reentry circuits, facilitating atrial arrhythmias. In this case, the changing pattern over time is a manifestation of progressive atrial remodeling and conduction delay. The terminal negative component of the P wave in the inferior leads suggests block of the electrical impulse in the Bachman bundle zone, with retrograde activation of the left atria via muscular connections at the coronary sinus. This has been reproduced in experimental models and confirmed by endocardial mapping. Physicians should be aware of the association between advanced interatrial block and development of atrial arrhythmias as its recognition could prompt early and aggressive antiarrhythmic treatment.
Keywords: interatrial block, atrial fibrillation, atrial flutter
CASE PRESENTATION
A 48‐year‐old male with hypertensive cardiomyopathy presented successively with atrial fibrillation (AF), typical atrial flutter, and left atrial tachycardia over a 6‐year period to the Emergency Department (ED). After rate control with beta‐blockers started in the ED, an electrophysiology study revealed a counterclockwise perimitral macroreentry that terminated with a mitral isthmus ablation (Fig. 1). A cavotricuspid isthmus line and pulmonary vein isolation were additionally performed in the same procedure (Fig. 2). Retrospective serial ECGs analysis in sinus rhythm during this period, revealed progressive interatrial conduction delay or “interatrial block” (IAB), evolving from a P wave of 120 ms (partial IAB) to a P wave of 135 ms with biphasic morphology (±) in the inferior leads (advanced IAB), according to the definition of a recent consensus (Fig. 3).1, 2
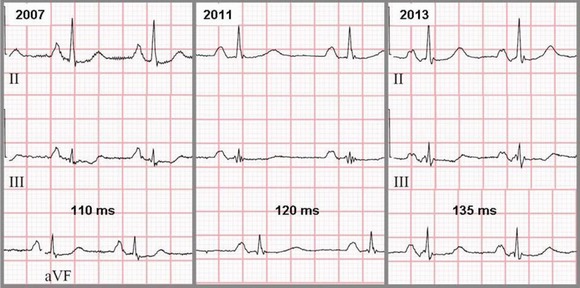
Figure 1.
Electrocardiographic progression of P‐wave width and morphology over a 6‐year period. 2007: P wave of 110 ms. 2011: P wave of 120 ms with a small negative deflection at the terminal portion. 2013: P wave of 135 ms with biphasic morphology (±) in II, III, and aVF.
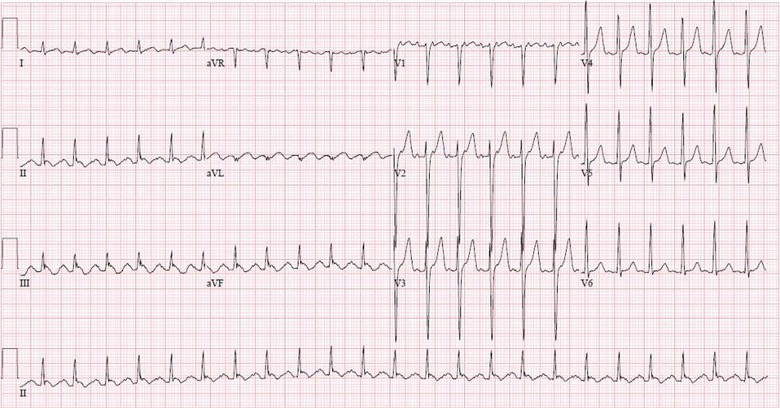
Figure 2.
Twelve‐lead ECG of left atrial tachycardia with 2:1 atrioventricular conduction.
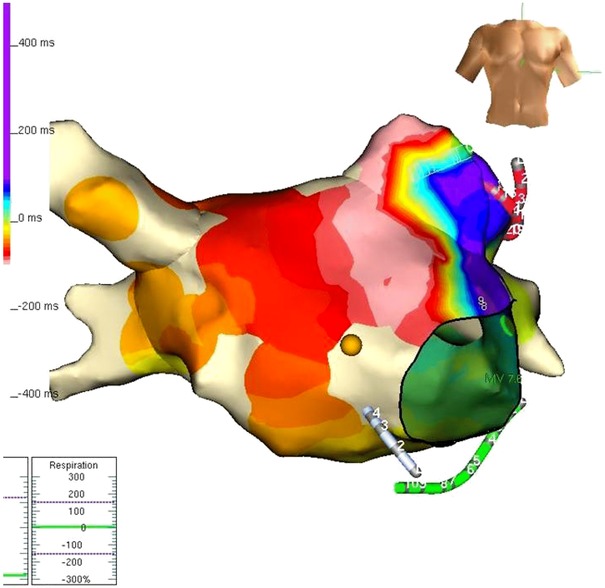
Figure 3.
Activation map of the tachycardia in NavX depicting a counterclockwise perimitral macroreentry. Colors indicate activation time from red (early) to purple (late).
Interatrial conduction disorders are frequent in patients with structural heart diseases, including hypertension, coronary disease, and hypertrophic cardiomyopathy, and they are strongly associated with atrial tachyarrhythmias, especially AF and flutter. This association was first described by Bayes de Luna3 and later confirmed by others.4, 5 Intra‐ and interatrial conduction delays lead to dispersion of refractory periods and participate in initiating and maintaining reentry circuits, facilitating atrial arrhythmias.
In this case, the changing pattern over time is a manifestation of progressive atrial remodeling and conduction delay.2 The terminal negative component of the P wave in the inferior leads suggests block of the electrical impulse in the Bachman bundle zone, with retrograde activation of the LA via muscular connections at the coronary sinus. This has been reproduced in experimental models and confirmed by endocardial mapping.
Physicians should be aware of the association between advanced IAB and development of atrial arrhythmias as its recognition could prompt early and aggressive antiarrhythmic treatment.
Disclosures: None.
REFERENCES
- 1. Bayés de Luna A, Platonov P, Cosio FG, et al. Interatrial blocks. A separate entity from left atrial enlargement: a consensus report. J Electrocardiol 2012;45:445–451. [DOI] [PubMed] [Google Scholar]
- 2. Ariyarajah V, Spodick DH. Progression of partial to advanced interatrial block. J Electrocardiol 2006;39(2):177–179 [DOI] [PubMed] [Google Scholar]
- 3. Bayés de Luna A, Cladellas M, Oter R, et al. Interatrial conduction block and retrograde activation of the left atrium and paroxysmal supraventricular tachyarrhythmia. Eur Heart J 1988;9:1112–1118. [DOI] [PubMed] [Google Scholar]
- 4. Conde D, Baranchuk A. Interatrial block as anatomical‐electrical substrate for supraventricular arrhythmias: Bayes’ syndrome. Arch Mex Cardiol 2014;84(1):32–40. [DOI] [PubMed] [Google Scholar]
- 5. Caldwell J, Koppikar S, Barake W, et al. Prolonged P‐wave duration is associated with atrial fibrillation recurrence after successful pulmonary vein isolation for paroxysmal atrial fibrillation. J Interv Card Electrophysiol 2014;39(2):131–138. [DOI] [PubMed] [Google Scholar]